i
NUTRITIONAL STATUS OF CHRONIC RENAL FAILURE PATIENTS (PRE-DIALYSIS) WITH DIFFERENT LEVELS OF RENAL INSUFFICIENCY.
BY
CLEMENT OYEDELE OLADELE
M.B.B.S (ILR)
DEPARTMENT OF MEDICINE UNIVERSITY OF BENIN
TEACHING HOSPITAL BENIN CITY.
BEING A DISSERTATION SUBMITTED TO THE NATIONAL
POST GRADUATE MEDICAL COLLEGE OF NIGERIA IN
PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE
AWARD OF THE FELLOWSHIP OF THE FACULTY OF
INTERNAL MEDICINE, NEPHROLOGY SUBSPECIALTY.
MAY, 2007.

ii
DECLARATION
It is hereby declared that this work is original unless otherwise
acknowledged. The work has not been submitted to anybody for an
award.
______________________________________________
CLEMENT OYEDELE OLADELE M.B.B.S [ILR).
DEPARTMENT OF MEDICINE
UNIVERSITY OF BENIN TEACHING HOSPITAL,
BENIN CITY.

iii
DEDICATION
This work is dedicated to the glory of God who makes things happen.

iv
CERTIFICATION
I certify that this study has been carried out by Dr. Clement Oyedele
Oladele of the department of medicine, University of Benin Teaching
Hospital, Benin City. Under the supervision of Professor L.I Ojogwu and
Dr. (Mrs.) E.I.Unuigbe
___________________________ __________________
Dr. (Mrs) E.I. Unuigbe Date
Ag. Head, Department of Medicine,
University of Benin Teaching Hospital,
Benin City.

v
ATTESTATION
We certify that this study has been carried out by Dr. Clement Oyedele
Oladele of the department of medicine, University of Benin Teaching
Hospital, Benin City under our supervision
1. ____________________
Professor L.I Ojogwu.
Professor of medicine,
Department of medicine
University of Benin
Teaching hospital
Benin City.
2. ____________________
Dr (Mrs.) E. I. Unuigbe
Senior Lecturer,
Department of Medicine
University of Benin
Teaching Hospital
Benin City.

vi
ACKNOWLEDGEMENT
I am highly indebted to Prof Ojogwu for his fatherly role, the supply
of the materials for this work, his constant pressure on me and his
encouragement too numerous to mention.
I wish to appreciate in no small measure the motherly role of
Dr (Mrs.) Unuigbe for her moral support, encouragement,
understanding and her patience with me.
I thankfully acknowledge and appreciate the immense
contribution of Prof E. Oviasu, for his encouragement, the moral
support and guidance in my work.
I am also grateful to my parents, and my brothers. I appreciate
the prayers and the moral support of my sister Mrs. L.O Ajayi and her
loving children.
The generosity of Mr. Ohizua, nutrition unit, Edo State Ministry
of Health for releasing the caliper that was used for measuring Triceps
skin fold thickness, is highly appreciated.
I thank Dr. Liman Hamidu for his brotherly role in my life.
I am very grateful to my brother and a friend in nephrology, Dr
Ralph Onyemekeihia who stimulated my interest in Nephrology. I thank
Dr. Imarhiaghe for his love, concern and foresightness.
I must thank all the consultants in the department of
medicine for contributing to my training. I wish to thank the entire staff
of the haemodialysis unit for their cooperation including the office staff

vii
of the department of medicine, UBTH and my colleagues in the
department of medicine.
Finally to my wife, Gloria, and our children Ore-oluwa and
Oluwa-seyi who have allowed me to stay away from them for several
hours in the day and sometimes night during the time of this work. I
thank you for your prayers and patience.
To God Almighty be the Glory

viii
TABLE OF CONTENTS
PAGES
Title i
Declaration ii
Dedication iii
Certification iv
Attestation v
Acknowledgement vi
Table of content viii
List of tables ix
List of figures x
List of appendices xi
List of abbreviation xii
Summary xiii
Chapter 1: Introduction 1
Chapter 2: Literature review 8
Chapter 3: Materials and methods 24
Chapter 4: Results 35
Chapter 5: Discussion 56
Chapter 6: Conclusion and recommendation 63
Limitations of the study 66
References 67
Appendices 77

ix
LIST OF TABLES
TABLE PAGES
1. Characteristics of CRF patients and control group 36
2. Glomerular filtration rates of subject and control using MDRD 37
3. Stage of CKD by duration of illness 38
4. Distribution of malnourished patients and control by 40
indices of malnutrition.
5. Nutritional status by SGA criteria 41
6. Stage of CKD by degree of malnutrition using SGA. 43
7. SGA of CKD patients and control by age group distribution 44
8. Characteristics of the 5 patients in stage 5 CRF that 45
were severely malnourished by SGA criteria
9. Comparison of anthropometric and biochemical 51
characteristics between well nourished and malnourished
chronic renal failure patients before commencement
of dialysis therapy

x
LIST OF FIGURES
FIGURES PAGES
1. Mean average daily protein intake by stage of CRF 53
2. Mean average daily protein intake of CKD patients 55
and control by degree of malnutrition.

xi
LIST OF APPENDICES
APPENDIX PAGES
1 Consent form 76
2 Nutritional status of CRF patients 77
(pre-dialysis) with different levels of
chronic renal insufficiency questionnaire
3 Initial nutrition history and assessment 80
4 Subjective Global Assessment Rating Form 81
5. List of food items 84
6. Picture of the investigator 86

xii
LIST OF ABBREVIATIONS
alb albumin
BMI Body Mass Index
CKD Chronic Kidney Disease
CRF Chronic Renal Failure
DEXA Dual Energy X-ray Absorptiometry
ESKD End Stage Kidney Disease
GFR Glomerular Filtration Rate
IGF-1 Insulin-like Growth Factor – 1
IL-1 Interleukin – 1
KDQOL Kidney Disease Quality of Life
MDRD Modification of Diet in Renal Disease
MUAC Mid-Upper Arm Circumference
NPNA Normalized Protein Equivalent
Scr Serum creatinine
SGA Subjective Global Assessment
SUN Serum urea nitrogen
TNF-α Tumour Necrosis Factor - α
TSFT Triceps Skin Fold Thickness

xiii
SUMMARY
The nutritional status of patients with chronic renal failure
(CRF) at the initiation of dialysis therapy and while on maintenance
dialysis therapy is an important determinant of the morbidity and
mortality associated with the disease.
The nutritional status of our CRF patients population has not
being well characterized. In Nigeria, there is paucity of data on the
prevalence of malnutrition amongst our CRF patients especially before
the initiation of dialysis therapy. There is the need to know the
prevalence and appreciate the magnitude of the problem in order to
formulate a policy on routine nutritional assessment and intervention.
66 chronic renal failure patients being managed at the Renal Unit of
University of Benin Teaching Hospital, Benin City were studied. The
patients were made up of 45 males and 21 females with ages ranging
between 18 years and 65 years. Patients with no evidence of nephrotic
syndrome, chronic liver disease, HIV, tuberculosis, malignancy or
steroid therapy were recruited for the study. 40 age and sex matched
control subjects were also studied.
A multiparametic method of nutrition assessment was
employed and this method involved the use of the well validated, tested
and verified subjective global assessment (SGA). Weight change over six
months of follow up, body mass index, mid-upper arm circumference,
triceps skin fold thickness, serum albumin concentration were also

xiv
used to assess nutritional status. A three-day food diary was used to
determine the average daily protein intake of the patients.
Malnutrition was present in 46% of the patients studied
using SGA criteria and in 42% using two or more nutritional
markers. Malnutrition in CRF patients (Pre-dialysis) is
predominantly mild to moderate. Severe malnutrition is relatively
uncommon in CRF patients before dialysis therapy. There is
worsening of nutritional status as dietary protein intake decreases
and renal function deteriorates from moderate renal insufficiency
to end stage renal failure. When compared with SGA, serum
albumin underestimated patients with malnutrition.
In conclusion there is a high prevalence of malnutrition in our
CRF patients before the commencement of dialysis therapy, and the
nutritional status of these patients at the start of dialysis therapy is a
strong predictor of their short term and long term outcome. It is
recommended that nutritional status of all chronic renal failure
patients should be evaluated routinely using multiparametric method
whenever they present at the hospital.

1
CHAPTER ONE
1.0 INTRODUCTION
Chronic renal failure (CRF) is defined as either kidney damage or
GFR<60mL/min/1.73m2 for≥3months. Kidney damage is defined as
pathologic abnormalities or markers of damage, including abnormalities
in blood or urine test or imaging studies.1
In United Kingdom the prevalence of CRF is approximately 600
individuals per million population per year (0.06%).2 The incidence of
end stage renal failure (ESRF) is of the order of 200 per million
population per year (0.02%)2. In Nigeria, although accurate figures are
not available, the size of the problem has been estimated using hospital
admission records. Hospital admission rates of CRF in South-West
Nigeria vary from 1.6%to 6.7%-8%.3,4 However, much earlier reports by
Adetuyibi et al showed that CRF accounted for 11.4% of deaths on the
medical wards of a major teaching hospital in the region5. Hence CRF is
not uncommon amongst Nigerians.
Chronic glomerulonephritis, hypertension and diabetes mellitus
account for the majority of CRF cases in Nigeria with obstructive
uropathy and autosomal dorminant polycystic kidney diseases
accounting for smaller proportions4.Uptill two decades ago,
diabetes mellitus was reported to be an uncommon cause of CRF in
Nigeria, but in the last few years, reports from several Renal Units in
the country now place diabetes nephropathy as the third most common
cause of CRF3,6.

2
There are several irreversible but modifiable complications of
chronic renal failure and these include anemia, cardiovascular disease,
metabolic bone disease and malnutrition. These complications begin
early in the course of renal failure7. Patients on maintenance
haemodialysis are at risk of developing malnutrition. Malnutrition in
these patients is associated with reduced life expectancy because of
infections and cardiovascular complications8.
Adequate nutrition is essential to life. Many of the major medical
problems of public health importance in all parts of the world have
either a nutritional basis or at least an important nutritional
contribution. This includes chronic renal failure. This is particularly
important because of the huge economic cost of maintaining such
patients on renal replacement therapy9.
It has been shown that renal diet is not palatable to most patients
and this therefore modifies their eating habit10.
Previous study has identified protein malnutrition as the main
factor responsible for mortality and morbidity in dialysis patients.11,
Low serum albumin has also been reported to be an adverse prognostic
factor in adults with end stage renal disease on continuous peritoneal
dialysis11,12. Malnutrition has been shown to lead to progressive decline
in glomerular filtration rate, decreased excretion of acid or osmolar
load, decreased urinary phosphate excretion, diminished response to
expanded extra cellular volume and higher incidence of urinary tract
infection.13 Addition of soybeans protein to low protein diet has been

3
demonstrated to have effectively reduced the rate of chronic renal
failure progression.
1.1 ASSESSMENT OF NUTRITIONAL STATUS
No single method is appropriate in evaluating nutritional status in
CRF patients before the initiation of dialysis therapy and when on
haemodialysis. Most authors agree that a multiparametric evaluation in
which various assessments are included is most appropriate.8,14
Nutritional status is conventionally assessed by means of a
combination of anthropometric measurements and laboratory
assessments14,15.
The National Kidney Foundation recommends the following tools
for use in adult dialysis patients and these include; (a) normalized
protein equivalent of nitrogen appearance (n PNA), which is derived
from the daily net generation of urea and is normalized to the body
weight. (b) serum albumin and pre-albumin which measure proteins in
the blood. (c) subjective global assessment, which is a set of observation
based on patients symptoms and physical examination findings (d)
anthropometry is a measure of skin fold thickness and other aspects of
body composition. (e) dual energy x-ray absorptiomentry (DEXA) which
is an x ray technique measuring the components of body mass69.
Some studies have also recommended the use of total daily
protein intake as a nutritional marker 16,17,18. However, measurement of
food intake is difficult because individual food intake fluctuates and the

4
fluctuation can be due to social and economic reasons. Change in
appetite also accounts for substantial change in food intake from day to
day and week to week. Measuring food intake also does not absolutely
indicate whether or not an individual is malnourished, since this will
depend on the effectiveness of absorption, on the individual’s specific
needs and on any metabolic change in utilization. Accurate assessment
of the nutritional status of an individual therefore requires direct
measurement of body size, nutrient stores, metabolism and functional
capacity.19,20
Anthropometry involves measurements of subcutaneous fat as
skin fold thickness and skeletal muscles as mid arm circumference,
these are important to determine the severity of malnutrition. Other
anthropometric factors associated with malnutrition include low body
weight and hand grip strength. The use of anthropometry is limited by
the requirement of specialized calipers, the experience of the observer,
and the potential confounding effects of oedema or dehydration.20
Biochemical factors that are associated with malnutrition include
visceral proteins like serum albumin, pre_ albumin, transferring, serum
levels of creatinine, plasma levels of insulin – like growth factor 1 (IGF-
1) and branched chain amino acid (isoleucine, leucine and valine).
Factors that can influence albumin values include age, sex and serum
c-reactive protein. Other studies have reported the use of serum levels
of tumor necrosis factor - 1, cholesterol, Immunoglbulins, urea,
phosphorus, potassium bicarbonate, transferrin, total lymphocyte

5
count, alpha -1-acid glycoprotein and ceruloplasmin as markers of
either nutritional intake or body protein or muscle mass.18,20
Malnutrition is present in 42% - 77% of end-stage renal disease
population in developing countries, is strongly associated with
increased morbidity and mortality21 and is common in patients on
maintenance haemodialysis. However, in another study, a 40%
prevalence of malnutrition was found in patients with advanced renal
failure at the beginning of dialysis treatment8,16. In other studies it has
been demonstrated that about one third of patients have mild to
moderate malnutrition and 6 to 8% have severe malnutrition8. Signs of
malnutrition are observed in 10-70% of haemodialysis patients and 18-
51% of patients on continuous ambulatory peritoneal dialysis.22
There is paucity of data regarding the prevalence of protein
malnutrition in the CRF population in developing countries. However,
Agaba et al using body mass index (BMI) and serum protein levels
studied the prevalence of malnutrition among 74 Nigerians with CRF
before commencement of dialysis therapy. Protein malnutrition (serum
albumin < 29g/l) was present in 32 (43.2 %) of patients with CRF and
only one (2%) of the control subjects23 suggesting protein malnutrition
is common in Nigerian CRF patients.

6
1.2 OBJECTIVES OF THE STUDY
1.2.1 a) General:- To assess the nutritional status of CRF patients
before the initiation of dialysis therapy.
1.2.2 b) Specific: (1) - To determine the baseline prevalence of
malnutrition in CRF patients before dialysis therapy.
(2) To correlate the nutritional status with the glomerular
filtration rate (GFR) of CRF patients.

7
1.3 Relevance of the study
1. Malnutrition often begins before patients with chronic kidney
disease develop end stage renal failure. The physical fitness of these
patients as evident by their nutritional status at the time of initiation of
dialysis therapy plays a pivotal role in their long term survival.
Screening for malnutrition early in the course of CKD can help detect
patients at risk of malnutrition so that health care providers can offer
nutrition intervention, thus improving out comes and lowering cost.
2. Most of the previous work done on nutrition in CRF patients were
either carried out in patients on maintenance dialysis therapy or ESRF
with little known about the prevalence of malnutrition before dialysis
treatment and its relationship with the level of renal insufficiency.
Hitherto, there has been only one local study on the prevalence of
malnutrition before dialysis but it was not correlated with the level of
renal function, neither was the multiparametric method used to assess
nutritional status.
3. To add to our knowledge of what is already known about
malnutrition in CRF and the prevalence.

8
CHAPTER TWO
2.0 LITERATURE REVIEW
Studies have indicated that patients undergoing maintenance
haemodialysis, intermittent peritoneal dialysis or continuous
ambulatory peritoneal dialysis, are malnourished. Evidence for
malnutrition is present in CRF patients even at commencement of
dialysis therapy24.
However, literature is sparse on the assessment of nutritional
status in chronic renal failure patients not undergoing dialysis. The
high prevalence of malnutrition is a source of concern because
parameters of nutritional status are among the most powerful
predictors of morbidity and mortality in patients with CRF. Malnutrition
often begins before patients with chronic kidney disease develop ESRF
and before commencement of dialysis. Several reports have alluded to
this. In the Modification of Diet in Renal Disease Study Group, where
1785 patients were evaluated, nutritional status correlated significantly
with the level of GFR13. Barril et al evaluated the nutritional status of
56 patients with chromic renal failure in a pre-dialysis unit and found
also significant correlation between the nutritional status and the level
of GFR reduction25. Agaba et al studied the prevalence of malnutrition
among Nigerians with chronic renal failure before commencement of
dialysis using the body mass index (BMI) and serum albumin. 74
patients with CRF who have not been on dialysis and 48 control

9
subjects were studied. Low BMI (less than 20kg/m2) was present in 16
(21.6%) of the patients compared with one of the controls. The mean
serum total protein and albumin were also significantly lower in the
patients compared with the controls. Protein malnutrition, (serum
albumin <29g/L) was present in 32(43.21%) of patients with CRF and
1(2.1%) of the control subject. However, these results were not
correlated to the levels of renal failure (GFR).
2.1 MALNUTRITION IN CHRONIC RENAL FAILURE
During the evolution of CRF, malnutrition may become
apparent when the glomerular filtration rate (assessed by creatinine
clearance) is less than 40mls/min/1.73m26,27 but largely, malnutrition
is frequently found in patients with CRF before and after initiation of
dialysis23
Causes of malnutrition in CKD patients include inadequate
protein and calorie intake due to excessive dietary restriction by
physician / dietician. Infection causing increased catabolic state
resulting in tissue breakdown. Tissue resistance to anabolic hormones
namely insulin, growth hormone and insulin growth factor -1.15
Gastrointestinal abnormalities vary from mild mucosal oedema to
severe inflammation, ulceration and mucosal necrosis also contribute
to malnutrition in these patients.15

10
In patients undergoing maintenance dialysis, malnutrition is
further increased with the use of bio-incompatible membranes and
external loss of albumin.23
There is a direct relationship between the glomerular filtration
rate (GRF) and the level of malnutrition in CRF patients. This is part of
the conclusion of the study carried out on ninety-five (95) subjects who
participated in the pilot phase of the Modification of Diet in Renal
Disease (MDRD). This was apparent from the direct correlation
between the GFR and the serum transferrin level at the end of the
study in men and women combined, as well as the correlation between
arm muscle area and GFR in men only.
The mechanism responsible for the tendency for serum transferin
to be lower and the body weight to fall in the patients with the lower
GFR level is not clear.8 This could be a subtle manifestation of uraemia
with the accumulation of toxins, the development of altered hormone
levels and or loss of endocrine and metabolic activity of the kidney.28
2.2 DIETARY PROTEIN RESTRICTION
Low protein diets are routinely prescribed for CRF patients
before they go into ESRF. A recurring criticism of low – protein diets is
that they may cause protein malnutrition. However, protein
malnutrition is not an acute condition, it develops over weeks of
negative nitrogen balance. This negative balance can be detected early if
patients on dietary therapy are subjected to regular checks. Reports

11
suggest that low protein diet is not the sole cause of protein
malnutrition in uraemic patients. The commonest cause of protein
malnutrition in chronic uraemic patients on low-protein diet is
inadequate calorie intake. Questionnaires are available to help
clinicians ascertain the calorie intake of their patients and where
present, protein malnutrition is an absolute contraindication for a low
protein diet29. In patients where the cause of protein malnutrition can
not be recognized and rapidly removed, then renal replacement therapy
is indicated. Reports29 suggest that malnutrition (resulting in cachexia)
though attributed to the low protein diet could be due to inappropriate
prescription of diets or to inadequate monitoring of nitrogen balance.
Similarly if patients are uraemic and malnourished when they are
started on a haemodialysis programme after being treated for chronic
uraemia with a low-protein diet, it is not the diet that should be blamed
but the undue persistence with conservative therapy when it was no
longer indicated. When correctly employed, a low-protein diet even
when it has been given for several years should enable a patient to start
dialysis in a well-nourished state by correcting the metabolic and
hormonal derangements29.
The most serious hazard of dietary protein restriction is
malnutrition. Therefore, it is very important to avoid muscle-wasting in
patients on a low-protein diet. In patients on dialysis, morbidity is
largely related to physical fitness at the start of replacement therapy. It
would be a great disadvantage if the postponement of dialysis therapy

12
secured by treatment with a low protein diet was paid for by loss of
fitness at the time dialysis is started30.
2.3 CAUSES AND AETIOPATHOGENESIS OF MALNUTRITION IN
CHRONIC RENAL FAILURE PATIENT.
There are multiple factors that contribute to protein-energy
malnutrition in patients with CRF. They include: decreased energy or
protein intake, concurrent chronic illness and possibly increase in
inflammatory cytokines. A close relationship between malnutrition,
inflammation and artherosclerosis in patients with renal disease has
been suggested by many studies. It was suggested that pro
_inflammatory cytokines represent a common link between
malnutrition, inflammination and artherosclerosis (MIA syndrome) in
patients with chronic renal disease 31,32,33.
There could be two types of malnutrition in patients with CRF.
First is related to low protein and energy intake; here co morbid
conditions are unusual and serum albumin may be normal or only
slightly decreased. The second type of malnutrition is associated with
inflammation and artherosclerotic cardiovascular disease (MIA
syndrome) co morbid conditions are common and serum albumin levels
are usually decreased32.
It is pertinent to note that serum IL – 1, IL – 6, and TNF alpha
levels are increased in patients with CRF already before the initiation of
dialysis, suggesting that renal failure is a contributing factor and the

13
catabolic stimulus of haemodialysis. Also nutrients such as amino
acids, peptides, protein (with peritoneal dialysis), glucose (when
haemodialysis is performed with glucose free dialysate) and water
soluble vitamins are lost into dialysate during dialysis. Diagnostic or
therapeutic (eg prednisolone therapy) procedures that reduce nutrients
intake or engender net protein breakdown also contribute. Other
theoretically possible causes of protein-energy malnutrition include
chronic blood loss, endocrine disorders (especially resistance to insulin
and insulin – like growth factor – 1, hyperglucagonaemia,
hyperparathyroidism and deficiency of 1, 25 dihydroxycholecalciferol),
accumulation of products of metabolism in renal failure such as
organic and inorganic acids which may induce wasting, and the
accumulation of toxic compounds that are taken up from the
environment (eg aluminium).34
Apart from above factors, many religious practices in developing
countries promote abstinence from meat, fish and eggs, a vegetarian
dietary pattern (which is becoming increasingly popular) and ingestion
of inadequate protein and calories in the diet to arrest the progression
of chronic renal failure, may lead to malnutrition in CRF patients21.
Other factors that may explain malnutrition are the facts that these
patients are chronically exposed to the risk of inadequate diet
counseling/self designed restrictions, repeated hospitalization which
disturb dietary habits and reduce intake, and super imposed acute or
chronic illnesses. Also low protein and low phosphate diets which are

14
routinely prescribed for CRF patients before commencement of dialysis
are sometimes hypocaloric and may be deleterious to the patient’s
nutritional status if not adequately monitored by skilled dietitian.
Previous reports8 suggest that protein calorie malnutrition often
begins incipiently when the GFR is about 30 to 59 mls/min/173m2 or
even higher and continues to fall gradually as the GFR decrease below
these values. However patients do not usually manifest florid symptoms
of malnutrition until the GFR is markedly reduced below this range8
Other mechanisms that have also been incriminated in the
development of malnutrition include,
Disorders in metabolism of the main nutrients
Increased protein catabolism due to acidosis and related
infections or inflammation.
Dialysis which in itself is a hyper catabolism factor.
Anorexia is a potential cause of reduced nutrient intake and it is
thought to be due to the retention and accumulation of anorexigen
molecules, but these molecules are essentially unknown. Anderstain et
al8, using a rodent model to assess spontaneous food intake,
demonstrated that substances in the plasma of uraemic patients can
suppress appetite. Attempts to determine the chemical composition of
this factor indicated that it probably falls in the middle molecule size
and may be a peptide.

15
2.4 Methods of Nutritional Status assessment in Chronic
Renal Failure Patients
No single method is appropriate in order to evaluate
nutritional status of chronic renal failure patients. Most authors agree
that a multiparametric evaluation in which various assessments are
included is most appropriate14,15,35,36.. There is no single readily
available measure of malnutrition that is both sensitive and specific in
ill patients. The following assessments are usually made.
Assessment of dietary intake.
This method is very simple to carry out it is one of the most
important aspects of nutritional assessment. It originally involves the
use of 24 hours or 72 hours dietary recall. However the two were befell
with difficulty in memory recall of food item eaten 24 hours or 72 hours
earlier. It has now been replaced by 3 days diet diaries. The limitation
of the use of this method is falsification of food item eaten by the
patients15.
Anthropometry:
Measurement of subcutaneous fat and skeletal muscles are
important to determine the severity of malnutrition. Using specialized
calipers and a tape measure, anthropometry estimates body fat from
the thickness of the skin fold of the posterior mid upper arm.
Usefulness of anthropometry include its non-invasiveness, inexpensive,
requires little training, easy to perform. The use of anthropometry is

16
limited by the requirement of specialized calipers, the experience of the
observer (operator dependent), low precision, high intra and inter
observer variances and the potential confounding effects of oedema or
dehydration15.
The mid arm circumference:
This measurement is a standardized means of assessing
nutritional status that has the advantage of being quick and easy to
carry out. This has facilitated its use in developing world. Arbitrary
minimum values are around 22cm in females and 25cm in males.
Subtracting triceps skin fold thickness, the mid arm circumference can
be used to calculate the approximate mid arm muscle circumference.
However, the latter variable is dependent on numerous factors
including age and race, it is far better to monitor the trend in arm
circumference with time in one individual37
Body Mass index (BMI)
Most studies have used body mass index (BMI = weight
kg/height (m)2 and or anthropometry (measurement of skin fold
thickness) to assess patients nutritional status.
BMI is a measure of fat that is practically independent of height.
It is a useful tool particularly when a trend is followed for monitoring
relative nutritional status. However, it is not fully dissociated from

17
height and its accuracy decreases with age as vertebral height
diminishes. BMI alone is not a sensitive indicator of protein /energy
malnutrition, as it does not distinguish between depletion of fat or
muscle.
According to Lukaski and Garrow classification, nutritional status
of any individual is regarded as normal when BMI is 21-24 kg/m2,
moderately malnourished when BMI is 18- 20 kg/m2, severely
malnourished at <18kg/m2 and over weight when BMI is 25-30 kg/m2
and obese when BMI is above 30kg/m2.38 In a large number of studies,
malnutrition has been defined as BMI < 20 kg/m2 and a Triceps Skin
Fold Thickness (TSFT) or mid arm muscle circumference (MAC) < 5th
percentile. Patients with a BMI of < 18 and 16 kg /m 2 with
anthropometry measurement below 5th percentile were considered to
have moderate and severe malnutrition respectively. Weight loss
exceeding 10% of ideal body weight also suggests malnutrition.35,37
The most commonly used laboratory parameters for routine
assessment of nutritional status are plasma concentrations of albumin,
transferrin, pre-albumin and other liver derived proteins.
Among the available biochemical nutritional indices, serum
albumin has been the most commonly used for the assessment of
nutritional status especially in maintenance haemodialysis patients.
The reasons for this include the routine availability of albumin measure
and the power of predicting clinical outcomes10,39. Several studies
have identified hypoalbuminaemia as the strongest predictor of

18
morbidity and mortality in the haemodialysis population40. Albumin
synthesis decreases in malnutrition, hypoalbuminaemia has been
reported to be a consequence of reduced food intake and serum
albumin levels are directly and strongly correlated with dietary protein
intake41,42,43. However, other studies have found no relationship
between protein intake and serum albumin levels44.
Recent literature has emphasized the influence of inflammatory
response on serum albumin concentration. Albumin is a negative acute
- phase protein and its synthesis is suppressed by inflammation
regardless of nutritional status. Thus the use of albumin to evaluate
nutritional status of ESRF patient does have limitation as serum
albumin levels can be affected by both malnutrition and inflammatory
reactions40. It must be emphasized that oedema and extracorporeal
losses may influence serum albumin levels. It is also important to note
that serum albumin varies according to the method of measurement
which include bromcresol green technique, bromocresol purple
technique, immunonephelometry.40 Serum pre- albumin has a shorter
half life than albumin, has a close relationship with nutritional status
and is a good predictor of clinical outcome. However, its levels are
elevated in ESRF patients even in the presence of malnutrition (because
of reduced filtration and diminished tubular metabolism). In conclusion
evidence suggests that pre-albumin is more sensitive than albumin.15,45
Serum transferrin has a short half life and may be a more

19
sensitive indicator of acute changes in protein metabolism. However, it
is influenced by iron status, infections and inflammation.8
The method of nutritional assessment that has been increasingly
used with wide popularity in both dialysis patients and in pre-dialysis
chronic renal failure patient is the Subjective Global Assessment
(SGA).10,40,46,47,48 It correlates well with the other nutritional markers in
patients with chronic renal disease.20,46,47 It was initially designed for
patients undergoing gastrointestinal surgery and is based on subjective
aspect of medical history and physical examination. It is a simple and
rapid method, reproducible, inexpensive, requires little training and its
measurement is focused on nutrient intake and body composition.
Briefly, the medical history focused on weight loss,
gastrointestinal symptoms (anorexia, nausea, vomiting and diarrhea)
and functional capacity related to nutritional status.
The physical examination focused on loss of subcutaneous fat
and muscle, the presence of ankle oedema and or ascites related to
nutritional status. SGA can identify patient as well, moderately and
severely malnourished.
Generally, patients are rated as severely malnourished when
they loose at least 10% of their body weight over 6 months. Moderately
malnourished patient loose at least 5% of their weight over 6 month
with modest physical sign of malnutrition such as subcutaneous
tissues loss. One potential draw back to the use of SGA is its

20
subjectivity which may reduce its reproducibility hence small difference
in SGA score must be interpreted with caution.
The objective monitoring of muscle mass or lean body mass
relies on the use of Dual Energy X-ray Absorptiometry (DEXA) which
is able to estimate bone minerals, fat and lean body mass distribution
directly.
The use of anthropometric method is an indirect and rather
insensitive measure of nutritional status because of errors including
the influence of hydration status. The result of anthropometry agrees
reasonably well with the result obtained by DEXA.69.
2.5 Consequences of Malnutrition In CRF.
Sub-optimal nutritional status has been associated with an
increased morbidity and mortality. Serum albumin below 3.5g/dl and
serum pre-albumin below 300mg/l have been shown to be independent
predictors of increased morbidity and mortality.
The multi-centre Canadian haemodialysis morbidity study
reported a direct correlation between the serum albumin level and the
morbidity and mortality rate in 486 haemodialysis patients8.
The French multi-centre study on 1600 patients confirmed a
significant influence of serum level of albumin and pre-albumin on
survival. Malnutrition increases the risk of serious infections and poor
responses to erythropoetin use. It has been proposed that malnutrition
may also contribute to cardiovascular disease that in turn is the main

21
cause of patient mortality. Various mechanisms have been proposed for
the increased cardiovascular morbidity and mortality. They include:
Malnutrition perse may markedly reduce myocardial mass and
the content of myofibrils and other functional elements
Low albumin levels may influence the generation of lipoproteins
associated with atherosclerosis as shown invitro in human
hepatoma cell-line
Accumulation of asymmetric dimethyl-l-arginine (ADMA), which is
an endogenous competitive inhibitor of nitric oxide (NO) synthase,
may inhibit nitric oxides induced vasodilatation, thus pre-
disposing to hypertension and cardiovascular disease. However,
it has been reported that ADMA levels are higher in ESRD (end-
stage renal disease) than in controls but always lower than the
concentrations that induce vaso constriction invivo8
Rational And Goals Of Nutritional Therapy: There are three major
goals for the nutritional therapy of patients with renal diseases.
1. To maintain good nutritional status
2. To arrest or retard further progression of renal failure.
3. To prevent or ameliorate uraemic toxicity and other metabolic
disorders that occur with advanced renal failure. Although the
evidence is not conclusive, data from clinical and experimental studies
indicate that a reduction of dietary protein and phosphate may retard
the progression of CRF. Diets for patients with renal disease are
designed to be low in protein and phosphorus contents. Such diet will

22
also reduce uraemic toxicity in patients with advanced renal failure48,49.
Large randomized controlled trials and meta-analysis were performed to
confirm the initial uncontrolled studies on the slowing effect of low
protein, low phosphorus diet on the rate of deterioration of renal
functions. However, the study was not conclusive.
Metabolic acidosis, hyperparathyroidism, renal osteodystroply,
hyperkalaemia, neuropathy as well as symptoms like fatigue, anorexia
and itching, are better controlled if the protein intake is low. This was
the main if not the only aim of nutritional treatment of uraemic patients
in the sixties. However, feeding a low protein diet to patients with renal
disease carries the risk of inducing malnutrition and it is now evident
that severe protein energy malnutrition (PEM) could be accelerated by
these restrictive diets8.
Cupisti et al conducted a cross sectional survey of 70 pre-
dialysis out-patients with severe CRF (GFR<15mls/min) being treated
with low protein diet (0.6g/kg/day) or a very low protein diet
(0.3g/kg/day) supplemented with essential amino acids and ketoacids.
They performed biochemistry, anthropometry, bioelectrical impedance
vector analysis (BIVA) and subjective global assessment (SGA) in the
patients. Values of anthropometry and BIVA were similar in patients
and controls. SGA scores showed a normal nutritional status (SGA-O)
in 50 patients (71.4%) and mild to moderate SGA abnormalities (SGA-1)
in 20 patients 28.6%). None had severe malnutrition49.The study
concluded that with a planned dietary regimen, severe or overt

23
malnutrition does not occur in pre dialysis CRF without other serious
illness. However, some mild to moderate subjective Global Assessment
(SGA) abnormalities were detected in association with a more severe
renal insufficiency, a lower serum bicarbonate, a higher serum urea
and dietary protein levels and were predictive of poor renal outcome.
The result of this study emphasizes the role of proper dietary
monitoring, correction of metabolic acidosis and clinical monitoring
including SGA in the pre- dialysis conservative care of CRF patients.49

24
CHAPTER THREE
3.0 Materials and Methods
3.1 Place of study
The study was carried out at the University of Benin Teaching
hospital (UBTH) Benin City, which is a 444 bedded tertiary hospital. It
has a renal unit that provides dialysis services. UBTH provides tertiary
health care to Edo State and her environs including Ondo, Delta,
Anambra, Kogi and Bayelsa States.
3.2 Type of study.
It was a prospective, observational and hospital based study.
3.3 Sample Population
The sample population was made up of consecutive chronic renal
failure patients on conservative treatment (pre-dialysis) attending
UBTH.
3.3.1 Inclusion Criteria
Chronic renal failure patients with a serum creatinine
persistently above 1.5mg/dl.
Patients above 18years of age.
Ultrasonographic findings of bilaterally shrunken kidneys or
normal sized kidneys with evidence of chronic renal failure.
The patients were recruited after obtaining informed consent

25
from them (and or relations where necessary), approval for the study
was obtained from the Ethical Committee of UBTH.
3.3.2 Exclusion criteria
Patients on maintenance dialysis (haemodialysis or peritoneal
dialysis).
Patients with clinical and biochemical evidence of nephrotic
syndrome
Chronic liver disease, infectious disease (Tuberculosis, HIV).
Evidence of malignancy.
Patients under 18 years of age.
Concomitant steroid therapy.
Unwillingness to give informed consent.
History of chronic illness.
3.3.3 Samples size
Fisher’s formular for determining sample size was used50.
This is;
n = Z2 Pq
d2
n= Minimum sample size
P- Prevalence of chronic renal failure in the population
q=1-p
z= 95% confidence interval =1.96

26
d= level of precision =0.05
n= 60
3.4 Materials and equipment
A total of 96 CRF patients who were not on dialysis therapy were
enrolled into the study.
3.4.1 Materials
1. Tape measure for mid arm circumference and triceps skin fold
thickness.
2. Sample bottles for the assessment of serum albumin, urea and
creatinine
3. Questionnaires
4. Needles and syringes.
3.4.2 Equipments
5. Refrigerator to store sample
6. Centrifuge machine to separate samples
7. Harpenden skin fold caliper.
8. Clinical weighing scale.
9. Ultrasound machine Sonoacee 1500 (medison) 3.5 MHz sector
probe was used This is a standard machine with good resolution
Renal ultrasound scan was carried out by an experienced sonographer

27
3.5 Nutritional status assessment
3.5.1 Patients and methods
A total of 96 consecutive CRF patients who had not commenced
dialysis therapy and attending UBTH were initially enrolled into the
study according to the inclusion criteria. Detailed history and physical
examination were done at the first contact with the patients to
ascertain whether the patients had features suggestive of CRF and also
whether the patients met the inclusion criteria. Majority of the patients
were referred to the consultant nephrologists with accompanying
results of ultrasound, urine and blood investigations, all of which were
repeated by me for certainty. Those with obvious exclusion criteria were
dropped from the study at this level. At the end of six months of study,
only 66 patients had been followed up. The drop-outs of the study were
those patients who commenced dialysis therapy before the end of six
months, those who died of complications from CRF, those who stopped
coming to clinic for unknown reasons and those who withdrew their
consent.
40 subjects who were aged and sex matched were recruited as
controls. These control subjects were the normal relations of patients
attending UBTH, hospital staff and subjects who came to UBTH for pre-
employment medical examinations. They were all subjected to the same
method of examination and follow-up as the CRF patients for six
months.

28
3.5.2 Study Design
A questionnaire was assigned (by me) to each of the patients who
met the inclusion criteria, to obtain the following information: age, sex,
occupation, marital status, level of education, the cause of chronic
renal failure, biochemical parameters, anthropometric parameter and
subjective global assessment.
They were subjected to clinical examination by me and were
taught how to fill in the food diaries. Subjective global assessment was
done for each of them, anthropometric and biochemical measurements
were also done at the time of enrolment for the study. The
questionnaire was pre-tested using 15 patients with chronic renal
failure.
Nutritional status was assessed using subjective global
assessment questionnaires, anthropometry and serum levels of
albumin.
3.5.3 Anthropometric measurement
The following indices were measured, body weight (kg), height
(metres), mid arm circumference (MAC), triceps skin fold thickness
(TSFT). BMI was calculated using the formula weight(kg)/height (m2).
Measurements were taken at the first visit and six months later. The
average values of each parameter was used for the analysis.

29
Weight:
A clinical weighing scale was used. Every subject was weighed
while standing still in the centre of the weighing scale platform, with
the patient not holding any object. Weights were recorded to the nearest
0.1kg. To determine the percentage weight loss of each patient, the
weight was taken at the time of enrolment into the study and at 6
months after the initial assessment.
Height:
The height was measured using a height scale built into the
weighing scale. The subjects heights were measured without foot wears.
They were instructed to stand on a flat surface with weight distributed
evenly on both feet, heels together and the head positioned so that the
line of vision is perpendicular to the body. The arms hanged freely by
the sides and the head, back, buttocks and the heels were against the
wall. The subjects were asked to inhale deeply and maintain a fully
erect position. The movable headboard brought onto the topmost point
on the head with sufficient pressure to compress the hair. The height
was recorded to the nearest 0.1cm.
The body mass index was calculated using the formula BM1=
weight (kg) /Height (m2). BMI value of less than 20 kg/m2 was regarded
as malnutrition in this study.

30
Triceps skin fold thickness measurement –
The triceps skin fold was measured in the mid line of the
posterior aspect of the arm, over the triceps muscles at a level half way
between the lateral projections of the acromium process and the
olecranon process at the elbow joint. With the elbow flexed to 900, the
mid point was determined by measuring the distance between the two
land marks using a tape measure which was marked on the side of the
arm.
The subjects were measured while standing with the arm
hanging loosely and comfortably at the side. The harpenden caliper was
held in the right hand. A vertical fold of skin and subcutaneous tissue
was picked gently with the left thumbs and index finger approximately
1cm proximal to the mark level, and the tips of the caliper applied
perpendicular to the skin fold at the marked level. Measurements were
recorded to the smallest unit of graduation. The left arms of the
patients were used. TSFT values of less than 10mm in men and of less
than 13mm in women were regarded as malnutrition in this study.
The mid-upper arm circumference:
This was measured with a measuring tape, mid way between the
olecranon process of the ulna and the tip of the shoulder of the left
arm. MUAC values of less than 22cm in women and less than 25cm in
men were considered as malnutrition in this study.

31
3.5.4 Subjective Global assessment
The subjective global assessment was performed by one observer
for all patients. SGA refers to the overall evaluation of a patient by an
experienced clinician. This is based on medical history and physical
examination described by Detsky et al48
Review of the medical history included an assessment of weight
and weight change, dietary intake, gastrointestinal symptoms, disease
state and the patient’s functional capacity related to nutritional status
The physical examination focused on loss of subcutaneous fat
and muscle, the presence of ankle oedema and ascites related to
nutritional status were evaluated. All these features were categorized as
normal O, mild (1+) moderate (2+), severe (3+). On the basis of
subjective weighting of the data of medical history and physical
examination the patients were classified into three group “A” well
nourished, “B” mild/moderately malnourished, “C” severely
malnourished.
3.5.5 Dietary Assessment:
Protein intakes were estimated from 3 – day food diaries in the
week of first contact with the patient.(food intakes were recorded at
2days interval). With the assistance of the hospital dietitian, using a
table of nutrient, due instruction was given to every patient on how to
measure his/her food ration.

32
3.6 Estimation of glomerular filtration rate:
The GFR was calculated using the 6-variable MDRD study
formula by Levey and colleagues51. This formula is unique as it takes
into consideration age, race, gender, serum albumin, serum creatinine
and serum urea nitrogen. Using this formula, GFR = 170 x (Scr) – 0.999 x
(Age,yr) – 0. 176 x 0.762 (If patient is a female) or x 1.18 (if Patient is black)
x (SUN) -0.17 x (alb) + 0.318. For ease of calculation a commercially
available software for renal multi-calculation was used to arrive at the
final GFR.
3.7 Sample collection
Blood samples were taken on two occasions after an over night
fast from an ante – cubital vein for the assessment of serum albumin,
creatinine and urea. The average serum albumin was used for the
analysis.
3.8 Analysis of the sample
The serum creatinine was analysed using Jaffe’s reaction71 while
the serum urea was analysed using Urease Bethaloth method72.
3.8.1 Determination of serum Albumin
Bromocresol green (BCG) method was used to analyse serum
albumin73.

33
Procedure.
Both reagents and samples were brought to room temperature.
Three test tubes labeled Blank (BL), standard (Std) and sample (SA)
were arranged on the stand.
To each of the test tubes was pipetted l ml (1000μl) of the
reagent, the solution was well mixed and incubated for approximately
10minutes at 20 – 25oc. The absorbance against reagent blank was
read within 60 minutes.
Calculation of Albumin in g/dl
= Absorbance of test x concentration of Std
Absorbance of Std
Normal serum albumin was taken as 3.5 – 5.2 g/dl.
Test principle:
The procedure is based on the binding of bromcresol green (BCG)
to albumin. The intensity of the blue-green colour produced in the
reaction is proportional to the concentration of albumin in the sample.
3.8.2 Determination of malnutrition:-
A patient was considered malnourished in this study with two or
more of the following nutritional parameters52.
1. Weight loss of >10% at 6 months of follow-up.
2. Overall subjective global assessment score of B or C.

34
3. BMI < 20kg/m2.
4. Mid upper Arm circumference less than 22cm in females and
25cm in males.
5. Triceps skin fold thickness less than 10mm in males and < 13mm
in females.
6. Serum albumin Concentration < 3g/dl.
3.8.3 Statistical analysis.
Data obtained from the study were analyzed using Statistical
Package for Social Sciences (SPSS) version 13.0. Descriptive statistics
such as means and ranges or variables of interest were computed.
Statistical comparison of the arithmetic means was determined using
Student’s t- test.
Comparison of percentages or proportion was done using
Chi–square test. Pearson’s correlation coefficient was used to determine
the relationship between malnutrition and renal function. A p value <
0.05 was considered to be significant.

35
CHAPTER FOUR
4.0 RESULTS
4.1 CHARACTERISTICS OF THE SUBJECTS STUDIED
A total of 96 patients were enrolled into the study. 66 of them
were evaluable. This was made up of 45 (68%) males and 21(32%
females). 40 aged and sex matched controls made up of 21 (53% males)
and 19 (47% females) were also studied. The age range of CRF patients
was 23 to 65 years with a mean of 47.1 + 13.2 years while controls were
also aged between 23 and 65 years with a mean of 44.1 + 14.3 years.
Table 1 shows the characteristics of both the CRF and control
group. The mean age of CRF patients (47.1 + 13.2 years) was not
significantly different from the control of 44.1 + 14.3 years. (p > 0.05).
The mean serum creatinine of CRF patients and control were 3.47
+ 1.7mg/dl and 0.82 + 0.13mg/dl respectively and this difference was
statistically significant. (p < 0.05).
The mean serum albumin of CRF patients and control were 3.6 +
0.7g/dl and 4.3 + 0.4g/dl respectively. There was a statistically
significant difference between the means (p = 0.0001).
The mean GFR of CRF patients (23.9 + 10.8 mls/min) was
significantly lower than the GFR of 115.5 + 16.7 mls/min in the control
subjects. (p = 0.0001).
The mean BMI of CRF patients and control were 24.4 + 3.1kg/m2
and 24.7 + 3.3kg/m2 respectively and this difference was not
significant.

36
The mean MUAC of CRF patients (27.8 + 3.8cm) was significantly
lower than the MUAC of 29.5 + 3.4cm in the control subjects (p = 0.02).
TABLE 1: CHARACTERISTICS OF CRF PATIENTS AND CONTROL
GROUP
CHARACTERISTICS
CRF PATIENTS
n =66 MEAN ±SD
CONTROL GROUP n=40
MEAN ±SD P VALUE
SEX M 45(68.2%)
F 21 (31.8%)
M 21(52.5%)
F 19(47.5%)
-
-
AGE (yrs) 47.1± 13.2 44.1 ± 14.3 > 0.05
UREA(mg/dl) 120.1 ± 44.2 27.8 ± 6.1 < 0.05
SERUM
CREATININE (mg/dl)
3.47 ± 1.7 0.82± 0.13 < 0.05
SERUM ALBUMIN
(g/dl) 3.6 ± 0.7 4.3 ± 0.4 0.0001
TSFT(mm) 11.1±4.3 14.0 ± 4.3 0.001
MUAC (cm) 27.8± 3.8 29.5 ± 3.4 0.02
GFR(ml/min) 23.9 ±10.8 115.5 ± 16.7 0.0001
AVERAGE DAILY
PROTEIN
INTAKE(gm/day)
36.7± 8.3 45.6 ± 5.2 0.0001
BMI(kg/m2) 24.4±3.1 24.7± 3.3 0.508

37
Table 2 shows the glomerular filtration rate of subjects using
MDRD formula. Out of the 66 patients studied, 19 (29%) were in stage
3 CRF, 35 (53%) were in stage 4 CRF, and 12 (18%) were in stage 5
CRF. The mean GFR of the CRF patients and controls were 23.9 + 10.8
mls/min and 115.5 + 16.7 mls/min respectively (P value 0.0001). All
the control subjects had GFR > 89mls/min.
TABLE 2: GLOMERULAR FILTRATION RATE OF CKD PATIENTS
AND CONTROL USING MDRD
Stages of CKD Stage 3 Stage 4 Stage 5 Total Control
n=40
N=66 (%) 19(28.8) 35 (53.0) 12 (18.2) 66 (100) -
GFR (by MDRD)
ml/min/1.73m2
30-59 15-29 <15 - > 89

38
Table 3 shows the stages of CKD by duration of illness. Out of the
66 patients that were evaluable, 29 (43.9%) were ill for less than 3
months, among these 18 (62.1%) were in stage 4 CKD, 37 (56.1%) were
ill for not less than 3 months of which 17 (45.9%) were in stage 4 CKD.
There was no statistically significant difference between the stages of
CKD and the duration of illness (X2 = 2.570, p = 0.277).
TABLE 3: STAGE OF CKD BY DURATION OF ILLNESS
Duration of
illness
Stage of CKD
Total X2
p
value Stage 3 Stage 4 Stage 5
<3 Months 8(27.6%) 18(62.1%) 3(10.3%) 29(100.0%)
2.570 0.277 3 Months
and above
11(29.7%) 17(45.9%) 9(24.3%) 37(100.0%)
Total 19(28.8%) 35(53.0%) 12(18.2%) 66(100.0%)

39
4.2 NUTRITIONAL STATUS ASSESSMENT.
Table 4 shows the proportion of malnourished CRF patients and
control by nutritional indices.
Out of the 66 CRF patients studied, 4 lost > 10% of their body
weight at the end of 6 months of follow-up. There was no significant
weight loss in the control population.
The BMI was low (< 20kg/m2) in 8 (12.1%) of CRF patients, while
3 (7.5%) subjects in the control population had BMI of < 20kg/m2.
The serum albumin was less than 3g/dl in 7 (10.6%) of the CRF
patients, no subject in the control population had serum albumin
concentration of < 3g/dl.
SGA identified malnutrition in 30 (46%) of CRF patients and no
subject amongst the control population was malnourished by SGA

40
TABLE 4: DISTRIBUTION OF MALNOURISHED PATIENTS AND
CONTROL BY INDICES OF MALNUTRITION.
Indices of
Malnutrition
CRF PATIENTS
n=66(%)
Control
Population=40(%)
x2 P value
A WEIGHT.
No. With weight loss
>10% over 6 months.
4 (6.1)
0 (0)
2.519
0.112
B BMI < 20kg/m2 8 (12.1) 3 (7.5) 0.572 0.450
C TSFT
males <10mm
Female <13mm
34 (51.5)
9 (22.5)
8.697
0.003
D Serum Albumin
< 3g/dl
7 (10.6)
0 (0)
4.452
0.033
E MUAC
Male< 25cm
Female < 22cm
15 (22.7) 3 (7.5) 4.096 0.043
F SGA. 30 (45.5) 0 (0) 25.359 0.00001
G 2 or more criteria 28 (42.4) 5 (12.5) 14.994 0.001

41
A: Nutritional status by SGA criteria
Table 5 shows that out of 66 patients studied, 36 (54%) were well
nourished, 25 (38%) were mild/moderately malnourished and 5 (8%)
severely malnourished using SGA criteria. No subject in the control
population was malnourished. Thus, 36 patients were well nourished
while 30 (46%) of the patients were malnourished by this criteria.
TABLE 5: NUTRITIONAL STATUS BY SGA CRITERIA
SGA CRF PATIENTS n= 66
n (%)
CONTROL n = 40
n (%)
Well nourished 36 (54.5) 40 (100)
Mild/Moderately malnourished 25 (37.9) -
Severely malnourished 5 (7.6) -

42
Table 6 shows the stages of CRF by degree of malnutrition using
SGA. In the mild/moderately malnourished group, 1 (5%) was in stage
3 CRF, 19 (54%) in stage 4 CRF and 5(41%) were in stage 5 CRF.
Table 7 shows SGA of CRF patients and control by age group
distribution. In this study mild/moderate malnutrition was common in
the 40 – 49 years age group which was the predominant age group
affected by CRF while severe malnutrition was found in the 60 years
and above age group.
In the control population, all were well nourished by SGA criteria.
7 of them were in the age group < 30 years, 13 of them were in the age
range 30 – 39 years, 5 were in the age range 40 – 49 years, 6 were in
the age range 50 – 59 years and 9 of them were in the 60 years and
above age group.

43
TABLE 6: STAGES OF CHRONIC KIDNEY DISEASE BY DEGREE OF
MALNUTRITION USING SGA
Stage of CKD
SGA
Well nourished n=36 Mild/moderately
Malnourished n=25
Severely
Malnourished n=5
n (%) n (%) n %
Stage 3 18 (94.7) 1 (5.3) 0 (0)
Stage 4 16 (45.7) 19 (54.3) 0 (0)
Stage 5 2 (16.7) 5 (41.7) 5 (41.7)
Total 36 (54.5) 25 (37.9) 5 (7.6)

44
TABLE 7: SGA OF CRF PATIENTS AND CONTROL BY AGE GROUP
DISTRIBUTION
SGA
Age Group
Total
n=66
x2
P
value
<30
n=12
(%)
30 – 39
n=7
(%)
40 – 49
n=18
(%)
50 - 59
n=14
(%)
>60
n=11
(%)
Sample Well
nourished
6(50.0)
3 (43.0)
9 (50.0)
9 (64.0)
9 (60.0)
36(54.5)
4.230
0.865 Moderately
malnourished
6(50.0)
3 (43.0)
8 (44.0)
4 (29.0)
4 (27.0)
25(37.9)
Severely
malnourished
(0)
1(13.0)
1 (6.0)
1 (7.0)
2 (13.0)
5 (7.6)
Control Well
nourished
7(100)
13 (100)
5 (100)
6 (100)
9 (100)
40(100)

45
Table 8 shows the characteristics of the 5 patients in stage 5 CRF
who were severely malnourished by SGA criteria.
The 5 severely malnourished patients were all in stage 5 CKD (GFR <
15mls/min), 2 of them had serum albumin concentration of at least
4.0g/dl. The percentage weight loss was significant (> 10%) in 4 of
these patients.
TABLE 8: CHARACTERISTICS OF THE 5 PATIENTS IN STAGE
5 CRF THAT WERE SEVERELY MALNOURISHED BY SGA
CRITERIA.
BMI
(Kg/m2)
Serum
albumin
(gm/dl)
SGA TSFT
(mm)
MUAC
(cm)
GFR
(ml/min)
Percentage
Weight loss
27.64 4.40 C 8.80 26 13.72 4.8
22.66 2.90 C 6.0 24 13.19 12.60
15.87 4.00 C 4.0 23 13.34 11.3
24.46 2.90 C 8.40 24 13.08 10.8
18.69 2.8 C 7.0 24 12.95 12.20

46
Nutritional status assessment by other nutritional indices.
B. Body mass index
BMI of the CRF patients and controls were 24.4 + 3.1kg/m2 and
24.7 + 3.33kg/m2 respectively, there was no significant difference in
their means (P > 0.05), table 1.
Using BMI as a nutrition marker 8(12%) of CRF patients were
malnourished and 58 (88%) were well nourished, while among the
controls 3(8%) were malnourished and 37 (92%) were well nourished.
The difference in the level of nutrition in CRF patients and controls was
not significant (x2 = 0.572, P = 0.450), table 4.
The mean BMI of well nourished (25.97 + 2.22kg/m2) CRF
patients was significantly higher than the BMI of 22.31 + 2.79kg/m2 in
malnourished patients (P = 0.0001) table 9.
There was a statistically significant correlation between BMI and
the GFR (r = 0.3 p = 0.042), such that the BMI decreases with
progressive deterioration in renal function.
C: Triceps skin fold thickness
As in table 4, 34(51.5%) patients were malnourished by this
criterion and of this 25(37.9%) were males and 9(13.6%) were females.
In the control population only 9(22.5%) subjects were malnourished,
and of this 8(20%) were males and 1(2.5%) was a female. As shown in
table 1, the mean TSFT for CRF patients and controls were 11.14 +

47
4.3mm and 14.03 + 4.3m respectively, there was a statistically
significant difference between both means. (p = 0.001). The mean TSFT
of well nourished (13.19 + 4.31mm) CRF patients was significantly
higher than the TSFT of 8.69 + 2.85mm in malnourished patients (P =
0.0001) table 9.
There was a positive correlation between TSFT and the GFR (r =
0.2, p = 0.178) as the renal function diminishes, the TSFT also
decreases.
D: Mid upper arm circumference
MUAC of the CRF patients and controls were 27.8 + 3.8cm and
29.5 + 3.4cm respectively, and this difference was statistically
significant (P = 0.02) as shown in table 1. Using MUAC as a nutrition
marker 15 (23%) of CRF patients were malnourished and 51 (77%) were
well nourished while amongst the control 3(8%) were malnourished
and 37(92%) were well nourished. The difference in the level of nutrition
in CRF patients and controls was significant (x2 = 4.096, P = 0.043),
table 4.
The mean MUAC of well nourished (29.66 + 3.20cm) CRF
patients was significantly higher than the MUAC of 25.56 + 3.34cm in
malnourished patients (P = 0.0001), table 9.
There was a positive correlation between the MUAC and the GFR
(r = 0.2, p = 0.105) such that there was worsening of MUAC with
progressive renal insufficiency.

48
E: Weight loss.
As shown in table 4, only 4 (6%) patients were malnourished by
this criterion having lost > 10% of their body weight at the end of the
study, while 62(94%) were well nourished and there was no significant
weight loss in the control group during the six months of follow up.
The mean percentage weight loss of the well nourished and
malnourished patients were 1.5 + 2.62% and 3.71 + 4.14% respectively
(Table 9) and this difference was statistically significant (P = 0.011).
There was a negative correlation between the percentage weight loss
and GFR (r = -0.4, p = 0.002) such that the percent weight loss
increases with decreasing renal function.
F: Serum albumin.
Serum albumin concentration of the CRF and controls were 3.6 +
0.7g/dl and 4.3 + 0.4g/dl respectively and these difference was
statistically significant (P = 0.0001) Table 1. Using serum albumin as a
nutrition marker, 7(11%) of CRF patients were malnourished, 59(89%)
were well nourished, while no subject amongst the control was
malnourished using this criterion. The difference in the level of
nutrition in CRF patients and controls was significant (x2 = 4.452, p =
0.03) Table 4. There was no significant difference between the mean
serum albumin concentration of the well nourished (3.96 + 0.61g/dl)
CRF patients and the malnourished (3.65 + 0.67g/dl) CRF patients.

49
Table 9. There was a positive and significant correlation between the
serum albumin concentration and the GFR (r = 0.4, p = 0.001).
G: Two or more criteria
As in table 4, using two or more nutritional parameters to classify
patients as being malnourished, 28(42%) CRF patients were
malnourished while in the control population 5(13%) of the subjects
were malnourished. Of all the nutrition markers, TSFT recorded the
highest proportion of malnourished patients in the CRF population
34(52%), followed by SGA 46%, MUAC 23% and BMI 12%. While serum
albumin and weight loss recorded the least (11% and 6% respectively).
The use of percentage weight loss as a criterion for determining
malnutrition recorded the least number of CRF patients in pre-dialysis
stage. The 4 patients that recorded significant weight loss in this study
were all in stage 5 CRF with GFR below 15mls/min. Table 8.

50
Table 9 Shows the comparison of anthropometric and biochemical
characteristics between well nourished and malnourished CRF patients
before dialysis therapy.
The mean BMI of the well nourished and malnourished CRF
patients were 25.97 + 2.22kg/m2 and 22.31 + 2.79kg/m2 respectively,
and the difference was statistically significant. (p = 0.0001).
There was no significant difference between the mean serum
albumin concentration of the well nourished (3.96 + 0.61g/dl) CRF
patients and malnourished (3.65 + 0.67g/dl) CRF patients. (P = 0.056).
The mean GFR of the well nourished and malnourished CRF
patients were 29.74 + 11.20mls/min and 17.08 + 4.15mls/min
respectively. The difference in the mean GFR was significant (p =
0.0001).
The mean percentage weight loss of malnourished (3.71 + 4.14%)
CRF patients was significantly higher than the percentage weight loss of
1.50 + 2.62% in the well nourished patients (p = 0.011).
The mean MUAC of well nourished and malnourished CRF
patients were 29.66 + 3.20cm and 25.56 + 3.34cm respectively. The
difference was significant (p = 0.0001).

51
TABLE 9: COMPARISON OF ANTHROPOMETRIC AND
BIOCHEMICAL CHARACTERISTICS BETWEEN WELL NOURISHED
AND MALNOURISHED CHRONIC RENAL FAILURE PATIENTS
BEFORE COMMENCEMENT OF DIALYSIS THERAPY
Indices
Well nourished
n=36
Malnourished
n=30 t value P value
BMI (kg/m2) 25.97±2.22 22.31±2.79 5.928 0.0001
TSFT (mm) 13.19± 4,31 8.69± 2.85 4.898 0.0001
MUAC (cm) 29.66± 3.20 25.56±3.34 5.068 0.0001
Mean average
daily protein
intake (gm)
41.55±6.04 30.82± 6.67 6.842 0.0001
Serum Albumin
(g/dl) 3.96± 0.61 3.65±0.67 1.945 0.056
GFR (ml/min) 29.74 + 11.20 17.08±4.15 5.85 0.0001
Weight (kg) 73.73±9.85 62.68±9.78 4.54 0.0001
Serum urea
(mg/dl)
95.08±36.2 150.2±32.72 - 6.42 0.0001
Serum creatinine
(mg/dl) 2.92±1.15 4.12±0.96 - 4.54 0.001
Weight loss (%) 1.50±2.62 3.71±4.14 - 2.62 0.011

52
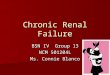
4.3 PROTEIN INTAKE
The mean average daily protein intake for CRF patients and
controls were 36.67 + 8.27gm/day and 45.35 + 5.21gm/day
respectively. (P value 0.0001, (table 2). The mean average daily protein
intake in the various stages of CRF is represented by figure 1. The
mean average daily protein intake of patients in stage 3 and 4 were
44.05 + 25 gm/day and 36.03 + 5.92gm/day respectively, while the
mean average daily protein intake of patients in stage 5 was 26.85 +
8.16gm/day. Patients in stage 3 and 4 CRF had more protein intake
than the patients in stage 5 CRF. This difference in average daily
protein intake at each stage of CRF was statistically significant (p =
0.0001). Thus daily protein intake decreases as the renal function
worsens with the patient in ESRF taking the least quantity of protein.
The mean average daily protein intake of the well nourished and
malnourished CRF patients were 41.5 + 6.04 gm/day and 30.82 + 6.67
gm/day respectively, (P = 0.0001). There was a positive and significant
correlation between the average daily protein intake and the serum
concentration of albumin (r = 0.4, P = 0.0001), such that the serum
albumin may be low as daily protein intake decreases.

53
Stage 5Stage 4Stage 3
Stage of CRF
50.00
40.00
30.00
20.00
10.00
0.00
Mean
Avera
ge d
aily p
rote
in in
take
26.85
44.05
36.04
FIGURE 1: MEAN AVERAGE DAILY PROTEIN INTAKE BY STAGE
OF CRF
f = 30.878
p = 0.0001
(gm
)

54
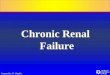
Figure 2 shows the mean average daily protein intake of CRF
patients and control by degree of malnutrition.
The mean average daily protein intake of the well nourished and
mild/moderately malnourished CRF patients were 41.55 + 6.04gm/day
and 32.77 + 5.46gm/day respectively, while the mean average daily
protein intake of the severely malnourished CRF patients was 21.07 +
1.40 (figure 2). The mean average daily protein intake of the control
population was 45.35 + 5.22 gm/day. There was a statistically
significant difference between the mean average daily protein intake of
the well nourished CKD patients and control group (t = -2.943, p =
0.004).
The severely malnourished and mild/moderately malnourished
CRF patients had less protein intake than the well nourished patients.
The mean average daily protein intake at each level of malnutrition was
statistically significant (f = 38.579, p = 0.0001) (figure 2).
Protein intake reduced as the degree of malnutrition worsens,
patients who were severely malnourished had the least protein intake.

55
FIGURE 2: MEAN AVERAGE DAILY PROTEIN INTAKE OF CRF
PATIENTS AND CONTROL BY DEGREE OF MALNUTRITION
Severly MalnourishedMild/ModeratelyMalnourhised
Well Nourished
SGA
50.00
40.00
30.00
20.00
10.00
0.00
Mean
Avera
ge d
aily p
rote
in in
take (
gm
)
45.35
21.07
32.77
41.55
Control
Sample
Identificaiton

56
CHAPTER FIVE
5.0 DISCUSSION
The prevalence of malnutrition in Nigerians with chronic renal
failure before the initiation of dialysis therapy has not received enough
attention and has not been well characterized. This report highlights
the prevalence of malnutrition before the initiation of dialysis therapy
and its relationship with renal insufficiency. Majority of the patients in
this study (53%) were in stage 4 chronic kidney disease (CKD), this
suggests that a large proportion of patients with undiagnosed CKD are
progressing to ESRF in our population. The few number of patients in
stage 5 CKD in this prospective study suggests that our patients with
CKD present late in end-stage when they are in need of dialysis
therapy.53, 54, 55, 61
This trend of patients population distribution in the various
stages of CKD is quite different from what is reported in developed
countries. Epidemiological data from the United States suggest that
ESKD constitutes a barely visible tip of an enormous ice berg of chronic
kidney disease. According to the NHANES III estimates, 64% of CKD
patient are in stage 1, 31% in Stage II, 4.3% in stage III, 0.2% in stage
IV and only 0.02% in stage V56.
The large population of patients( 64%) in stage 1 in developed countries
is a pointer to the effectiveness of early detecting tool and population
screening exercise which has not been fully established in most
developing countries in Africa.

57
The main findings of the study are (1) Malnutrition is prevalent in
our CRF patients even before the commencement of renal replacement
therapy, (2) Worsening of nutritional status with progression of renal
insufficiency and (3) Serum albumin is a poor detector of malnutrition
when compared with the subjective global assessment.
Malnutrition is common in our chronic renal failure patients
before the commencement of renal replacement therapy, it was found in
46% of the patients studied. Malnutrition is a common problem in
chronic renal failure patients. However, when compared with patients
on renal replacement therapy (haemodialysis and peritoneal dialysis),
the prevalence of malnutrition is low in pre-dialysis patients but the
value is still significantly high23,59. At least three previous international
studies have used subjective global assessment (SGA) to assess
nutritional status before the start of renal replacement therapy with a
prevalence of mild to moderate malnutrition ranging from 28% to
74%39,60,61. The finding of predominantly mild to moderate degree of
malnutrition in my study also agrees with the results of these studies.
Hitherto, only one local study has been carried out to determine
the prevalence of malnutrition in CRF patients before the initiation of
dialysis therapy. The result of this study compares strongly with that of
Agaba et al who reported 43% prevalence of malnutrition using the
body mass index (BMI) and serum proteins23. Francisco et al66 in their

58
study of uraemic symptoms, nutritional status and renal function in
pre-dialysis end stage renal failure patients found 64% patients
without malnutrition, 31% had mild to moderate malnutrition and 5%
had severe malnutrition66, this result compares with my finding of 54%
well nourished, 38% mild to moderate malnourished and 8% severely
malnourished. They also reported worsening of nutritional status with
diminishing renal function. The findings of Maarten et al67 on renal
function and nutritional status at the start of chronic dialysis treatment
using SGA revealed that 64% of the patients had a normal nutritional
status, 33% had mild to moderate malnutrition and 3% had severe
malnutrition. My findings also agree with that of CANUSA study67,
where 45% of the patients were well nourished using SGA at base line,
51% had mild to moderate malnutrition, and 4% were severely
malnourished.
Although malnutrition is prevalent in our CRF patients, it is
however predominantly mild to moderate. Severe malnutrition was not
common in this study and it was only encountered in a few patients
who were already in ESRF and were in need of renal replacement
therapy. The nutritional parameters of patients in this category
compare to a large extent with that seen in patients on dialysis therapy.
Malnutrition according to the use of SGA cuts across all the stages of
CKD. When compared with the result of the work done by Limman , 59
the prevalence is lower in pre-dialysis population of patients, this

59
observed higher prevalence may be due to the inclusion of dialysis
patients.
The results of this study suggest that the progression of renal
failure from stages 3 to stage 5 is associated with spontaneous decrease
in dietary protein intake and thus most nutritional indices in CRF
patients worsen as the GFR and dietary protein intake decrease.
Patients in stages 4 and 5 CKD were more malnourished than those in
stage 3 CKD. These patients in stages 4 and 5 CKD also had less
protein intake and this is worse with patients in stage 5 CKD.
These observations agree strongly with the findings of Ikizler et
al65 that progression of renal failure is associated with spontaneous
decrease in dietary protein intake, especially below creatinine clearance
of 25mls/min and that nutritional status worsens as creatinine
clearance and dietary protein intake decrease.
Kopple et al13 in their study on the evaluation of nutritional status
of patients that participated in the feasibility phase of MDRD study
reported that patients who are not in need of maintenance dialysis
treatment , in general, do not suffer from malnutrition. The findings of
my study contradict the initial observation of Kopple et al as
malnutrition was seen in our CRF patients even before the
commencement of dialysis therapy. However, it was predominantly
mild to moderate. The findings of a positive correlation between
worsening of nutritional indices and GFR reduction in my study agrees
with that of Kopple et al at the end of their follow up study.

60
There were variations in the ability of the different nutritional
tools to detect malnutrition when compared with the use of subjective
global assessment. The use of triceps skin fold thickness over estimated
patients with malnutrition. The use of two or more nutritional criteria
as well as MUAC compare favorably with SGA in detecting malnutrition.
The use of percentage weight loss and serum albumin were the least in
detecting malnutrition followed by the body mass index. This means
that the use of significant weight loss in pre-dialysis CRF patients has a
limited value in detecting malnutrition when compared with patients on
maintenance haemodiaysis. Infact, the four (4) patients with weight loss
in excess of 10% were those in ESRF who were in need of dialysis
therapy.
There was no significant difference between the mean serum
albumin concentration of the well nourished and malnourished
patients. The mean serum albumin concentration of the well nourished
and malnourished group was similar (3.9g/dl and 3.6g/dl, respectively)
and a considerable overlap of albumin values were observed. Further
more the mean serum albumin concentration of the two groups were
greater than the lower limit of 3.5g/dl.
Infact, in this study it was observed that amongst the patient
classified as severely malnourished by SGA, two (2) out of five (5) of
them had serum albumin concentration of at least 4.0g/dl which
confirms what was previously reported by Kenneth et al63. The
sensitivity of albumin in detecting malnutrition assessed by SGA in our

61
study was low. In fact, using 3.5g/dl as the cut off point, the sensitivity
was only 12.1% which compares with the findings of Nelma et al53 of
14.3% sensitivity using the same cut off point. For this reason some
authors have questioned the wide normal range of albumin levels.63
This poor sensitivity of albumin in identifying malnutrition might be
explained by its large body pool and long half life, which makes this
protein a late marker of malnutrition
Although serum albumin remains the most commonly used
parameter for the assessment of nutritional status in CRF patients, my
findings suggest its lack of sensitivity in detecting mild to moderate
malnutrition when SGA was considered for the analysis. The results of
this study agree with earlier reports that serum albumin has limited
value as a marker of nutritional status as previously reported40,44,62,64.
Serum albumin did not discriminate malnourished and well nourished
CRF patients thus, the use of albumin as a single nutritional marker
could delay an early nutritional intervention in malnourished patients.
This finding emphasizes the importance of associating albumin with
other nutritional parameters to correctly evaluate the nutritional status
of CRF patients. The discordance between the use of serum albumin
and clinical assessment SGA reflects limitations in both measures as
markers of nutritional status.
The SGA has some limitations as a measure of nutritional status
and some of this limitations probably also accounted for the poor
concordance between albumin levels and SGA ratings63. First SGA was

62
designed to enhance specificity at the expense of sensitivity. Second the
SGA does not allow for the categorization of mild malnutrition. Third,
the SGA focus on chronic nutritional changes instead of acute changes.
As a result of these three limitations it is possible that patients with
clinically important malnutrition may not be recognized using SGA.
It is therefore likely that hypoalbuminaemia may identify some patients
with malnutrition that would not be identified by clinical examination.
Another potential limitation of the SGA is that it was initially developed
in surgical patients and most of the data documenting its reliability and
validity are drawn from this population63.

63
CHAPTER SIX
6.0 CONCLUSION AND RECOMMENDATION
6.1 Conclusion
Earlier it was thought that patients who were not on maintenance
dialysis therapy (haemodialysis or petritoneal dialysis) were not
malnourished but more recent reports suggest that malnutrition is a
problem in them.
The findings of this study suggest that malnutrition is prevalent
in our CRF patients. Few of the studies done in the past on pre-dialysis
patients were essentially on ESRF patients but this study included the
other stages of CKD, moderate to severe stages 3 to 5 CKD thus giving a
wider insight into malnutrition in CKD patients. The results showed
that malnutrition in CKD starts before ESRF however, it is mild to
moderate which has the propensity to progress to severe malnutrition if
early and appropriate intervention was not made as the renal function
worsens.
The nutritional status of these patients at the start of dialysis
therapy is a strong predictor of their morbidity and mortality while on
maintenance dialysis. The study has also shown that many more
subjects (undiscovered) with early CKD are in our population as
evidence by the large percentage of patients in stages 3 and 4 CKD.
Serum albumin did not discriminate between malnourished and well
nourished CRF patients. In effect the reliance on serum albumin as the
sole determinant of malnutrition could delay an early nutritional

64
intervention in malnourished CRF patients. It is therefore wise to
associate serum albumin with other nutritional indices in order to
detect early malnutrition. Both serum albumin and SGA are not
without their limitations as measures of nutritional status, clinically
based assessment is still proven to be the best method of assessment.
When compared with SGA the use of weight loss as a marker of
malnutrition in predialysis CRF Patients has a limited value as it could
not detect malnutrition in the early stages of CKD but i still considered
it’s use relevant especially in the late stage of CKD and in patients on
maintenance dialysis therapy who are more prone to weight loss.

65
6.2 RECOMMENDATIONS.
1. The assessment of the nutritional status of our CRF patients
should form part of the general evaluation and care of these
patients, and when malnutrition is detected, early nutritional
intervention is recommended
2. A competent skilled dietitian is an indispensable part of the
management team.
3. The use of multiparametric method of nutritional assessment
should be encouraged rather than the use of serum albumin as
the sole determinant of nutritional status in chronic renal failure
patients.
4. Similar studies of this nature should be carried out in other
centers in Nigeria.
5. There is need to emphasize on community population screening
for chronic kidney disease for the benefit of early detection and
intervention.
6. Expensive kits for assessing malnutrition should be subsidized
and readily available.

66
LIMITATIONS OF THE STUDY
The study had some limitations listed below.
1. Patients drop outs of the study that could not be followed up for 6
months as a result of death, initiation of dialysis therapy in emergency
situation and lack of clinic attendance.
2. A very reliable biochemical marker of malnutrition such as serum
transferrin kit was not available at the time this study was carried out.
3. The study was limited to our centre and therefore may not be a
true reflection of the situation in other centers.
4. Albumin levels may also have differred if measured in different
centers or by different methods; in this study the popular bromocresol
green was used.
5. The average daily protein intake may not be truly representative of
what the patients took as this could be falsified.

67
REFERENCES
1 National Kidney Foundation-k/DOQI. Clinical practice guidelines
for chronic kidney disease; Evaluation, classification and
stratification. Am.J.Kidney Dis 2002;39(suppl 1): S1-266
2. Baker L.R.I. Renal disease. In: Clinical Medicine. Published by
W.B. Saunders. Pgs 572-573, 1999; 4th edition. London.
3. Oyediran A.B.O. Akinkugbe O.O. Chronic renal failure in Nigeria.
Trop. Geogr. Med. 1979; 22: 41-44.
4. Akinsola W, Odesanmi W.O, Ogunniyi J.O. Oladipo G.O.N.
Diseases causing renal failure in Nigeria, a prospective study of
100 cases. Africa J. Med. Sc. 1989; 18:131-5
5. Adetuyibi A, Akisanya J.B. Onadeko B.O. Analysis of the cause of
death on the medical wards of UCH, Ibadan over a 14 year period
(1960-1973). Trans. Roy. Soc.Trop. Med. Hyp. 1976; 70:466-473.
6. Sanusi A.A., Ekwere T.R. Adelekun T.A. Akinsola A. Magnitude of
the problem of chronic renal failure in Nigeria. A survey of
experience from renal centre, paper presented at the 9th annul
scientific conference of Nigeria association of nephrology, feb.
1997.
7. Parmar M S;Early identification and active management of
patients with renal impairment in primary care can improve
outcomes. BMJ 2002; 325: 83-89.
8. Bossola M. Tazza L., Panocchia N, Cicciarelli A, Liberatori M,
Luciani G; Malnutrition in haemodialysis patients: Rivista Italiana

68
di Nutrizione Parenterale ed Enterale-Anno 2001; 1: 1-8
9. Smith R and James W.P.T. Nutrition. In: Oxford Textbook of
Medicine. Published by Weatherall D.J, Ledingham J.G.G, Warrell
D.A. Pgs 1267 – 1271, 1998; 3rd edition. Edinburgh.
10. Qureshi AR., Anders A, Anders D, et al. Factors predicting
malnutrition in haemodialysis patients: A cross-sectional study.
Kidney International 1998; Vol 53: 773-782.
11. J.B.R Monteiro, P.P Oliveira and E.L. Rosado. Nutritional follow
up of uraemic patients in haemodialysis program at Sao Joao
Batista Hospital, Vicosa: Nutrition September 1996; 12 (9): 658 –
660.
12. Hakim R.M, Levin N. Malnutrition in haemodialysis patients. Am
J Kidney Dis 1993; 21: 125 – 137.
13. Kopple J.D, Greene T, Chumlea W.C, et al. Relationship between
nutritional status and the glomerular filtration rate : Results from
the MDRD study. Kidney Int. 2000; 57: 1688 – 1703.
14. Charles H, Halsted. Malnutrition and nutritional assessment. In:
Principles of Internal Medicine. Published by Harrison’s. Pgs 455 –
460, 2001; 15th edition
15. Nigerian Association of Nephrology; Regional workshop on
nutrition in CRF patients; Ife 2005.
16 Ikizler T A,Hakim R M. Nutrition in end-stage renal disease.
Kidney int.1996 Aug; 50(2): 343-357.
17. Sherman R.A, Cody R.P, Rogers M.E et al. Interdialytic weight

69
gain and nutritional parameters in chronic haemodialysis
patients. American Journal of Kidney Disease 1995 jun; 25: 579 –
83.
18. Shenkin, G. Cederblad, M. Elia, et al. Laboratory assessment of
protein-energy status; Clinica Chimica Acta; September 1996; Vol
252 (1 – 2): S5 – S59.
19. Heimburger O, Qureshi A.R, Blanner B, et al. Hand-grip muscle
strength, lean body mass and plasma proteins as markers of
nutritional status in patients with advanced renal failure. Am J
Kidney Dis 2000; 36: 1213 – 1225.
20. Johansen K.L, Mulligan T, Tai V, et al. Leptin, body composition
and indices of malnutrition in patients on dialysis. Journal of
American Society of Nephrology 1998; 9: 1080 – 1082.
21. Abraham G. Varsha P; Mathew M; Sairam VK; Gupta A.
Malnutrition and nutritional therapy of chronic kidney diseases in
developing countries; the Asian perspective Adv. Ren. Replace.
Ther. 2003 July; 10(3): 213-21.
22. Bergstrum J. Why are dialysis patients malnourished? Am J
Kidney Dis 1995; 26: 229 – 241.
23. Agaba E. prevalence of malnutrition in Nigeria with chronic renal
failure. International urology and nephrology. 2003; 36(1): 89-93.
24. Winbor AL, Banaszek NK, Freed BA, et al. A protocol for
nutritional assessment in a community hospital. J. Am Diet Assoc.
1981; 78; 129-34.

70
25 Barril G, Cigarran S, Farre M, Mancha A, Ulibarri I, Selgas R:
Importance of the evaluation of nutritional status in patients with
chronic renal failure in a predialysis unit. 2nd International
congress of nephrology in Intern.CIN2001.
26. Aparicio M; Nutritional status in chronic renal failure. An
essential assessment objective nutrition N053 (Sept. 2000).
27. Aparicio M, Cano N, Chanvean P, et al. Nutritional status of
haemodialysis patients; A French national cooperative study.
Nephrol Dial transplant 1999; 14: 1679-86.
28. Kopple J.D., Jahn H, Massry S.G, Heidland A. Nutritional status
of patients with different levels of chronic renal insufficiency.
Kidney international suppl. 1989; 27: (S-184).
29. Giovannetti S; Answers to ten questions on the dietary treatment
of chronic renal failure. The lancet 1986; 1: 1140-1142.
30. El-Nahas; Coles G A. Dietary treatment of chronic renal
failure:Ten unanswered questions. The Lancet 1986; 1: 597-602.
31. Stenvinkel P, Heimburger O, Paultre F, et al. Strong association
between malnutrtion, inflammation and atherosclerosis in chronic
renal failure. Kidney Int 1999; 55: 1899 – 1911.
32. Stenvinkel P, Heimburger O, Lindhom B, et al. Are there two
types of malnutrition in chronic renal failure? Nephrol Dial
Transplant 2000; 15: 953 – 960.
33. Kamyar K, T. Alp Ikizler, Gladys Block, et al. Malnutrition –
inflammation complex syndrome in dialysis patients: Causes and

71
consequences. American Journal of Kidney Diseases 2003; Vol.
42 (5): 864 – 81.
34. Kopple JD. Pathophysiology of protein-energy wasting in chronic
renal failure J Nutr. 1999 Jan; 129 (Is supply): 247S-251S.
35. Chumlea W.C. Anthropometric assessment of nutritional status
in renal disease. J Renal Nutr 1997; 7: 176 – 81.
36. Prichard S.S. Comorbidities and their impact on outcome in
patients with end-stage renal disease. Kidney International 2000
Jan; 57(74): 100-102
37. Kerr P.G, Strasuss B.J.G, Atkins R.C. Assessment of the
nutritional state of dialysis patients. Blood Purif 1996; 14: 382 –
387.
38. Ogbeide O. Okojie O., Wagbatsoma V. Isah E. Nutritional status of
lactating mothers in Benin City, Nigeria. Community and
international nutrition. Nig. J. Nutri. Sci 1994; 15: 37-39.
39. Dwyer J.T, Cunnif P.J, Maroni BJ, et al. The Haemodialysis pilot
study: nutrition program and participant characteristics at
baseline. The HEMO Study Group. Journal and real Nutrition 1998
Jan; 8(1): 11-20.
40. Nelma S.J, Sergio A.D, Maria A.K, et al. Is serum albumin a
marker of nutritional status in haemodialysis patients without
evidence of inflammation? Artificial organs 2003; 27 (8): 681 –
686.
41. Baker J.P, Detsky A.S, Wesson D.E, et al. Nutritional

72
assessment. A comparison of clinical judgment and objective
measurements. N Engl J Med 1982; 306: 969 – 72.
42. DiMaggio D, Vincenzo T and Vincenzo B. Daily variations of
protein intake in haemodialyzed patients. Nephrol Dial Trans
1998; 13: 2978 – 2980.
43. Burrowes JD, Cockram DB, Dwyer JT, et al. Cross-sectional
relationship between dietary protein and energy intake,
nutritional status, functional status, and comorbidity in older
versus younger haemodialysis patients. Journal of Renal Nutrition
2000 Apr; 12 (2): 87-95.
44. Yeun J.Y and Kaysen G.A. Factors influencing serum albumin in
dialysis patients. Am J Kidney Dis 1998; 32 (4): S118 – 25.
45. Spreedhara R, Avram M.M, Blanco M, et al. Prealbumin is the
best nutritional predictor of survival in haemodialysis and
peritoneal dialysis. Am J Kidney Dis 1996; 28: 937 – 942.
46. Young G.A, Kopple J.D, Lindholm B, et al. Nutritional
assessment of CAPD patients: An international study. Am J
Kidney Dis 1991; 17: 462 – 471.
47. Enia G, C. Sicuso, G. Alati and C. Zoccali. Subjective global
assessment of nutrition in dialysis patients. Nephrol Dial
Transplant 1993; 8 (10): 1094 – 1098.
48. Raimund R H,Kopple J D.Nutritional therapy in patients with
renal failure .Care of the renal patients.2nd edition Levine,1996;
15: 169-180.

73
49. Cupisti A, Dalessandro C., Nutritional status and dietary
manipulation in Pre-dialysis chronic renal failure patients. J.
Ren. Nutri. 2004; 14(3): 127-33
50. Araoye M.O. Sample size determination, research methodology
with statistics for health and social sciences. 2003, 6 (115-119).
51. Guruprasad Manjunath, Mark J. Sarnak, Andrew S. Levey,
Estimating the glomerular filtration rate, dos and don’ts for
assessing kidney function. Post graduate medicine 2001: 55- 60.
52. Lene Thoresen. Nutritional status of patients with advanced
cancer: The value of using the subjective global assessment of
nutritional status as a screening tool: Palliative Medicine 2002;
16: 33 – 42.
53. Ifudu O. Henry R, Peter H and Friedman E.A. Predictive value of
functional status for mortality in patients on maintenance
haemodialysis. American Journal of Nephrology 1998; 18 (2): 109-
116.
54. Arije A, Kadiri S, Akinkugbe O.O and Osobamiro O.
Haemodialysis in Ibadan: A preliminary report on the first 100
dialysis. African Journal of Medicine and Medical Sciences 1995;
24: 255 – 259.
55. Bappa Adamu, Aliyu Abdu, et al. Three years follow-up of the
first renal transplant in Aminu Kano Teaching Hospital: A Case
report. Tropical Journal of Nephrology Vol 1, January 2006: 29 –
32.

74
56. Rashad S, Barsoum, et al. Epidemiology of ESRD: A worldwide
perspective. In Kidney Diseases in the developing world and
Ethnic minorities textbook 2005: 1 – 10
57. Anteyi E.A and Garba M.R. Haemodialysis in Jos, Nigeria: An
experience from a new center. Nig. Med J 1996; 30 (2): 59 – 61.
58. Ojogwu L.I and Anah C.O. Renal failure and hypertension in
tropical Africa – a pre-dialysis experience from Nigeria. East
African Medical Journal 1983; 60: 478 – 484.
59. Limman H.M. Cross sectional study of nutritional status and its
relationship to quality of life in a sample of chronic renal failure
patients. National Postgraduate Medical College of Nigeria, May
2005.
60. Lawson J. A. and Kelly JL. Prognostic significance of nutritional
status in pre-dialysis chronic renal failure. Nephrology 2000; 5:
108-110.
61. Jansen M.A.M, Korevaar J.C, Dekkar F.W, et al. Renal function
and nutritional status at the start of chronic dialysis treatment. J
Am Soc Nephrol 2001; 12: 157 – 163.
62. Zimmermann J, Herrlinger S, Pruy A, et al. Inflammation
enhances cardiovascular risk and mortality in haemodialysis
patients. Kidney Inter 1999;55:648-658.
63. Kenneth E.C, Michael H.C, Robert M.P, et al. Serum albumin
concentration and clinical assessments of nutritional status in
hospitalized older people: Different sides of different coins?

75
Journal American Geriatric Society 2002; 50: 631 – 637.
64. Locatelli F, Alberti D, Graziani D, et al. Prospective randomized
multicentre trial of effect of protein restriction on progression of
chronic renal insufficiency. Northern Italian cooperative study
Group. Lancet 1991; 337: 1299 – 1304.
65. Ikizler T.A, Hakim R.M. Nutrition in end stage renal disease.
Kidney Int 1996; 50: 343 – 357
66. Francisco C, Manuel A, Jose, et al. uraemic Symptoms,
nutritional status and renal function in pre-dialysis end-stage
renal failure patients. Nephrol Dial Transplant 2001; 16: 776 –
782.
67. Maarten A.M, Janseen, Johanna, et al. Renal function and
nutritional status at the start of chronic dialysis treatment. J Am
Soc Nephrol 2001; 12: 157 – 263.
68. Owen W.F. Jr, Lew NJ, Liu Y, et al. The urea reduction ratio and
serum albumin concentration as predictors of mortality in
patients undergoing haemodialysis. N. Engl J. Med 1993; 329:
1001 – 1006.
69. Dialysis Outcomes Quality Initiative Guidelines. Clinical practice
guidelines for nutrition in chronic renal failure. I. Adult guidelines
A. Maintenance dialysis; Evaluation of protein-energy nutritional
status; NFK-DOQI. American Journal of Kidney Disease; 35 (2):
519 – 520.
70. Sources of error in weighing and measuring children in CDC

76
nutrition surveillance, DHEW publication No 4, (CDC) 76-8295.
Atlanta, GA, 1975, P6.
71. Crocker H, Shepard M.D.S, White G.H. Evaluation of an
enzymatic method for determining creatinine in plasma. J. clin
Pathol 1988 41:576 – 581
72. Chaney A. L. Marbach E. P. Modified reagents for determination of
urea and ammonia Clin Chem 1962; 8: 131.
73. Doumas B. T, Watson W. A, Biggs H. G. Albumin standards and
the measurement of serum albumin with bromocresol green. Clin
Chem Acta. 1971; 13: 87.

77
APPENDIX 1
CONSENT FORM
I _______________________________________________ of __________________
______________________________________________________________hereby
consent to the performance of some investigations on me to find out the
nutritional status of chronic renal failure patients before the initiation
of dialysis therapy.
Dr. ___________________________________________________________has
explained to me that the investigations would require taking about
12mls of blood from me in addition to other non invasive procedures.
I understand that the investigations are for medical research I am
willing to volunteer to act for that purpose on the understanding and I
am entitled to withdraw this consent at any time. I also recognize that
the study may be of benefit to mankind and especially to me since any
abnormalities found would result in early initiation of treatment.
Date________________________________________Signature________________
I confirm that I have explained to the patient the purpose and nature of
these investigations including the fact that his refusal to participate will
not in any way affect his normal care by me or any other member of the
managing team . I know the consequences of false declaration on this
or any other form.
Date__________________________________Signature______________________

78
APPENDIX 2
NUTRITIONAL STATUS OF CRF PATIENTS (PRE-DIALYSIS) WITH
DIFFERENT LEVELS OF CHRONIC RENAL INSUFFICIENCY
QUESTIONNAIRE
A. 1. Patient’s Name: ___________________________________
2. Hospital Number: __________________________________
3. Sex: _________________
4. Age: _________________
5. Marital Status: __________
6. Religion: _______________
7. Educational Status: __________________________________
8. Occupation: ________________________________________
B. 9. When were you diagnosed of chronic renal failure?
_______________ weeks, months, years
10. Duration of illness: __________________
11. Are you seeing a doctor for any ailment other than kidney
disease? Yes / No
12. If yes, please state the disease condition __________________
13. Have you undergone any form of renal replacement therapy?
Yes/ No
14. Are you on drug /s e.g. steroid? Yes / No
State other drugs that you are taking: ____________________
C. 15. Urinalysis result: ____________________________________
16. 24 hours urine for protein estimation: ____________________

79
17. Liver function test: ___________________________________
18. Abdominal ultrasound scan:
• Kidney sizes: Rt _________ Lt ___________
• Liver size: _________________
19. Glomerular filtration rate by MDRD _______mls/min/1.73m2
20. Stage of CKD 1.
2.
3.
4.
5.
NUTRITIONAL ASSESSMENT
A. SUBJECTIVE GLOBAL ASSESSMENT
Parameter Value Date
Over all Subjective
Global Assessment
Rating
B. ANTHROPOMETRIC PARAMETERS
Parameter Value Date
Weight
% Weight loss

80
Parameter Value Date
Height
BMI
MUAC
Triceps Skin
Fold thickness
Parameter Value Date
Albumin
Creatinine
Urea

81
APPENDIX 3
UNIVERSITY OF BENIN, BENIN CITY
INITIAL NUTRITION HISTORY AND ASSESSMENT
PATIENT’S NAME : ________________________________
DATE ______________
AGE: ___________ SEX __________ HOSP. NO _________
I. CURRENT INTAKES AND TIME OF MEALS
BREAKFAST/TIME LUNCH/TIME DINNER/TIME
DAY ONE __________________ _______________ _______________
__________________ _______________ _______________
__________________ _______________ _______________
__________________ _______________ _______________
__________________ _______________ _______________
ESTIMATED DAILY PROTEIN INTAKE (GRAM/DAY)
DAY TWO __________________ _______________ _______________
__________________ _______________ _______________
__________________ _______________ _______________
__________________ _______________ _______________
__________________ _______________ _______________
ESTIMATED DAILY PROTEIN INTAKE (GRAM/DAY)
DAY THREE_________________ _______________ _______________
__________________ _______________ _______________
__________________ _______________ _______________
__________________ _______________ _______________
__________________ _______________ _______________
ESTIMATED DAILY PROTEIN INTAKE (gram/day)
II. AVERAGE DAILY PROTEIN INTAKE (GRAM/DAY)_____________

82

83

84

85

86

87

88
Picture showing the investigator measuring Triceps Skin Fold
Thickness.
Recommended