PAUL ALLYN, MDAFRICAN AMERICAN HIV
UNIVERSITYUNIVERSITY OF CALIFORNIA LOS
ANGELESAUGUST 28, 2014
THE NATURAL HISTORY OF UNTREATED HIV-1
INFECTION
OBJECTIVESTo illustrate the natural progression of untreated
HIV-1To highlight common clinical manifestations of
HIV during this progressionTo discuss exceptions to this overall trend
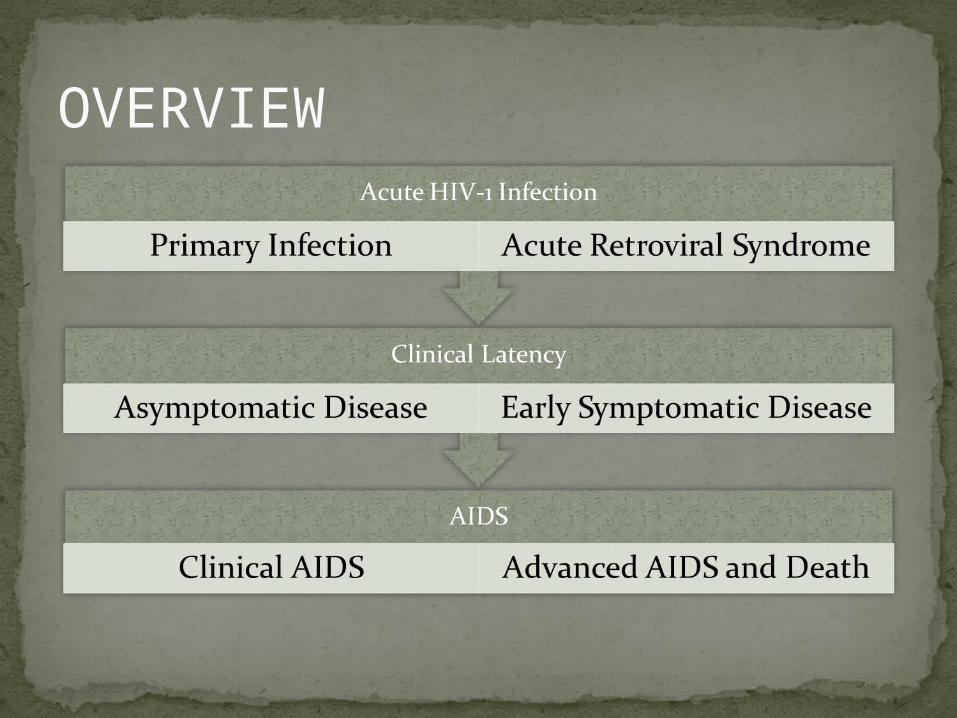
OVERVIEW
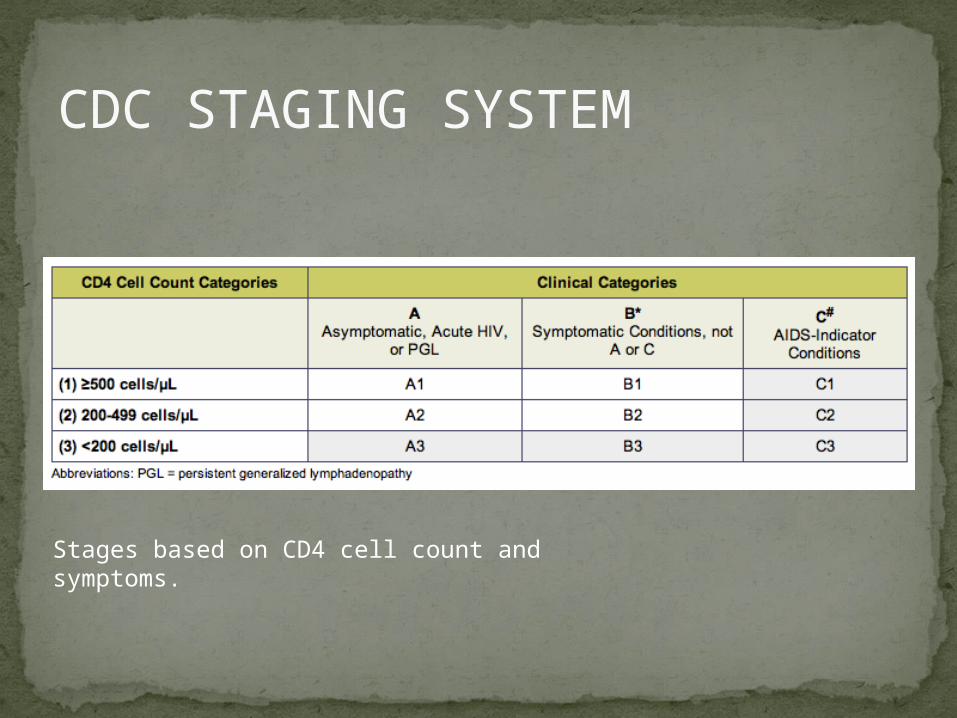
CDC STAGING SYSTEM
Stages based on CD4 cell count and symptoms.
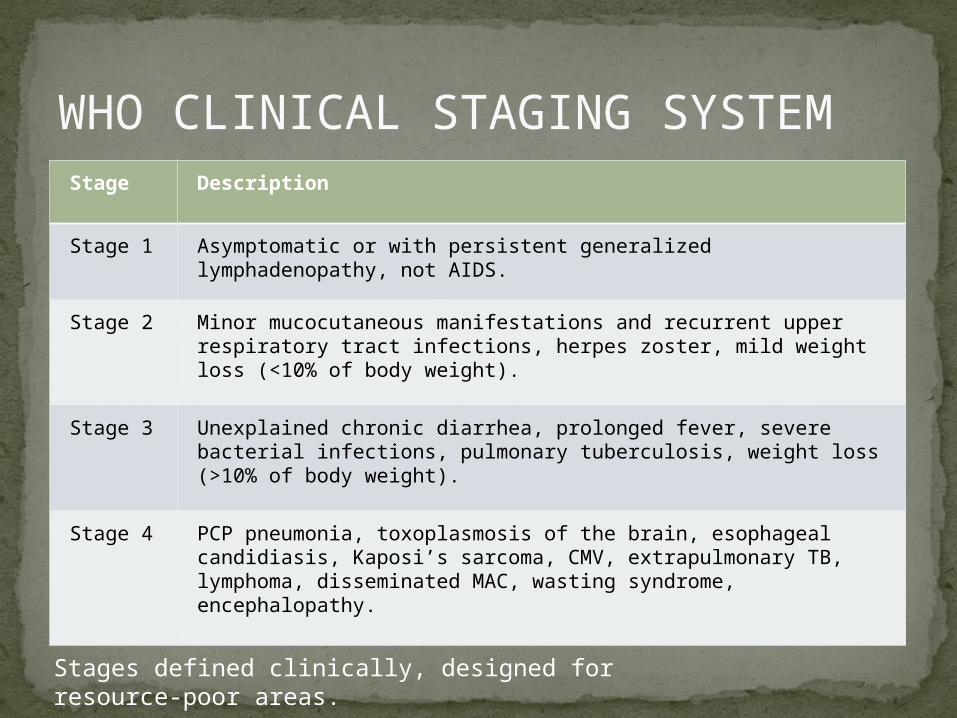
WHO CLINICAL STAGING SYSTEMStage Description
Stage 1 Asymptomatic or with persistent generalized lymphadenopathy, not AIDS.
Stage 2 Minor mucocutaneous manifestations and recurrent upper respiratory tract infections, herpes zoster, mild weight loss (<10% of body weight).
Stage 3 Unexplained chronic diarrhea, prolonged fever, severe bacterial infections, pulmonary tuberculosis, weight loss (>10% of body weight).
Stage 4 PCP pneumonia, toxoplasmosis of the brain, esophageal candidiasis, Kaposi’s sarcoma, CMV, extrapulmonary TB, lymphoma, disseminated MAC, wasting syndrome, encephalopathy.
Stages defined clinically, designed for resource-poor areas.
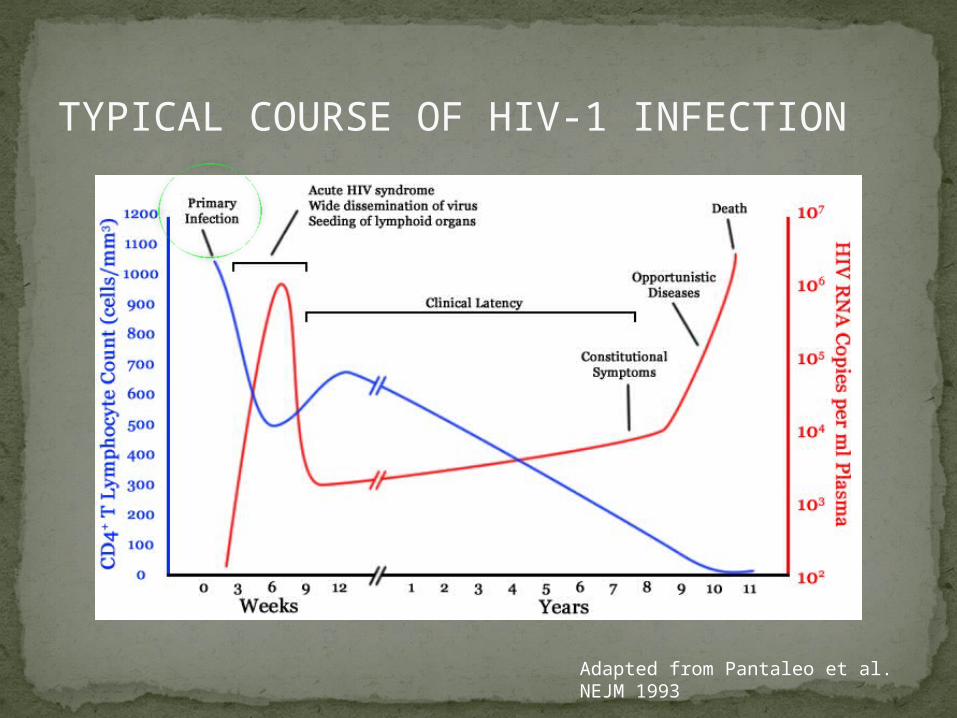
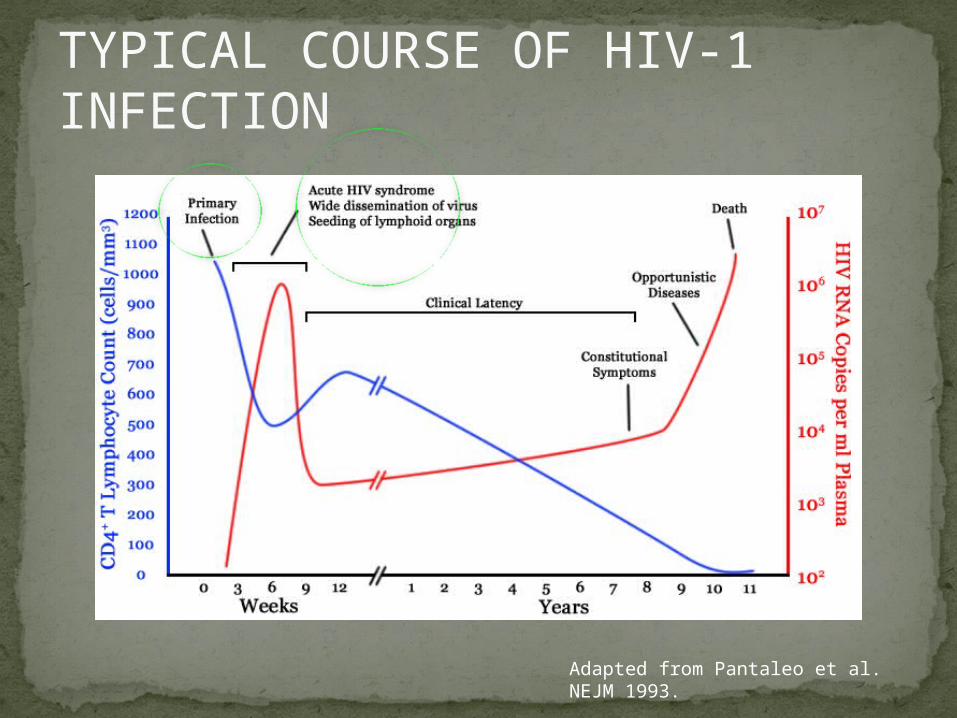
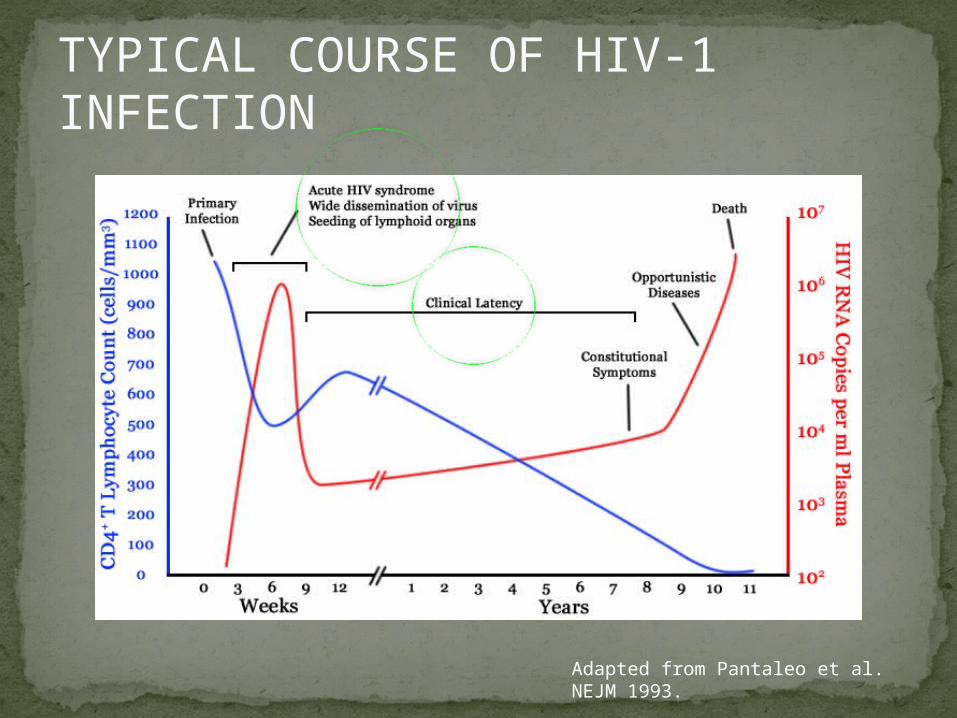
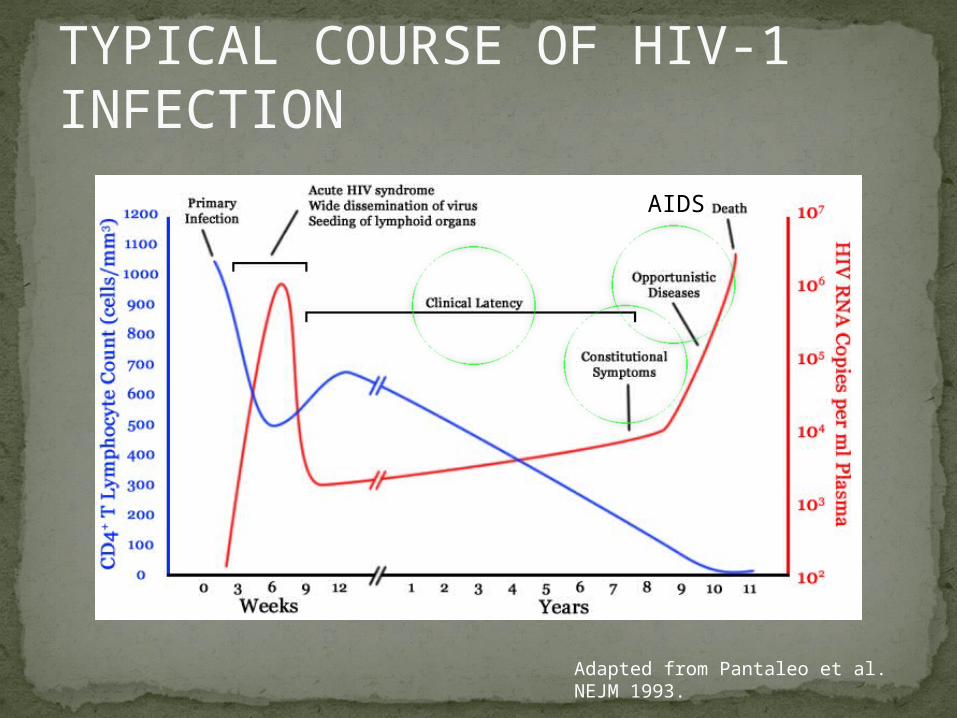
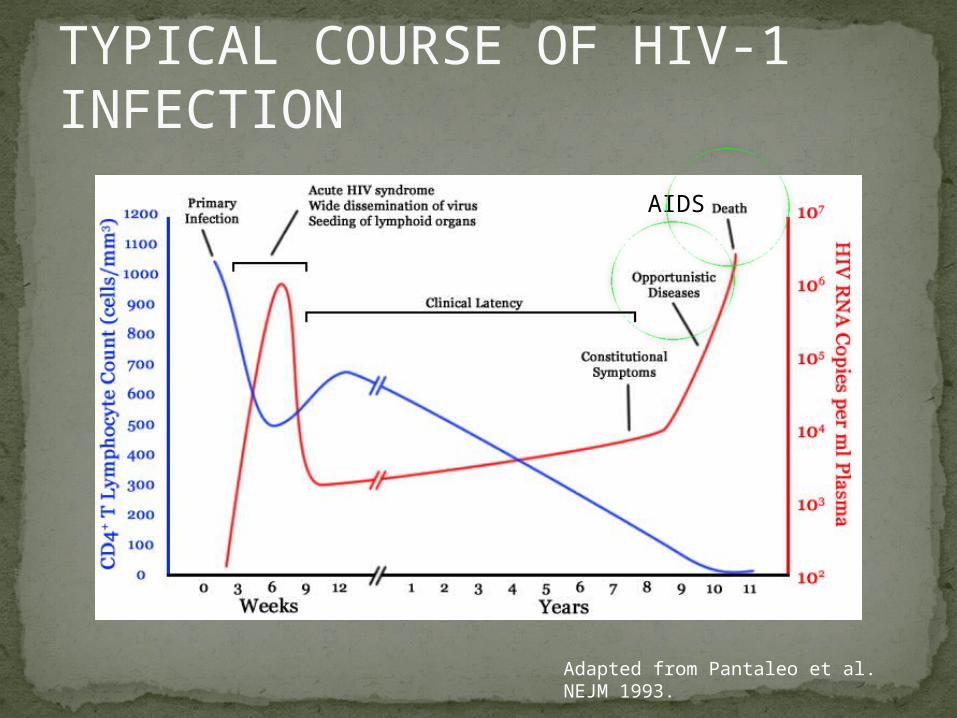
TYPICAL COURSE OF HIV-1 INFECTION
Adapted from Pantaleo et al. NEJM 1993
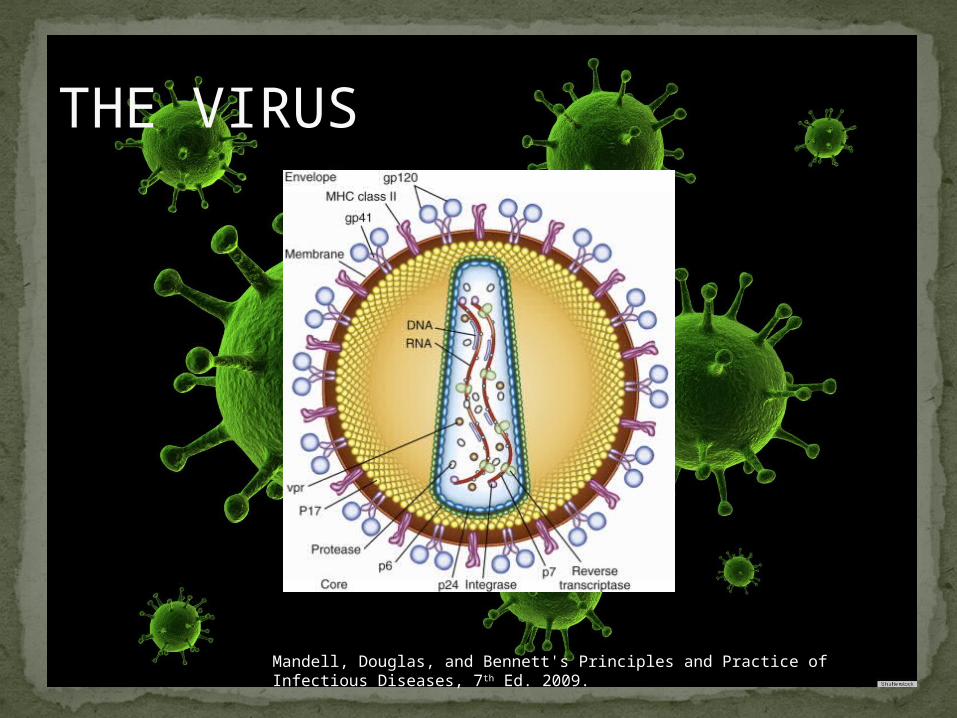
THE VIRUS
Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 7th Ed. 2009.
TRANSMISSION
PRIMARY HIV INFECTIONTimeframe: 0 weeks (immediately after
transmission)Characterized by:
High viral load (high concentration of HIV RNA in the blood)
Declining CD4+ lymphocyte count (average about 1000 cells/mm3 prior to infection)
Initially asymptomatic
TYPICAL COURSE OF HIV-1 INFECTION
Adapted from Pantaleo et al. NEJM 1993.
ACUTE RETROVIRAL SYNDROMETimeframe: 1-6 weeks after exposure
(peaks at 3 weeks)High viral load, low CD4 countMononucleosis-like illness in 1/2 -2/3 of
patientsSymptoms typically resolve within 10-15
daysUp to 50% patients asymptomatic
Symptoms variable in those who have them:Fever (96%)Enlarged lymph nodes (74%)Sore throat/Pharyngitis (70%)Rash (70%)Muscle or joint aches (54%)Low blood counts, platelets, and white cells (45%,
38%)Diarrhea (32%)Headache (32%) Nausea/Vomiting (27%)Hair loss (alopecia)Mood changes (depression, irritability)
Data from Niu MT et al. JID 1993.
ACUTE RETROVIRAL SYNDROME
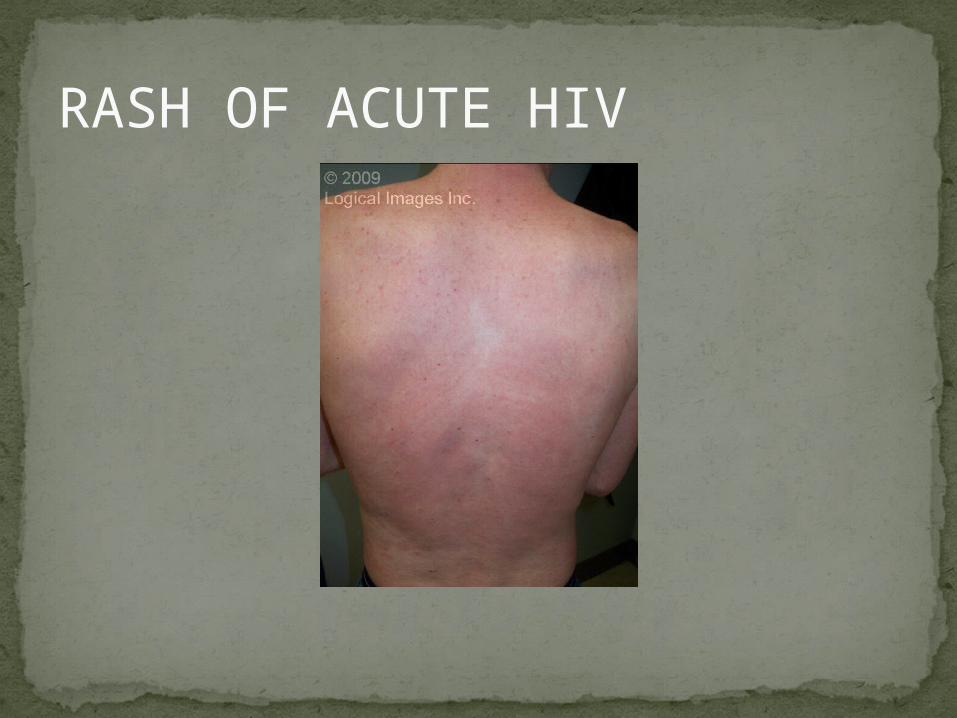
RASH OF ACUTE HIV
TYPICAL COURSE OF HIV-1 INFECTION
Adapted from Pantaleo et al. NEJM 1993.
CLINICAL LATENCY (ASYMPTOMATIC INFECTION) After acute infection, most patients remain asymptomatic
for years Immune system develops antibodies to suppress the virus and
the viral load stabilizes (viral set point) Over time, there is typically a gradual decline in CD4+
lymphocytes (on average 50-75 cells per year) Median time from infection to development of AIDS is
approximately 8-10 years Some may develop AIDS in <5 years (approximately 20%) Few will remain asymptomatic without evidence of
immunosuppression for more than 10 years (<5%) Many factors impact prognosis, but HIV-1 RNA levels
(viral load) combined with CD4+ cell counts are the best predictor of disease progression to AIDS and death from AIDS
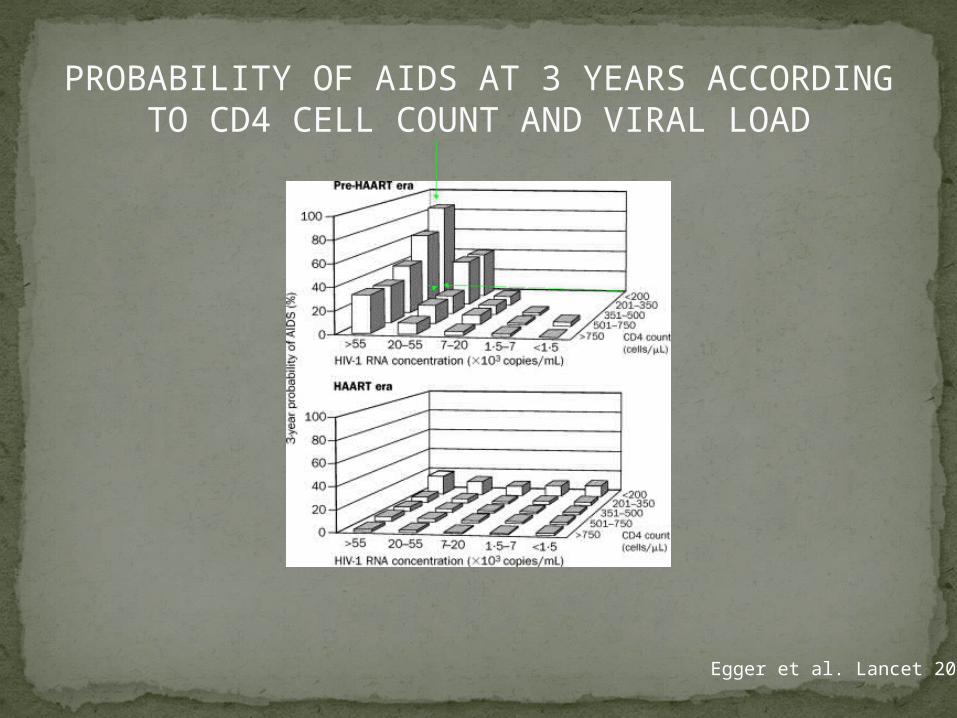
PROBABILITY OF AIDS AT 3 YEARS ACCORDING TO CD4 CELL COUNT AND
VIRAL LOAD
Egger et al. Lancet 2002.
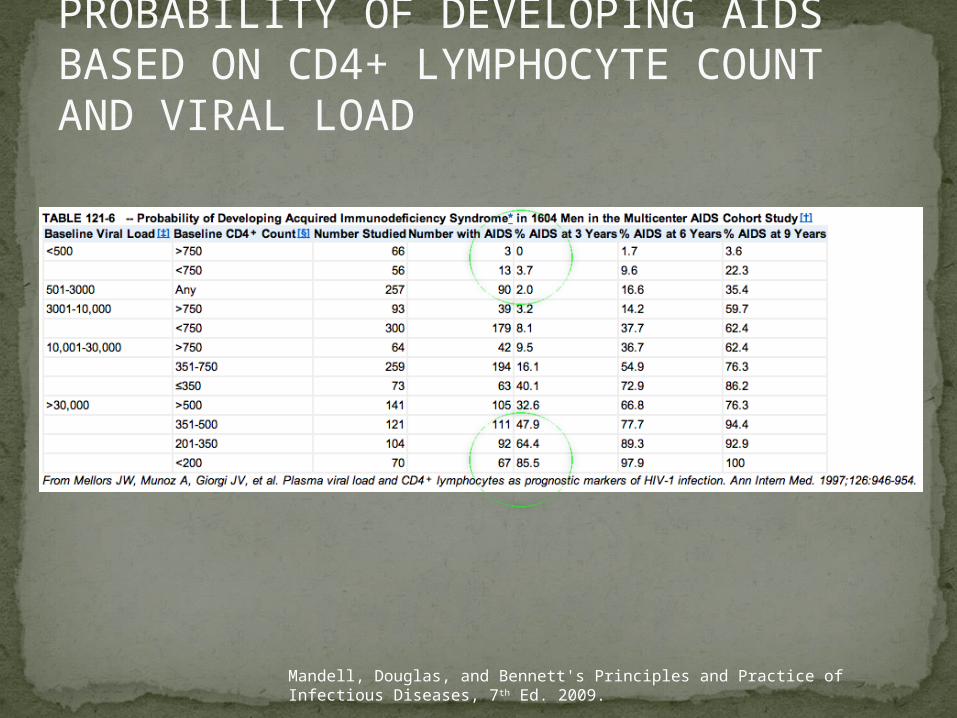
PROBABILITY OF DEVELOPING AIDS BASED ON CD4+ LYMPHOCYTE COUNT AND VIRAL LOAD
Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 7th Ed. 2009.
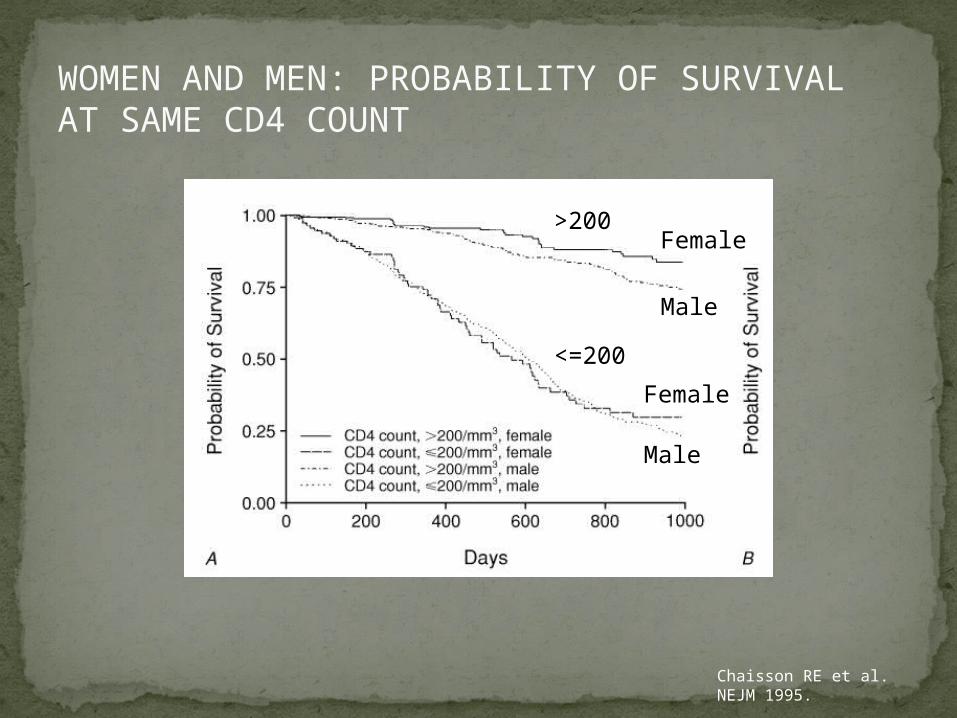
WOMEN AND MEN: PROBABILITY OF SURVIVAL AT SAME CD4 COUNT
Chaisson RE et al. NEJM 1995.
>200
<=200
Female
Male
Female
Male
DOES EVERYONE DEVELOP AIDS IF LEFT UNTREATED?
SPECIAL CIRCUMSTANCESLong-term nonprogressors:
Remain asymptomatic without treatment or evidence of immunologic decline for many years
2 Groups: 1. Those with detectable viral load but adequate
CD4+ cells to protect them from opportunistic disease (though these gradually decline over time)
2. Elite Controllers: Small group, have undetectable viral loads and
maintain normal CD4+ lymphocyte countsAble to contain viral replication
CLINICAL MANIFESTATIONS BY CD4 COUNT
CD4+ COUNT >500Patients with CD4+ counts > 500 generally
asymptomaticMay have mild or moderate lymphadenopathy
(persistent generalized lymphadenopathy)Recurrent herpes infections may be present as
wellMay have exacerbation of skin conditions:
PsoriasisEosinophilic folliculitisAphthous ulcersHairy Leukoplakia (benign white plaques on tongue)
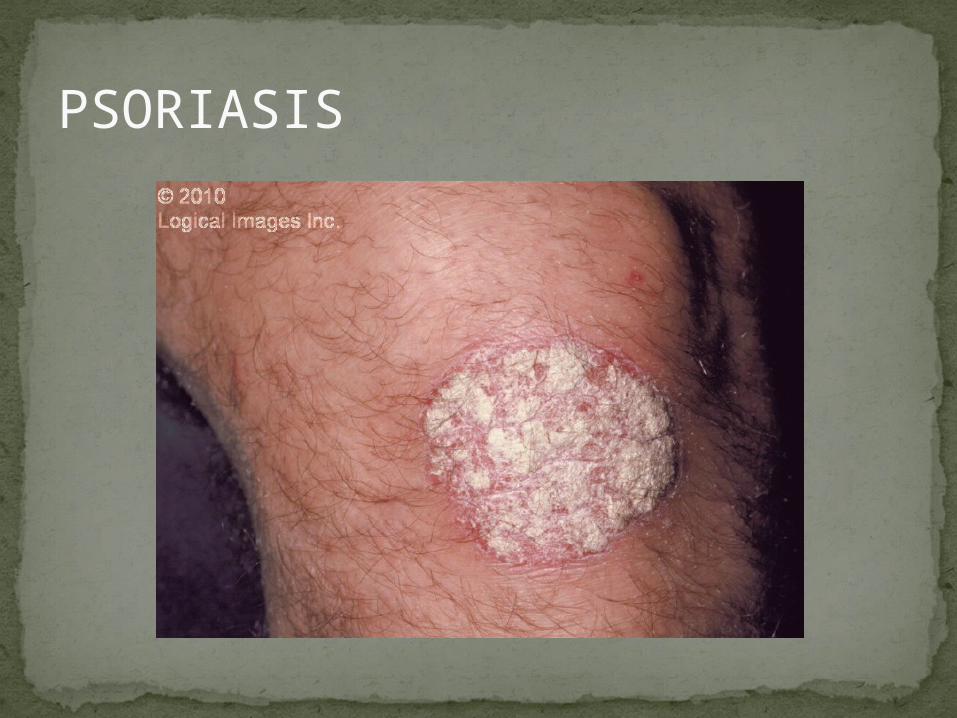
PSORIASIS
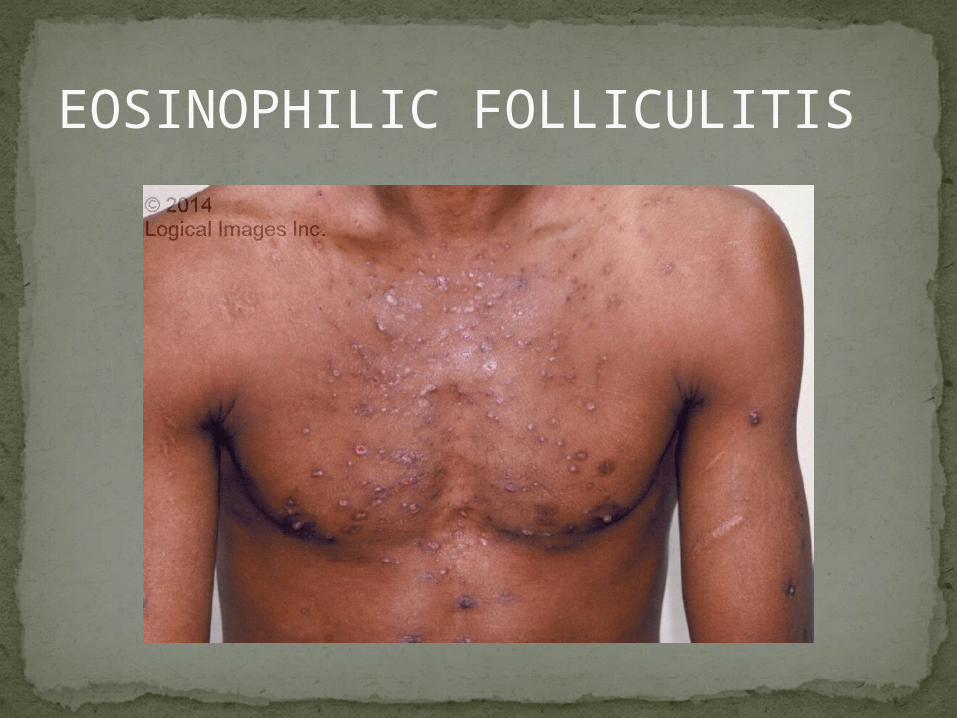
EOSINOPHILIC FOLLICULITIS
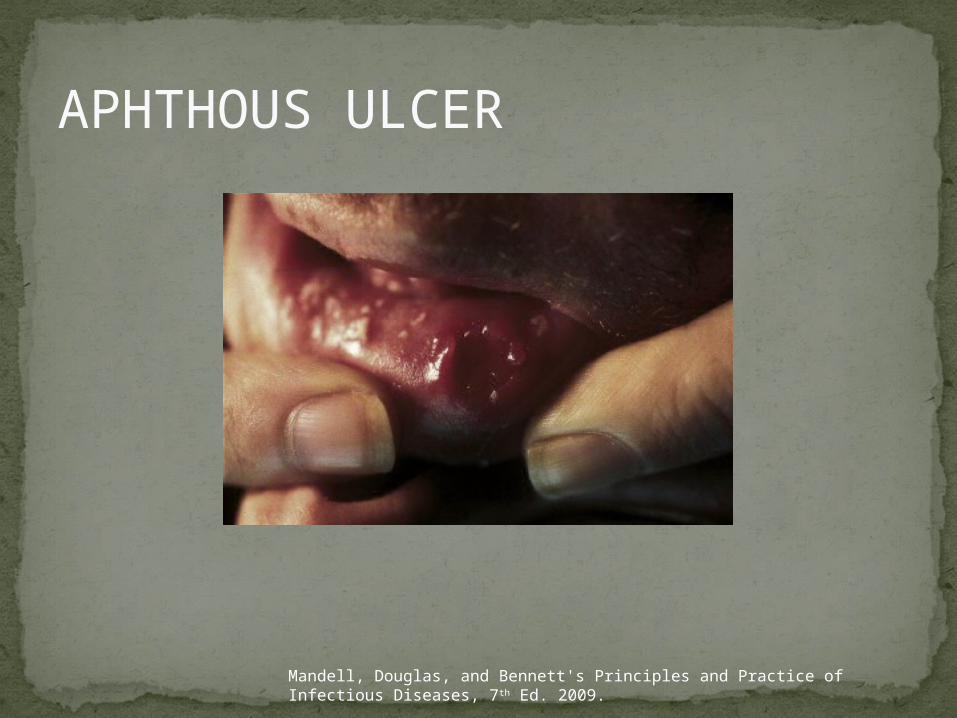
APHTHOUS ULCER
Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 7th Ed. 2009.

ORAL HAIRY LEUKOPLAKIA

CD4+ COUNT 200-500Most patients with CD4+ counts between 200 and
500 cells remain asymptomatic or have mild disease. May have:Worsening of chronic skin conditionsRecurrent herpes simplex or varicella-zoster virus
(shingles)Vaginal or oropharyngeal candidiasis (thrush)Recurrent diarrhea Intermittent feverWeight lossMuscle aches, joint aches, headache, and fatigue
commonly reportedCommon to have bacterial sinusitis, bronchitis,
pneumonia
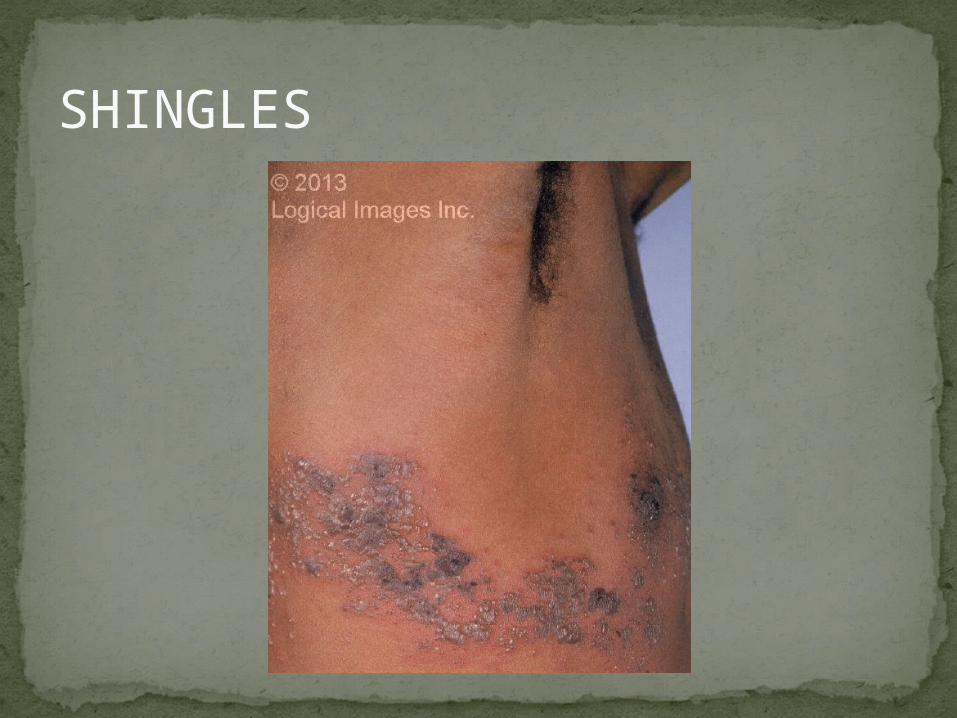
SHINGLES
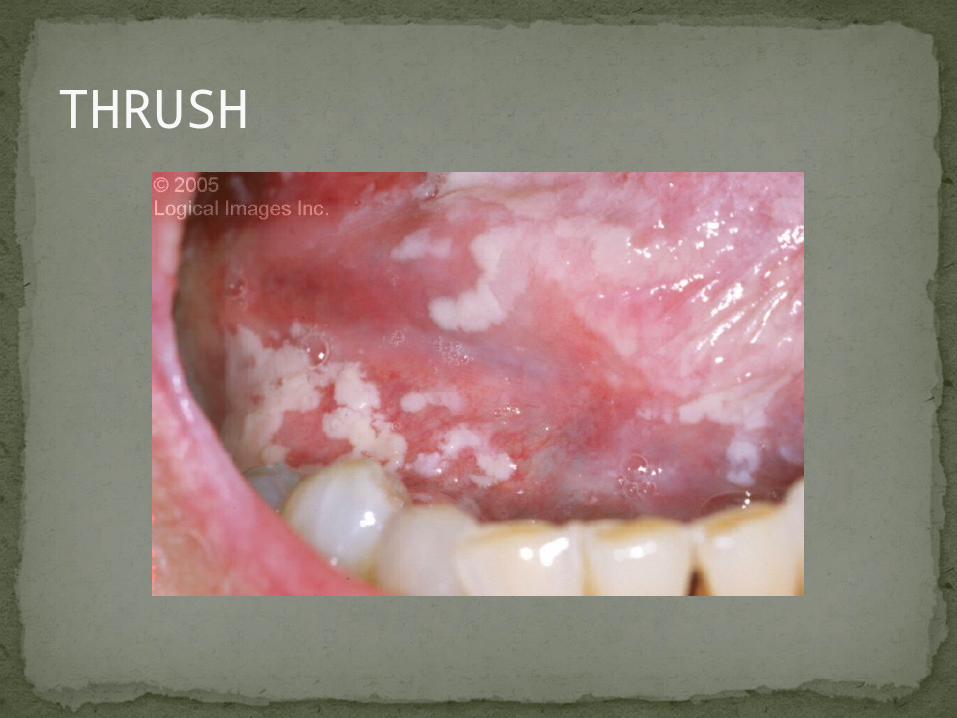
THRUSH
TYPICAL COURSE OF HIV-1 INFECTION
Adapted from Pantaleo et al. NEJM 1993.
AIDS
AIDSPatients with CD4+ Cells <200 are classified as
having AIDS by 1993 CDC definitionCertain opportunistic infections seen at this stage
are indicative of AIDS, including: Pneumocystis carinii (jirovecii) pneumonia (PCP) Toxoplasmosis Cryptosporidiosis Esophageal candidiasis Tuberculosis
Increased risk of certain cancers: Invasive cervical cancer in women Rectal or anal carcinoma in men
Hematologic abnormalities (ITP, anemia, neutropenia)
HIV-associated nephropathy (kidney disease)
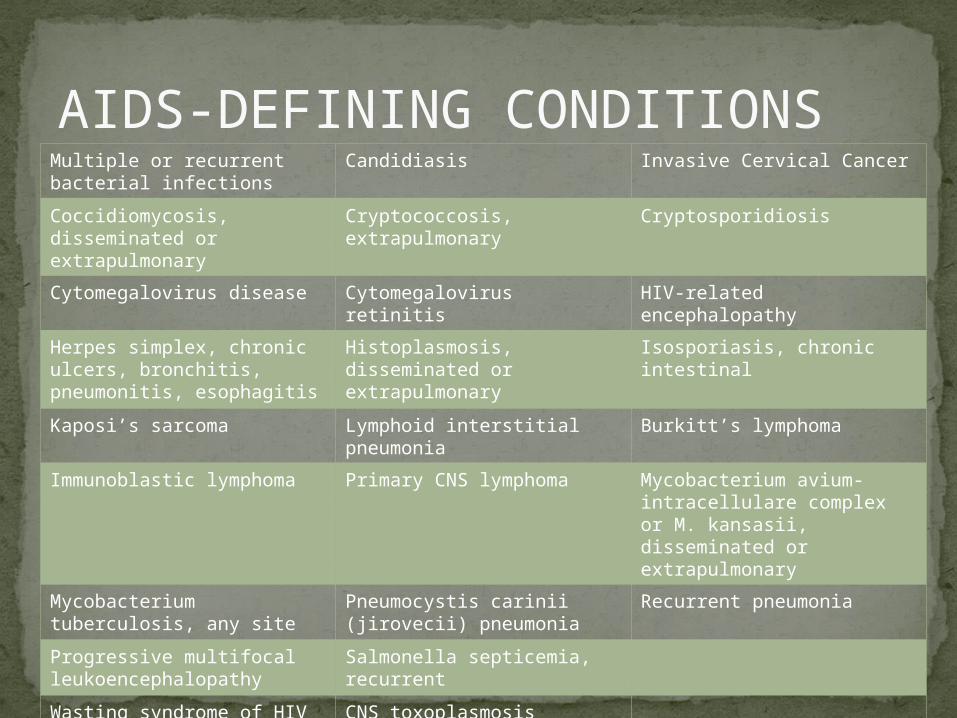
AIDS-DEFINING CONDITIONS
Multiple or recurrent bacterial infections
Candidiasis Invasive Cervical Cancer
Coccidiomycosis, disseminated or extrapulmonary
Cryptococcosis, extrapulmonary
Cryptosporidiosis
Cytomegalovirus disease Cytomegalovirus retinitis HIV-related encephalopathy
Herpes simplex, chronic ulcers, bronchitis, pneumonitis, esophagitis
Histoplasmosis, disseminated or extrapulmonary
Isosporiasis, chronic intestinal
Kaposi’s sarcoma Lymphoid interstitial pneumonia
Burkitt’s lymphoma
Immunoblastic lymphoma Primary CNS lymphoma Mycobacterium avium-intracellulare complex or M. kansasii, disseminated or extrapulmonary
Mycobacterium tuberculosis, any site
Pneumocystis carinii (jirovecii) pneumonia
Recurrent pneumonia
Progressive multifocal leukoencephalopathy
Salmonella septicemia, recurrent
Wasting syndrome of HIV infection
CNS toxoplasmosis
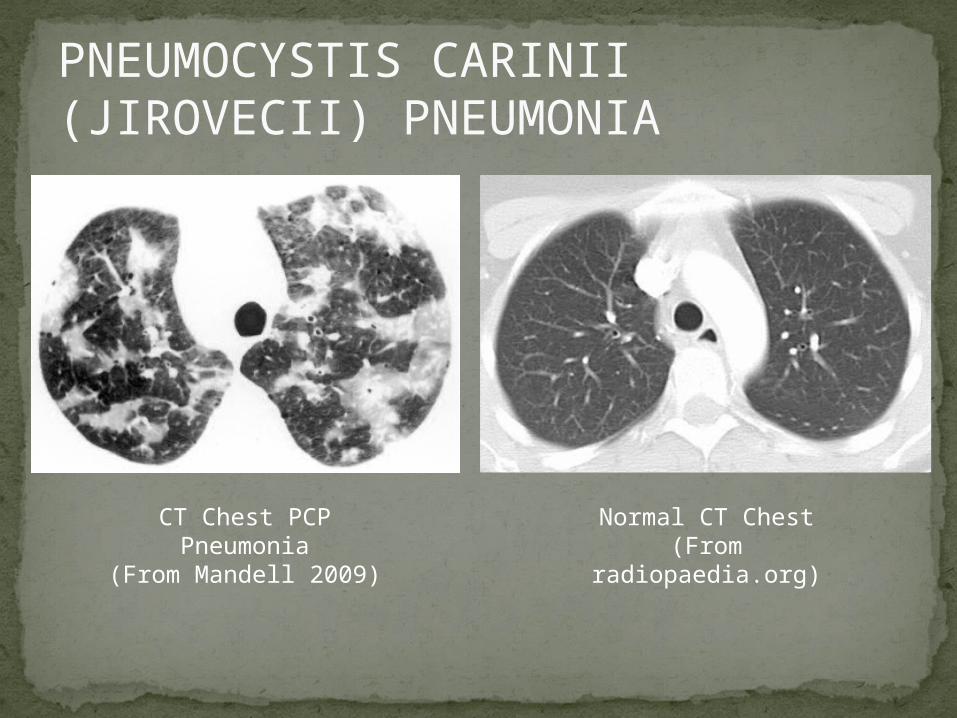
PNEUMOCYSTIS CARINII (JIROVECII) PNEUMONIA
CT Chest PCP Pneumonia
(From Mandell 2009)
Normal CT Chest(From radiopaedia.org)
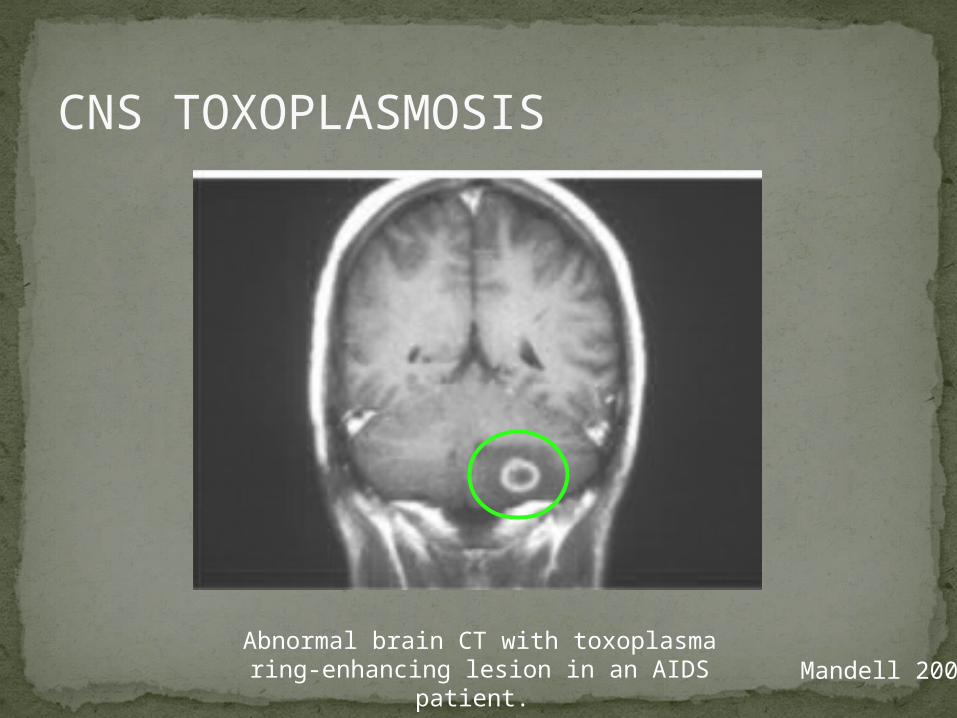
CNS TOXOPLASMOSIS
Mandell 2009Abnormal brain CT with toxoplasma
ring-enhancing lesion in an AIDS patient.
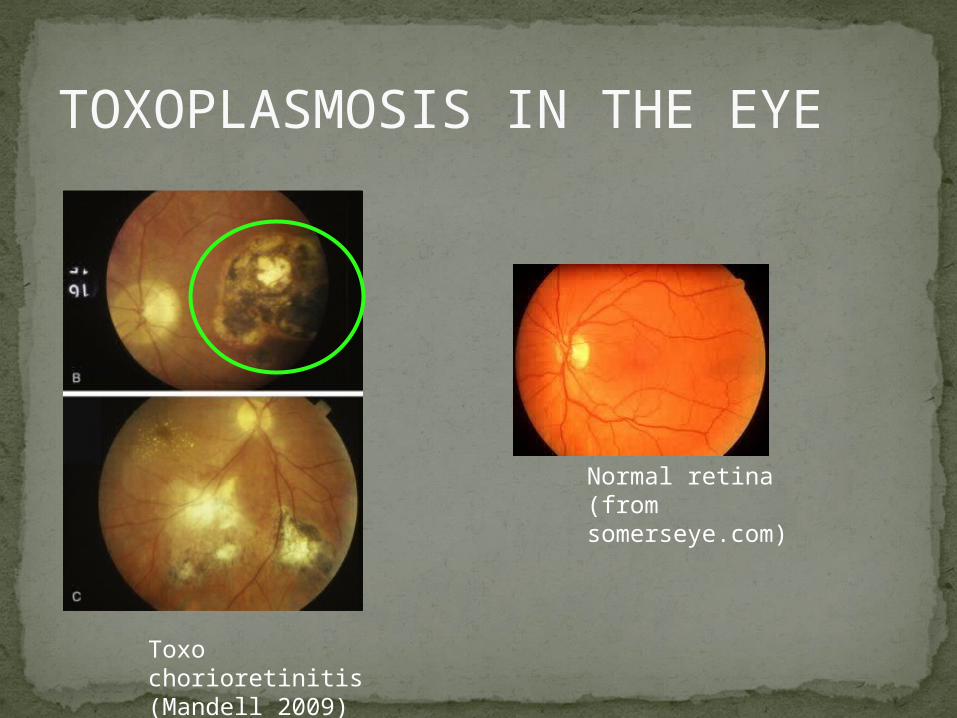
TOXOPLASMOSIS IN THE EYE
Normal retina (from somerseye.com)
Toxo chorioretinitis(Mandell 2009)
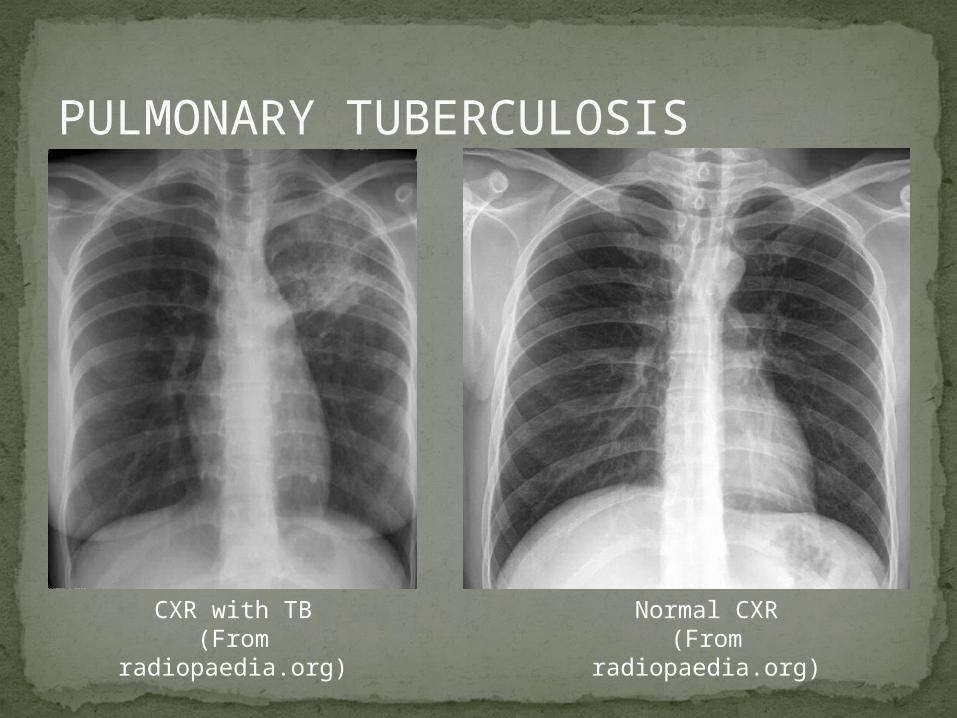
PULMONARY TUBERCULOSIS
CXR with TB(From radiopaedia.org)
Normal CXR(From radiopaedia.org)
END-STAGE AIDSPatients with CD4+ cells < 50 have end-stage
immunodeficiencyAt risk for additional opportunistic illnesses:
Disseminated Mycobacterium avium complex (MAC)Progressive multifocal leukoencephalopathy (PML)Cryptococcal meningitisOther disseminated fungal infections
(coccidiomycosis, histoplasmosis, aspergillosis, Penicillium marneffei)
Primary CNS lymphomaCMV RetinitisWasting syndrome
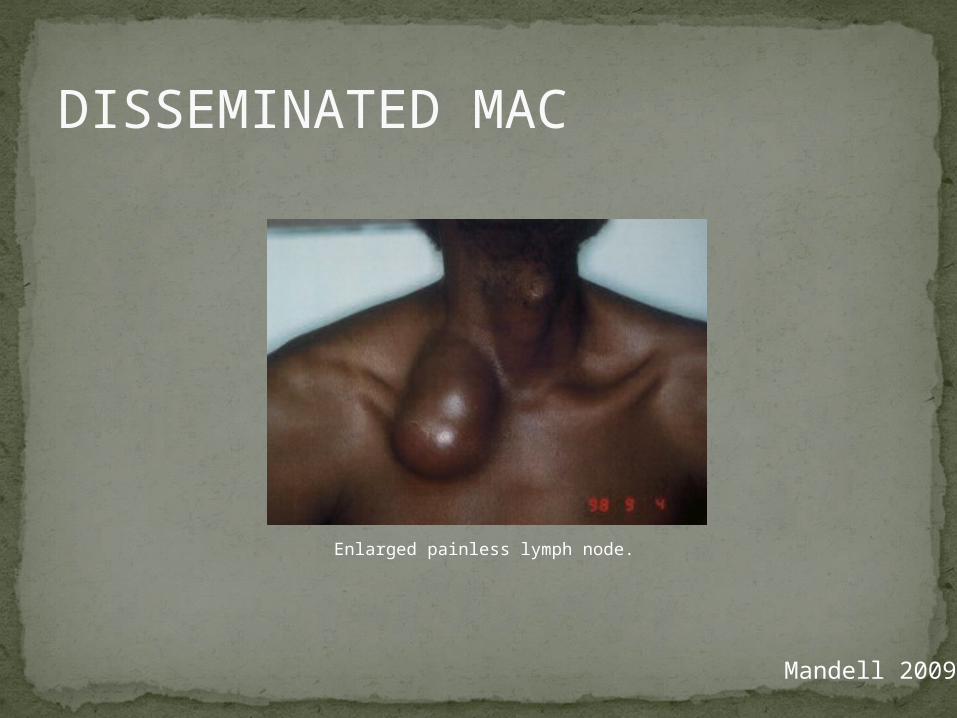
DISSEMINATED MAC
Enlarged painless lymph node.
Mandell 2009
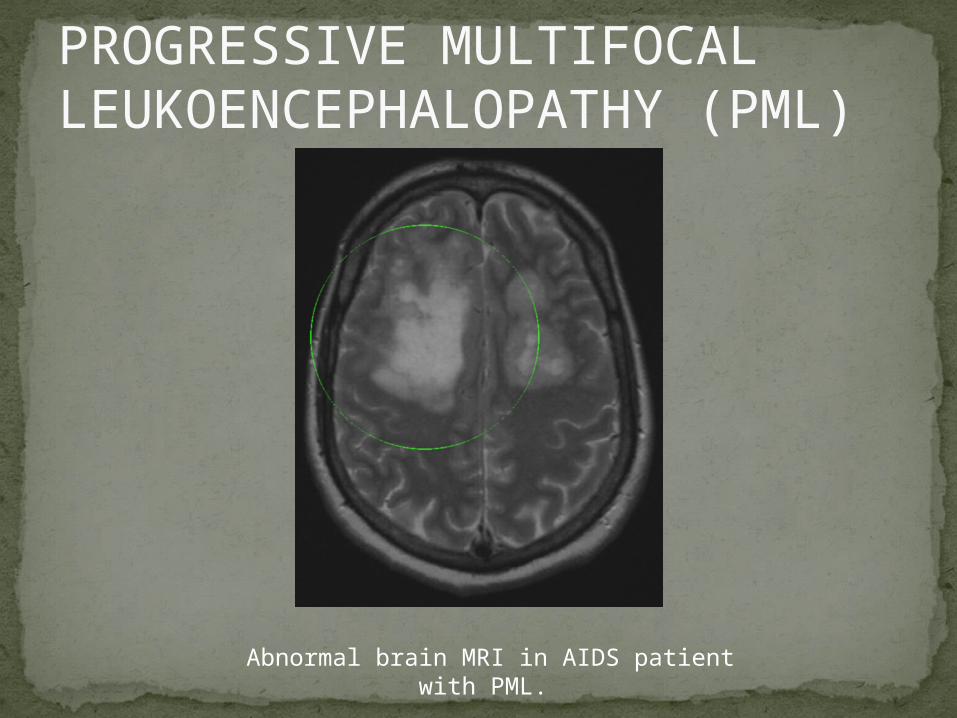
PROGRESSIVE MULTIFOCAL LEUKOENCEPHALOPATHY (PML)
Abnormal brain MRI in AIDS patient with PML.
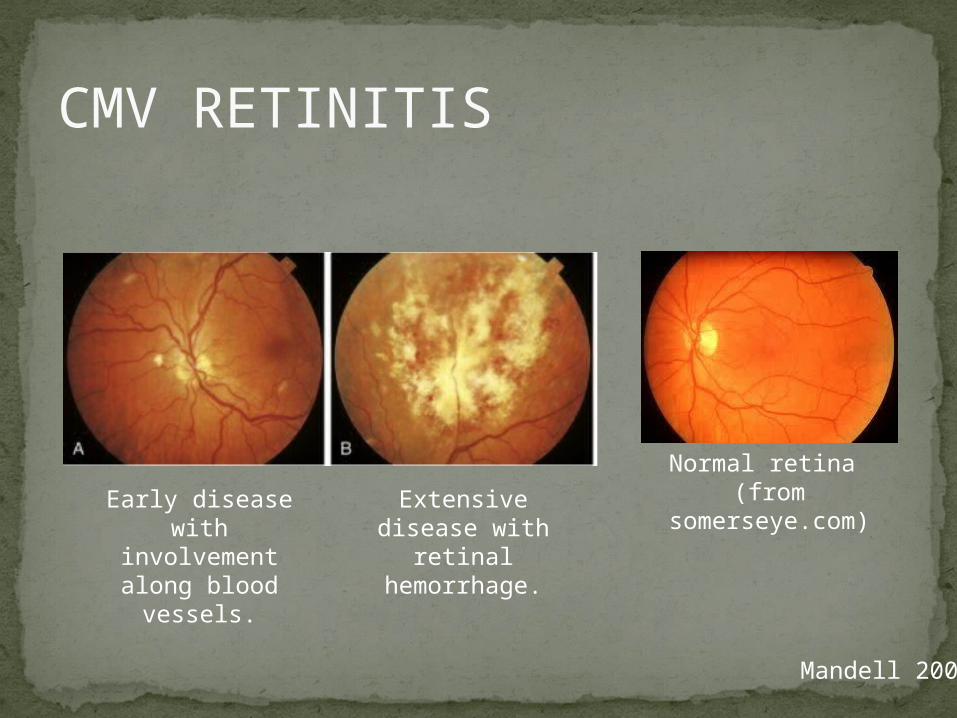
CMV RETINITIS
Normal retina (from
somerseye.com)Early disease
with involvement along blood
vessels.
Extensive disease with retinal
hemorrhage.
Mandell 2009
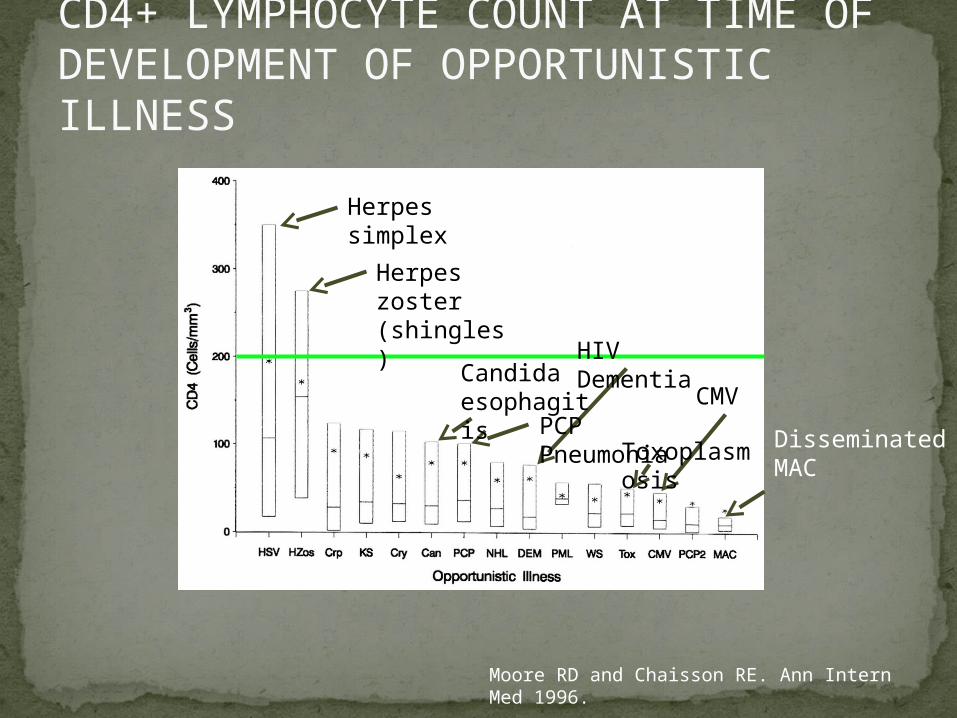
CD4+ LYMPHOCYTE COUNT AT TIME OF DEVELOPMENT OF OPPORTUNISTIC ILLNESS
Moore RD and Chaisson RE. Ann Intern Med 1996.
Herpes simplex
Herpes zoster (shingles)
Candida esophagitis
PCP PneumoniaToxoplasmosis
CMV
Disseminated MAC
HIV Dementia
TYPICAL COURSE OF HIV-1 INFECTION
Adapted from Pantaleo et al. NEJM 1993.
AIDS
AIDS DEATHMean survival after reaching a CD4+ count
of 200 is 38-40 months without treatmentMean survival after the development of
clinically-defined AIDS is 12-18 months (9 months in initial San Francisco cohort)
Opportunistic infections independently increase risk of death
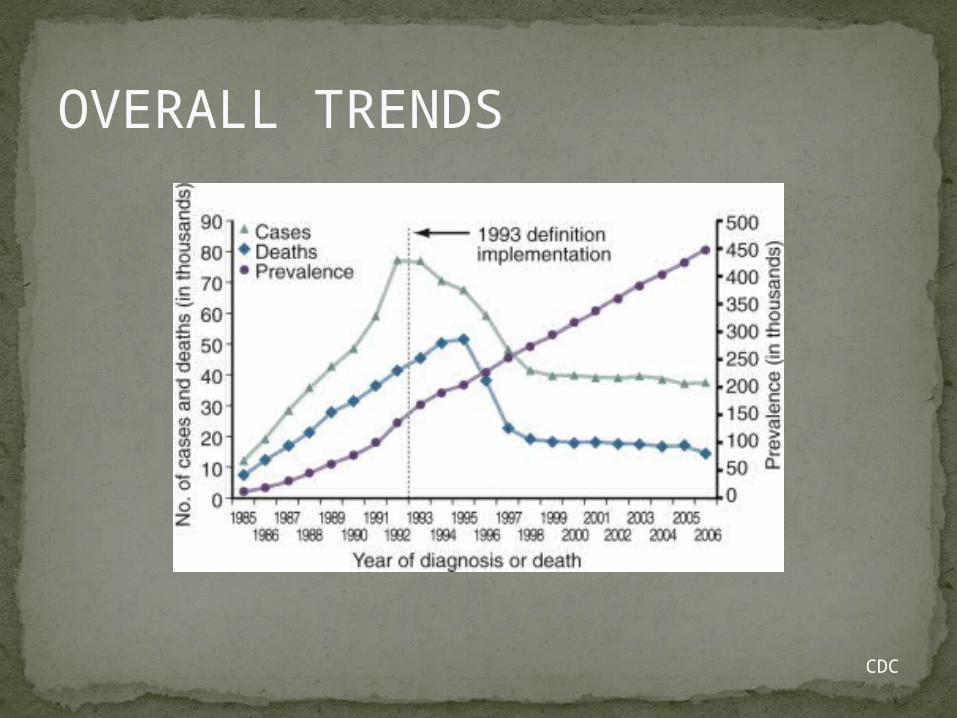
OVERALL TRENDS
CDC
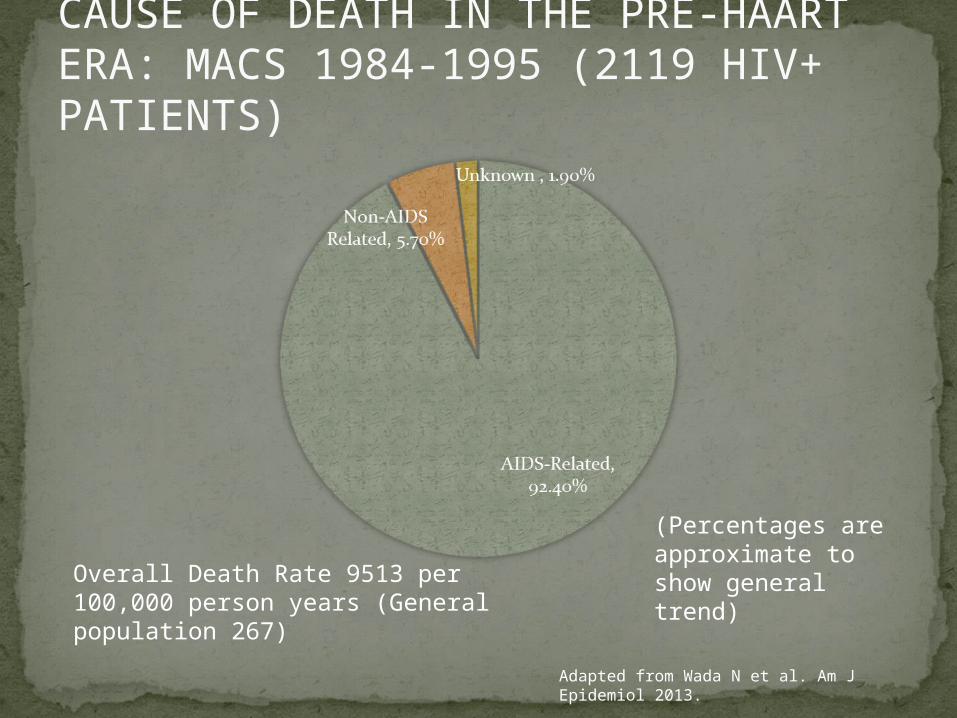
CAUSE OF DEATH IN THE PRE-HAART ERA: MACS 1984-1995 (2119 HIV+ PATIENTS)
Overall Death Rate 9513 per 100,000 person years (General population 267)
Adapted from Wada N et al. Am J Epidemiol 2013.
(Percentages are approximate to show general trend)
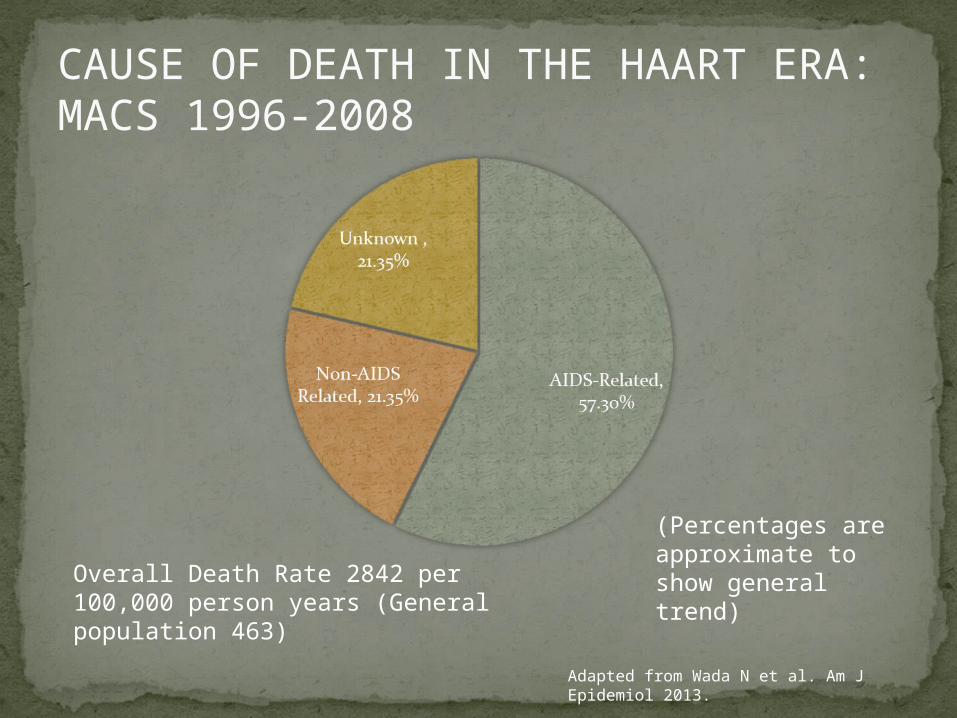
CAUSE OF DEATH IN THE HAART ERA: MACS 1996-2008
Overall Death Rate 2842 per 100,000 person years (General population 463)
Adapted from Wada N et al. Am J Epidemiol 2013.
(Percentages are approximate to show general trend)
SUMMARY 1-6 weeks (average 3 weeks) after primary infection 1/2 to
2/3 of patients develop an acute mononucleosis-like illness called the acute retroviral syndrome that lasts 10-15 days.
Following the acute infection, patients enter a period of clinical latency where they may remain mostly asymptomatic for up to 8-10 years on average, though this duration varies considerably.
Disease progression can be predicted by baseline viral load and CD4+ cell count.
Over time most patients (except for nonprogressors) will have declining CD4+ cells with increasing risk of developing symptoms.
When CD4+ cells fall below 200 or with specific opportunistic infections, patients are defined as having AIDS.
Risk of death increases dramatically when patients develop clinical symptoms of AIDS.
HAART dramatically reduces this risk.

KEY RESOURCESMandell, Douglas, and Bennett’s Principles and
Practice of Infectious Diseases, 7th Edition. Churchill Livingstone. 2009.
Vergis EN and Mellors JW. Natural History of HIV-1 Infection. Infectious Disease Clinics of North America 2000.
CDC: www.cdc.gov/hivWHO: http://www.who.int/hiv/en/
QUESTIONS?
Recommended

















