Measuring Primary Care and Its Benefits
Barbara Starfield, MD, MPH
University of Hong KongHong Kong
October 15, 2009

Life Expectancy Compared with GDP per Capita for Selected Countries
Source: Economist Intelligence Unit. Healthcare International. 4th quarter 1999. London, UK: Economist Intelligence Unit, 1999.
Country codes:AG=ArgentinaAU=AustraliaBZ=BrazilCH=ChinaCN=CanadaFR=FranceGE=GermanyHU=HungaryIN=IndiaIS=IsraelIT=ItalyJA=JapanMA=MalaysiaME=Mexico
Starfield 11/06IC 3493 n
NE=NetherlandsPO=PolandRU=RussiaSA=South AfricaSI=SingaporeSK=South KoreaSP=SpainSW=SwedenSZ=SwitzerlandTK=TurkeyTW=TaiwanUK=United KingdomUS=United States

Why Is Primary Care Important?
Better health outcomes
Lower costs
Greater equity in health
Starfield 07/07PC 3757 n

Good Primary Care Requires• Health system POLICIES conducive to primary care
practice: What can we learn from other countries about the relative merits of direct provision of services rather than just financing of services?
• Health services delivery that achieves the important FUNCTIONS of primary care: What can be done to enhance practitioners’ recognition of and responsiveness to patients’ problems (patient-focus) rather than on the professional priorities of diagnoses (diagnosis-focus)?
Starfield 06/08PC 4042

PRIMARY HEALTH CARE “works”because it has definable system functions that provide the policy context for primary care.
Starfield 03/08PC 3987
PRIMARY CARE “works” because it has defined functions that include structural and process features of clinical health services that are known to improve outcomes of care.

Key system factors in achieving primary health care in both developing and industrialized countries are:• Universal financial coverage, under
governmental control or regulation• Efforts to distribute resources equitably
(according to degree of need)• No or low co-payments• Comprehensiveness of services
Starfield 07/07GH 3794 n
Sources: Starfield & Shi, Health Policy 2002; 60:201-18. Gilson et al, Challenging Inequity through Health Systems (http://www.who.int/social_determinants/resources/csdh_media/hskn_final_2007_en.pdf; accessed March 17, 2009).

0123456789
101112
0 1 2 3 4 5 6 7 8 9 10 11 12 13
System Characteristics (Rank*)
Prac
tice
Char
acte
ristic
s (R
ank*
)
UK
NTH
SP
FIN CANAUS
SWE JAP
GER FRBEL
US
DK
*Best level of health indicator is ranked 1; worst is ranked 13; thus, lower average ranks indicate better performance.Based on data in Starfield & Shi, Health Policy 2002; 60:201-18.
System (PHC) and Practice (PC) Characteristics Facilitating Primary Care, Early-Mid 1990s
Starfield 03/05ICTC 3099 n

At the clinical level,
• The critical structural features are Accessibility, mechanisms of Continuity/Information Systems, and the Range of Services available in primary care.
• The critical process features are Problem Recognition on the part of practitioners (both for initial problems and for reassessment), and Utilization of primary care services, both over time and for new problems as they arise.
Starfield 04/08EVAL 4018
Together, these features achieve the evidence-based FUNCTIONS of primary care: first contact, person-focused (not disease-focused) care over time, comprehensiveness, and coordination.

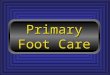
Primary Care Strength and Premature Mortality in 18 OECD Countries
*Predicted PYLL (both genders) estimated by fixed effects, using pooled cross-sectional time series design. Analysis controlled for GDP, percent elderly, doctors/capita, average income (ppp), alcohol and tobacco use. R2(within)=0.77.
Source: Macinko et al, Health Serv Res 2003; 38:831-65.
Year
High PC Countries*
Low PC Countries*
10000
PYLL
1970 1980 1990 20000
5000
Starfield 11/06IC 3496 n

Primary Care Oriented Countries Have
• Fewer low birth weight infants• Lower infant mortality, especially
postneonatal• Fewer years of life lost due to suicide• Fewer years of life lost due to “all except
external” causes• Higher life expectancy at all ages except
at age 80Starfield 07/07IC 3762 n
Sources: Starfield. Primary Care: Balancing Health Needs, Services, and Technology. Oxford U. Press, 1998. Starfield & Shi, Health Policy 2002; 60:201-18.

0
0.5
1
1.5
2
1000 1500 2000 2500 3000 3500 4000
Per Capita Health Care Expenditures
Prim
ary
Care
Sco
re
Primary Care Score vs. Health Care Expenditures, 1997
US
NTH
CANAUS
SWE JAP
BEL FRGER
SP
DK
FIN
UK
Starfield 11/06ICTC 3495 n

• Have more equitable resource distributions• Have health insurance or services that are
provided by the government• Have little or no private health insurance• Have no or low co-payments for health services• Are rated as better by their populations• Have primary care that includes a wider range
of services and is family oriented• Have better health at lower costs
Primary health care oriented countries
Sources: Starfield and Shi, Health Policy 2002; 60:201-18. van Doorslaer et al, Health Econ 2004; 13:629-47. Schoen et al, Health Aff 2005; W5: 509-25.
Starfield 11/05IC 3326

Is Primary Care as important within
countries as it is among countries?
Starfield 07/07WC 3765 n

State Level Analysis:Primary Care and Life Expectancy
Source: Shi, Int J Health Serv 1994;24:431-58. Starfield 04/09WCUS 4178 n
71
72
73
74
75
76
77
78
4.0 4.5 5.0 5.5 6.0 6.5 7.0 7.5
Primary care physicians per 10,000 population
Life
exp
ecta
ncy
at b
irth
ME
NHVT
MA
RICT
NY
NJ
PAOH
IN
IL
MI
WI
MN
IA
MO
ND
SD
NE
KSDE MDVA
WV NC
SC
GA
FL
KYTN
AL
MS
AR
LA
OK TX MT
ID
WY
CO
NMAZ
UT
NV
WAOR
CA
AK
HI

Many other studies done WITHIN countries, both industrialized and developing, show that areas with better primary care have better health outcomes, including total mortality rates, heart disease mortality rates, and infant mortality, and earlier detection of cancers such as colorectal cancer, breast cancer, uterine/cervical cancer, and melanoma. The opposite is the case for higher specialist supply, which is associated with worse outcomes.
Starfield 09/0404-167
Sources: Starfield et al, Milbank Q 2005;83:457-502. Macinko et al, J Ambul Care Manage 2009;32:150-71.
Starfield 09/04WC 2957

Why Does Primary Care Enhance Effectiveness of Health Services?
• Greater accessibility• Better person-focused prevention• Better person-focused quality of clinical
care• Earlier management of problems (avoiding
hospitalizations)• The accumulated benefits of the four
features of primary careStarfield 05/09PC 4185Source: Starfield et al, Milbank Q 2005;83:457-502.

Does primary care reduce inequity in
health?
Starfield 07/07EQ 3769 n

Source: Shi et al, Soc Sci Med 2005; 61(1):65-75.
In the United States, an increase of 1 primary care doctor is associated with 1.44 fewer deaths per 10,000 population.
The association of primary care with decreased mortality is greater in the African-American population than in the white population.
Starfield 07/07WCUS 3770 n

A comparison of age-adjusted survival from breast cancer showed that
• Low SES is strongly associated with decreased survival in US, but not Canada.
• The survival advantage in Canada is present in low income areas only.
• The survival advantage in Canada is much larger at ages under 65.
• The Canadian survival advantage is larger for later stage diagnosis. That is, there is almost certainly a medical care benefit to equity in the Canadian context.
Source: Gorey, Breast cancer survival in Canada and the USA: meta-analytic evidence of a Canadian advantage in low-income areas, Int J Epidemiol 2009 forthcoming.
Starfield 08/09IC 4230

Why Does Primary Care Enhance Equity in Health?
• Greater comprehensiveness of services (especially important in the presence of multi-morbidity)
• Person-focused care over time (better knowledge of patient and better recognition of problems)
• Greater accessibility of services• Better coordination, thus facilitating care for
people of limited flexibility • Better person-focused prevention
Starfield 05/09PC 4184Source: Starfield et al, Milbank Q 2005;83:457-502.

Many other studies done WITHIN countries, both industrialized and developing, show that areas with better primary care have better health outcomes, including total mortality rates, heart disease mortality rates, and infant mortality, and earlier detection of cancers such as colorectal cancer, breast cancer, uterine/cervical cancer, and melanoma. The opposite is the case for higher specialist supply, which is associated with worse outcomes.
Starfield 09/0404-167
Sources: Starfield et al, Milbank Q 2005;83:457-502. Macinko et al, J Ambul Care Manage 2009;32:150-71.
Starfield 09/04WC 2957

In 35 US analyses dealing with differences between types of areas (7) and 5 rates of mortality (total, heart, cancer, stroke, infant), the greater the primary care physician supply, the lower the mortality for 28. The higher the specialist ratio, the higher the mortality in 25.
Controlled only for income inequalitySource: Shi et al, J Am Board Fam Pract 2003; 16:412-22.
Starfield 11/06SP 3499 n
Above a certain level of specialist supply, the more specialists per population, the worse the outcomes.

Use of Specialists in the US• REFERRAL rates from primary care to
specialty care in the US are HIGH.• Between 1/3 and 3/4 (depending on
the type of specialist) of visits to specialists are for routine follow-up.
• The percentage of people SEEN BY a specialist in a year is high, especially in the presence of high morbidity burden.
Starfield 03/06SP 3396Sources: Forrest et al, BMJ 2002; 325:370-1. Valderas et al, Ann Fam Med 2009;7:104-11.

Resource Use, Controlling for Morbidity Burden*
• More DIFFERENT specialists seen: higher total costs, medical costs, diagnostic tests and interventions, and types of medication
• More DIFFERENT generalists seen: higher total costs, medical costs, diagnostic tests and interventions
• More generalists seen (LESS CONTINUITY): more DIFFERENT specialists seen among patients with high morbidity burdens. The effect is independent of the number of generalist visits. That is, the benefits of primary care are greatest for people with the greatest burden of illness.
Starfield 09/07CMOS 3854
*Using the Johns Hopkins Adjusted Clinical Groups (ACGs)
Source: Starfield et al, Ambulatory specialist use by patients in US health plans: correlates and consequences. J Ambul Care Manage 2009 forthcoming.

Family Physicians, General Internists, and Pediatricians
A nationally representative study showed that adults and children with a family physician (rather than a general internist, pediatrician, or sub-specialist) as their regular source of care had lower annual cost of care, made fewer visits, had 25% fewer prescriptions, and reported less difficulty in accessing care, even after controlling for case-mix, demographic characteristics (age, gender, income, race, region, and self-reported health status). Half of the excess is in hospital and ER spending; one-fifth is in physician payments; and one-third is for medications.
Starfield 03/09 PC 4162Source: Phillips et al, Health Aff 2009;28:567-77.

We know that1. Inappropriate referrals to specialists lead to
greater frequency of tests and more false positive results than appropriate referrals to specialists.
2. Inappropriate referrals to specialists lead to poorer outcomes than appropriate referrals.
3. The socially advantaged have higher rates of visits to specialists than the socially disadvantaged.
4. The more the training of MDs, the more the referrals.
Source: Starfield et al, Health Aff 2005; W5:97-107 (http://content.healthaffairs.org/cgi/reprint/hlthaff.w5.97v1). van Doorslaer et al, Health Econ 2004; 13:629-47;
Starfield 08/05SP 3241
A MAJOR ROLE OF PRIMARY CARE IS TO ASSURE THAT SPECIALTY CARE IS MORE APPROPRIATE AND, THEREFORE, MORE EFFECTIVE.

Joint Principles of the Patient-centered Medical Home
• Personal physician: ongoing relationship for first contact, continuous, comprehensive care
• Physician directed medical practice• Whole person oriented• Coordinated and/or integrated care• Quality and safety• Enhanced access• Added value payment
Starfield 03/08MH 4005Source: AAFP/AAP/ACP/AOA. Joint Principles. March 2007.

Proposed PC/MH (Patient-centered Medical Home) Criteria
• Electronic health record• Teams• Chronic care guidelines
Starfield 06/08MH 4043
Question: Do these “enhancements”improve primary care?
This requires evaluation.

Is a Focus on Chronic Disease Compatible with the Patient-
Centered Medical Home?In Pennsylvania, the Governor’s Office of Health Care Reform convened several health plans and physician societies in the southeastern part of the state to “institute a PCMH approach to manage the care of chronically ill patients”.
To what extent is this approach consistent with the principles of population-oriented primary care and the patient-centered medical home? Who is left out?
Starfield 03/09 D 4163

There is more variability in disease manifestations and persistence within diseases than across diseases because:• diseases are not necessarily unique
pathophysiological entities• variability in diagnostic styles and
practices• presence of co-morbidity
Starfield 10/01D 3887

Co- and Multi-morbidity(Morbidity Burden)
Starfield 09/07CM 3864 n

Co-morbidity is the concurrent existence of one or more unrelated conditions in an individual with any given condition. Multi-morbidity is the co-occurrence of biologically unrelated illnesses.
Starfield 03/06CM 3375
For convenience and by common terminology, we use co-morbidity to represent both co- and multi-morbidity.

Morbidity Burdens of Socially Disadvantaged and Socially Advantaged People
0 5 10 15 20 25 30
10+ Morbidity-Types
6-9 MorbidityTypes
% of Total Population
HMO
CHC (Disadvantaged)
Starfield 09/07CM 3866 n

The high frequency of
Co-morbidity
Multi-morbidity
Morbidity burden
makes it inappropriate to focus on single diseases
Starfield 03/08CM 3985 n

Co-morbidity, Inpatient Hospitalization, Avoidable Events, and Costs*
11
362
296
267
216
169
119
74
40
208
1734
57
86
119
152
182
233
84
211
1154
2394
4701
13,973
0
50
100
150
200
250
300
350
400
0 1 2 3 4 5 6 7 8 9 10+
Number of types of conditions
Rate
per
100
0 be
nefic
iari
es
0
2000
4000
6000
8000
10000
12000
14000
16000
Cos
ts
ACSC Complications Costs
(4 or moreconditions)
Source: Wolff et al, Arch Intern Med 2002; 162:2269-76. *ages 65+, chronic conditions only
Starfield 11/06CM 3503 n

Expected Resource Use (Relative to Adult Population Average) by Level of Co-Morbidity, British Columbia, 1997-98
Starfield 09/07CM 3867 n
None Low Medium HighVery High
Acute conditions only
0.1 0.4 1.2 3.3 9.5
Chronic condition 0.2 0.5 1.3 3.5 9.8High impact chronic condition
0.2 0.5 1.3 3.6 9.9
Source: Broemeling et al. Chronic Conditions and Co-morbidity among Residents of British Columbia. Vancouver, BC: University of British Columbia, 2005.
Thus, it is co-morbidity, rather than presence or impact of chronic conditions, that generates resource use.

As thresholds for diagnosing disease are lowered over time, the variability within “diseases”will increase even further, as will the prevalence of multiple simultaneous or sequential diseases.
Starfield 03/08D 3986

Increase in Treated Prevalence: Selected Conditions, US, People with Private
Insurance, 1987-2002Treated Prevalence
Percentage Change, 1987-2002Hyperlipidemia 437(Heart disease 9) Bone disorders 227Upper GI problems 169Cerebrovascular disease 161Mental problems 136Diabetes 64Endocrine disorders 24Hypertension 17Bronchitis 13
Source: Thorp et al, Health Affairs 2005; W5:317-25, 2005.Starfield 09/06D 3858 n

What is needed is person-focused care over time, NOT disease-focused care.
Starfield 10/06PC 3462

When people (not diseases) are the focus of attention
• Outcomes are better• Side effects are fewer• Costs are lower• Population health is greater
Starfield 09/07PC 3868 nSource: Starfield et al, Health Aff 2005; W5:97-107.

What Is the Appropriate Care Model?
• Primary care that meets primary care (not disease-specific) standards*
• Specialty referrals that are appropriate, i.e., evidence-based**
• Specialty care that meets specialty care standards**
Starfield 03/06PC 3377
*exist**do not exist

Modern medicine is largely atheoretical. With the exception of a few rare genetic conditions, we do not understand why some people have greater susceptibility to disease and, particularly why some people are more prone to multimorbidity than other people. On the other hand, some people seem to be more resilient to health problems. Why?
Starfield 08/09D 4246

Diseases• are professional constructs• can be and are artificially created to suit
special interests; the sum of deaths attributed to diseases exceeds the number of deaths
• do not exist in isolation from other diseases and are, therefore, not an independent representation of illness
• are but one manifestation of ill health
Starfield 08/07D 3831
Sources: Chin. The AIDS Pandemic: the Collision of Epidemiology with Political Correctness. Radcliffe Publishing, 2007. De Maeseneer et al. Primary Health Care as a Strategy for Achieving Equitable Care: a Literature Review Commissioned by the Health Systems Knowledge Network. WHO Health Systems Knowledge Network, 2007. Available at: http://www.wits.ac.za/chp/kn/De%20Maeseneer%202007%20PHC%20as%20strategy.pdf. Mangin et al, BMJ 2007; 335:285-7. Murray et al, BMJ 2004; 329:1096-1100. Tinetti & Fried, Am J Med 2004; 116:179-85. Walker et al, Lancet 2007; 369:956-963. Rosenberg, Milbank Q 2002;80:237-60. Moynihan & Henry, PLoS Med 2006;3:e191.

Despite large improvements in behavior of populations from the 1970s to the 19990s (e.g., a very large decrease in consumption of fats as a proportion of energy), the prevalence of obesity and diabetes increased greatly. Researchers have linked a growing number of chronic diseases (type 2 diabetes, coronary artery disease, stroke, non-alcoholic liver disease, fatty liver disease, polycystic ovary syndrome, asthma, some cancers, and Alzheimer’s disease) to the metabolic disorder known as insulin resistance, with widely divergent views of the pathogenesis by which it occurs.
Starfield 08/09D 4247
Sources: Willett & Leibel, Am J Med 2002;113 Suppl 9B:47S-59S. Taubes, Science 2009;325:256-60

What characterizes illness is its variability, not its average manifestations. Virtually all of the conclusions of randomized controlled clinical trials are based on the average response. Variability, which underlies the genesis of illness, the role of risk factors, and the impact of interventions, goes unrecognized.
Starfield 08/09D 4248

If many people with relatively low risk are subjected to the same interventions (e.g., the polypill) as those with high risk, two of the three principles of prevention (avoiding unintended effects and low cost-effectiveness) will be violated.
Starfield 09/09PREV 4271


Ambulatory Diagnostic Groups (ADGs)
Time limited (4)AllergiesAsthma
Likely to recur (3)Malignancy
Chronic medical (2)Chronic specialty (6)
DermatologicInjuries (2)Psychosocial/psychophysiologic (3)Signs/symptoms (3)
DiscretionarySee and reassurePreventive/administrativePregnancyDental
Total number of ADGs = 32Starfield 199797-018
Starfield 12/97AC 1260

Going from ADGs to ACGs• During a single year, a patient’s diagnoses may fall into as many as 32
distinct ADGs. The potential permutations are vast. For practicality, a case-mix system must have a manageable number of mutually-exclusive categories
• Clinically similar ADGs are combined into CADGs (collapsed ADGs).• Individual CADGs and the most common combinations are designated
as MACs (Major Ambulatory Categories) with one additional MAC for “all other combinations”
• ACGs are formed from the MACs, based upon relative contributions to resources use
• Some ACGs are subgroups of a MAC based on– age and/or sex– total number of ADGs– total number of major ADGs
Starfield 199797-093
Starfield 04/97AC 1145

Entire Population
Age >= 1
Age < 1 MAC-26
MACMAC--11
MACMAC--22ACG 0400
MACMAC--44ACG 0700
MACMAC--55ACG 0800
MACMAC--33 MACMAC--2525MACMAC--1919
MACMAC--2020ACG 3400
MACMAC--2222ACG 3600
MACMAC--2323ACG 3700
MACMAC--2121ACG 3500
MACMAC--1313ACG 1800
MACMAC--1414 MACMAC--1616ACG2400
MACMAC--1717MACMAC--1515ACG2300
MACMAC--77ACG 1000
MACMAC--88ACG 1100
MACMAC--1010
MACMAC--1111ACG 1600
MACMAC--99ACG 1200
MACMAC--66ACG 0900
MACMAC--1212 MACMAC--1818ACG 2800
MACMAC--2424
To MAC 26
tree
Split into MACs,Based on CADGs
To MAC 24
tree
To MAC 12
tree
Age
1
2-5
6 +
ACG 0100
ACG 0200
ACG 0300
ADG05 ?
Yes
No
ACG 0600
ACG 0500
ADG25 ?
ADG24?
NoYes
Yes
No
ACG 1300
ACG 1400
ACG 1500
Age
1
2-5
6 + ADG05 ?
Yes No
ACG 2200
ACG 2000
ACG 2100
ADG25?
ADG24?
NoYes
Yes
NoACG 2600
ACG 2500
ACG 2700
1 or 2 input files?
Age
1
2-5
6 +
ADG05 ?
Yes No
12 +
ACG 3100
ACG 3000
ACG 2900
ACG 3200ACG 3300
2
Claims info?
Yes
No
1
ACG 5100
ACG 5200
ACG 5110
ACG 1900
ACG 9900Missing Age
MAC Major Ambulatory CategoryADG Ambulatory Diagnostic GroupCADG Collapsed ADGACG Ambulatory Care Group
Key
Starfield 199898-007
Decision Tree for ACGs
Source: JHU ACG Case Mix Adjustment System, V. 4.0, 1997.Starfield 04/97AC 1091

MAC-12
# of ADGs
Provides warning if :Gender = Male,Age < 10 or age > 55
0 -1 2-3
# of MajorADGs
ACG 1730
0 1+
4-5
# of MajorADGs
0 1+
6+
# of MajorADGs
ACG 1731
ACG 1732
Yes
No
Delivered?
ACG 1741
ACG 1742
Yes
No
Delivered?
ACG 1751
ACG 1752
Yes
No
Delivered?
ACG 1761
ACG 1762
Yes
No
Delivered?
ACG 1771
ACG 1772
Yes
No
Delivered?
0 1+
ACG 1721
ACG 1722
Yes
No
ACG 1720
Delivered?
ACG 1740 ACG 1750 ACG 1760 ACG 1770
MAC Major Ambulatory CategoryADG Ambulatory Diagnostic GroupACG Ambulatory Care Group
Key
ACG 1711
ACG 1712
Yes
No
ACG 1710
Delivered?Note: This level of branching is optional
Starfield 199898-008
Decision Tree for MAC 12 – Pregnant Women
Starfield 04/97AC 1092

# of ADGs
0-5 6+
Note: This level ofbranching is optional
* Low birth weight refers to infants less than 2500 grams
# of MajorADGs
1+0
Yes
No
Yes
No
Yes
No
Yes
No
0 1+
MAC Major Ambulatory CategoryADG Ambulatory Diagnostic GroupACG Ambulatory Care Group
Key
ACG 5310 ACG 5320 ACG 5330 ACG 5340
Lowbirth weight *
Lowbirth weight *
Lowbirth weight *
Lowbirth weight *
ACG 5312
ACG 5311
ACG 5322
ACG 5321
ACG 5332
ACG 5331
ACG 5342
ACG 5341
MAC-26
# of MajorADGs
Starfield 199898-009
Decision Tree for MAC 26 – Infants
Starfield 04/97AC 1093

MAC-24MAC-24
# of ADGs
# of ADGs
ACG 38001-16
35 +
17-34 SexSex
ACG 3900
ACG 4000
ACG 4100
Female
Male
AgeAge
2-3
AgeAge
1-16 # ofMajorADGs
17 + # ofMajorADGs
0
ACG 5020
ACG 50101
ACG 50302 +
0 - 1
ACG 5050
ACG 50402
ACG 50603
ACG 50704 +
10 +
17-44 # of Major ADGs
0
ACG 4320
ACG 43101
ACG 43302 +
1 - 16 # of Major ADGs
45 + # ofMajorADGs
0
ACG 4420
ACG 44101
ACG 44302 +
AgeAge
4-5
0ACG 4210
ACG 42201 +
35 +# of
MajorADGs
ACG 4920
ACG 49102
ACG 49303
ACG 49404 +
AgeAge
6-9
17-34 SexSex
6- 16 # of Major ADGs
1 - 5 # of Major ADGs
0 - 1
M
F
# ofMajorADGs
# ofMajorADGs
0
ACG 4720
ACG 47101
ACG 47302 +
0
ACG 4820
ACG 48101
ACG 48302 +
ACG 4510
ACG 45201 +
0
ACG 4610
ACG 46201 +
0
MAC Major Ambulatory CategoryADG Ambulatory Diagnostic GroupACG Ambulatory Care Group
Key
Starfield 199797-060
Decision Tree for MAC 24 – Multiple ADG Categories
Starfield 04/97AC 1094

AC 1095Figure 2: Decision Tree for MAC 12 -- Pregnant women
MAC-12
# of ADG s
Provides warning if : Gender = Male, Age < 10 or age > 55
0 -1 2-3
# of MajorADG s
ACG 1730
0 1+
4-5
# of MajorADG s
0 1+
6+
# of MajorADG s
ACG 1731
ACG 1732
Yes
No
Delivered?
ACG 1741
ACG 1742
Yes
No
Delivered?
ACG 1751
ACG 1752
Yes
No
Delivered?
ACG 1761
ACG 1762
Yes
No
Delivered?
ACG 1771
ACG 1772
Yes
No
Delivered?
0 1+
ACG 1721
ACG 1722
Yes
No
ACG 1720
Delivered?
ACG 1740 ACG 1750 ACG 1760 ACG 1770
MAC Major Am bulatory CategoryADG Ambulatory Diagnost ic GroupACG Ambulatory Care Group
Key
ACG 1711
ACG 1712
Yes
No
ACG 1710
Delivered?Note: This l evel of branchi ng is opt ional
Entire Population
Age >= 1
Age < 1 MAC-26
MAC-1MAC-1
MAC-2MAC-2ACG 0400
MAC-4MAC-4ACG 0700
MAC-5MAC-5ACG 0800
MAC-3MAC-3 MAC-25MAC-25MAC-19MAC-19
MAC-20MAC-20ACG 3400
MAC-22MAC-22ACG 3600
MAC-23MAC-23ACG 3700
MAC-21MAC-21ACG 3500
MAC-13MAC-13ACG 1800
MAC-14MAC-14 MAC-16MAC-16ACG 2400
MAC-17MAC-17MAC-15MAC-15ACG 2300
MAC-7MAC-7ACG 1000
MAC-8MAC-8ACG 1100
MAC-10MAC-10
MAC-11MAC-11ACG 1600
MAC-9MAC-9ACG 1200
MAC-6MAC-6ACG 0900
MAC-12MAC-12 MAC-18MAC-18ACG 2800
MAC-24MAC-24
To MAC 26
tree
Spl it into MACs,Based on CADGs
To MAC 24
tree
To MAC 12
tree
Figure 1: Decision Tree for ACGs
Age
1
2-5
6 +
ACG 0100
ACG 0200
ACG 0300
ADG05 ?
Yes
No
ACG 0600
ACG 0500
ADG25 ?
ADG24?
NoYes
Yes
No
ACG 1300
ACG 1400
ACG 1500
Age
1
2-5
6 + ADG05 ?
Yes No
ACG 2200
ACG 2000
ACG 2100
ADG25?
ADG24?
NoYes
Yes
NoACG 2600
ACG 2500
ACG 2700
1 or 2 input f iles?
Age
1
2-5
6 +
ADG05 ?
Yes No
12 +
ACG 3100
ACG 3000
ACG 2900
ACG 3200ACG 3300
2
Claim s info?
Yes
No
1
ACG 5100
ACG 5200
ACG 5110
ACG 1900
ACG 9900Mi ssing Age
MAC Major Am bulatory CategoryADG Ambulatory Diagnost ic GroupCADG Coll apsed ADGACG Ambulatory Care Group
Key
Figure 3: Decision Tree for MAC 26 -- Infants
# ofADG s
0-5 6+
Note: This l evel ofbranchi ng is opt ional
* Low Birthweight refers to infants less than 2500 grams
#of Maj orADG s
#of Maj orADG s
1+0
Yes
No
Yes
No
Yes
No
Yes
No
0 1+
MAC Major Am bulatory CategoryADG Ambulatory Diagnost ic GroupACG Ambulatory Care Group
Key
ACG 5310 ACG 5320 ACG 5330 ACG 5340
LowB irthweight *
LowB irthweight *
LowB irthweight *
LowB irthweight *
ACG 5312
ACG 5311
ACG 5322
ACG 5321
ACG 5332
ACG 5331
ACG 5342
ACG 5341
MAC-26
MAC-24
# of ADG s
ACG 3800 1-16
35 +
17-34 Sex
ACG 3900
ACG 4000
ACG 4100
Female
Male
Age
2-3
Age
1-16 # ofMaj orADG s
17 + # ofMaj orADG s
0
ACG 5020
ACG 50101
ACG 50302 +
0 - 1
ACG 5050
ACG 50402
ACG 50603
ACG 50704 +
10 +
Figure 4: Decision Tree for MAC 24 -- Multiple ADG categories
17-44 # of Maj or ADG s
0
ACG 4320
ACG 43101
ACG 43302 +
1 - 16 # of Maj or ADG s
45 + # ofMaj orADG s
0
ACG 4420
ACG 44101
ACG 44302 +
Age
4-5
0ACG 4210
ACG 42201 +
35 +# of
Maj orADG s
ACG 4920
ACG 49102
ACG 49303
ACG 49404 +
Age
6-9
17-34 Sex
6- 16 # of Maj or ADG s
1 - 5 # of Maj or ADG s
0 - 1
M
F
# ofMaj orADG s
# ofMaj orADG s
0
ACG 4720
ACG 47101
ACG 47302 +
0
ACG 4820
ACG 48101
ACG 48302 +
ACG 4510
ACG 45201 +
0
ACG 4610
ACG 46201 +
0
MAC Major Am bulatory CategoryADG Ambulatory Diagnost ic GroupACG Ambulatory Care Group
KeyStarfield 04/97AC 1095
Recommended