
Managing Complex Diabetic Patients in the Primary Care Setting
Tyree Morrison, CRNP, CDE
Laura Previte, RN, BSN

OBJECTIVES
• Discuss epidemiology of diabetes
• Present overview of current treatment guidelines
• Discuss challenges of caring for diabetics in primary care setting
• Using medical home model of care
• Understand what we created at FPCA
• Case studies from FPCA

DIABETES FACTS
CDC Data, 2014
• 29.1 million people have diabetes
• 1 out of 4 do not know they have diabetes
• 86 million have prediabetes – more than 1 out of 3 adults
• $245 billion a year in medical costs and lost work wages
• Medical costs twice as high Continued…

DIABETES FACTS
• 9 out of 10 do not know they have prediabetes
• Without weight loss and moderate physical activity, 15-30% of people with prediabetes will develop type 2 diabetes within 5 years
• Risk of death for adults with diabetes is 50% higher than for those without diabetes
– 7th leading cause of death in U.S.
• Medical costs are twice as high for those with diabetes

DIAGNOSTIC CRITERIA
Diagnostic criteria for pre-diabetes and type 2 diabetes mellitus
OR 2 hour plasma glucose > 200 mg/dL during oral glucose tolerance test
Random plasma glucose > 200 mg/dL with classic symptoms of hyperglycemia
2 fasting glucose readings of > 126 mg/dL
OR

THE COMPLEX DIABETIC PATIENT
What constitutes a “complex” diabetic patient -Hyperglycemia plus Multiple Co-Morbid Conditions and Complications which include:
• Dyslipidemia • Hypertension • Obesity/Weight Management Issues • Renal Disease • Peripheral and Autonomic Neuropathy • Diabetic Eye Disease • Gastrointestinal • Peripheral Vascular Disease • Dental disease • Heart failure

CURRENT TREATMENT GUIDELINES
ADA AND JOSLIN Cornerstones of Treatment: • Lifestyle modification #1 intervention • Individual approach to medication and glycemic
control targets • Team approach
– Medical specialists – Diabetes educators
• Patient-centered – self-management • Individualized treatment plan
CHALLENGES IN PRIMARY CARE SETTING
To refer or not refer… Decision Tree
Acuity and age of patient
Availability of endocrinologists
Cost of specialists
Wait time for appointments
Losing patient
connection
FPCA STATS
At Frederick Primary Care Associates (FPCA) • 9 practice sites • 45 providers • ~73,000 active patients • Office hours 7 days a week, including evenings
and walk-ins • 1 out of 10 adult patients have diabetes (~6,000
patients) • 1 out of 3 adult patients with BMI >30 (~23,000
patients)
EDUCATION – THE MISSING PIECE
History of FPCA’s clinical education program • Comprehensive Wellness Program with focus on diabetes • 6-week diabetes education class • One-on-one 30-minute consultations • Continuous glucose monitor • Insulin pumps • Weight management/nutritional counseling • Seasonal food seminars • Newsletter • Support groups And more….

WHAT FPCA OFFERS DIABETICS
• One-on-one diabetes education consultations
• Insulin and oral medication management
• Continuous glucose monitoring
• Insulin pump training and management
• Registered Nurse who provides care coordination

DISADVANTAGES FOR PATIENTS…
• Stigma of not seeing specialist
• Limited scope of practice
• No hospital rounding

ADVANTAGES FOR PATIENTS…
• Continuity of care
• Facilitated communication between providers
• Comprehensive patient data available through EMR
• Familiarity with practice
• Non-diabetes needs addressed
• Lower cost of co-pay
• More 1-on-1 attention

THEIR STORIES…

IDENTIFYING PATIENTS
Patient must be:
• Appropriate for outpatient management
• Engaged in self-management
Identified by:
• PCP referrals
• Outside referrals
• Health IT reports – i.e., diagnostic studies, hospitalizations, CRISP, PCMH program, etc.
• Patient/Self referrals
PATIENT-CENTERED MEDICAL HOME (PCMH)
According to National Committee for Quality Assurance (NCQA) – A way of organizing primary care
• Emphasizes care coordination
• Emphasizes communication
– Higher quality
– Lower costs
– Improve experience of care for patients and providers
– Care coordination (goal-oriented)
– Population health http://www.ncqa.org/Programs/Recognition/Practices/PatientCenteredMedicalHomePCMH.aspx

WHAT IS CARE COORDINATION?
NCQA definition: “…ensure that…beneficiaries’ health care needs, preferences
for health services and information sharing across health care staff and facilities are met over time. Care coordination maximizes the use of effective, efficient, safe, and high-quality patient services…that ultimately lead to improved health care outcomes.”
National Quality Forum definition: “Conscious effort by two or more health care professionals to
facilitate and coordinate the appropriate delivery of health care services for a patient.”

PCMH AND DIABETES CARE
• Team/holistic care and facilitate coordination with appropriate resources – i.e., PCP, specialist, medical resources, community programs, prescription assistance plans, etc.
• Closer monitoring • Avoid unnecessary hospital or emergency room encounters • Provide education about health condition • Encourage patient to actively participate in health care
decisions and self-management • Discuss concerns or questions with nurse • Support to patient and family • Solicit input regarding goals and management plan
COSTS AND BENEFITS
COSTS
• Nurse care coordinator salary
• Health information technology support
• Ramp up to become a qualified PCMH through NCQA
• Patient support resources www.acponline.com
BENEFITS
• Quality time spent with patients
• Early intervention
• Support
• Liaison
• Engage patients in their care
BENEFITS OF THE PROGRAM
LET’S MEET BETSY…
Betsy…
• 59-year-old, married, white female
• No children
• Self-employed writer
• No smoking/alcohol/substance use
• 8-year history of diabetes
CARE PLAN GOALS
PCP’S GOALS
• Diabetes education
• Diabetes control
• Lower cholesterol
• Weight loss
• Medication management
PATIENT’S GOALS
• Weight loss
• Diabetes control

PATIENT HISTORY
Past Medical History: Ovarian cyst, bronchitis, asthma, anemia, allergies, congenital duplicate kidney, osteoarthritis hips and knees
Past Surgical History: Right nephrectomy, bilateral total knee replacements, tubal ligation, breast reduction
Family History: Heart disease, mental health issues

BARRIERS TO OPTIMAL HEALTH
• Transportation
• Financial
• Non-adherence (medication)
• Knowledge deficit/lack of understanding
• Mobility
• Caregiver duties

UNCONTROLLED CONDITIONS
• DIABETES
• OBESITY
• HYPERLIPIDEMIA
• DEPRESSION
DIABETES
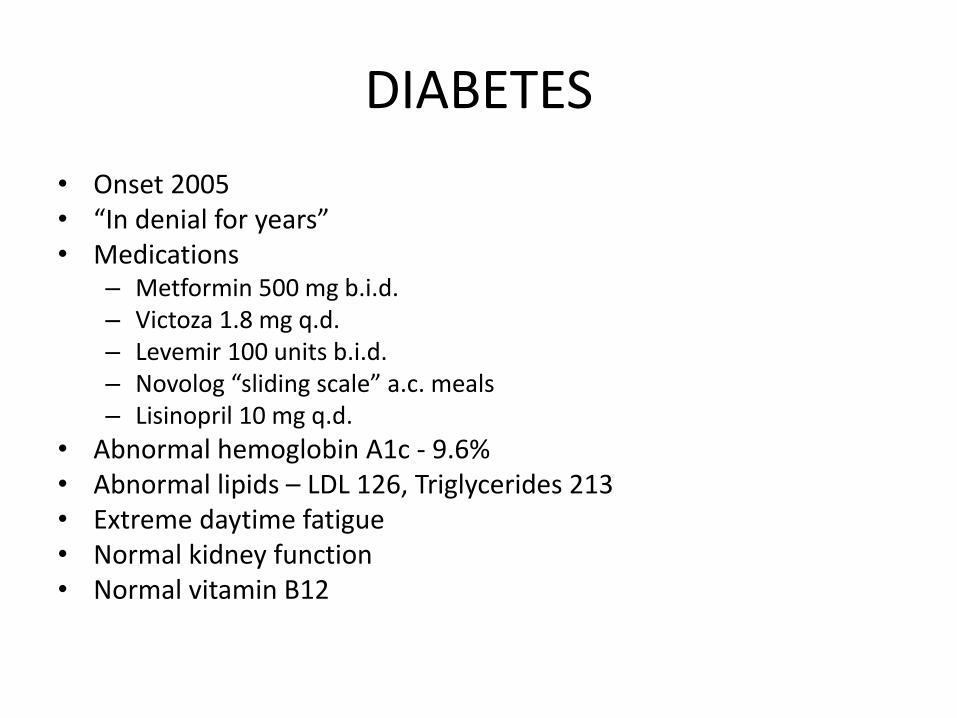
• Onset 2005 • “In denial for years” • Medications
– Metformin 500 mg b.i.d. – Victoza 1.8 mg q.d. – Levemir 100 units b.i.d. – Novolog “sliding scale” a.c. meals – Lisinopril 10 mg q.d.
• Abnormal hemoglobin A1c - 9.6% • Abnormal lipids – LDL 126, Triglycerides 213 • Extreme daytime fatigue • Normal kidney function • Normal vitamin B12
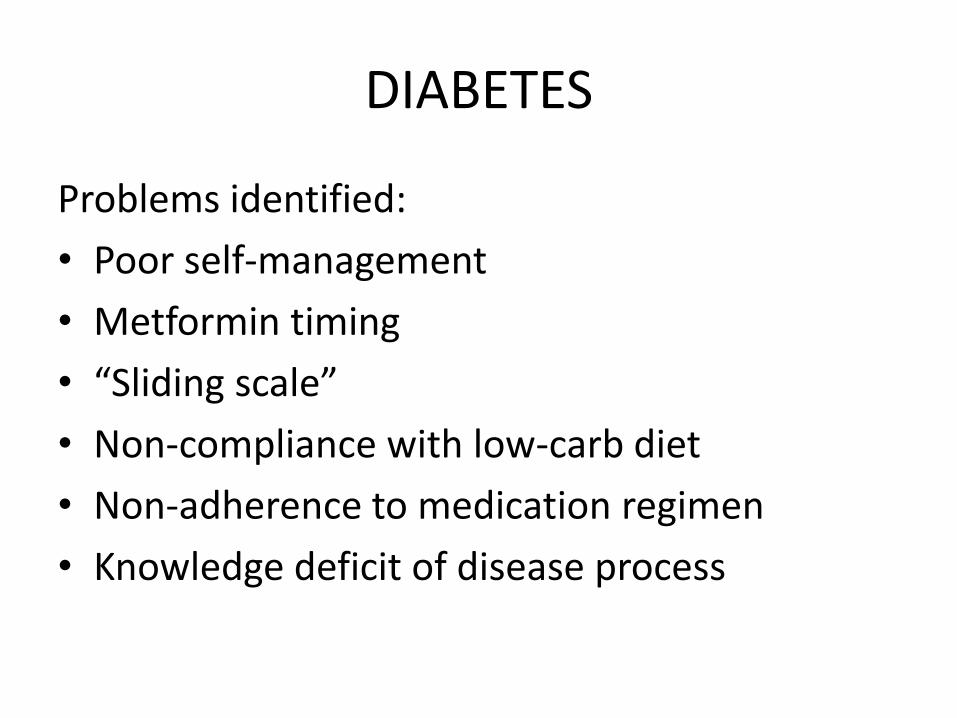
DIABETES
Problems identified:
• Poor self-management
• Metformin timing
• “Sliding scale”
• Non-compliance with low-carb diet
• Non-adherence to medication regimen
• Knowledge deficit of disease process

OBESITY
• 20+ year history
• Weight fluctuations – 275-317 over past 10 years
• “Never exercised”
• Bilateral TKRs
• Extreme fatigue

HYPERLIPIDEMIA
• Onset 15 years ago
• Non-compliant with low-fat diet
• Strong family history of heart disease
• Abnormal lipid panel: – Total cholesterol 230 mg/dL
– Triglycerides 213 mg/dL
– HDL 61 mg/dL
– LDL 126 mg/dL
• Pravastatin 80 mg daily
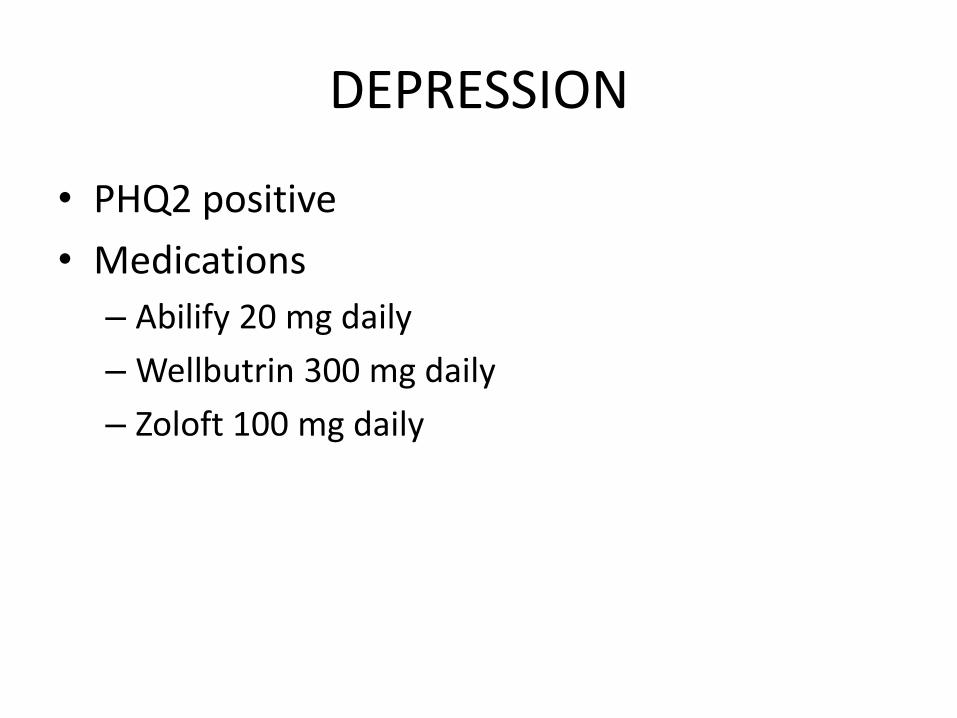
DEPRESSION
• PHQ2 positive
• Medications
– Abilify 20 mg daily
– Wellbutrin 300 mg daily
– Zoloft 100 mg daily

FALL 2013
CARE PLAN INITIATED Focused on diabetes • Diabetes education • “Sliding scale” insulin regimen • Metformin timing • Diabetes education class • Pill organizer • Excedrin Migraine changed to caffeine tablets • Started baby aspirin • Hemoglobin A1c 8.5% (down from 9.6%) • Started hepatitis B series • Foot exam • Diabetes education class (transportation issue) • Started exercising 15 minutes 3x/week • Continuous glucose monitoring performed

CGM PRIOR TO INSULIN PUMP
Average blood sugar 156 + highest blood sugar 277 + lowest blood sugar 73 + ~280 units of insulin daily + extended postprandial excursions =
GOOD CANDIDATE FOR INSULIN PUMP

A1Cs PRIOR TO INSULIN PUMP
4
5
6
7
8
9
10
11
12
13
14
HEMOGLOBIN A1Cs

WINTER 2013
• A1c 7.1% (down from 8.5%) • Insulin pump process started
– Indecision – Fear – Financial concerns
• Support from PCP, CDE, and Medtronic • Insulin pump started January
– Oral diabetic meds stopped
• Total daily insulin use ~130u/day • Attending insulin pump support group • Weight gain Tradjenta vs. Victoza • Hypoglycemia unawareness discovered
– Education performed by care coordinator and CDE
• Continues exercising 15 minutes 3-5x/week

SPRING 2014
“I feel so much better. I’m not fatigued anymore.” • Stopped caffeine! • Hemoglobin A1c 6.5% (down from 7.1%)!! • Blood sugars in 70-100 range a.c. • Final hep B and shingles vaccinations • Regular exercise 30 minutes 3x/week – bike/treadmill • Daily insulin usage 100 units/day max no meal boluses • Monthly insulin pump downloads interim phone contact • DRE scheduled • WWE by PCP • Agrees to Outcomes medication review
– Interested in decreasing antidepressant usage tapering schedule for Abilify provided by PCP
– Switched to Victoza
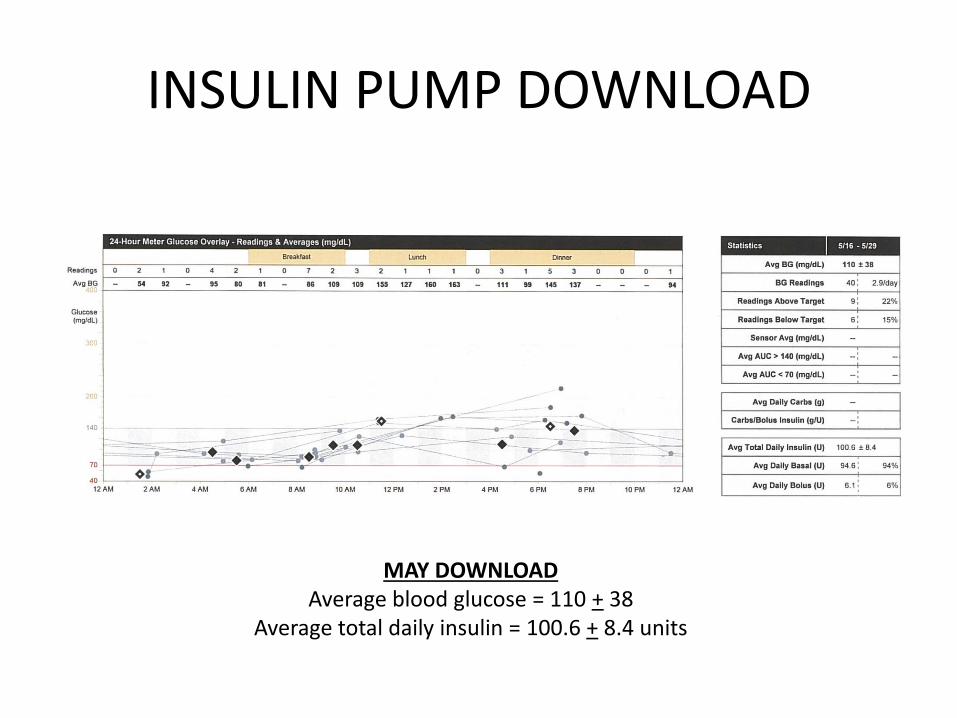
INSULIN PUMP DOWNLOAD
MAY DOWNLOAD Average blood glucose = 110 + 38
Average total daily insulin = 100.6 + 8.4 units

SUMMER 2014
• Hemoglobin A1c 5.8%!!
• Monthly insulin pump downloads
• Mentoring/supporting other “pumpers”
• Weight loss
• Exercise – treadmill, bike, Zumba!
• Weaning off Abilify
• Recent labs WNL diabetes, renal, lipids
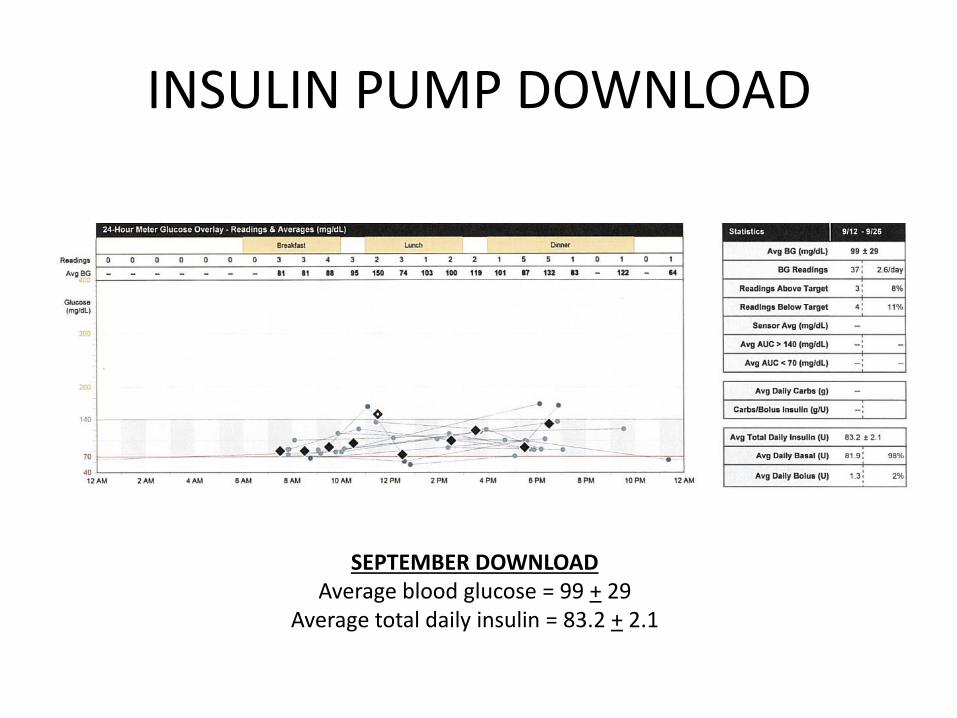
INSULIN PUMP DOWNLOAD
SEPTEMBER DOWNLOAD Average blood glucose = 99 + 29
Average total daily insulin = 83.2 + 2.1

A1Cs POST INSULIN PUMP
4
5
6
7
8
9
10
HEMOGLOBIN A1Cs

BENEFITS OF PUMP

CARE PLAN GOALS
PCP’S GOALS
• Diabetes education
• Diabetes control
• Lower cholesterol
• Weight loss
• Medication management
PATIENT’S GOALS
• Weight loss
• Diabetes control
CARE PLAN GOALS
PCP’S GOALS
Diabetes education
Diabetes control
Lower cholesterol
Weight loss
Medication management
PATIENT’S GOALS
Weight loss
Diabetes control
SUMMARY
How did Care Coordination benefit patient?
• Optimal diabetes control accomplished through support, education, resources, communication.
• Medication management/compliance
• Improved depression – weaning off high-volatility medications
• Improved energy and overall sense of well being
• Exercising regularly

LESSONS LEARNED
• Have a 5-year plan • Support of Board of Directors • Budget • Adequate staffing • Marketing plan • Referral base • Funding • Clinic space • Ongoing training/education • Develop relationships with community groups and
pharmaceutical/medical equipment companies
REFERENCES
Recommended

















