Non-Communicable Diseases:Role of Government versus Individuals Responsibilities
Feisul Idzwan Mustapha MBBS, MPH, AM(M)Public Health Physician, NCD Section, Disease Control Division
Ministry of Health, Malaysia
Symposium 1: Managing NCDs10th Allied Health Scientific Conference Malaysia 2014
9 September 2014Kuala Lumpur
Ministry of Health Malaysia

There are Four Major Groups of Non-Communicable Diseases;Four major lifestyles related risk factors
Modifiable causative risk factors
Tobacco use Unhealthy diets
Physical inactivity
Harmful use of alcohol
Noncommunicable diseases
Heart disease and stroke
Diabetes
Cancers
Chronic lung disease
2

Proportional mortality, Malaysia (% of total deaths, all ages, both sexes)
3

Premature mortality due to NCDs, Malaysia
4
The probability of dying between ages 30 and 70 years from the 4 main NCDs is 20%

5
Source of icons: World Heart Federation Champion Advocates Programme
Global NCD Targets

Sub-analysis of NHMS 2011 data
• At least 15% (18 years and above) already with known NCD risk factors (diabetes, hypertension or hypercholesterolemia).
• Undiagnosed high blood sugar, high blood pressure or high cholesterol: 42.1% (18 years and above).
• Or, if include obesity: 48.3% (18 years and above).
• Therefore our high risk and at risk population: 63.3% (18 years and above)
6

DALYs attributable to risk factors
7
10.8%
10.7%
9.0%8.3%
5.2%4.3%
3.1%0.7%
0.1%
10.8%
0.7%11.4%
12.1%
5.1%0.9%
4.3%0.7%
0.1%
15.0% 10.0% 5.0% 0.0% 5.0% 10.0% 15.0%
High BP
Tobacco
Diabetes Mellitus
High BMI
High Cholesterol
Alcohol
Physical Inactivity
UnderweightPoor Water & Sanitation
Male Female
Burden of Disease Study Malaysia, slide courtesy of Dr Mohd. Azahadi Omar, Institute for public health

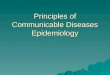
19.4%
15.7%
8.5%
7.3%
7.0%
5.0%
2.3%
0.2%
0.1%
22.8%
1.2%
9.1%
8.1%
8.2%
7.1%
0.3%
0.2%
0.1%
25% 20% 15% 10% 5% 0% 5% 10% 15% 20% 25%
High BP
Tobacco
Diabetes Mellitus
High Cholesterol
High BMI
Physical Inactivity
Alcohol
Underweight
Poor Water & Sanitation
Male Female
Deaths attributable to risk factors
Burden of Disease Study Malaysia, slide courtesy of Dr Mohd. Azahadi Omar, Institute for public health
8

National Strategic Plan for Non-Communicable Diseases (NSP-NCD) 2010-2014
• Presented and approved by the Cabinet on 17 December 2010.• Provides the framework for strengthening NCD prevention & control
program in Malaysia.• Adopts the “whole-of-government” and “whole-of-society approach”.• Diabetes & obesity are used as the entry points.
Seven Strategies:1. Prevention and Promotion
2. Clinical Management
3. Increasing Patient Compliance
4. Action with NGOs,
Professional Bodies & Other
Stakeholders
5. Monitoring, Research and
Surveillance
6. Capacity Building
7. Policy and Regulatory
interventions
9

Cost effective NCD interventions…
• What works, what can we afford, and what should we adopt?• The challenge? Identify interventions that:
• are effective;• can lead to measurable declines in NCD death rates quickly (e.g.
over 10 years);• are affordable; and• can easily be implemented and sustained.
The Lancet. December 8, 2007 Volume 370:Gaziano T, Galea G and Reddy K. Scaling up interventions for chronic disease prevention: the evidence. pp 1939-1946.
The Lancet. December 15, 2007. Volume 370:Asaria P, Crisholm D, Mathers C, Ezzati M, Beaglehole R. Chronic disease prevention: health effects and financial costs of strategies to reduce salt intake and control tobacco use. pp 2044-2053.Lim S, et. al. Prevention of cardiovascular disease in high-risk individuals in low-income and middle-income countries: health effects and costs. pp 2054-2061.
10

Cost effective NCD interventions…
• What is effective? The intervention must:• targets behaviours or risk factors that are causally associated with
NCDs; and• is proven, through evidence, to lead to favourable changes in
behaviours/risk factors, thereby reducing risk of death from NCDs.
11

Cost effective interventions to address NCDs
Population-based interventions addressing NCD risk factors
Tobacco use
- Excise tax increases - Smoke-free indoor workplaces and public places- Health information and warnings about tobacco - Bans on advertising and promotion
Harmful use of alcohol
- Excise tax increases on alcoholic beverages - Comprehensive restrictions and bans on alcohol
marketing- Restrictions on the availability of retailed alcohol
Unhealthy diet and physical inactivity
- Salt reduction through mass media campaigns and reduced salt content in processed foods
- Replacement of trans-fats with polyunsaturated fats- Public awareness programme about diet and physical
activity
Individual-based interventionsaddressing NCDs in primary care
Cancer - Prevention of liver cancer through hepatitis B immunization
- Prevention of cervical cancer through screening (visual inspection with acetic acid [VIA]) and treatment of pre-cancerous lesions
CVD and diabetes
- Multi-drug therapy (including glycaemic control for diabetes mellitus) for individuals who have had a heart attack or stroke, and to persons at high risk (> 30%) of a cardiovascular event within 10 years
- Providing aspirin to people having an acute heart attack
12

Strategy 7 NSP-NCD: Policy & Regulatory Interventions• Main thrust of NSP-NCD• Health promotion and education will increase awareness and
knowledge• However changes in behaviour is strongly influenced by our
living environment
Awareness Knowledge Behavioural Change
Supportive living environment
Health promotion & educations
Policies & regulations13

14

Individuals Populations
Lifestyle medicine Public health policy
Policy approaches:Change the environment
Policy approaches: educate, inform to change behaviours
15

The Great Prevention Debate
Personal choice
versus
government responsibility
16

Personal Choice is Important
17

BUT … If we want people to make healthy choices we have to make healthy choices available, accessible and affordable
18

Prevention is BOTH a personal and
government responsibility
19

Current Approaches to NCD From Birth To Tomb
Intervention Package
Health Promotion
Intervention Package
Health Promotion
Pregnancy
Pregnancy
Pre-conceptio
n
Pre-conceptio
n
Infant/
Toddler
Infant/
Toddler
First 1,000 Days
To reduce obesity and NCDs-birth weight
Lifestyle during pregnancy – fetal health
First 1,000 Days
To reduce obesity and NCDs-birth weight
Lifestyle during pregnancy – fetal health
Pre-School
Pre-School
School-going Age
School-going Age
Garispanduan Pemasaran Makanan & Minuman kepada
Kanak-kanak
Garispanduan Pemasaran Makanan & Minuman kepada
Kanak-kanak
Garispanduan Penguatkuasaan Larangan
Penjualan Makanan & Minuman Di Luar Pagar
Sekolah
Garispanduan Penguatkuasaan Larangan
Penjualan Makanan & Minuman Di Luar Pagar
Sekolah
Higher Education
Higher Education AdultsAdults
Elderly
Elderly
School SettingSchool Setting
NCDP1MNCDP1M
Workplace / Community Setting
Workplace / Community Setting
KOSPENKOSPEN
AktivitiFizikalAktivitiFizikal
Program Warga Aktif Warga Produktif
Program Warga Aktif Warga Produktif
Healthy Workplace for Healthy Workforce
Healthy Workplace for Healthy Workforce
Garispanduan Pengurusan Kantin
Sihat
Garispanduan Pengurusan Kantin
Sihat
Garispanduan Perlaksanaan Vending Machine Makanan &
Minuman Sihat dlm Perkhidmatan Awam
Garispanduan Perlaksanaan Vending Machine Makanan &
Minuman Sihat dlm Perkhidmatan Awam
Kafeteria SihatKafeteria Sihat
Hidangan Sihat Semasa Mesyuarat
Hidangan Sihat Semasa Mesyuarat
Amalan Pemakanan Sihat
Amalan Pemakanan Sihat
Jom Mama Initiatives
Jom Mama Initiatives
20

Strategy 7 NSP-NCD: Policy & Regulatory Interventions, Progress thus far…
• Guideline on marketing of foods and non-alcoholic beverages to children (Self-regulatory, August 2013).
• Strengthening implementation of the Framework Convention for Tobacco Control (FCTC).
• Guideline on food and beverages sold in school canteens (revised guideline, January 2012).
• Banning of sale of food & beverages by mobile vendors outside of school perimeters (2012)
• Health-promoting workplaces in the public sector• Healthy menus during meetings• Healthy vending machines• Healthy cafeterias
There is still much that needs to be done….
21

Objective 3 GAP NCD 2013-2020:Healthy Diet• Three (3) relevant global targets:
• A 30% relative reduction in mean population intake of salt/sodium
• A halt in the rise in diabetes and obesity• A 25% relative reduction in the prevalence of raised blood
pressure or containment of the prevalence of raised blood pressure according to national circumstances.
22

Objective 3 GAP NCD 2013-2020:Healthy Diet• Promote and support exclusive breastfeeding for the first six
months of life, continued breastfeeding until two years old and beyond and adequate and timely complementary feeding.
• Implement WHO’s set of recommendations on the marketing of foods and non-alcoholic beverages to children, including mechanisms for monitoring.
23

• Develop guidelines, recommendations or policy measures that engage different relevant sectors, such as food producers and processors, and other relevant commercial operators, as well as consumers, to:• Reduce the level of salt/sodium added to food (prepared or
processed).• Increase availability, affordability and consumption of fruit and
vegetables.• Reduce saturated fatty acids in food and replace them with
unsaturated fatty acids.• Replace trans-fats with unsaturated fats.• Reduce the content of free and added sugars in food and non-
alcoholic beverages.• Limit excess calorie intake, reduce portion size and energy density
of foods.
24
Objective 3 GAP NCD 2013-2020:Healthy Diet

Objective 3 GAP NCD 2013-2020:Healthy Diet• Develop policy measures that engage food retailers and
caterers to improve the availability, affordability and acceptability of healthier food products (plant foods, including fruit and vegetables, and products with reduced content of salt/sodium, saturated fatty acids, trans-fatty acids and free sugars).
• Promote the provision and availability of healthy food in all public institutions including schools, other educational institutions and the workplace. (e.g. through nutrition standards for public sector catering establishments and use of government contracts for food purchasing)
25

Objective 3 GAP NCD 2013-2020:Healthy Diet• As appropriate to national context, consider economic tools
that are justified by evidence, and may include taxes and subsidies, that create incentives for behaviours associated with improved health outcomes, improve the affordability and encourage consumption of healthier food products and discourage the consumption of less healthy options.
• Develop policy measures in cooperation with the agricultural sector to reinforce the measures directed at food processors, retailers, caterers and public institutions, and provide greater opportunities for utilization of healthy agricultural products and foods.
26

Objective 3 GAP NCD 2013-2020:Healthy Diet• Conduct evidence-informed public campaigns and social
marketing initiatives to inform and encourage consumers about healthy dietary practices. Campaigns should be linked to supporting actions across the community and within specific settings for maximum benefit and impact.
• Create health- and nutrition-promoting environments, including through nutrition education, in schools, child care centres and other educational institutions, workplaces, clinics and hospitals, and other public and private institutions.
• Promote nutrition labelling, according to but not limited to, international standards, in particular the Codex Alimentarius, for all pre-packaged foods including those for which nutrition or health claims are made. 27

Objective 3 GAP NCD 2013-2020:Promoting Physical Activity• Three (3) relevant global targets:
• A 10% relative reduction in prevalence of insufficient physical activity.
• Halt the rise in diabetes and obesity.• A 25% relative reduction in the prevalence of raised blood
pressure or contain the prevalence of raised blood pressure according to national circumstances.
28

Objective 3 GAP NCD 2013-2020:Promoting Physical Activity• Adopt and implement national guidelines on physical activity
for health.• Consider establishing a multi-sectoral committee or similar
body to provide strategic leadership and coordination.• Develop appropriate partnerships and engage all stakeholders,
across government, NGOs and civil society and economic operators, in actively and appropriately implementing actions aimed at increasing physical activity across all ages.
29

Objective 3 GAP NCD 2013-2020:Promoting Physical Activity• Develop policy measures in cooperation with relevant sectors to
promote physical activity through activities of daily living, including through “active transport,” recreation, leisure and sport, for example:• National and sub-national urban planning and transport policies to
improve the accessibility, acceptability and safety of, and supportive infrastructure for, walking and cycling.
• Improved provision of quality physical education in educational settings (from infant years to tertiary level) including opportunities for physical activity before, during and after the formal school day.
• Actions to support and encourage “physical activity for all” initiatives for all ages.
• Creation and preservation of built and natural environments which support physical activity in schools, universities, workplaces, clinics and hospitals, and in the wider community, with a particular focus on providing infrastructure to support active transport i.e. walking and cycling, active recreation and play, and participation in sports.
• Promotion of community involvement in implementing local actions aimed at increasing physical activity.
30

Objective 3 GAP NCD 2013-2020:Promoting Physical Activity• Conduct evidence-informed public campaigns through mass
media, social media and at the community level and social marketing initiatives to inform and motivate adults and young people about the benefits of physical activity and to facilitate healthy behaviours. Campaigns should be linked to supporting actions across the community and within specific settings for maximum benefit and impact.
• Encourage the evaluation of actions aimed at increasing physical activity, to contribute to the development of an evidence base of effective and cost-effective actions.
31

KOmuniti Sihat, PErkasa Negara (KOSPEN): Empowering Communities, Strengthening the Nation
Ministry of Health Malaysia

Background of KOSPEN• Empowering individuals and communities in self-care to
reduce the exposure to NCD risk factors.
• Blue Ocean Strategy between MOH and other government departments and agencies with existing programs and activities at the grassroot levels• E.g. KEMAS (Department of Community Department), Rukun
Tetangga (Neighbourhood Watch)
• Attempts to add value to the existing program and activities of these different departments and agencies, but incorporating elements of NCD risk factor screening and intervention.
33

Five (5) scopes of healthy living• Not smoking or smoke-free• Weight management• Healthy eating• Active living• Early detection of NCD risk factors
KOSPEN: Empowering individuals and communities in healthy living
Three (3) Main
Strategies
1. Increasing awareness
2. Translation of knowledge into sustainable actions
3. Health-promoting living environment
34

Behavioural Changes through intervention in KOSPEN
Scope Behavioural Changes
Healthy eating 1. Culture: separating sugar / creamer from hot beverages.2. Culture: increasing availability of fruits and vegetables.3. Culture: increasing availability of plain drinking water.
Not smoking / smoke-free
1. Enforcement or implementation of smoke-free areas – both by regulation and volunteerism (e.g. smoke-free house, smoke-free events).
Active living 1. Creation of 10,000-steps walking tracks in the community/village.
Weight management
1. Self-monitoring of body mass index (BMI) at set and regular intervals.
Know your health status
1. Self-monitoring of BMI, blood pressure and blood sugar at set and regular intervals.
2. Use of health diaries.35

KOSPEN Launching Ceremony, National level, 13 February 2014, Segamat, Johor
36

Lessons learned from the past and current attempts to work with other sectors
• Go for the path of least resistance.• Perhaps less impact, but at least establish the link and develop
trust.
• Compromise, find the “middle path”• You cannot force the other sectors to go 100% your way.
• Be creative – think “out-of-the-box”• Use other existing mechanisms not previously used to move the
NCD prevention agenda forward.
• Be sensitive to current global/national trends.• Use any opportunity to move the NCD prevention agenda
forward.37

Summary
• We know what needs to be done for the prevention and control of NCD.
• What we do not know is how best to implement in real life situations and within the socio-cultural context of Malaysia.• Implementation-type research, including behavioural (qualitative
research) can provide evidence in answering this question.• Multisectoral approach, not only in implementation but in
research as well.
38

39
Summary

Thank you
Facebook: Feisul Mustapha
40
Recommended