FIFTH INTERNATIONAL COURSE ON THERAPEUTIC ENDOSCOPY-
Percutaneous gastrostomy and jejunostomy:
Lessons from the first decade
_I ( )!IN :S G OFF, MI)
JS GOFF. Percutaneous gastrostomy and jejunostomy: Lessons from the first decade. Can J Gastroenterol 1992;6(3): 149-154. Percutaneous gastrostomies and jcjunostomics have inc reas ingly been used for long term cnteml feeding in patients with functioning gastrointestinal tracts but who arc unable, for a variety of reasons, to use the sranJnrd oropharyngeal route. S ince these devices can be placed without the use of genera l anesthesia, the morbidity anJ mortality generally are less than for placement of a surgical gascrosromy. A permanent gastrost0my tube is easy to manage in most patients who require prolonged tube focding. There are four basic types of percutaneous gastrostomy techniques; three employ an endoscope and one uses only rad iographic or ultrasonic guidance. All gastrostomy tubes may be convened to feeding jejunostomies if the clinical situation wmrants. Jejuna[ feeding tubes are prone to many technical problems and do not a lways solve the problems of gastric dysfunction and reflux chat make gastroscomy tubes less dcsircable. Percutaneous endoscopic gastrosromics are technically simple to perform and have become the main method for access to the gastro intestina l trace in many patients. If judiciously used, the percutaneous enterostomy offers many benefits over a nasogastric tube for long term ente ral feeding.
Key Words: Endoscopy, Gascroswmy, ]ejimostomy
Gastrostomie et jejunostomie percutanees: bilan d'une premiere decennie
RESUME: Les gastrostomies et jcjunostomies pcrcutances ont ere de plus en plus utilisces pour l'alimcntation parentcralc pro longec chez J es patients <lone les voics digestives sonc fonct ionnclles, mais qui sonr incapables pour diver cs raisons de recourir a la voic oropharyngee normale. Puisque les disposicifs peuvent CtrC installcs sans recours a l'anesthcsic gcne ra le, lcs taux de mortali tc Ct de morbiJite sont gcnc ra lement moindres quc !ors d 'une gastrostomic chirurgicale. Le tube de gastrostomie permanent est gfoeralcment facile a utiliser chez la
Uni1•<'rsi1 \' of C:ulorndu 11<.'alch >c1.:nn•.1 C<'ma ,md D<.'11wr \ ',:terans Admirnsrraticm Mt:diClcl Cenrer. Denwr. Colunulo. USA
Con es/lml(/ence mul r<!Jn-i11l.\ : Dr JS (,off, 2Ql) Norrh Uwrlcmd Trail , Fort Col/m.,. CO 80521. USA. Telt:{llionc Ull.~J .J84-l)7n
S.l IRl ,ICAl.l Y CREATED CA STRO.
st1lmie~ have hecn u,cd for over I 00 years. They prn"idc usctul and convcnienr accc~, tn the gastrtiintcs ti n al tract t1, a llow feeding and medicating patients w1rl1 a variety of problem~ that 111Tvcnr use n l thc oral route. S urg ical gastro,tomic~ have genera lly hecn placed w ith the patient under general anes1 hcsia which probably contributes to thb procedure's morbidity and mL)rtaliLy since mnst nf the p,1ticnts arc quire il l 11r debilitated (making them a higher mk group for complicmions from the general anesthesia). Minor comp I ic it iorn, tr,1m surgical gastmsto m ics range from 7 to 51 % while majLJr cnmrl ica t ions range from 7 en 71 1
){, ( I ). An cndnscopic approach co placement nf a gastm ·tomy tube under local anesthesia was first reported approximately 10 years ago (2) . W e have learned many things since the first placement nf ,1 percutaneous endoscopic gastrnsromy (PEU) . Thb technique and irs many variations have hl'cnme stamhird practice (or gast rocntcrologists, surgeons and radicilogi, b all over the world.
TECHNIQUES A lthough there arc numerous l'EC
kits on the market , there arc \\nly four ha,ic mcthL1d, [1,r placement of ,1 l'El , :
149
plupart des patients q ui rcquicrent unc a limcnta tion parcnte ra lc prolon gcc. 1l existe quatre types principaux de techniques J c gastrostomic pcrc ucancc. T ro is J'cntrc e lles supposcnt l'emploi d 'un e ndoscope ct la demicrc recourt au guiJagc raJiologiq ue ou cchographiq uc. T o us lcs tubes de gastrostomics peuvcnt etre adaptes pour l'alimcn tation pa r jcjunostomie, selon la situation clinique. Les tubes d 'alimentation je junale sont assoc ies a d i verses d ifflcultes techn iques et ne reglc nt pas coujours Les problcmes d e dysfonction gastrique ct de re flux qui rcndcnt moins favorables lcs tubes de gascrostomic. Le gastrostcomies endoscopiqucs pcrc utanccs sont s imples a executer au plan technique ct Slln t devcn ues lcs princ ipalcs voics <l'acccs a u systemc digestif chez J c nombreux patients. U tilisee jud ic ieusement , l'cntc rosto mie percutance off re plusie urs avantagcs sur la sondc nasogastriquc pour l'alime nrn tion parcnrerale prolongcc.
the P,m sky-Gnudere r or pul l technique; t he Sach:.-Vine or pu:,h -pull techniquc; th e Russell tech nique; and the tota lly nonendoscopic rad iograph ic techniqul' (3-6) (Figu re l ) . Each of these has pros and com, anJ each has a place in the proper and safe placement of a PE<., depen~ling mi the cl inica l situation.
The Plmsky-Gaudc rc r ,md the Snch~Vinc technique~ arc sim ilar. Ruth sta rt with establishi ng the s ite llt punc ture on the abdominal wall by ;i cnmbin,1-t il1n of tramilluminminn of the nhdomina l wall and observing the indention oft he gast ric lumen created by a finger pmbing the abdn minal wall (Figure 2) . T he indention uf the gast ric lumen h as become more importan t than trnn , illuminntinn hecausc many of thl' ne w ,·ideo endoscopes do nm produce enough light rn trans il luminate. O nce
the s itt' is selected , it is sterili :ed and nncschcti :cd with a lidoca inc inject ion. A skin incision is made with a scalpel fol lowed by insert ion nf a need le with a trocar (Sc ld ingc r need le ). The needle is grasped by a snare passed through the e ndoscope. O ne passes a string ( Ponsky-Gaudcrcr) ,ir a guidewi rc (Sachs-Vine) through the needle which is the n grasped by the sna re anJ pulled tiut the mouth wirh the cndosrnpe (Figure >). ln the P,1mkyG audcrer technique, thl' string (or soft wire k1op) is secured to simila r mmerial on the tapered tip of the gast rostnmy rube (G-tuhe). T h e tube is pulled re trograde th rnugh the mouth , gm,tric wall and abdominal wall (Figure 4). The nthcr end of the G- tuhc has a bumper which rests aga inst t he gastric mucosa and pulls the ~tomach inrn close proximi ty with th e abdl1mina l
Figure l ) A la1'gc vmict)' of commercial pe1-clltlmcm1s endosco/J1C g-asirnswm)' kics arc availahle, some of which are shown
wall . A nother bumper i~ slipped m·er the cxLernal port ion of the G-tuhc to , ccure the po,ili\m of the t ube with the c1 hdorninal wall. The , tiff tarcred tip 1, trimmed off the G- tubc and ,in nd,1ptor is placed on the tube so it ca n be ucc luded or arrnched to feed ing tuhe, (Figure 5). T he Sachs-Vine technique is very sim ila r except t hat the guidc\Y1re is passed th1\ 1ugh the G- tube. Th e Gtubc is then passed over t he guidewirc through the mouth and pu, hcd forward until the t ip protrudes frnm the ,,h. dnm inal wall. T he tip is grasped hy Lhc cndoscopist ,m d pulled out the rest llf t he way. The endo,copisl passes the cndo,cope back into the , t01rn1ch tn he sure the internal humpcr i,, prope r!) positioned for hoth technique,.
The Ru,sell technique is ~nmewh,n d ifferent. T he cnduscopist locates thl' , itc of placement hy the ,amc mcthl>cl. A fter t he Seklinger needle i, passed in to the stomach , a short guidewire b passed intn the gast ric lumen and the needle is removed. Tape red dilcllors arc then passed in seque nce l1,·cr the guidcwire unt il th e truct i, large ennugh l,) accept the la rge, t one which has an outer hrcaknway sheath . The final dilator is removed and a h,1 llnon tip cath eter (G-w he) is passed thro ugh the shc;:ith . T he b:1lloon is in flated with wate r nnd pulled up aga in~l t he ga,rric mucos,1. T h e hreak-away , heath is removed and ,1 hum pe r b secured LO the extcrnnl port ion lif thl' G-lllhc rn keep iL in place ;md to oppm c the gu,tric ,ind abdominal \\'alls. Finally, the endoscope is remo\'cd . Advanrnges nf thi, technique arc that the e ndoscope ha~ to he passed o nly nnce and il can he am ~izc, and th at rhc CJ- tuhe d \ll', nut hm·e lo pas~ t hrough the mouth ; thi, partic ula rly is usc(ul (or pati ents with part ia l obstruction of the oropharynx or esophagus. I c also prevents contamination of the G-lllbe with oral flora .
The rll1ncndoscopic met hnd fur placemenr of a G- tuhc als() employs the u,e of a Sc ldingcr need le to penetrate the stomach from rhc , kin , hut the stomach is localized by e ithe r s tandard rndingral'hY or ult rasound . T he ~to much ,ifrcn i~ inflated with ci ir from a nasogastric rube ,1r inge~ tiun \lf ~odium bicarbonate . O nce the ~tl)mach i,
150 CAN J G,, -;TROfNTrRl 11 Vo1 6 N,) 1 MAY/) llNr 1992
Percutaneous enterostomies
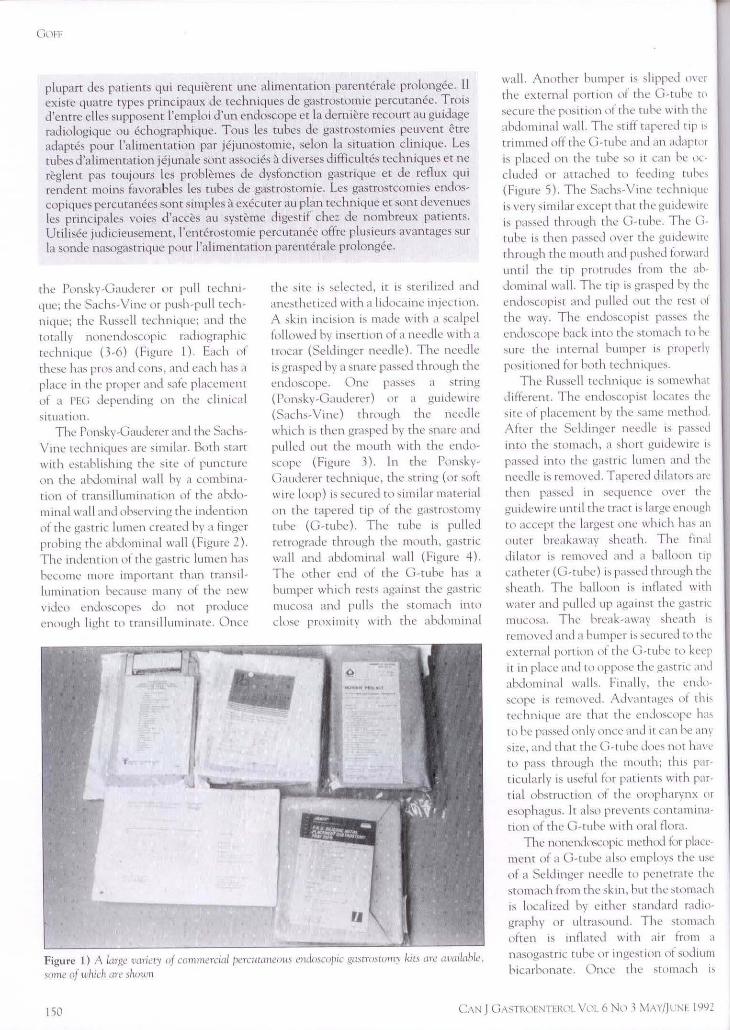
Figure 2) Tltl· f,r,q .,tl'I> m />lc1ciu.~ 11 (; •Cllhl' 1., to ,,•b 1 11 /irn{'l'> ,,r,• 011 thl' ahdomiual mill; rim" dont• I'! uh.,l•rdng ind,·1w,m of chc> ,gcl\tnC tm/1
Ir, cht! ,·,,nnr11111g Jiugcr fill· ,u, ,/10111,1 h.: ,m·,,.., from ch.: ril, m<1rg11111u.l u1•er th,• hod:; of 1/i.: ,c1111111ch
Figure 3) \fen sdl'cC111g cl1l' \IC/?, l>rl'f><1rmg ch, ,km H'ICh ,111 ,ocllll,' " '/1111011, ,nw,thl·11~111g tltt! .,km aud m,1kmg ,111 wlt·,71111rc ,kin mn ,11111 , ch, n.:dlt·" n1't'r!,·tl mro ch.: ,com,1d1 11mll•r il,recr 1·1.\/oll Tht' ,rrn1g or t1·11<· /><1."f!tl 1/m,11,gh che lll'l'tlll' i.11-.rrn1{ld tl'ith a 1,11!l'l' ,md 1n1ll.:.I 0111 the> nw11rl1
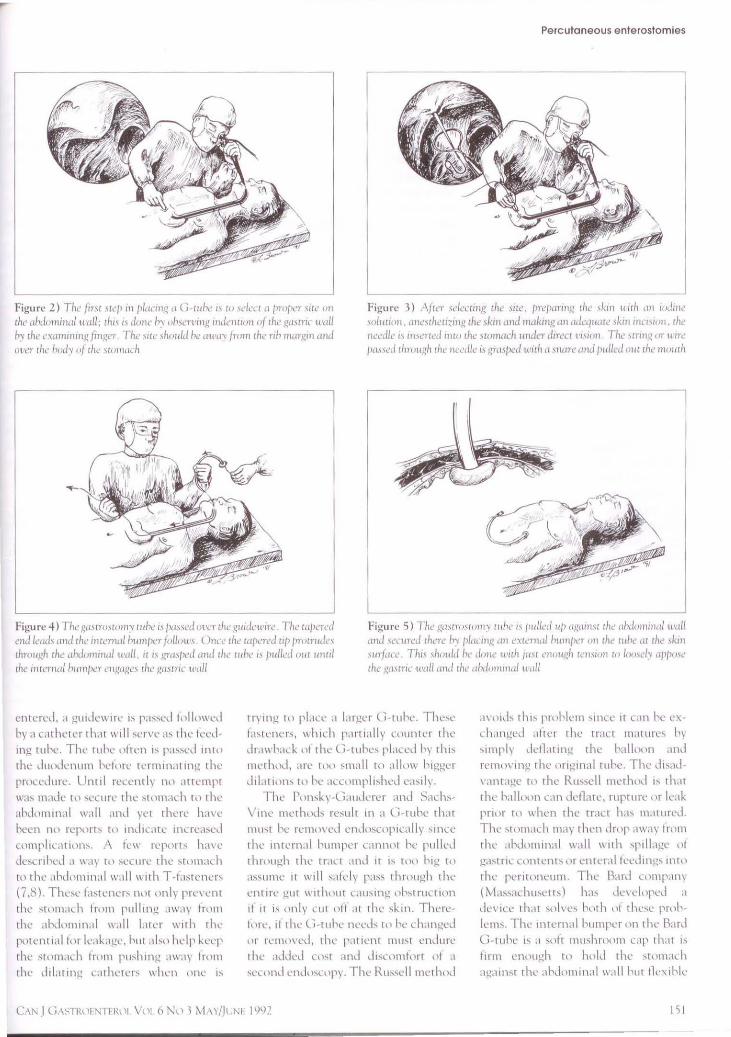
Figure 4) Tlw g11,crrncw11,• wht! i.1 {l1L",·cl ot'l'l' the 1!11ide11•,re The 111/>crl'll l'ml b11i.l 1111d ch,• ilHl'm11/ h11mp,:r /olluu·, ( )nrl r/1.: w/wrd 111, {'wrn1d,•1 chro11gh r/1e ,1hdom111al m1ll. ,r ,, wmp,:d m1tl 1he whc ,, Jmlle,l 0111 111111/
ch<! 11Hernal /,11111/><!r ,•11,gC1,gc, c/1e ,gmcric mill
Figure 5) The ga,crn,wm,• r11hl' 11 /1111/d 11/J ,c.g,un\C 1/1t! 11htlunw1c1/ 1mll ,md 1t!rnrl.'d rltcrc Ir. pl,1Cm,g ,m l'\Ccrna/ h1m1f><'r 011 ch.: wh.: ,u ch.: ,km rnrfiire Tit" ,/11111/d he dun,• 1r,r/1 /11\C l'l10t1.gh tt!u,11111 tu lornl•h• <1/>/>ml' ch<.' ga<Cric u•a/1 ,md till' 11hdu111nw/ tn1//
cntcrl'J, ,1 gu1Jew1rl' 1, p,1ssL·J 11111,,\\'l'd
hy a ult hetL'I th,11 will ~l'r\'l' a, the fcl'd
mg tuhl'. Thl' ruhl· nhen 1, pa,,l'J 1nt1>
ch..: Ju11dl'n um hcf1 ire Cl'rnl mat mg clw procedure. Unul recent!, n11 ,lltcmpt
\\'as 111.1de tl1 ,euirl' the stllmad1 r1i thL' ahdllmmal 11',il l and n·t clwrl' hm·l'
hecn nll rl'p11n, to md1L.llL' llllre,bcd
complkalllllh. A kll' rq1<11'ls ha\'l'
llcsLrJhl'<I a \\,l) t, 1 ,ecurl' the ,tllm,1d1
Ill th L' .ihdummal w.111 ll'ith T -ta,tem·r,
(7.8) Thl',L' f,Ml'lll'r, n11f 1>n lv prl'\ ent
rhc ,t1>111.1l h fnim pul l mg ,iwa) fr,1111
the ahd11111111al 11,dl l.Hl'r \\'ith tlw potl'nt 1al for b1L1gl', hut .il,u hdp keL'P
thl' ,t1>111,1Lh from pu,hmg a\\'a) fn1111
the Jd,irmg c.::athl·tcr, \\'hl'n ,111l' 1,
trymg to pl.ill' ,I l,Hgl'r (1 -tuhc. Thc,c
h,tl'm'r,, which parri;dly counter thl'
dr.m hal k uf t hl' l,-ruhc, pl.tLed h, t 111,
nwth,1d, arc t11u ,mall to .illllw h1gger
dd.1ti1111' t11 hl' .1cu11npli,hl'd easih. ThL· l\imk) (1;1u1.k·rcr and ::-.ad1,
V111l' tlll'thod, resu lt 111 a (, tube that
mu,t hl· rL'll1\l\'l'J endllsn1p1Lally ,mcl'
the llltL'rnal humpe1 L,ll111llt hl· pulled
1hn1ugh the rraLt ,lllll 1t 1, tll11 h1g tll a,.,ulllL' it will ,atL·ly pa,, thrnugh the
ent 1rc gut 11·11 hllut c1u,mg 11hsrn1L t1lln
11 It i, only cut off at the sk111. Thl're
f1,1T, 1f till' <., -tuhe 11l'l'd, r11 hL' 1.h,111gl'J
111· rc11111\'ed, t hl' p,ll 1cnt must en,lure thl' addl'J C\ht ,rnd d1su1111t,,rt 11f a
,l'u md L'nJ,1,LllP). Thl' Ru,,ell 111l't hlld
,l\'\llll, thi- prohll'm 'lllll' n Lan hl' l''
d1.111ged ,1ftl'r t hl' t rall 111,11111-c, h,
,1111ply ddl.1tmJ,! the h,1lluon ,tlld
1-emo1·111g the 111·1gmal ruh..:. Thl' d1,ad-
1·anrage tn thl' Ru"cll method h th.n the h.dluon L,m Jl'flatl', rupt1111.· or b1k
pmir ro when tlw tr.ill has maturl'd. Till' ,1,1mad1 rn.iy then drnp .1w:1) fn>1n thl' .ihdo111111al \\'all 111th ,pillage 11! ga,t rlL c11m..:nt, 111 l'ntl'ral feed mg, mt 11
t h1.· pcl'll1111l'Ulll. ThL· H.ird L<lmpam (M,1,.,.1chu,eth) h.b de,·el1>pl'd ,I
de1·1cc tha1 snll'c, hill h llf thl''l' proh
ll'm,. Tlw 111tcm,d humpL'r 1m the R.ml
U -tuhe 1, ;1 soft mushmom c.::.ip that 1,
firm en11ugh w huld thl' ,rum.11..h
agn1mr rh1.· ahd11111m,1I wall hut llcx1hk·
I 5 I

l,())f
enough tn be drawn thruugh a llghr 11rnpharyngeal or esnphageal stricture,
l,r he extracted 1hrm1gh a mature g,1,tmst nmy tract if the G-tuhe needs to
he replaced or discontinued. Mnst patient, will nut require a tuhL'
L' xchange hecause the ruhes arc m;ide llf mmcri,1ls that do nlll hreak dnwn readily and the patients are often VL' ry ill with short lik expectanc ies. 1-fowevcr,
fo r those whn me active a nd cxpecred w survive ,1 long tim<.:, the long (;, tube
pru1rud111g Imm their abdominal wall o ft en b um11.:ceptahle. Fl1r these p,nients, a butt, ,n device can he 111-
serted unce th e rrnct has matured and aft<.:r the ,tandard C-tu he is remtl\Td (9). The hutl\>ns arc flush with tlw skin ,urfoce and, d1us, ,11-e well-liked hy r,u1cnts. The buttons can c,1s il y be ex
c hanged if they malfunctiPn hy simply insert ing ,l style r tu stretch the mushmum pl1rrillt1 th,ll hnlds it in the
swmach ,111d remllv ing n . The new nn<.: 1s rL'placcd hy th<.: same technique.
A new tme-stqi huttun placement te(hnique curn:ndy is heing ev,tluated;
this t<.:chniquc U\eS the Sachs-Vine push-pull technique, bur the styler port inn nf the C-tuhe ph1cement C:ll h eter contains a hutton folded 111t11 a bre,1k
away CllC\ltll1. Once the G-tuhe is pulled out to where the internal
bumper has engaged the gastric wall, the cnn1(1n b opetlL'd and the externa l flap, llf the button ,,re Jepluyed Llnto
the abdominal wall.
JEJUNOSTOMY TUBES Some pat ients will need to he fed
inro the ~m,111 bowel hernu~c their
~ttm1achs will nor ttilcrnte cnteral fccJings (gastroparc,i,, t)U I let obstruct ion, etc) or hccau,e the patient is exper
iencing excess ive gastmesophageal reflux and thcrefnre is at high risk of
Llc\·elnping nspi ratiun l'neumon ia. 1 n these si t u:iri~ms Llll<.: c:m use a small feeding tuhc pas,cJ t hrnugh a G-ruhe which h a lready in place (percutaneous cmlnscnpic jejunostorny IPEJI) ( 10). A
well-placed jejunnstomy tube (J -t ube) can eliminate the reflu x risk and thus reduce the aspiration risk, hut thes<c ruhe, ca nnllt totally prevent aspi ration
because patients will reflu x feeding all the way hack into the ,tumach and
152
<.:sophagu.,, they will reflux and aspirate no rma l gast ri c cuntenr, (acid) nr will
aspirate ornl ~ecret inns. There arc tuhe, available thar will a llmv nne to asrirnte the gastric Clmtents while (ceding the patient thrnugh a coaxial tube that passes inw the small bowel. Jejuna! fceJing
tuhcs havL· nnt proven to he a panacea (or feed ing patients with aspiration
pniblcms. Several itwestigatnrs ( I 0, 11 )
have shown that rhe presence of a Jtuhe docs not prevent as1iirnti1)n of
en teral feedings. Abo, the J-tuhcs a rc more prone to mechanic,! fa ilure, c,pe
l ially from clogg111g due to the ir ,mallcr
dif1mctcr (ll,12). Thes<.: tuhcs will need to have further mndificat iom w clim111atc snme uf the mech,mical problems cr<.:ated by their small si:c and punr connect inn, \\'ith th e gast ril pnr-
11nn of the device.
TIPS FOR SUCCESSFUL PLACEMENT O n e of the maJllr pn1hlems with G
rube placement b the develt)pmenr nf w,1unJ infect inns. lnfccuons can he minimi:ed h) rhuroughly cleaning the
nropharynx prior to the prticcdurc and hy giv111g the patient 111tnwenuu, antih1utics (13,14). Investigators have
shuwn that the risk of wtnmd infection em he reduced by giving a first geneni
tiun cephalo~porin ,1111 ibintic incrnvenuusly immediately hcfore and se,-cral hnur~ aft<.: r th<.: pn1cedure (l \14). A
wide skin incision wil l a llow the tube w pass through mure easi ly and lessens the chances ui infection because ni less
trauma/tem,ion nn the tissues and bett<:r It ,cal drainage. One must closely fol
low the incision sicc ro look for signs nf early infection. If one can identify an infection early, ic c.111 he treated with
antibiotics alone ur, if needed, in conjunction with a small drainage incisiL,n
around the C-cuhe site. Early dctecciun and prompt treatment may prc\·ent having to perform wide drainage and
tube rem ova I. Migration nf the G-wbe's internal
humper into the gast ri c or abdnminal
wal l has hcen described ( l 5) and i~ most likely t11 11ccur with rhe device~
t hat hav<.: an internal crossbar humper
(these arc more likely to exert fllcal
pressure that wi ll lc,1d ro erosion inw
the mucosa than fl:11 nr rnushmom
bumpers). Thb migrnt1nn um he prevented hy performing a ,ccond passage uf the endoscope immediatcl)
after the G-cube has been placed to ensure the burnr cr is seated ctirrectly and can be turned easily after rhe external bumper has hcen secured. Appn,i thm nf the gastric ,md abdnm111al \\'.lib
promntcs trnct dcvclupmcnr and ma) allow earlier maturation, hut there ls nu hencfit in having t hese ,tructures
drawn tighrly wgether. The cxccrnal humrer should he 11)\lscned nr remnved afrer 10 w 14 days, cspecinll y 1( rhe patient b g;iining weigh t rapid ly. Thl' bumper needs tu he left in place longer 111 patients whti a rc sc\·erely malnl1urishcd or nn 1rnmt111thuppre~,ion
(prcdnisonc) hccausc the tract may take longer to mature and sc,11 in the,c
pat ients. Determining rhc ln(ntiun of che
stomach can he difficult in ohcsc
pariems, pat ients stall" post a partial gastrectomy, patients with thei r ,tomach high up under the rihs and when using some nf the ,·lllco endoscnp<.:s char do not proJu(c cn11t1gh light t\l
trnnsillu minarc rcl iahly the stnmm:h
and ahdrnrnnal wall. In the,c situntinn~. ulrrnsnund, computed 10111(1-grnphy and pla in films nf the ;ihdrnnL·n
may help confirm the locaunn \lf thL· ,trnmich and determine if there arc any
overlying loops ol huwel. Occn~iuna llv
che stomach c.mn\lt he reached frnm rhe sk in wi th the ne<.:dles pnwicled in
the gastrostnmy kits hccau,e they arc nnr long enough. ThL' direction nnc pa,ses a needle tnro thL' , tomach is nut
always straight 111; one ncca,kmally needs to aim ,l ightly to 1rn1dcra1ely tq'ward (wwmd the hl'ad) l1) achieve the
cnrrecc angle for entry into the gastric lumen. This can he eas ily dererm111ed
by th<.: cndnscnp1~t prior to needle insertion it he duscly nhscrvcs the finger's indcnrnri1111 nn the gastric lumen and only accept, the J irectiun nf mm when he 1s sure the finger is prn
duc111g the maximum direct effect nn
the ga,-tric lumen. Gastroparesb ucca~innally ,., seen
after gastro~tomy placement. Th" usually is caused hy plac ing the G-tube
111 the antrum rnther t han Ill thL' hod)
CAN J (iASTRUENTERl 11 VL 11 6 N L) 1 M \ )/JL;NI· 1992
nt thl' ,1umac h . The <., -t uhe shll1dJ hL' placeJ II) the hnJ y n ( the Stlll11,1L h if ill ,Iii pos-.1hlc tll .l\'(lh.l , 111) plllL'l1t 1:d pmhle1m with alte n:d gastric llHlt ilit y .111d empt y mg.
COMPLICATIONS Nunwrou, u1mpl1cat 11u1, h,l\·e hl'en
de,crihed fmm plac ing e nLL'nlstomy tube, ( 16- 19); the,e indudl' mku inn (from lnc1l w ,y,1cm11.. ), ruhl· ,1Cclu ,1nn, tuhe <.::-.t n1s11m , mcl h :mical fa ilure ,if rhc tuhl', h lc1..·J111g, .1, p1rat llll1 pneumonia, pn1..' um,iperiLoneum, leakage 1if ca,rric u1nrenh or fcedmgs inw tl 1L' perit oneum , hnwl'I oh, tnict1nn , ga,t n1-parcs i,, k :1kag1..· 111110 the ahdnmina l 11.111 and death. t\1m111 uHnpl1c.:at1o n, ,K:cur in 10 tll 20",, n( p,ll1enh, while maJnr 11111rhidi t) 1>ccur, 111 5 111 8°0. l\~ath ra 11..·, a rc ha rd 111 e ,·.i lu ,He , im_c mn,t p,1t1cnts hm·mg a !'Fl, arc \'cry ill 111d ar1..• 11fren 1..•kle rh. The rcp11rt ed ,lcath r,n e, Ju1..· Lll the pmcedur1..' ll ~l'lf consistently ,cl'lll 1,1 he ,m1und I "o.
INDICATIONS Mo,t l'Fl i, ill'l' plall'd hc1..,1U,1..' 1 he
paucnr 1, no t ahlc 1,1 mgest enough calorics hy lllllulh . T he majority o f these p,ll lL'nt, h,I\ L' ,01111..• type llf ncurolog1ca l impa irment. A nother Cllmmnn re,Nm b that thL· patient ha~ re1..Lirrcnt .1,p1rnt1on pncum11n1a caused hy a,p1 rnmm of ingested f1111d and liquid. Mech ,mical ohstruc t 111n llf rh 1..' \lrnpharynx or t'sophagus (esp1:ciall y c.mc1:rs t h:11 ,ire ~oing to he trea ted \\' ii h radi.111011 o r chemnrhe rapy) c m a l,o he :1 goud rc,Nlll for :1 gas t 1\istnmy. Pa tie nt s with urr er , m.tll ho\\e l m g,1stric.: m1tle1 obstructio m chm cannot he surg1c:1lly rd1cvcd m:iy hcne fit from dcu1mpr.:,,11m ,·1a .1 l'Fl, . The 1'1:l usu,ill ) 1, 1.:,ms1-,lt: red for patie nts with 1:xce,si,·1: ~,htmeM 1ph.1gea I rctl u, t() pre\'ent asp1rn t inn pncumlln in. A l'l:J may ab() he u~cful tl1r 1~,ll icm , with ,cvere ga, tru parcs1s.
G as trnstnm y tube., are gene rally c.1s1cr w manage than nas11gastn c.: tu hes ,md bette r toleratL'd hy the pa tie nt, hut this ~hl1ukl n ,>1 111e,111 tha t L'Vl' ryom· needing enteral nutnuon (.1nJ 11n,1hk w use the standard urnpharyngca l mute) needs a rH,. Man ) patie nt s will have transient prohlcm, that inte rfere
wnh lccdmg and can be hL'st managed h) a , ma ll cal1 hre nas\lgnstnc 1uhe. There are p,1t1en1 , who arc ex tremely ill .ind wh\l \\' ill necJ lting te rm fo1:d111g \' t,l .1 tuhc tf thl'\ , un·t\'l', hut the) should 11l1t have a !'Et, or l'EJ pl,1ced 1111111 t he ir stn tLh ,h .1 likely lung te rm M ir\ 1n1r ha, hct·n clearly c,rnbltshed . The e thic, of plali ng !'FU tuhes in pa t tl'nts wh11 cannu t p,micipatc m med1 c,1 I Gll"C dec isions need w he 1..arefull 1 um,1Lk red ,m a Las1:- hy-case hasts.
CONTRAINDICATIONS l'H ,, ,ire rd.1t1, c h u1n t ramd11.,ll1..·d
in pn11enh Wtl h known 'L'\'l' t"C gast mcs11phagl·,tl rdl u,. A l'EJ , h,1ukl he u1t1-s1dered th11ugh rctl u:-. m.iy nur he l\>ta lly prewntcd , 1..•vcn w11 h the (L·.:d-111!! t ube p l,tLcd 11·cll in t() rhe , mall bowel ( 10. 11 ). O hL·, t1 y 1s,1boa rcl:1t1 ve contrninJi1.:,1ti\ln to l'H, pl.1C1..' 111L' l1t , inc.:1..· the , tomac h tna) h1..' harder ro 1dc n11fy ,md the mt roduL1..' r needle 111
tlw l'h, k It 1, nl1t ,·er) I, mg. Orn: lllLhl he 1..a111 111u, ,1hout I'l l, ,md l'EJ pl.11..1:-1111:n ts in , lcmc ntc,l pat ient , hcLau,c
th1..·y mm pull th1..· tuhe 11u1 hct"i1rL' the trall ha, matured a nd GHN' pcrit1111itis.
Asc 1te, 11f an) amount \\' ill make rH, pl,1Lem1..·nt modl'rate ly m ky. T he st11m,tch may he difficult to locatl', rlw abtl1ty ,1t tlw st()lll,ICh to fllrm a g()od seal with 1h1..• ,1hdomina l \\'a ll can he a long, dclayul process and the re ma\ he prom111cn t \'ariCl'' 111 rhc hl1d) uf thl' stumach which cou ld hlced if they arc ina,k ertently p i1..•rc1..'d wi t h the mt roduc.:er needk. Th e mfccn on rn,k .1 lso is increased in patie nt, wit h L irrhos1, and ,hl..ltl'S.
Patient, who h ave hnd paru nl ga,tr1:uom1cs m:iy ha,'l' a PH i ,uc1.:c,,fully p l.1u·d 111 the rc,1dua l g,1,trtc p11uch . I low1:ver, t he pu uLh may he di fficult t\1
enter h1..-c.1u,1..· nt ih ... mall , 1:c o r l,1c.1-tion a hm'l' the rih marg in. The re 1, also a highern, k that a l,111p n fho\\'cl \\'di he adhe rcn1 tll rhc ga,rril remnant frn m the pril>r surgery. Occas1ona lly u ne must e nter the efferent or .1fte rent l1mh \lf a gastn>JeJLmnswmy ,1r gastroduudetwsto my d ue 1,1 the hll,ll i\ln nf the stlll11,1Ch .
Pat ient s who :ire pnmly n11 un , hcJ are ufrcn 111 need tif a rEl, to impr,1,·c tlw Ir cond 1t 1on . hut the risk nf c11m-
Percutaneous enterostomies
pl1u 1t i\lns 1..·,11cually nnn lwa li nt.: ,if 1h1: L!.t,t nistnlll\ traLt ts higher. Thi, 1s.1l,11 true ,it p:tlll't1t, \\'ho arl' 1mm11n1>u 1mprntn i,l·d .ind l',peu,11 h I hn,e nn preJn t'I 111<.:.
SURGICAL VERSUS ENDOSCOPlC
GASTROSTOMY TUBES A , urgtCal h p l.11...:J U- t11h1..· ma) h1..·
assou med wtth ,1 h igh amount of mnrhidi t) nnJ m11rta l11y (6 t\l 72"o) ,it which ,11mc may h1..' rl'L1t1..·d 11> thl' se,·crit yofthe undcrly1ngc\lnd1tilln, 111
th l'se patients ; howc,Tr, the ,llll hor ,ind othL'P, have kit chat the use ,if general ,inc,the,m muea,e, the r,11 1..· l1f c11mpltc.1t 1nn,. W hen u1mparcd pn1sp1..·v ti Vl' ly, a , urgirn l ga,tmsllltn) (Stamm
meth,id) perfnrmeJ \\' t1h 101...il am·sthe,1,1 .111J mm11nal ,cd,mon 1, cqu,11 to ,t l'H i (20-22). Hot h h,1\'e tntal wm 1~ltL,ll h>11 r,lll', ,if .1huuc 25''.,. I lo1H·,·1..·r, the l lllll' tn 111..·rfurm .1 l'Lt, 1., con, idcr.1hl) k,_..., a, 1, the Uht l''l'L'U,1lh , 111Ll' th1..• 1111niJ11Lt111n 11tl, tuhc, t h,ll Jo nnt require ;1 ,eu>11d endos1.:,ipy to 1-cmn\<.: t h 1..· tuhc tf tt ,hnu lJ f,11 1 nr nn lnngcr he needed.
REFERENCES I 1'.l.11nd JJ. l\·r,ur.m,·1111, cnd11,,,,J'IL
g.1,t r,1,t,11ll1 \111 I li,),tf11l.'Hl,·r<1J 191N :l'H. 7L~ ~ l L\
2 l,,111,krer ~tWI. Pnn,J..1 Jl .. l:.tnt RJ l i.istn"t,Hll\ 1111h<1t11 l.1p;m11nm1 A p,·r,ut.tnL'<1lls <:n,J,,...,opK ll'Lhntqu<: I l\·,l 1,1tr Surg l 9HL\ l 'i:87 2 'i
t 1'11n,k1 JL. l,.111,lcr,·r ~IWL Peru I taHl.'\llls l't1d\ls1.1 'J'll g.1,t n 1,1rnny: A 111,n11p<:r,1un· In hn1qu<: t,,r ic-l.'ding ).!,t,lf<"llllll\ (1,1Slr<11lltl.'sl l.:n,[1"L 191-il .27:9-11.
4. 11,,gan RH. [)l'l\.bru, LX', I l,1n11lwn JK, W.1lk<:r ( '(\ f'nlr,:r l)l.:. l\·ru11.1n<:nu, <:ndn,,, ,p11. g,tsl r, ist,Hlt\
T\l push 1>1 pull. A pn>,pl'clt\'L' r,111,I, 11111:,·,l 111.il l,,1,1 r<111111..·,1 [ nd11,, 1%6;12 :2511-i.
5 Russt·II TR. llr,itm,111 M, Nlln1, F. l\·rutl,llll.'< 111, g.1~ln "lnmy: \ n,•11 'illlJ'[tftl.'d ,111d Uhl•l.'lklli\e ll.'d1t11qt1c'. Am J Surg I 9H4 ; l 48· 112 -7.
(1. l l.tlkt,·r HK. ( 'h1a-S111g 11, Y,·e -\( 'N l\:r,u1.111l'llt1, kc,lmg g,1'1n,,1,1111) 11·11h
thl' '-icld1n~er 1echn1quc': RL·1·1i:w Ill 252 p.1liL'l1ls R.,dtlllng\ 1989; 171 : '59-62.
7. S.11111 S, Mudb l'R, l i,1a J. <:t al. Pere Ul,tne, 111, ga,1 n 1s1, 1111 \ 11 11 h g;1'lfl'J'e'.\ l:.xpl.'ril.'llLc' 111 I 2'i p,lltl'll t, i\ m J Rad1lll I ll9(\; I 'i4: I L1L11 6.
8. Cukman CC. C<1,,m HC,, C,,pc C. c·t al. l'cn:utancous cmcni,t,Hll ) wi th I 1. thc Cnpc ,uturc· :mclwr. Radilllt1g) ! 99l\ 174:889-9 1.
9. foutch P(,, Talhl'rt GA. Uainc, JA. S,tnll\\•,k i RA. T lw g:btm,tumy hutr\>n: A pnispcct ivc :b,l'"lllc'nl 14. ul ,afo.:ty, ,ucLe" and ,pl'ctrum nf u,l'. (i,1, t n ,in1 l'>l Enclose 1989;, 5:4 1-4.
10. K,q,hin I )S, Munhy UK, Lin,chco.:r 15. WG. Percutaneou, cnJo,cnpK JeJ11n,is1,,my: Long-term tollo\\'-lll' ,,1 21 palil'nts. Ga,trointl',t Endnsc l 989; 15:40, -6.
1 l. DiS:1r111 MA. Foutch Pl,, Sarn1w,ki 16. RA. Pnnr re,ult, wnh pl'rcutanellu, endoscopic jciuno,tomy. l,astmintc,r Endn,c 1990:,6:257-60. 17.
12. Wolt'.,l'n HC. Ko:arck RA. Ball TJ, Pnw:r,on DJ, Bowm,m VA. T uhc dy,funcl ion folh ming pl'rcuuml'ou, endo,c,,p1c g:1,rrn,1nmy ,1ml 18. jcjuno, t<1my. Ga,m1inre,t End,1,c
154
l 990; ,(i:26 1- \. jllna, SK, Nil'mnrk S, l\1mvnlkn AP. Effect ,11 an11hiotic prnphylax1, 111
pcrc· ur.111l'<H1, cncl<1,cnpil ga,t ni,wmy. A 1\1 J G,hl n1entcrnl l 98'i;8(H 18-4 ,. Wa1; A. M1,kt,wn: P. The dlirney tif prnphylact1c ant1h1t111cs 111
,,ercuwncm1, gn,tn isu 1my. G,i,t rnintl',t EndllsC ! 987;11: l6'i. Fkhrle KM, Dc•ktw1ch AA. Amm,,n HV. Spontanl'<l\1' tube extrusion followmg pl'rc111 :ml'ou, cndn,cnp1c gast rn,t, m1y. C a, t roi nte>t EndllsL 1989; 15:'>6-8. Shcllit,1 PC, M:1lt RA. Tubt: g;lstro,1<m1y. Tedinique, and compli..:alinns. Ann S urg 1985;204: 180-5. l )1tc,he1m JA, Richard, W. Sharp K. Fm al and ,lisa,tnn1, c,,mpl iut1 1t in,
t, 111, m·1 11g pcrcut,me, 1us l'ml, lSC< 1pi..: g,1,lrl>Sl<llll\. Am Surg 1989;55:92-6. Lm,m DE, Burton DD, Schrnl',ler KW. D11'fagm> EP. Percutane<1us
endosu1p1, g,1slrt1'llll\1y. lnd1c.H11>n,, sue cc•,.,, ..:, impliL,11 i,,n,, .111d 111<1rtal11y 111 114 u ,n,l'c'ut1,·c p:11 icn I\. l,,1s1 n >l'lllcr, ,I, >g\ 19H7;9M8-'i2.
19. K1rhy [)F, Craig RM. T,,mu T-K. PllHn1ck Bl I. Pnu1tanL·ous o.:ndo,cop1, g,t,tin:,wm1es: A prosp<'Cl il'l' l'\'alual 1,\\1 and revicw of thl' l11cra1urc. J l'arc•ntc'r Enter,1l Nutri 1986;10:155-9.
20. Shellito PC. M:dt RA. Tuh,· ga,rn,stomv. Technique, and c,,mplicat1<ln,. Ann Surg 1985;201:180-5.
21. Gram JP. C,,mpan",n ,ii per..:ul:1ne,H1s end, ,scnp1c g:i-tn >sl<H111 with S1amm g:1srnisr,11n\. Ann Surg I 981U07:598-60,.
22. S1iegm,mn GV. Gt>ffJS. Si l.1, L). Pl',1rlm~n N, Sun J, N,1rt"n L EndtlSCOp1c versus oper.1l 11"e gasrn,,tnmy: Final result,,,( ,1 prnspc'Cl i 1·e rn ml, 1m 1:cd l n a I. Cim,1ro111tc.,l End,,sc 1990;16:l -'i .
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com
Recommended