Low Cardiac Output Syndrome, what we can
Do???
Dr. Minati ChoudhuryProfessor
Department of cardiac AnaesthesiaAIIMS
New Delhi
Why to measure CO???
CO—the primary determinant of global O2 transport No absolute value that reflect circulatory adequacy A low CO is clearly detrimental
Achievement of satisfactory cardiac output is the primary aim cardio vascular management during the post operative scenario and ICU management

Satisfactory cardiac output?----
Cardiac index > 2 l/min/m2
Left sided filling pressures < 20mmHg
HR < 100/min
Warm well perfused extremities
Good urine output

Low cardiac output CI < 2 L/min/m2
Left sided filling pressures >20mmHg
SVR >1500dynes/sec/cm5
Requirement of IABP / inotropic support for more than 30 min in ICU to maintain SBP >90mmHg & CI > 2.2 L/min/m2
JCTVS 1996;112:38-51
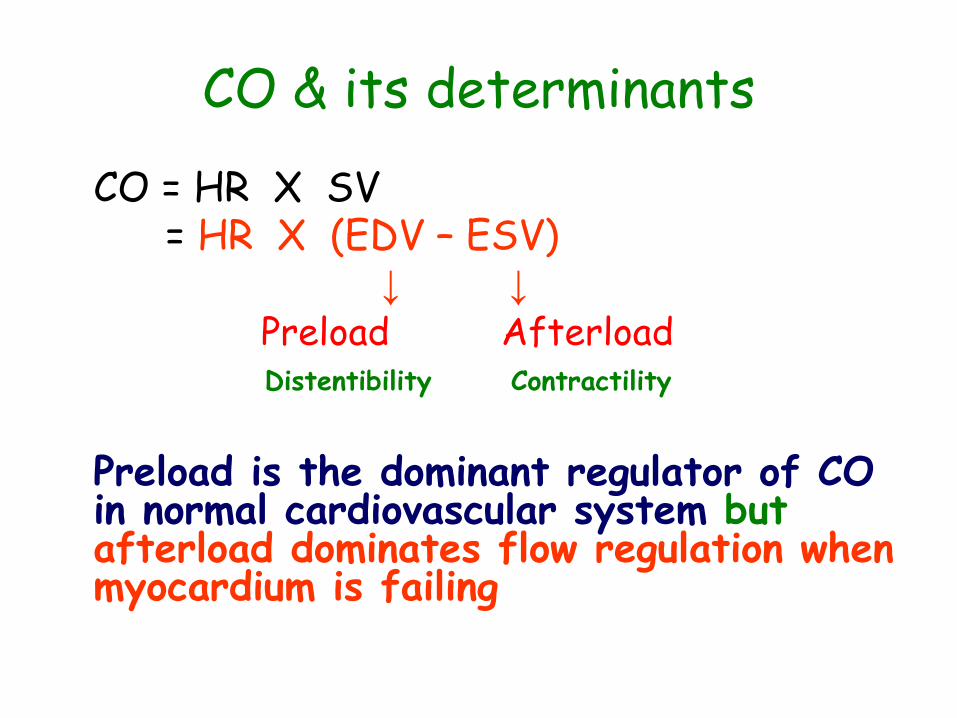
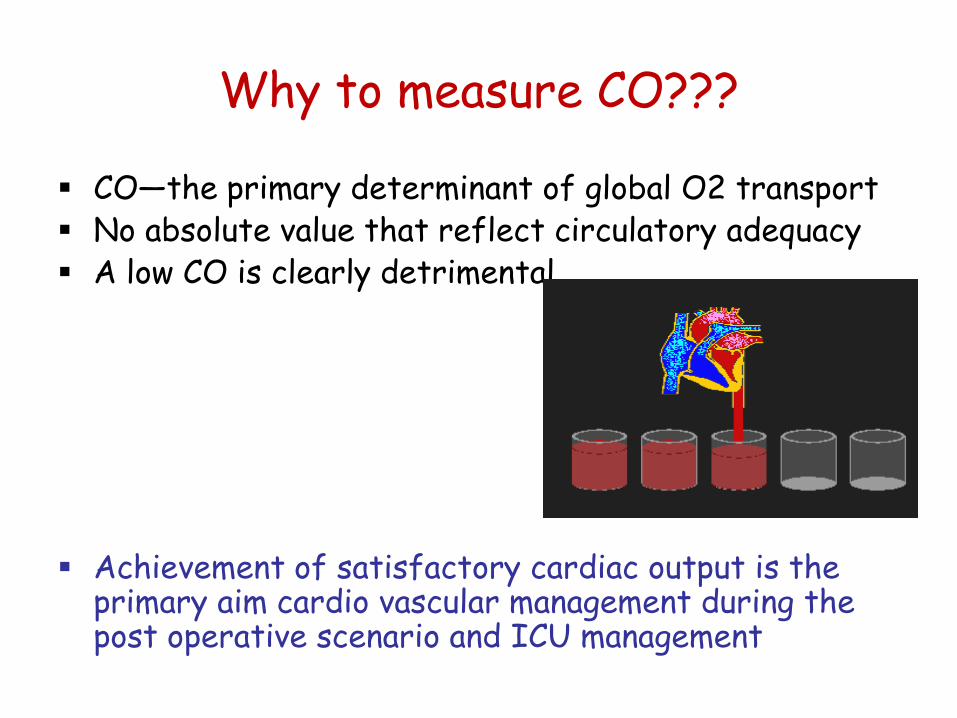
CO & its determinants
CO = HR X SV= HR X (EDV – ESV)
↓ ↓
Preload AfterloadDistentibility Contractility
Preload is the dominant regulator of CO in normal cardiovascular system but afterload dominates flow regulation when myocardium is failing

CO & its determinants
CO & its determinantsLUSITROPISM Abnormality of myocardial relaxation(Characteristic of aging
myocardium)
Diastolic dysfunction – ↓ diastolic complaince----- impaired systolic relaxation-------------inappropriate tachycardia
End result is LCOS with a small LV chamber at end diastole yet high filling pressures
ACE inhibitors improve diastolic compliance; lusitropicdrugs (CCB) improve impaired systolic relaxation; bradycardiac drugs (BB &CCB) correct inappropriate tachycardia & diuretics ↓ myocardial edema ------------improve compliance.
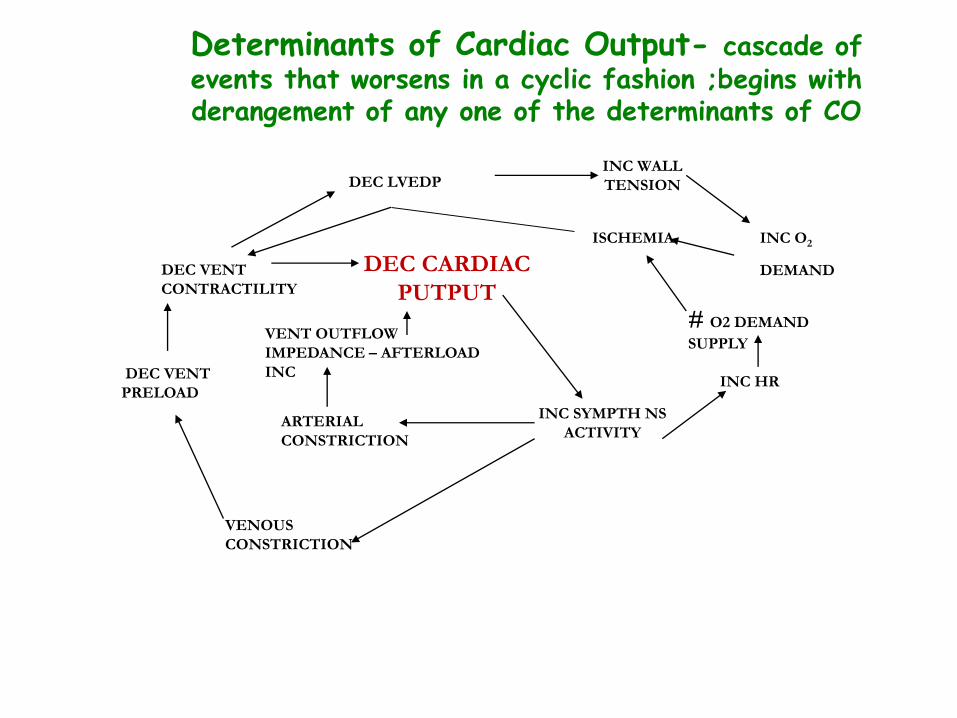
Determinants of Cardiac Output- cascade of events that worsens in a cyclic fashion ;begins with derangement of any one of the determinants of CO
DEC VENT
CONTRACTILITY
DEC VENT
PRELOAD
VENOUS
CONSTRICTION
ARTERIAL
CONSTRICTION
VENT OUTFLOW
IMPEDANCE – AFTERLOAD
INC
DEC CARDIAC
PUTPUT
DEC LVEDP
ISCHEMIA INC O2
DEMAND
INC SYMPTH NS
ACTIVITY
INC HR
# O2 DEMAND
SUPPLY
INC WALL
TENSION
EtiologyDec left vent preload
• Hypovolemia , bleeding vasodilatations for weaning, narcotics, sedatives
• Cardiac tamponade
• PPV & PEEP
• Rt. vent. dysfunction (RV infarction, Pul. HTN)
• Tension pneumothorax

Etiology
ed Contractility
• ed ejection fraction
• Myocardial stunting , ischemic / infarction poor intraoperative myocardial protection incomplete myocardial revascularization Anastomotic stenosis Coronary A. stenosis
• Hypoxia , hypercarbia acidosis

Etiology
Tachycardia & Bradycardia
Tachycardia will reduced cardiac filling time Bradycardia Atrial arrhtymias with loss of artial contraction Ventricular arrythmias

Etiology
ed after load• Vasoconstriction• Fluid overload
Diastolic dysfunction ( common finding after cardioplegic arrest)

EtiologySyndrome ass. with CV instability and hypotension.
• Sepsis ( Hypotension with ed SVR)
• Anaphylactic reaction (blood products , drugs)
• Adrenal insufficiency (primary or pt with preoperative steroids)
• Protamine reaction

Etiology
• Neurogenic Shock
Spinal anaesthesia
Direct damage to the vasomotor center of medulla
Altered function of the vasomotor center in response to low blood glucose( insulin shock)
Action of trainquilizers,narcotics or sedatives
Spinal cord injury
• Vasoplegic symptoms during liver transplantation

Factors Influencing LCOS
Preoperative
Intra operative
Postoperative

Factors Influencing LCOS-------Preoperative factors
• Age
Extremes of age
• Hypoxia
Experimental -----hearts of animals made cyanotic appear to be more susceptible to ischemia and re-perfusion injury than normal hearts.
• Hypertrophy
• Ischemia ---------myocardial dysfunction.
• Left to right shunts Large LR shunts -----------------postoperative LCOS
when the left ventricular run-off across the VSD is closed.

Factors Influencing LCOS------- Intra Operative Factors
• Anesthetic induction
Major surgery and cardiac surgery Hypertrophic myocardium….more risk
• Hypotension
Sudden decreased SVR as after induction may lead to a spell in cyanotic patients.

• Myocardial preservation …… cardiac surgery
• CPB Avoid Factors associated with myocardial injury during CPB
Persistent VF
Ventricular distension
Coronary embolism
Reperfusion
• Aortic cross clamp
Long aortic cross clamp -------------more chances of reperfusion injury -------------a direct predictor of postoperative LCOS and death.
Factors Influencing LCOS--------------Post Operative Factors
Preload After load Contractility Heart rate & rhythm Residual lesions (pulm regurg after transannular patch repair
of TOFResidual VSDResidual outflow obstruction )
All predispose to post op LCOS d/t vol & pressure overload on the myocardium
Pulmonary factors Extra cardiac causes
Assessment
Bedside physical examination (breath sounds, murmurs, warmth of extremities, peripheral pulses)
Hemodynamic measurements: assess filling pressures & determine CO with PAC, calculate SVR, measure SvO2
ABG (hypoxia, hypercarbia, acidosis/alkalosis), hematocrit (anemia), and serum potassium (hypo or hyperkalemia)

Assessment
• Agitation• Pulse Rate – tachycardia
volume – low• Blood pressure - borderline or low• Skin - pale, cool to touch• Rapid shallow breathing• Mucus membranes – dry• Urine output <1ml/kg/hr• Reduced peripheral temperature
Assessment
Capillary refill
May be useful marker of hypovolemia and myocardial function
Easy but many confounding factors: fever,roomtemp,vasoactive drugs…careful
Core temp vs peripheral temp difference
>3 degrees associated with LCO
Toe Temp -------------
• Hennings et al. -----cardiac index and the normalization of toe temperatures within 6 hours in adults following surgery are associated with good postoperative haemodynamic recovery.
• Knight -----in infants and children after cardiac surgery, toe temperature persistently <32°C even 6 hours after surgery was associated with a poor outcome.
• N. the toe temperature is 1/2way between environmental and core temp
• Toe temperature to environmental temperature gradient is
• less than 2°C poor perfusion state.• Approaches 0.5°C low output state is life
threatening

Assessment • Non-invasive blood pressure monitoring
In patients without edema, values obtained by non-invasive arterial blood pressure monitoring are very close to the values of invasive pressure measurements.
The principal cause of non reliable values with non-invasive pressure measurement is selecting a non-appropriate size of the cuff.
Assessment
• Pulse oximetry
Not accurate with low or very high values (below 80% or with values above 90%-95%)
Be aware of the presence of abnormal hemoglobins
Assessment
• Non Invasive monitoring Chest X-ray
ECG
Urine Output
Chest tube Drainage (Mediastinal Bleeding)
Echocardiography

Assessment
• Invasive monitoring Arterial blood pressure
Central venous pressure
Left atrial pressure
Thermodilution catheters
ABG
Mix venous blood gases

Assessment
• Arterial blood pressure
Hypotension is always pathologic and indicative of dysfunction of the cardiovascular system.

Assessment
2D echo --------very helpful• Quick; non-invasive
• Information
Residual defects
Degree and deviation of shunting
Ventricular function
Systolic
Diastolic
Degree of ventricular filling
Pericardial collections

Normal heart during systole and diastole

LCOS-ECHO
Monitoring Of Low CO State
Central venous, pulmonary artery, RA and LA Pressures
• Central venous or right atrial lines -------- RV filling or preload in the presence of AV concordance.
• Low CVP inadequate preload ----- Need for volume• High CVP Fluid overload ----------- Diuretic therapy • & Fluid restriction
Diminished RV systolic or diastolic function (in the absence of TV disease or
shunts)• Persistently elevated PAP in relation to systemic BP----
RV dysfunction
Monitoring Of Low CO State
Cardiac Output Measurement
Continuous CO measurement to diagnose LCOS with the help of PA catheter, FloTrac, Picco…………………………..best used to interpret trends& to access response to change in therapy, rather than suggest need for intervention because of an abnormal absolute value

Monitoring Of Low CO StateMETABOLIC INDICATORS
LCOS ------- a state of impaired global perfusion anaerobic metabolism and ↑ metabolic acidosis.
Serial ABG analysis reveal ↑ levels of base deficit and ↓HCO3- levels
Frank et al……………….metab acidosis with ↑ pH is a late feature of ↓peripheral perfusion & care takers should not wait for this sign to diagnose LCOS
↑ in arterial lactate levels from 2 to 8 mmol/L; remaining near 8mmol/l for 2 hrs or more ↓ survival to 10% in acute LOS.
Normal plasma values for lactate 0.7-2.1 meq/l.Mild to moderate metabolic acidosis 5 meq/L
Severe metabolic acidosis 10 meq/L

Monitoring Of Low CO State
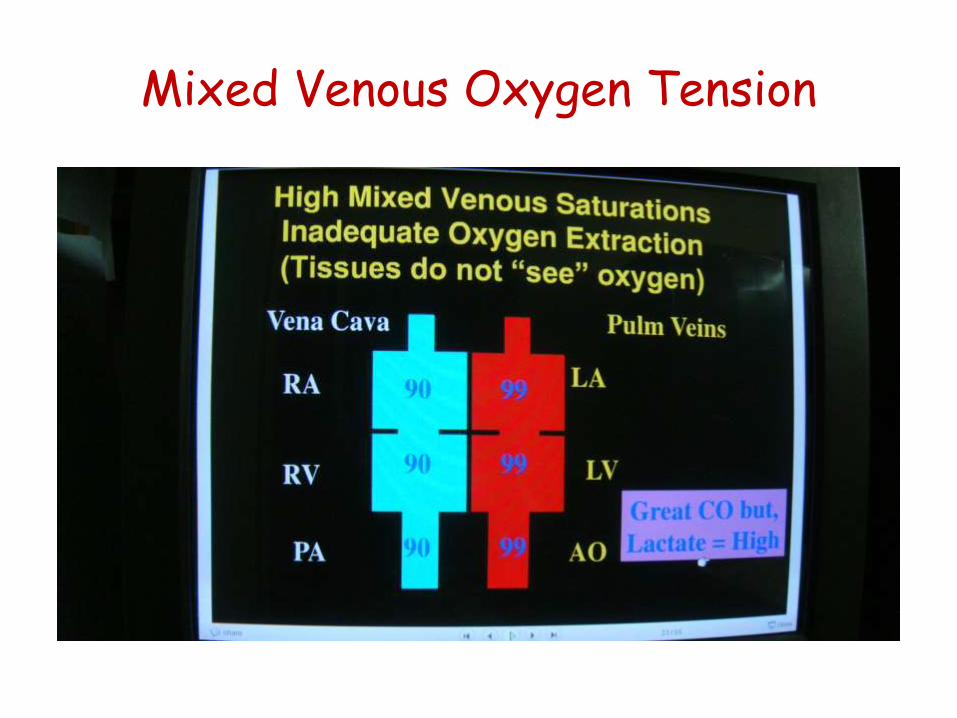
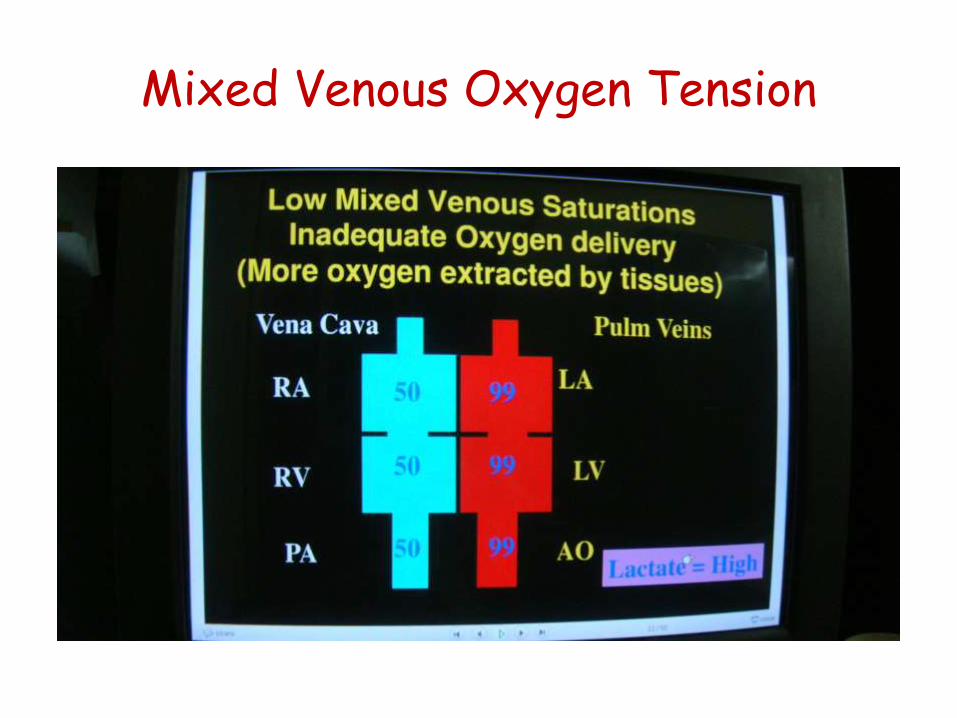
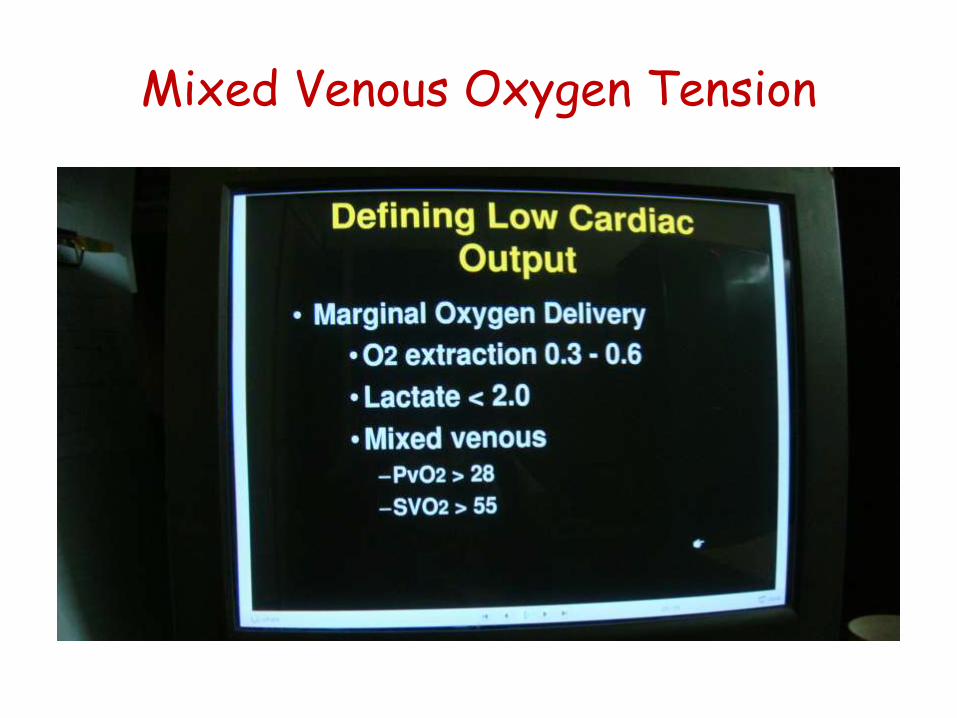
Mixed Venous Oxygen Tension
• Useful index of circulatory adequacy ……………….reflects to some extent near tissue oxygen levels.
• Relation b/w CO & SVO2 is not linear; a ↓ in SVO2 ----------proportionately larger ↓ in CO
• Sample for SVO2 ………PA catheter or central vein
SVO2 <30 mmHg CO inadequate
SVO2 < 23mmHg severely inadequate CO

Mixed Venous Oxygen Tension
Mixed Venous Oxygen Tension
Mixed Venous Oxygen Tension

Mixed Venous Oxygen Tension
Mixed Venous Oxygen Tension

How to manage??

MANAGEMENT OF HEMODYNAMIC PROBLEMS
BP PCWP CO SVR Plan
↓ ↓ ↓ ↓ Volume
N ↑ N ↑ Diuretic
↓ ↑ ↓ ↑ Inotrope
↑ ↑ ↓ ↑ Vasodilator
V ↑ ↓ ↑ Ino/vaso/IABP
↓ N N ↓ Alpha-agent
Management------------
Ensure satisfactory oxygenation & ventilation.
Treat ischemia or coronary spasm if suspected to be present --------- -NTG / CCB
Management------------
Optimize preload – + & curvilinear relation b/w EDV & contractility & appropriate vol loading remains the easiest, most rapid & most effective method of improving CO & tissue perfusion
a) Ideal LA pressure
Pts with preserved Pts with poorLV function LV function
↓ ↓
15 mmHg Low 20’s(Stiff hypertrophied LV with diastolic
dysfunctionSmall LV Chamber –MS: after LV
resectionPre existing pulm HTN from MV ds)

Management------
b) Response to volume infusion
• Failure of filling pressures to rise with volume
Capillary leak present in the early postop period
Vasodilatation associated with re-warning
Use of medications with vasodilatation properties like Propofol, narcotics
• Rise in filling pressures without ↑CO
INOTROPIC SUPPORT NECESSARY• Harmful effects of excessive preload- LV wall tension ↑ myocardial ischemia
(↓ Trans – myocardial gradient for CBF↑ myocardial o2 demand.)
- Interstitial edema of lungs V/Q abnormalitieshypoxemia
- Systemic venous HTN ↓ Perfusion pressure to other organs.
Kidneys – diuresisGIT – splanchnic congestionBrain – mental state altered

Management of LCOS Heart Rate and Rhythm
Atrio – venticular synchrony with HR of 90-100 b/min------------- 15-20 % improvement in CO provided by atrial contractionAtrial or atrio-ventricular pacing
Reduce Afterload
VasodilatorsMarginal C.O---------------------avoid hypotensionPoor C.O-----------------Cautions use of Vasodilators coz ↑ SVR from intense vasoconstriction is a compensatory mechanism to maintain perfusion to vital organs.
( SVR > 1500, vasodilators indicated)

Management ------------- Maintain blood pressure
Satisfactory C.O. & low SVR ---------- Moderate volume infusion may improve B.P. Commonly seen in sedated patients receiving medications with potent
vasodilator properties.
Marginal C.O.& low SVRNor-epinephrine is preferred (B- agonist prop.; maintenance of peripheral
venous tone ;avoid flooding the pt with volume).
BP & CO Marginal despite multiples ionotropsNorephinephrine
↓
CO still remain low ↓
IABP
Management ----------
If refractory hypotension – vasoplegiaMAP< 50,
Low filling pressures – CVP < 5, PCWP<10
Normal or elevated CI >2.5L/min/m2
Low SVR < 800
VasopressorMethylene blue 1.5 – 2mg/kg – 1 hr
Vasopressin 0.1- 0.4 U/min
Management ------------
Correct Anemia
Blood TransfusionsHct 24%
Difficult to wean from CPB-----/has haemodynamicevidence of severe ventricular dysfunction despite maximal medical therapy and IABP use of circulatory assist devices should be considered

Management ----------

Management---Inotropic and vasoactivedrugs
Selection of drugs
Adequate understanding of underlying cardiac pathophysiology.
Knowledge of α, ß or non adrenergic haemodynamic effects of these drugs.

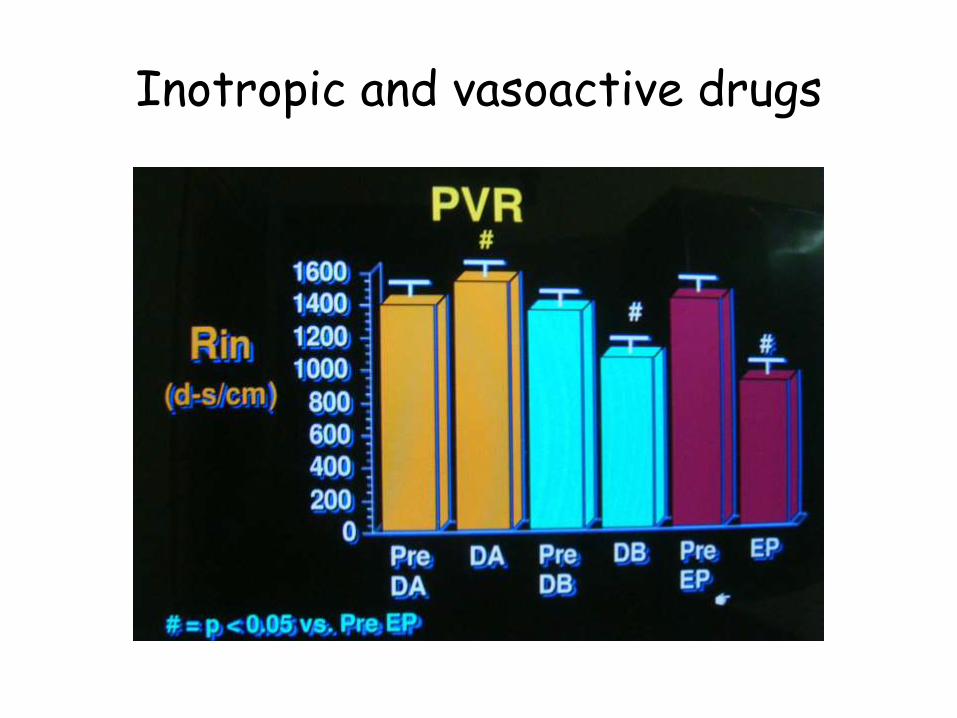
Inotropic and vasoactive drugs
DOPAMINE1. 2-3 ug/kg/mt ……………………Selective Dopaminergic effect – dilates
renal arteries - ↑ RBF & urine output.2. 3-8 ug/kg/mt……………………..Strong ß1 inotropic effect3. >8 ug/kg/mt ……………………….. Predominant œ effects (direct & by
endogenous NE release) ↑ SVR, ↑ BP, ↑ filling pressures.myocardial O2 consumption ↑
Indications
1st line drug for LCOS especially when SVR is low & BP marginal Profound tachycardia & excessive urine output.

Inotropic and vasoactive drugs
DOBUTAMINE
• Strong ß1 effect : increase contractivity & HR• Mild ß2 effect : ↓ SVR
Indications CO marginal ; Mild elevation in SVR Useful if Dopamine produces profound tachycardia
or excessive urine output.Synergistic effect PDE Inhibitors.

Inotropic and vasoactive drugs
Inotropic and vasoactive drugs
NOREPHINEPHRINE VERSUS DOBUTAMINE in LCOS septic shock
• Difficulty in determining which treatments are most helpful
• Norepinephrine to raising cardiac output in septic shock patients
• EACH PATIENT IS DIFFERENTDellinger RP, Vincent JL. Maintenance of high cardiac output in severe sepsis.
Presented at: 32nd Critical Care Congress; January 30, 2003; San Antonio, Tex.

Inotropic and vasoactive drugs
EPINEPHRINE
Potent ß1 inotropic agent – ↑ CO by ↑ in HR & contractility
<2 ug/mt ß2 effect that produces mild peripheral vasodilatation.
>2 ug/mt, œ effects ↑SVR & ↑ BP with A/E on myocardial O2 metabolism.
Usefulness is limited by the development of tachycardia & arrhythmias

Inotropic and vasoactive drugs
NOREPINEPHRINEPredominant œ effect ↑ SVR & BP ß1 effect ↑ contractility-------------- ↑ myocardial O2
demand & may prove detrimental to ischemic myocardium.
INDICATIONS
Low BP caused by low SVR.
1 - 20µg/mt (0.015-0.2µg/kg/min)
Inotropic and vasoactive drugs
ISOPROTERENOL
Strong ß1 effects but tachycardia limits utilityß2 effects lower SVR, PVR helpful in ↓ Rt. ventricular
after load
INDICATIONS
RV dysfunction with ↑ PVR.
Supplemented by Amrinone / milrinone
0.5 ug/mt -10 ug/mt (0.01- 0.1ug/kg/min)

Inotropic and vasoactive drugs
AMRINONE & MILRINONE
Improve CO by ↓ SVR & PVR and by a moderate + inotropic effect
Indications
Poor CO without initial response to catecholamine or when their use is limited by tachycardia.
RV Dysfunction associated with elevation in PVR
Inotropic and vasoactive drugs
Amrinone : 0.75 mg/kg bolus over 10 mts ------continuous infusion of 10-15 ug/kg/mt
Milrione : 50 ug/kg bolus over 10 mts -----------continuous infusion of 0.375-075 ug/kg/mt

Inotropic and vasoactive drugs
• Mechanisms of a reduced cardiac output and the effects of milrinone and levosimendan in a model of infant cardiopulmonary bypass
Christian F Critical care medicine20-07
Inotropic and vasoactive drugs
Calcium Chloride
Provides ionized Ca2+ which produces a strong but
transient inotropic effect if hypocalcaemia is
present and more sustained ↑SVR even if
normocalcemia is present
Dose : 0.5 -1g slow iv

Inotropic and vasoactive drugs
Tri lodo thyronine (T3)
↑ CO & ↓ SVR in patients with depressed ventricular function.
Randomized studies have not demonstrated a ↓ in inotropicrequirement or an improvement in overall outcome with use of T3 upon weaning from CPB.
It may ↓ incidence of post-op AF through an unknown mechanism.
Current role of ------as salvage when CPB cannot be terminated with maximal inotropic support and IABP.
Dose : 0.05 – 0.08 ug/kg iv

Vasodilators
• NTG
• SNP
Other drugs
Nesritide Recombinant B type natriuretic peptide
↓ sympathetic responses & inhibits neurohumoral response in HF
↓ preload (PAP) & afterload (SVR) Indirectly inc CO without inc HR or myocardial O2 demand lusitropic, dilates native coronaries, arterial conduits, has no
proarrhythmic activity Dilates renal afferent & efferent arterioles, inc GFR –
strong diuretic synergistic with loop diruretics
N-terminal probrain natriuretic peptide level inversely correlates with cardiac index after arterial switch operation in neonates.Breuer T PaediatrAnaesth. 2007 Aug;17(8):782-8.

Other drugs
• Indications
Diastolic dysfunction
Postcardiotomy systolic dysfunction with elevated PAP
• Dose 2 µg/kg over 1 min followed by 0.01 – 0.03 µg/kg/min
• Rapid onset with peak effect within 30 min, half life 18 min
Other drugs
• Natriuretic Peptides in Septic Patients might eventually prove useful for the diagnosis and/or the treatment of septic patients . Piechota M 2009 current med Chem
Other drugs
Dopexamine• Synthetic catecholamine D as well β2 & less β1
activity
• Inotropic effect by inhibiting neuronal uptake of catecholamines and inc HR dose related
• Dec SVR and improves renal & splanchnic perfusion
• Dec PVR and improves RV function
• Dose 1-4 µg/kg/min

Other drugs
Enoximone• Dec systemic, pulmonary and coronary resistance and
has a positive inotropic activity with minimal effect on HR
• Not associated with thrombocytopenia
• Dose 0.5 -1 mg/kg
• Enoximone in low-output states following cardiac valve replacement was at least equally effective in comparison with standard therapy with epinephrine and nitrolycerin. Werner Zwölfer, Clinical Cardiology,2009
• The Role of Enoximone in the Treatment of Cardiogenic Shock=== Unpredictable.

Other drugs
Levosimendan• Calcium sensitising inodilator• Inc CO by improving both stroke volume &HR and dec
preload and afterload• Dose 12 µg/kg over 10 min, 0.1 µg/kg/min
Other drugs
• Corticosteroids…??
• i.v. infusion of methylene blue (0.5 mg/kg)……………..Vasopegic syndrome
Cao Z,Anesth Analg 2009
Intra aortic ballon Pump
• The augmentation of diastolic pressure, to a level higher than systolic pressure, increases coronary perfusion as well as that of other tissues
• Cardiac patients

Indications for Circulatory Assist Devices
Cardiac Surgery
Complete & adequate surgical procedure
Correction of all metabolic problems (ABG, electrolytes)
Inability to wean off bypass despite max pharmalogictherapy & use of IABP
Cardiac Index < 1.8 – 2L/min/m2

Summary and Conclusion
Hypotension is always pathologic and indicative of dysfunction of the cardiovascular system
Do not forget the importance of Toe temperature
Investigations caries some Value
CO may be misleading esp in septic shock
No drug is best
Prevention is better than cure
Mortality can be avoided by timely management in majority of cases
Thank You
Recommended