
Phase 1/2, Multicenter, Open-label, Pharmacokinetic, Safety, Tolerability, and Antiviral Activity Study of Dolutegravir (DTG),
a Novel Integrase Inhibitor, in Combination Regimens in HIV-1 Infected Infants, Children, and Adolescents: P1093
Rohan Hazra, Rolando Viani, Edward Acosta, Nan Zheng, Carmelita Alvero, Ellen O’Gara, Elizabeth Petzold,
Barb Heckman, Debra Steimers, Ivy Song, Steve Piscitelli, Andrew Wiznia, on behalf of the P1093 Study Team
July 24, 2012

Key Characteristics of DTG
• Once-daily, unboosted integrase inhibitor
• Low to moderate PK variability1
• Few drug interactions requiring dose adjustment
• Rapid and durable virologic response in adults2
– 10-50 mg DTG doses studied– 50 mg QD selected for phase 3, integrase inhibitor-naive subjects– Phase 3 treatment naïve adult data to be presented on Thursday
(SPRING-2)3
1. Song et al. 13th International Workshop on Clinical Pharmacology of HIV Therapy 2012; Barcelona, Spain. Abstract O_07.2. Stellbrink et al. CROI 2012; Seattle, WA. Abstract K-1002.3. Raffi et al. IAC 2012; Washington, DC. Abstract LBB04.
P1093 Study Design
• Phase 1/2 multicenter, open-label, noncomparative study of HIV-1 infected infants, children, and adolescents aged ≥6 wk to <18 y, of DTG when administered both prior to starting and in combination with OBT– Cohort 1: 12 to <18 y – Cohort 2: 6 to <12 y – Cohort 3: 2 to <6 y– Cohort 4: 6 mo to <2 y– Cohort 5: 6 wk to <6 mo

Enrollment Criteria
• INI-naïve• HIV-1 RNA >1000 copies/mL
• ARV treatment experienced–On ART
• Unchanged, failing regimen at least 8 wk
–Off ART• Off treatment 4 wk
• Must have at least 1 fully active drug for the OBT

P1093 Study Design
Day 1 Week 4 (PK and safety)Day 5-10Intensive PK visit
Functional monotherapy or
monotherapy phase
Optimize therapy continuation phase
48 wkDTG + OBT
Cohort 1: 12 to <18 yIntensive PK group n=10

Primary Objectives
• Select DTG dose that achieves similar exposure as the adult dose (AUC(0-24) as primary endpoint and C24 as secondary endpoint)
• Determine short- and long-term safety and tolerability• Evaluate steady-state PK of DTG in combination with
other antiretrovirals (OBT)
Protocol-Defined Targets
AUC(0-24) (µg*h/mL) C24 (µg/mL)
Targets 46 960
Target range 37-67 770-2260
Lower limit 25 500
Upper limit 92 NA
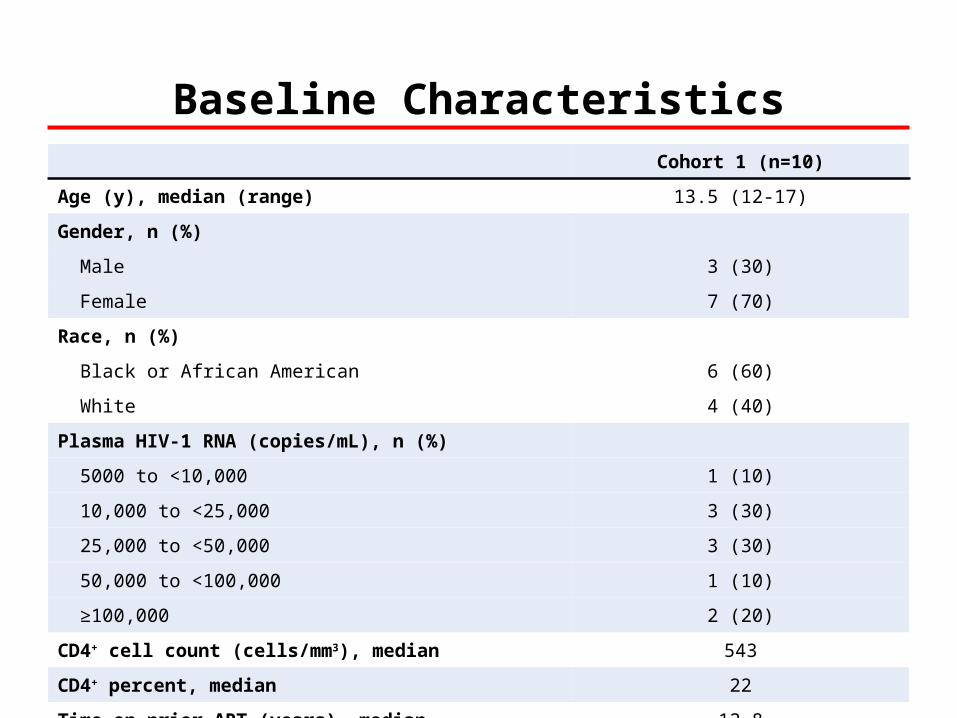
Baseline CharacteristicsCohort 1 (n=10)
Age (y), median (range) 13.5 (12-17)
Gender, n (%)
Male 3 (30)
Female 7 (70)
Race, n (%)
Black or African American 6 (60)
White 4 (40)
Plasma HIV-1 RNA (copies/mL), n (%)
5000 to <10,000 1 (10)
10,000 to <25,000 3 (30)
25,000 to <50,000 3 (30)
50,000 to <100,000 1 (10)
≥100,000 2 (20)
CD4+ cell count (cells/mm3), median 543
CD4+ percent, median 22
Time on prior ART (years), median 12.8

Prior Antiretroviral TherapiesART class n (%)
NRTI 10 (100)
PI 9 (90)
NNRTI 4 (40)
Triple class experienced 4 (40)
To minimize the potential impact of drug-drug interactions on PK variability, use of ATV, NVP, ATV/r, EFV, FPV, FPV/r, and TPV/r was not allowed PRIOR to the initial PK evaluation but could be added as part of optimized background therapy

P1093 Dosing Table for Cohort 1 (Tablet Formulation)
Dose range
Weight range (kg)
Dose (mg) n DTG tablets taken
DTG dose in mg/kg for lower-weight subjects
DTG dose in mg/kg for upper-weight subjects
15 to <20 20 0 Two 10 mg tablets 1.33 1.00
20 to <30 25 0 One 25 mg tablet 1.25 0.83
30 to <40 35 1 One 10 mg tablet AND one 25 mg tablet
1.17 0.88
≥40 50 9 One 50 mg tablet 1.25 ≤1.25

5000
4500
4000
3500
3000
2500
2000
1500
1000
500
0Mea
n (
SD
) p
las
ma
DT
G c
on
cen
trat
ion
(n
g/m
L)
0 5 10 15 20 25
Adult
Time (h)
PK Result: DTG Exposure in Cohort 1 (12 to <18 y) is Similar to Adults
Adult profile is based on pooled data from Study ING111521 and SPRING-1: Min et al. AIDS. 2011; 25(14): 1737-45. Stellbrink et al. CROI 2012; Seattle, WA. Abstract K-1002. van Lunzen et al. Lancet Infect Dis. 2012;12(2):111-118.
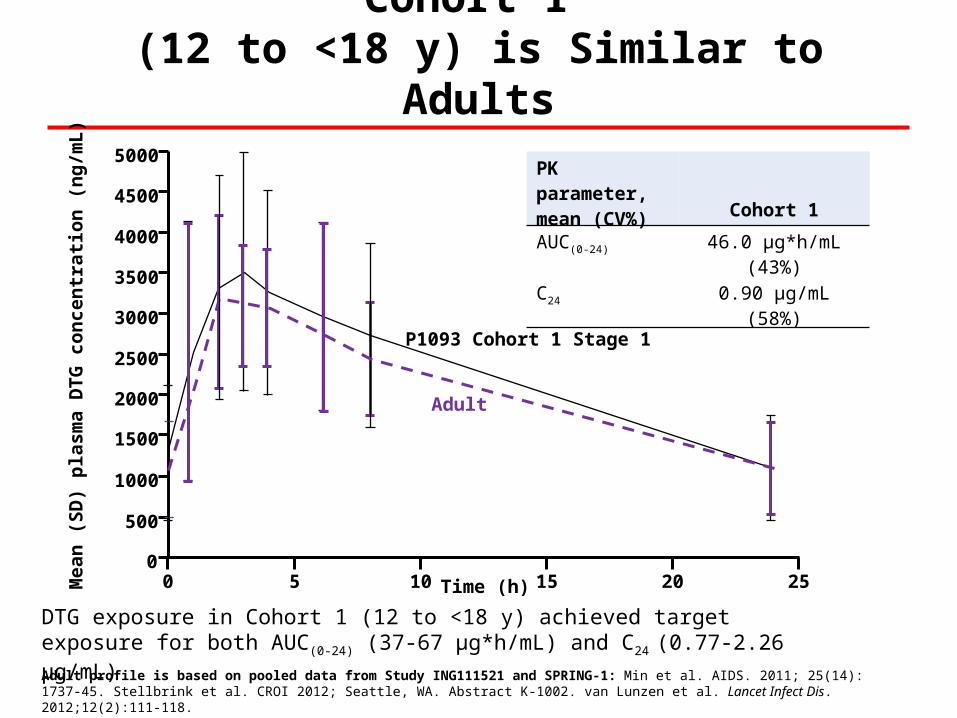
DTG exposure in Cohort 1 (12 to <18 y) achieved target exposure for both AUC(0-24) (37-67 µg*h/mL) and C24 (0.77-2.26 µg/mL)
PK Result: DTG Exposure in Cohort 1 (12 to <18 y) is Similar to Adults
5000
4500
4000
3500
3000
2500
2000
1500
1000
500
0Mea
n (
SD
) p
las
ma
DT
G c
on
cen
trat
ion
(n
g/m
L)
0 5 10 15 20 25
Adult
P1093 Cohort 1 Stage 1
Time (h)
PK parameter, mean (CV%) Cohort 1
AUC(0-24) 46.0 µg*h/mL (43%)
C24 0.90 µg/mL (58%)
Adult profile is based on pooled data from Study ING111521 and SPRING-1: Min et al. AIDS. 2011; 25(14): 1737-45. Stellbrink et al. CROI 2012; Seattle, WA. Abstract K-1002. van Lunzen et al. Lancet Infect Dis. 2012;12(2):111-118.

Safety at Week 4
• DTG was generally well tolerated
– No discontinuations
– No drug-related AEs
– No grade 3 or 4 clinical or laboratory events
– No trends in lab abnormalities

HIV-1 RNA Results at Week 4
Outcomes n/N Percent (95% CI)
HIV-1 RNA <40 copies/mL 7/10 70 (34.7, 93.3)
HIV-1 RNA <400 copies/mL 9/10 90 (55.5, 99.8)
Achieved at least 1 log10 drop in HIV-1 RNA or HIV-1 RNA <400 copies/mL
10/10 100 (69.1, 100)
Median change from baseline was -2.8 log10 copies/mL (95% CI: -3.1, -2.6)
Conclusions
• DTG achieved mean AUC(0-24) and C24 within target range in children aged 12 to <18 y– PK/safety/tolerability data support dose selection of 50 mg
in children aged 12 to <18 y weighing ≥40 kg– Supported further enrollment in remainder of this cohort
(now n=22) – Data support further DTG initiation in the younger pediatric
cohort (6 to <12 y)
• DTG plus OBT was well tolerated and potent through Week 4
• Development of pediatric formulation is ongoing

Acknowledgments
• Thanks to IMPAACT investigators and all of the participants and their families!
• Sites:– UCSF– Chicago Children’s– Children’s Hospital of Boston– Jacobi Medical Center
• Funding:– IMPAACT is funded by NIH,
NIAID, NICHD, and NIMH– Shionogi-ViiV Healthcare LLC
P1093• Rolando M. Viani, MD, MTP• Andrew Wiznia, MD• Rohan Hazra, MD• Paul Palumbo, MD• Edward P. Acosta, PharmD• Ellen Townley O'Gara, MSN, FNP• Elizabeth Petzold, PhD• Terence Fenton, EdD• Carmelita Alvero, MS• Nan Zheng, MA• Barbara Heckman, BS• Katherine Shin, PharmD• Linda Barlow-Mosha, MD, MPH• Mutsa Bwakura-Dangarembizi, MD• Derek Weibel• Jennifer Bryant, MPA• Linda Lambrecht, MS• Sherene Min, MD, MPH• Debra McCarty-Steimers, BS• Ivy Song, PhD• Stephen Piscitelli, PharmD
Recommended





![CELERA RUO INTEGRASE RESISTANCE ASSAY PERFORMS WELL … · integrase resistance is available (ViroSeq™ HIV-1 Integrase RUO Genotyping Kit [Celera, US]). In the current study we](https://img.dokumen.tips/doc/110x75/5e9a345cda348744545081fc/celera-ruo-integrase-resistance-assay-performs-well-integrase-resistance-is-available.jpg)










