Personalised Medicine
Gavin Giovannoni
Version 2.0
Disclosures
Over the last 15 years I have received personal compensation for participating in advisory boards in relation to clinical trial design, trial steering committees, and data and safety monitoring committees from: Abbvie, Bayer-Schering Healthcare, Biogen, Canbex, Eisai, Elan, Fiveprime, Genzyme, Genentech, GSK, GW Pharma, Ironwood, MSD, Merck Serono, Novartis, Pfizer, Roche, Sanofi, Synthon BV, Teva, UCB Pharma and Vertex Pharmaceuticals
Patient
Healthcare Professional(HCP)

ESF December 2012
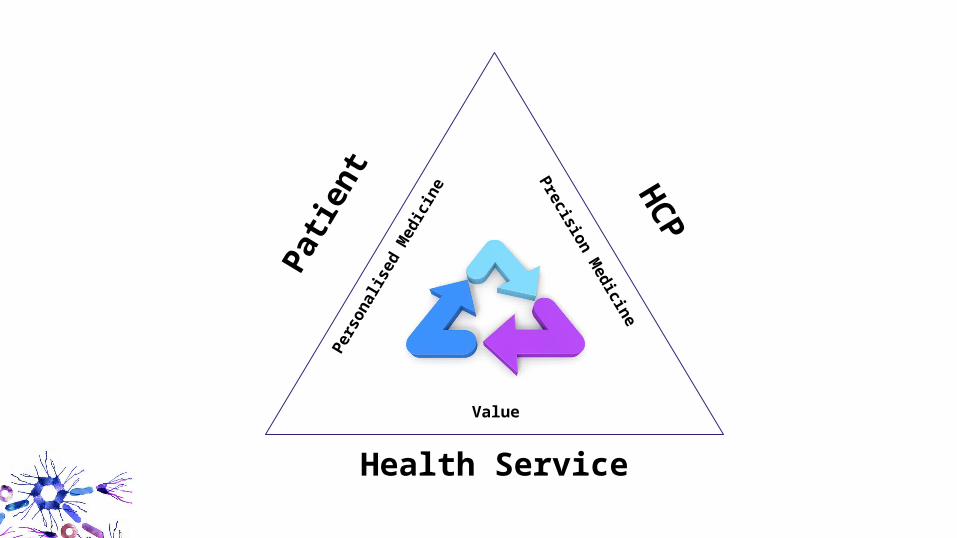
Patient
HCP
Patie
nt HCP
Health Service
Pers
onal
ised
Med
icin
e Precision Medicine
Value
Classification of MS
Multiple Sclerosis
Shared decision-making
Health Services
Databasing
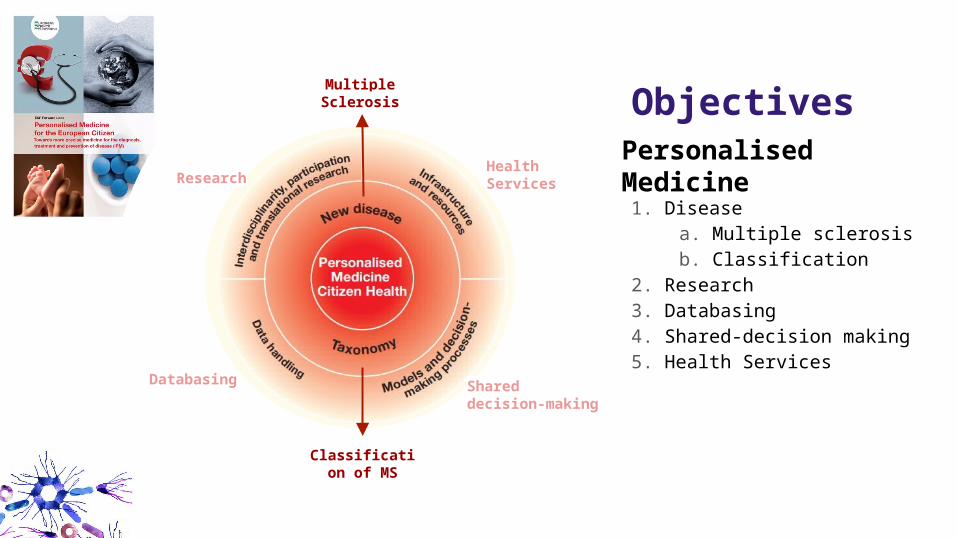
Research Personalised Medicine1. Disease
a. Multiple sclerosisb. Classification
2. Research3. Databasing4. Shared-decision making5. Health Services
Objectives
MRI Lesions
1st clinicalattack
Time (Years)
Asymptomaticdisease
Inflammation
Brain volume lossNerve cell loss
Dise
ase
Seve
rity
SPMSRRMS
1st MRI lesion
Relapses
CISRIS R-SPMS
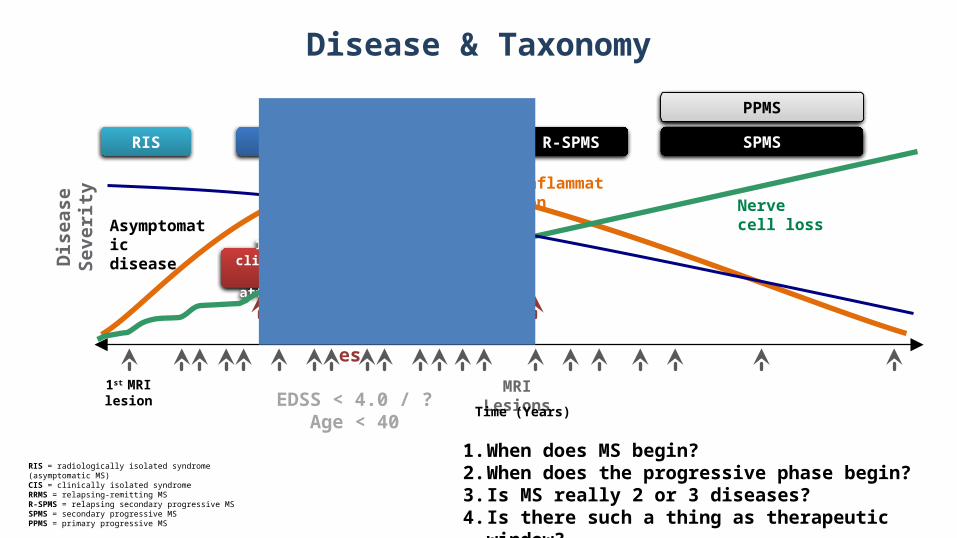
RIS = radiologically isolated syndrome (asymptomatic MS)CIS = clinically isolated syndromeRRMS = relapsing-remitting MS R-SPMS = relapsing secondary progressive MSSPMS = secondary progressive MSPPMS = primary progressive MS
PPMS
EDSS < 4.0 / ? Age < 40
Disease & Taxonomy
1. When does MS begin?2. When does the progressive phase begin?3. Is MS really 2 or 3 diseases?4. Is there such a thing as therapeutic window?
When does MS begin?
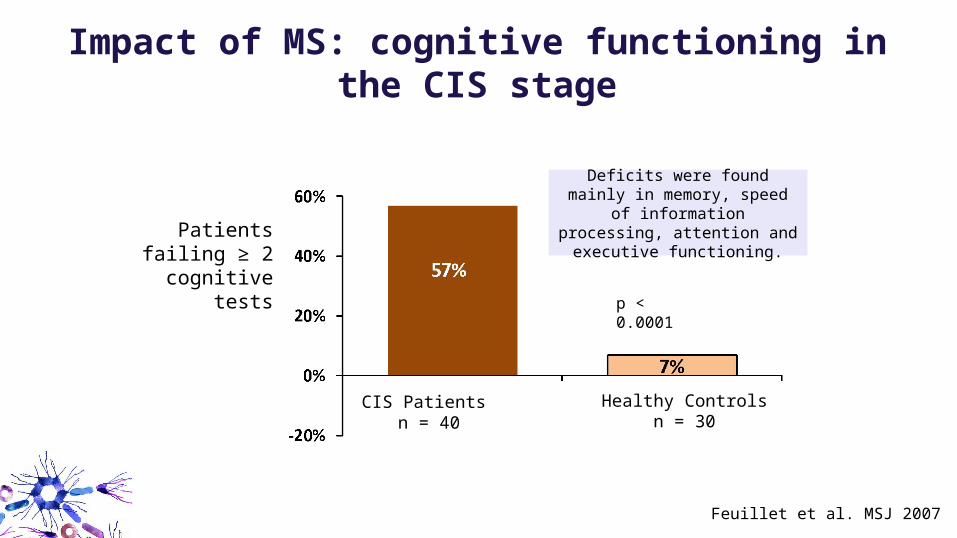
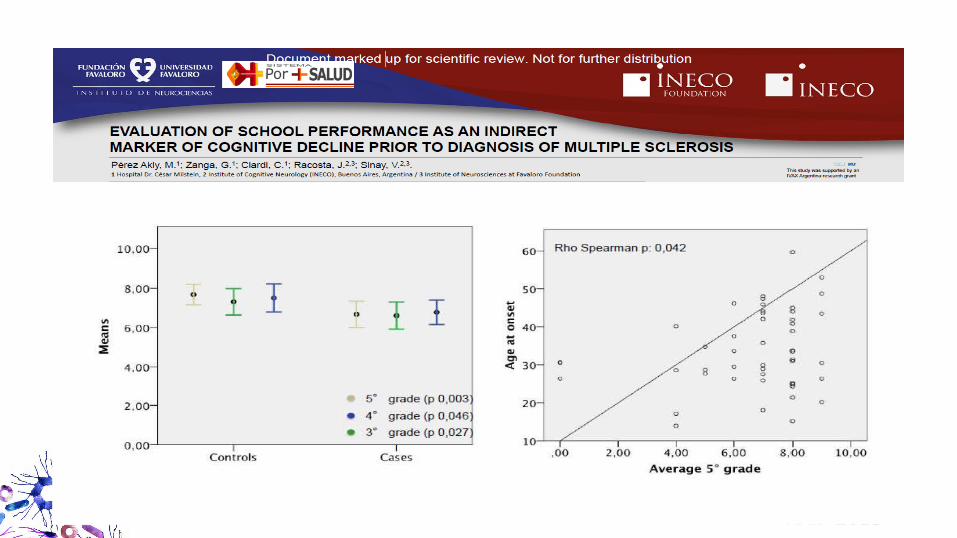
Impact of MS: cognitive functioning in the CIS stage
Feuillet et al. MSJ 2007
CIS Patients n = 40
Healthy Controlsn = 30
p < 0.0001
Deficits were found mainly in memory, speed of information
processing, attention and executive functioning.
Patients failing ≥ 2 cognitive
tests
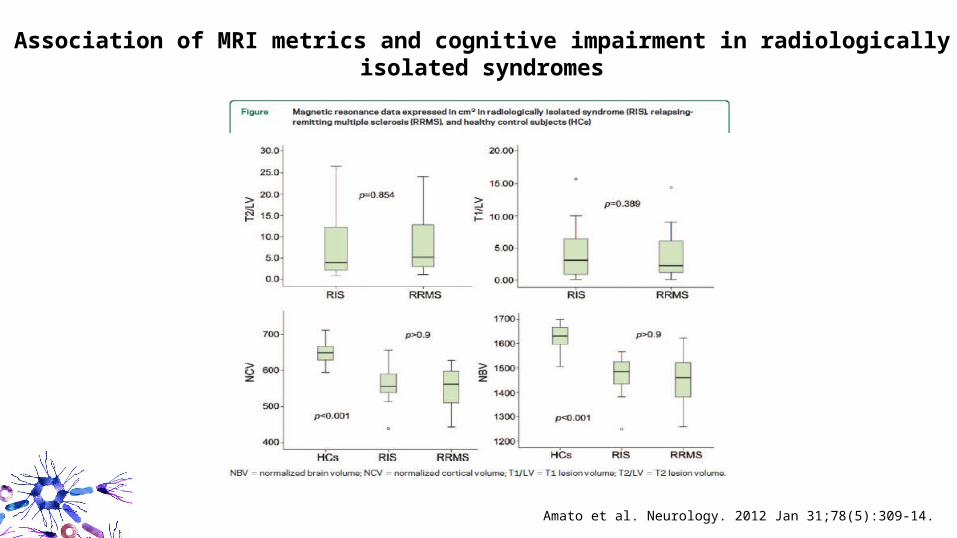
Association of MRI metrics and cognitive impairment in radiologically isolated syndromes
Amato et al. Neurology. 2012 Jan 31;78(5):309-14.
AAN 2013
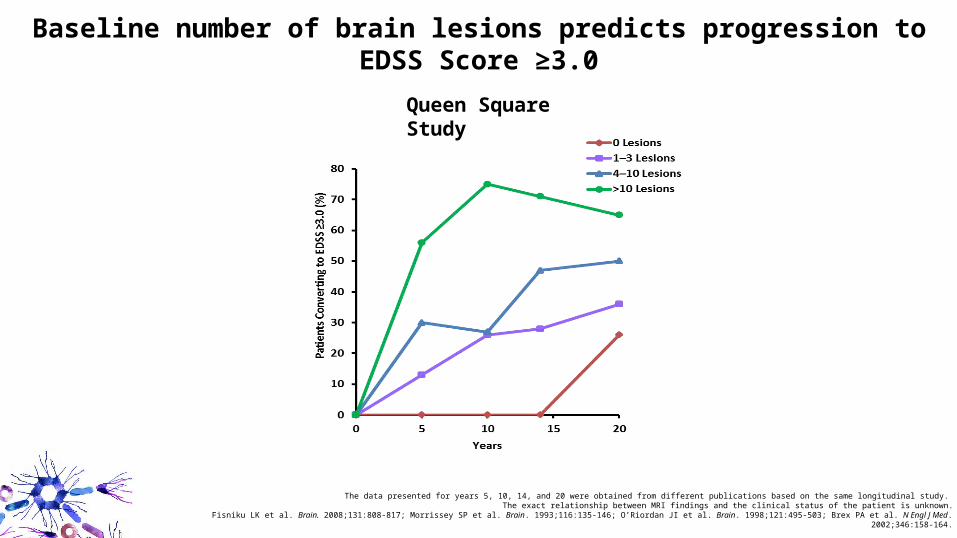
The data presented for years 5, 10, 14, and 20 were obtained from different publications based on the same longitudinal study. The exact relationship between MRI findings and the clinical status of the patient is unknown.
Fisniku LK et al. Brain. 2008;131:808-817; Morrissey SP et al. Brain. 1993;116:135-146; O’Riordan JI et al. Brain. 1998;121:495-503; Brex PA et al. N Engl J Med. 2002;346:158-164.
Baseline number of brain lesions predicts progression to EDSS Score ≥3.0
Queen Square Study
When does the progressive phase begin?
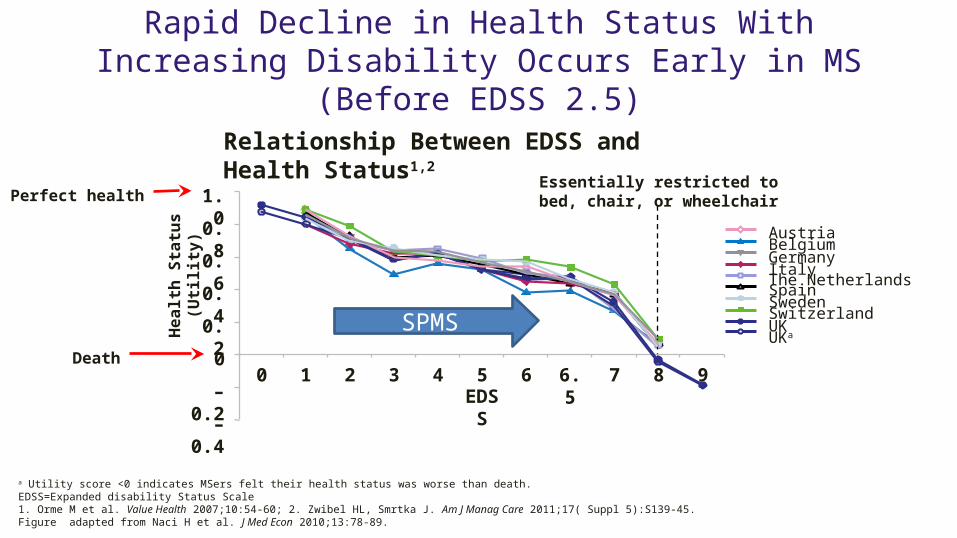
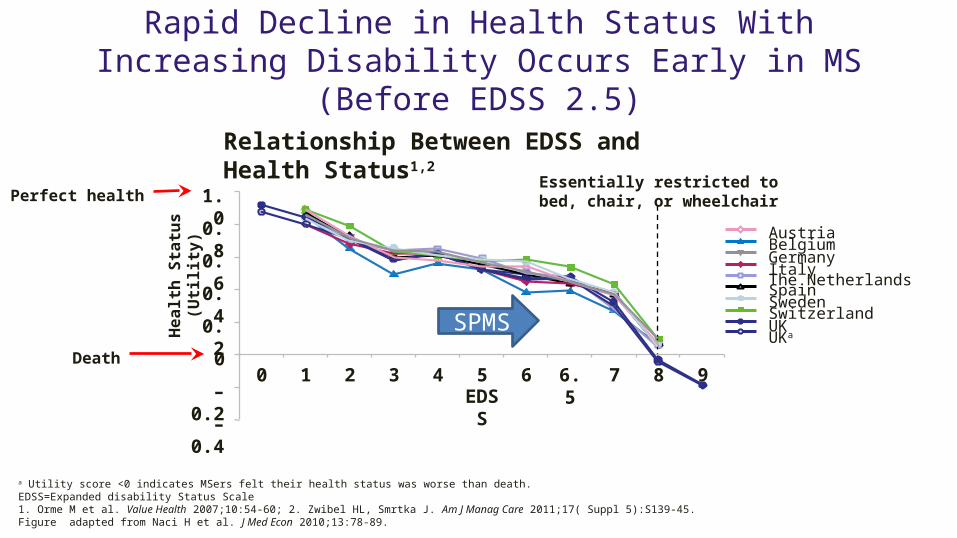
Rapid Decline in Health Status With Increasing Disability Occurs Early in MS (Before EDSS 2.5)
a Utility score <0 indicates MSers felt their health status was worse than death. EDSS=Expanded disability Status Scale1. Orme M et al. Value Health 2007;10:54-60; 2. Zwibel HL, Smrtka J. Am J Manag Care 2011;17( Suppl 5):S139-45. Figure adapted from Naci H et al. J Med Econ 2010;13:78-89.
Relationship Between EDSS and Health Status1,2
1.0
0.8
0.6
0.4
0.2
0
–0.2
–0.4
0 1 2 3 4 5 6 6.5 7 8 9
Heal
th S
tatu
s (U
tility
)
EDSS
Essentially restricted to bed, chair, or wheelchair
AustriaBelgiumGermany Italy The NetherlandsSpainSwedenSwitzerlandUK UKa
Perfect health
Death
SPMS
Rapid Decline in Health Status With Increasing Disability Occurs Early in MS (Before EDSS 2.5)
a Utility score <0 indicates MSers felt their health status was worse than death. EDSS=Expanded disability Status Scale1. Orme M et al. Value Health 2007;10:54-60; 2. Zwibel HL, Smrtka J. Am J Manag Care 2011;17( Suppl 5):S139-45. Figure adapted from Naci H et al. J Med Econ 2010;13:78-89.
Relationship Between EDSS and Health Status1,2
1.0
0.8
0.6
0.4
0.2
0
–0.2
–0.4
0 1 2 3 4 5 6 6.5 7 8 9
Heal
th S
tatu
s (U
tility
)
EDSS
Essentially restricted to bed, chair, or wheelchair
AustriaBelgiumGermany Italy The NetherlandsSpainSwedenSwitzerlandUK UKa
Perfect health
Death
SPMS
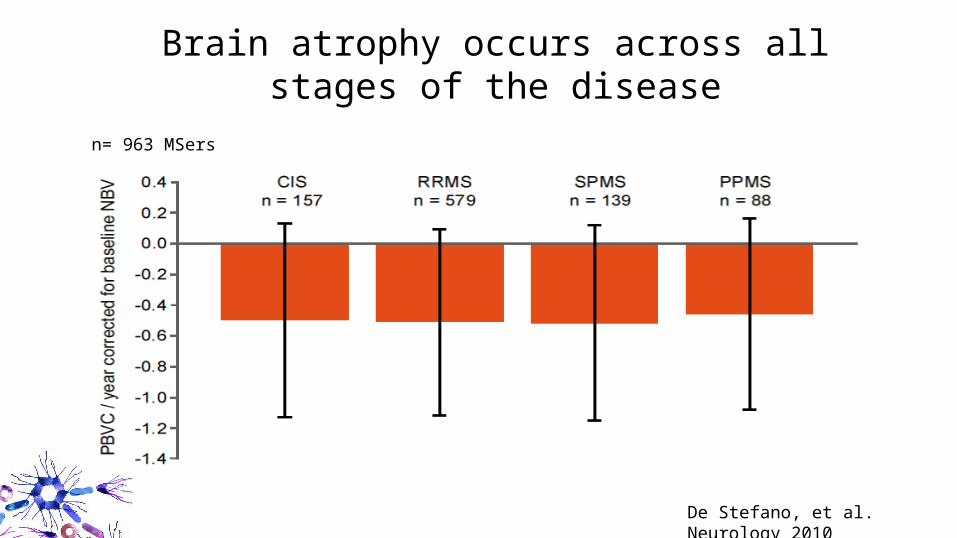
Brain atrophy occurs across all stages of the disease
De Stefano, et al. Neurology 2010
n= 963 MSers
Is MS really 2 or 3 diseases?
Is multiple sclerosis?
a. One disease
b. Two diseases; relapse-onset and primary progressive MS
c. Three diseases; relapsing-remitting MS, secondary progressive MS and primary progressive MS
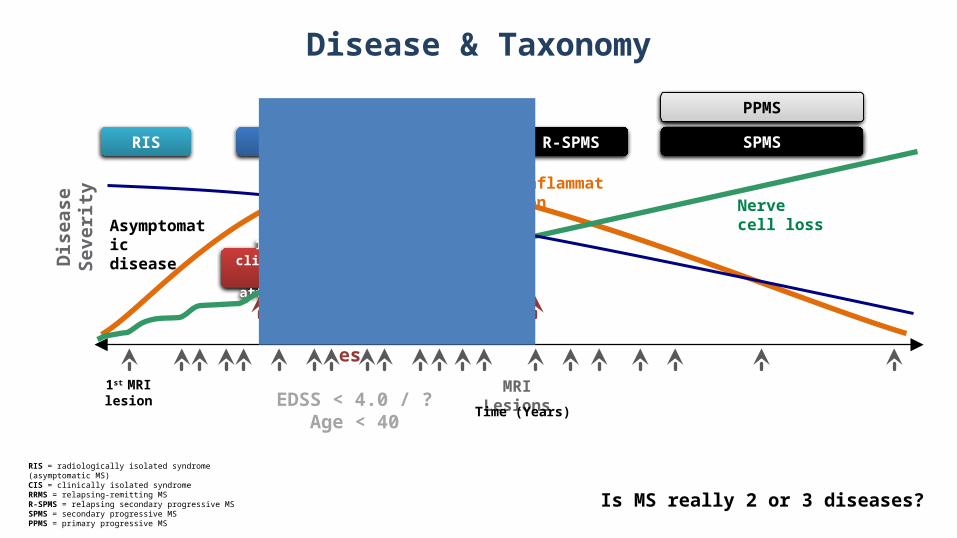
MRI Lesions
1st clinicalattack
Time (Years)
Asymptomaticdisease
Inflammation
Brain volume lossNerve cell loss
Dise
ase
Seve
rity
SPMSRRMS
1st MRI lesion
Relapses
CISRIS R-SPMS
RIS = radiologically isolated syndrome (asymptomatic MS)CIS = clinically isolated syndromeRRMS = relapsing-remitting MS R-SPMS = relapsing secondary progressive MSSPMS = secondary progressive MSPPMS = primary progressive MS
PPMS
EDSS < 4.0 / ? Age < 40
Disease & Taxonomy
Is MS really 2 or 3 diseases?
1983 U.S. Orphan Drug Act
● Eligibility– Disease affects few people in U.S. (<200,000)– Or no reasonable expectation that profitable– Low expected returns sufficient not necessary
● Incentives– R&D tax credits: ½ clinical, even if not approved– Clinical research grant programs– FDA counseling and priority review– Guaranteed market exclusivity of 7 years
#MS-is-1-not-2-or-3-diseases
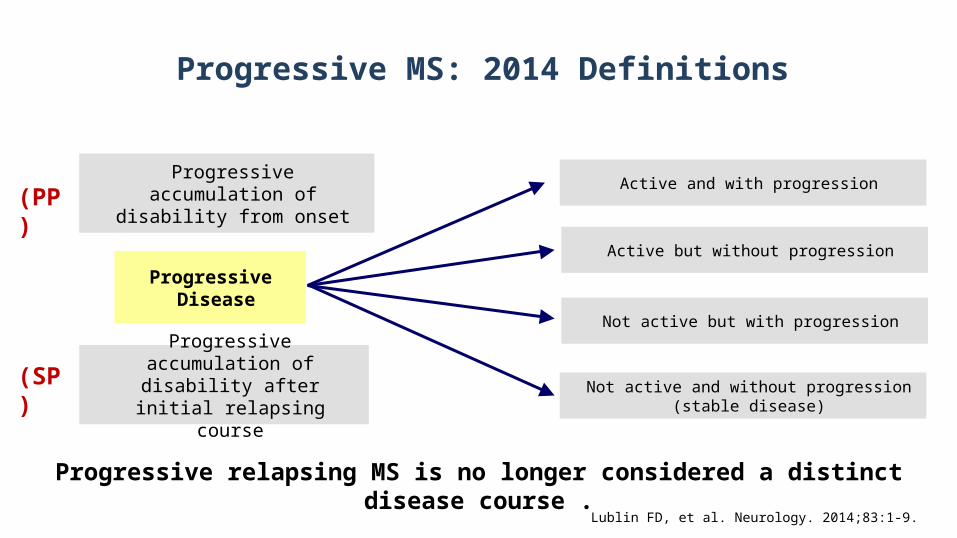
Progressive MS: 2014 Definitions
Progressive Disease
Progressive accumulation of disability from onset(PP)
Progressive accumulation of disability after initial relapsing
course
(SP)
Active and with progression
Active but without progression
Not active but with progression
Not active and without progression(stable disease)
Lublin FD, et al. Neurology. 2014;83:1-9.
Progressive relapsing MS is no longer considered a distinct disease course .
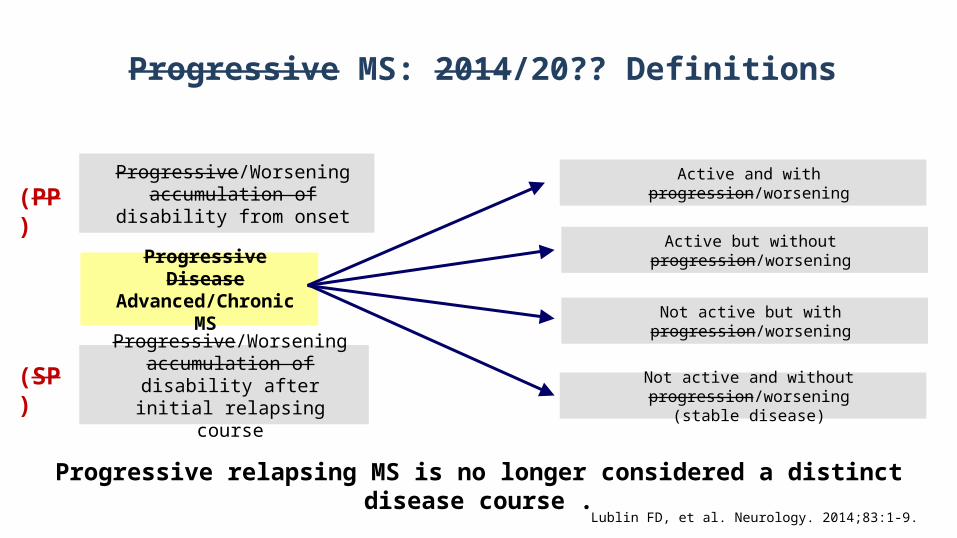
Progressive MS: 2014/20?? Definitions
Progressive DiseaseAdvanced/Chronic MS
Progressive/Worsening accumulation of disability from
onset(PP)
Progressive/Worsening accumulation of disability after
initial relapsing course
(SP)
Active and with progression/worsening
Active but without progression/worsening
Not active but with progression/worsening
Not active and without progression/worsening(stable disease)
Lublin FD, et al. Neurology. 2014;83:1-9.
Progressive relapsing MS is no longer considered a distinct disease course .
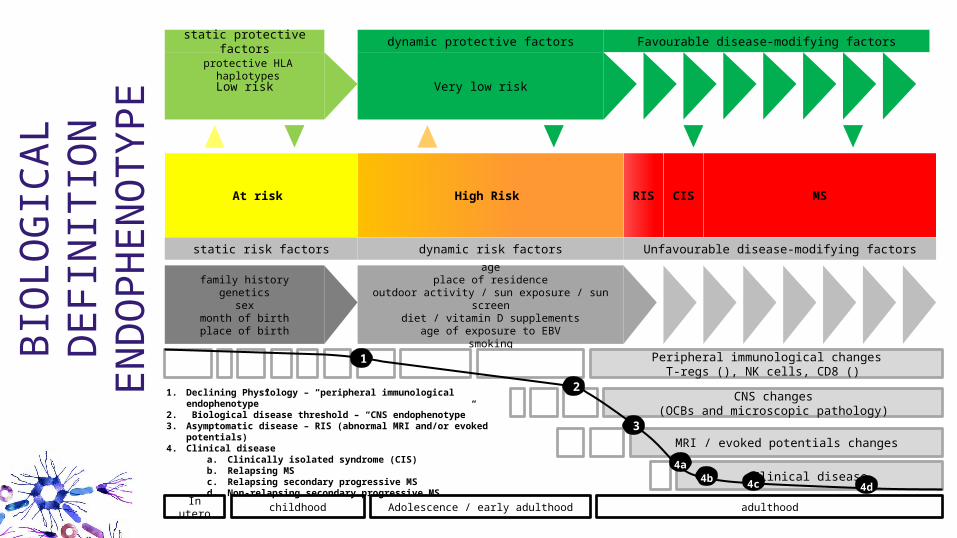
Very low risk
ageplace of residence
outdoor activity / sun exposure / sun screendiet / vitamin D supplements
age of exposure to EBVsmoking
At risk High Risk
Low risk
RIS CIS MS
family historygenetics
sexmonth of birthplace of birth
Unfavourable disease-modifying factorsdynamic risk factorsstatic risk factors
dynamic protective factorsstatic protective factors
MRI / evoked potentials changes
Peripheral immunological changesT-regs (), NK cells, CD8 ()
Clinical disease
In utero childhood Adolescence / early adulthood adulthood
1. Declining Physiology – “peripheral immunological endophenotype”2. Biological disease threshold – “CNS endophenotype”3. Asymptomatic disease – RIS (abnormal MRI and/or evoked
potentials)4. Clinical disease
a. Clinically isolated syndrome (CIS)b. Relapsing MSc. Relapsing secondary progressive MSd. Non-relapsing secondary progressive MS
Favourable disease-modifying factors
protective HLA haplotypes
CNS changes(OCBs and microscopic pathology)
2
3
24b 24c 24d
24a
1
BIO
LOGI
CAL
DEFI
NIT
ION
ENDO
PHEN
OTY
PE
Is there such a thing as therapeutic window?
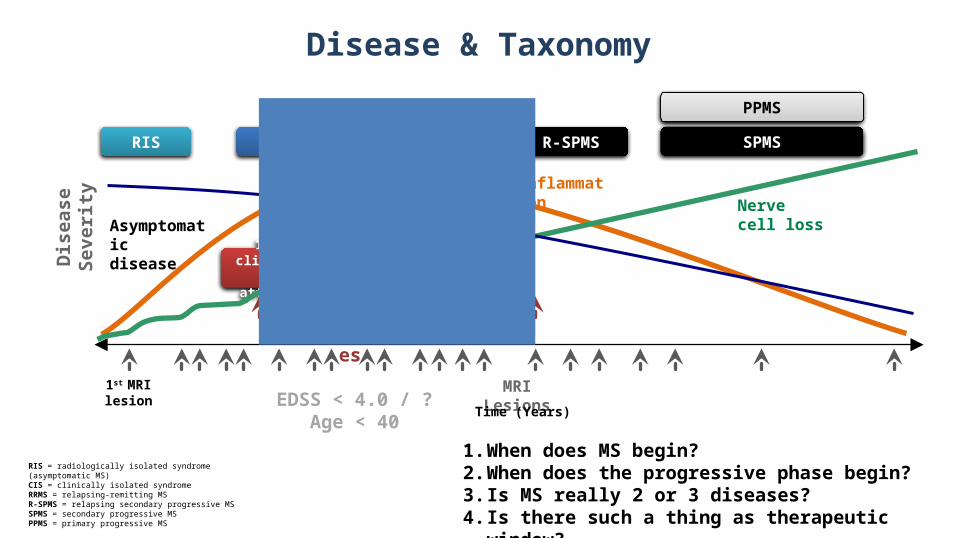
MRI Lesions
1st clinicalattack
Time (Years)
Asymptomaticdisease
Inflammation
Brain volume lossNerve cell loss
Dise
ase
Seve
rity
SPMSRRMS
1st MRI lesion
Relapses
CISRIS R-SPMS
RIS = radiologically isolated syndrome (asymptomatic MS)CIS = clinically isolated syndromeRRMS = relapsing-remitting MS R-SPMS = relapsing secondary progressive MSSPMS = secondary progressive MSPPMS = primary progressive MS
PPMS
EDSS < 4.0 / ? Age < 40
Disease & Taxonomy
1. When does MS begin?2. When does the progressive phase begin?3. Is MS really 2 or 3 diseases?4. Is there such a thing as therapeutic window?
29
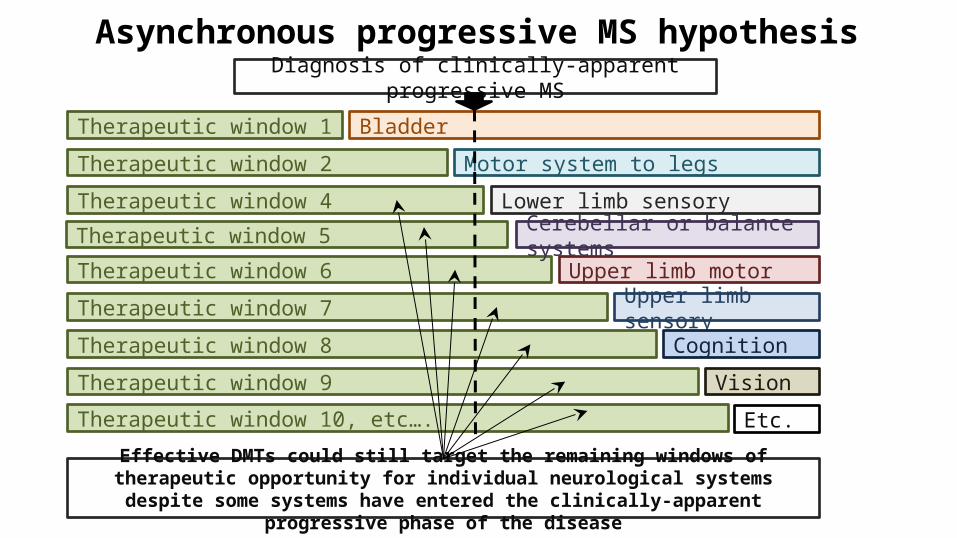
Therapeutic window 5
Asynchronous progressive MS hypothesis
Motor system to legs
Lower limb sensory
BladderTherapeutic window 1
Therapeutic window 2
Therapeutic window 4
Upper limb sensory
Upper limb motor
Cognition
Vision
Etc.
Therapeutic window 6
Therapeutic window 7
Therapeutic window 8
Therapeutic window 9
Therapeutic window 10, etc….
Diagnosis of clinically-apparent progressive MS
Effective DMTs could still target the remaining windows of therapeutic opportunity for individual neurological systems despite some systems have entered the clinically-apparent
progressive phase of the disease
Cerebellar or balance systems
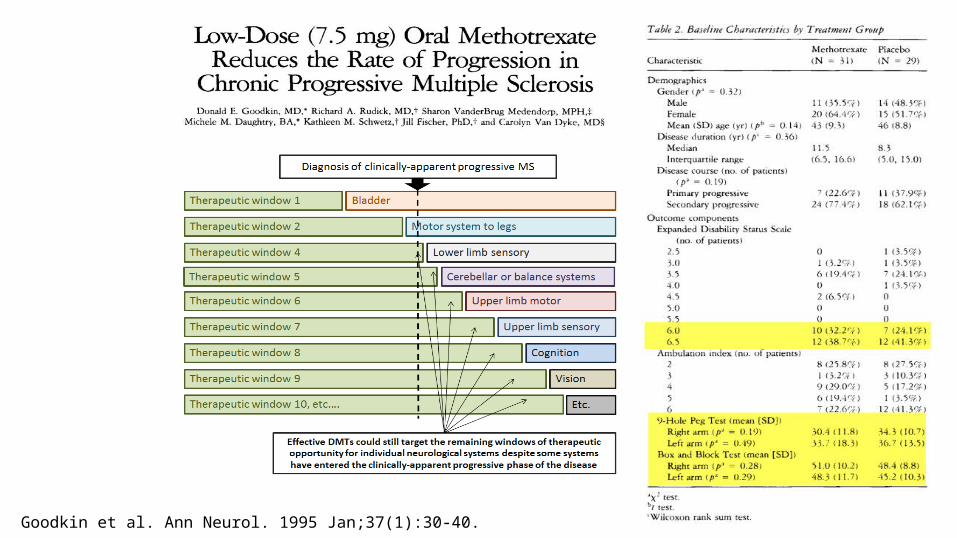
Goodkin et al. Ann Neurol. 1995 Jan;37(1):30-40.
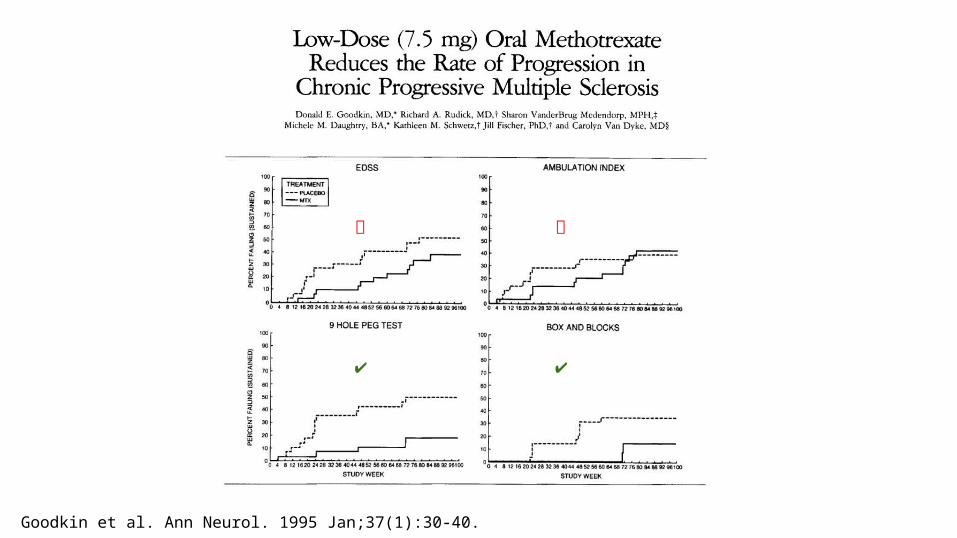
Goodkin et al. Ann Neurol. 1995 Jan;37(1):30-40.
❌❌
✔ ✔

32
Methods and resultsStandard analysis:KM survival curves and Cox model (proportional hazard assumption=HR constant over time)
SPECTRIMS PROMISEHR=0.88 (0.72-1.07), p=0.19 HR=0.88 (0.71-1.07), p=0.18
Slide courtesy of Maria Pia-Sormani
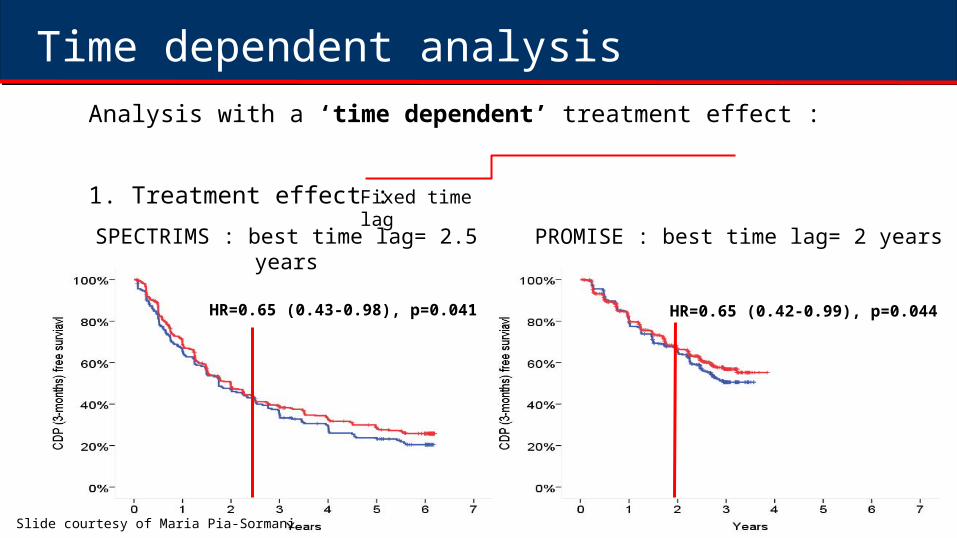
Time dependent analysisAnalysis with a ‘time dependent’ treatment effect :
1. Treatment effect : SPECTRIMS : best time lag= 2.5 years
HR=0.65 (0.43-0.98), p=0.041
Fixed time lag
PROMISE : best time lag= 2 years
HR=0.65 (0.42-0.99), p=0.044
Slide courtesy of Maria Pia-Sormani
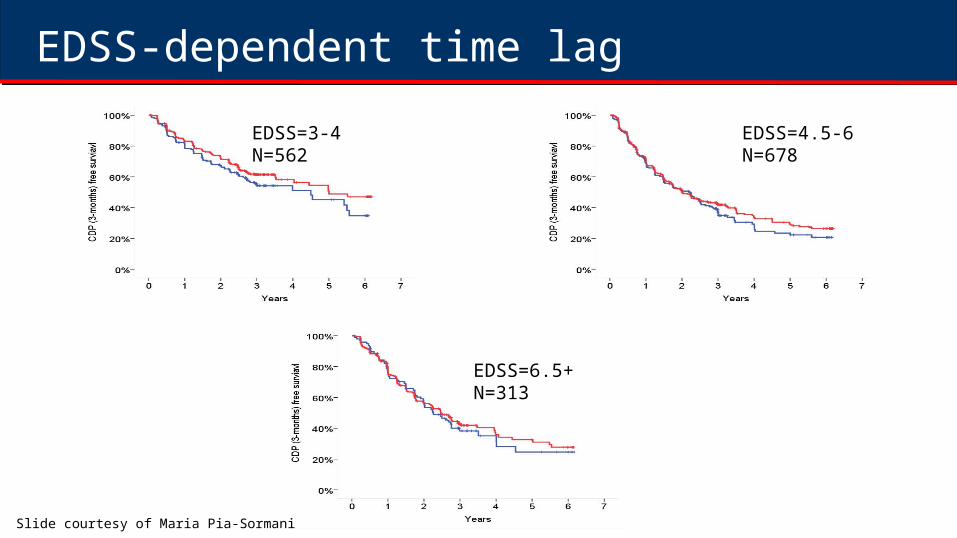
EDSS-dependent time lagEDSS=3-4N=562
EDSS=4.5-6N=678
EDSS=6.5+N=313
Slide courtesy of Maria Pia-Sormani
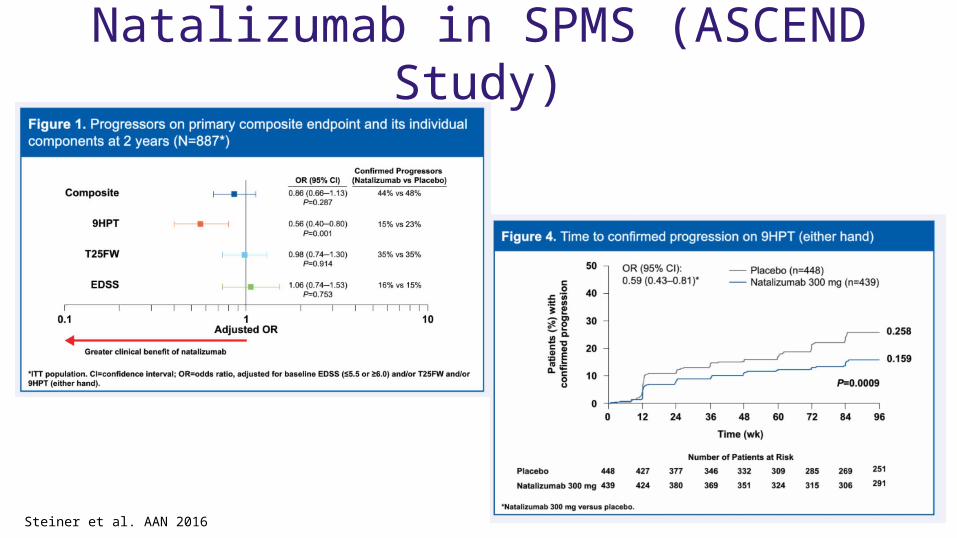
Natalizumab in SPMS (ASCEND Study)
Steiner et al. AAN 2016
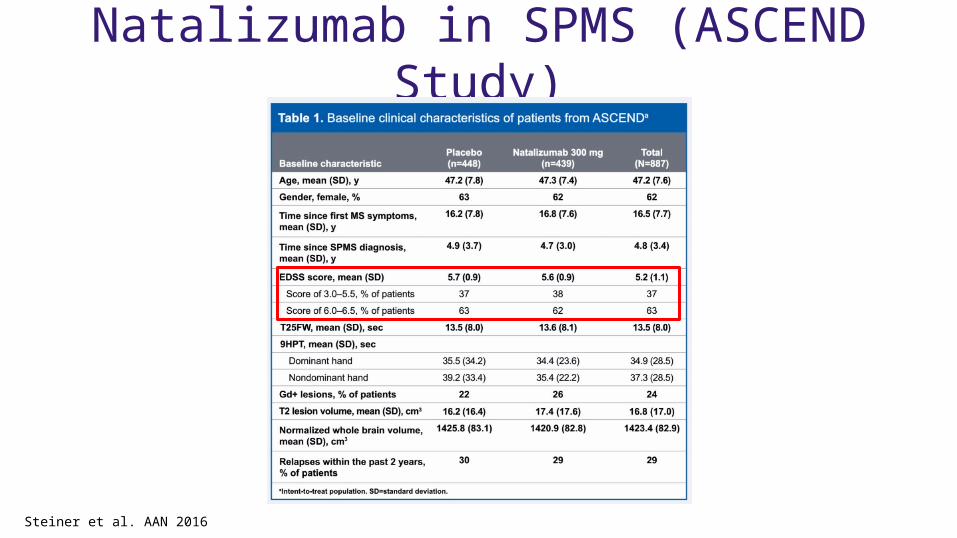
Natalizumab in SPMS (ASCEND Study)
Steiner et al. AAN 2016
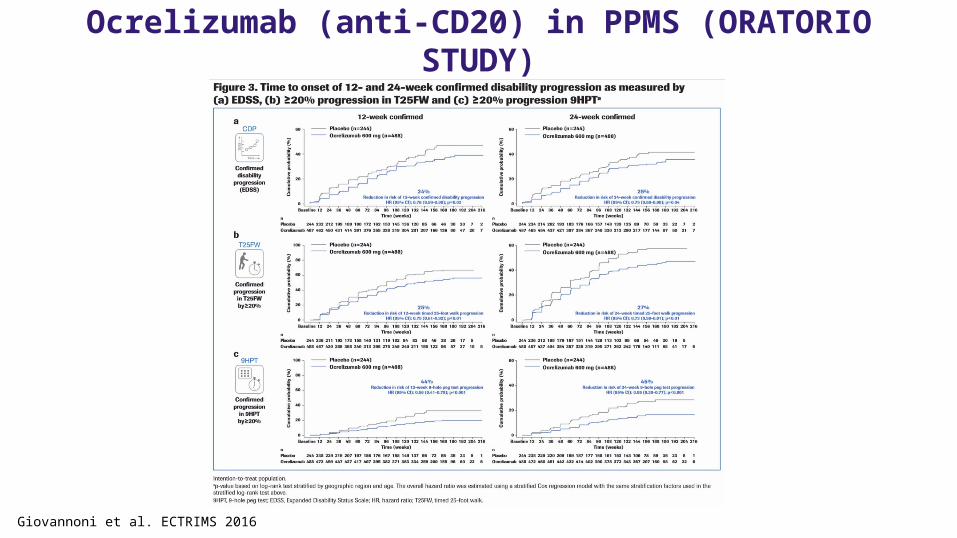
Ocrelizumab (anti-CD20) in PPMS (ORATORIO STUDY)
Giovannoni et al. ECTRIMS 2016
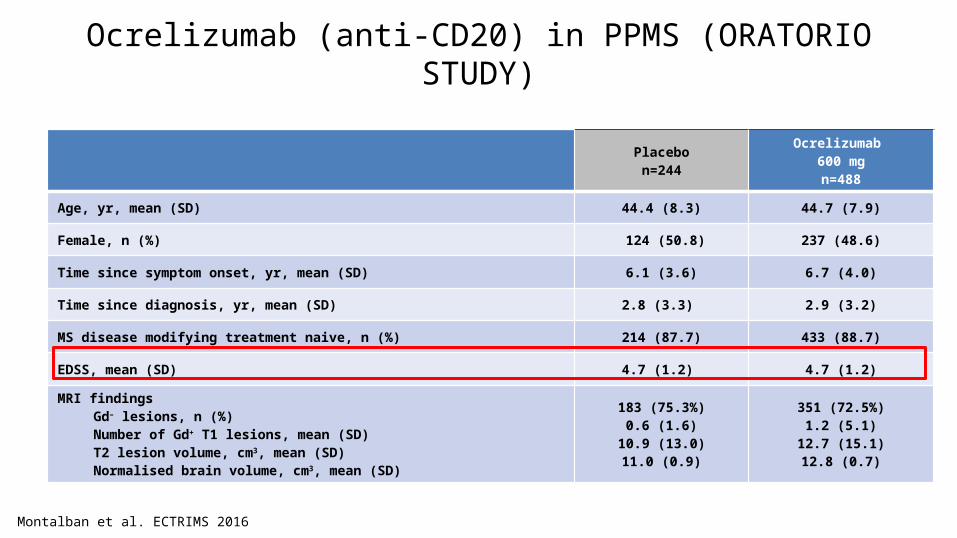
Ocrelizumab (anti-CD20) in PPMS (ORATORIO STUDY)
Montalban et al. ECTRIMS 2016
Placebon=244
Ocrelizumab 600 mgn=488
Age, yr, mean (SD) 44.4 (8.3) 44.7 (7.9)
Female, n (%) 124 (50.8) 237 (48.6)
Time since symptom onset, yr, mean (SD) 6.1 (3.6) 6.7 (4.0)
Time since diagnosis, yr, mean (SD) 2.8 (3.3) 2.9 (3.2)
MS disease modifying treatment naive, n (%) 214 (87.7) 433 (88.7)
EDSS, mean (SD) 4.7 (1.2) 4.7 (1.2)
MRI findingsGd– lesions, n (%)Number of Gd+ T1 lesions, mean (SD)T2 lesion volume, cm3, mean (SD)
Normalised brain volume, cm3, mean (SD)
183 (75.3%)0.6 (1.6)
10.9 (13.0)11.0 (0.9)
351 (72.5%)1.2 (5.1)
12.7 (15.1)12.8 (0.7)
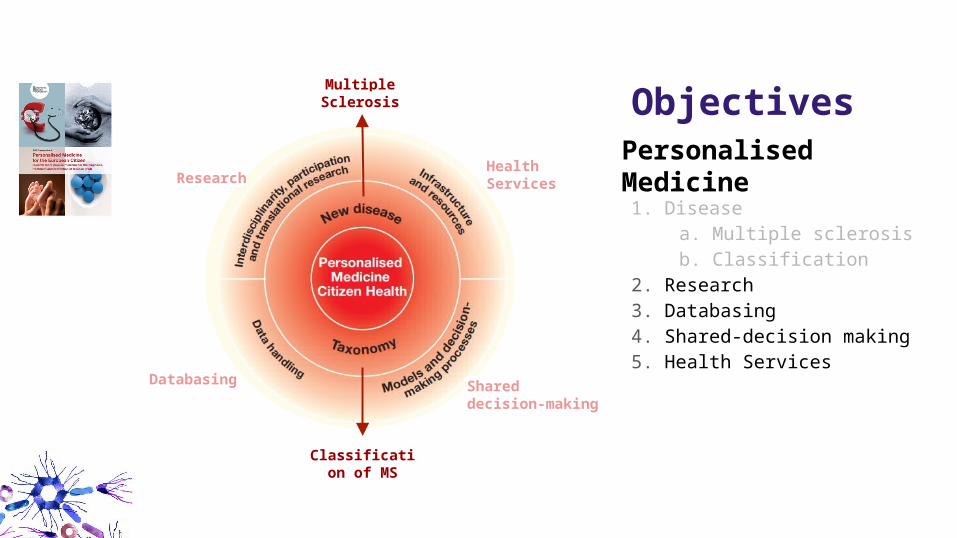
Classification of MS
Multiple Sclerosis
Shared decision-making
Health Services
Databasing
Research Personalised Medicine1. Disease
a. Multiple sclerosisb. Classification
2. Research3. Databasing4. Shared-decision making5. Health Services
Objectives
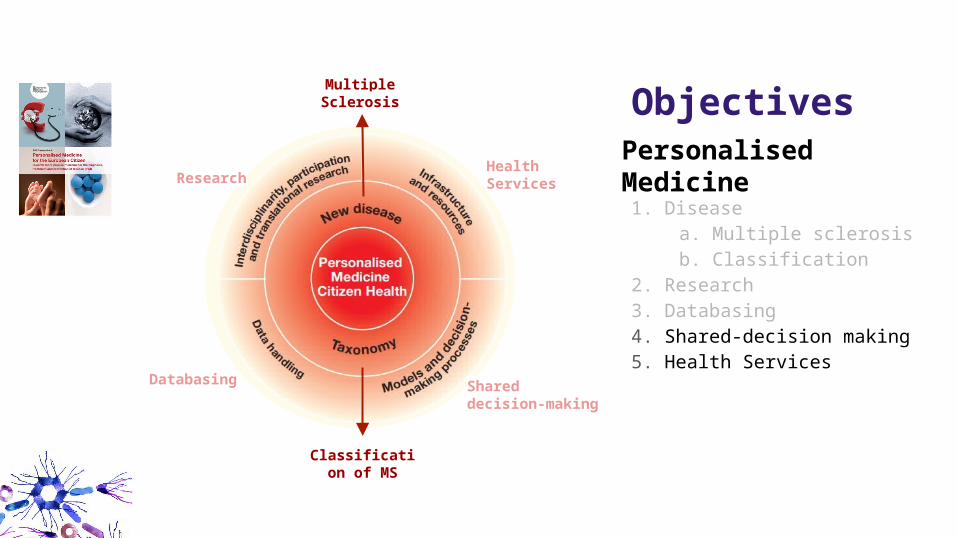
Classification of MS
Multiple Sclerosis
Shared decision-making
Health Services
Databasing
Research Personalised Medicine1. Disease
a. Multiple sclerosisb. Classification
2. Research3. Databasing4. Shared-decision making5. Health Services
Objectives
Shared decision-making

Health Services
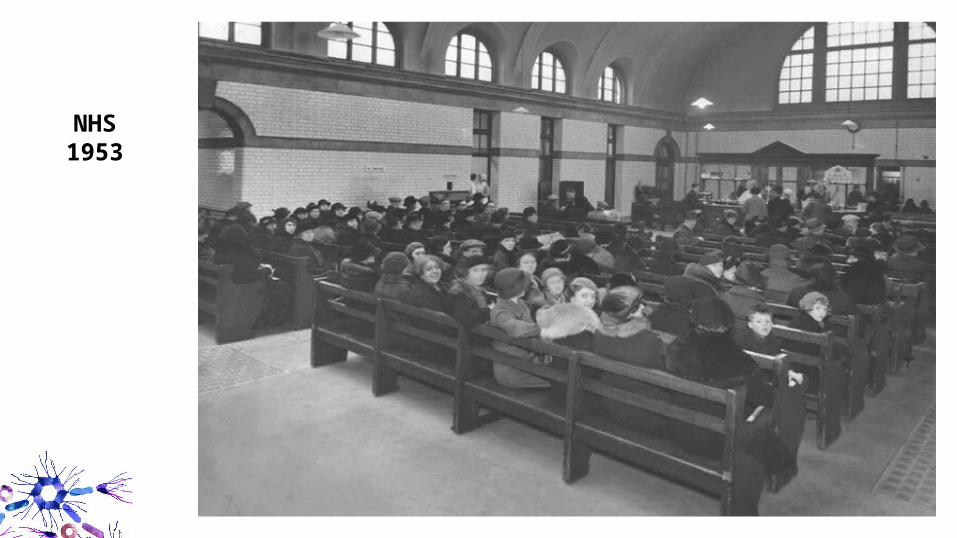
NHS1953
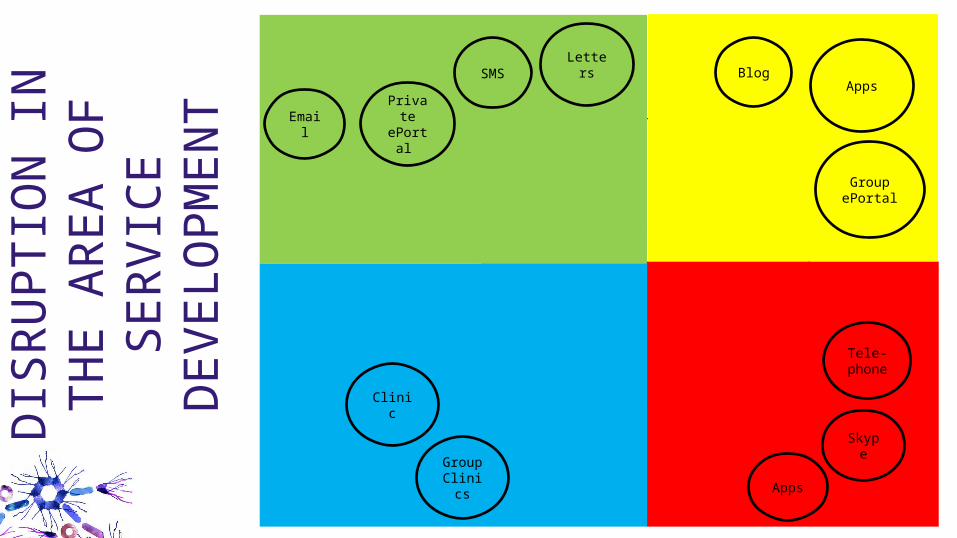
SMS
PrivateePortal
Letters
Clinic
GroupClinics
Tele-phone
Skype
Apps
Apps
GroupePortal
BlogDI
SRU
PTIO
N IN
THE
AR
EA O
F SE
RVIC
E DE
VELO
PMEN
T
Michelin Star Service
Fast-food Service
MS Brain Health – a potential ‘tripadvisor’ for MS …
msAdvisor
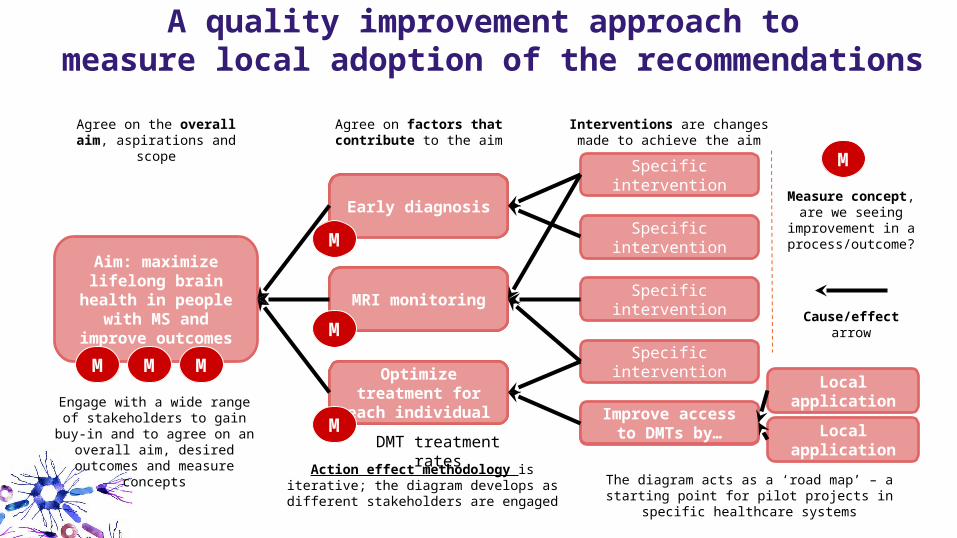
A quality improvement approach to measure local adoption of the recommendations
Example intervention
Specificintervention
Specificintervention
Specificintervention
Specificintervention
Improve accessto DMTs by…
Contributing factor
Early diagnosis
Aim: maximize lifelong brain health in
people with MS and improve outcomes
Contributing factor
MRI monitoring
Contributing factor
Optimize treatment for each individual
Action effect methodology is iterative; the diagram develops as different stakeholders are
engaged
Engage with a wide range of stakeholders to gain buy-in and to agree on an overall aim, desired outcomes and measure concepts DMT treatment rates
The diagram acts as a ‘road map’ – a starting point for pilot projects in specific healthcare systems
Local application
Agree on the overall aim, aspirations and scope
Agree on factors that contribute to the aim
Interventions are changes made to achieve the aim
Measure concept, are we seeing
improvement in a process/outcome?
Cause/effect arrow
Local application
M M M
M
M
M
M
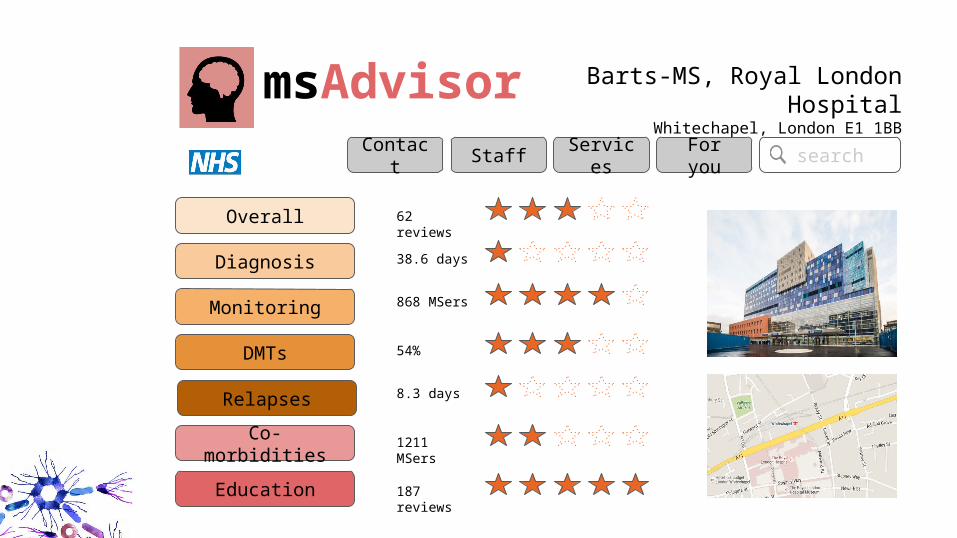
msAdvisor Barts-MS, Royal London HospitalWhitechapel, London E1 1BB
Overall
Diagnosis
Monitoring
DMTs
Co-morbidities
Education
Relapses
62 reviews
38.6 days
868 MSers
54%
8.3 days
1211 MSers
187 reviews
Contact Staff Services For you search
Conclusions
●Personalised medicine is soft construct relative to precision medicine, which is a harder construct
●Patient focused
●Theoretical construct (ESF - Personalised Medicine for the EU Citizen)
●Need we get our house in order
○ Disease definitions
○ Research & Databasing
○ Shared-decision making
○ Health Services
●Revolution in how we deliver health services to pwMS
Recommended

















