인제대학교
서울백병원
김 원

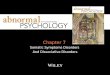
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
* total
suicidal ideation
* guilt
* low energy
depressed mood
* anhedonia
* psychomotor retardation
* poor concentraion
* psychomotor agitaion
* decreased sleep
* decreased appetite
controls past MDD current MDD
* < 0.05
Psychiatry Res, 2002

Painless somatic symptoms in depression ◦
vague and exaggerated multiple somatic complaints (usually ≥ 3)
◦
fatigue, weakness, non-specific and painless musculoskeletal problems, sensations of heaviness or lightness in at least one part of the body, gastrointestinal dysfunction, shortness of breath, palpitations, dizziness, double vision, changes in sleep patterns and appetite, and polyuria
Painful somatic symptoms ◦
joint pains, lumbar pain and headache
Age, female gender, and unemployment◦
associated with the presence of somatic symptoms.
The severity of the depression is greater in patients with moderate to severe discomfort due to somatic symptoms.

DSM system◦
emphasize psychological sx. as key fx. of MDD◦
underestimate somatic depression
Masked depression in primary care◦
1st stage, 442 patients, 1.8% prevalent.◦
2nd stage, 62 patients with high somatization score, 39 (63%) prevalent.◦
Most were diagnosed with Musculoskeletal disease◦
Underestimation is crucial in minority population.
Posse and Hallstrom, 1998

Nakao and Yano (2006)◦
1066 Japanese workers (mean age 35 years), ◦
annual health examinations, in 2 successive years, ◦
Prediction of depression in the following year◦
3.4~3.7% MDD seen among the Japanese workers◦
WHO reported that 77% of Japanese depressive subjects complained of somatic symptoms. ◦
Fatigue was the most common and powerful predictor of core depressive symptoms
Insomnia was closely related to depressive mood and diminished interest or pleasure. Headache was the second most common symptom, less predictive than fatigue and insomnia.

Depressed moodMontgomery–Asberg Depression Rating Scale (MADRS)Only 3 items : physical symptomsHamilton depression rating scale (HAM-D)8 items : physical symptoms18/56 point (32%)PHQ-9
Somatic symptoms Patient Health Questionnaire-15 (PHQ-15)Somatic Symptom Inventory (SSI) Visual Analog Scale (VAS) for pain (DeLoach et al., 1998)≥ 20 (on a scale of 0–100)Symptom questionnaire

Patient Health Questionnaire-15 (PHQ-15)◦
self-report, somatic symptom type and severity over, the prior 4 weeks
Somatic Symptom Inventory (SSI) ◦
26-item questionnaire, painless and painful ◦
patients' degree of discomfort for each symptom is rated from 1 to 5 (1 = absent; 3 = moderate; 5 = a great deal)
MADRS relies less than HAM-D does on somatic symptoms.

157 MDD patients
0
5
10
15
20
25
30
HAMD-17 HAMD-S MADRS MADRS-S
0wk 8wk Change on somatic symptoms correlated with global improvement in MDD.
Improvement in somatic symptoms is highly correlated with a favorable outcome in depression.
Nonremitting responders had a significant smaller baseline-to-end point decrease in somatic symptoms.
Nonremitter vs Remitter based on MADRS
-2.45
-3.71-4
-3
-2
-1
0
0-8w
k of
HA
MD
-S
nonremitting responder remitter
p=0.011
J Psychosom Res. 2006

Adapted from: Greco T, et al. J Gen Intern Med. 2004;19(8):813-818.
Nonsomatic depressive symptoms
Positive well-being
Nonpain somatic symptoms
Pain somatic symptoms
Impr
ovem
ent
Trea
tmen
t Effe
ct S
ize
Emotional Symptoms
Physical Symptoms
A Randomized Trial Investigating SSRI Treatment
0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
Baseline 1 Month 3 Months 6 Months 9 Months
N=573

Gender differences in prevalence of MDD◦
may be due to the high prevalence of anxious depression, atypical depression and somatic depression in women.
These three subtypes of depression ◦
are also very prevalent during pregnancy, the post partum period, perimenstrually and during the menopause transition (perimenopause) period◦
vulnerability and hormone instability in their pathobiology.

Atypical depression▪
Mood reactivity1
▪
Increased appetite1
▪
Increased weight1
▪
Hypersomnia1
▪
Leaden paralysis1
▪
Sensitivity to interpersonal rejection1
▪
Intensified mood reactivity2
▪
Mood Lability2
▪
Anxiety, Irritability2
Anxious depression phenotype3
▪
Depressed mood
▪
Negative self-evaluation▪
Discouragement▪
Diurnal variation▪
Depersonalization or derealization
▪
Somatic overconcern▪
Difficulty concentrating▪
Insomnia▪
Lack of energy▪
Psychomotor agitation▪
Subjectively experienced anger
▪
Distrustfulness▪
Nonreactivity of mood to changes in circumstances
1 APA, 1994. 2.West and Dally, 1959. 3 Clayton PJ et al, 1991. 4
Silverstein, 1999, 2002.
“Somatic Depression”4
▪
Depression▪
Sleep disturbances▪
Fatigue▪
Anxiety▪
Diversified pain and aches

Lifetime prevalence of somatic depression◦
(F: 15.2%, M: 7.5%)
but a prevalence of pure depression ◦
(F: 6.9% , M: 6%)
Somatic depression have a tendency with coexisting anxiety disorder
Silverstein, 1999

Serotonin (5-HT) and norepinephrine (NE) pathways mediate various functions in the brain1-3
Descending spinal projections modulate nociception2,3
Disturbance in these pathways are thought to be associated with the emotional and physical symptoms of depression3
Dorsal raphe nuclei
Caudal raphenuclei
Lateral tegmental NA cell system
Locus ceruleus
NE
Depressed mood
Suicidal ideation
Sleep disturbances
Changes in appetite/Lack of pleasure
Vague pain in joints, limbs, back,
abdomen, etc
Headaches
GI complaints
Modulatory effects on nociception
5-HT
–Adapted from: 1Kaplan HI, Sadock BJ. In: Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. 8th ed. Lippincott Williams & Wilkins; 1998:114-115.
2Fields HL, et al. Annu Rev Neurosci. 1991;14:219-245.3Stahl SM. J Clin Psychiatry. 2002;63:382-383.

Atypical depression ◦
MAOI > TCA , still in debate ◦
SSRI + benzodiazepine
Somatic depression◦
Very few studies◦
Secondary analysis
Chronic pain◦
TCA = SNRI ? > SSRI◦
TCA + anticonvulsant => gabapentin ?
Antonijevic, 2006; Matza et al., 2003

SNRI◦
Venlafaxine, Milnacipran, Duloxetine◦
Analgesic effect via descending pain pathway

3
4
5
6
7
8
0 1 2 3 4 5 6 7 8Week
Mea
n H
AM
-D S
core
on
6 A
nxie
ty-
Som
atiz
atio
n Fa
ctor
Item
s*Venlafaxine XR (N=1136)Placebo (N=691)
†
‡
‡
‡
‡‡
Venlafaxine XR in the Reduction of Anxiety- Somatization Symptoms Associated with MDD*
†P<0.05 venlafaxine XR vs placebo; ‡P<0.001 venlafaxine XR vs placebo
*HAM-D Anxiety-Somatization Factors include Anxiety-Psychic, Anxiety-Somatic, Somatic-Gastrointestinal, Somatic-General, Hypochondriasis, and Insight.Data on File, Wyeth Pharmaceuticals
Pooled Data from 7 Randomized Placebo-Controlled Studies


In Depressed PatientsEffective in reducing pain associated with depression1
1 Detke et al, 2003
-45-40-35-30-25-20-15-10-50
Overall Head Back Shoulder
PlaceboDuloxetine
*p<0.05 vs. placebo
Mean R
eductio
n in
VAS
follo
win
g tre
atm
ent


Effectiveness of mirtazapine in the treatment of depression with associatedsomatic symptoms.
García Campayo. Actas Esp Psiquiatr. 2008 Jan-Feb;36(1):25-32.
Somatic section on HAM-D, SPPI




Quetiapine◦
Antipsychotics for anxious depression ?◦
perphenazine

Omega-3 fatty acid (DHA & EPA)◦
The deficit of omega-3 PUFAs is associated with depression. ◦
Societies that consume a small amount of omega-3 PUFAs appear to have a higher prevalence of MDD. ◦
depressive pt. showed a lower level of omega-3 PUFAs◦
the antidepressant effect of PUFAs had been reported in a number of clinical trials.◦
EPA and DHA are not synthesized in human body and can only be obtained directly from fish.
the role of n-3 fatty acids in psychoneuroimmunology,somatic presentation, and medical illness comorbidity of depression. Su KP, Asia Pac J Clin Nutr.2008

Education◦
Caffeine, alcohol
Psychotherapy◦
Supportive◦
Cognitive-behavioral◦
Mindfulness
Biofeedback, relaxationExerciseMeditation, Yoga

New dimension of diagnosis
Detailed and precise measurement of somatic symptoms
New pharmacotherapy tailored to…
Recommended