Refresher in Blood Cell Morphology
Tracy I. George, MD Professor of Pathology
University of Utah

No financial conflicts of interest

Objectives
• Recognize non-neoplastic and neoplastic disorders in the peripheral blood smear
• Distinguish reactive from malignant lymphocytosis
• Discuss the differential diagnosis of cytopenias • Triage peripheral blood specimens for
appropriate ancillary testing

Examination of the Blood Smear
• A good quality smear has three zones – Feathered edge – Monolayer – Body

Case 1 46 year old male with fever, myalgias, purpura, and neutrophilia for 6 months • No splenomegaly or lymphadenopathy • Radiologic examination negative • ESR, CRP, ANA negative • Cultures of bone marrow negative WBC: 49 x 109/L Differential: neuts 96%, mono 1%, meta 1%, myelo 1%, pro 1% Hgb and PLT: normal

Case 1, Peripheral Blood Smear

Case 1

Case 1, Bone marrow aspirate smear

Case 1, Bone marrow biopsy

Case 1, Cytogenetic karyotype
BCR-ABL1 negative by RT- PCR

Case 1, CSF3R T618I

Case 1
What is your diagnosis? a. Steroid effect b. Endogenous G-CSF effect c. Chronic myeloid leukemia d. Atypical chronic myeloid leukemia e. Chronic neutrophilic leukemia

Case 1
What is your diagnosis? a. Steroid effect b. Endogenous G-CSF effect c. Chronic myeloid leukemia d. Atypical chronic myeloid leukemia e. Chronic neutrophilic leukemia

Chronic neutrophilic leukemia
• Leukocytosis ≥25 x 109/L >80% seg neuts, <10% immature grans, <1% blasts, <1 x 109/L monos, no dysgranulopoiesis
• Hypercellular marrow, <5% blasts • Hepatosplenomegaly • Exclude underlying cause for neutrophilia or
document clonality (infection, inflammation, drugs, neoplasms including plasma cell myeloma)
• Exclude: CML, PV, ET, PMF, PDGFRA/ PDGFRB /FGFR1 /PCM1-JAK2

N Engl J Med 368:1781-1790, 2013

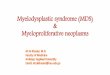
Model for Activation and Signaling of CSF3R Mutations.
Maxson JE et al. N Engl J Med 2013;368:1781-1790.

© 2016 College of American Pathologists. Materials are used with the permission of the faculty.
Chronic Neutrophilic Leukemia
• Usually indolent prognosis • Disease progression
– Increased neutrophilia – Splenomegaly – Thrombocytopenia and bleeding – Infection – Bone marrow failure – Blast phase
• JAK2 inhibitor or dasatinib depending on mutation
17 © 2016 College of American Pathologists. Materials are used with the permission of the faculty.

Other Neoplastic Neutrophilias
• Myeloproliferative neoplasms – Chronic myeloid leukemia – Other MPN (PV, ET, PMF)
• MDS/MPN – Atypical chronic myeloid leukemia – Chronic myelomonocytic leukemia

Chronic myeloid leukemia
• Associated with BCR-ABL1 translocation • Usually shows prominent left shift • Basophilia • Neutrophilic variant shows significant
maturation – Basophilia may be subtle – Associated with p230 BCR-ABL1 transcript

Chronic myeloid leukemia

Other Myeloproliferative Neoplasms
• May show erythrocytosis or thrombocytosis • Polycythemia vera shows decreased
erythropoietin • Granulocyte proliferation less than in CNL • More likely to have dacrocytes • Associated with mutations in
– JAK2 V617F – JAK2 exon 12 – CALR – MPL

Polycythemia vera

Myeloproliferative/Myelodysplastic syndromes
• Atypical chronic myeloid leukemia – Shows significant
dysplasia – >10% left shifted
granulocytes – Associated with more
significant anemia – More likely to have
SETBP1 mutation

Chronic myelomonocytic leukemia – Monocytosis >1 x
109/L and 10% of WBC
– Increased immature monocytes
– Shows significant dysplasia
– Mutations seen are not specific but can support diagnosis
Lynch DT, Hall J, Foucar K. How I investigate monocytosis. Int J Lab Hematol 2018;40:107-114.

Neoplastic Neutrophilias
• Significant elevation in neutrophils – May be >50 x 109/L
• Other CBC parameters abnormal – Cytopenias – Basophilia
• Immature forms and blasts present • Sustained over time • Clonal cytogenetic or molecular abnormality

Reactive Neutrophilias
• Neutrophils are the most abundant leukocyte • Most neutrophilias are reactive
– Infection – Inflammation – Medication – Stress – Pregnancy – Secondary to plasma cell neoplasm – Secondary to other neoplasm

Reactive Neutrophilia

Reactive Neutrophilia
• Smaller elevation in WBC – Other CBC parameters normal or mildly abnormal
• Activated changes – Toxic granulation – Vacuoles – DÖhle bodies
• Transitory • Symptoms of inflammation • Presence of other malignancy • No evidence of clonality

Case 2
• 42-year-old man with 2 wk history of shortness of breath, bleeding gums, epistaxis, tingling sensation over whole body, weight loss, weakness and strong clinical suspicion for thrombotic thrombocytopenic purpura (TTP)
WBC: 3.2 x 109/L Hgb: 4.7 g/dL MCV: 122 fL PLT: 27 x 109/L Retic: 5.9%

Case 2

Case 2

Case 2

Case 2
What is your diagnosis? a. Megaloblastic anemia b. Microangiopathic hemolytic anemia c. Myelodysplasia d. Oxidative hemolysis

Case 2
What is your diagnosis? a. Megaloblastic anemia b. Microangiopathic hemolytic anemia c. Myelodysplasia d. Oxidative hemolysis

Case 2: Additional Studies
• LDH: 1600 U/L [117-224] • Haptoglobin: <8 mg/dL [30-200] • Vitamin B12: 93 pg/mL [193-986] • Intrinsic factor antibody: positive • Parietal cell antibody: negative • MMA: 3.08 umol/L [0-0.40] • ADAMTS13 activity: 71% [>=67]

Severe vitamin B12 deficiency mimicking thrombotic thrombocytopenic purpura
JK Routh, SC Koenig. ASH image bank, 9/12/2014.

Diagnosis of Megaloblastic Anemias 1. CBC with macrocytic anemia (pancytopenia in severe cases)* 2. Peripheral blood smear:
– Oval macrocytes – Hypersegmented neutrophils – Marked anisocytosis and poikilocytosis – Can see nRBCs, schistocytes, Howell-Jolly bodies, basophilic
stippling, or Cabot rings
3. Vitamin B12 4. Folate 5. Methylmalonic acid (MMA) 6. Total homocysteine
*Some patients may present with neurologic symptoms (subacute combined cord degeneration) without anemia, macrocytosis without anemia, or neither macrocytosis nor anemia. MCV can be very high.

Vitamin B12 deficiency testing
• Patients with intrinsic factor antibodies can be vitamin B12 deficient with spuriously high measured B12 level.
• Measurement problems with vitamin B12 level assays with certain testing platforms
• When B12 levels low-normal, reflex to serum MMA
Scarpa E et al. Undetected vitamin B12 deficiency due to false normal assay results. Blood Transfus 2013;11:627-9. Merrigan SD et al. Intrinsic factor blocking antibody interference is not detected in five automated cobalamin immunoassays. Am J Clin Pathol 2014;141:701-5. Yang DR, Cook RJ. Spurious elevations of vitamin B12 with pernicious anemia. N Engl J Med 2012;366:1742-3. Carmel R, Agrawal YP. Failure of cobalamin assays in pernicious anemia. N Engl J Med 2012;367:385-6.

Differential diagnosis of macrocytic anemia
• Megaloblastic anemia • Myelodysplastic syndrome • Alcohol/liver disease • Drugs • Hypothyroidism • Hemolysis • Myeloma (spurious) • Aplastic anemia • Chronic lung disease with hypoxia • Heavy smoking • Physiological (normal neonates, subset of normal pregnancy)

Hemolysis

Hemolysis

Hemolysis
Immune mediated
Cold agglutinin disease
Warm autoimmune hemolytic anemia

Hemolysis
Intravascular hemolysis (microangiopathic hemolytic anemia)
Toxic shock syndrome Hemolytic uremic syndrome

Hemolysis
Oxidative hemolysis
Type 1 G6PD deficiency
Supravital stain Dapsone-induced hemolysis

Hemolysis
Immune mediated Intravascular hemolysis
(microangiopathic hemolytic anemia)
Oxidative hemolysis

Hemolysis follow-up • Reticulocyte count • Haptoglobin • LDH • Total bilirubin • D-dimers • Fibrinogen • Urine hemosiderin • Direct Coombs test • PT/PTT if possible DIC • ADAMSTS13 if possible TTP
Clinical history

Case 3
• 60-year-old woman with WBC: 8 x 109/L – Lymphocytes 52% – Mild neutropenia and anemia
• Long history of rheumatoid arthritis • Recurrent bacterial infections

Case 3

Case 3
Flow cytometry
T-cell gene rearrangement studies showed a clonal rearrangement

Case 3
What is your diagnosis? a. Reactive T-cell expansion due to autoimmune
disease b. Reactive T-cell expansion due to infection c. T-cell large granular lymphocytic leukemia d. Chronic NK cell leukemia e. Sezary syndrome

Case 3
What is your diagnosis? a. Reactive T-cell expansion due to autoimmune
disease b. Reactive T-cell expansion due to infection c. T-cell large granular lymphocytic leukemia d. Chronic NK cell leukemia e. Sezary syndrome

T-cell Large Granulocytic Leukemia
• Persistent, clonal proliferation of T-cell large granular lymphocytes
• 2-3% of chronic lymphocytic leukemias • Associated with autoimmune disorders
– Rheumatoid arthritis in 25% of patients
• Associated with bone marrow transplant • Likely due to chronic antigenic stimulation
– Develops following benign proliferation of T-LGLs

T-cell Large Granulocytic Leukemia
• LGLs >2 x 109/L • >15% of WBCs • Neutropenia common
– May have anemia or thrombocytopenia
• Flow immunophenotype – CD3, CD57, CD16 – Usually CD8, TCR α/β – May show loss of normal T-cell antigens

T-cell Large Granulocytic Leukemia
• Normal cytogenetics in almost all cases
• STAT3 mutation in 40% of cases – Not specific
• T-cell gene rearrangement studies positive – Testing is required in
majority of cases

T-cell Large Granulocytic Leukemia
• Heterogeneous course • Some cases spontaneously regress • Others progress and require treatment
– Progressive cytopenias – Recurrent infections – Other immune disfunctions

Other Chronic Lymphoproliferative Disorders
• B-cell disorders – Chronic lymphocytic leukemia – Monoclonal B-cell Lymphocytosis
• T-cell disorders – Sezary syndrome – T-cell prolymphocytic leukemia – Adult T-cell leukemia/lymphoma
• NK cell disorders – Chronic lymphoproliferative disorders of NK cells

B-Cell Disorders
• Chronic lymphocytic leukemia – Primary differential
diagnosis in older adult with lymphocytosis
– Usually shows small, mature lymphocytes
– Clumped chromatin – CD5+ B-cells

T-Cell Disorders
• Sezary Syndrome – Overlap with mycosis
fungoides – Primary presentation in
blood or bone marrow – Cerebriform nuclear
appearance – CD4 positive in majority
of cases

T-Cell Disorders
• T-cell prolymphocytic leukemia – Similar incidence to T-LGL
leukemia – Rapidly rising, very high
WBC count – Bulky lymphadenopathy – CD4 positive or CD4/CD8
double positive – Inv(14)(q11;q32) in 90% of
cases

T-Cell Disorders • Adult T-cell
leukemia – Very rare with
endemic disease distribution
– Associated with chronic HTLV-1 infection
– Usually CD4 and CD26 positive, CD57 negative

NK-Cell Disorders
• Chronic lymphoproliferative disorders of NK cells – Morphology
indistinguishable from LGLs
– CD2 and CD56 positive, surface CD3 negative
– T-cell clonality studies negative
– KIR receptor restricted

Reactive Granular Lymphocyte Expansions
• Viral infection – EBV, CMV most common – Morphologic spectrum of lymphocytes with reactive
features • Following stem cell transplant
– Associated with CMV infection • With autoimmune disease
– Due to chronic immune stimulation • With other neoplasm
– Solid tumor – Lymphoma

Reactive vs. Neoplastic Lymphocytosis
Features Favoring Reactive • Young age • Pleomorphic morphology
• Small mature cells, larger activated cells, LGLs, immunoblasts
• Clinical history consistent with infection
Features favoring neoplastic • Adult patients • Monomorphic morphology
• Small, round nuclei • Folded or cleaved nuclei • Convoluted nuclei • Villous cytoplasm • Plasmacytoid • Granules • Prominent nucleoli • Large cells

Case 4
• 75-year-old man presenting to ED with abdominal pain, nausea, and vomiting. Abdominal X-ray concerning for possible abdominal aortic aneurysm.
• WBC: Normal • Hgb: 9.9 g/dL • MCV: 84 fL • PLT: 56 x 109/L

Case 4

Case 4

Case 4

Case 4

Case 4

Case 4
What is your diagnosis? a. Acute myeloid leukemia b. Autoimmune hemolysis c. Intravascular hemolysis d. Myelodysplastic syndrome

Case 4
What is your diagnosis? a. Acute myeloid leukemia b. Autoimmune hemolysis c. Intravascular hemolysis d. Myelodysplastic syndrome

Best Practices: blood smear morphology
• Well prepared blood smear is key! • 200-leukocyte differential • Percentage of blasts • Auer rods in blasts: yes or no • Dysplasia: type and degree
– Granulocytes – Red blood cells – Platelets

WHO 2016/2017 Updates in MDS
WHO Tumour Classification 4th edition, IARC 2008, Arber D, Orazi A, Hasserjian R et al, Blood 2016;127:2391-405. Chart by David Steensma, MD

WHO 2016/2017 Updates in MDS
WHO Tumour Classification 4th edition, IARC 2008, Arber D, Orazi A, Hasserjian R et al, Blood 2016;127:2391-405. Chart by David Steensma, MD
Ring sideroblasts
≥ 15% of erythroid precursors
or ≥ 5% if SF3B1
mutation is present

WHO 2016/2017 Updates in MDS Dysplastic lineages
Cytopenias RS BM, PB blasts
MDS-SLD 1 1-2 <15/<5%* <5%, <1%
MDS-MLD 2-3 1-3 <15/<5%* <5%, <1%
MDS-RS-SLD 1 1-2 <15/<5%* <5%, <1%
MDS-RS-MLD 2-3 1-3 <15/<5%* <5%, <1%
Del(5q) 1-3 1-2 - <5%, <1%
MDS-EB-1 0-3 1-3 - 5-9%, 2-4%
MDS-EB-2 0-3 1-3 - 10-19%, 5-19% or Auer rods
MDS-U
+ 1% blasts 1-3 1-3 - <5%, 1%
+SLD+pancytopenia 1 3 - <5%, <1%
Based on cytog only 0 1-3 <15% <5%, <1%
RCC 1-3 1-3 none <5%, <2%
Adapted from Arber et al. Blood 2016.

But dyspoiesis can be seen with:
• Stress erythrocytosis • Autoimmune disease • Hemoglobinopathies/thalassemias • Aplastic anemia • Nutritional deficiencies • Alcohol • Medications/Toxins • Infections
DP Steensma. Dysplasia has a differential diagnosis: distinguishing genuine myelodysplastic syndromes (MDS) from mimics, imitators, copycats and imposters. Curr Hematol Malig Rep 2012;7:310-20.

Acquired sideroblastic anemia secondary to alcoholism
Hgb: 8.5 g/dL MCV: 88 fL RDW: 27.5% Normal WBC, PLT, ANC.

Acquired Pelger-Huet anomaly
Courtesy of Joan Etzell, MD
Neutropenia and morphologic changes resolved 1 month after reducing MMF dose.
Etzell JE, Wang E. Acquired Pelger-Huet anomaly in association with concomitant tacrolimus and mycophenolate mofetil in a liver transplant: a case report and review of the literature. Arch Pathol Lab Med 2006;130:93-6.

Other causes of cytopenias: a long list!
• Drugs • Collagen vascular diseases • Autoimmune disorders • Sequestration • Nutritional deficiencies • Infection • Inflammatory disorders • Hemolysis • Congenital disorders • Neoplasms

ICUS: idiopathic cytopenias of undetermined significance
• MDS is possible, but not proven • Age-related clonal hematopoiesis of
indeterminate potential (CHIP) • MDS-associated somatic mutations and clonal
hematopoiesis are common in ICUS • Clonal cytopenias of undetermined
significance (CCUS) • MDS-associated somatic mutations alone are
not diagnostic of MDS Malcovati L, Cazzola M. The shadowlands of MDS: idiopathic cytopenias of undetermined
significance (ICUS) and clonal hematopoiesis of indeterminate potential (CHIP). Hematology Am Soc Hematol Educ Program. 2015;299-307.

Clonal hematopoiesis of indeterminate potential
‘Non-clonal’ ICUS
CHIP CCUS
Clonality
Dysplasia
Cytopenias
Overall Risk
– + + – – – + – +
Very Low(?) Very Low Low (?)
BM Blast % < 5% < 5% < 5%
Lower Risk MDS
Higher Risk MDS
MDS by WHO 2008
+ + + + + +
Low High
< 5% < 19%
Traditional ICUS
Clonal Cytopenias
Treatments Obs/BSC Observation Obs/BSC/GF Obs/BSC/GF IMiD/IST
HMA/HCST
Steensma DP, Bejar R, Jaiswal S et al. Blood 2015;126:9-16.

References
• D Chabot-Richards, TI George. Leukocytosis. Int J Lab Hematol 2014;36(3):279-88.
• TI George. Malignant or Benign Leukocytosis. Hematology Am Soc Hematol Educ Program. 2012: 475-84.
• I Pereira, TI George, MD, DA Arber. Atlas of Peripheral Blood. The Primary Diagnostic Tool. Wolters Kluwer, Lippincott Williams and Wilkins, Inc., Philadelphia, PA, 2012.
Recommended