
Promises and Perils of Translational Research at Academic Health Centers: The CCHMC Model
Timothy P. Cripe, MD, PhD
Faculty Cross-Talk
October 5, 2006

Public Mandate
It is no longer good enough
to cure a mouse.
Translational research is…
“...moving a basic discovery
into early clinical trials.”
-J Kaiser, in “Translational Research: A Cure for Medicine’s Ailments?”
Science 311:1852, 31 Mar 2006
Promises
Discovery Development Delivery

Is it safe? Does it work? Can we make it better?
Discovery
DevelopmentDelivery

Translational Research is a Two-Way Bridge
Laboratory
Bench
Petri Dish
Clinic
Bedside
Patient
Analogy compliments of S. Davies

Peril #1: Time and Money

Time and Money
• Preclinical: 3-5 yrs, $3-5 million
• Manufacturing: 1-2 yrs, $1-2 million
• IND: 3-6 months, $0.5-1 million
• Phase I: 1-2 yrs, $1-3 million
• Phase II: 2-3 yrs, $3-6 million
• Phase III: 3-4 yrs, $10-20 million
• FDA: 1-3 yrs, $2-4 million
Source: http://www.wistechnology.com/article.php?id=377

Pharmaceutical Drug Development: Saganesque
From: DeMasi et al., J Health Economics 22:151, 2003
• 15-20 years15-20 years
• Direct costs: $403 millionDirect costs: $403 million
• Add in marketing: $802 millionAdd in marketing: $802 million
• Some estimates up to $1.7 billionSome estimates up to $1.7 billion
“…billions and billions…”

“…does anybody truly believe that academic translational research centers will be as
efficient, let alone competitive, at developing drugs as pharma?”
“…investing in translational research is akin to building a bridge to nowhere.”
-J Erickson, in Commentary: “Translational Research and Drug Development”
Science 312:997, 19 May 2006

Is AHC Translational Research Successful?
From: Contopoulos-Ioannidis et al., Am J Med 114:477, 2003
Nature, Cell, Science, JBC, JCI, J Exp Med

20 Year Follow-up of Promising Basic Science Technology
From: Contopoulos-Ioannidis et al., Am J Med 114:477, 2003
Of those identified over 5 year period:
• 1 in 4 led to published randomized trial
• 1 in 6 validated in positive trial
• <1 in 10 entered routine clinical use
• Only 1 deemed to have major impact(ACE inhibitors)

From: Contopoulos-Ioannidis et al., Am J Med 114:477, 2003

Peril #2: Regulatory Hurdles
Human Subject Research
• Extensive pre-clinical (laboratory) research precedes clinical trials
• History has shown that safeguards are necessary to protect people in clinical trials
• Safeguards are extensive• Enormous effort, time, costs underlie trials
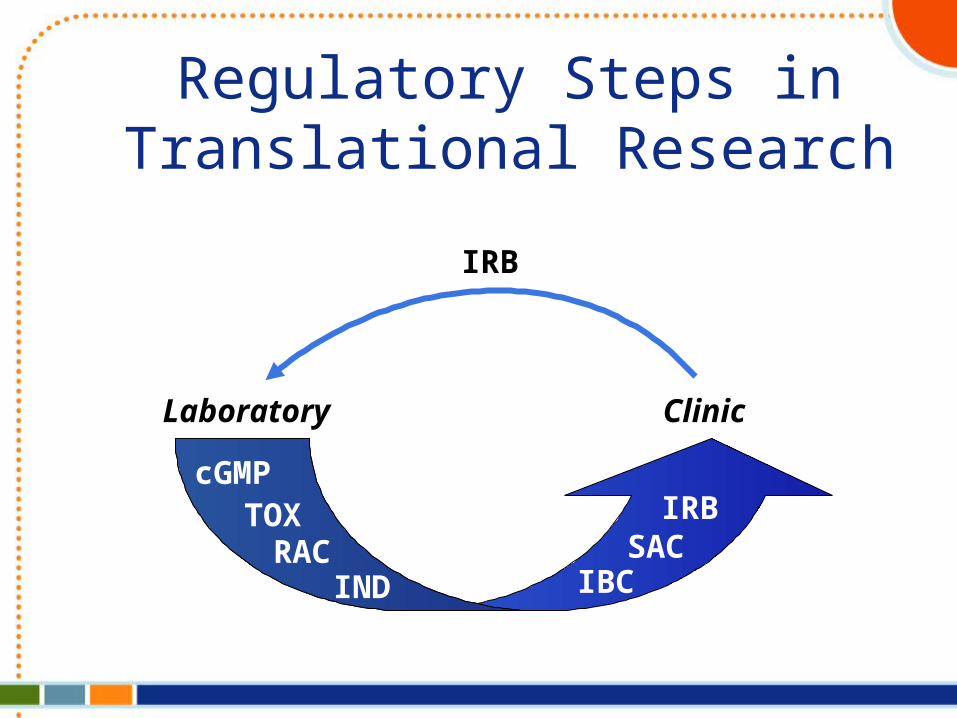
Regulatory Steps in Translational Research
Laboratory Clinic
IRB
RACIND
SACIRB
IBC
cGMPTOX

Levels of Burden: Sponsor vs. Investigator
• No IND– Fulfill PI level obligations (GCP)
• Company-held IND– Fulfill PI level obligations (GCP)
• Investigator-held, cross-referenced IND– Fulfill PI and Sponsor obligations (GCP)
• Investigator-held IND– Manufacture product (GMP)– Conduct non-clinical studies (GLP)– Fulfill PI and Sponsor obligations (GCP)
(Be the pharmaceutical company)

Peril #3: Academic Metrics

Hurdles for Patient-Oriented Translational Clinical Researchers
• Training– Extended– Requires scientist-clinician mentoring– Typically has been “on the job”
• Funding– Especially for orphan diseases, childhood diseases!
• Slow results (may take years for 1 trial)• Regulatory burdens• Fragmented infrastructure• Traditional metrics of success inadequate
– Publications– Grants– Patient revenues
From: Nathan DG, J Clin Invest 115:795, 2005
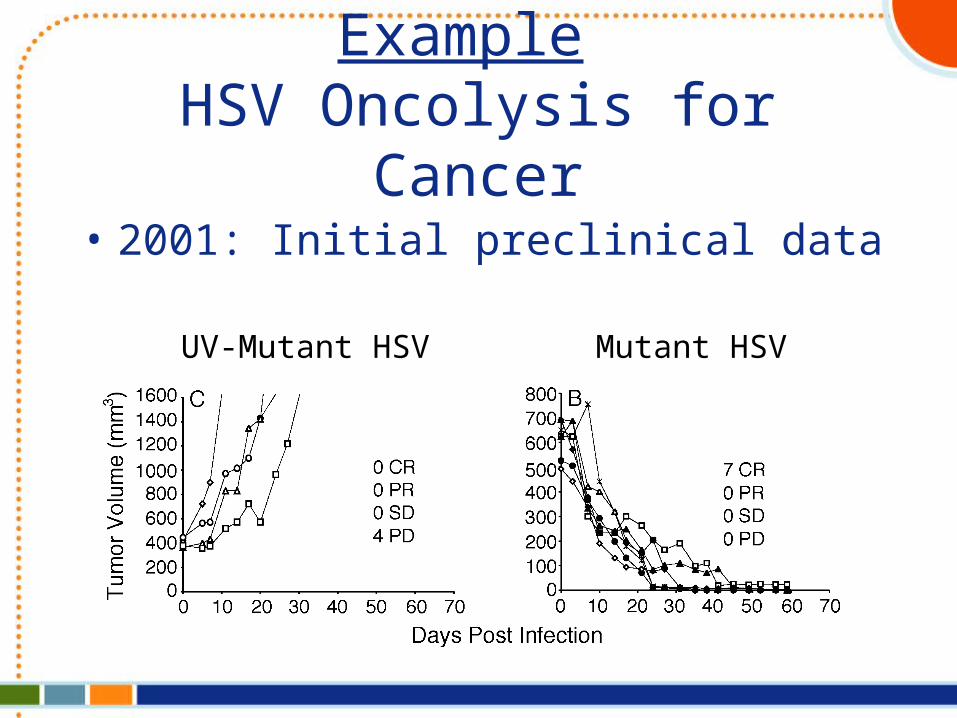
Example HSV Oncolysis for Cancer
• 2001: Initial preclinical data
UV-Mutant HSV Mutant HSV
• 2001: Clinical trial concept proposed• 2001-2004: More animal efficacy/safety• 2004-2006: Regulatory/funding hurdles
– Local• GCRC SAC, IBC, Radiation, IRB
– National• NGVL, NIH RAC, FDA IND
Example HSV Oncolysis for Cancer
My IND: 1 year and counting

Why should AHCs Conduct Translational Research?
• AHCs are birthplaces of ideas– Lionshare of basic science research
– Unburdened by company constraints
• Tantalizing translational data needed to engage industry
• AHCs can promote agendas with low market value– Orphan diseases
– Pediatric diseases
What’s an Institution to do?
•Enhance scientific and clinical interactions
•Build scientific infrastructure through grants program
•Build clinical operations to facilitate complex and multidisciplinary translational and clinical trials
•Provide support for complex regulatory help/oversight
CCHMC TRI NIH CTSA
CCHMC Translational Research Initiative (TRI):
• Founded in 2001• Supported by clinical revenues• Two-tiered mission
– To stimulate translational research via grants (financial support)• Pre-clinical and early phase clinical trials• Includes collection/analysis of biological samples
– To create infrastructure (regulatory support)• New cores• Workshops for clinical/research interactions• Education
– Annual symposium– Faculty scholar– Masters program for fellows
• Translational Research Trials Office
Cripe et al. Acad Med 80:1012, 2005
TRI Projects Funded 2001-2004• Translational research projects
– 31 projects– 30 investigators– 21 divisions/departments– $2.475 million
• Cores– 3 cores
• Fanconi anemia cell repository• Human milk bank• Mouse genotoxicity
– $250,000
• Workshops/symposia/retreats– 13 – $39,000
Results: First Four Years(30 Investigators given $2,475,000)
• 44 manuscripts • 18 extramural grants
– Total direct costs: $27,691,304 • 7 patents• 12 clinical trials launched

TRTO Office: First Five Years
• 11 INDs (plus 2 in development)• 48 IRB-approved protocols
– 15 Therapeutic– 33 Biologic/specimen collection
• Utilized by 8 CCHMC divisions• Normal donor program for lab research
– Blood (124)– G-CSF mobilized peripheral blood stem cells (86)– Bone marrow (173)– Umbilical cord blood (380)
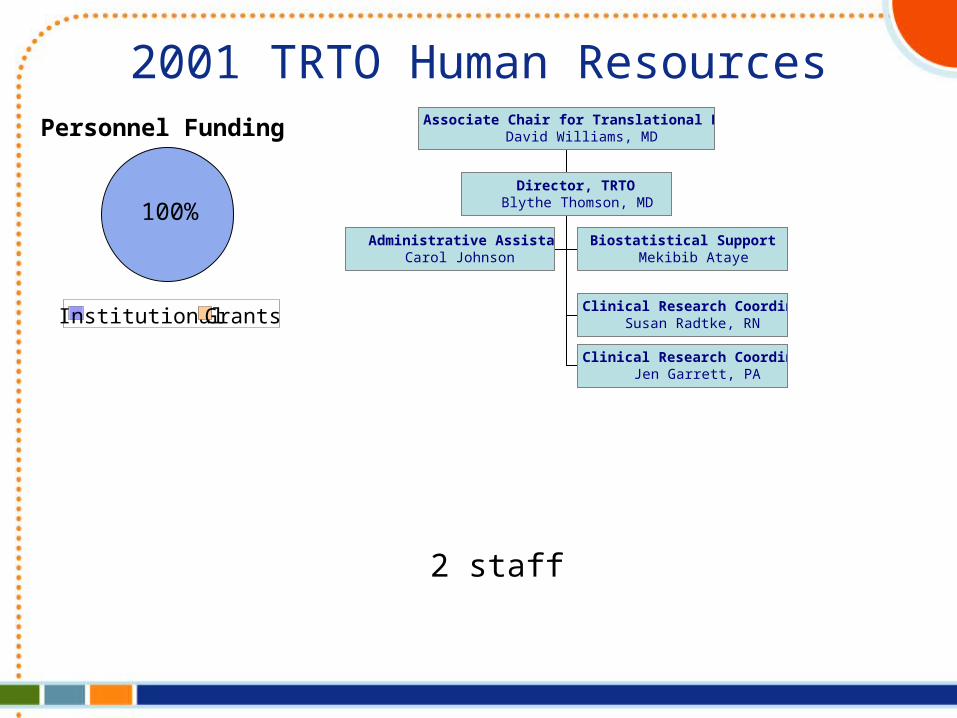
2001 TRTO Human Resources
Administrative AssistantCarol Johnson
Biostatistical Support (10%)Mekibib Ataye
Clinical Research CoordinatorSusan Radtke, RN
Clinical Research CoordinatorJen Garrett, PA
Director, TRTOBlythe Thomson, MD
Associate Chair for Translational ResearchDavid Williams, MDPersonnel Funding
100%
Institutional Grants
2 staff

Administrative AssistantCarol Johnson
Biostatistical Support (25%)Mi-ok Kim
Clinical Research CoordinatorJeanie Bailey
Research NurseRuth Spencer
Rare Lung Disease Network Normal Donor ProgramCarrie Stevens
Fanconi Anemia ProgramVivian Arnold
Clinical Research CoordinatorSusan Radtke
Clinical Research CoordinatorRubina Dosani
General/IND Studies
Clinical Coordinators QA CoodinatorElva Turner
Data Manager(open)
Clinical Research ManagerPeg Kaiser (interim)
Director, TRTOTimothy P. Cripe, MD, PhD
Associate Chair for Translational ResearchDavid Williams, MD
2006 TRTO Human ResourcesPersonnel Funding
54%46%
Institutional Grants
8 staff

In conclusion…

TranslationalTranslationalResearch:Research:MissionMissionImpossible?Impossible?

Proceed cautiously, hang in there

Pre-clinical testing is essential

Usually testing in multiple species is required

Other ideas may also work
When it comes to getting water to the fire…
Recommended

















