-
8/12/2019 Malformations of Oesophagus
1/24
-
8/12/2019 Malformations of Oesophagus
2/24
DEFINITION
It is the failure of the esophagus to form a continuous
passagefrom pharynx to stomach during embryonic development
resultingin obstruction in infants normal swallowing routes.
INCIDENCE
Approximately in infants of 3,000-3,500 live births.Occur Both
males and females, frequently associated withprematurity.It is the
25th most common birth defect.
-
8/12/2019 Malformations of Oesophagus
3/24
ETIOLOGYUnknownChromosomal anomalies (trisomy 18, trisomy 21,
and trisomy 13)Failure of embryonic developmentDigestive tract
problems(diaphragmatic hernia, intestinal atresia or
imperforated anus.)Congenital heart diseases(ventricular septal
defect,tetralogy offallot or patent ductus arteriosus.)Renal and
urinary tract problems(horseshoe or polycystickidney,absent kidney
or hypospadias)
-
8/12/2019 Malformations of Oesophagus
4/24
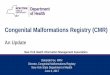
"LONG GAP", PURE OR ISOLATED ESOPHAGEAL ATRESIA ESOPH AGEAL
ATRESIA WITH PROXIMAL TEF
(TRACHEOESOPHAGEAL FISTULA) ESOPHAGEAL ATRESIA WITH DISTAL TEF
(TRACHEOESOPHAGEA
FISTULA) ESOPHAGEAL ATRESIA WITH BOTH PROXIMAL AND DISTAL TEF
(TWO TRACHEOESOPHAGEAL FISTULAS) TEF (TRACHEOESOPHAGEAL FISTULA)
ONLY WITH NO
ESOPHAGEAL ATRESIA ESOPHAGEAL STENOSIS
-
8/12/2019 Malformations of Oesophagus
5/24
-
8/12/2019 Malformations of Oesophagus
6/24
PathophysiologyEsophagus developed from first segment of
embryonic gut.During the 4 th and 5 th week of gestation ,forgut
normally
lengthens and separate longitudinally and longitudinal
portion
fuse to form parallel channels. Anomalies involving trachea
and
esophagus are caused by defective incomplete fusion of the
tracheal folds following separation or altered cellular
growth
during embryonic development.
-
8/12/2019 Malformations of Oesophagus
7/24
CLINIC L M NIFEST TION
Excessive Salivation & DroolingFrothy white bubbles in babys
mouth 3CS of TEF
Chocking (when the baby is feeding)
Coughing (when the baby is feeding)Cyanosis (when the baby is
feeding)
VomitingBreathing Difficulty
Abdominal Distension( very round full abdomen)
-
8/12/2019 Malformations of Oesophagus
8/24
ApneaIncreased respiratory distressPneumonitisRegurgitation or
Gagging
Signs of gastro esophageal refluxChronic respiratory
problems
-
8/12/2019 Malformations of Oesophagus
9/24
DI GNOSTIC EV LU TION
History collectionPhysical ExaminationECGBronchoscopy
Radiographic Studies (X-Ray, Ultrasound, CT scan, MRI)
-
8/12/2019 Malformations of Oesophagus
10/24
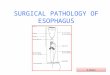
PLAIN X-RAY WITH CONTRAST IN THEUPPER ESOPHAGUS SHOWING
ATRESIA
-
8/12/2019 Malformations of Oesophagus
11/24
Genetic testing. Molecular genetic testing Chromosome
analysis
EA/TEF may be suspected Prenatally by:-
Ultrasound examination Fetal MRI
-
8/12/2019 Malformations of Oesophagus
12/24
EA may be detected Postnatally by:Failure to pass a nasogastric
(NG) tube and
radiographs that demonstrate coiling of the NG tubethe
pouch.
Tracheal compression and deviation on plain
chestradiographs.
Absence of a gastric bubble on plain radiographs,which may
suggest EA without a TEF or EA with a
proximal TEF. Three-dimensional CT scanning.
-
8/12/2019 Malformations of Oesophagus
13/24
MEDIC L M N GEMENT
Treatment include:-Maintanance of patient airway.Prevention of
pneumonia.Gastric pouch decompression.
Surgical repair of anomalies.Supportive therapy.Stop oral
intake, start IV fluids.
SURGIC L M N GEMENT
-
8/12/2019 Malformations of Oesophagus
14/24
SURGIC L M N GEMENTtransoesophageal fistula and
esophagealatresia repair
Normal anatomy
-
8/12/2019 Malformations of Oesophagus
15/24
Procedure, part 1 Part 2
-
8/12/2019 Malformations of Oesophagus
16/24
-
8/12/2019 Malformations of Oesophagus
17/24
Cervical EsophagostomyBauginageEsophageal replacement
procedure
1. Colon Interposition .
2. Gastric tube interposition. ET Tube intubation
-
8/12/2019 Malformations of Oesophagus
18/24
Complication Of Surgery
Reaction to medicines.Breathing problems.Bleeding.Infection.
Collapsed lung(pneumothorax).Food leakage from the area that is
repair.Low body temperature(hypothermia).Narrowing of the repaired
organ.
Re-opening of the fistula.
-
8/12/2019 Malformations of Oesophagus
19/24
Esophageal strictures / Esophageal stenosis An esophageal
stricture which is also known as esophageal stenosis is were
the esophagus gradually narrows. Which can lead to problems
withswallowing.
Etiology The strictures are caused by inflammation in the
esophagus which leads to
scar tissue building up causing it to slowly over time narrow.
It can be caused by or associated with gastroesophageal reflux or
esophagitis Disfunctional lower esophageal sphincter Disordered
motiity Hiatal hernia Post esophageal treatment i.e lasre therapy
or photodynamic therapy.
Pathology The esophagus in very server cases may be reduced to
an opening the size of
a pencil or smaller which then causes food and fluids to be
delayed and tomove across the opening into the stomach slowly.
-
8/12/2019 Malformations of Oesophagus
20/24
Symptoms
A feeling that food is getting stuck in the esophagus difficulty
in swallowing (this may gradually occur over time) Swallowing may
be uncomfortable, (not necessarily painful) Bitter taste in the
mouth
Choking Coughing Shortness of breath Patient may be present with
aspiration or recurrent pneumonia
Weight loss
-
8/12/2019 Malformations of Oesophagus
21/24
Diagnosis
Anamnesis ; history of dysphagia and regurgitations X-ray with
barium meal CT scan Endoscopy
-
8/12/2019 Malformations of Oesophagus
22/24
-
8/12/2019 Malformations of Oesophagus
23/24
Treatment Endoscopic dilation of the stenosis Dilation, which
may be done at
the same time as the upper endoscopy examination and diagnosis.
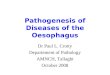
Techniques Bougie - soft rubber or plastic dilators are moved
across the
stricture, gently opening it., and the surgeon with increase the
size
of the dilator accordingly. Guided wire - A thin wire, placed
across the stricture, is used to
guide increasingly wider dilators over it. Balloons - balloons
shaped like sausages can be placed across the
stricture. Then the balloon is sharply inflated to open the
narrowed
area.
If gastroesphageal reflux has been the cause of the stricture
itneeds to be treated with proton pump inhibitor or H2
antagonist
-
8/12/2019 Malformations of Oesophagus
24/24
Balloon and Bougie soft rubber or plastic dilators