Making the Case for ACS:
Applying New Data and Guidelines to Real-World Practice
8:00 AM–3:30 PMSaturday, November 15, 2008
New York, NY
Pri-Med Clinical Focus for Cardiologists
New York, NY
November 15, 2008 8:00AM –3:30 PM
Education Sponsor Education Partner Commercial Supporters
This program is supported by educational grants from Daiichi Sankyo Inc. and Eli Lilly and Company, GlaxoSmithKline, and sanofi-aventis U.S.
Pri-Med is an M|C Communications, LLC program 101 Huntington Avenue, Boston, MA 02199 | 877.477.4633 | www.pri-med.com
Dear Clinician: Welcome to Pri-Med Clinical Focus for Cardiologists, continuing education for healthcare providers that’s focused on clinically relevant, practice and patient-care oriented issues from nationally recognized experts. What began as one live program in Boston in 1995 has developed into over 135 meetings around the country that present the latest evidence-based research and guidelines and real-life case studies, delivered by a faculty of expert speakers in an interactive learning environment. This year’s curriculum for the Pri-Med Clinical Focus for Cardiologists is comprised of practice-based topics derived from a comprehensive needs assessment and feedback from you and your colleagues—timely sessions designed to support your patient diagnoses, treatment, and management. We welcome your questions and encourage you to participate in the audience response portion of this activity. After the sessions, be sure to take advantage of our other multi-channel offerings, all of which are designed to complement the learning you’ll take away from this Pri-Med Clinical Focus for Cardiologists. For example, you can go online to Pri-Med.com and interact with thought leaders through our online CME Expert Perspectives. Whether you are a first-time attendee to one of our programs or a seasoned Pri-Med veteran, our goal remains the same: to give you a complete and targeted educational experience, one that lets you make informed decisions with greater confidence and deliver the highest levels of quality care. Thank you for joining us at Pri-Med Clinical Focus for Cardiologists. We look forward to meeting you and hearing your input throughout the program. If you have any questions about Pri-Med, please visit us on the web at www.pri-med.com. You may also contact us and share your feedback via email at [email protected]. Sincerely,
John M. Connolly Chief Executive Officer Pri-Med
Marissa Seligman, PharmD Chief Clinical & Regulatory Affairs Officer & Senior Vice President Pri-Med Institute

Pri-Med programs are owned and operated by M|C Communications, LLC located in Boston, MA. The clinical education division of M|C Communications, LLC is Pri-Med Institute, which was established in 2001 and is structured to provide accredited continuing education programs.
Pri-Med Institute Identifying the needs of health care professionals and ensuring these needs are met with world-class educational programs is the goal of Pri-Med Institute. Accredited by the ACCME and ACPE and approved as a provider of contact hours by the AANP and ANCC, Pri-Med Institute (PMI) is an integral part of Pri-Med educational programs. From needs assessment to accreditation to partnering with content collaborators, Pri-Med Institute ensures that Pri-Med continuing education programs are high-quality credited learning experiences for participants, faculty speakers, and supporters alike. Pri-Med Institute sponsors conferences as well as other innovative forms of distance education in order to contribute to the continuing professional development of health care providers. The offerings are intended to enhance physicians’ and other health care professionals’ ongoing professional development and influence their clinical practice behaviors for the purpose of improving health outcomes. Pri-Med Institute Disclosure Information Medical Advisory Board Financial Disclosure George Mejicano, MD has nothing to disclose. Victor Diaz, MD has nothing to disclose. Stephen Goldfinger, MD has nothing to disclose. Michael Bloch, MD is a member of speakers bureaus for AstraZeneca Pharmaceuticals LP, Novartis Pharmaceuticals Corporation, Pfizer Inc., and sanofi-aventis US; and receives research support from AstraZeneca Pharmaceuticals LP and Novartis Pharmaceuticals Corporation. He also receives honorarium from Pfizer Inc. and sanofi-aventis U.S.
PMI Clinical Staff, University of Wisconsin School of Medicine and Public Health Expert and Tufts Health Care Institute Peer Reviewer Financial Disclosure As a continuing medical education provider accredited by the ACCME, it is the policy of Pri-Med Institute to require any individual in a position to influence educational content to disclose the existence of any financial interest or other personal relationship with the manufacturer(s) of any commercial product(s). Pri-Med clinical staff and University of Wisconsin School of Medicine and Public Health and Tufts Health Care Institute expert content reviewers have provided financial disclosure. Carolyn Skowronski, PMI Clinical Editor, has disclosed that she owns stock in Merck. All others have no financial disclosure or conflicts of interest to resolve for each of the sessions related to this activity. Conflict of Interest Resolution Statement When individuals in a position to control content have reported financial relationships with one or more commercial interests, as listed above, Pri-Med Institute works with them to resolve such conflicts to ensure that the content presented is free of commercial bias. The content of this presentation was vetted by the following mechanisms and modified as required to meet this standard:
• Content peer review by external topic expert • Content validation by external topic expert and internal Pri-Med Institute clinical editorial staff
© 2008 M/C Communications, LLC. All rights reserved. Pri-Med is a registered trademark and KNOWLEDGE THAT TOUCHES PATIENTS is a trademark of M/C Communications, LLC. All other trademarks are the property of their respective owners.
Zorba Paster, MD is a member of speakers bureaus for Ortho-McNeil, Pfizer Inc., and T Pharmaceuticaleceives research support from Pfizer Inc., T Pharmaceutical Inc., Aventis, and
akeda s Northakeda s North America America Inc., and r
Endo Pharmaceuticals.

L E A R N E R B I L L O F R I G H T S
ri-MmeIns
ed Institute recognizes that you are a life-long learner who has chosen to engage in continuing dical education to identify or fill a gap in knowledge, skill, or performance. As part of Pri-Med titute’s duty to you as a learner, you have the right to expect that your continuing medical education
experience will include: Content that:
Is driven and based on independent survey and analysis of learner needs
Promotes improvements or quality in health care
Is current, valid, reliable, accurate, and evidence-based
Offers balanced presentations that are free of commercial bias for, or against, a product/service
Is vetted through a process that resolves any conflicts of interests of planners and faculty
Is driven and based on learning needs, not commercial interests
Addresses the stated objectives or purpose
Is evaluated for its effectiveness in meeting the identified educational need
A learning environment that:
Is based on adult learning principles that support the use of various modalities
Supports learners’ ability to meet their individual needs
Respects and attends to any special needs of the learners
Respects the diversity of groups of learners
Is free of promotional, commercial, and/or sales activities
Disclosure of:
Relevant financial relationships planners, teachers, and authors have with commercial interests related to the content of the activity
Commercial support (funding or in-kind resources) of the activity
P

Making the Case for ACS: Applying New Data and Guidelines to Real World Practice
To access the full set of presented slides, please visit www.pri-med.com/57MAN08A/syllabus and click on the “Print Syllabus” link. Upon completion of the educational activities, learners should be able to: • Outline evidence-based treatment of ACS as recommended by recently updated ACC/AHA
guidelines. • Apply strategies for improving ACS care in their own clinical practices and system(s) of care. • Discuss emerging science relative to the management of acute ACS.
8:00 – 8:05 Welcome and Introduction (E. Magnus Ohman, MD)
Session 1 8:05 – 8:50 STEMI Patient Case Simulation (Charles Pollack, MD) STEMI patient case will be introduced and, through advanced case simulation, the participants will walk through the optimal triage, diagnosis, and treatment of the patient from symptom onset to post-discharge, incorporating new evidence, guidelines, and registry data into the discussion, with regard to:
Reducing time to reperfusion Reperfusion method selection Adjunctive pharmacotherapy Discharge therapy
• Examine updated ACC/AHA STEMI guidelines. • Apply evidence-based STEMI guidelines to ACS patient scenarios. • Implement changes in your practice based on review and application of the updated STEMI
guidelines. 8:50 – 9:20 STEMI Guideline Update (E. Magnus Ohman, MD) • Examine updated ACC/AHA STEMI guidelines. • Apply evidence-based STEMI guidelines to ACS patient scenarios. • Implement changes in your practice based on review and application of the updated STEMI
guidelines. Session 2 9:20 – 9:35 Case Discussion and Q&A (Faculty and Attendees) Key learning points will be reviewed in a Q&A session with attendees. • Examine updated ACC/AHA STEMI guidelines. • Apply evidence-based STEMI guidelines to ACS patient scenario. • Implement changes in your practice based on review and application of the updated STEMI
guidelines.

Session 3 9:35 – 10:20 NSTEMI Patient Case Simulation (Attendees) NSTEMI patient case will be introduced and, through advanced case simulation, the participants will walk through the optimal triage, diagnosis, and treatment of the patient from symptom onset to post-discharge, incorporating new evidence, guidelines, and registry data into the discussion, with regard to:
Optimal diagnosis Invasive versus conservative strategy Adjunctive pharmacotherapy Discharge therapy
• Examine updated ACC/AHA UA/NSTEMI guidelines. • Apply evidence-based UA/NSTEMI guidelines to ACS patient scenarios. • Implement changes in your practice based on review and application of the updated UA/NSTEMI
guidelines. 10:20 – 10:35 Break Session 4 10:35 – 11:05 NSTEMI Guideline Update (James de Lemos, MD) • Examine updated ACC/AHA UA/NSTEMI guidelines. • Apply evidence-based UA/NSTEMI guidelines to ACS patient scenarios. • Implement changes in your practice based on review and application of the updated UA/NSTEMI
guidelines. Session 5 11:05 – 11:20 Case Discussion and Q&A (Faculty and Attendees) Key learning points will be reviewed in a Q&A session with attendees • Examine updated ACC/AHA UA/NSTEMI guidelines. • Apply evidence-based UA/NSTEMI guidelines to ACS patient scenario. • Implement changes in your practice based on review and application of the updated UA/NSTEMI
guidelines. Session 6 11:20 – 12:35 Bridging the Gap Between Emergency Medicine and Cardiology (Charles Pollack, MD) A 45-minute presentation concerning the barriers and gaps to translating new guidelines and evidence into ACS practice and ensuring continuity of care. Optimal critical care treatment for the ACS patient, as well as barriers to such treatment, will be identified utilizing interactive ARS technology to foster attendee participation and discussion of experiences in their own practice areas. 30-minute faculty-led discussion of effective practices to enhance communication and cooperation between emergency and cardiology departments, based on barriers to improved processes identified during the preceding presentation, with the overall goal of improving patient outcomes in ACS emergent medical care. • Analyze the implications of updated ACC/AHA ACS guidelines for emergency medical care.
• Enhance cooperation between the emergency department (ED) and the emergency transport team, hospital administration, catheterization laboratory, and cardiac care unit (CCU) so as to improve ACS patient care.
• Adapt quality improvement strategies and evidence-based algorithms to align STEMI and UA/NSTEMI ED practice with current scientific data.
12:35 – 1:20 Lunch Session 7 1:20 – 2:05 Bleeding and Transfusion: Recognizing the Impact on Vascular Outcomes (James de Lemos, MD) Antithrombotic/antiplatelets (existing and emerging); the link between bleeding and worse outcomes; and implications for targeting therapies to specific patients. • Delineate the implications of major bleeding in the ACS patient. • Analyze the bleeding risks posed by various therapeutic interventions in ACS. • Enumerate strategies for reducing bleeding risk in diverse ACS patients.
Session 8 2:05 – 2:35 The Future of ACS Treatment: New Therapies in Development (E. Magnus Ohman, MD) Exploration of new science related to anticoagulants and stents in development with a focus on potential effects of treatment: bioavailability, variability, predictability of response, and safety—especially within certain populations. • Identify emerging pharmacotherapies for the ACS patient. • Compare and contrast the roles of existing and evolving therapies in different ACS patient
populations.
Session 9 2:35 – 3:20 Solutions for Toughest Cases (Attendees and Faculty) Participants will be able to submit their tough cases and questions for discussion. They will be able to either submit a word file, 1-2 PowerPoint slides, or an audio or video question. Several cases will be selected for presentation and discussion. • Apply evidence-based ACS care to complex patient cases. • Probe difficult ACS issues in light of research evidence and common medical practice.
3:20 – 3:35 Final Q&A (Attendees and Faculty)
Sessions with this symbol have related Online activities. See full list following agenda or visit www.pri-med.com to reinforce your learning and earn additional CME credits.

Reinforce your learning and earn additional credits by completing these related Online CME activities
Improving MI Outcomes From Symptoms to Discharge and Beyond Complications due to cardiovascular disease are the chief cause of morbidity and mortality in the US, but recently updated treatment guidelines may improve that profile. Three patients are currently in our virtual waiting room; log on and see if you agree with the choices their clinicians make at each treatment juncture.
www.pri-med.com/activity/122948
For more Online CME from Pri-Med visit www.pri-med.com
®
TM

Making the Case for ACS: Applying New Data and Guidelines to Real-World Practice Learning Objectives
• Outline evidence-based treatment of acute coronary syndrome (ACS) as recommended by recently updated American College of Cardiology (ACC)/American Heart Association (AHA) guidelines.
• Apply strategies for improving ACS care in your own clinical practices and system(s) of care. • Discuss emerging science relative to the management of acute ACS.
Faculty
E. Magnus Ohman, MD, Chair Professor of Medicine Director, Program for Advanced Coronary Disease Duke University Medical Center Durham, North Carolina
E. Magnus Ohman, MD, received his medical degree from the Royal College of Surgeons in Dublin, Ireland, in 1981, followed by residencies in general internal medicine at St. Laurence’s Hospital and St. Vincent’s Hospital in Ireland and fellowships in cardiology at St. Laurence’s Hospital and at Duke University Medical Center. He is a Fellow of the Royal College of Physicians of Ireland, the European Society of Cardiology, and the American College of Cardiology. Dr Ohman’s clinical interests focus on interventional cardiology, the treatment of advanced/complex coronary disease, and secondary prevention. The main focus of his research is on the management of acute myocardial infarction, including the use of interventional procedures such as balloon angioplasty, intra-aortic balloon pumping, and other support devices. Through participating in and designing a number of randomized trials, he has helped crystallize the management to sustain patency of the infarct-related coronary artery in acute myocardial infarction. Furthermore, he has conducted several large multicenter clinical trials on the use of intra-aortic counterpulsation and angioplasty to better understand the pathophysiology of interventional procedures. Another major focus has been in the area of risk stratification in acute myocardial infarction. Early observations done abroad have led him to use new cardiac markers to identify high- and low-risk patients. Further research in this area will integrate early and rapid triage along with monitoring of the effect of thrombolysis after reperfusion in patients. A patent in the latter category has already been issued. His continued focus in the performance of multi-center international clinical trials has allowed him to explore different treatment strategies for the management of acute myocardial infarction from an international perspective. He has also collected angioplasty data on nearly 6000 patients from around North America to further explore international differences in the management of patients using percutaneous interventions.
James A. de Lemos, MD Director, Coronary Care Unit Parkland Memorial Hospital Director, Cardiology Fellowship Associate Professor of Medicine University of Texas Southwestern Medical School Dallas, Texas
James A. de Lemos, MD, is director of the Coronary Care Unit at Parkland Memorial Hospital and an associate professor of medicine at the University of Texas Southwestern Medical School in Dallas, where he holds the J. Fred Schoelkopf Endowed Chair in Cardiology Research. He is closely affiliated with the Thrombolysis in Myocardial Ischemia/Infarction (TIMI) research group and is an active investigator with the Donald W. Reynolds Clinical Research Center. A graduate of Harvard Medical School, Dr de Lemos completed an internal medicine residency at the University of Texas Southwestern Medical Center, where he also served as chief medical resident. He completed a fellowship in cardiovascular medicine at the Brigham and Women’s Hospital in Boston, and served on the faculty of the Brigham and Women’s Hospital and Harvard Medical School before moving to the University of Texas Southwestern Medical School. Dr de Lemos’ primary research interests include risk assessment and the management of acute and chronic coronary artery disease. Other research interests include electrocardiography as a means of assessing coronary microcirculation after thrombolysis or percutaneous coronary intervention, and the use of novel biomarkers for prognostic assessment among patients with coronary artery disease. He has worked extensively with biomarkers such as BNP, monocyte chemoattractant protein-1, and soluble CD40 ligand. Dr de Lemos was the lead author of the Z phase of the A to Z trial, investigating different cholesterol-lowering strategies in patients with ACS. Dr de Lemos is the author of more than 120 manuscripts or book chapters, and he has won several teaching awards.
Charles V. Pollack, Jr, MA, MD Professor and Chairman Department of Emergency Medicine Pennsylvania Hospital University of Pennsylvania Philadelphia, Pennsylvania
Charles Pollack, MD, is professor of emergency medicine at the University of Pennsylvania School of Medicine and is chair of emergency medicine at Pennsylvania Hospital in Philadelphia. From 1992-2001, Dr Pollack served in various positions in the Department of Emergency Medicine at Maricopa Medical Center in Phoenix, an urban, tertiary care teaching hospital affiliated with the Medical College of the University of Arizona and the Mayo Graduate School of Medicine. He was research director from 1994 to 2000, and he chaired the department from 1997 to 2001. From 2000 through mid-2001, Dr Pollack was also director of emergency medicine at Arizona Heart Hospital. He graduated summa cum laude from Emory University with bachelor’s degrees in history and chemistry and with a master’s degree in the history of science and medicine. He was also elected to Phi Beta Kappa. Dr Pollack earned his medical degree from Tulane University School of Medicine and is a member of Alpha Omega Alpha. Dr Pollack has long been active in teaching and clinical research and is an international leader in emergency medicine. He is the only physician to have received the American College of Emergency Physicians’ highest national awards in both teaching and research; he also received the national teaching award from the Council of
Emergency Medicine Residency Directors. His primary research interests are in the management of cardiopulmonary emergencies, especially acute thrombosis and acutely decompensated heart failure. He has published more than 300 original articles, reviews, editorials, book chapters, and electronic publications, and serves on the editorial boards of several journals and on the steering committees of multiple cardiology trials. Dr Pollack also lectures widely on many varied topics in emergency medicine. Dr Pollack is the PI of the new VELOCITY and EMPEROR studies, and he serves on the Executive Committee for the ongoing CHAMPION trials. Faculty Financial Disclosure Statement As a continuing medical education provider accredited by the ACCME, it is the policy of Pri-Med Institute to require any individual in a position to influence educational content to disclose the existence of any financial interest or other personal relationship with the manufacturer(s) of any commercial product(s). The presenting faculty reported the following: Dr de Lemos receives honoraria from Bristol-Myers Squibb/sanofi-aventis U.S. Dr Ohman receives grant support from Bristol-Myers Squibb; sanofi-aventis U.S.; Schering-Plough Pharmaceuticals; Millennium Pharmaceuticals; Eli Lilly and Company; Daiichi Sankyo, Inc.; and The Medicines Company; he serves as a consultant to Inovise, Liposcience, Response Biomedical, The Medicines Company, Datascope, and Abiomed; he serves on a speakers bureau for CV Therapeutics, Schering-Plough Pharmaceuticals, and The Medicines Company; and owns stock in Inovise and Medtronic. Dr Pollack receives direct research support from GlaxoSmithKline; serves on speakers bureaus for Schering-Plough Pharmaceuticals and sanofi-aventis U.S.; and serves as a consultant for sanofi-aventis U.S., Schering-Plough Pharmaceuticals, and The Medicines Company. Education Partner Financial Disclosure Statement The content collaborators at INNOVIA Education Institute have nothing to disclose. Conflict of Interest Resolution Statement When individuals in a position to control content have reported financial relationships with one or more commercial interests, as listed above, Pri-Med Institute works with them to resolve such conflicts to ensure that the content presented is free of commercial bias. The content of this presentation was vetted by the following mechanisms and modified as required to meet this standard:
• Content peer review by external topic expert • Content validation by external topic expert and internal Pri-Med Institute clinical editorial staff
Off-label/Investigational Disclosure In accordance with Pri-Med Institute policy, the audience is advised that Drs Ohman and Pollack indicated they may discuss unlabeled or unapproved use of drugs or devices. Drug List Generic Trade abciximab ReoPro acetaminophen various alteplase Activase APC (drotrecogin alfa) Xigris aspirin various atorvastatin Lipitor bivalirudin Angiomax, Cangrelor clopidogrel Plavix enoxaparin Lovenox eptifibatide Integrilin fondaparinux Arixtra hydrochlorothiazide various lisinopril Prinivil, Zestril
Generic Trade metoprolol Lopressor, Toprol-XL paclitaxel Taxol reteplase Retavase simvastatin Zocor streptokinase Streptase tenecteplase TNKase ticlopidine Ticlid tirofiban Aggrastat unfractionated heparin Tramadol Ultram

Investigational apixaban AZD6140 BX667 dabigatran (Pradaxa) DU-176b DX-9065a E5555 idraparinux INS50589 NCX-4016
otamixaban prasugrel (Effient) PRT-054021 PRT128 reviparin ridogrel S18886 SCH530348 STM (ART-123) YM150
Suggested Reading List Alexander KP, Chen AY, Roe MT, et al. Excess dosing of antiplatelet and antithrombin agents in the treatment of non-ST-segment elevation acute coronary syndromes. JAMA. 2005;294(24):3108-3016. Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons, and endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50:e1-e157. Antman EM, Anbe DT, Armstrong PW et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction – executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1999 guidelines for the management of patients with acute myocardial infarction). J Am Coll Cardiol. 2004;44(3):671-719. Antman EM, Hand M, Armstrong PW et al. 2007 Focused Update of the ACC/AHA 2004 Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: developed in collaboration With the Canadian Cardiovascular Society endorsed by the American Academy of Family Physicians: 2007 Writing Group to Review New Evidence and Update the ACC/AHA 2004 Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction, Writing on Behalf of the 2004 Writing Committee. Circulation. 2008;117(2):296-329. Antman EM, Morrow, DA, McCabe, CH et al., Enoxaparin versus unfractionated heparin with fibrinolysis for ST-elevation myocardial infarction. N Engl J Med. 2006;354(14):1477-1488. Boden WE, Eagle K, and Granger CB. Reperfusion strategies in acute ST-segment elevation myocardial infarction: a comprehensive review of contemporary management options. J Am Coll Cardiol. 2007;50(10):917-929. Cannon CP, Husted S, Harrington RA, et al. Safety, tolerability, and initial efficacy of AZD6140, the first reversible oral adenosine diphosphate receptor antagonist, compared with clopidogrel, in patients with non-ST-segment elevation acute coronary syndrome: primary results of the DISPERSE-2 trial. J Am Coll Cardiol. 2007;50(19):1844-1851. Chen ZM, Jiang LX, Chen YP et al. Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet. 2005;366:1607-1621. Ferguson JJ, Califf RM, Antman EM, et al. Enoxaparin vs unfractionated heparin in high-risk patients with non-ST-segment elevation acute coronary syndromes managed with an intended early invasive strategy: primary results of the SYNERGY randomized trial. JAMA. 2004;292(1):45-54. Fifth Organization to Assess Strategies in Acute Ischemic Syndromes Investigators, Yusuf S, Mehta SR, et al. Comparison of fondaparinux and enoxaparin in acute coronary syndromes. J Am Coll Cardiol. 2007;49:734-739.
Grines CL, Bonow RO, Casey DE, Jr., et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians. J Am Coll Cardiol. 2007;50(10):917-929. Jacobs AK, Antman EM, Ellrodt G, et al. Recommendation to develop strategies to increase the number of ST-segment-elevation myocardial infarction patients with timely access to primary percutaneous coronary intervention. Circulation. 2006;113(17):2152-2163. King SB III, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 Focused Update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention, Writing on Behalf of the 2005 Writing Committee. Circulation. 2008;117:261-295. Moscucci M, Fox KA, Cannon CP et al. Predictors of major bleeding in acute coronary syndromes: the Global Registry of Acute Coronary Events (GRACE). Eur Heart J. 2003;(20):1815-1823. Peterson ED, Roe MT, Mulgund J, et al. Association between hospital process performance and outcomes among patients with acute coronary syndromes. JAMA. 2006;295:1912-1920. Pollack CV Jr. and Braunwald E. 2007 update to the ACC/AHA guidelines for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: implications for emergency department practice. Ann Emerg Med. 2008;51(5):591-606. Pollack CV Jr., Antman EM, and Hollander JE. 2007 focused update to the ACC/AHA guidelines for the management of patients with ST-segment elevation myocardial infarction: implications for emergency department practice. Ann Emerg Med. May 31, 2008 [Epub ahead of print]. Rao SV, O’Grady K, Pieper KS, et al. Impact of bleeding severity on clinical outcomes among patients with acute coronary syndromes. Am J Cardiol. 2005;96(9):1200-1206. Sabatine MS, Morrow DA, Montalescot G, et al. Angiographic and clinical outcomes in patients receiving low-molecular-weight heparin versus unfractionated heparin in ST-elevation myocardial infarction treated with fibrinolytics in the CLARITY-TIMI 28 Trial. Circulation. 2005;112:3846-3854. Spencer FA, Moscucci M, Granger CG et al. Does comorbidity account for the excess mortality in patients with major bleeding in acute myocardial infarction? Circulation. 2007;116(24):2793-2801. Steinhubl SR, Kastrati A, and Berger PB. Variation in the definitions of bleeding in clinical trials of patients with acute coronary syndromes and undergoing percutaneous coronary interventions and its impact on the apparent safety of antithrombotic drugs. Am Heart J. 2007;154(1):3-11. Steinhubl SR, Schneider DJ, Berger PB, et al. Determining the efficacy of antiplatelet therapies for the individual: lessons from clinical trials. J Thromb Thrombolysis. 2008;26(1):8-13. Stone GW, Ware JH, Bertrand ME, et al. Antithrombotic strategies in patients with acute coronary syndromes undergoing early invasive management: one-year results from the ACUITY trial. JAMA. 2007;298(21):2497-2506. Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007;357:2001-2015. Yusuf S, Mehta SR, Chrolavicius S, et al. Effects of fondaparinux on mortality and reinfarction in patients with acute ST-segment elevation myocardial infarction: the OASIS-6 randomized trial. JAMA. 2006;295(13):1519-1530.

Disclosure Policy
It is the policy of the Pri-Med Institute and M|C Communications, LLC, to ensure balance, independence, objectivity and scientific rigor in all its sponsored educational programs. All faculty participating in the sponsored programs are expected to disclose to the program audiences any real or apparent conflict(s) of interest related to the content of their presentation(s).
During the course of their presentations, the faculty may mention uses of products that have not been approved in the United States for the indication being discussed. Faculty have been instructed to notify participants when they are discussing unapproved uses or investigational agents. Views presented during this program related to unapproved uses of products are solely those of the presenter and are not endorsed by Pri-Med Institute or M|C Communications, LLC.
Copyright notice: No part of the Pri-Med Clinical Focus for Cardiologists syllabus may be reproduced or otherwise incorporated into any information retrieval system, without the written permission of Pri-Med Institute, a division of M|C Communications, LLC.
The opinions, ideas, recommendations, and perspectives expressed in the syllabus and accompanying presentations for Pri-Med Clinical Focus for Cardiologists are those of the faculty only and do not necessarily reflect the opinions, ideas, recommendations or perspectives of their affiliated institutions, Pri-Med Institute, Pri-Med Institute Advisory Boards and Consultants, M|C Communications, LLC, or commercial supporters. Clinical judgment must guide each clinician in weighing the benefit of any diagnostic intervention or treatment approach or intervention against the risk of the intervention or treatment. Dosage, indications and methods of use for products referred to in this activity are not necessarily the same as indicated in the package insert for the product and may reflect the clinical experience or expertise of the individual faculty speaker. Any diagnostic procedures or treatments should not be utilized by clinicians or other healthcare professionals without evaluation of their patients’ conditions, and of possible contraindications or risks and without a review of any applicable manufacturer's product information and comparison with the recommendations of other authorities. Copyright notice: No part of the Pri-Med Clinical Focus for Cardiologists syllabus may be reproduced, distributed or otherwise incorporated into any information retrieval system, without the written permission of Pri-Med Institute, a division of M|C Communications, LLC.
Check out your CME Tracker at Pri-Med.com today: www.Pri-Med.com
Getting your CME certifi cate from any Pri-Med live program
is easier than ever. By visiting Pri-Med.com, you can quickly
see what credits you’ve earned, and then print or save your
certifi cates.
How does it work? We simply send you an email when
your certifi cate is online and ready to print. See other side
for easy instructions on how to print your certifi cate(s)
on Pri-Med.com
www.Pri-Med.com
Our CME tracker lets you:
• Store an electronic library
of your CME certifi cates
• Print and download
your certifi cate as soon
as it’s ready
• Print a summary of
credits earned to submit
to licensing board
• Enter non-Pri-Med CME
activities for a complete
summary of all of your
credits earned through
the year
Get your CME certifi cates faster with Pri-Med’s online CME Tracker.
®
TM

Visit www.Pri-Med.com today
HOW TO PRINT YOUR CERTIFICATE IN THREE EASY STEPS:
1
2
Visit www.Pri-Med.com. Log in using your
username and password** Our improved “Forgot My Password”
management can help you retrieve a forgotten username or password.
Scroll down to “Credit Summary” at the bottom of the page and click “View All.”
Once logged in, you’ll see your “Summary of Credits Earned.” Click on “Print Certifi cate.” After opening your certifi cate, you can print it and/or save it to your computer.
3

NatioNal Schedule FoR PRiMaRY caRe®
TM
dates subject to change. 6/08
Pri-Med Conference & ExhibitionFor over 14 years, Pri-Med conference & exhibition has provided continuing medical education on the best available patient care practices as well as insights into the latest advances in research, treatment protocols, and technology that physicians will need to deliver cutting-edge medical care. over the course of Pre-conference Symposia day* and 3 core Program days, Pri-Med conference & exhibition provides a diverse spectrum of learning opportunities from national experts in 1 place, offering up to 30 AMA PRA Category 1 Credit(s)™.
CITY DATES Pri-Med New York New York, NY october 2-5, 2008 Pri-Med east Boston, Ma November 6-9, 2008 Pri-Med Mid-atlantic Baltimore, Md december 3-6, 2008 Pri-Med South Fort lauderdale, Fl February 12-15, 2009 Pri-Med Midwest Rosemont, il March 4-7, 2009 Pri-Med Southwest houston, tX March 18-21, 2009 Pri-Med West anaheim, ca May 6-9, 2009
Pri-Med Updates – The Next GenerationPri-Med updates features the latest practice-based education. Now, experience an enhanced cMe environment while also benefiting from opportunities to engage in interactive non-cMe activities. in addition to a prominent keynote speaker, you’ll experience 2 track-based, information-filled days of therapeutically aligned cMe content and informative discussions around the most advanced clinical updates and treatment options.
Plus, for the first time, we’re providing an innovative networking area where you can meet with industry representatives. With individual interactions and group presentations, you’ll get the latest, most up-to-date perspectives on practice and patient care management in multiple clinical areas. earn up to 13.5 complimentary AMA PRA Category 1 Credit(s)™.
FALL 2008 cincinnati, oh october 29-30 houston, tX September 19-20 long Beach, ca october 10-11
Pri-Med Updates and Conference & Exhibition Locations
Pri-Med UpdatesPri-Med updates is designed to reflect the practitioner’s patient appointment schedule. the curriculum is composed of different sessions, each focused on a specific clinical condition and each presented by nationally recognized speakers. Sessions include didactic presentations as well as interactive, case-based learning opportunities. earn complimentary AMA PRA Category 1 Credit(s)™ or aaNP contact hours.
FALL 2008 atlanta, Ga december 2-3 charlotte, Nc September 3-4 chicago, il december 2-3 dallas, tX September 23-24 dearborn, Mi october 28-29 los angeles, ca November 13-14 Melville, NY November 19-20 Minneapolis, MN September 19 New orleans, la October 23-24 oakbrook, il october 30-31 orlando, Fl November 6-7 Philadelphia, Pa November 4-5 Phoenix, aZ october 2 Pittsburgh, Pa december 11-12 Portland, oR october 22 Princeton, NJ September 4-5 San Jose, ca November 19 Seattle, Wa September 26 St louis, Mo November 13-14 tampa, Fl december 4 Washington, dc october 16-17
For a complete list of Pri-Med events or to register, visit www.pri-med.com or call 877-477-4633.
Welcome to Pri-Med®, the industry leader in continuing Medical education. our mission is to help you access the best medical education available and we want to make it easy for you to do so. through our partnerships with leading academic institutions and teaching centers—including the faculty and thought leaders on the front lines of discovery and patient care—we bring you comprehensive continuing medical education curriculums delivered through live meetings, print publications on a monthly and quarterly basis, and online platforms with new content added daily. We have created this national schedule to highlight the cMe opportunities available to you throughout the year.
* This activity is sponsored by Pri-Med Institute.
NatioNal Schedule FoR PRiMaRY caRe®
TM
Diabetes In Depth diabetes in depth is a cMe program designed to meet the education and practice needs of clinicians who regularly diagnose and manage patients with diabetes. at every session, leading experts will provide world-class information on the comorbidities and risk factors associated with diabetes. earn up to 8.5 complimentary AMA PRA Category 1 Credit(s)™ or aaNP contact hours.
Presented in collaboration with the American Diabetes Association
FALL 2008cleveland, oh december 11houston, tX November 8Kansas city, Mo october 25Melville, NY december 10Nashville, tN November 22Phoenix, aZ November 6 Pittsburgh, Pa September 25 Rosemont, il September 4San diego, ca october 24tampa, Fl october 18
Clinical Focus in Cardiovascular Risk
Join faculty from the american college of cardiology Foundation (accF) in this 31/2-hour session focused on cardiovascular risk stratification and evidence-based primary prevention approaches and strategies. the accF, the leading cardiovascular educator, recognizes the pivotal role that primary care physicians play in managing the burden of cardiovascular disease and developed this interactive, case-based program to help improve patient outcomes. earn up to 3.5 complimentary AMA PRA Category 1 Credit(s)™ or aaNP contact hours.
Co-sponsored by Pri-Med Institute and the American College of Cardiology Foundation
FALL 2008dallas, tX September 25Melville, NY November 21 orlando, Fl November 8Phoenix, aZ october 3Seattle, Wa September 27Washington, dc october 18
Pri-Med Clinical Focus in ADHD
Pri-Med clinical Focus in adhd is a 3-hour, in-depth session dedicated to innovations in attention-deficit/hyperactivity disorder management. the curriculum will feature case-based patient simulation provided by a faculty composed of primary care physicians, psychiatrists, and pediatricians. earn up to 3 complimentary AMA PRA Category 1 Credit(s)™ or aaNP contact hours.
FALL 2008dallas, tX September 25Melville, NY November 21Washington, dc october 18
Online CME
over 300 no-cost online cMe activities covering key therapeutic topics in primary care help extend the learning of topics presented at live programs. thoroughly examine any topic through 4 learning formats: patient case studies, clinical reviews, expert perspectives, and slide lecture series.
certified for category 1 credit toward the aMa Physician’s Recognition award. Select activities are certified for aaNP contact hours, which includes hours of pharmacology.
Print CME
Primary care–focused cMe publications available online:
Pri-Med in Practice, a 12- to 16-page newsletter covering key topics in primary care.
Pri-Med Pocket Guides, a series of 32- to 48-page single-topic reference guides.
Pri-Med Hospital CME, poster-sized cMe designed to promote improvements in hospital care.
For a complete list of Pri-Med events or to register, visit www.pri-med.com or call 877-477-4633.

STATE OF THE UNION: NEW YORK HEALTH FACTS
Totals for the Top Five Causes of Death** for
New York, 2005
Rank Cause of Death Totals
- All Causes 150,987 1 Diseases of the Heart 52,002 2 Malignant Neoplasms (Cancer) 35,303 3 Chronic Lower Respiratory Diseases 6,805 4 Cerebrovascular Disease 6,566 5 Influenza and Pneumonia 5,549
** Data based on continuous file of records received from the States and does not include contributory diagnoses
Sources: Vital Statistics of New York State-2005 Tables. New York Department of Public
Health; 2008.
Comparison of Health Statistics: New York vs. US Cigarette Smoking Rate by Gender, 2007
NY% vs. US% Male 21 21 Female 16 17 Number of Deaths: Rate per 100,000 Population by Race/Ethnicity, 2004
NY% vs. US White 732 786 Black 810 1027 Other 376 478
Number of Diabetes Deaths: Rate per 100,000 Population by Race/Ethnicity, 2005
NY% vs. US White 17 23 Black 38 47 Other 12 21 Number of Heart Disease Deaths: Rate per 100,000 Population by Race/Ethnicity, 2004
NY vs. US White 246 213 Black 276 281 Other 134 123
Pri-Med Institute Health Facts November 2008

Number of Stroke and other Cerebrovascular Disease Deaths: Rate per 100,000 Population by Race/Ethnicity, 2004
NY vs. US White 33 48 Black 33 70 Other 23 40
Overweight and Obesity Rate by Race/Ethnicity, 2007
*Not Sufficient Data
NY% vs. US% White 58 59 Black 64 69 Hispanic 62 62 Asian/ Pacific Islander NSD* 38 American Indian/ Alaska Native NSD* 63 Other 60 60
Number of Cancer Deaths: Rate per 100,000 Population by Race/Ethnicity, 2004
NY vs. US White 183 189 Black 182 232 Other 97 115
Percent of Mothers Beginning Prenatal Care in the First Trimester by Race/Ethnicity, 2004
NY% vs. US% White 82 89 Black 61 77 Hispanic 61 78 Total 77 84
Statistical Sources for facts and figures: 1) New York State Department of Health. http://www.health.state.ny.us/. Accessed 6/20/08. 2) Centers for Disease Control and Prevention, Behavioral Risk Factor Surveillance System Survey Data (BRFSS),
2007, unpublished data. Information about the BRFSS is available at http://www.cdc.gov/brfss/index.htm. 3) United States Department of Health and Human Services (US DHHS), Centers for Disease Control and
Prevention (CDC), National Center for Health Statistics (NCHS), Compressed Mortality File (CMF) compiled from 1999-2004, Series 20, No. 2J 2007 on CDC WONDER On-line Database, queried November 2007.
4) United States Department of Health and Human Services (US DHHS), Centers for Disease Control and Prevention (CDC), National Center for Health Statistics (NCHS), Compressed Mortality File (CMF) compiled from 2005, Series 20, No. 2K 2008 on CDC WONDER On-line Database.
5) United States Department of Health and Human Services (US DHHS), Centers for Disease Control and Prevention (CDC), National Center for Health Statistics (NCHS), Compressed Mortality File (CMF) compiled from 1999-2004, CDC WONDER On-line Database.
6) Centers for Disease Control and Prevention, Behavioral Risk Factor Surveillance System Survey Data, 2007, unpublished data. Information about the BRFSS is available at http://www.cdc.gov/brfss/index.htm.
7) United States Department of Health and Human Services (US DHHS), Centers for Disease Control and Prevention (CDC), National Center for Health Statistics (NCHS), Compressed Mortality File (CMF) compiled from 1999-2004,CDC WONDER On-line Database.
8) Martin JA, et. al., Births: Final Data for 2004, Table 26(a) and Table 26(b), National Vital Statistics Report, Vol. 55, No. 1, September 29, 2006, Division of Vital Statistics, National Center for Health Statistics. Available at http://www.cdc.gov/nchs/data/nvsr/nvsr55/nvsr55_01.pdf.
Pri-Med Institute Health Facts November 2008
Acute Coronary Syndrome
• Coronary heart disease (CHD) caused 1 in 5 US deaths in 2004. o Single largest killer of American men and women o 50% of men and 64% of women who die suddenly of CHD had no previous symptoms
• While in-hospital acute myocardial infarction (MI) mortality declined by more than 15% in the last decade, it remains approximately 10%.
• Mortality increases for every 30 minutes that elapse before an ST-segment elevation myocardial infarction patient is treated.
• In the United States, approximately 850,000 drug-eluting stents (DES) are used each year. o Average number of stents per patient: 1.45 o 60% of DES usage is off-label
• The number of discharges with ACS from hospitals in 2004 was 840,000. o Of these, an estimated 476,000 are male and 364,000 were female. o This figure was derived by adding the first-listed inpatient hospital discharges for MI
(732,000) to those for unstable angina (108,000) • When including secondary discharge diagnoses in 2004, the corresponding numbers of inpatient
hospital discharges were: o 1.57 million unique hospitalizations for ACS o 896,000 for MI o 669,000 for unstable angina o 21,000 hospitalizations received both diagnoses
• According to studies, 21% of ACS patients have ST-elevation MI. • Comorbidities are typically more frequent in women; previous coronary disease and typical anginal
pain on admission are more frequent in men. AHA Statistics Committee and Stroke Subcommittee. Heart Disease and Stroke Statistics--2007 Update. Published online Dec 28, 2006. Available at: http://circ.ahajournals.org. Wiviott SD, Morrow DA, Frederick PD, et al. Performance of the thrombolysis in myocardial infarction risk index in the National Registry of Myocardial Infarction-3 and -4: a simple index that predicts mortality in ST-segment elevation myocardial infarction. J Am Coll Cardiol. 2004;44:783-789.
®
TM
Notes ___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
®
TM
Notes ___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________

®
TM
Notes ___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
®
TM
Notes ___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
®
TM
Notes ___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
®
TM
Notes ___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________

1
Accredited Provider:
Pri-Med Institute
Session: 8:00 AM – 3:35 PM
Making the Case for ACS:Applying New Data and Guidelines to
Real-World Practice
Speakers:E. Magnus Ohman, MDJames A. de Lemos, MD
Charles V. Pollack, Jr., MD
Accredited Provider:
Pri-Med Institute
Presenter Disclosure InformationThe following relationships exist related to this presentation:
Off Label/Investigational DiscussionIn accordance with Pri-Med Institute policy, faculty have been asked to disclose discussion of unlabeled or unapproved use(s) of drugs or devices during the course of their presentations.
Dr. de Lemos has received honoraria from Bristol-Myers Squibb/sanofi-aventis.
Dr. Ohman has received grant support from Bristol-Myers Squibb, sanofi-aventis U.S., Schering-Plough Pharmaceuticals, Millennium Pharmaceuticals, Eli Lilly and Company, Daiichi Sankyo, Inc., and The Medicines Company; has served as a consultant to Inovise, Liposcience, Response Biomedical, The Medicines Company, Datascope, and Abiomed; has served on a speakers bureau for CV Therapeutics, Schering-Plough Pharmaceuticals, and The Medicines Company; and owns stock in Inovise and Medtronic.
Dr. Pollack has received direct research support from GlaxoSmithKline; has served on speakers’ bureaus for Schering-Plough and sanofi-aventis; and has served as a consultant for sanofi-aventis, Schering-Plough, and The Medicines Company.
Making the Case for ACS:Applying New Data and Guidelines to
Real‐world Practice
•Outline evidence‐based treatment of ACS as recommended by recently
updated ACC/AHA guidelines
•Apply strategies for improving ACS care in your own clinical
practices and system(s) of care
•Discuss emerging science relative to the management
of acute ACS
Learning Objectives
What degree of improvement is required for the treatment of acute myocardial infarction in the US?
1. A great deal2. A fair amount 3. Somewhat4. Not at all
STEMI Patient Simulation
Charles V. Pollack Jr., MDProfessor and Chairman
Department of Emergency MedicinePennsylvania Hospital
Philadelphia, PA

2
2007 ACC/AHA STEMI Focused Update
E. Magnus Ohman, MDDirector, Program for Advanced Coronary Disease
Duke University Medical CenterDurham, NC
•Examine updated ACC/AHA STEMI guidelines
•Apply evidence‐based STEMI guidelines to ACS patient
scenarios
•Implement changes in your practice based on review and
application of the updated STEMI guidelines
Learning Objectives
Antman EM, et al. Circulation. 2004;110:588-636.
Antman EM, et al. Circulation. 2008;117:296-329.
Class I
Benefit >>> Risk
Procedure/ Treatment SHOULD be performed/ administered
Class IIa
Benefit >> RiskAdditional studies with focused objectives needed
IT IS REASONABLE to perform procedure/administer treatment
Class IIb
Benefit ≥ RiskAdditional studies with broad objectives needed; Additional registry data would be helpful
Procedure/Treatment MAY BE CONSIDERED
Class III
Risk ≥ BenefitNo additional studies needed
Procedure/Treatment should NOT be performed/administeredSINCE IT IS NOT HELPFUL AND MAY BE HARMFUL
Applying Classification of Recommendations and Level of Evidence
Level A: Recommendation based on evidence from multiple randomized trials or meta-analyses Multiple (3-5) population risk strata evaluated; General consistency of direction and magnitude of effect
Level B: Recommendation based on evidence from a single randomized trial or non-randomized studies Limited (2-3) population risk strata evaluated
Level C: Recommendation based on expert opinion, case studies, or standard-of-care Very limited (1-2) population risk strata evaluated
Beta-Blockers
Effects of Metoprolol
Chen ZM, Pan, HC, Chen YP, et al. Lancet. 2005;366:1622-1632.
Death13%
P=0.0006
ReMI22%
P=0.0002
VF15%
P=0.002
Totality of Evidence (N=52,411)COMMIT (N=45,852)
Increased early risk of
shock
Risk factors for cardiogenic shock: heart failure, age > 70, systolic blood pressure < 120, sinus tachycardia > 110 or heart rate < 60, increased time since onset of STEMI symptoms
3
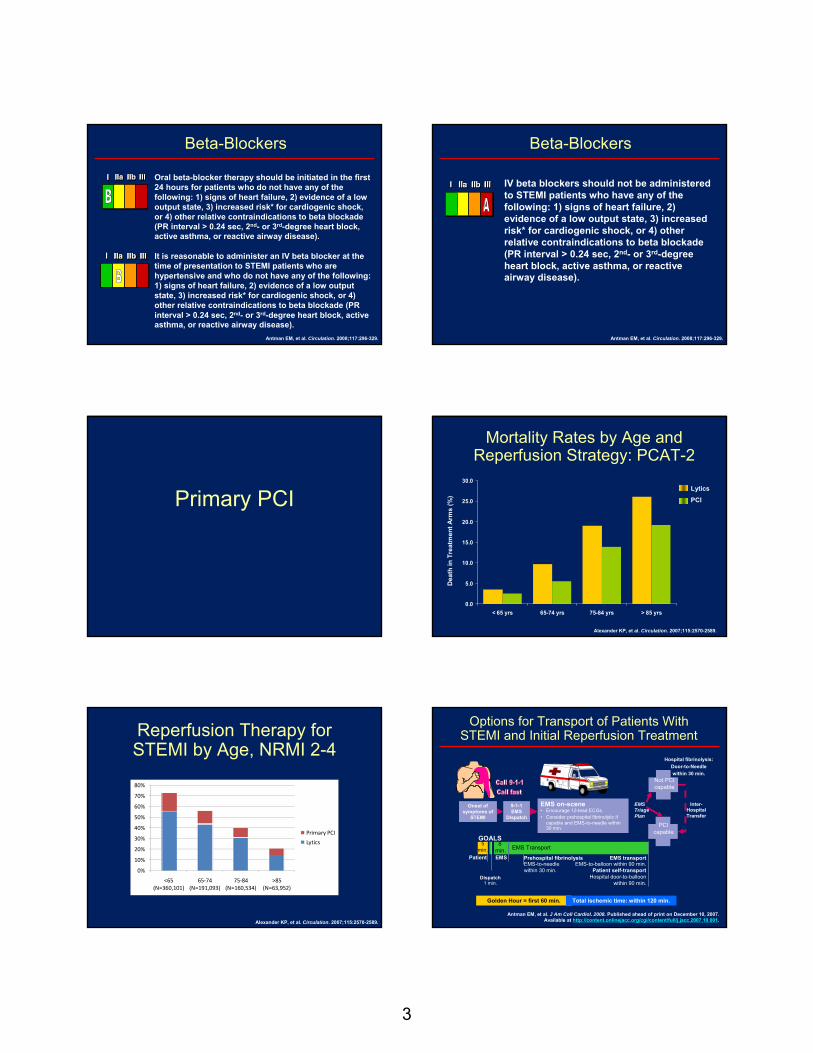
Oral beta-blocker therapy should be initiated in the first 24 hours for patients who do not have any of the following: 1) signs of heart failure, 2) evidence of a low output state, 3) increased risk* for cardiogenic shock, or 4) other relative contraindications to beta blockade (PR interval > 0.24 sec, 2nd- or 3rd-degree heart block, active asthma, or reactive airway disease).
It is reasonable to administer an IV beta blocker at the time of presentation to STEMI patients who are hypertensive and who do not have any of the following: 1) signs of heart failure, 2) evidence of a low output state, 3) increased risk* for cardiogenic shock, or 4) other relative contraindications to beta blockade (PR interval > 0.24 sec, 2nd- or 3rd-degree heart block, active asthma, or reactive airway disease).
Beta-Blockers
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.
IV beta blockers should not be administered to STEMI patients who have any of the following: 1) signs of heart failure, 2) evidence of a low output state, 3) increased risk* for cardiogenic shock, or 4) other relative contraindications to beta blockade (PR interval > 0.24 sec, 2nd- or 3rd-degree heart block, active asthma, or reactive airway disease).
Beta-Blockers
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.
Primary PCI
Mortality Rates by Age and Reperfusion Strategy: PCAT-2
Alexander KP, et al. Circulation. 2007;115:2570-2589.
0.0
5.0
10.0
15.0
20.0
25.0
30.0
< 65 yrs 65-74 yrs 75-84 yrs > 85 yrs
Dea
th in
Tre
atm
ent A
rms
(%)
Lytics
PCI
Reperfusion Therapy for STEMI by Age, NRMI 2-4
0%
10%
20%
30%
40%
50%
60%
70%
80%
<65 (N=360,101)
65‐74 (N=191,093)
75‐84 (N=160,534)
>85 (N=63,952)
Primary PCI
Lytics
Alexander KP, et al. Circulation. 2007;115:2570-2589.
Options for Transport of Patients With STEMI and Initial Reperfusion Treatment
EMS Transport
Onset of symptoms of
STEMI
9-1-1EMS
Dispatch
EMS on-scene• Encourage 12-lead ECGs.• Consider prehospital fibrinolytic if
capable and EMS-to-needle within 30 min.
GOALS
PCIcapable
Not PCIcapable
Hospital fibrinolysis: Door-to-Needle within 30 min.
EMS Triage Plan
Inter-HospitalTransfer
Golden Hour = first 60 min. Total ischemic time: within 120 min.
Patient EMS Prehospital fibrinolysisEMS-to-needlewithin 30 min.
EMS transportEMS-to-balloon within 90 min.
Patient self-transportHospital door-to-balloon
within 90 min.Dispatch
1 min.
5 min.
8 min.
Antman EM, et al. J Am Coll Cardiol. 2008. Published ahead of print on December 10, 2007. Available at http://content.onlinejacc.org/cgi/content/full/j.jacc.2007.10.001.

4
Primary PCI
STEMI patients presenting to a hospital with PCI capability should be treated with primary PCI within 90 min of first medical contact as a systems goal.
STEMI patients presenting to a hospital without PCI capability, and who cannot be transferred to a PCI center and undergo PCI within 90 min of first medical contact, should be treated with fibrinolytic therapy within 30 min of hospital presentation as a systems goal, unless fibrinolytic therapy is contraindicated.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.
Facilitated PCI
Meta-analysis: Facilitated PCI vsPrimary PCI
1.03(0.15-7.13)
3.07(0.18-52.0)
1.43(1.01-2.02)
1.03(0.49-2.17)
Mortality Reinfarction Major Bleeding
Fac. PCIBetter
PPCIBetter
Fac. PCIBetter
PPCIBetter
Fac. PCIBetter
PPCIBetter
Keeley E, et al. Lancet. 2006;367:579.
0.1 1 10 0.1 1 10 0.1 1 10
1.38 (1.01-1.87)
1.71(1.16 - 2.51)
1.51(1.10 - 2.08 )
Lytic alone N=2953
IIb/IIIa alone N=1148
Lytic +IIb/IIIaN=399
All (N=4500)
1.40 (0.49-3.98)
1.81 (1.19-2.77)
A planned reperfusion strategy using full-dose fibrinolytic therapy followed by immediate PCI is not recommended and may be harmful.
Facilitated PCI using regimens other than full-dose fibrinolytic therapy might be considered as a reperfusion strategy when all of the following are present:a. Patients are at high risk,b. PCI is not immediately available within 90 minutes, andc. Bleeding risk is low (younger age, absence of poorly controlled hypertension, normal body weight).
Facilitated PCI
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.
Rescue PCI
Wijeysundera HC, et al. J Am Coll Cardiol. 2007;49:422-430.
Meta-analysis: Rescue PCI vs Conservative Tx
Outcome Rescue PCI Conservative Treatment
RR (95% CI) P
Mortality, %(n)
7.3(454)
10.4(457)
0.69(0.46–1.05)
.09
HF, % (n)
12.7(424)
17.8(427)
0.73(0.54–1.00)
.05
Reinfarction,% (n)
6.1(346)
10.7(354)
0.58(0.35–0.97)
.04
Stroke, % (n) 3.4(297)
0.7(295)
4.98(1.10–22.48)
.04
Minor bleeding,% (n)
16.6(313)
3.6(307)
4.58(2.46–8.55)
<.001
In 3 trials, enrolling 700 patients that reported the composite end point of all-cause mortality, reinfarction, and HF, rescue PCI was associated with a significant RR reduction of 28% (RR 0.72; 95% CI, 0.59-0.88; P=.001)

5
A strategy of coronary angiography with intent toperform PCI (or emergency CABG) isrecommended in patients who have receivedfibrinolytic therapy and have:
a. Cardiogenic shock in patients < 75 years who are suitable candidates for revascularization
b. Severe congestive heart failure and/or pulmonary edema (Killip class III)
c. Hemodynamically compromising ventricular arrhythmias.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Rescue PCI
Antman EM, et al. Circulation. 2008;117:296-329.
Rescue PCI
Reasonable in patients ≥ 75 years who havereceived fibrinolytic therapy, and are incardiogenic shock, provided they are suitablecandidates for revascularization.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII Reasonable for patients in whom fibrinolytic therapy has failed and a moderate or large area of myocardium at risk [anterior MI, inferior MI with right ventricular involvement or precordial ST-segment depression].
Rescue PCI
Might be reasonable in the absence of any of the above Class I or IIa indications in moderate- or high-risk patients, but its benefits and risks are not well established. The benefits of rescue PCI are greater the earlier it is initiated after the onset of ischemic discomfort.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.
Anticoagulants
Unfractionated Heparin
Indirect thrombin inhibitor so does not inhibit clot-bound thrombin Nonspecific binding to:― Serine proteases― Endothelial cells
(can lead to variability in level of anticoagulation)
Reduced effect in ACS― Inhibited by PF-4
Causes platelet aggregation
Nonlinear pharmacokinetics
Risk of HIT
DisadvantagesImmediate anticoagulation
Multiple sites of action in coagulation cascade
Long history of successful clinical use
Readily monitored by aPTTand ACT
Advantages
aPTT=activated partial thromboplastin time; ACT=activated coagulation time; PF-4=platelet factor 4; HIT=heparin-induced thrombocytopenia.
Hirsh J, et al. Circulation. 2001;103:2994-3018.
ExTRACT-TIMI 25: Primary End Point (ITT) Death or Nonfatal MI
0
3
6
9
12
15
0 5 10 15 20 25 30
Prim
ary
End
Poin
t (%
)
Enoxaparin
UFH
Relative Risk0.83 (95% CI, 0.77 to 0.90)
P<.001
Days after Randomization
9.9%
12.0%
Lost to follow-up = 3
17% RRR
Adapted with permission from Antman EM, et al. N Engl J Med. 2006;354:1477-1488.
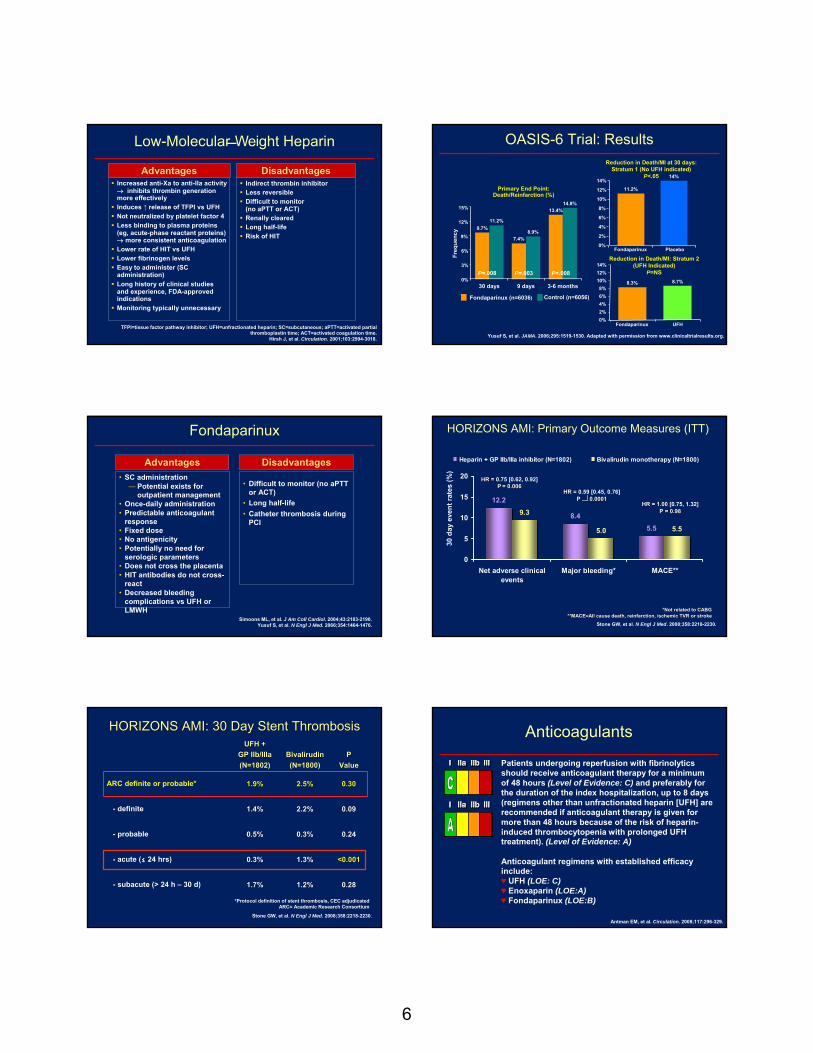
6
Low-MolecularWeight Heparin
Indirect thrombin inhibitorLess reversibleDifficult to monitor(no aPTT or ACT)Renally clearedLong half-lifeRisk of HIT
DisadvantagesIncreased anti-Xa to anti-IIa activity → inhibits thrombin generation more effectivelyInduces ↑ release of TFPI vs UFH Not neutralized by platelet factor 4Less binding to plasma proteins (eg, acute-phase reactant proteins) → more consistent anticoagulationLower rate of HIT vs UFH Lower fibrinogen levels Easy to administer (SC administration)Long history of clinical studies and experience, FDA-approved indicationsMonitoring typically unnecessary
Advantages
TFPI=tissue factor pathway inhibitor; UFH=unfractionated heparin; SC=subcutaneous; aPTT=activated partial thromboplastin time; ACT=activated coagulation time.
Hirsh J, et al. Circulation. 2001;103:2994-3018.
OASIS-6 Trial: Results
15%
Primary End Point: Death/Reinfarction (%)
P=.008 P=.003 P=.008
Freq
uenc
y
12%
9%
6%
3%
0%
9.7%11.2%
7.4%8.9%
13.4%14.8%
30 days 9 days 3-6 months
Fondaparinux (n=6036) Control (n=6056)
14%
Reduction in Death/MI at 30 days: Stratum 1 (No UFH indicated)
P<.05
Reduction in Death/MI: Stratum 2(UFH Indicated)
P=NS
p=0.97p=0.97
12%
10%
8%
6%
4%
2%
0%
11.2%
14%
Fondaparinux Placebo
14%12%10%8%6%4%2%0%
Fondaparinux UFH
8.3% 8.7%
Yusuf S, et al. JAMA. 2006;295:1519-1530. Adapted with permission from www.clinicaltrialresults.org.
Fondaparinux
• Difficult to monitor (no aPTTor ACT)
• Long half-life• Catheter thrombosis during
PCI
DisadvantagesAdvantages• SC administration
― Potential exists for outpatient management
• Once-daily administration• Predictable anticoagulant
response• Fixed dose• No antigenicity• Potentially no need for
serologic parameters• Does not cross the placenta• HIT antibodies do not cross-
react• Decreased bleeding
complications vs UFH or LMWH
Simoons ML, et al. J Am Coll Cardiol. 2004;43:2183-2190.Yusuf S, et al. N Engl J Med. 2066;354:1464-1476.
12.2
8.45.5
9.3
5.0 5.5
0
5
10
15
20
Net adverse clinicalevents
Major bleeding* MACE**
30 d
ay e
vent
rate
s (%
)Heparin + GP IIb/IIIa inhibitor (N=1802) Bivalirudin monotherapy (N=1800)
HR = 1.00HR = 1.00 [0.75, 1.32]P = 0.98P = 0.98
HORIZONS AMI: Primary Outcome Measures (ITT)
HR = HR = 0.59 [0.45, 0.76]P P dd 0.00010.0001
HR = HR = 0.75 [0.62, 0.92]PP = 0.006= 0.006
*Not related to CABG*Not related to CABG**MACE=All cause death, **MACE=All cause death, reinfarctionreinfarction, ischemic TVR or stroke, ischemic TVR or stroke
Stone GW, et al. N Engl J Med. 2008;358:2218-2230.
HORIZONS AMI: 30 Day Stent ThrombosisHORIZONS AMI: 30 Day Stent ThrombosisUFH + UFH +
GP GP IIb/IIIaIIb/IIIa(N=1802)(N=1802)
BivalirudinBivalirudin(N=1800)(N=1800)
PPValueValue
ARC definite or probable* 1.9%1.9% 2.5%2.5% 0.300.30
- definite 1.4%1.4% 2.2%2.2% 0.090.09
- probable 0.5%0.5% 0.3%0.3% 0.240.24
- acute (≤ 24 hrs) 0.3%0.3% 1.3%1.3% <0.001<0.001
- subacute (> 24 h – 30 d) 1.7%1.7% 1.2%1.2% 0.280.28
*Protocol definition of stent thrombosis, CEC adjudicatedARC= Academic Research Consortium
Stone GW, et al. N Engl J Med. 2008;358:2218-2230.
Anticoagulants
Patients undergoing reperfusion with fibrinolyticsshould receive anticoagulant therapy for a minimum of 48 hours (Level of Evidence: C) and preferably for the duration of the index hospitalization, up to 8 days (regimens other than unfractionated heparin [UFH] are recommended if anticoagulant therapy is given for more than 48 hours because of the risk of heparin-induced thrombocytopenia with prolonged UFH treatment). (Level of Evidence: A)
Anticoagulant regimens with established efficacy include:♥ UFH (LOE: C)♥ Enoxaparin (LOE:A)♥ Fondaparinux (LOE:B)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.

7
Anticoagulants
For patients undergoing PCI after havingreceived an anticoagulant regimen, the
followingdosing recommendations should be followed:
a. For prior treatment with UFH: administer additional boluses of UFH as needed to support the procedure taking into account whether GP IIb/IIIa receptor antagonists have been administered. (Level of Evidence: C) Bivalirudin may also be used in patients treated previously with UFH. (Level of Evidence: C)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Recommendation continues on the next slide. Antman EM, et al. Circulation. 2008;117:296-329.
Anticoagulants
b. For prior treatment with enoxaparin: if the last SC dose was administered within the prior 8 hours, no additional enoxaparin should be given; if the last SC dose was administered at least 8 to 12 hours earlier, an IV dose of 0.3 mg/kg of enoxaparin should be given.
c. For prior treatment with fondaparinux: administer additional intravenous treatment with an anticoagulant possessing anti-IIa activity taking into account whether GP IIb/IIIa receptor antagonists have been administered.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.
Anticoagulants
Because of the risk of catheter thrombosis,fondaparinux should not be used as the soleanticoagulant to support PCI. An additionalanticoagulant with anti-IIa activity should beadministered.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.
It is reasonable for patients with STEMI who do not undergo reperfusion therapy to be treated with anticoagulant therapy (non-UFH regimen) for the duration of the index hospitalization, up to 8 days.
Convenient strategies that can be used include those with LMWH (Level of Evidence: C) or fondaparinux (Level of Evidence: B)using the same dosing regimens as for patients who receive fibrinolytic therapy.
Anticoagulants
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.
Thienopyridines
CLARITY-TIMI 28 Primary Endpoint:Occluded Artery (or D/MI thru Angio/HD)*
PlaceboClopidogrelLD 300 mgMD 75 mg
P=0.00000036P=0.00000036
Odds Ratio 0.64(95% CI 0.53-0.76)
Odds Ratio 0.64(95% CI 0.53-0.76)
Clopidogrelbetter
Placebobetter
n=1752 n=1739
D/MI thru Angio/HD, death or myocardial infarction before angiography or hospital discharge.Sabatine MS. N Eng J Med. 2005;352:1179.
STEMI, Age 18-75
15.0
21.7
0
5
10
15
20
25
Occ
lude
d A
rter
y or
Dea
th/M
I (%
)
1.00.4 0.6 0.8 1.2 1.6
36%Odds Reduction
36%Odds Reduction
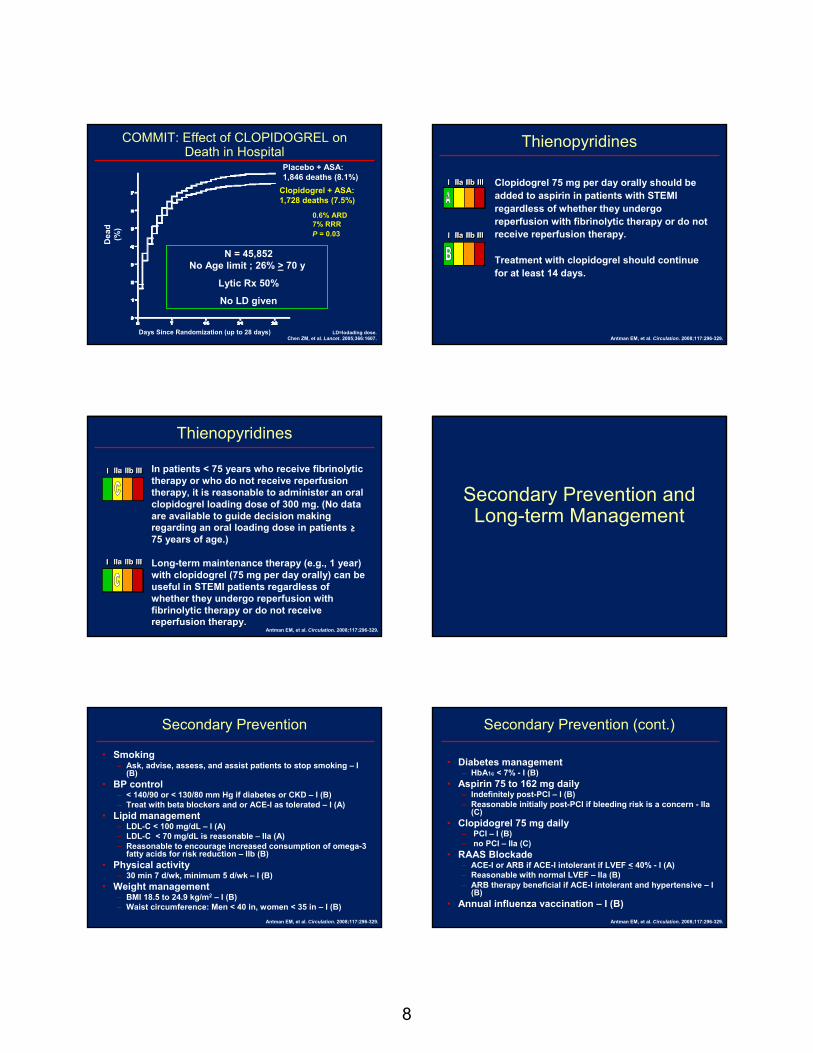
8
Dea
d (%
)
Days Since Randomization (up to 28 days)
Placebo + ASA: 1,846 deaths (8.1%)
Clopidogrel + ASA:1,728 deaths (7.5%)
0.6% ARD7% RRR P = 0.03
N = 45,852 No Age limit ; 26% > 70 y
Lytic Rx 50%
No LD given
COMMIT: Effect of CLOPIDOGREL on Death in Hospital
LD=lodading dose.Chen ZM, et al. Lancet. 2005;366:1607.
Clopidogrel 75 mg per day orally should be added to aspirin in patients with STEMI regardless of whether they undergo reperfusion with fibrinolytic therapy or do not receive reperfusion therapy.
Treatment with clopidogrel should continue for at least 14 days.
Thienopyridines
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.
In patients < 75 years who receive fibrinolytictherapy or who do not receive reperfusion therapy, it is reasonable to administer an oral clopidogrel loading dose of 300 mg. (No data are available to guide decision making regarding an oral loading dose in patients ≥75 years of age.)
Long-term maintenance therapy (e.g., 1 year) with clopidogrel (75 mg per day orally) can be useful in STEMI patients regardless of whether they undergo reperfusion with fibrinolytic therapy or do not receive reperfusion therapy.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Thienopyridines
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antman EM, et al. Circulation. 2008;117:296-329.
Secondary Prevention and Long-term Management
Secondary Prevention
• Smoking– Ask, advise, assess, and assist patients to stop smoking – I
(B)• BP control
– < 140/90 or < 130/80 mm Hg if diabetes or CKD – I (B)– Treat with beta blockers and or ACE-I as tolerated – I (A)
• Lipid management– LDL-C < 100 mg/dL – I (A)– LDL-C < 70 mg/dL is reasonable – IIa (A)– Reasonable to encourage increased consumption of omega-3
fatty acids for risk reduction – IIb (B)• Physical activity
– 30 min 7 d/wk, minimum 5 d/wk – I (B)• Weight management
– BMI 18.5 to 24.9 kg/m2 – I (B)– Waist circumference: Men < 40 in, women < 35 in – I (B)
Antman EM, et al. Circulation. 2008;117:296-329.
Secondary Prevention (cont.)
• Diabetes management– HbA1c < 7% - I (B)
• Aspirin 75 to 162 mg daily– Indefinitely post-PCI – I (B)– Reasonable initially post-PCI if bleeding risk is a concern - IIa
(C)• Clopidogrel 75 mg daily
– PCI – I (B) – no PCI – IIa (C)
• RAAS Blockade– ACE-I or ARB if ACE-I intolerant if LVEF < 40% - I (A)– Reasonable with normal LVEF – IIa (B)– ARB therapy beneficial if ACE-I intolerant and hypertensive – I
(B)• Annual influenza vaccination – I (B)
Antman EM, et al. Circulation. 2008;117:296-329.

9
Questions NSTEMI Patient Simulation
Please log in now…Please log in now…
2007 ACC/AHA UA/NSTEMI Updated Guidelines
James A. de Lemos, MDDirector, Coronary Care UnitParkland Memorial Hospital
Dallas, TX
•Examine updated ACC/AHA UA/NSTEMI guidelines
•Apply evidence‐based UA/NSTEMI guidelines to ACS
patient scenarios
•Implement changes in your practice based on review and
application of the updated UA/NSTEMI guidelines
Learning Objectives
UA/NSTEMI Guidelines Slide Set
ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non–ST-Elevation Myocardial Infarction
Developed In Collaboration with the American College of Emergency Physicians, the Society for
Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons
Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the
Society for Academic Emergency Medicine
Special Thanks to
The UA/NSTEMI Guidelines Writing Committee Members
Jeffrey L. Anderson, MD, FACC, FAHA, Chair Francis M. Fesmire, MD, FACEP
Cynthia D. Adams, RN, PhD, FAHA Judith S. Hochman, MD, FACC, FAHA
Elliott M. Antman, MD, FACC, FAHA Thomas N. Levin, MD, FACC, FSCAI
Charles R. Bridges, ScD, MD, FACC, FAHA A. Michael Lincoff, MD, FACC
Robert M. Califf, MD, MACC Eric D. Peterson, MD, MPH, FACC, FAHA
Donald E. Casey, Jr, MD, MPH, MBA, FACP Nanette Kass Wenger, MD, FACC, FAHA
William E. Chavey II, MD, MS R. Scott Wright, MD, FACC, FAHA
Slide Set EditorNanette Kass Wenger, MD, FACC, FAHA

10
Select Management Strategy:
Initial Invasive Versus Initial Conservative Strategy
Major ChangesNew Trial Data
Selection of Initial Treatment Strategy: Initial Invasive vs Conservative Strategy
Invasive Recurrent angina/ischemia at rest with low-level activities despite intensive medical therapyElevated cardiac biomarkers (TnT or TnI)New/presumably new ST-segment depression
Signs/symptoms of heart failure or new/worsening mitral regurgitationHigh-risk findings from noninvasive testingHemodynamic instabilitySustained ventricular tachycardiaPCI within 6 monthsPrior CABGHigh risk score (eg, TIMI, GRACE)Reduced left ventricular function (LVEF < 40%)
Conservative Low risk score (eg, TIMI, GRACE)Patient/physician preference in the absence of high-risk features
Initial Invasive Strategy
Major Changes•New Drugs•Longer Duration of Antiplatelet Rx•Revised Algorithm
Algorithm for Patients with UA/NSTEMI Managed by an Initial Invasive Strategy
Proceed to Diagnostic Angiography
ASA (Class I, LOE: A)Clopidogrel if ASA intolerant (Class I,
LOE: A)
Diagnosis of UA/NSTEMI is Likely or Definite
Invasive StrategyInit ACT (Class I, LOE: A)
Acceptable options: enoxaparin or UFH (Class I, LOE: A) bivalirudin or fondaparinux (Class I, LOE: B)
Select Management StrategyProceed with an
Initial Conservative
Strategy
ACT=anticoagulation therapy; LOE=level of evidence. Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157.
A
B
B1
B2
Prior to AngiographyInit at least one (Class I, LOE: A) or
both (Class IIa, LOE: B) of the following:
ClopidogrelIV GP IIb/IIIa inhibitor
Factors favoring admin of both clopidogrel and GP IIb/IIIa inhibitor include delay to
angiography, high-risk features, and early recurrent ischemic discomfort
Initial Invasive Strategy: Antiplatelet TherapyFor UA/NSTEMI patients in whom an initial invasive strategy is selected, antiplatelet therapy in addition to ASA should be initiated before diagnostic angiography (upstream) with either clopidogrel (loading dose followed by daily maintenance dose)* or an IV GP IIb/IIIa inhibitor.
Abciximab as the choice for upstream GP IIb/IIIatherapy is indicated only if there is no appreciable delay to angiography and PCI is likely to be performed; otherwise, IV eptifibatideor tirofiban is the preferred choice of GP IIb/IIIainhibitor.†
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
*Some uncertainty exists about optimum dosing of clopidogrel. Randomized trials establishing its efficacy and providing data on bleeding risks used a loading dose of 300 mg orally followed by a daily oral maintenance dose of 75 mg. Higher oral loading doses such as 600 or 900 mg of clopidogrel more rapidly inhibit platelet aggregation and achieve a higher absolute level of inhibition of platelet aggregation, but the additive clinical efficacy and the safety of higher oral loading doses have not been rigorously established; †Factors favoring administration of both clopidogrel and a GP IIb/IIIainhibitor include: delay to angiography, high-risk features, and early ischemic discomfort.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Clopidogrel in UA/NSTEMI to preventRecurrent ischemic Events (CURE)
•12,562 patients within 24 h UA/NSTEMI•Placebo vs clopidogrel (LD 300 mg → 75 mg qd)•Other meds: ASA•↓ CV death, MI, or stroke, rate of recurrent ischemia & revasc with clopidogrel•↑ Major (non–life-threatening) bleeding with clopidogrel•No routine inv strategy, 23% revasc during initial admission•Although well tolerated, < 10% GP IIb/IIIa + ASA + clopidogrel + heparin use in study patients
Yusuf S, et al. N Engl J Med. 2001;345:494–502.
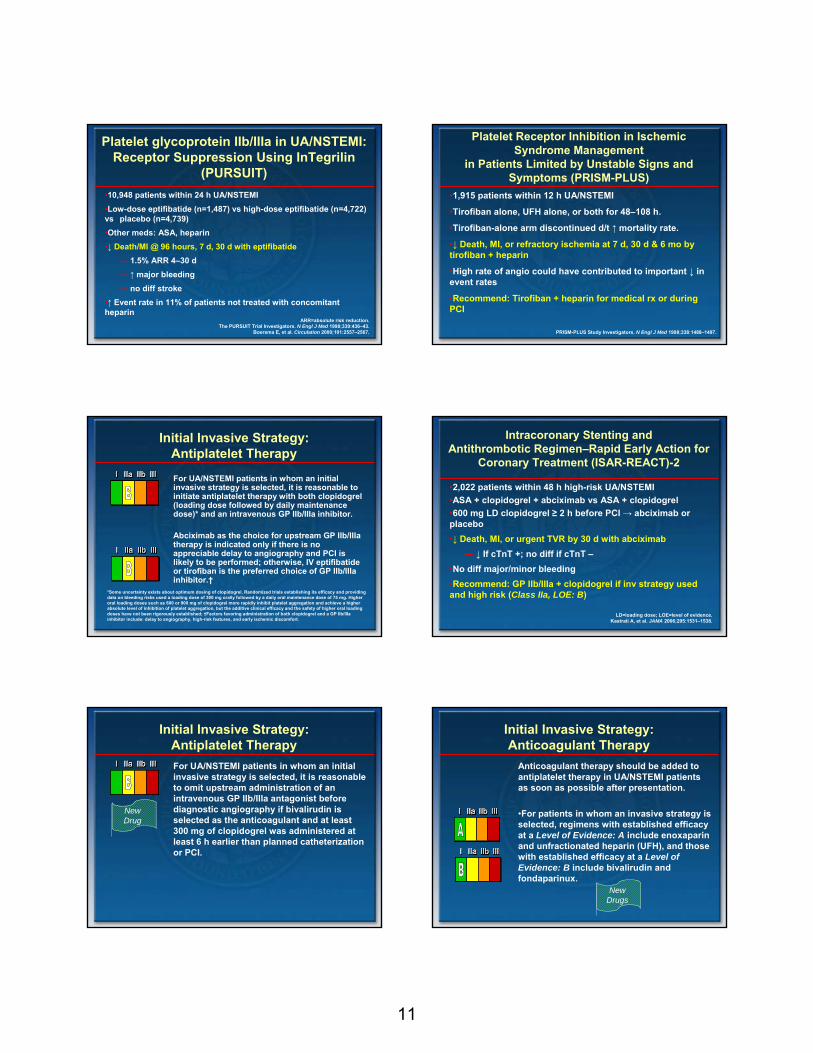
11
Platelet glycoprotein IIb/IIIa in UA/NSTEMI: Receptor Suppression Using InTegrilin
(PURSUIT)•10,948 patients within 24 h UA/NSTEMI•Low-dose eptifibatide (n=1,487) vs high-dose eptifibatide (n=4,722) vs placebo (n=4,739)•Other meds: ASA, heparin•↓ Death/MI @ 96 hours, 7 d, 30 d with eptifibatide
― 1.5% ARR 4–30 d― ↑ major bleeding― no diff stroke
•↑ Event rate in 11% of patients not treated with concomitant heparin
ARR=absolute risk reduction.The PURSUIT Trial Investigators. N Engl J Med 1998;339:436–43.
Boersma E, et al. Circulation 2000;101:2557–2567.
Platelet Receptor Inhibition in Ischemic Syndrome Management
in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS)
•1,915 patients within 12 h UA/NSTEMI
•Tirofiban alone, UFH alone, or both for 48–108 h.
•Tirofiban-alone arm discontinued d/t ↑ mortality rate.
•↓ Death, MI, or refractory ischemia at 7 d, 30 d & 6 mo by tirofiban + heparin
•High rate of angio could have contributed to important ↓ in event rates
•Recommend: Tirofiban + heparin for medical rx or during PCI
PRISM-PLUS Study Investigators. N Engl J Med 1998;338:1488–1497.
Initial Invasive Strategy:Antiplatelet Therapy
For UA/NSTEMI patients in whom an initial invasive strategy is selected, it is reasonable to initiate antiplatelet therapy with both clopidogrel(loading dose followed by daily maintenance dose)* and an intravenous GP IIb/IIIa inhibitor.
Abciximab as the choice for upstream GP IIb/IIIatherapy is indicated only if there is no appreciable delay to angiography and PCI is likely to be performed; otherwise, IV eptifibatideor tirofiban is the preferred choice of GP IIb/IIIainhibitor.†
*Some uncertainty exists about optimum dosing of clopidogrel. Randomized trials establishing its efficacy and providing data on bleeding risks used a loading dose of 300 mg orally followed by a daily oral maintenance dose of 75 mg. Higher oral loading doses such as 600 or 900 mg of clopidogrel more rapidly inhibit platelet aggregation and achieve a higher absolute level of inhibition of platelet aggregation, but the additive clinical efficacy and the safety of higher oral loading doses have not been rigorously established; †Factors favoring administration of both clopidogrel and a GP IIb/IIIainhibitor include: delay to angiography, high-risk features, and early ischemic discomfort.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Intracoronary Stenting andAntithrombotic Regimen–Rapid Early Action for
Coronary Treatment (ISAR-REACT)-2
•2,022 patients within 48 h high-risk UA/NSTEMI•ASA + clopidogrel + abciximab vs ASA + clopidogrel•600 mg LD clopidogrel ≥ 2 h before PCI → abciximab or placebo•↓ Death, MI, or urgent TVR by 30 d with abciximab
― ↓ If cTnT +; no diff if cTnT –•No diff major/minor bleeding•Recommend: GP IIb/IIIa + clopidogrel if inv strategy used and high risk (Class IIa, LOE: B)
LD=loading dose; LOE=level of evidence.Kastrati A, et al. JAMA 2006;295:1531–1538.
Initial Invasive Strategy:Antiplatelet TherapyFor UA/NSTEMI patients in whom an initial invasive strategy is selected, it is reasonable to omit upstream administration of an intravenous GP IIb/IIIa antagonist before diagnostic angiography if bivalirudin is selected as the anticoagulant and at least 300 mg of clopidogrel was administered at least 6 h earlier than planned catheterization or PCI.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
New Drug
Initial Invasive Strategy:Anticoagulant Therapy
Anticoagulant therapy should be added to antiplatelet therapy in UA/NSTEMI patients as soon as possible after presentation.
•For patients in whom an invasive strategy is selected, regimens with established efficacy at a Level of Evidence: A include enoxaparinand unfractionated heparin (UFH), and those with established efficacy at a Level of Evidence: B include bivalirudin and fondaparinux.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
New Drugs

12
Efficacy and Safety ofSubcutaneous Enoxaparin in Non-Q-Wave
Coronary Events (ESSENCE) Trial
•3,171 patients within 24 h UA/NSTEMI
•Enoxaparin vs UFH
•Other meds: ASA
•↓ Death, MI or recurrent angina for enox @ 14 d, 30d and 1 y
― minor bleeding ↑
― major bleeding ↔
Cohen M, et al. N Engl J Med. 1997;337:447–452. Cohen M, et al. Am J Cardiol. 1998;82:19L–24L (bleeding).
Goodman SG, et al. J Am Coll Cardiol. 2000;36:6934–6938 (1-y results).
Thrombolysis In Myocardial Ischemia trial, phase 11B (TIMI 11B)
•3,910 patients within 24 h UA/NSTEMI
•Enoxaparin vs UFH
•Other meds: ASA
•↓ Death, MI or urgent revasc for enox @ 48 h, 8 d, 14 d, & 43 d
•↑ major & minor bleeding (inhosp) with enox
Antman EM, et al. Circulation. 1999;100:1593–1601.
Superior Yield of the New strategy ofEnoxaparin, Revascularization and GlYcoprotein
IIb/IIIa Inhibitors (SYNERGY)
Ferguson JJ, et al. JAMA. 2004;292:45–54. Mahaffey KW, et al. Am Heart J. 2005;149:S81–S90 (6 mo & 1-y results).
•9,978 patients within 24 h high-risk UA/NSTEMI
•Enoxaparin vs UFH → early inv strategy
•Other meds: ASA, GP IIb/IIIa @ physician discretion
•Enox noninferior for death/MI @ 30 d, 6 mo 1 y
•↑ Major bleeding with enox
― ? due to crossover to UFH @ time of PCI
SYNERGY Primary Outcomes
14.5 14
0
2
4
6
8
10
12
14
16
Death or MIat 30 d
UFHEnoxaparin
Absolute Risk Reduction 0.5Hazard Ratio 0.9695% CI 0.86–1.06p 0.40
Free
dom
from
Dea
th/M
I
0.8
0.85
0.9
0.95
1.0
0 5 10 15 20 25 30
Days from Randomization
Kaplan Meier Curve
UFH
Enoxaparin
Reprinted with permission from Ferguson JJ, et al. JAMA. 2004;292:45–54.
Antithrombotic CombinationUsing Tirofiban and Enoxaparin (ACUTE II)
•525 patients within 24 h UA/NSTEMI •Enoxaparin vs UFH •Other meds: ASA, tirofiban LD 0.4 mcg/kg over 30 min →0.1 mcg/kg/min
•No ↓ death/MI during first 30 d― Trend to lower event rates with enox
•No ↓ major/minor bleeding
LD=loading dose.Cohen M, et al. Am Heart J 2002;144:470–477.
INTegrilin and Enoxaparin Randomized Assessment of Acute Coronary syndrome
Treatment (INTERACT)•746 patients within 24 h high-risk UA/NSTEMI
•Enoxaparin vs UFH
•Other meds: ASA, eptifibatide 180 mcg/kg IV bolus → 2.0 mcg/kg/min infusion for 48 hours
•↓ Death/MI for enox @ 30 d
•Minor bleeding - ↑ for enox @ 96 h, no diff by 30 d
•Major bleeding - ↓ for enox @ 96 h (1o safety endpoint)
Goodman SG, et al. Circulation. 2003;107:238–244.

13
Aggrastat to Zocor (A to Z)
•3,987 patients within 24 h UA/NSTEMI on ASA & tirofiban•Enoxaparin vs UFH •Coronary angio in 60% of pts•No ↓ all-cause mortality, MI or refractory ischemia w/in 7 d by enox― Nonsig trend to ↓ ischemic events with enox
•↑ Major bleeding with enox
Blazing MA, et al. JAMA 2004;292:55–64.
Acute Catheterization and Urgent Intervention Triage strategY (ACUITY)
•Within 24 h UA/NSTEMI → heparin (enox/UFH) ± upstream GP IIb/IIIa (n=4603) vs bivalirudin (bival) ± upstream GP IIb/IIIa(n=4604) vs bival alone + provisional GP IIb/IIIa (n=4612)•Compared to heparin + GP IIb/IIa:― Bival + GP IIb/IIIa noninferior for composite ischemia, major
bleeding & net clinical outcomes @ 30 d― Bival alone noninferior for composite ischemia; ↓ major bleeding; ↓ net clinical outcomes @ 30 d
•Caution using bival alone, esp with delay to angio and high-risk features, or if early ischemic discomfort occurs after initial
antithrombotic strategy implemented•Recommend: Concomitant use of GP IIb/IIIa or thienopyridinebefore angio whether bival-based or heparin-based strategy used
Stone GW, et al. N Engl J Med. 2006;355:2203–2216.
7.3
5.7
11.7
7.7
5.3
11.8
0
2
4
6
8
10
12
14
ACUITY Compositeischemia endpoint at 30
days
ACUITY Major bleeding at30 days
ACUITY Net clinicaloutcome at 30 days
UFH or Enoxaparin + GP IIb/IIIa
Bivalirudin + GP IIb/IIIa
ACUITY Clinical Outcomes at 30 d
Absolute Risk Reduction -0.4 0.4 -0.1Hazard Ratio 1.07 0.93 1.0195% CI 0.92–1.23 0.78–1.10 0.90–1.12p 0.007* < 0.001* < 0.001* *p for noninferiority.
Stone GW, et al. N Engl J Med. 2006;355:2203–2216.
Net
clin
ical
out
com
e (%
)
ACUITY Composite Ischemia and Bleeding Outcomes
Absolute Risk Reduction -0.5 0.3 -2.0 2.7Hazard Ratio 1.08 0.97 1.29 0.5395% CI 0.93–1.24 0.80–1.17 1.03–1.63 0.43–0.65p 0.32 0.054 (for interaction) < 0.001
Stone GW, et al. N Engl J Med. 2006;355:2203–2216.
7.3 7.3 7.1
5.7
7.8
7.0
9.1
3.0
0
1
2
3
4
5
6
7
8
9
10
ACUITY Composite ischemiaendpoint at 30 days
Ischemia endpoint bythienopyridine loading before angiography or PCI YES
Ischemia endpoint bythienopyridine loading before
angiography or PCI No
ACUITY Major bleeding at 30days
UFH + GP IIb/IIIa
Bivalirudin alone
Isch
emia
/ble
edin
g ou
tcom
es (%
)
Organization toAssess Strategies for Ischaemic
Syndromes (OASIS-5)•Fondaparinux (fonda) (2.5 mg/day, n=10,057) vs enox (1.0 mg/kg BID, n=10,021) in UA/NSTEMI patients― Enox patients undergoing PCI → UFH if last dose of enox > 6 h
before PCI•Other meds: ASA, clopidogrel, GP IIb/IIIa @ investigator discretion•No ↓ death, MI or refractory ischemia @ 9 d by fonda
― Noninferiority criteria met•↓ Major bleeding with fonda•↓ Death @ 30 d and 180 d and ↓ death, MI and stroke @ 180 d with fonda•↑ Catheter-assoc thrombus with fondaYusuf S, et al. N Engl J Med. 2006;354:1464–1476.
Also see Section 3.2.5.5 in Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157 for detailed discussion of trial results and dosing protocol.
OASIS 5 Cumulative Risk of Death, MI, or Refractory Ischemia
*p for noninferiority; †p for superiority. Yusuf S, et al. N Engl J Med. 2006;354:1464–1476.
5.7
4.1
9.0
5.8
2.2
7.3
0123456789
10
OASIS 5 Death, MI, or refractoryischemia at 9 days
OASIS 5 Major bleeding at 9 days
OASIS 5 Composite primaryoutcome and major bleeding at 9 days
Enoxaparin
Fondaparinux
Absolute Risk Reduction -0.1 1.9 1.7Hazard Ratio 1.01 0.52 0.81Confidence Interval 0.90–1.13 0.44–0.61 0.73–0.89p 0.007* < 0.001† < 0.001†
Mai
n ef
ficac
y an
d sa
fety
out
com
es (%
)

14
Initial Conservative Strategy
Major Changes•New Drugs•Longer Duration of Antiplatelet Rx•Revised Algorithm
Init clopidogrel (Class I, LOE: A) Consider adding IV eptifibatide or tirofiban
(Class IIb, LOE: B)
Conservative StrategyInit ACT (Class I, LOE: A):
Acceptable options: enoxaparin or UFH (Class I, LOE: A) or fondaparinux (Class I, LOE: B), but
enoxaparin or fondaparinux are preferable (Class IIa, LOE: B)
Select Management Strategy
ASA (Class I, LOE: A)Clopidogrel if ASA intolerant (Class I, LOE:
A)
Diagnosis of UA/NSTEMI is Likely or Definite
Algorithm for Patients with UA/NSTEMI Managed by an Initial Conservative Strategy
Proceed with Invasive Strategy
(Continued)ACT=anticoagulation therapy.
LOE=level of evidence.Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157.
C2
C1
A
Any subsequent events necessitating angiography?
EF greater than 40%
Evaluate LVEF
Low Risk
Cont ASA (Class I, LOE A) Cont clopidogrel (Class I, LOE A) and ideally up to 1 yr (Class I, LOE B)
DC IV GP IIb/IIIa if started previously (Class I, LOE A) DC ACT (Class I, LOE A)
(Class I, LOE: B)
Proceed to DxAngiography
Yes
EF 40% or less Stress Test
(Class I, LOE: A)
No
Not Low Risk
(Class IIa, LOE: B)
Algorithm for Patients with UA/NSTEMI Managed by an Initial Conservative Strategy
(Continued)
ACT=anticoagulation therapy; LOE=level of evidence. Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157.
(Class I, LOE: A)
(Class IIa, LOE: B)
O
L
MN
K
E-1 E-2
D
(Class I,
LOE: B)
(Class I, LOE: A)
Initial Conservative Strategy:Antiplatelet TherapyFor UA/NSTEMI patients in whom an initial conservative (ie, noninvasive) strategy is selected, clopidogrel (loading dose followed by daily maintenance dose)* should be added to ASA and anticoagulant therapy as soon as possible after admission and administered for at least 1 month (Level of Evidence: A) and ideally up to 1 year. (Level of Evidence: B)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
*Some uncertainty exists about optimum dosing of clopidogrel. Randomized trials establishing its efficacy and providing data on bleeding risks used a loading dose of 300 mg orally followed by a daily oral maintenance dose of 75 mg. Higher oral loading doses such as 600 or 900 mg of clopidogrel more rapidly inhibit platelet aggregation and achieve a higher absolute level of inhibition of platelet aggregation, but the additive clinical efficacy and the safety of higher oral loading doses have not been rigorously established.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Antiplatelet therapy forReduction of MYocardial Damage during
Angioplasty (ARMYDA-2)•Patients with stable angina or UA/NSTEMI
•Clopidogrel 600 mg LD (n=126) vs clopidogrel 300 mg LD (n=129) 4 to 8 h before PCI
•↓ Death, MI or TVR up to 30 days by 600 mg LD
― Benefit d/t ↓ periprocedural MI
•Small study of relatively low-risk patients, low use of GP IIb/IIIa
LD=loading dose.Patti G, et al. Circulation. 2005;111:2099 –2106.
Initial Conservative Strategy:Antiplatelet Therapy
For UA/NSTEMI patients in whom an initial conservative strategy is selected, if recurrent symptoms/ischemia, HF, or serious arrhythmias subsequently appear, then diagnostic angiography should be performed. (Level of Evidence: A) Either an IV GP IIb/IIIa inhibitor (eptifibatide or tirofiban; Level of Evidence: A) or clopidogrel (loading dose followed by daily maintenance dose; Level of Evidence: A)* should be added to ASA and anticoagulant therapy before diagnostic angiography (upstream). (Level of Evidence: C)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
*Some uncertainty exists about optimum dosing of clopidogrel. Randomized trials establishing its efficacy and providing data on bleeding risks used a loading dose of 300 mg orally followed by a daily oral maintenance dose of 75 mg. Higher oral loading doses such as 600 or 900 mg of clopidogrel more rapidly inhibit platelet aggregation and achieve a higher absolute level of inhibition of platelet aggregation, but the additive clinical efficacy and the safety of higher oral loading doses have not been rigorously established.
See recommendation
for LOE

15
Platelet Receptor Inhibition in Ischemic Syndrome Management
(PRISM)•3,232 patients within 24 h UA/NSTEMI
•Tirofiban vs UFH over 48 h
•Other meds: ASA
•↓ Death, MI, or refractory ischemia at 48 h & 7 d by tirofiban
― ↓ Death/MI @ 30 d
― No ↑ bleeding; thrombocytopenia ↑
PRISM Study Investigators. N Engl J Med. 1998;338:1498–1505.
Initial Conservative Strategy:Antiplatelet TherapyFor UA/NSTEMI patients in whom an initial conservative strategy is selected and who have recurrent ischemic discomfort with clopidogrel, ASA, and anticoagulant therapy, it is reasonable to add a GP IIb/IIIaantagonist before diagnostic angiography.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Initial Conservative Strategy:Antiplatelet TherapyFor UA/NSTEMI patients in whom an initial conservative (ie, noninvasive) strategy is selected, it may be reasonable to add eptifibatide or tirofiban to anticoagulant and oral antiplatelet therapy.
Abciximab should not be administered to patients in whom PCI is not planned.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Initial Conservative Strategy:Anticoagulant Therapy
Anticoagulant therapy should be added to antiplatelet therapy in UA/NSTEMI patients as soon as possible after presentation.
•For patients in whom a conservative strategy is selected, regimens using either enoxaparin* or UFH (Level of Evidence: A) or fondaparinux (Level of Evidence: B) have established efficacy.
•In patients in whom a conservative strategy is selected and who have an increased risk of bleeding, fondaparinux is preferable.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
*Limited data are available for the use of other low-molecular-weight heparins (LMWHs), eg, dalteparin.
New Drugs
Initial Conservative Strategy:Anticoagulant Therapy
For UA/NSTEMI patients in whom an initial conservative strategy is selected, enoxaparin* or fondaparinux is preferable to UFH as anticoagulant therapy, unless CABG is planned within 24 h.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
*Limited data are available for the use of other low-molecular-weight heparins (LMWHs), eg, dalteparin.
Initial Conservative Strategy:Additional Management Considerations
For UA/NSTEMI patients in whom an initial conservative strategy is selected and no subsequent features appear that would necessitate diagnostic angiography (recurrent symptoms/ischemia, HF, or serious arrhythmias), a stress test should be performed.
a. If, after stress testing, the patient is classified as not at low risk, diagnostic angiography should be performed.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
This recommendation continues on the next slide.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
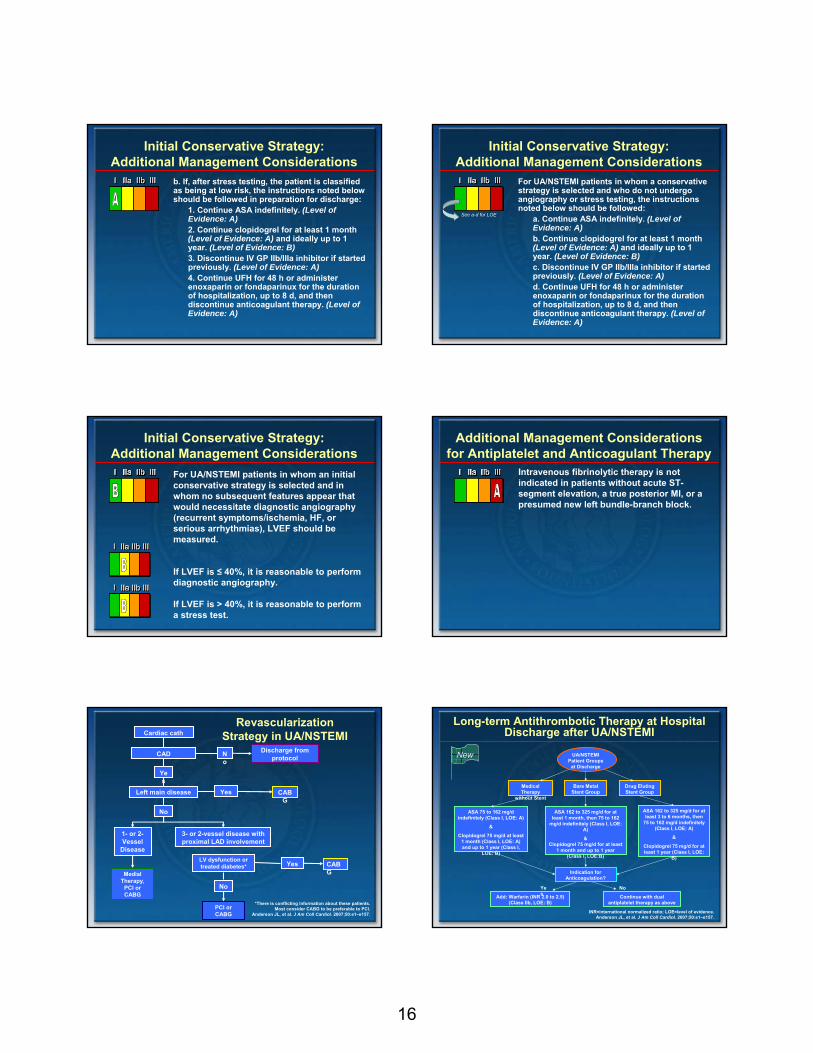
16
Initial Conservative Strategy:Additional Management Considerations
b. If, after stress testing, the patient is classified as being at low risk, the instructions noted below should be followed in preparation for discharge:
1. Continue ASA indefinitely. (Level of Evidence: A)2. Continue clopidogrel for at least 1 month (Level of Evidence: A) and ideally up to 1 year. (Level of Evidence: B)3. Discontinue IV GP IIb/IIIa inhibitor if started previously. (Level of Evidence: A)4. Continue UFH for 48 h or administer enoxaparin or fondaparinux for the duration of hospitalization, up to 8 d, and then discontinue anticoagulant therapy. (Level of Evidence: A)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Initial Conservative Strategy:Additional Management Considerations
For UA/NSTEMI patients in whom a conservative strategy is selected and who do not undergo angiography or stress testing, the instructions noted below should be followed:
a. Continue ASA indefinitely. (Level of Evidence: A)b. Continue clopidogrel for at least 1 month (Level of Evidence: A) and ideally up to 1 year. (Level of Evidence: B)c. Discontinue IV GP IIb/IIIa inhibitor if started previously. (Level of Evidence: A)d. Continue UFH for 48 h or administer enoxaparin or fondaparinux for the duration of hospitalization, up to 8 d, and then discontinue anticoagulant therapy. (Level of Evidence: A)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
See a-d for LOE
Initial Conservative Strategy:Additional Management Considerations
For UA/NSTEMI patients in whom an initial conservative strategy is selected and in whom no subsequent features appear that would necessitate diagnostic angiography (recurrent symptoms/ischemia, HF, or serious arrhythmias), LVEF should be measured.
If LVEF is ≤ 40%, it is reasonable to perform diagnostic angiography.
If LVEF is > 40%, it is reasonable to perform a stress test.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Additional Management Considerations for Antiplatelet and Anticoagulant Therapy
Intravenous fibrinolytic therapy is not indicated in patients without acute ST-segment elevation, a true posterior MI, or a presumed new left bundle-branch block.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Cardiac cath
CAD No
Discharge from protocol
Yes
Left main disease Yes CABG
No
1- or 2-Vessel
Disease
3- or 2-vessel disease with proximal LAD involvement
LV dysfunction or treated diabetes*
No
PCI or CABG
Medial Therapy,
PCI or CABG
Yes CABG
*There is conflicting information about these patients. Most consider CABG to be preferable to PCI.
Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1–e157.
Revascularization Strategy in UA/NSTEMI
Long-term Antithrombotic Therapy at Hospital Discharge after UA/NSTEMI
Medical Therapy
without Stent
Bare Metal Stent Group
Drug Eluting Stent Group
ASA 162 to 325 mg/d for at least 1 month, then 75 to 162
mg/d indefinitely (Class I, LOE: A)
&Clopidogrel 75 mg/d for at least
1 month and up to 1 year (Class I, LOE:B)
Add: Warfarin (INR 2.0 to 2.5) (Class IIb, LOE: B)
Continue with dual antiplatelet therapy as above
Yes
No
Indication for Anticoagulation?
ASA 75 to 162 mg/d indefinitely (Class I, LOE: A)
&
Clopidogrel 75 mg/d at least 1 month (Class I, LOE: A) and up to 1 year (Class I,
LOE: B)
ASA 162 to 325 mg/d for at least 3 to 6 months, then
75 to 162 mg/d indefinitely (Class I, LOE: A)
&
Clopidogrel 75 mg/d for at least 1 year (Class I, LOE:
B)
INR=international normalized ratio; LOE=level of evidence.Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1–e157.
UA/NSTEMI Patient Groups
at Discharge
New

17
Questions Bridging the Gap Between Emergency Medicine and
Cardiology
Charles V. Pollack Jr., MDProfessor and Chairman
Department of Emergency MedicinePennsylvania Hospital
Philadelphia, PA
•Analyze the implications of updated ACC/AHA ACS guidelines for emergency
medical care
•Enhance cooperation between the emergency department (ED) and the emergency transport team, hospital
administration, catheterization laboratory, and CCU
•Adapt quality improvement strategies and evidence‐based algorithms to align STEMI and UA/NSTEMI ED practice with
current scientific data
Learning Objectives What Is the State of Emergency Care?
Y=2.86 (±1.46) + 0.0045X1 + 0.000043X2
P<.001
Trends in ED Visits: US 1995-2005
5,000
4,500
4,000
3,500
3,000
2,500
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Num
ber o
f em
erge
ncy
depa
rtm
ents
Visits
Emergency departments
00
90
95
100
105
110
115
120
Num
ber o
f em
erge
ncy
depa
rtm
ent v
isits
in
mill
ions
Trends in numbers of emergency departments and related visits: United States 1995-2005
Nawar EW, et al. Advance Data. 2007;29(386):1.

18
Trends in ED Visits: US 1995-2005
5,000
4,500
4,000
3,500
3,000
2,500
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Num
ber o
f em
erge
ncy
depa
rtm
ents
Visits
Emergency departments
00
90
95
100
105
110
115
120
Num
ber o
f em
erge
ncy
depa
rtm
ent v
isits
in
mill
ions
Trends in numbers of emergency departments and related visits: United States 1995-2005
Nawar EW, et al. Advance Data. 2007;29(386):1.
••In the last 10 years ED visits have In the last 10 years ED visits have increased by 20% while the number increased by 20% while the number of of EDsEDs has decreased by 7%has decreased by 7%
••The second most common reason The second most common reason given by patients for coming to the given by patients for coming to the ED is chest pain and related ED is chest pain and related symptomssymptoms
Does Evidence-based ACS Care
Matter?
RCTs Exclude the Elderly: Review of 593 UA/MI Trials
0102030405060708090
100
1966–70 1971–80 1981–90 1991–95 1996–00
Explicit exclusion > 75 No patient > 75 enrolled
Tria
ls n
ot in
clud
ing
elde
rly (%
)
Lee PY, et al. JAMA. 2001;286:708-713.
Comparison of Co-morbid Burden in Trials
Age group (%) Trials
Community1624
211
HTN (%)Trials
Community5975
5773
Diabetes (%)Trials
Community2536
2025
CHF (%)Trials
Community1626
2236
Prior stroke (%)Trials
Community9
178
18
ST depression (%)Trials
Community6142
6440
Age 75–84 Age ≥ 85
Alexander KP, et al. Circulation. 2007;115:2549-2569.
CRUSADE Community and VIGOUR Trials
Lower Guideline Adherence = Poorer Outcomes
No. of events (%) by hospital adherence quartile
Population 1 (lowest) 2 3 4 (highest) P Value
Overall (N=64,775)
(n=12,329) (n=15,255) (n=18,364) (n=18,827)
Death 784 (6.36) 772 (5.06) 850 (4.63) 786 (4.17) < .001
Death/MI 1119 (9.08) 1280 (8.39) 1223 (6.66) 1201 (6.38) < .001
Stroke 96 (0.78) 146 (0.96) 171 (0.93) 134 (0.71) .31
CHF 908 (7.36) 1747 (11.45) 1727 (9.40) 1541 (8.19) .24
Peterson ED, et al. JAMA.2006;295:1912-1920.
In-hospital Mortality in Elderly and Very Elderly NSTE-ACS Patients and
Guideline Adherence
Skolnick, AH et al. JACC. 2007;49:1790-1797.
20
25
15
10
5
00-25 26-50 51-75 76-100
Percent Adherence Score
In-H
ospi
tal M
orta
lity
(%)
Age ≥ 90 Age 75-89
P-value for trend <0.001
P-value for age-treatment interaction = NS14.7
18.9
11.08.3
10.2
6.7
11.1
6.2

19
What Is the State of Evidence-based ACS
Care in the ED?
What degree of improvement is required for the treatment of acute myocardial infarction in the US?
1. A great deal2. A fair amount 3. Somewhat4. Not at all
More than Half of Surveyed US Physicians Point to Need for
Improved MI Treatment
Peacock WF, et al. Tex Heart Inst J. 2008;35(2):152-161.
How would you characterize your familiarity with the ACC/AHA STEMI Guidelines?
1. Very familiar2. Familiar3. Somewhat familiar4. Not at all familiar
STEMI Guideline Familiarity Still Lacking
Peacock WF, et al. Tex Heart Inst J. 2008;35(2):152-161.
Physician Views of Hospital Conformance with STEMI Guidelines
78% of surveyed physicians indicated their hospital had a written MI treatment protocol, but
23% deemed the protocol ineffective in helping providers determine AMI treatment50% said that the protocol was followed only sometimes or rarely
40% believed time to reperfusion could be significantly improved, but
Most (69%) did not believe primary PCI within 90 minutes was realistic in transfer patients20% viewed performing PCI in less than 90 minutes as unrealistic even in a PCI-capable facility
Peacock WF, et al. Tex Heart Inst J. 2008;35(2):152-161.
20
What Is Your Experience?Does your hospital have a written STEMI protocol?
1. Yes2. No3. Unsure
If your hospital has a written STEMI protocol, is it implemented?
1. Yes2. No3. Unsure4. Not applicable
Does the written STEMI protocol at your hospital improve MI care?
1. Yes2. No3. Unsure4. Not applicable
Which of the following best characterizes your hospital (select one)?
1. No catheterization lab2. Interventional catheterization
capability3. Diagnostic catheterization capability4. Interventional catheterization and
CABG capability
What is the estimated mean time to balloon inflation in your hospital for STEMI patients?
1. 60 minutes or less 2. 90 minutes3. 120 minutes4. More than 120 minutes5. Not applicable6. Unsure
Do you think achievement of primary PCI in 90 minutes or less is feasible when a patient must be transferred?
1. Yes2. No3. Unsure
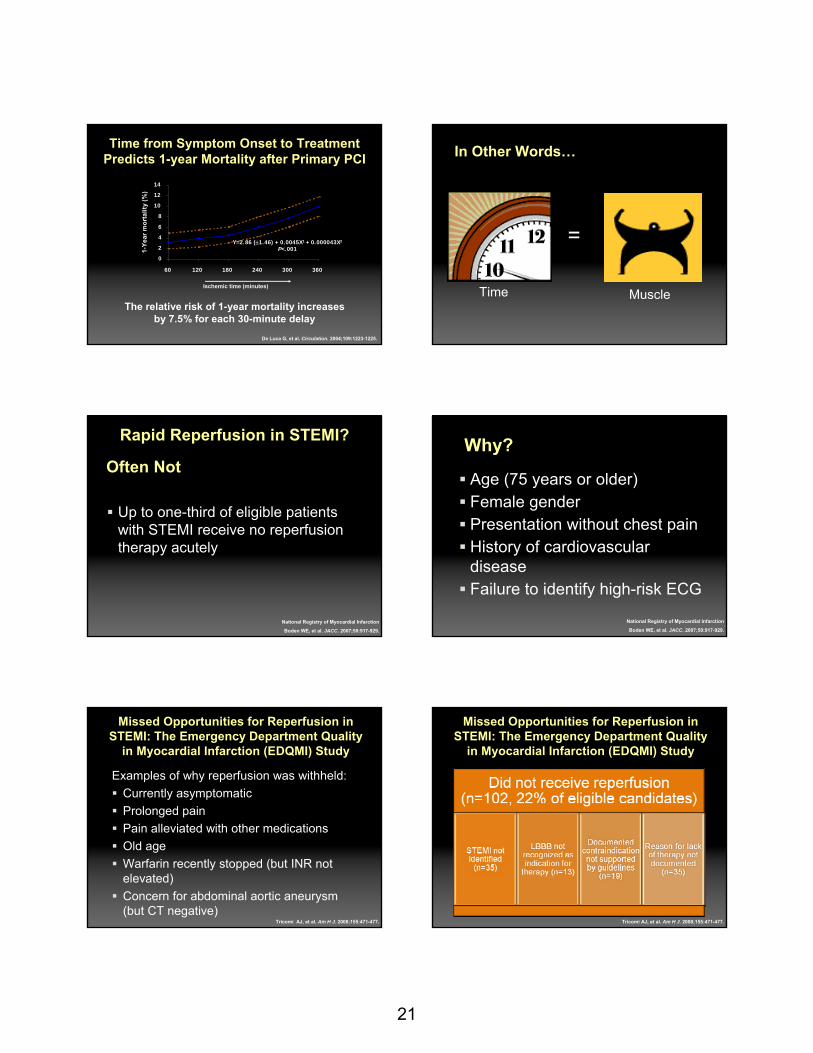
21
Time from Symptom Onset to TreatmentPredicts 1-year Mortality after Primary PCI
The relative risk of 1-year mortality increases by 7.5% for each 30-minute delay
De Luca G, et al. Circulation. 2004;109:1223-1225.
Y=2.86 (±1.46) + 0.0045X1 + 0.000043X2
P<.001
0
2
4
6
8
10
12
14
60 120 180 240 300 360
Ischemic time (minutes)
1-Ye
ar m
orta
lity
(%)
In Other Words…
=
MuscleTime
Rapid Reperfusion in STEMI?
Up to one-third of eligible patients with STEMI receive no reperfusion therapy acutely
National Registry of Myocardial Infarction
Boden WE, et al. JACC. 2007;50:917-929.
Often NotWhy?
Age (75 years or older)Female gender Presentation without chest painHistory of cardiovascular disease Failure to identify high-risk ECG
National Registry of Myocardial Infarction
Boden WE, et al. JACC. 2007;50:917-929.
Missed Opportunities for Reperfusion in STEMI: The Emergency Department Quality
in Myocardial Infarction (EDQMI) Study
Examples of why reperfusion was withheld: Currently asymptomaticProlonged painPain alleviated with other medicationsOld ageWarfarin recently stopped (but INR not elevated)Concern for abdominal aortic aneurysm (but CT negative)
Tricomi AJ, et al. Am H J. 2008;155:471-477.
Missed Opportunities for Reperfusion in STEMI: The Emergency Department Quality
in Myocardial Infarction (EDQMI) Study
Tricomi AJ, et al. Am H J. 2008;155:471-477.

22
Rates of Reperfusion By Patient Subgroup
Nallamothu BK, et al. Am J Med. 2007;120:693-699.
6560
5550
80
75
70
95
90
85
100
Patie
nts
(%)
June 1994 to May 1997
June 1997 to May 2000
June 2000 to May 2003
Age ≥ 75
Women
Non-whites
No chest pain
Delayed presentation
Atypical Symptoms in Elderly STEMI Patients in NRMI
Population < 65 yr(%)
65-74 yr(%)
75-84 yr(%)
≥ 85 yr(%)
Killip class II-IV
11.7 23.4 33.3 44.6
LBBB 4.8 14.7 24.0 33.8
Chest pain 89.9 80.1 69.9 56.8
Alexander KP, et al. Circulation. 2007;115:2570-2589.
Reperfusion Therapy Based on Age in NRMI
Alexander KP, et al. Circulation. 2007;115:2570-2589.
Primary PCI
Lytics
< 65N=360,101
65-74191,093
75-84160,534
> 8563,952
Patient Age
2030405060
8070
100
% o
f Age
Gro
up
Absolute Mortality Advantage of PCI Over Fibrinolysis
1.04.2
5.1
6.9
(501) (452) (69) (78)(958)(894)(1892)(1919)No. of patients
< 65 yrs 65-74 yrs 75-84 yrs ≥ 85 yrs
Adapted from the Primary Coronary Angioplasty Trialist’s (PCAT)-2 Investigators.Boersma E, The Primary Coronary Angioplasty vs Thrombolysis Group. Eur Heart J. 2006;27(7):779-788.
0
5
10
15
20
25
30D
eath
in tr
eatm
ent a
rms
(%)
3.53.5
2.52.5
9.79.7
5.55.5
19.019.0
13.913.9
26.126.1
19.219.2
Primary PCI
Lytics
The Problem with Primary PCI
60% to 70% of STEMI patients present initially to hospitals without ready access to primary PCIData from NRMI-3 and -4 registries show that only 4% of STEMI patients who are transferred for primary PCI achieve door-to-balloon times of 90 min
National Registry of Myocardial Infarction
Boden WE, et al. JACC. 2007;50:917-929.
ACC/AHA 2004 STEMI Guidelines: Recommendations for Reperfusion Therapy
Early presentation ≤ 3 hrs of symptom onset and delay to invasive strategy
Invasive strategy is not an optionCatheterization lab occupied/not availableVascular access difficultiesLack of access to a skilled PCI lab (operator experience > 75 PCI cases/yr; team experience > 36 PCI cases/yr)
Delay to invasive strategyProlonged transport(Door-to-balloon) – (door-to-needle) time is > 1 hrMedical contact-to-balloon time is > 90 min
Primary PCI Preferred
Skilled PCI laboratory available with surgical backup
Medical contact-to-balloon time is < 90 min;(door-to-balloon) – (door-to-needle time) is< 1 hr
High risk from STEMICardiogenic shock Killip class ≥ 3
Contraindications to fibrinolysisIncluding increased risk of bleeding and ICH
Late presentationSymptom onset > 3 hrs ago
Diagnosis of STEMI is in doubt
Fibrinolytic Preferred
ICH=intracranial hemorrhage; PCI=percutaneous coronary intervention.
Antman EM, et al. J Am Coll Cardiol. 2004;44:671-719.
If presentation is < 3 hours and there is no delay to an invasive strategy, there is no preference for either strategy

23
Time to PCI Associated with Equilibration of PCI and Fibrinolysis
Fibr
inol
ysis
Bet
ter
PCI B
ette
r
2.0
1.5
1.25
1.0
0.8
0.560 75 90 105 114 135 150 165 180
Odd
s of
Dea
th w
ith F
ibrin
olys
is
PCI Related Delay (DB-DN) (min)Ant=anterior; NonAnt=non anterior; DB=door-to-balloon time; DN=door-to-needle time.
Based on a multivariate model that included: treatment type, age, gender, race, diabetes mellitus, hypertension, angina, Killip class 2/3, Killip class 4, previous infarction, current smoking, stroke, pulse,
systolic blood pressure, payer, symptom duration, infarct location, and discharge year.Pinto DS, et al. Circulation. 2006;114:2019.
Ant=anterior; NonAnt=non anteriorBased on a multivariate model that included: treatment type, age, gender, race, diabetes mellitus,
hypertension, angina, Killip class 2/3, Killip class 4, previous infarction, current smoking, stroke, pulse, systolic blood pressure, payer, symptom duration, infarct location, and discharge year.
Pinto DS, et al. Circulation. 2006;114:2019.
PCI R
elat
ed D
elay
(DB
-DN
) W
here
PC
I and
Fib
rinol
ytic
Mor
talit
y A
re E
qual
(Min
)
0-120 PrehospitalDelay (min)
121+
N=125,737
179
168148
107 103
58 43
40
Factors Associated with Equilibration of Mortality Benefit with Fibrinolysis
67%
7%
39%
0%
20%
40%
60%
80%
DTB ? 90 min—non-transfer in
DTB ? 90 min—transferin
DTN ? 30 min—all
Impact of Transfer on Door-to-balloon and –needle Time in STEMI Patients
DTB, 1st door to balloon for primary PCI; DTN, door to needle for lytics.NCDR ACTION Registry®–GWTGTM data: January 1, 2007–December 31, 2007 (n=19,523).
http://www.ncdr.com/webncdr/ACTION/Default.aspx
% o
f pat
ient
s
Door-to-balloon Time for Patients Transferred for Primary PCI
(N=4278)
Total door-to-balloon time (hours)
% o
f pat
ient
s
Nallamothu BK, et al. Circulation. 2005;111:761–767.
0.3
15.9
33.2
21.8
13.6
7.8
4.43.0
0
5
10
15
20
25
30
35
<1 1 to <2 2 to <3 3 to <4 4 to <5 5 to <6 6 to <7 >=7
Mortality rate for in-hospital fibrinolysis
00.
020.
040.
060.
080.
100.
120.
14
Mor
talit
y ra
te fo
r pre
-hos
pita
l fib
rinol
ysis
0 0.02 0.04 0.06 0.08 0.10 0.12 0.14
Favors in-hospital fibrinolysis
Favors pre-hospital fibrinolysis
Mortality Benefit with Pre-hospital Fibrinolysis vs In-hospital Fibrinolysis
Morrison LJ, et al. JAMA. 2000;283:2686–2692.
Six (6) studies were included in meta-analysis. Plot shows rate of hospital mortality measured in each study, demonstrating consistent outcome rates favoring pre-hospital fibrinolysis.
ED-Pertinent Changes in STEMI Guideline RecommendationsPrimary PCI vs Fibrinolysis
Primary PCI is recommended within 90 minutes as a systems goal (I-A)Fibrinolysis is recommended within 30 minutes as a system goal if primary PCI cannot be accomplished within 90 minutes (I-B)
Pollack CV, et al. Ann Emerg Med. 2008 [Epub ahead of print].
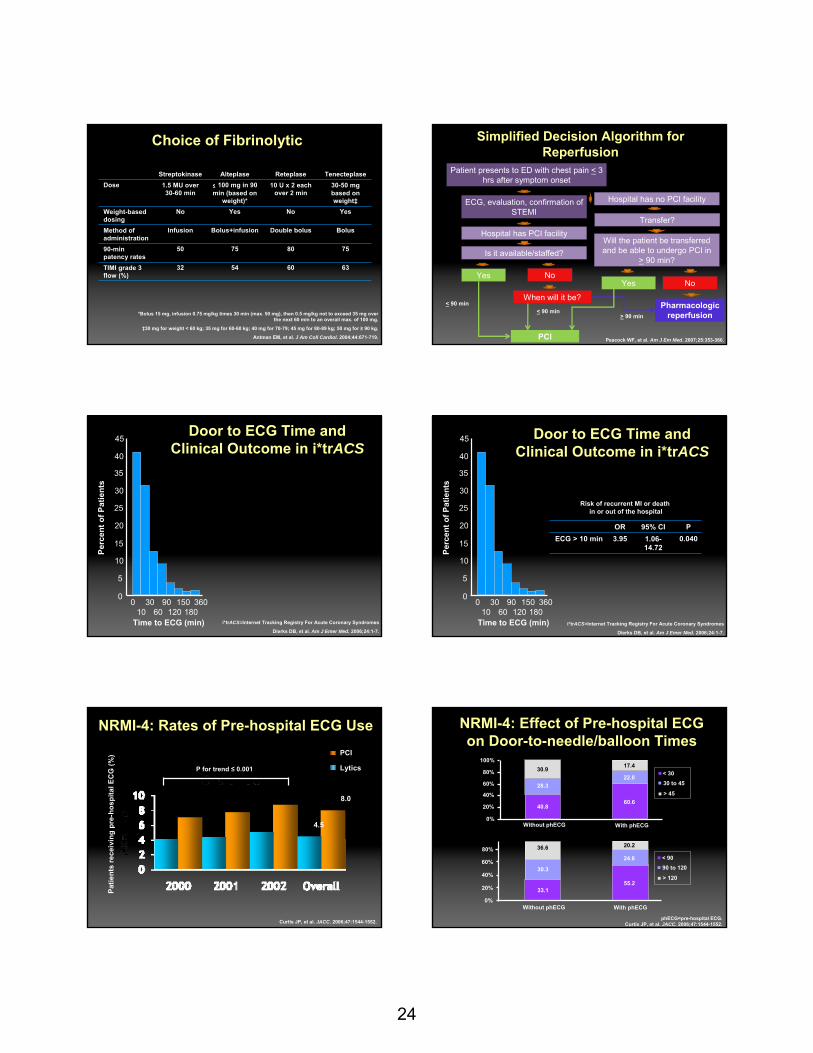
24
Choice of Fibrinolytic
Streptokinase Alteplase Reteplase TenecteplaseDose 1.5 MU over
30-60 min≤ 100 mg in 90 min (based on
weight)*
10 U x 2 each over 2 min
30-50 mg based on weight‡
Weight-based dosing
No Yes No Yes
Method of administration
Infusion Bolus+infusion Double bolus Bolus
90-min patency rates
50 75 80 75
TIMI grade 3 flow (%)
32 54 60 63
*Bolus 15 mg, infusion 0.75 mg/kg times 30 min (max. 50 mg), then 0.5 mg/kg not to exceed 35 mg over the next 60 min to an overall max. of 100 mg.
‡30 mg for weight < 60 kg; 35 mg for 60-60 kg; 40 mg for 70-79; 45 mg for 80-89 kg; 50 mg for ≥ 90 kg.
Antman EM, et al. J Am Coll Cardiol. 2004;44:671-719.
Simplified Decision Algorithm for Reperfusion
Patient presents to ED with chest pain < 3 hrs after symptom onset
ECG, evaluation, confirmation of STEMI
Hospital has no PCI facility
Transfer?
Will the patient be transferred and be able to undergo PCI in
> 90 min?
NoYes
Pharmacologic reperfusion
Hospital has PCI facility
Is it available/staffed?
Yes No
PCI
When will it be?< 90 min
> 90 min
< 90 min
Peacock WF, et al. Am J Em Med. 2007;25:353-366.
Door to ECG Time and Clinical Outcome in i*trACS
i*trACS=Internet Tracking Registry For Acute Coronary Syndromes
Dierks DB, et al. Am J Emer Med. 2006;24:1-7.
Perc
ent o
f Pat
ient
s
45
40
35
30
25
20
15
10
5
0360
180150
12090
6030
100
Time to ECG (min) i*trACS=Internet Tracking Registry For Acute Coronary Syndromes
Dierks DB, et al. Am J Emer Med. 2006;24:1-7.
OR 95% CI PECG > 10 min 3.95 1.06-
14.720.040
Risk of recurrent MI or death in or out of the hospital
Perc
ent o
f Pat
ient
s45
40
35
30
25
20
15
10
5
0360
180150
12090
6030
100
Time to ECG (min)
Door to ECG Time and Clinical Outcome in i*trACS
NRMI-4: Rates of Pre-hospital ECG Use
P for trend ≤ 0.001
4.5
8.0
Curtis JP, et al. JACC. 2006;47:1544-1552.
Patie
nts
rece
ivin
g pr
e-ho
spita
l EC
G (%
) PCI
Lytics
NRMI-4: Effect of Pre-hospital ECG on Door-to-needle/balloon Times
60.6
22.0
17.430.9
28.3
40.8
36.6
30.3
33.155.2
24.6
20.2
100%
80%
60%
40%
20%
0%Without phECG With phECG
< 3030 to 45
> 45
80%
60%
40%
20%
0%Without phECG With phECG
< 9090 to 120
> 120
phECG=pre-hospital ECG. Curtis JP, et al. JACC. 2006;47:1544-1552.

25
ED Activation of and Immediate Transfer to Cath Lab Saves Time
Cardiol eval
Cath lab activation
Cath lab staff arrival
Cath lab setup
Transfer to cath lab
Door
EKG
ED eval
Cath/PCI
Cardiology Activation/Routine Transfer ED Activation/Immediate Transfer
Cath lab Transfer to Cath lab Cardiolactivation cath lab setup eval
Door
EKG
ED eval
Cath/PCI
5% with door-to-balloon < 60 min
17% with door-to-balloon
< 60 min*
*P<0.0001; proportion of patients treated within < 60 minutes. Khot UN, et al. Circulation. 2007;116:67-76.
RACE Regions and Hospitals According to Reperfusion System
RACE: Reperfusion of Acute Myocardial Infarction in North Caroline Emergency DepartmentsJollis JG, et al. JAMA. 2007;298(20):2371-2380.
RACE: Treatment Times for Patients at PCI Hospitals
Pre-intervention
Post-intervention
P value
All primary PCI patients N=266 N=359Door-to-device, median (min) 106 90 < .001% Patients < 90 min 36.5% 51.3% < .001
Patients presenting directly to PCI hospital
N=164 n=232
Door-to-device median (min) 85 74 < .001% Patients < 90 min 56.7% 72.0% .002
Patients transferred to PCI hospital
N=102 N=127
Door-to-device median (min) 165 128 < .001% Patients < 90 min 3.9 13.4 .01
Jollis JG, et al. JAMA. 2007;298(20):2371-2380.
RACE: Treatment Times for Patients at non-PCI Hospitals
Pre-intervention
Post-intervention
P value
All patients N=515 N=404Door-in to door-out, median (min) 120 71 < .001% Patients < 60 min 15.7% 37.6% < .001% Patients < 30 min 3.1% 10.2% < .001
Patients at fibrinolysis hospitals N=239 N=201Door-in to door-out, median (min) 125 87 < .001% Patients < 60 min 5.4% 18.4% < .001% Patients < 30 min 0.8% 0.5% .67
Fibrinolysis N=233 N=158Door-to-needle, median (min) 35 29 .002% Patients < 30 min 34.8% 51.9% < .001
Jollis JG, et al. JAMA. 2007;298(20):2371-2380.
Identification: Medic paramedics are trained to acquire and read 12-lead electrocardiograms (ECG) on patients suspected of a heart attack. The ECG result is quickly transmitted from the field to an ED physician at CMC.Activation: If the ECG shows specific changes in certain electrical impulses (ST segments) within the heart, the Emergency physician activates “Code STEMI” initiating an immediate response from the Code STEMI Team. Treatment: Patient is received by Code STEMI Team upon arrival to CMC ED with a rapid triage process to confirm STEMI and then immediately transported to the cardiac catheterization lab where the coronary artery is opened
Program objective: develop a coordinated system of care - modeled after Code Trauma - that streamlines the identification, activation, and provision of
treatment for STEMI that surpasses national targets.
New CMC ProcessCode STEMI – Protocol Driven Program
Carolinas Medical Center, 2008.
Critical Success FactorsEMS and ED Physician initiate Code STEMI Single page activates entire team => parallel actions commence
ED and Cath Lab begin preparationsOn-Call Cardiologist and CCU Nurse go to EDRespiratory Care and Laboratory are available in EDJoint assessment occurs in the EDCardiologist and CCU Nurse assist EMS in transporting patient to Cath LabPatient is prepared for PCIBed Management finds accommodations
Trust in revised roles and responsibilitiesCarolinas Medical Center, 2008.

26
Lessons Learned fromCarolinas Medical Center
It takes real commitment from the Multi-disciplinary TeamEMS, ED Physicians, Cardiologists, ED Staff, Cath Lab, CCU, Bed Management, Lab, Radiology, Respiratory Care, House Supervisor
Establish a specific goal to Meet or Exceed ACC Standard Adopt a continuous process improvement philosophy => on-going monitoring and modification of the processIntensive education for EMS on acquiring and interpreting ECGsRecognize that a cultural change is necessaryBe flexible – forward thinking => all play in same sandboxTrust in revised roles and responsibilities
Carolinas Medical Center, 2008.
Two Questions the ED Should Answer for Patients Presenting
with Potential ACS
Pollack CV, Jr. and Braunwald E. Ann Emerg Med. 2008;51:591-606.
What is the likelihood that the presenting symptoms represent acute coronary syndrome as a result of coronary artery disease?What is the likelihood of an adverse cardiovascular outcome?
ACC/AHA 2007 UA/NSTEMI Guidelines: Features that Make ACS Secondary to CAD Highly Likely
Anderson JL, et al. JACC. 2007;50(7):1-157.
Feature Any of the following:History Chest or left arm pain or discomfort as chief symptom
reproducing prior documented anginaKnown history of CAD, including MI
Examination Transient MR, murmur, hypotension, diaphoresis, pulmonary edema, or rales
ECG New, or presumably new, transient ST-segment deviation (1 mm or greater) or T-wave inversion in multiple precordial leads
Cardiac markers
Elevated cardiac Tnl, TnT, or CK-MB
Serum Cardiac Biomarker Concentrations Following AMI
cTn=cardiac troponin.
Wu AHB, et al. Clin Chem. 1999;45:1104-1121.
A. Early release of myoglobin or CKMBB. cTn after AMIC. CKMB after AMID. cTn after UA
D.
C.
B.
A.
5
10
20
50
0
1
2
4 5 6 7 81 2 30
Days After Onset of AMI
Mul
tiple
s of
the
AM
I Cut
off L
imit
AMI decision limitUpper reference limit
Odds of ACS: Concordant and Discordant Biomarkers in NSTEMI
Patients
Storrow AB, et al. Ann Emerg Med. 2006;48:660-665.
Biomarkers Odds Ratio 95% CI (Odds Ratio)
CKMB(+)/CK(-) 5.70 (4.38-7.40)
CKMB(+)/CK(+) 4.36 (3.64-5.23)
CKMB(-)/cTn(+) 4.79 (3.40-6.76)
CKMB(+)/cTn(-) 2.17 (1.72-2.75)
CKMB(+)/cTn(+) 26.58 (18.00-39.30)
ACC/AHA 2007 UA/NSTEMI Guidelines: Short-term High Risk of Death or Nonfatal
MI in UA/NSTEMI Patients
Anderson JL, et al. JACC. 2007;50(7):1-157.
Feature At least one of the following:History Accelerating ischemic symptoms in preceding 48 hrs
Character of pain
Prolonged ongoing (greater than 20 min) rest pain
Clinical findings
- Pulmonary edema, most likely due to ischemia- New or worsening MR murmur- S3 or new/worsening rales- Hypotension, bradycardia, tachycardia- Age > 75 years
ECG - Angina at rest with transient ST-segment changes > .5 mm- BBB, new or presumed new- Sustained ventricular tachycardia
Cardiac markers
Elevated cardiac TnT, TnI, or CK-MB

27
ACC/AHA 2007 UA/NSTEMI Guidelines: Early Risk Stratification for Likely ACS
Patients
*Level of evidenceAnderson JL, et al. JACC. 2007;50(7):1-157.
Class I RecommendationsRapid determination of risk of obstructive CAD (C)*Determine risk of CV events (C)12-lead ECG within 10 min of ED arrival (B)
Serial ECGs for symptomatic patients with nondiagnostic initial ECG (B)Measure cardiac biomarkers (B)- Cardiac-specific troponin is preferred (B)- Remeasure at 8-12 h if initially negative
Consider noncoronary causes for unexplained symptoms (C)
ACC/AHA 2007 UA/NSTEMI Guidelines: Early Risk Stratification for Likely ACS
Patients
*Level of evidenceAnderson JL, et al. JACC. 2007;50(7):1-157.
Class IIa Recommendations
Risk-stratification models (eg, TIMI/GRACE risk score or PURSUIT risk model) can be useful (B)*
Reasonable to remeasure positive biomarkers at 6- to 8-h to assess infarct size/necrosis (B)
Reasonable to obtain supplemental ECG leads V7-V9 in patients with initial nondiagnostic ECG (B)
Continuous 12-lead ECG in appropriate patients (B)
LMWH Dosing Often Incorrect in NSTEMI Patients
LaPointe NM, et al. Am J Med. 2007;167(14):1539-1544.
2000
0
6000
4000
Patie
nts
(num
ber)
Lower-than-recommended
doseExcess
dose
> -100 -100to
< -30
-30to
< -10
-10to10
> 10to30
> 30to
100
> 100
Administered dose-recommended dose (mg/d)
Improper LMWH Dosing Has Negative Consequences
LaPointe NM, et al. Am J Med. 2007;167(14):1539-1544.
10
0
20
15
5Patie
nts
(%)
Lower-than-recommended doseRecommended doseExcess dose
Major bleeding Death(%) (%)
7.9 7.3
14.2
3.3 2.4
5.6
P = .50
P < .001
P = .11
P < .001
In-hospital Impact of GP IIb/IIIaInhibitor Use: CRUSADE Data
* Upstream GP IIb/IIIa inhibitors vs periprocedural GP IIb/IIIa inhibitors; † No GP IIb/IIIa inhibitors versus upstream GP IIb/IIIa inhibitor.
Tricoci P, et al. Am J Cardiol. 2007;99(10):1389-93.
IIb/IIIaOverall
(%)UpstreamIIb/IIIa (%)
Peri-proceduralIIb/IIIa (%)
P value*
No IIb/IIIa (%)
P value†
Death 1.3 1.3 1.4 .352 2.1 < .001
Recurrent MI 3.0 2.8 3.1 .085 3.4 .009
Death or reinfarction 4.1 3.8 4.3 .046 5.0 .001
Cardiogenicshock 2.3 2.1 2.5 .029 2.7 .004
Heart failure 4.7 4.9 4.5 .151 7.0 < .001
Stroke 0.4 0.3 0.4 .285 0.6 .003
Any RBC transfusion 7.1 7.3 7.0 .323 1.06 < .001
ED-pertinent Data on NonheparinAnticoagulation in STEMI Therapy
Anticoagulant Efficacy with Lysis
Safety with Lysis Use in Primary PCI
Use in PCI after Lysis
Enoxaparin Superior to UFH
Increased major bleeding events, but not ICH, compared with UFH
Not adequately studied
Can be used to support PCI without additional anticoagulation
Fondaparinux* Superior to UFH/placebo (relative performance uncertain)
Trend toward fewer major bleeding events compared with UFH/placebo
Increased risk of catheter thrombosis
Not adequately studied
Bivalirudin* Not adequately studied
Not adequately studied
Appears to be noninferior to UFH+GPI for efficacy with reduced bleeding
Not specifically studied
*Not approved by FDA for indicationPollack CV, et al. Ann Emerg Med. 2008 [Epub ahead of print].

28
Recommendations for Antithrombotic Therapy in NSTEMI ACS Patients in the
2007 ACC/AHA Guidelines
LOE=Level of evidenceAdapted from Pollack CV, Jr. and Braunwald E. Ann Emerg Med. 2008;51:591-606.
Agent Invasive Strategy (LOE)*
Conservative Strategy (LOE)*
UFH Initiate(I-A) Initiate (I-A)Enoxaparin Initiate (I-A) Initiate (I-A)Fondaparinux Initiate (I-B) Initiate (I-B)Bivalirudin Initiate (I-B) -
Recommendations for Antiplatelet Therapy in NSTEMI ACS in 2007 ACC/AHA Guidelines
Agent Recommendation Level of Evidence
ASA Initiate promptly I-A
Clopidogrel 1. Initiate promptly in ASA-allergy (loading dose)2. EIS: Initiate with loading dose ASAP OR give
small molecule GPI3. Hold if CABG planned within 5-7 days4. SIS: Initiate with loading dose ASAP OR give
small-molecule GPI
1. I-A2. I-A
3. I-B
4. I-A
Small-molecule GPI
1. EIS: Initiate OR give loading dose of clopidogrel2. EIS: Initiate AND give loading dose of clopidogrel3. SIS with later high risk: Initiate upstream4. EIS: May omit upstream GPI if patient receives
bivalirudin and at least 300 mg clopidogrel <6 h before cath and PCI
1. I-A2. IIa-B3. IIa-C4. IIa-B
Large-molecule GPI
1. EIS: initiate2. Not appropriate for medical management when
PCI not planned < 24 h
1. I-A2. III-A
EIS-Early invasive strategy; SIS-Selective invasive strategy; GPI – Iib/IIIa glycoprotein inhibitorAdapted from Pollack CV, Jr. and Braunwald E. Ann Emerg Med. 2008;51:591-606.
Do you think primary PCI is unduly preferred over fibrinolysis? If so, why?
What strategies has your hospital implemented to shorten time to
reperfusion in STEMI?
What are the barriers to system-wide changes to reduce
time to reperfusion in STEMI?
How can EDs improve evidence-based
MI and ACS care for the elderly?
For women?
Questions for Discussion
166
Bleeding and TransfusionRecognizing the Impact on
Vascular Outcomes
James A. de Lemos, MDDirector, Coronary Care UnitParkland Memorial Hospital
Dallas, TX
167
•Delineate the implications of major bleeding in the ACS
patient•Analyze the bleeding risks
posed by various therapeutic interventions in ACS
•Enumerate strategies for reducing bleeding risk in
diverse ACS patients
Learning Objectives In your view, which is more important in acute ACS treatment?
1. Reperfusion success2. Avoiding bleeding3. Both are equally important4. Unsure

29
Which statement most closely reflects your point of view in the context of acute ACS therapy?
1. Major bleeding is the necessary cost of improved reperfusion therapies
2. Little can be done to avoid major bleeding3. Newer anticoagulants can significantly
reduce major bleeding4. Newer anticoagulants make major bleeding
a more likely outcome
Moscucci M, et al. Eur Heart J. 2003;24:1815-1823.
Rates of Major Bleeding in ACS:The GRACE Registry
• Life-threatening with transfusion ≥ 2 units• Life-threatening with decrease in HCT >10%• Resulting in death• Hemorrhagic, subdural hematoma
3.9
2.3
4.7 4.8
0
1
2
3
4
5
6
OverallACS
UnstableAngina
NSTEMI STEMI
Major BleedingMajor Bleeding
Patie
nts
(%)
Patie
nts
(%)
(N=24,045)
171
How Is Bleeding Defined (and Does It Matter)?
Temporal Trends in Major Bleeding: The University of Michigan Experience
Motivala AA, et al. Am J Cardiol. 2007;100:1359-1363.
Which of the following have been included in major bleeding criteria in clinical trials?
1. Intracranial hemorrhage2. Decreased hematocrit3. Need for transfusion4. Pulse above 120 bpm5. 1, 2, and 36. All of the above
Bleeding Classifications
ICH=intracranial hemorrhage; Hb=hemoglobin. TIMI definitions take transfusion into account, so Hb and hematocrit
are adjusted by 1 g/dl or 3%, respectively, for each unit of blood transfused.The GUSTO Investigators. NEJM. 1993;329:673-682.
Chesebro JH, et al. Circulation. 1987;76:142-154.Rao SV, et al. JACC. 2006;47:809-816.
TIMI Bleeding ClassificationMajor ICH or a ≥ 5 g/dl decrease in Hb or a ≥ 15% absolute decrease in hematocrit
Minor Observed blood loss: ≥ 3 g/dl decrease in Hb or ≥ 10% decrease in hematocritNo observed blood loss: ≥ 4 g/dl decrease in Hb or ≥ 12% decrease in hematocrit
Minimal Any clinically overt sign of hemorrhage (including imaging) that is associated with a < 3 g/dl decrease in Hb or < 9%decrease in hematocrit
GUSTO Bleeding ClassificationSevere or life-threatening
Either ICH or bleeding causing hemodynamic compromise and requiring intervention
Moderate Bleeding requiring blood transfusion but not resulting in hemodynamic compromise
Mild Bleeding that doesn’t meet Severe/Moderate criteria
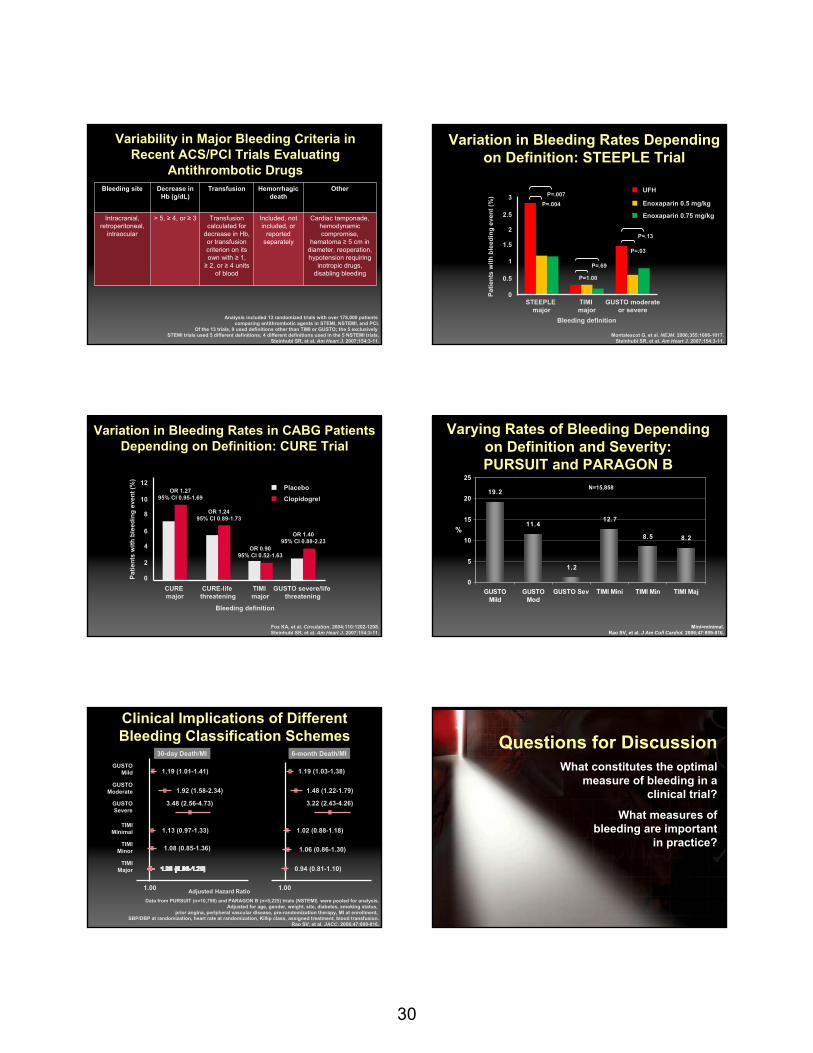
30
Variability in Major Bleeding Criteria in Recent ACS/PCI Trials Evaluating
Antithrombotic Drugs
Analysis included 13 randomized trials with over 178,000 patients comparing antithrombotic agents in STEMI, NSTEMI, and PCI.
Of the 13 trials, 9 used definitions other than TIMI or GUSTO; the 5 exclusively STEMI trials used 5 different definitions; 4 different definitions used in the 5 NSTEMI trials.
Steinhubl SR, et al. Am Heart J. 2007;154:3-11.
Bleeding site Decrease in Hb (g/dL)
Transfusion Hemorrhagic death
Other
Intracranial, retroperitoneal,
intraocular
> 5, ≥ 4, or ≥ 3 Transfusion calculated for
decrease in Hb, or transfusion criterion on its own with ≥ 1, ≥ 2, or ≥ 4 units
of blood
Included, not included, or
reported separately
Cardiac tamponade, hemodynamic compromise,
hematoma ≥ 5 cm in diameter, reoperation, hypotension requiring
inotropic drugs, disabling bleeding
Variation in Bleeding Rates Depending on Definition: STEEPLE Trial
Montalescot G, et al. NEJM. 2006;355:1006-1017.Steinhubl SR, et al. Am Heart J. 2007;154:3-11.
STEEPLE major
TIMI major
GUSTO moderateor severe
Bleeding definition
Patie
nts
with
ble
edin
g ev
ent (
%)
0
0.5
1
1.5
2
2.5
3UFH
Enoxaparin 0.5 mg/kg
Enoxaparin 0.75 mg/kg
P=.007P=.004
P=.69
P=1.00
P=.13
P=.03
Variation in Bleeding Rates in CABG Patients Depending on Definition: CURE Trial
Bleeding definition
CURE major
CURE-life threatening
TIMI major
0
2
4
6
8
10
12PlaceboClopidogrel
OR 1.2795% CI 0.95-1.69
OR 1.2495% CI 0.89-1.73
OR 0.9095% CI 0.52-1.63
OR 1.4095% CI 0.88-2.23
GUSTO severe/life threatening
Patie
nts
with
ble
edin
g ev
ent (
%)
Fox KA, et al. Circulation. 2004;110:1202-1208.Steinhubl SR, et al. Am Heart J. 2007;154:3-11.
Varying Rates of Bleeding Depending on Definition and Severity: PURSUIT and PARAGON B
8.5 8.2
12.7
1.2
11.4
19.2
0
5
10
15
20
25
GUSTOMild
GUSTOMod
GUSTO Sev TIMI Mini TIMI Min TIMI Maj
%
N=15,858
Mini=minimal. Rao SV, et al. J Am Coll Cardiol. 2006;47:809-816.
Clinical Implications of Different Bleeding Classification Schemes
GUSTOMild
GUSTOModerate
GUSTOSevere
TIMIMinimal
TIMIMinor
TIMIMajor
1.00 1.00
1.19 (1.01-1.41)
1.92 (1.58-2.34)
3.48 (2.56-4.73)
1.13 (0.97-1.33)
1.08 (0.85-1.36)
1.19 (1.03-1.38)
1.48 (1.22-1.79)
3.22 (2.43-4.26)
1.02 (0.88-1.18)
1.06 (0.86-1.30)
0.94 (0.81-1.10)
Data from PURSUIT (n=10,798) and PARAGON B (n=5,225) trials (NSTEMI) were pooled for analysis.Adjusted for age, gender, weight, site, diabetes, smoking status,
prior angina, peripheral vascular disease, pre-randomization therapy, MI at enrollment, SBP/DBP at randomization, heart rate at randomization, Killip class, assigned treatment, blood transfusion.
Rao SV, et al. JACC. 2006;47:809-816.
30-day Death/MI 6-month Death/MI
Adjusted Hazard Ratio
180
Questions for DiscussionWhat constitutes the optimal
measure of bleeding in a clinical trial?
What measures of bleeding are important
in practice?
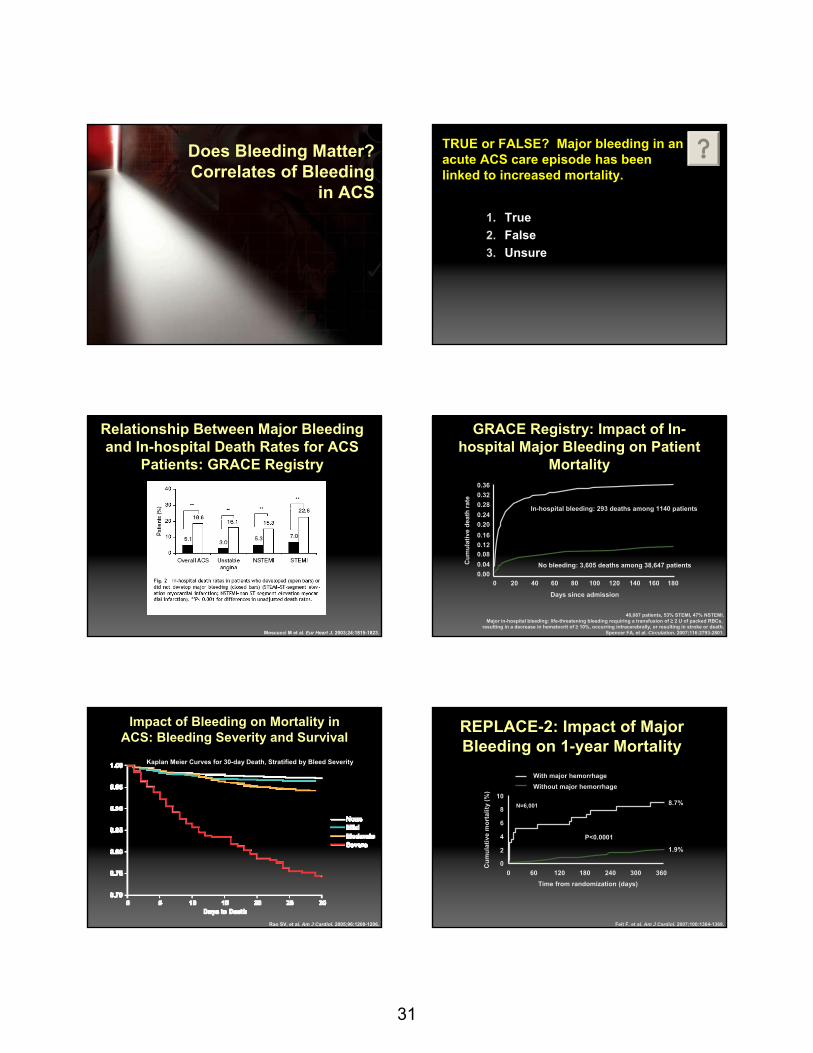
31
181
Does Bleeding Matter? Correlates of Bleeding
in ACS
TRUE or FALSE? Major bleeding in an acute ACS care episode has been linked to increased mortality.
1. True2. False3. Unsure
Relationship Between Major Bleeding and In-hospital Death Rates for ACS
Patients: GRACE Registry
Moscucci M et al. Eur Heart J. 2003;24:1815-1823.
GRACE Registry: Impact of In-hospital Major Bleeding on Patient
Mortality
40,087 patients, 53% STEMI, 47% NSTEMI.Major in-hospital bleeding: life-threatening bleeding requiring a transfusion of ≥ 2 U of packed RBCs,
resulting in a decrease in hematocrit of ≥ 10%, occurring intracerebrally, or resulting in stroke or death.Spencer FA, et al. Circulation. 2007;116:2793-2801.
In-hospital bleeding: 293 deaths among 1140 patients
No bleeding: 3,605 deaths among 38,647 patients
Days since admission
Cum
ulat
ive
deat
h ra
te
0 20 40 60 80 100 120 140 160 1800.000.040.080.120.160.200.240.280.320.36
Impact of Bleeding on Mortality in ACS: Bleeding Severity and Survival
Kaplan Meier Curves for 30-day Death, Stratified by Bleed Severity
Rao SV, et al. Am J Cardiol. 2005;96:1200-1206.
REPLACE-2: Impact of Major Bleeding on 1-year Mortality
Feit F, et al. Am J Cardiol. 2007;100:1364-1369.
0 60 120 180 240 300 3600
2
4
6
8
10
Cum
ulat
ive
mor
talit
y (%
)
Time from randomization (days)
8.7%
1.9%
P<0.0001
Without major hemorrhageWith major hemorrhage
N=6,001

32
Impact of Baseline Hemoglobin Levels on CV Death: STEMI
41,637 patients from 16 TIMI trials, 25,419 STEMI patients,14,503 NSTEMI patients.Sabatine MS, et al. Circulation.2005;111:2042-2049.
Impact of Baseline Hemoglobin Levels on CV Death: NSTEMI
41,637 patients from 16 TIMI trials, 25,419 STEMI patients, 14,503 NSTEMI patients.Sabatine MS, et al. Circulation. 2005;111:2042-2049.
GUSTO-1: In-hospital Predictors of Late Death
Califf RM, et al. Circulation. 2000;101:2231-2238.
Is Bleeding Associated with Higher Mortality? TIMI Major Bleeding
Steinhubl SR, et al. Am Heart J. 2007;154:3-11.
Bleeding definition
Patient population
Early mortality and/or other major CV events (in-hospital or 30-day)
Late mortality (6-month or 1-year)
TIMI major bleeding
STEMI ― ―
NSTEMI Higher adjusted mortality/MI rates
Higher adjusted mortality/MI rates
PCI Independent predictor Higher mortality rates, but not an independent
predictorOverall
ConclusionYes Conflicting
Is Bleeding Associated with Higher Mortality?GUSTO Moderate or Severe Bleeding
Steinhubl SR, et al. Am Heart J. 2007;154:3-11.
Bleeding definition
Patient Population
Early mortality and/or other major CV events (in-hospital or 30-day)
Late mortality (6-month or 1-year)
GUSTO moderate or severe bleeding
STEMI Higher mortality/MI rates
Higher mortality rates, but not an independent
predictor in 30-day survivors
NSTEMI Higher mortality/MI rates; independent
predictor
Higher adjusted mortality/MI hazard
PCI ― ―Overall
conclusionYes Conflicting
Is Bleeding Associated with Higher Mortality?Blood Transfusion and Hemoglobin Levels
Bleeding definition
Patient population Early mortality and/or other major
cardiovascular events (in-hospital or 30-day)
Late mortality (6-month or
1-year)
Blood transfusion STEMI Not a predictor ―
NSTEMI Higher mortality rates ―
Both STEMI and NSTEMI
Mortality association depending on hematocrit
levels and NSTEMI vs. STEMI
―
PCI Independent predictor Independent predictor
Overall conclusion Conflicting Yes
Drop in hemoglobin
Both STEMI and NSTEMI
Independent predictor ―
Overall conclusion Yes ―
Steinhubl SR, et al. Am Heart J. 2007;154:3-11.
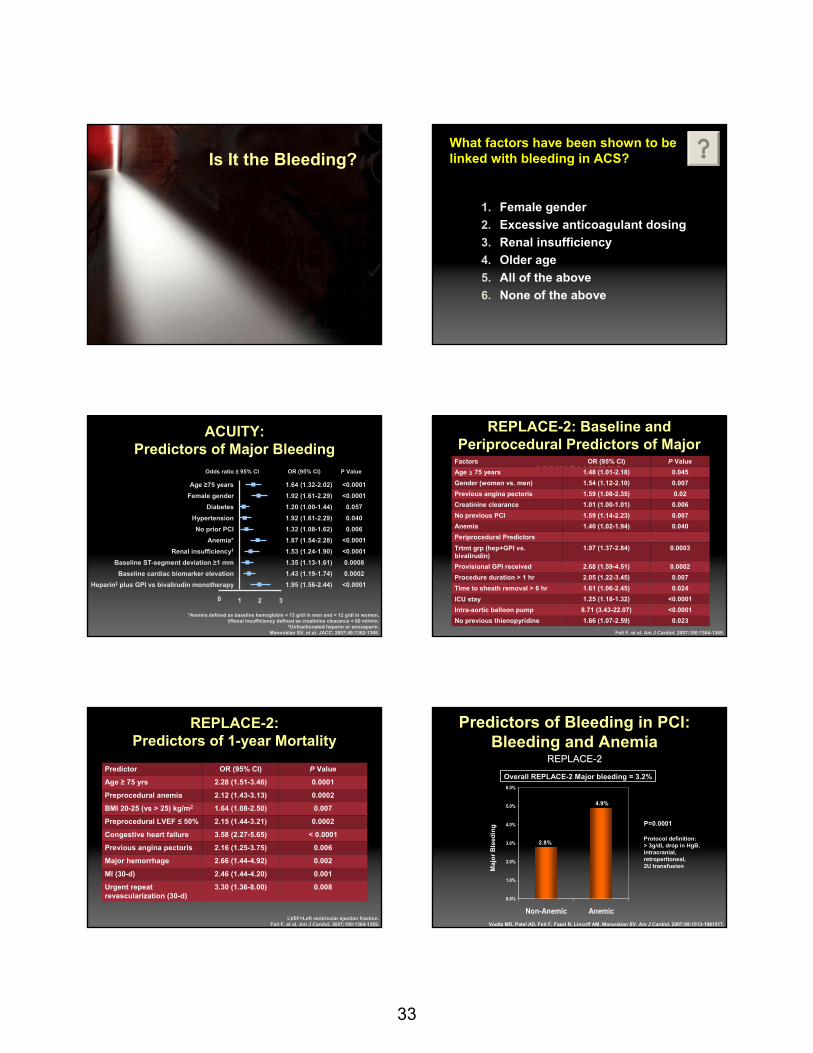
33
193
Is It the Bleeding?What factors have been shown to be linked with bleeding in ACS?
1. Female gender2. Excessive anticoagulant dosing3. Renal insufficiency4. Older age5. All of the above6. None of the above
ACUITY: Predictors of Major Bleeding
Age ≥75 yearsFemale gender
DiabetesHypertensionNo prior PCI
Anemia*Renal insufficiency†
Baseline ST-segment deviation ≥1 mmBaseline cardiac biomarker elevation
Heparin‡ plus GPI vs bivalirudin monotherapy
0 1 2 3
1.64 (1.32-2.02) <0.0001
Odds ratio ± 95% CI OR (95% CI) P Value
1.92 (1.61-2.29)
<0.00011.20 (1.00-1.44) 0.0571.92 (1.61-2.29)
0.0401.32 (1.08-1.62) 0.0061.87 (1.54-2.28) <0.00011.53 (1.24-1.90) <0.00011.35 (1.13-1.61) 0.00081.43 (1.19-1.74) 0.00021.95 (1.56-2.44) <0.0001
*Anemia defined as baseline hemoglobin < 13 g/dl in men and < 12 g/dl in women.†Renal insufficiency defined as creatinine clearance < 60 ml/min.
‡Unfractionated heparin or enoxaparin.Manoukian SV, et al. JACC. 2007;49:1362-1368.
REPLACE-2: Baseline and Periprocedural Predictors of Major
Hemorrhage
Feit F, et al. Am J Cardiol. 2007;100:1364-1369.
Factors OR (95% CI) P ValueAge ≥ 75 years 1.48 (1.01-2.18) 0.045Gender (women vs. men) 1.54 (1.12-2.10) 0.007Previous angina pectoris 1.59 (1.08-2.35) 0.02Creatinine clearance 1.01 (1.00-1.01) 0.006No previous PCI 1.59 (1.14-2.23) 0.007Anemia 1.40 (1.02-1.94) 0.040Periprocedural PredictorsTrtmt grp (hep+GPI vs. bivalirudin)
1.97 (1.37-2.84) 0.0003
Provisional GPI received 2.68 (1.59-4.51) 0.0002Procedure duration > 1 hr 2.05 (1.22-3.45) 0.007Time to sheath removal > 6 hr 1.61 (1.06-2.45) 0.024ICU stay 1.25 (1.18-1.32) <0.0001Intra-aortic balloon pump 8.71 (3.43-22.07) <0.0001No previous thienopyridine 1.66 (1.07-2.59) 0.023
REPLACE-2: Predictors of 1-year Mortality
LVEF=Left ventricular ejection fraction.Feit F, et al. Am J Cardiol. 2007;100:1364-1369.
Predictor OR (95% CI) P Value
Age ≥ 75 yrs 2.28 (1.51-3.46) 0.0001
Preprocedural anemia 2.12 (1.43-3.13) 0.0002
BMI 20-25 (vs > 25) kg/m2 1.64 (1.08-2.50) 0.007
Preprocedural LVEF ≤ 50% 2.15 (1.44-3.21) 0.0002
Congestive heart failure 3.58 (2.27-5.65) < 0.0001
Previous angina pectoris 2.16 (1.25-3.75) 0.006
Major hemorrhage 2.66 (1.44-4.92) 0.002
MI (30-d) 2.46 (1.44-4.20) 0.001
Urgent repeat revascularization (30-d)
3.30 (1.36-8.00) 0.008
Predictors of Bleeding in PCI:Bleeding and Anemia
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
Non-Anemic Anemic
Overall REPLACE-2 Major bleeding = 3.2%
Maj
or B
leed
ing
2.8%
4.9%
P=0.0001
Protocol definition: > 3g/dL drop in HgB, intracranial, retroperitoneal, 2U transfusion
Voeltz MD, Patel AD, Feit F, Fazel R, Lincoff AM, Manoukian SV. Am J Cardiol. 2007;99:1513-1981517.
REPLACE-2REPLACEREPLACE--22

34
Predictors of In-hospital Bleeding Within 30 Days: GRACE Registry, Patient Characteristics
Variable Total Cohort,† HR (95% CI)
History of prior bleeding 2.70 (1.84-3.96)
Glomerular filtration rate < 30mL/min‡Early bleeding (0-2d)/Late bleeding (3-30 d) 2.40 (1.76-3.29)/1.83 (1.25-2.68)
Pulmonary artery catheterEarly bleeding (0-1 d)/ Late bleeding (2-30 d)
1.65 (1.18-2.29)/2.04 (1.53-2.72)
Female sexEarly bleeding (0-2 d)/Late bleeding (3-30 d)
1.36 (1.12-1.65)/1.84 (1.44-2.35)
Age per 10-y increaseEarly bleeding (0-2 d)/Late bleeding (3-30 d) 1.35 (1.25-1.47)/1.53 (1.36-1.72)
ST deviation on initial ECG 1.47 (1.21-1.80)
Glomerular filtration rate 30-59 mL/minEarly bleeding (0-2 d)/Late bleeding (3-30 d) 1.44 (1.16-1.79)/1.12 (0.85-1.46)
History of atrial fibrillationEarly bleeding (0-2 d)/Late bleeding (3-30 d) 0.95 (0.69-1.31)/1.41 (1.01-1.96)
†Data for n=28,327 patients with complete covariate information, 766 with major bleeding; ‡Reference category: glomerular filtration rate ≥ 60 mL/min
Spencer FA, et al. Circulation. 2007;116:2793-2801.
Predictors of In-hospital Bleeding Within 30 Days: GRACE Registry,
Patient Characteristics (con’t) Variable Total Cohort,† HR (95% CI)
History of peripheral arterial disease 1.37 (1.11-1.68)
History of smoking 1.23 (1.0-1.44)
Heart rate per 30 bpm increaseEarly bleeding (0-1 d)/Late bleeding (2-30 d) 1.05 (0.92-1.20)/1.16 (1.03-1.30)
History of hypertensionEarly bleeding (0-1 d)/Late bleeding (2-30 d) 0.79 (0.64-0.98)/1.22 (0.98-1.53)
History of atrial fibrillationEarly bleeding (0-2 d)/Late bleeding (3-30 d) 0.95 (0.69-1.31)/1.41 (1.01-1.96)
ST elevation on initial ECGEarly bleeding (0-2 d)/Late bleeding (3-30 d)
0.81 (0.64-1.02)/0.46 (0.35-0.61)
†Data for n=28,327 patients with complete covariate information, 766 with major bleeding Spencer FA, et al. Circulation. 2007;116:2793-2801.
Predictors of In-hospital Bleeding Within 30 Days: GRACE Registry, Treatment
Characteristics Variable Total Cohort,† HR (95% CI)
Pulmonary artery catheterEarly bleeding (0-1 d)/ Late bleeding (2-30 d)
1.65 (1.18-2.29)/2.04 (1.53-2.72)
PCI 1.94 (1.51-2.50)
Treatment with IV vasopressors in first 24 h 1.94 (1.57-2.39)
Fibrinolytic therapy 1.50 (1.16-1.92)
Treatment with GP IIb/IIIa inhibitor in first 24 h 1.48 (1.23-1.77)
Intra-aortic balloon pulsation device 1.46 (1.12-1.91)
Cardiac catheterization 1.42 (1.10-1.83)
Treated with LMWH in first 24 hEarly bleeding (0-1 d)/Late bleeding (2-30 d) 0.43 (0.33-0.55)/0.95 (0.76-1.19)
Treated with UFH in first 24 h 0.74 (0.62-0.89)
Treated with ASA in first 24 h 0.56 (0.47-0.68)
†Data for n=28,327 patients with complete covariate information, 766 with major bleeding Spencer FA, et al. Circulation. 2007;116:2793-2801.
In-hospital Mortality Among Patients Experiencing Major Bleeding Whose Antithrombotic Medication
was Continued vs Discontinued
0
10
20
30
40
50
60
70
Perc
ent
Therapy discontinued after day 1†
Therapy continued after day 1‡
Aspirin* THN* LMWH UFH** GP IIb/IIIan/N †
‡43/8344/353
26/4529/218
17/5714/72
47/17922/140
31/1494/29
506 patients suffered major bleeding on or the day after admission for AMI and had received at least 1 antithrombotic medication.
THN=thienopyridine; LMWH=low molecular weight heparin; UFH=unfractionated heparin.*P<0.001; **P<0.05.
Spencer FA, et al. Circulation. 2007;116:2793-2801.
Conclusions from GRACE Investigators
“…bleeding remained associated with in-hospital mortality after controlling for important confounders.”
“…although patients in our study who suffered major bleeding experienced higher postdischarge mortality (7.9% vs 5.2%), bleeding was no longer a predictor of late mortality after controlling for differences in clinical and treatment characteristics.”
“…our data suggest that in the community setting, bleeding, although still associated with worse outcomes, also is a marker for patients with more severe illness or comorbidities.”
Spencer FA, et al. Circulation. 2007;116:2793-2801.
ACS Patient Trends: The University of Michigan
Motivala AA, et al. Am J Cardiol. 2007;100:1359-1363.
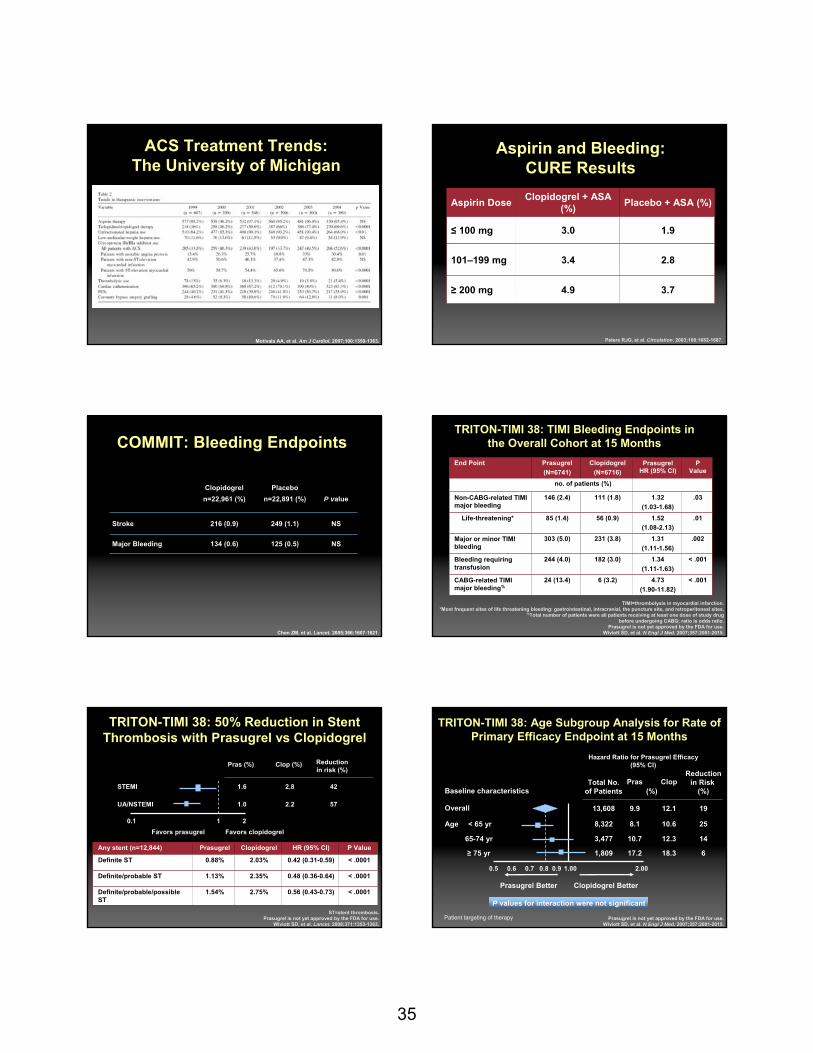
35
ACS Treatment Trends: The University of Michigan
Motivala AA, et al. Am J Cardiol. 2007;100:1359-1363. Peters RJG, et al. Circulation. 2003;108:1682-1687.
Aspirin Dose Clopidogrel + ASA (%) Placebo + ASA (%)
≤ 100 mg 3.0 1.9
101–199 mg 3.4 2.8
≥ 200 mg 4.9 3.7
Aspirin and Bleeding: CURE Results
COMMIT: Bleeding Endpoints
Chen ZM, et al. Lancet. 2005;366:1607-1621.
Clopidogreln=22,961 (%)
Placebon=22,891 (%) P value
Stroke 216 (0.9) 249 (1.1) NS
Major Bleeding 134 (0.6) 125 (0.5) NS
TRITON-TIMI 38: TIMI Bleeding Endpoints in the Overall Cohort at 15 Months
TIMI=thrombolysis in myocardial infarction.*Most frequent sites of life threatening bleeding: gastrointestinal, intracranial, the puncture site, and retroperitoneal sites.
%Total number of patients were all patients receiving at least one dose of study drugbefore undergoing CABG; ratio is odds ratio.
Prasugrel is not yet approved by the FDA for use.Wiviott SD, et al. N Engl J Med. 2007;357:2001-2015.
End Point Prasugrel(N=6741)
Clopidogrel(N=6716)
PrasugrelHR (95% CI)
P Value
no. of patients (%)
Non-CABG-related TIMI major bleeding
146 (2.4) 111 (1.8) 1.32(1.03-1.68)
.03
Life-threatening* 85 (1.4) 56 (0.9) 1.52(1.08-2.13)
.01
Major or minor TIMI bleeding
303 (5.0) 231 (3.8) 1.31 (1.11-1.56)
.002
Bleeding requiring transfusion
244 (4.0) 182 (3.0) 1.34(1.11-1.63)
< .001
CABG-related TIMI major bleeding%
24 (13.4) 6 (3.2) 4.73(1.90-11.82)
< .001
TRITON-TIMI 38: 50% Reduction in Stent Thrombosis with Prasugrel vs Clopidogrel
UA/NSTEMI
STEMI
0.1 1 2
Pras (%) Clop (%) Reductionin risk (%)
1.6 2.8 42
1.0 2.2 57
Favors prasugrel Favors clopidogrel
Any stent (n=12,844) Prasugrel Clopidogrel HR (95% CI) P Value
Definite ST 0.88% 2.03% 0.42 (0.31-0.59) < .0001
Definite/probable ST 1.13% 2.35% 0.48 (0.36-0.64) < .0001
Definite/probable/possible ST
1.54% 2.75% 0.56 (0.43-0.73) < .0001
ST=stent thrombosis.Prasugrel is not yet approved by the FDA for use.
Wiviott SD, et al. Lancet. 2008;371:1353-1363.
TRITON-TIMI 38: Age Subgroup Analysis for Rate of Primary Efficacy Endpoint at 15 Months
Prasugrel is not yet approved by the FDA for use.Wiviott SD, et al. N Engl J Med. 2007;357:2001-2015.
Overall
Baseline characteristics
Age
Hazard Ratio for Prasugrel Efficacy(95% CI)
Total No.of Patients
Pras ClopReduction
in Risk (%)
13,608
(%)
9.9 12.1 19
1,809 17.2 18.3 6
0.5 0.6 0.7 0.8 0.9 1.00 2.00
Prasugrel Better Clopidogrel Better
< 65 yr
65-74 yr
≥ 75 yr
8,322 8.1 10.6 25
3,477 10.7 12.3 14
P values for interaction were not significant
Patient targeting of therapy
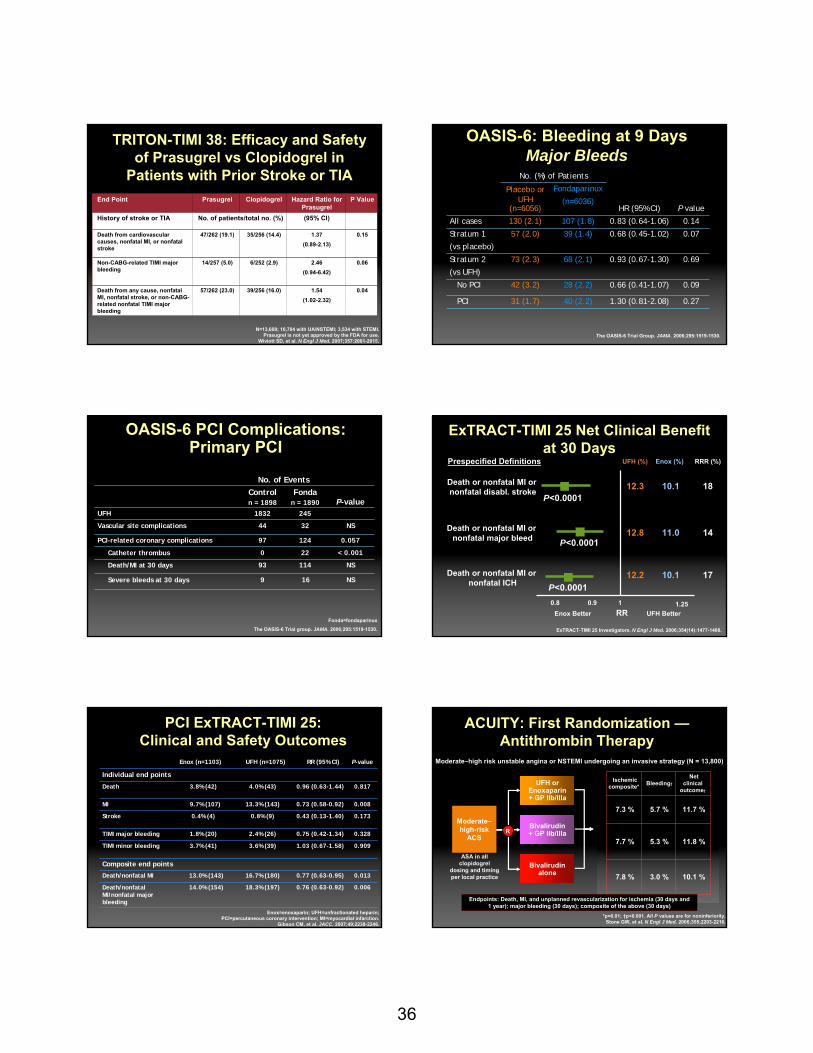
36
TRITON-TIMI 38: Efficacy and Safety of Prasugrel vs Clopidogrel in
Patients with Prior Stroke or TIA
N=13,608; 10,704 with UA/NSTEMI; 3,534 with STEMI.Prasugrel is not yet approved by the FDA for use.
Wiviott SD, et al. N Engl J Med. 2007;357:2001-2015.
End Point Prasugrel Clopidogrel Hazard Ratio for Prasugrel
P Value
History of stroke or TIA No. of patients/total no. (%) (95% CI)
Death from cardiovascular causes, nonfatal MI, or nonfatal stroke
47/262 (19.1) 35/256 (14.4) 1.37(0.89-2.13)
0.15
Non-CABG-related TIMI major bleeding
14/257 (5.0) 6/252 (2.9) 2.46(0.94-6.42)
0.06
Death from any cause, nonfatal MI, nonfatal stroke, or non-CABG-related nonfatal TIMI major bleeding
57/262 (23.0) 39/256 (16.0) 1.54(1.02-2.32)
0.04
No. (%) of Patients
HR (95% CI) P value
Placebo or UFH
(n=6056)
Fondaparinux
(n=6036)
All cases 130 (2.1) 107 (1.8) 0.83 (0.64-1.06) 0.14
Stratum 1
(vs placebo)
57 (2.0) 39 (1.4) 0.68 (0.45-1.02) 0.07
Stratum 2
(vs UFH)
73 (2.3) 68 (2.1) 0.93 (0.67-1.30) 0.69
No PCI 42 (3.2) 28 (2.2) 0.66 (0.41-1.07) 0.09
PCI 31 (1.7) 40 (2.2) 1.30 (0.81-2.08) 0.27
The OASIS-6 Trial Group. JAMA. 2006;295:1519-1530.
OASIS-6: Bleeding at 9 DaysMajor Bleeds
OASIS-6 PCI Complications: Primary PCI
No. of EventsControln = 1898
Fondan = 1890 P-value
UFH 1832 245
Vascular site complications 44 32 NS
PCI-related coronary complications 97 124 0.057
Catheter thrombus 0 22 < 0.001
Death/MI at 30 days 93 114 NS
Severe bleeds at 30 days 9 16 NS
Fonda=fondaparinux
The OASIS-6 Trial group. JAMA. 2006;295:1519-1530.
ExTRACT-TIMI 25 Net Clinical Benefit at 30 Days
1 1.250.90.8
Death or nonfatal MI or nonfatal ICH
Death or nonfatal MI or nonfatal major bleed
Death or nonfatal MI ornonfatal disabl. stroke
Enox Better UFH BetterRR
UFH (%) Enox (%) RRR (%)
12.3 10.1 18
12.8 11.0 14
10.1
Prespecified Definitions
P<0.0001
P<0.0001
P<0.000112.2 17
ExTRACT-TIMI 25 Investigators. N Engl J Med. 2006;354(14):1477-1488.
Enox (n=1103) UFH (n=1075) RR (95% CI) P-value
Individual end points
Death 3.8% (42) 4.0% (43) 0.96 (0.63-1.44) 0.817
MI 9.7% (107) 13.3% (143) 0.73 (0.58-0.92) 0.008
Stroke 0.4% (4) 0.8% (9) 0.43 (0.13-1.40) 0.173
TIMI major bleeding 1.8% (20) 2.4% (26) 0.75 (0.42-1.34) 0.328
TIMI minor bleeding 3.7% (41) 3.6% (39) 1.03 (0.67-1.58) 0.909
Composite end points
Death/nonfatal MI 13.0% (143) 16.7% (180) 0.77 (0.63-0.95) 0.013
Death/nonfatal MI/nonfatal major bleeding
14.0% (154) 18.3% (197) 0.76 (0.63-0.92) 0.006
Enox=enoxaparin; UFH=unfractionated heparin; PCI=percutaneous coronary intervention; MI=myocardial infarction.
Gibson CM, et al. JACC. 2007;49;2238-2246.
PCI ExTRACT-TIMI 25: Clinical and Safety Outcomes
ACUITY: First Randomization —Antithrombin Therapy
Medicalmanagement
PCI
CABG
Ischemic composite* Bleeding†
Net clinical
outcome†
7.3 % 5.7 % 11.7 %
7.7 % 5.3 % 11.8 %
7.8 % 3.0 % 10.1 %
Endpoints: Death, MI, and unplanned revascularization for ischemia (30 days and 1 year); major bleeding (30 days); composite of the above (30 days)
*p=0.01; †p<0.001. All P values are for noninferiority.Stone GW, et al. N Engl J Med. 2006;355;2203-2216.
UFH orEnoxaparin+ GP IIb/IIIa
Moderate–high-risk
ACS
ASA in allclopidogrel
dosing and timingper local practice
Bivalirudin+ GP IIb/IIIa
Bivalirudinalone
R
Moderate–high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,800)

37
Age and ACS Outcomes: CRUSADE Registry Data
Alexander KP, et al. JAMA. 2005;294:3108-3116.
Anticoagulant Dosing and Age in ACS: CRUSADE Registry Data
P<.001 for all 3 treatment groups.Alexander KP, et al. JAMA. 2005;294:3108-3116.
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
UFH LMWH GP IIb/IIIa Inhibitors
< 65 65-74 > 75Patient Age, y
n = 4300
n = 2054
n = 2586
n = 4293 n = 2278
n = 3410
n = 5610
n = 2450
n = 2319
Exce
ss D
ose
Am
ong
All
Patie
nts
Rec
eivi
ng T
reat
men
t, %
Patient-level and Practice-level Predictors of Excess Antithrombotic Dosing
Alexander KP, et al. JAMA. 2005;294:3108-3116.
Patient Characteristics
UFH LMWH GP IIb/IIIa Inhibitor
Age, y65-74
> 75
0.93 (0.79-1.11)
0.81 (0.68-0.96)
0.76(0.65-0.89)
0.75 (0.63-0.89)
4.23 (3.67-4.86)
14.39 (12.24-6.90)
Renal insufficiency 1.25 (1.07-1.46) 0.82 (0.67-1.00) 4.2 (2.95-5.75)
Women 0.92 (0.80-1.46) 0.73 (0.63-0.84) 3.74 (3.29-4.25)
Diabetes mellitus 1.04 (0.93-1.16) 1.16 (1.03-1.31) 1.35 (1.20-1.51)
Prior congestive heart failure
0.86 (0.73-1.02) 1.14 (0.97-1.33) 1.49 (1.23-1.81)
Weight, per 5-kg decrease 1.28 (1.22-1.35) 1.26 (1.23-1.29) 1.02 (1.00-1.04)
Academic hospital 1.02 (0.55-1.58) 1.26 (1.03-1.54) 0.93 (0.76-1.15)
Cardiologist 0.90 (0.77-1.06) 1.17 (1.02-1.34) 0.94 (0.82-1.06)
Medication adherence,per 5% decrease
1.12 (0.97-1.30) 1.02 (0.97-1.08) 1.06 (1.01-1.12)
Likelihood of Receiving Excess Dose, Adjusted OR (95% CI)
Antithrombotic Dosing and Major Bleeding: CRUSADE Registry
P<.001 for UFH and GP IIb/IIa; P=.25 for LMWH.Alexander KP, et al. JAMA. 2005;294:3108-3116.
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
UFH LMWH GP IIb/IIIa Inhibitors
Underdosed Recommended Mild ExcessDose Group
Major Excess
Maj
or B
leed
ing,
%
n = 2074 n = 2063n = 2073
n = 714
n = 2327n = 3998
n =922
n = 237
n = 5879
n = 1955
n = 178
UFH Infusion and Bolus Dosing in ACS and Major Bleeding: CRUSADE Registry Data
Melloni C, et al. Am H J. 2008;156:209-215.
Factors Associated with Excessive UFH Dosing: CRUSADE Registry Data
Melloni C, et al. Am H J. 2008;156:209-215.
Variable OR 95% CI Χ 2 P value
Diabetes 0.77 0.73-0.81 03.1 <.0001
Female 1.45 1.33-1.59 69.4 <.0001
Age (per 10-y increase) 1.11 1.08-1.15 40.8 <.0001
Hypertension 0.86 0.81-0.91 31.3 <.0001
Baseline HCT (per 5% decrease) 0.95 0.93-0.97 24.7 <.0001
Prior stroke 1.15 1.07-1.24 14.6 .0001
Prior PAD 1.13 1.04-1.22 8.4 .0038
Prior MI 1.08 1.02-1.13 7.7 .0054
SBP (per 10-mm Hg increase) 0.99 0.98-1.00 6.1 .0138
White (vs. others) 0.93 0.87-0.99 4.9 .0267
Prior CHF 0.92 0.86-0.99 4.8 .0283
GFR (per 10 mL/min decrease) 1.01 1.00-1.02 4.1 .0434

38
Evidence-based Care for the Very Old ACS Patient
Skolnick AH, et al. JACC. 2007;49:1790-1797.
In-hospital Outcomes for the Very Old ACS Patient
Skolnick AH, et al. JACC. 2007;49:1790-1797.
Number of Therapies and the Very Old
Skolnick AH, et al. JACC. 2007;49:1790-1797.
Excessive Dosing by Gender, Cr, and Patient Age
Parameters are independent & cumulative
Alexander KP, et al. Circulation. 2006;114:1380-1387.
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Overall Men Women >2.0 mg/dL<=2.0 mg/dL< 75 yrs >= 75 yrs
Sex Serum Creatinine Patient Age
Among CrCL < 50 mL/min
% E
xces
s D
ose
26.9%
17.2%
46.4%
62.9%
90.8%
16.0%
64.2%
Major Bleeding by Gender and GP IIb/IIIa Inhibitor Use
Alexander KP, et al. Circulation. 2006;114:1380-1387.
0.0
5.0
10.0
15.0
20.0
25.0
Men Women
% M
ajor
Ble
edin
g
P=0.08
P<0.0001P<0.0001
P<0.0001 No GP IIb/IIa
GP IIb/IIIa (Appropriate)
GP IIb/IIIa (Excess)
Transfusion Trends in ACS Patients: CRUSADE Registry Data
Alexander KP, et al. Am H J. 2008;155:1047-1053.
Hospital-level transfusion quartiles (low to high % transfusion)
Quartile 1st 2nd 3rd 4th
Any transfusion (%) 0 7.3 11.4 19.1
Baseline HCT 40.5 (39.4, 42.0) 40.9 (39.9, 41.6) 40.2 (39.4, 41.0) 38.7 (37.6, 40.3)
Nadir HCT 36.5 (34.9, 37.7) 35.9 (35.0, 36.6) 34.7 (34.0, 35.8) 33.6 (31.3, 34.7)
Nadir HCT† 25.6 (24.4, 27.2) 25.7 (24.4, 26.6) 25.6 (24.9, 26.7) 25.5 (24.4, 26.4)
Age (y) 66.5 (60.5, 71.8) 66.8 (64.0, 70.5) 70.0 (65.0, 75.0) 74.0 (69.0, 79.0)
Female (%) 39.0 38.1 42.9 45.4
CrCl (mL/min) 55.9 (47.3, 63.0) 54.7 (51.3, 59.0) 50.2 (42.8, 55.6) 42.1 (32.9, 50.1)
Diabetes (%) 30.2 31.1 34.6 35.5
Signs of CHF (%) 17.6 20.6 26.8 33.3
Cardiac catherization (%) 94.3 94.6 91.9 82.8
Acute heparin (%)* 89.6 89.4 89.4 91.8
Acute GP IIb/IIIa (%)* 45.5 50.0 46.2 40.0
Major Bleeding (%) 3.9 8.7 12.5 18.8
P values <.001 except for (*). Values represent median (25th, 75th) or % as indicated.

39
Mortality and Blood Transfusions by Nadir
Hematocrit
Alexander KP, et al. Am H J. 2008;155:1047-1053. 230
Questions for DiscussionWhat practical steps can clinicians take
to reduce bleeding associated with acute ACS care?
-Therapeutic choices
- Dose considerations
- Special populations
The Future of ACS Treatment:
New Therapies in Development
E. Magnus Ohman, MDDirector, Program for
Advanced Coronary Disease Duke University Medical Center
Durham, NC
•Identify emerging pharmacotherapies for
the ACS patient
•Compare and contrast the roles of existing and
evolving therapies in different ACS patient
populations
Learning Objectives
In your view, what is the most important limitation of current antiplatelet therapies?
1. Variable treatment response2. Slow onset3. Limited efficacy4. Too long-acting/irreversible5. Cost6. Other7. Unsure
Platelet Activation
Multiple potential agonistsMajor agonists include collagen, ADP, thromboxane A2 (TxA2) and thrombinTissue factor (TF) released from damaged endothelial wall leads to generation of thrombinGenerated thrombin binds to the platelet PAR1 receptor and contributes heightened platelet response
Wu KK. J Intern Med. 1996;236:17-34. Ruggeri ZM, et al. J Thromb Haemost. 2003;1:1335-1342. Jackson SP, et al. J Thromb Haemost. 2003;1:1602-1612.
Brass LF. Chest. 2003;124(3 suppl):18S-25S. Dorsam RT, et al. J Thromb Haemost. 2004;2:804-812.
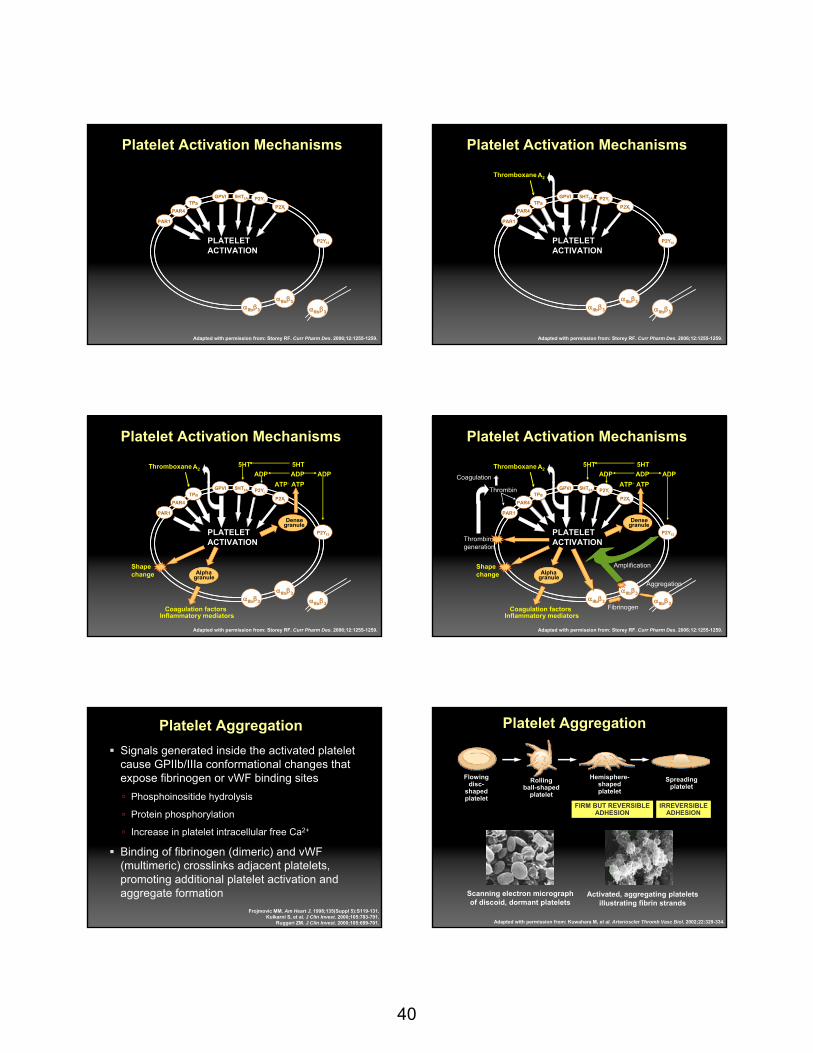
40
Platelet Activation Mechanisms
Adapted with permission from: Storey RF. Curr Pharm Des. 2006;12:1255-1259.
PLATELETACTIVATION
P2Y12
P2Y5HT2A
PAR1
PAR4
αIIbβ3
αIIbβ3
αIIbβ3
TPGPVI
P2X1a
1
Platelet Activation Mechanisms
Adapted with permission from: Storey RF. Curr Pharm Des. 2006;12:1255-1259.
PLATELETACTIVATION
P2Y12
P2Y5HT2A
PAR1
PAR4
αIIbβ3
αIIbβ3
αIIbβ3
TPGPVI
P2X1a
1
Thromboxane A2
Platelet Activation Mechanisms
Adapted with permission from: Storey RF. Curr Pharm Des. 2006;12:1255-1259.
PLATELETACTIVATION
P2Y12
P2Y5HT2A
PAR1
PAR4
αIIbβ3
αIIbβ3
αIIbβ3
TPGPVI
P2X1a
1
ThromboxaneA2
Coagulation factorsInflammatory mediators
Shapechange
Densegranule
Alphagranule
5HTADP ADPADP
5HT
ATPATP
Platelet Activation Mechanisms
Adapted with permission from: Storey RF. Curr Pharm Des. 2006;12:1255-1259.
PLATELETACTIVATION
P2Y12
P2Y5HT2A
PAR1
PAR4
αIIbβ3
αIIbβ3
αIIbβ3
TPGPVI
P2X1a
1
Thromboxane A2
Coagulation factorsInflammatory mediators
Shapechange
Densegranule
Alphagranule
5HTADP ADPADP
5HT
ATPATPThrombin
Thrombingeneration
Coagulation
Fibrinogen
Aggregation
Amplification
Platelet AggregationSignals generated inside the activated platelet cause GPIIb/IIIa conformational changes that expose fibrinogen or vWF binding sites
Phosphoinositide hydrolysis
Protein phosphorylation
Increase in platelet intracellular free Ca2+
Binding of fibrinogen (dimeric) and vWF(multimeric) crosslinks adjacent platelets, promoting additional platelet activation and aggregate formation
Frojmovic MM. Am Heart J. 1998;135(Suppl 5):S119-131.Kulkarni S, et al. J Clin Invest. 2000;105:783-791.
Ruggeri ZM. J Clin Invest. 2000;105:699-701. Adapted with permission from: Kuwahara M, et al. Arterioscler Thromb Vasc Biol. 2002;22:329-334.
Platelet Aggregation
Scanning electron micrograph of discoid, dormant platelets
Activated, aggregating platelets illustrating fibrin strands
FIRM BUT REVERSIBLEADHESION
IRREVERSIBLEADHESION
Flowingdisc-
shapedplatelet
Rollingball-shaped
platelet
Hemisphere-shapedplatelet
Spreadingplatelet
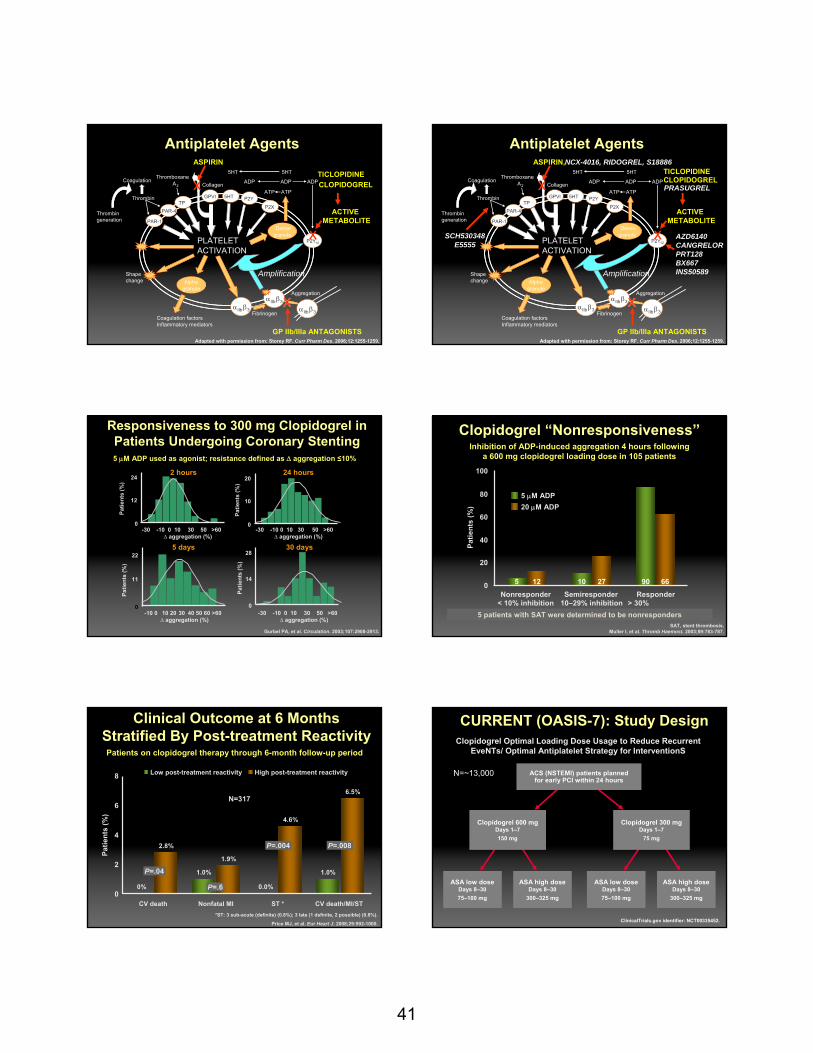
41
Antiplatelet Agents
Thrombin
ThromboxaneA2
5HT
P2Y12
ADP ADPADP
5HT
PLATELETACTIVATION
P2Y15HT2A
PAR-1
PAR-4
Densegranule
Thrombingeneration
Shapechange
αIIb β3
αIIb β3
FibrinogenαIIb β3
Aggregation
AmplificationAlpha
granule
Coagulation factorsInflammatory mediators
TPa
Coagulation
GPVI
CollagenATPATP
P2X1
ASPIRIN
xACTIVE
METABOLITE
x
GP IIb/IIIa ANTAGONISTS
xx
Adapted with permission from: Storey RF. Curr Pharm Des. 2006;12:1255-1259.
TICLOPIDINECLOPIDOGREL
Antiplatelet Agents
Thrombin
ThromboxaneA2
5HT
P2Y12
ADP ADPADP
5HT
PLATELETACTIVATION
P2Y15HT2A
PAR-1
PAR-4
Densegranule
Thrombingeneration
Shapechange
αIIb β3
αIIb β3
FibrinogenαIIb β3
Aggregation
AmplificationAlpha
granule
Coagulation factorsInflammatory mediators
TPa
Coagulation
GPVI
CollagenATPATP
P2X1
ASPIRIN,
xACTIVE
METABOLITE
x
GP IIb/IIIa ANTAGONISTS
xx
Adapted with permission from: Storey RF. Curr Pharm Des. 2006;12:1255-1259.
TICLOPIDINECLOPIDOGRELPRASUGREL
AZD6140 CANGRELORPRT128BX667INS50589
NCX-4016, RIDOGREL, S18886
SCH530348E5555
Gurbel PA, et al. Circulation. 2003;107:2908-2913.
Responsiveness to 300 mg Clopidogrel in Patients Undergoing Coronary Stenting
2 hours 24 hours
5 days 30 days
5 μM ADP used as agonist; resistance defined as Δ aggregation ≤10%
24
12
0
20
10
0
22
11
0
28
14
0
Patie
nts
(%)
Patie
nts
(%)
Patie
nts
(%)
Patie
nts
(%)
-30 -10 0 10 30 50 >60∆ aggregation (%)
-10 0 10 20 30 40 50 60 >60∆ aggregation (%)
-30 -10 0 10 30 50 >60∆ aggregation (%)
-30 -10 0 10 30 50 >60∆ aggregation (%)
Clopidogrel “Nonresponsiveness”
SAT, stent thrombosis. Muller I, et al. Thromb Haemost. 2003;89:783-787.
Inhibition of ADP-induced aggregation 4 hours following a 600 mg clopidogrel loading dose in 105 patients
Nonresponder ResponderSemiresponder0
40
60
80
100
20
5 μM ADP20 μM ADP
Patie
nts
(%)
5 12 10 27 6690
< 10% inhibition > 30% inhibition
10–29% inhibition5 patients with SAT were determined to be nonresponders
Clinical Outcome at 6 MonthsStratified By Post-treatment Reactivity
N=317
Patie
nts
(%)
*ST: 3 sub-acute (definite) (0.8%); 3 late (1 definite, 2 possible) (0.8%).
Price MJ, et al. Eur Heart J. 2008;29:992-1000.
Patients on clopidogrel therapy through 6-month follow-up period
0
2
4
6
8
1.0%
0.0%
1.0%
2.8%
1.9%
4.6%
6.5%
0%
CV death Nonfatal MI ST * CV death/MI/ST
Low post-treatment reactivity High post-treatment reactivity
P=.04
P=.6
P=.008P=.004
CURRENT (OASIS-7): Study Design
ACS (NSTEMI) patients planned for early PCI within 24 hours
Clopidogrel 600 mgDays 1–7 150 mg
ASA low doseDays 8–3075–100 mg
ASA high doseDays 8–30
300–325 mg
Clopidogrel 300 mgDays 1–7
75 mg
ASA low doseDays 8–3075–100 mg
ASA high doseDays 8–30
300–325 mg
N=~13,000
ClinicalTrials.gov identifier: NCT00335452.
Clopidogrel Optimal Loading Dose Usage to Reduce Recurrent EveNTs/ Optimal Antiplatelet Strategy for InterventionS

42
Prasugrel
Mechanism: inhibition of P2Y12
PharmacodynamicsRapid onset (within 2 hours)Irreversible binding
Different metabolic pathway of activation versus clopidogrel
More potent inhibition of ADP-induced platelet activation than clopidogrel
Prasugrel is an ivestigational agent; not yet approved by FDA.Farid NA. Clin Pharmacol Ther. 2007;81:735-741.
Active Metabolite Formation
Prasugrel
Herbert JM, et al. Sem Vasc Med. 2003;3:113-122.
Pro-drug
Oxidation(Cytochrome P450)
HOOC* HS
N
O
F
NS
O
FO
Hydrolysis(esterases)
NS
O
CH3
CO
FO
85% inactive
metabolitesesterases
NS
O
Cl
O CH3C
ON
S
O
Cl
O CH3C HOOC* HS
N
O
Cl
OCH3
NS
O
Cl
O CH3CClopidogrel
Active metabolite Active metabolite
Inhi
bitio
n of
pla
tele
t agg
rega
tion
(IPA
)(2
0 μM
AD
P) (%
)
Prasugrel 60 mgClopidogrel 300 mg
Clopidogrel responder*Clopidogrel nonresponder
n=66
Healthy volunteers
Prasugrel vs ClopidogrelCrossover Study
*Responder ≥ 25% IPA at 4 and 24 hours.Adapted with permission from: Brandt Jt, et al. Am Heart J. 2007;153:66e9-66e16.
-20
0
20
40
60
80
100
Prasugrel Compared with Clopidogrel: ADP-induced Platelet Aggregation
MP
A (%
)
0102030405060708090
100
Mean ± SD, excluding outliers†
20 µM ADP and 24 hr post-LD
†
†
Clopidogrel
59.6±20.1
(112)
BL 1
85.1±7.5
(111)
BL 2
84.1±7.8
(111)
Prasugrel
20.0±6.7
(91)(N)
MPA =
"Placebo"
Rel
ativ
e Fr
eque
ncy
0.0
0.1
0.2
0.3
0.4
Rel
ativ
e Fr
eque
ncy
0.0
0.1
0.2
0.3
0.4
IPA(%)-20 0 20 40 60 80 100
Rel
ativ
e Fr
eque
ncy
0.0
0.1
0.2
0.3
0.4
Clopidogrel
Prasugrel
Adapted with permission from: Weerakkody GJ, et al. Platelets. 2007;18:428-435.Stone GW. Abstract presented at the 2007 American College of Cardiology Scientific Sessions, New Orleans, LA.
BL=blood level; MPA= ean platelet aggregation
Prasugrel (40 mg LD/5 mg MD)Prasugrel (40 mg LD/7.5 mg MD)Prasugrel (60 mg LD/10 mg MD)Prasugrel (60 mg LD/15 mg MD)Clopidogrel (300 mg LD/75 mg MD)
Mea
n IP
A (%
)
-10
0
10
20
30
40
50
60
70
Day/hour post-dosing1/0 1/2 1/4 1/6 7/1 7/2 28/0 28/2 28/4 28/6
Loading dose (LD) Maintenance dose (MD)
Adapted with permission from: Jernberg T, et al. Eur Heart J. 2006;27:1166-1173.
Inhibition of Platelet Aggregation Induced by 20 μM ADP
Greater Platelet Inhibition in Prasugrel vsClopidogrel at Higher Loading Doses
LSM=least square mean; VASP PRI=vasodilator-stimulated phosphoprotein platelet reactivity index. Adapted with permission from: Wiviott SD, et al. Circulation. 2007:116;2923-2932.
20
40
60
80
100
0
20
40
60
80
100
00 4 8 12 16 20 24
Hours0 4 8 12 16 20 24
Hours
Clopidogrel 600 mg
Prasugrel 60 mg
4.920.3
31.8 32.630.8***
64.5***74.8*** 69.3***
*** P<.0001
IPA
(20μ
M A
DP,
%)
VASP
PR
I (%
)
21.5***7.4*** 10.3***
68.47564.3
*** P<.0001
0.5 hr 2 hr 6 hr 18–24 hr
n=70 n=74 n=72 Prasugrel n=39
n=73 n=78 n=77 Clopidogrel n=46
26.0 44.8 43.2 LSM 36.4(18.9– (38.4– (38.0– difference (29.0–33.2) 51.2) 48.4) (95% CI) 43.8)
0 2 hr 6 hr 18–24 hr
n=89 n=93 n=68 Prasugrel n=48
n=89 n=88 n=68 Clopidogrel n=54
54.3 60.5 LSM 56.2(47.4– (54.0– difference (49.2–61.2) 67.1) (95% CI) 63.2)
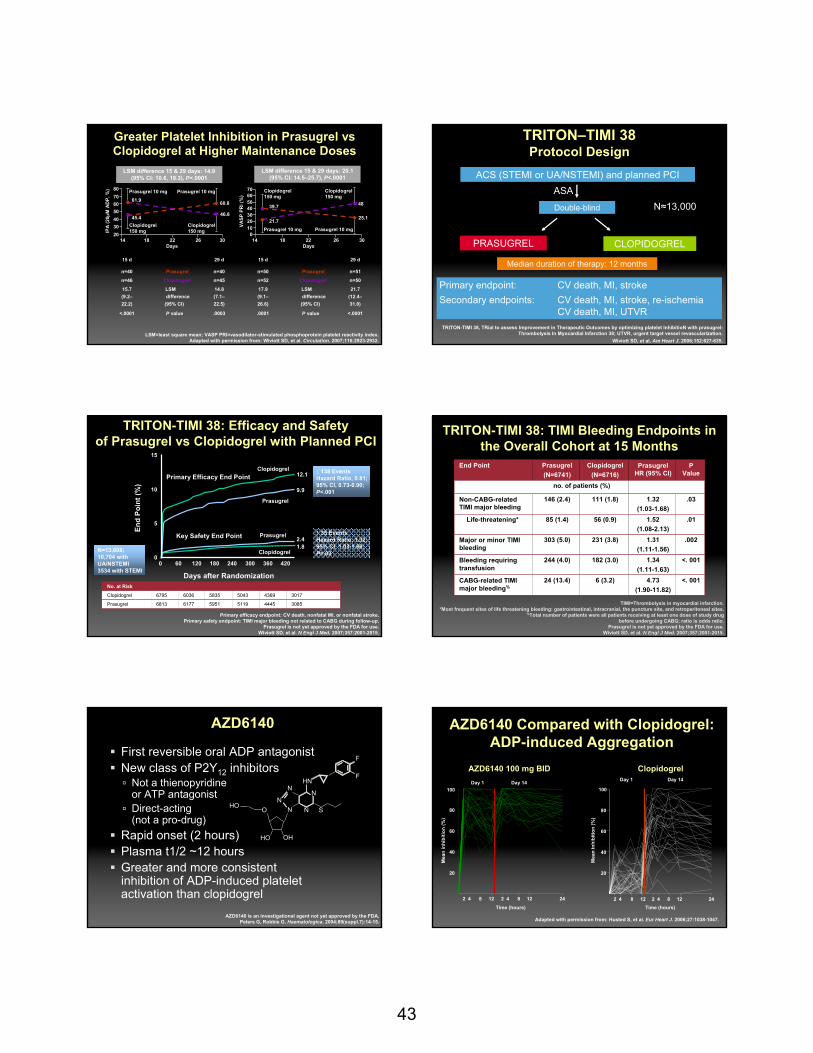
43
Greater Platelet Inhibition in Prasugrel vsClopidogrel at Higher Maintenance Doses
IPA
(20μ
M A
DP,
%)
VASP
PR
I (%
)20304050607080
203040506070
010Clopidogrel
150 mg
Prasugrel 10 mg Prasugrel 10 mg
Clopidogrel150 mg
Clopidogrel150 mg
Prasugrel 10 mg Prasugrel 10 mg
Clopidogrel150 mg
25.1
48
21.7
39.746.8
60.8
45.4
61.9
14 18 22 26 30Days
14 18 22 26 30Days
LSM difference 15 & 29 days: 14.9 (95% CI: 10.6, 19.3), P<.0001
LSM difference 15 & 29 days: 20.1 (95% CI: 14.5–25.7), P<.0001
15 d 29 d
n=40 Prasugrel n=40
n=46 Clopidogrel n=45
15.7 LSM 14.8(9.2– difference (7.1–22.2) (95% CI) 22.5)
<.0001 P value .0003
15 d 29 d
n=50 Prasugrel n=51
n=52 Clopidogrel n=50
17.9 LSM 21.7(9.1– difference (12.4–26.6) (95% CI) 31.0)
.0001 P value <.0001
LSM=least square mean; VASP PRI=vasodilator-stimulated phosphoprotein platelet reactivity index. Adapted with permission from: Wiviott SD, et al. Circulation. 2007;116:2923-2932.
TITAN
Double-blind
ACS (STEMI or UA/NSTEMI) and planned PCIASA
PRASUGREL CLOPIDOGREL
Primary endpoint: CV death, MI, strokeSecondary endpoints: CV death, MI, stroke, re-ischemia
CV death, MI, UTVR
Median duration of therapy: 12 months
N≈13,000
TRITON–TIMI 38Protocol Design
TRITON-TIMI 38, TRial to assess Improvement in Therapeutic Outcomes by optimizing platelet InhibitioN with prasugrel-Thrombolysis In Myocardial Infarction 38; UTVR, urgent target vessel revascularization.
Wiviott SD, et al. Am Heart J. 2006;152:627-635.
TRITON-TIMI 38: Efficacy and Safetyof Prasugrel vs Clopidogrel with Planned PCI
10
240180120600
5
0420360300
15
End
Poin
t (%
)
Days after Randomization
Primary Efficacy End Point
Key Safety End Point
Clopidogrel
Clopidogrel
Prasugrel
Prasugrel
1.82.4
9.9
12.1 ↓ 138 EventsHazard Ratio, 0.81;95% CI, 0.73-0.90;P<.001
↑ 35 EventsHazard Ratio, 1.32;95% CI, 1.03-1.68;P=.03
No. at Risk
Clopidogrel 6795 6036 5835 5043 4369 3017
Prasugrel 6813 6177 5951 5119 4445 3085
N=13,608; 10,704 with UA/NSTEMI3534 with STEMI
Primary efficacy endpoint: CV death, nonfatal MI, or nonfatal stroke.Primary safety endpoint: TIMI major bleeding not related to CABG during follow-up.
Prasugrel is not yet approved by the FDA for use.Wiviott SD, et al. N Engl J Med. 2007;357:2001-2015.
TRITON-TIMI 38: TIMI Bleeding Endpoints in the Overall Cohort at 15 Months
TIMI=Thrombolysis in myocardial infarction.*Most frequent sites of life threatening bleeding: gastrointestinal, intracranial, the puncture site, and retroperitoneal sites.
%Total number of patients were all patients receiving at least one dose of study drugbefore undergoing CABG; ratio is odds ratio.
Prasugrel is not yet approved by the FDA for use.Wiviott SD, et al. N Engl J Med. 2007;357:2001-2015.
End Point Prasugrel(N=6741)
Clopidogrel(N=6716)
PrasugrelHR (95% CI)
P Value
no. of patients (%)
Non-CABG-related TIMI major bleeding
146 (2.4) 111 (1.8) 1.32(1.03-1.68)
.03
Life-threatening* 85 (1.4) 56 (0.9) 1.52(1.08-2.13)
.01
Major or minor TIMI bleeding
303 (5.0) 231 (3.8) 1.31 (1.11-1.56)
.002
Bleeding requiring transfusion
244 (4.0) 182 (3.0) 1.34(1.11-1.63)
<. 001
CABG-related TIMI major bleeding%
24 (13.4) 6 (3.2) 4.73(1.90-11.82)
<. 001
AZD6140
First reversible oral ADP antagonistNew class of P2Y12 inhibitors
Not a thienopyridineor ATP antagonistDirect-acting (not a pro-drug)
Rapid onset (2 hours)Plasma t1/2 ~12 hoursGreater and more consistent inhibition of ADP-induced platelet activation than clopidogrel
AZD6140 is an investigational agent not yet approved by the FDA.Peters G, Robbie G. Haematologica. 2004;89(suppl.7):14-15.
F
F
HN
N
N S
N
NNO
HO OH
HO
AZD6140 Compared with Clopidogrel: ADP-induced Aggregation
Clopidogrel
Time (hours)
20
40
60
80
100
Day 1 Day 14
AZD6140 100 mg BID
Time (hours)
20
40
60
80
100
2 4 8 12 2 4 8 12 24
Day 1 Day 14
2 4 8 12 2 4 8 12 24
Mea
n in
hibi
tion
(%)
Mea
n in
hibi
tion
(%)
Adapted with permission from: Husted S, et al. Eur Heart J. 2006;27:1038-1047.

44
RandomizationV1
Day 1
V2 V3 V4 Follow-up
Week 4 Week 8 Week 12 Final visit+7 days
AZD6140 90 mg bid (n=334)
AZD6140 180 mg bid (n=323)
Clopidogrel 75 mg qd (n=327)
Onset of chestpain and 48 h maximum torandomization
N=990
DISPERSE2 Main Study Design
All patients received aspirin (≤ 325 mg first dose, then 75–100 mg qd) and heparin/LMWH and/or a GPIIb/IIIa antagonist
50% of AZD6140 patients in each arm received a 270 mg loading doseIn the clopidogrel group, thienopyridine-naïve patients received a 300-mg loading dose
DISPERSE2=Dose confirmatIon Study assessing anti-Platelet Effects of AZD6140 vs clopidogRel in NSTEMI.Cannon CP, et al. J Am Coll Cardiol. 2007;50:1844-1851.
DISPERSE2Adjudicated bleeding rates within 48 hours
4
3
2
0
1
Tota
l ble
edin
g ra
te (%
)
AZD614090 mg bid
N=168
2.4%
AZD6140180 mg bid
N=159
1.3%
AZD6140270 mg**
N=330
3.6%
Clopidogrel75 mg qd
N=327
2.8%
Minor bleeds*Major bleeds
* Minor bleeding without major bleeding; ** loading dose.Adapted with permission from: Cannon CP, et al. J Am Coll Cardiol. 2007;50:1844-1851.
DISPERSE2Cumulative adjudicated clinical endpoint of CV death/MI/stroke
No significant differences were found between the groups for clinical endpoints
AZD6140 90 mg bid AZD6140 180 mg bid Clopidogrel 75 mg QD
Study day4131211 11 91817151 61
0.10
0.05
0.00
Cum
ulat
ive
risk
of a
n ev
ent
Primary endpoint of the DISPERSE-2 trial was the Kaplan-Meier rate of major or minor bleeding through 4 weeks.Adapted with permission from: Cannon CP, et al. J Am Coll Cardiol. 2007;50:1844-1851.
DISPERSE2Non-bleeding adverse events
Preferredterm
AZD614090 mg bid
n=334
AZD6140180 mg bid
n=323
Clopidogrel75 mg qd
n=327Dyspnea 10.5 15.8 6.4
Chest pain 7.5 7.4 8.9
Headache 9.6 6.5 8.6
Nausea 6.6 6.5 3.4
Dyspepsia 4.8 3.1 2.8
Insomnia 5.4 4.6 2.8
Diarrhea 3.0 7.4 3.4
Hypotension 4.2 3.7 0.6
Discontinuation rates due to adverse events were low and similar between the groups: 21 (6%), 23 (7%), and 19 (6%) discontinued in the AZD6140 90 mg bid, AZD6140 180 mg bid, and clopidogrel 75 mg qd groups, respectively.
Cannon CP, et al. J Am Coll Cardiol. 2007;50:1844-1851.
PLATOCan PLATelet Inhibition Be Optimized to Prevent
Vascular Events?~16,000 patients within 24 hours
of an index ACS (STEMI or NSTEMI)
At least 2 inclusion criteria:1. ST segment changes2. ↑ biomarkers3. At least 1:
- > 60 years old- Previous MI/CABG- Known > 1V CAD- AODM- PVD- Renal dysfunction
ASA 75–100 mg QD
AZD6140 BID
Clopidogrel75 mg QD
Primary endpoint: Time to first occurrence of the composite of death, MI or stroke
Primary safety endpoint: Major bleeding
Double-blind, double-dummyMean follow-up ~12.5 months
Range 6–24
ClinicalTrials.gov Identifier: NCT00391872.
Cangrelor
ATP analogue Immediate onset (within 5 minutes)Plasma half-life of 5–9 minutes 20–60 minutes for return to normal platelet function
N N
N N
NH
SCF3
OHOH
OOP
OO
PP
OO
OClCl
OO
O
S
4Na+
Cangrelor is an invesigational agent not yet approved by the FDA.Storey RF, et al. Thromb Haemost. 2001;85:401-407.
Greenbaum AB, et al. Am Heart J. 2006;151:689e1-689e10.
Parenteral ADP-P2Y12 receptor antagonist

45
200
6040
10080
200
6040
10080
200
6040
10080
0.5 1.5 2.5 3.5 5 24 48 72 20 m 1 h
post post
Inhi
bitio
n of
agg
rega
tion
(%)
Time after onset of cangrelorinfusion (hrs) and time post-infusion
Adapted with permission from: Storey RF, et al. Thromb Haemost. 2001;85:401-407.
Rapid, Dose-dependent Inhibition of Platelet Aggregation with Cangrelor
n=12
Infusion rates:0.05 μg/kg/min (0.5 hours)0.2 μg/kg/min (1.5 hours)0.5 μg/kg/min (2.5 hours)2.0 μg/kg/min (3.5–24 hours)
n=13
Infusion rates:0.05 μg/kg/min (0.5 hours)0.2 μg/kg/min (1.5 hours)0.5 μg/kg/min (2.5 hours)2.0 μg/kg/min (3.5–24 hours)
n=14
Infusion rates:0.2 μg/kg/min (0.5 hours)1.0 μg/kg/min (1.5 hours)2.0 μg/kg/min (2.5 hours)4.0 μg/kg/min (3.5–24 hours)
Improved ADP Blockade with Cangrelorin Clopidogrel-treated Patients
VASP=vasodilator-stimulated phosphoprotein.Adapted with permission from: Aleil B. J Thromb Haemost.
2005;3:85-92.
Platelet Reactivity Index (PRI) determined by the difference in VASP fluorescence intensity between resting and ADP-activated platelets.
33 clopidogrel treated patients with a mean PRI of 61% and decreased to close to zero with in vitro cangrelor.
-20
-10
0
20
10
40
30
50
70
60
90
80
Healthy + in vitro + in vitrodonors cangrelor cangrelor
Patients Patientsnot treated treatedwith clop with clop
P<.001
Plat
elet
reac
tivity
inde
x (%
)
Cangrelor Phase II Clinical Data: Compared with Abciximab in PCI
Double-blind randomized trial performed in US
5.7%5.4%
2.1%
1.0%
Death, MI, revascularization Major bleed (TIMI criteria)
Abciximab (n=94)Cangrelor (n=105)
Incidence of events up to 7 days
AR-C69931MX report number: SC931-5129 Part 2. Unpublished data.
CHAMPION–PCIPCI for ACS
(N~9,000)
Primary endpoint: death, MI, and UTVR at 48 hours
Secondary endpoints:Death, MI, uRevasc at 30 daysDeath at 6 months and 1 year
Index procedure and study drug infusion (for at least 2 hours or the duration of the procedure, whichever is longer)
Clopidogrel600 mg
Placebobolus and infusion
Placebocapsules
Cangrelor 30 μg/kg bolus4 μg/kg/min Infusion
Clopidogrel600 mg
Placebocapsules
CHAMPION-PCI Trial=A Clinical Trial Comparing Cangrelor to Clopidogrelin subjects who require percutaneous coronary intervention.
ClinicalTrials.gov Identifier: NCT00305162.
0
20
40
60
80
100
0.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0Time (hours)
Ligh
t tra
nsm
ittan
ce (%
)
Clopidogrel 600mgClopidogrel 600mg at time of cangrelorbolus and 2hr infusion
Clopidogrel 600mg
Clopidogrel 600mg given at the end of a cangrelor infusion
Clopidogrel/Cangrelor Interaction
Adapted with permission from: Steinhubl SR, et al. Thromb Res. 2008;121:527-534.
Antiplatelet Agents
Thrombin
ThromboxaneA2
5HT
P2Y12
ADP ADPADP
5HT
PLATELETACTIVATION
P2Y15HT2A
PAR-1
PAR-4
Densegranule
Thrombingeneration
Shapechange
αIIb β3
αIIb β3
FibrinogenαIIb β3
Aggregation
AmplificationAlpha
granule
Coagulation factorsInflammatory mediators
TPa
Coagulation
GPVI
CollagenATPATP
P2X1
ASPIRIN,
x PRASUGREL
ACTIVE METABOLITE
x AZD6140 CANGRELORPRT128BX667INS50589
GP IIb/IIIa ANTAGONISTS
xx
Adapted with permission from: Storey RF. Curr Pharm Des. 2006;12:1255-1259.
xSCH530348
E5555
TICLOPIDINECLOPIDOGREL
NCX-4016, RIDOGREL, S18886

46
Protease Activated Receptor (PAR)-1
LDPR SFLLRNP LDPRNRLLFS
Thrombin
Signal
CC CC CC CC
Vu TH, et al. Cell. 1991;64:1057-1066.
Thrombin Receptor Antagonist (TRA SCH 530348)
First of a new classOral administration, long-acting Blocks the platelet PAR-1 receptor, primary thrombin receptor in humansDoes not interfere with thrombin-mediated generation of fibrinNo effect on bleeding time or PT/aPTT
TRA SCH 530348 is an investigational agent not yet approved by FDA.Husted S. Eur Heart J Suppl. 2007;9:D20-27.
TRA-PCI: Study DesignNon-urgent PCI or catheter with possible PCI (all receive aspirin)
No PCI**
Maintenance therapy qd for ~60 daysPlacebo loading dose → placebo
SCH 530348 loading dose → SCH 530348
Safety: TIMI major plus minor bleedingEfficacy: death/MACE at 60 days
Primary evaluable cohort **Secondary evaluable cohort
Catheterization
CABG Medical management
0.5 mgn ~100
1 mgn ~100
2.5 mgn ~100
Placebon ~100
SCH 530348
Randomization #1— 3:1 SCH530348:Placebo Sequential groups (loading dose x 1: 10 mg; 20 mg; 40 mg)
Randomization #2
PCI
Safety: TIMI major plus minor bleeding
No additional study drug
N=1030
TRA-PCI=Thrombin Receptor Antagonist in Percutaneous Coronary Intervention trial. Adapted with permission from: Moliterno DJ, et al. J Am Coll Cardiol. 2007;49 [abstract 2402-9].
TIMI major/minor bleeding
2.8%
PCI Cohort
P=.77
P=.35
P=.70
P=.73
3.3%
1.6%
2.5%
4.0%4
0
2
All TRAn=422
1
3
5
Placebon=151
10 mgn=129
20 mgn=120
40 mgn=173
SCH 530348P value relative to placebo.
Adapted with permission from: Moliterno DJ, et al. J Am Coll Cardiol. 2007;49 [abstract 2402-9].
Patie
nts
(%)
60-day death or MI
8
0
4
All TRAn=422
4.5%
TRA-PCI Efficacy Outcomes
2
6
10
Placebon=151
7.3%
10 mgn=129
20 mgn=120
40 mgn=173
5.4%
4.2% 4.0%
SCH 530348
P=.19P=.53
P=.28P=.20
P value relative to placebo.Adapted with permission from: Moliterno DJ, et al. J Am Coll Cardiol. 2007;49 [abstract 2402-9].
Patie
nts
(%)
TRA (SCH 530348) program(29,500 patients)
Primary endpoint: composite of CV death, MI,
stroke, and urgent revascularization
TRA (SCH 530348) ProgramEvaluation of efficacy and safety in acute and chronic atherothrombosis
NSTEACS10,000 patients
Secondary prevention19,500 patients
SCH 530348 Placebo SCH 530348 Placebo
Follow-up: at 30 days; at 4, 8, and 12 months; and at 6 months thereafter (I year minimum)
Primary endpoint: composite of
CV death, MI, stroke, urgent revascularization, and
recurrent ischemia with rehospitalization
ClinicalTrials.gov Identifier: NCT00527943. ClinicalTrials.gov Identifier: NCT00526474.
TRA-CER TRA2°P - TIMI 50

47
PAR-1 Antagonist–E5555
600 patientsages 55–80 with known ASCAD,
on ASA +/-clopidogrel, with hs-CRP > 3mg/L
E5555 Outcomes• MACE• hs-CRP
E5555 is an investigational agent not yet approved by FDA.ClinicalTrials.gov Identifier: NCT00312052.
LANCELOT
Tissue factor
Factor Xa
Prothrombin
Thrombin
Fibrinogen Fibrin Thrombus Fibrin degradationPlasmin
Collagen Leukocytes
Platelets
vWF ADP
Activated platelets
Fibrinogen cross-linking
Platelet aggregation
Thromboxane A2
Coagulation Platelets
Direct thrombin inhibitors
LMWHUH
LMWHUH
TFPI
Antithrombin
Antithrombin
LMWH
ThrombolyticsAdapted with permission from: Selwyn AP. Am J Cardiol. 2003;91(Suppl):3H-11H.
New and Investigational Anticoagulants
TFPI (tifacogin)
FondaparinuxIdraparinux
RivaroxabanApixabanLY517717YM150DU-176bPRT-054021
XimelagatranDabigatran
ORAL PARENTERAL
DX-9065aOtamixaban
Xa
IIa
TF/VIIa
X IX
IXaVIIIa
Va
II
FibrinFibrinogen
AT
APC (drotrecogin alfa)sTM (ART-123)
Adapted from Weitz & Bates. J Thromb Haemost. 2005;3(8):1843-1853.
TTP889
Factor Xa inhibitors
• FXa may be a better target than thrombin• Has few functions outside coagulation (compared with
thrombin)• Has a wider therapeutic window than thrombin
(separation of efficacy and bleeding), in vitro• Thrombin inhibitors are associated with rebound
thrombin generation – no evidence with FXa inhibitors• Efficacy of heparin-based anticoagulants improves as
selectivity for FXa increases: UFH < LMWH < fondaparinux
IIaIIaIIII
FibrinogenFibrinogen Fibrin clotFibrin clot
Extrinsic Extrinsic pathwaypathway
IntrinsicIntrinsicpathwaypathway
ATAT XaXaATAT ATAT
Fondaparinux Fondaparinux
XaXa
AntithrombinAntithrombin
Fondaparinux:Targeted Mechanism of Action
Turpie AGG, et al. N Engl J Med. 2001;344:619.
RivaroxabanHuman Factor Xa/rivaroxaban complex
Rivaroxaban is an oral, direct Factor Xa inhibitor, with high selectivity for Factor Xa (Ki 0.4±0.02 nM) 50% inhibition (IC50) for Factor VIIa, Factor XIa, thrombin, activated protein C, plasmin, urokinase, trypsin: >20,000 nM
Rivaroxaban is an investigational agent not yet approved by FDA.Roehrig S, et al. J Med Chem. 2005;48(19):5900-5908.
Perzborn P, et al. J Thromb Haemost. 2005;3(3):514-521.
S4
S1
N N ONH
O
SC l
O
O
O Rivaroxaban

48
APPRAISE-1
• ISTH major or CRNM bleeding: 7.9% for 10 mg apixaban, 5.7% for 5 mg apixaban, 3% for placebo (p=0.005 for high dose vs. placebo and p=0.09 for low dose vs placebo)
• Death, MI, recurrent ischemia, or stroke: 6.0%, 7.6%, 8.7% (p=0.07 for high dose vs placebo and p=0.21 for low dose vs placebo), respectively
Trial design: Patients recovering from an ACS were randomized to apixaban 10 mg daily (n=318), apixaban 2.5 mg twice daily (n=317), or placebo (n=611). Study medications were administered for 6 months.
Results
Conclusions• This dose-finding study reveals that bleeding
is increased among patients with a recent ACS with higher doses of apixaban compared with placebo
• Although this study was not powered for efficacy, adverse events appeared to be lowest with 10 mg apixaban
ISTH=International Society of Thrombosis and HaemostasisCRNM=clinically relevant non-major
Apixaban is an investigational agent not yet approved by FDA.Presented by Dr. John Alexander at ESC 2008.
%
7.9
5.7
3
p=0.005 for high dose vs
placebo
p=0.09 for low dose vs
placebo
Apixaban 10 mg Apixaban 5 mg
Placebo
0
3
6
9
ISTH major or CRNM bleedingISTH major or clinically relevant nonmajor bleeding
Rivaroxaban-Clinical Studies
- VTE Treatment
- Atrial Fibrillation
ACS treatment
Recent ACS PatientsStabilized 1-7 Days Post-Index Event
STRATUM 1STRATUM 1 STRATUM 2STRATUM 2
Primary Endpoint: TIMI Significant Bleeding
MD Decision to Treat with ClopidogrelMD Decision to Treat with Clopidogrel
Dose Levels5, 10, & 20 mg
N ~ 1,350
RIVAQD
3 Dose Levels
RIVAQD
3 Dose Levels
PLACEBO PLACEBO RIVABID
3 Dose Levels
RIVABID
3 Dose Levels
RIVAQD
3 Dose Levels
RIVAQD
3 Dose Levels
PLACEBOPLACEBORIVABID
3 Dose Levels
RIVABID
3 Dose Levels
Treat for 6 MonthsTreat for 6 Months
YESNO
STAGE 1: Dose Escalation
RIVA Rivaroxaban
ATLAS – TIMI 46
This study sponsored by Bayer/Johnson & Johnson Pharmaceutical Research & Development, LLC.
Recent ACS PatientsStabilized 1-7 Days Post-Index Event
STRATUM 1STRATUM 1 STRATUM 2STRATUM 2
Primary Endpoint: Death, MI, Stroke, or Recurrent Ischemia Requiring Revascularization
MD Decision to Treat with ClopidogrelMD Decision to Treat with ClopidogrelN ~ 2,100
RIVAQD
RIVAQDPLACEBOPLACEBO RIVA
BIDRIVABID
RIVAQD
RIVAQDPLACEBOPLACEBO RIVA
BIDRIVABID
Treat for 6 MonthsTreat for 6 Months
NO YES
STAGE 2: Dose Confirmation
RIVA=Rivaroxaban
ATLAS – TIMI 46
This study sponsored by Bayer/Johnson & Johnson Pharmaceutical Research & Development, LLC.
Mod-to-High Risk NSTE ACS w/ Planned Early Inv Strategy
OtamixGroup 1(n=450)
OtamixGroup 1(n=450)
RAspirin +clopidogrel
Bail-out eptifibatide in otamixaban
groups if rec. ischemia or thrombotic
complic. during PCI
Study druguntil end of PCI,
as clin. indicated, until Day 4 or hospital d/c,whichever comes first
1° EP: Death, MI, Urgent Revasc, Bail-out IIb/IIIa thru 7 d1° EP: Death, MI, Urgent Revasc, Bail-out IIb/IIIa thru 7 d
Coronary angiography ± PCI (Day 1-3)Coronary angiography ± PCI (Day 1-3)
OtamixGroup 2(n=450)
OtamixGroup 2(n=450)
OtamixGroup 4(n=450)
OtamixGroup 4(n=450)
OtamixGroup 5(n=450)
OtamixGroup 5(n=450)
OtamixGroup 3(n=450)
OtamixGroup 3(n=450)
UFH + Eptifi.(n=450)
UFH + Eptifi.(n=450)
at randomization
Day 30 Visit, Day 90 Tel f/up, Day 180 Tel. f/upDay 30 Visit, Day 90 Tel f/up, Day 180 Tel. f/up
Dose Ranging Study of Otomixaban - a Novel, Intravenous, Direct Xa Inhibitor
SEPIA-ACS 1 – TIMI 42
Otomixaban is an investigational agent not yet approved by FDA.This study sponsored by sanofi-aventis.
Factor Xa Inhibitors in DevelopmentIndicationIndication VTE prevention*VTE prevention* VTE treatmentVTE treatment Stroke
prevention in patients with AF
Other?Other?
IdraparinuxIdraparinux –– Phase III results Phase III results expected soonexpected soon
Long-term therapy caused
significantly more bleeding†
––
Rivaroxaban Rivaroxaban Phase IIIPhase III Phase IIIPhase III Phase III Phase II data in ACS to be presented at
AHA
LY517717LY517717 Phase IIb completedPhase IIb completed –– –– ––
YM150YM150 Phase IIa completedPhase IIa completed –– Planned ––
DUDU--176b176b Phase IIa completedPhase IIa completed –– Phase III planned ACS plannedACS planned
ApixabanApixaban Phase IIb Phase IIb completed; planned completed; planned in cancer patientsin cancer patients
Phase II Phase II underwayunderway
– Phase II data in ACS presented at ESC
PRTPRT--054021054021 Phase II plannedPhase II planned PlannedPlanned Planned Secondary Secondary prevention of stroke prevention of stroke
and MI plannedand MI planned
*Prevention of VTE after major orthopaedic surgery, unless indicated†The Amadeus Investigators. Lancet. 2008;371:315-321.

49
Factor Xa Inhibitors in Development
IndicationIndication VTE prevention*VTE prevention* VTE treatmentVTE treatment Stroke prevention in
patients with AF
Other?Other?
IdraparinuxIdraparinux –– Phase III results Phase III results expected soonexpected soon
Phase III halted ––
Rivaroxaban Rivaroxaban Phase IIIPhase III Phase IIIPhase III Phase III ACS ongoingACS ongoing
LY517717LY517717 Phase IIb completedPhase IIb completed –– – ––
YM150YM150 Phase IIa completedPhase IIa completed –– Planned ––
DUDU--176b176b Phase IIa completedPhase IIa completed –– Planned ACS plannedACS planned
ApixabanApixaban Phase IIb Phase IIb completed; planned completed; planned in cancer patientsin cancer patients
Phase II Phase II underwayunderway
– PostPost--ACS plannedACS planned
PRTPRT--054021054021 Phase II plannedPhase II planned PlannedPlanned Planned Secondary Secondary prevention of stroke prevention of stroke
and MI plannedand MI planned
*Prevention of VTE after major orthopaedic surgery, unless indicated
Questions for DiscussionWhat will optimal antiplatelet/antithrombin
therapy look like in 2015…
In PCI?
ACS medical management?
For patients who go onto CABG?
Long-term secondary prevention?
Among elderly patients?
Among patients with renal dysfunction?
Solutions for Toughest Cases •Apply evidence-based
ACS care to complex patient cases
•Probe difficult ACS issues in light of research
evidence and common medical practice
Learning Objectives
Recommended

















