
Improving patient flow & transfer of care
through risk assessment
Liz Lees RGN, Dip N., BSc (hons.), Dip HSM, MSc, PGR
PhD Student (NIHR CDR Fellowship)
University of Manchester &
Consultant Nurse Heart of England NHS Foundation Trust
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
ROAD: “Risk Objective Assessment for Discharge”

Today’s presentation
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
• Contextual introductions • What’s the problem anyway? • Let’s talk about risk & what we mean • My review of risk assessment tools • Practicalities of risk assessment • Centrality of patient and carer in the risk
process
Introduction • Year 2 PhD: Nurse with NIHR Fellowship
• Topic: Patient discharge from hospital
• Context: acute hospital, emergency care
• 2014: Realist literature review of risk assessment tools & Scoping review of Policy/best practice guidance
• Methodology: Case Study (Yin, 2011)
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
Context: Geographically
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
Context: Clinically
• Acute Medicine Unit • With 84 beds (assessment, ambulatory care,
admission beds, cardiac unit and CDU) • Length of patient stay permitted <48 hours • 2000 patients per month referred • Numerous contemporary roles
Focus is on: a. Patient assessment b. Patient stabilization c. Diagnosis & transfer d. Discharge
Presentation for: Inaugural Transfer of Care Conference, Sydney
2015
Discharge planning:
What is the problem?
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015

Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
“Unsafe transitions, uncoordinated visits and multiple and uncoordinated assessments on the part of professionals”……
Department of Health, 2013, p 11.
“reviewing patients ongoing risk level important to see if new risks had developed is important”
Graham et al, 2013.
Risk assessment tools focus upon the definition and refining of which questions are most pertinent to ask patients yet there is a paucity of literature, which includes carers and their perspectives
Grimmer et al, 2004, Huby et al, 2004.
“Anticipatory assessment of discharge needs will not anticipate obstacles to daily living if undertaken while still hospitalized”
Bobay et al, 2010

What do we mean by risk?
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
• Risk and readmissions • Risk and extended (perceived as prolonged) length of
stay • Risk and predictive use of resources post discharge • Risk and adverse outcomes (excluding readmissions,
e.g., functional decline). • Risk and the early identification of discharge planning
needs • Risk in relation to an ‘early discharge’

What do we mean by risk?
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
Antecedents: Less than satisfactory prior living circumstances (socially isolated) A sudden event e.g., a fall Being new to a caring role/in poor health as a carer Critical Attributes: Additional change in circumstances, e.g. mobility limitations Actual ability to of patient or carer to cope Number of occurrences of the problem Consequences: Limits persons self care ability/lifestyle Needs new services at home Permanency of change (s)

Scholarly Literature Review of ‘discharge’ risk assessment tools
To establish if there is a gap in the evidence base in relation to risk assessment in preparation for
discharge, to assess adult patients who are admitted to & discharged from
emergency care.
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015

Literature review questions 1. What, if any risk tools exist to assess
discharge needs for adult patients being admitted to & transferred from emergency care?
2. What is known about the issues related to the use of discharge risk assessment tools?
3. Are any risk tools embedded in practice?
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015

Search strategy
PATIENT DISCHARGE
“The administrative process of discharging the patient, live or dead from Hospitals or other
health facilities”
The US National Library of Medicine, (2005:2014)
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015

Presentation for: Inaugural Transfer of Care Conference, Sydney 2015

Inclusion & exclusion of tools Inclusion Exclusion
Patients in acute environment requiring discharge from hospital
Not used in acute clinical area
To identify items of risk to assist planning of discharge
Another focus of risk; readmissions, general nursing assessments
Aimed at reducing length of stay Functional decline
Improving quality of assessment of risk for discharge
Needs post discharge (assessment of services)
Risk tool must be in use Tool is in continued development
Steps to development discussed
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015

Question 1:Risk tools • Tools in evolution since 1998 from USA
• PRA – Priority Risk Assessment
• UNAI – Uniform Needs Assessment Instrument
• Gradually been reduced to 4 core questions
• DRS – Discharge Risk Screening tool
• Implemented (limited success) here in Sydney
• RHDS – Readiness for hospital discharge scale
• Sensitivity to respond to identified risk items
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
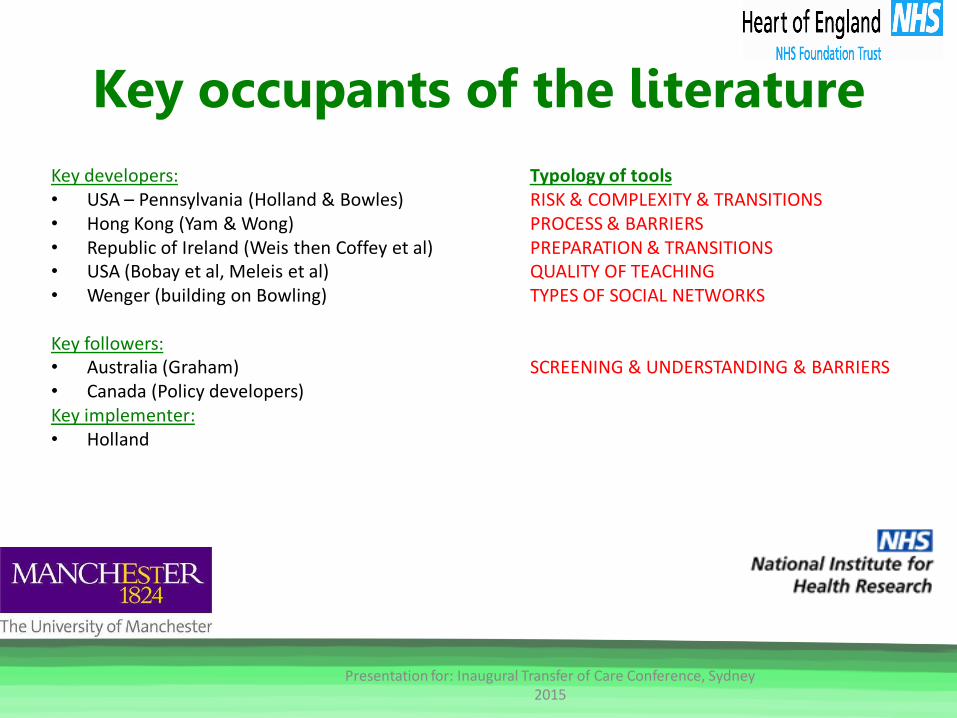
Key occupants of the literature Key developers: Typology of tools • USA – Pennsylvania (Holland & Bowles) RISK & COMPLEXITY & TRANSITIONS • Hong Kong (Yam & Wong) PROCESS & BARRIERS • Republic of Ireland (Weis then Coffey et al) PREPARATION & TRANSITIONS • USA (Bobay et al, Meleis et al) QUALITY OF TEACHING • Wenger (building on Bowling) TYPES OF SOCIAL NETWORKS
Key followers: • Australia (Graham) SCREENING & UNDERSTANDING & BARRIERS • Canada (Policy developers) Key implementer: • Holland
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015

Question 2: What were the issues?
1. The transferability of tools
2. The specificity and sensitivity of items
3. The lack of follow on re-assessment
4. Staff compliance
5. Dearth of implementation science
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015

Question 3: any tools embedded?
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
• Functional adaptation • Functional limited • Professional perception • Patients perception & expectation • Carers perception & expectation
= Weighting of risk Very tricky!

So, if you were trying to do this…… • Consider timing of assessments • Types of professionals who are best to
assess • Types of risk assessment used • Types of services needed (as a
consequence) • Needs that occur immediately after
discharge
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
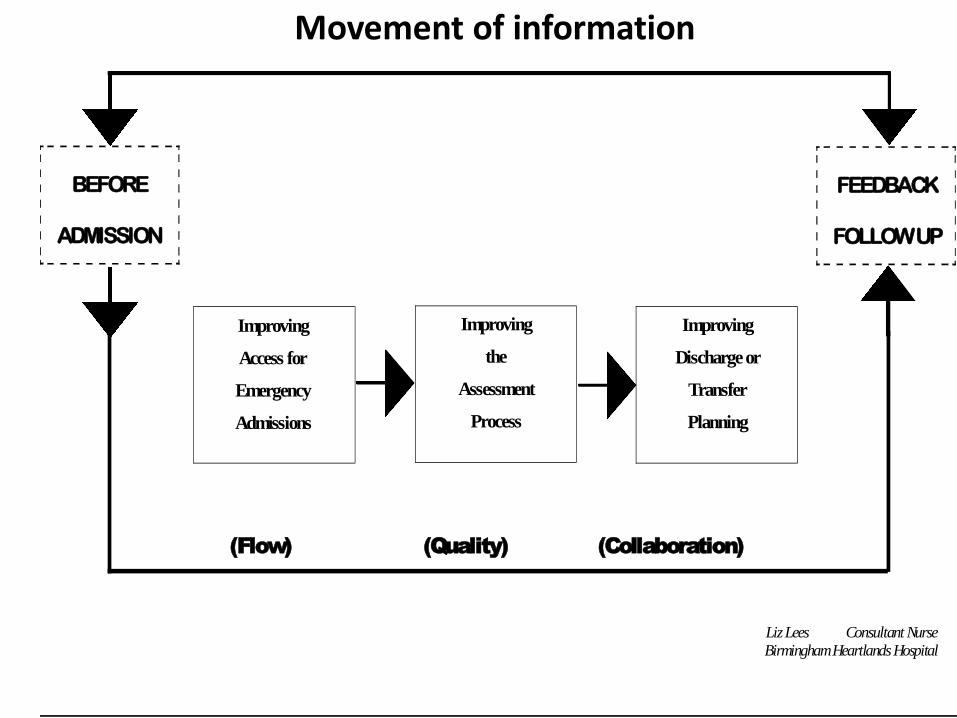
BEFORE
ADMISSION
FEEDBACK
FOLLOW UP
Improving
Access for
Emergency
Admissions
Improving
the
Assessment
Process
Improving
Discharge or
Transfer
Planning
(Flow) (Quality) (Collaboration)
Liz Lees Consultant Nurse
Birmingham Heartlands Hospital
Movement of information

Summary & Reflection
‘risk assessment for discharge & transfer may inform practice, the reality is that practice is substantiated through process contingencies
adopted by clinical staff’….
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
Moving forward: research aim
To explore and understand the feasibility issues & contingencies that surround discharge practice, process
and risk assessment;
prior to the introduction of discharge risk screening, within an exemplar acute medical unit in the UK.
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
Questions
Thank you for listening
Presentation for: Inaugural Transfer of Care Conference, Sydney 2015
Recommended

















