Promoting positive outcomes for people in transport accidents
Associate Professor John Pead Australian Centre for Posttraumatic Mental Health
Dr Samantha McLeod
Clinical Health Psychologist
Paul Coburn Physiotherapist, TAC Medical Panel

Australian Centre for Posttraumatic Mental Health 2
Workshop preparation Workshop pre-reading: Lambert, T. et al (2001). Using outcome data to enhance treatment effects. Journal of Consulting and Clinical Psychology, 69 159-172 Preferred outcome measures What are your preferred self report measures for routine use in measuring changes in clients. These may be measures you already routinely use or have considered using. Typical recovery trajectories after a transport accident Using the diagram draw the typical patterns of recovery for people who have been in a transport accident. What label would you give each pattern of recovery ?

Australian Centre for Posttraumatic Mental Health 3
Routine outcome measures What are your attitudes?
1. How regularly do you use outcome measures in your day to day practice? 2. How often have you participated in education activities in the last five years that have discussed outcome measures ? 3. Outcome measures are useful for working with people with mental health problems. 4. Using outcome measures in my practice involves more effort than it is worth. 5. The following are the reasons I think that outcome measures should be used. Supervision Reflect on own strengths Peer reviews Review of treatment Your other reasons ?
Decision- making about closure Decision- making about progress Reviews with clients Reflection on cases
6. Overall how useful do you think that outcome measures are?

Australian Centre for Posttraumatic Mental Health 4
Why promote positive outcomes? Strategy, standards and service
Ensuring that people benefit from effective psychology
treatments is an integral part of Australia’s mental health
strategy, the professional standards for psychologists and
increasingly a service requirement of informed consumers

Australian Centre for Posttraumatic Mental Health 5
Why promote positive outcomes? National Mental Health Strategy
• To undertake regular reviews of outcomes of services provided to people with serious mental health problems and mental health disorders, as a central component of the delivery of mental health services and
• To encourage the development of national outcomes
standards for mental health services, and systems for assessing whether services are meeting these standards
In order to achieve these objectives, routine outcome measures are being introduced throughout Australian public and private mental health services.

Australian Centre for Posttraumatic Mental Health 6
Why promote positive outcomes? Better Mental Health Outcomes (BOMH) Most people with a mental disorder who seek help from a health professional, ask for help from their general practitioner rather than from a specialist mental health professional. In recognition of this, the Commonwealth is supporting general practitioners to build a strong system of primary mental health care through the Better Outcomes in Mental Health Care Initiative (BOMHC). It encourages evidence-based practice in primary mental health care and recognises that good practice in mental health includes both pharmacological and non-pharmacological interventions. The use of outcome measures by GP’s and psychologists is a requirement of funding under this scheme. http://www.psychology.org.au/members/bomhc/overview.pdf

Australian Centre for Posttraumatic Mental Health 7
Why promote positive outcomes? Treatment without benefit is not ethical An ethical requirement of members of the APS is that:
19. Members must terminate a consulting relationship when it is reasonably clear that the client is not benefiting from it. They must offer to help the client locate alternative sources of assistance. When a client indicates to a member that he or she would like a second opinion the member must offer every practical assistance to obtain a competent second opinion. 20. When there is evidence of a problem or a condition with which the member is not competent to deal, the member must make this clear to the client and must refer the client to an appropriate source of expertise. (p.3., Australian Psychological Society, 2003. Code of Ethics ) http://www.psychology.org.au/members/ethics/code_of_ethics.pdf

Australian Centre for Posttraumatic Mental Health 8
Why promote positive outcomes? Consumers ‘….consumers support the introduction of routine outcome assessments and see the process as having potential to contribute to the treatment they receive.’ ‘Key process issues from the consumers’ perspective include how the consumer is approached for information, how outcome measurement is used to strengthen therapeutic dialogue and the use of consumer ratings in treatment planning.’ ‘….consumers ….. want to see strong consumer involvement at all stages’ Graham C, Coombs T, Buckingham W, Eagar K, Trauer T, and Callaly T (2001) The Victorian Mental Health Outcomes Measurement Strategy: Consumer Perspectives on Future Directions for Outcome Self-Assessment. Report of the Consumer Consultation Project. Department of Human Services, Victoria.
Australian Centre for Posttraumatic Mental Health 9
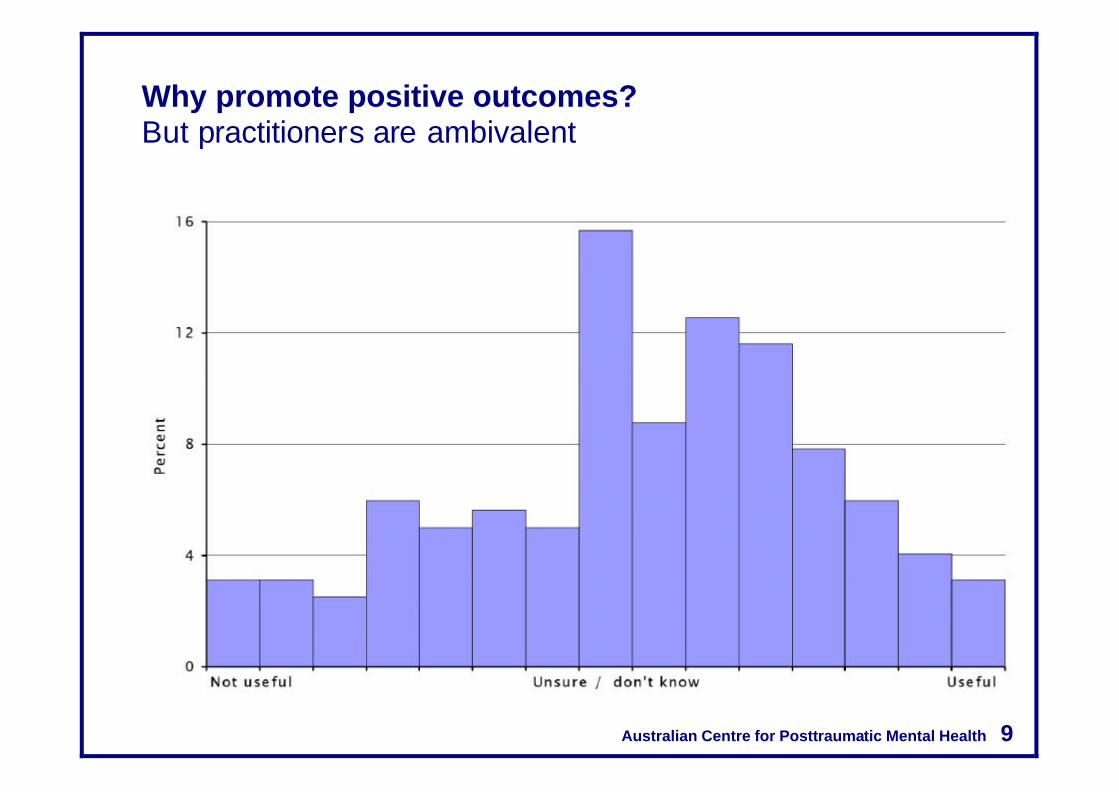
Why promote positive outcomes? But practitioners are ambivalent

Australian Centre for Posttraumatic Mental Health 10
Why promote positive outcomes? Practitioner ambivalence
Australian Centre for Posttraumatic Mental Health 11
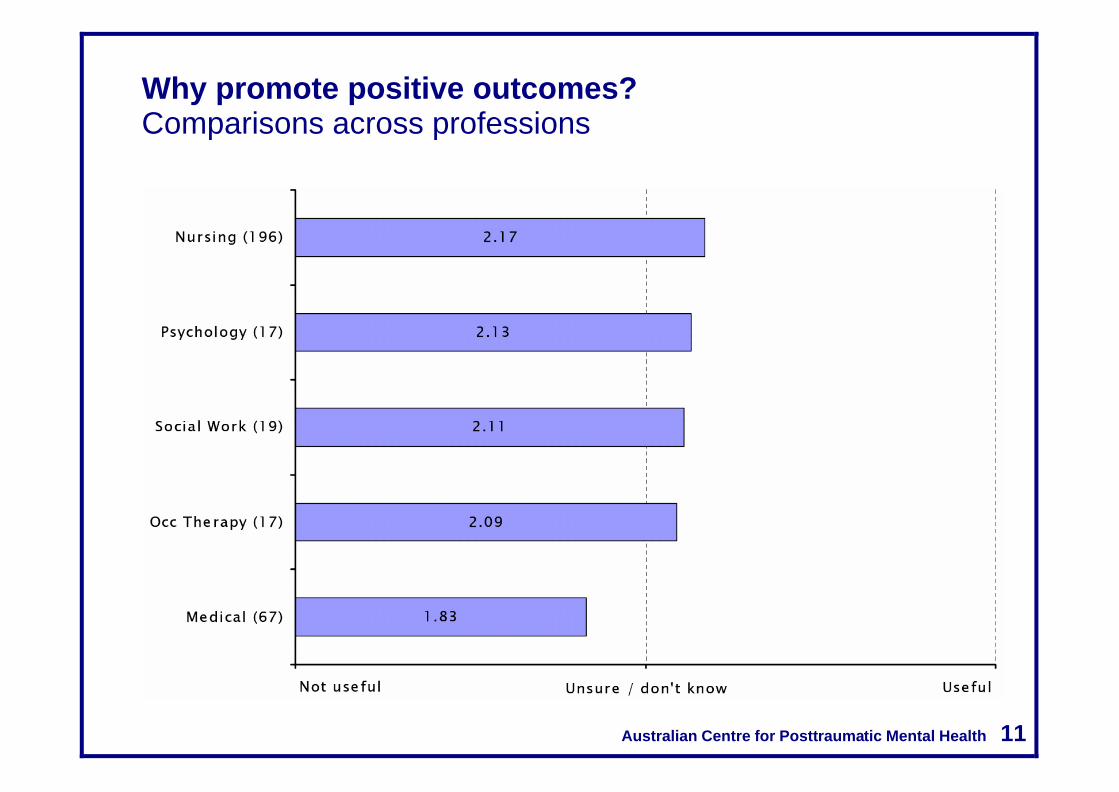
Why promote positive outcomes? Comparisons across professions

Australian Centre for Posttraumatic Mental Health 12
Why promote positive outcomes? Benefits must exist for practitioners
• to be of benefit to anyone, then the outcomes measures must be
seen by service providers to be “good measures with face validity,
that they will own.”
• Routine measurement of outcomes would provide a standardized
language for assessing clients and communicating results.
• Routine measurement of outcomes should be undertaken in a way
that is useful in planning of treatment
Stedman, T., Yellowlees, P., Mellsop, G., Clarke, R., and Drake, S. (1997). Measuring
Consumer Outcomes in Mental Health. Canberra, ACT: Department ofHealth and Family
Services.

Australian Centre for Posttraumatic Mental Health 13
Overview
• Introduction
• Trajectories
• Measures
• Challenges
• Treatment planning
Australian Centre for Posttraumatic Mental Health 14
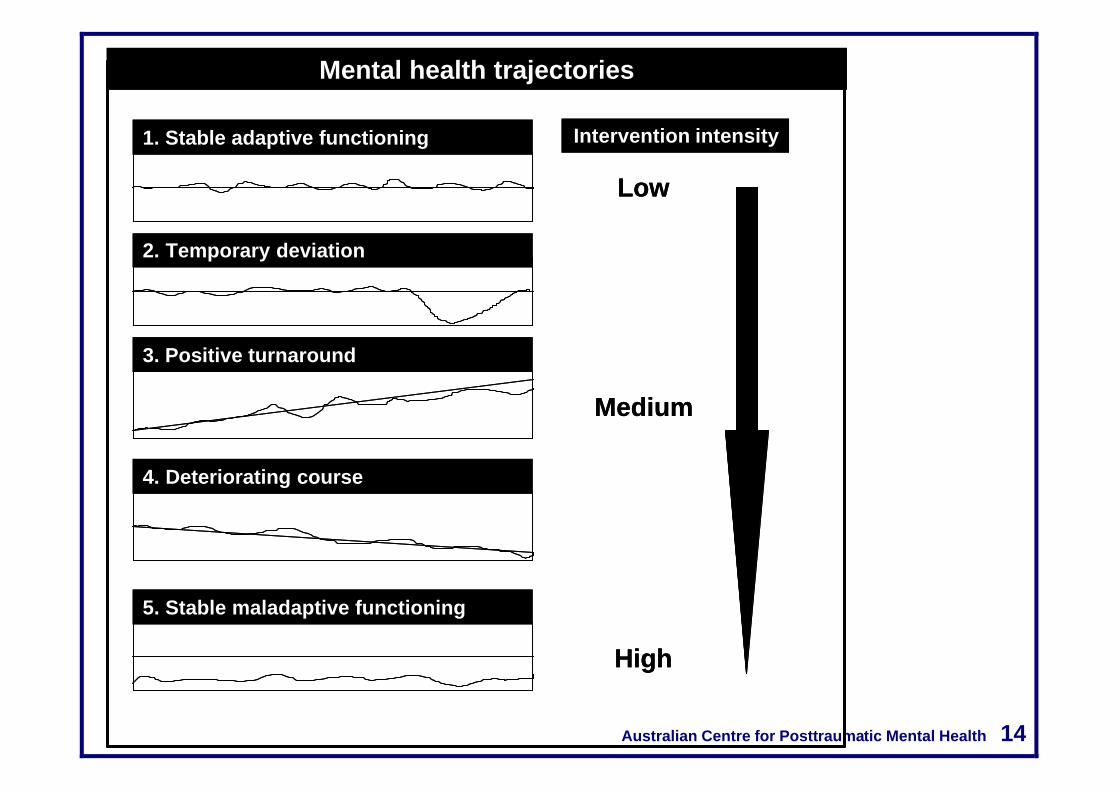
Mental health trajectories
1. Stable adaptive functioning
2. Temporary deviation
3. Positive turnaround
4. Deteriorating course
5. Stable maladaptive functioning
Low
Medium
High
Intervention intensity
Mental health trajectories
1. Stable adaptive functioning
2. Temporary deviation
3. Positive turnaround
4. Deteriorating course
5. Stable maladaptive functioning
Low
Medium
High
Intervention intensity

Australian Centre for Posttraumatic Mental Health 15
Pretrauma vulnerability and resilience
+
_
Pretrauma Trauma Posttrauma
Resilient
Vulnerable

Australian Centre for Posttraumatic Mental Health 16
The trauma features
+
_
Pretrauma Trauma Posttrauma

Australian Centre for Posttraumatic Mental Health 17
Health practitioners are naive
We are prone to everyday errors and biases in clinical judgment Biases and errors result from our judgment heuristics (shortcuts) that work well in everyday life, but lead to errors in clinical judgment e.g., longer term and attractive clients form the basis for our internal schemas Such errors are most likely under conditions of INFORMATION OVERLOAD. Precisely the situation in the fifty minute hour Only by being aware of this susceptibility and taking steps to address it can a clinician be as effective a decision maker as possible. Decision aids: be they actuarial benchmarks, treatment manuals, outcome measures are an effective means of limiting such bias and error.

Australian Centre for Posttraumatic Mental Health 18
RCT’s can be misleading
Time(Year)
Ou
tco
me
Accident 21 3+
+
-
Message: Most change <25hours; < 3 monthsup to 50% of gains made are lost at 2yrs

Australian Centre for Posttraumatic Mental Health 19
Effect sizes in RCT’s and real life

Australian Centre for Posttraumatic Mental Health 20
Routine treatment
Time(Year)
Ou
tco
me
Accident 21 3+
+
-
Comorbidity; >50% drop out; therapist factors are potent; treatment stays the same;> 25+ hours for effects; fluctuating outcomes

Australian Centre for Posttraumatic Mental Health 21
Alternative recovery trajectories
Time(Year)
Ou
tco
me
Accident 21 3+
+
-
A: Kick start, B: self managed, C: incremental, D: palliative
BC
D
A

Australian Centre for Posttraumatic Mental Health 22
What are outcome measures? Need to be distinguished from other kinds of measures of enduring characteristics such as personality traits, transient processes such as thoughts or expectations and satisfaction with treatment. Measure change in meaningful areas of a person’s life in a way that informs collaborative decisions about treatment. Enormous number of reasonably well constructed measures that are possible candidates for routine use by practitioners

Australian Centre for Posttraumatic Mental Health 23
Health outcome measures Is popular good?
Most widely evaluated outcome measures within 3921 reports (Garratt et al 2002) SF36 408 Sickness impact profile 111 Nottingham health profile 93 EORTC QLQC30 82 QALY 79 EuroQol 77 Health assessment questionnaire 62 Arthritis impact measurement scales 59 Quality of wellbeing scale 53 General health questionnaire 43 Health utilities index 41 COOP charts 33 Functional assessment of cancer 32 WHOQOL 24
Healthy years equivalent 24 *Beck depression inventory 23 Asthma quality of life questionnaire 21 *McGill pain questionnaire 19 WOMAC 18 *Hospital anxiety and depression scale 18 Duke health profile 17 SF12 15 *Psychological general wellbeing index 15 St George's respiratory disease questionnaire 15 MOSHIV 14 Rotterdam symptom check list 14

Australian Centre for Posttraumatic Mental Health 24
Selecting quality outcome measures
• Brevity and ease of administration favours self-report measures
• Can be scored by hand without an algorithm • Reliability has been demonstrated both internally and across
administrations
• Validity has been demonstrated by associations with established measures or clinical judgments
• Responsive to change means that the measure changes as the person problems change in nature and magnitude
• Australian norms so scores can be interpreted against average Australians who are well and have mental health problems
• In common languages, such as Greek, Italian, Chinese and Vietnamese
• Freely available at no cost Reduces the number of measures recommended for routine use

Australian Centre for Posttraumatic Mental Health 25
1. General mental health measures Widely used general measures covering the common mental health problems of anxiety and depression (Hickie, 2002). Reflect general mental distress. 4.1 Mental health screening: Kessler K10 (10 items) Australian norms across a national survey of 10,000+ people. The most widely used mental health measure by Australian general medical practitioners. 4.2 Anxiety/depression: Lovibond’s DASS(42 items) Australian norms. The second most widely used measure by GP’s. Together with the K10 is recommended as part of the Commonwealth’s Better Mental Health Outcomes (BOMH) scheme. Available in all common languages. 4.3 Anxiety/depression/health concerns: Hickie’s SPHERE (34 items) Australian norms across 49,000 GP attendances. Will be freely available on the TAC website.

Australian Centre for Posttraumatic Mental Health 26
2. Condition specific measures 2.1 Alcohol: Alcohol Use Disorders Identification Test (AUDIT) (Mandated best practice, Australian norms, large groups) 2.2 Cognitive: Wechsler Memory Scale (Australian norms, large groups) 2.3 Health concerns: SPHERE SOMA scale (Australian norms, large groups) 2.4 Trauma: Posttraumatic Checklist (PCL) (Australian norms for specific military and sexual assault populations only) 2.5 Pain: Orebro Musculoskeletal Pain Screening Questionnaire Wide range of other measures that each refer to particular sites of pain such as the neck, arms and legs. Unique in being generic. No Australian norms but overseas norms. In New Zealand used to predict outcomes using Yellow Flag approach (NZ Guidelines link).

Australian Centre for Posttraumatic Mental Health 27
3. Functional status These are measures of a persons day to day behaviour in undertaking activities of living in the areas of work, home and recreation. Surprisingly there are no Australian norms or widely accepted and used measures for activities of daily living or for those with mental health populations (Smith, 2001; Eager, 2000 ). 3.1 Health status: SF-12 and SF-36 (Australian norms) Require purchase and use of a computer based scoring algorithm 3.2 Orebro Musculoskeletal Pain Screening Questionnaire Until good measures are available adapting the wording of the Orebro items 15, 16, 20-24 is recommended irrespective of whether pain and physical disability is a feature. New Zealand guidelines for assessing risk and prognosis for recovery from lower back pain. 3.3 Multiaxial Pain Inventory Similar justification to Orebro. Use items 1-18 below.

Australian Centre for Posttraumatic Mental Health 28
Multiaxial Pain Inventory

Australian Centre for Posttraumatic Mental Health 29
Multiaxial Pain Inventory

Australian Centre for Posttraumatic Mental Health 30
Self-report measures Minimising response bias
Australian Centre for Posttraumatic Mental Health 31
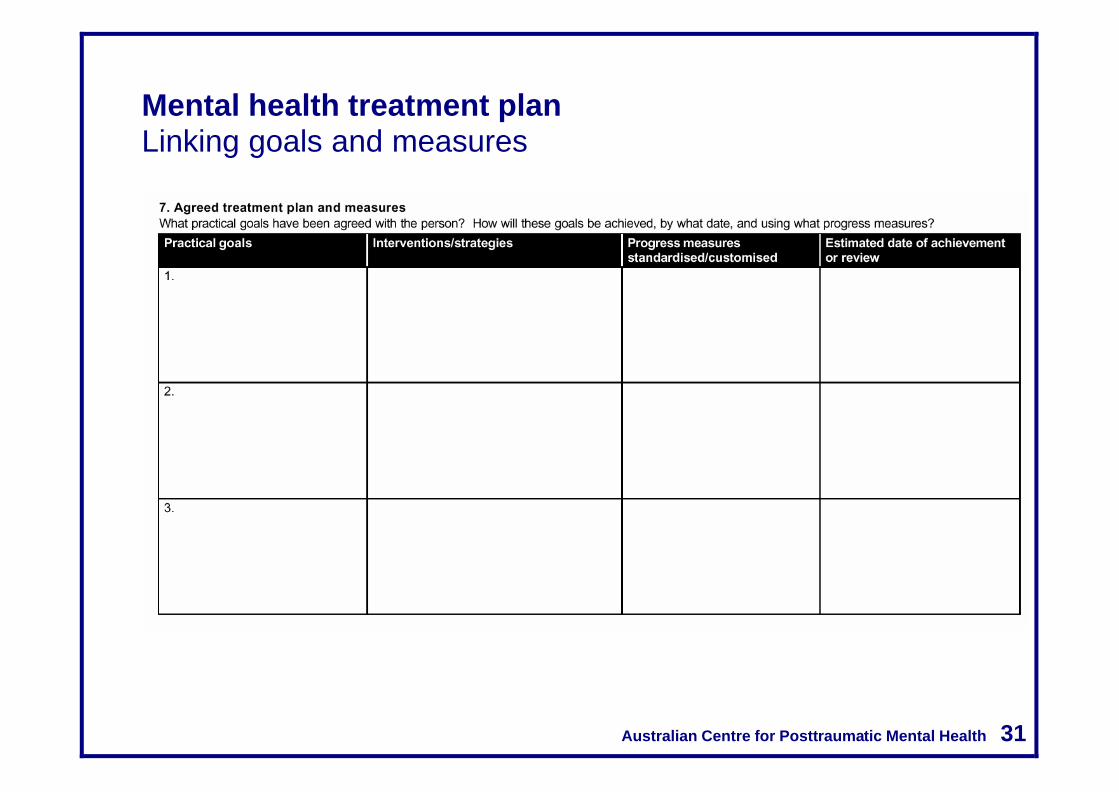
Mental health treatment plan Linking goals and measures

Australian Centre for Posttraumatic Mental Health 32
Why a few measures used regularly is best
• Become familiar with a few of the best available measures and use them regularly
• Provides practise in their administration, scoring and
interpretation and their utility for signalling the need for adjustments in the nature, intensity and duration of interventions.
• By using core measures over time the practitioner could build a
database of recovery curves that can be used for the purposes of benchmarking.
• With advances in the use of information technology it seems
likely that data like this could be combined across practitioners to develop norms for recovery from common mental health problems.

Australian Centre for Posttraumatic Mental Health 33
Small group exercises
1. Preferred outcome measures
• Break into small groups of 6-7 people) • Appoint a chairperson (the person whose last name comes first in
the alphabet) • Make a complete list of each persons top three preferred outcome
measures • Then, by giving each person three votes, take a vote to determine
the top three measures for the group • Why were these measures selected by your group?
2. What are the challenges in using routine outcome measures?
• Make a complete list of each persons top three challenges • Then, by giving each person three votes, take a vote to determine
the top three challenges

Australian Centre for Posttraumatic Mental Health 50
Questions and discussion Evaluation forms
Recommended

















