Le Peritoniti
Flavia Caputo

Although incidence rates of peritonitis have decreased substantially
with the introduction of the flush-before-fill double-bag principle, and the emergence of improved connection systems…
Peritonitis is still the achilles'heel of peritoneal dialysisMactier R.Perit Dial Int. 2009 May-Jun;29
Peritoneal dialysis-associated peritonitis is the most common acute complication of PD and has been the main cause of technique failure.
Repetitive or protracted peritonitis episodes can also damage the peritoneal membrane
Selgas R, Paiva A, Bajo MA et al. Adv Perit Dial1998; 14:

• Drop-out per peritonite: 5-10% dei paz/anno• Peritonite come causa di drop-out: 25- 40% • Degenza ospedaliera: 5 giorni/anno paziente
in trattamento• Mortalità per peritonite 2-12%

Peritonitis as a Cause of Peritoneal Dialysis Technique Failure
Study Study period Study patients Initial Cure Tecniques failure due to peritonitis
Kavanagh et al., 2004
1992-2002 All adult patients in Scotland
75% 42.6%
Johnson et al., 2007
2004-2006 All centers in Australia
78% (2006 data only)
29%
Davenport, 2009
2002-2003 All centers in London, UK
>80% in only 2 of 12 units
41.7%
Mactier R.Perit Dial Int. 2009 May-Jun;29

Factors affecting the rate of tecnique failure:
Kavanagh D, Prescott GJ, Mactier RA, NDT 2004;19

ISPD Standards and Guidelines Committee Minutes from the June 2008 Meeting in Istanbul
In attendance: Beth Piraino, Frank Schaefer, Judith Bernardini, Edwina Brown, Flavia Caputo,
Ana Figueiredo, Valerie Price
Update on Peritoneal Dialysis- Related Infections, 2005 published in 2005 in PDI
The committee felt that it was time to renew this guideline. It will be split into two parts. One will deal with Management of PD Related Infections. This guideline will be led by Dr Philip Li
who has been invited to join the committee to ensure good communication. He will put together the working group. Projected complete date: 2010.
Addendum: The part of the previous guideline on Prevention of PD related infections will be separated and developed as a position paper as there is not enough rigorous data for
guidelines. This will be led by Dr Beth Piraino. Dr Philip Li and Dr Beth Piraino will sit on each other’s work groups. Projected time table: completion by mid 2009. The committee will be
asked if they agree with this approach.

First published in 1983 and revised in 1989, 1993, 1996 and 1995
2010 UPDATEEvery program should regularly monitor
infection rates, at a minimum, on a yearly basis Opinion

The center’s peritonitis rate should be no more than 1 episode every 18 months (0,67/year)
Reported <0,29-0,23/year GOAL to achieve!Cheng YL, AJKD 2002, 40. 373Choi KH, Perit Dial Int 2004: 424-432
ISPD 2010

Methods1.As rates• Interval in months between episodes• Episodes for year2. As percentage of patients per period of time
who are peritonitis free3. As median peritonitis rate for the program
ISPD 2010

Comparison of Peritonitis Rates in Peritoneal Dialysis (PD) Patients Using the Double-Bag Disconnect System
Study (Ref. Study period
Study location
Patients (n) PD system Months between episodes of peritonitis
Monteon et al., 1998 (8)
- Multicenter; Mexico
147 CAPD 24,8
Li et al., 1999 (9) - Multicenter; Hong Kong
120 CAPD 33,5
Huang et al., 2001 (10)
1993–2001 Single center; Taipei, Taiwan
117 CAPD 45,4
Katz et al., 2001 (11)
1998-1999 Single center; Soweto, South Africa
84 CAPiva a 45 D
27,9
Kavanagh et al., 2004 (5)
1999–2002 All centers in Scotland
1205 APD/CAPD 19,2
Johnson et al., 2007 (6
2006 All centers in Australia
2021 APD/CAPD 21,0
Davenport, 2009 (7)
2002–2003 All centers in London, UK
863 at the end of 20021080 at the end of 2003
APD/CAPD 15,9

Esperienza del nostro centro
Dati 2008
o 25 episodi in 66 pazienti
o 1 episodio ogni 25mesi/pz
o 0.48 ep/anno/paz.
Dati 2009
20 episodi in 58 pazienti1 episodio ogni 29
mesi/pz0.41 ep/anno/paz.

PERITONITISPeritoneal dialysis patients presenting with cloud
effluent OR abdominal pain
Diagnosis is confirmed with cell count and culture1. ≥100 WBC per mcL with more than 50% PMN2. Positive cultureEVIDENCE
ISPD 2010

Differential Diagnosis of Cloud Effluent• Culture positive infectious peritonitis• Infectious peritonitis with sterile cultures• Chemical peritonitis• Eosinophilia of the effluent• Hemoperitoneum• Malignacy (rare)• Chylous effluent (rare)
ISPD 2010

Culture-negative peritonitis should not be greater than 20% episodes
Standard culture technique is the use of blood- culture bottles, but culturing the sediment after centrifuting 50 mL of effluent is ideal for low culture-negative results
EVIDENCE ISPD Guidelines 2010
In the ideal situation less than 10% rate of culture negative peritonitis
ISPD 2010

The correct microbiological culturing of peritoneal effluent is of the most importance to establish the microrganism responsible.
Centrifugation 50 mLperitoneal effluent at 3000g for 15 minutes……Rapidblood-culturetechniques (BACTEC)
Other novel diagnostic techniques:•Leukocyte esterase reagent strip •PCR withRNA/DNA assays•MMP 9
ISPD 2010

IntraluminaleStaf.epidermidis e altri SCN Staf.aureo (30/40%) Strept.Viridans
Periluminale
Staf. Epidermidis e altri SCN
Staf.Aureo (20/30%) Pseudomonas
Difterici
Funghi
TransmuraleColibacilli (25/30%)
Enterobacteriacee Anaerobi
Ematogena Streptococchi (5/10%) M. Tubercolosis
AscendenteLactobacilli (2/5%) Funghi
Vie di contaminazione e microrganismi

Vie di contaminazione
ESOGENA
ENDOGENA
• Endoluminale30-40%• Periluminale20-30%
• Transmurale25-30%• Ascendente2-5%• Ematogena/Linfatica5-10%
Adeguato training

La via endoluminale via endoluminale rappresenta il 40% delle vie di contaminazioneCause: Manovre non corrette nel cambio sacca Tramite rotture della sacca o del set Disconnessioni accidentali Soluzioni non sterili
Per tale motivo il TRAININGriveste un ruolo fondamentale nellaprevenzione delle peritoniti L’utilizzo di un incrementato metodo di training è positivamente associato con il
migliorato esito del paziente (evidence)
New directions in dialysis patient training Nephrol. Nurs. 2004

Il metodo di training influenza il rischio di infezioni in dialisi peritoneale (Evidence).EXIT SITE CARE ISPD GUIDELINES/RECOMMENDATIONS 2005
Le PD nurses sono fondamentali per un programma di dialisi peritoneale con un basso indice di infezioni:
•- Lavaggio mani
•- Exit site care
•- Uso della mascherina
•- Diagnosi precoce dell’ESI e del TI

Vie di contaminazione
ESOGENA
ENDOGENA
• Endoluminale30-40%• Periluminale20-30%
• Transmurale25-30%• Ascendente2-5%• Ematogena/Linfatica5-10%
Adeguato training
ESI / TICarriage Staph. Aureus

Peritonitis associated with exit-site infections
B. Piraino- AJKD, 1996

Episodes per year at risk
Bernardini J, Piraino B, JASN 2005 Feb; 16: 539-45

Gentamicin cream applied daily to the exit-sitecompared to mupirocin significantly reducedEXITE SITE INFECTION (57%)PERITONITIS (35%)
Bernardini J, Piraino B JASN 2005 Feb; 16: 539-45

Vie di contaminazione
ESOGENA
ENDOGENA
• Endoluminale30-40%• Periluminale20-30%
• Transmurale25-30%• Ascendente2-5%• Ematogena/Linfatica5-10%
Adeguato training
Exit-siteinfectionCarriageStaph. Aureus
Profilassi antibioticaEvitare la stipsi

There is an association between both severe constipation and enteritis and peritonitis due to enteric organisms
EVIDENCE ISPD Guidelines 2005
Possibly, peritonitis results from trans migration of micro-organisms across the bowel wall.
• Hipomotility disorders• Drugs contributing (oral iron, oral calcium, some analgesics)• Hypokaliemia
Training: AVOIDANCE OF CONSTIPATION!
ISPD 2005

Vie di contaminazione
ESOGENA
ENDOGENA
• Endoluminale30-40%• Periluminale20-30%
• Transmurale25-30%• Ascendente2-5%• Ematogena/Linfatica5-10%
Adeguato training
Exit-siteinfectionCarriageStaph. Aureus
Profilassi antibioticaEvitare la stipsi
Fistole vaginaliAscessiretroperitoneali

Vie di contaminazione
ESOGENA
ENDOGENA
• Endoluminale30-40%• Periluminale20-30%
• Transmurale25-30%• Ascendente2-5%• Ematogena/Linfatica5-10%
Adeguato training
Exit-siteinfectionCarriageStaph. Aureus
Profilassi antibioticaEvitare la stipsi
Fistole vaginaliAscessiretroperitoneali
Profilassi antibiotica in corso di procedure invasive

Invasive procedure may infrequently cause peritonitis in PD patients
EVIDENCE ISPD Guidelines 2005
Antibiotic prophylaxis:• A single oral dose of amoxicillin (2g) 2 hours before extensive dental
procedure Opinion• Patients undergoing colonscopy with polypectomy: Ampicillin 1g+ a single
dose of an aminoglycoside ± metroinidazole, given i.v. just prior the procedure Opinion
N.B. The abdomen must be empty of fluid prior to all procedures involved the abdomen or pelvis (colonsopy, renal transplantation, endometrialbiopsy) Opinion
ISPD 2005

A Bundle of Care of Clinical Practice to Reduce Risk of peritonitis
Mactier R.Perit Dial Int. 2009 May-Jun;29

Therapy should be initiated as soon is possible, after appropriate microbiological specimen have been obtained
PATIENT EDUCATIONAL
ISPD 2010

PATIENT EDUCATIONAL
• Immediately report cloudy effluent, abdominal pain and/or fever to PD unit
• Save drained cloudy dialysate and bring to clinic• Treatment will be adding intraperitoneal antibiotics
for up to 3 weeks• Report worsening symptoms or persistent cloudiness
to PD unit• Schedule retraining for technique issues
ISPD 2010

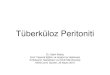
Start intraperitoneal antibiotics as soon as possibleAllow to dwell for at least 6 hoursEnsure gram-positive and gram negative coverage*Base selection on historical patient and center sensitivity patterns as available
Gram-positive coverageEither Vancomycin** or first generation cephalosporin
Gram-negative coverageEither third-generation cephalosporin*** or aminoglycoside0-
6 ho
urs
Determine and prescribe ongoing antibiotic treatmentEnsure follow-up arrangements are clear or patient admittedAwait sensitivity results
6-8
hour
s
ISPD 2010
INIT
IAL
MAN
AGEM
ENT
OF
PERI
TON
ITIS

• La dose I.P. è sempre preferibile. IP administration has the advantage of a high concentration of the antibiotic at the site of infection. The major drawback is that injection of the antibiotic into the bag induces a potential extra risk of contamination. In this regard, once-daily IP administration has great advantages. Intravenous administration should be avoided as this can destroy vascular access possibilities that are precious for the future
Van Biesen W, Vanholder R, Lameire N. Perit Dial Int 2000; 20
Intraperitoneal Drug Therapy: An Advantage. Chaudhary Curr Clin Pharmacol. 2010

THERAPY1. EMPIRIC THERAPY
(therapy is initiated prior to knowledge of causative organism)
The Committee reccomends center-specific selection of empiric therapy, dependent on the local history of sensitivies of organismies causing peritonitis
The protocol must cover all serious pathogens that are likely to be present
Opinion
ISPD 2010

EMPIRIC THERAPY
and
N.B. Short-term use of aminoglycoside therapy appears to be safe for the risk of ototoxicity (once day dose)
ISPD 2010
CefazolinOr
Vancomicin
CeftazidimeOr
Gentamicin

Monotherapy:• Imipenem/cilastatin 50mg = cefazolin+ceftazidime
Leung CB, Szeto CC, Chow KM, Perit Dial Int, 24: 440, 2004
• Cefepime 2 g = vancomycin+netilmicin Wong KM, Chan CY, Cheung CY, Leung SH, Am J Kidney Dis 38: 127, 2001
• Quinolones (oral levofloxacin 250 mg/day or perfloxacin 400 mg/day) = aminoglycosides for gram-negative
Yeung SM, Walker SE, Tailor SA, Perit Dial Int 18: 371, 2004
ISPD 2010

Other gram-positive organisms including coagulase negative staphylococcus on culture
Continue gram-positive coverage based on sensitivitiesStop gram-negative coverage
Assess clinical improvement, repeat dialysis effluent cell count and culture at days 3-5- Symptoms resolved
- Bags clear
Clinical improvement- Continue antibiotics;
- duration of therapy: 14 days
No clinical improvement- Re-culture & evaluate*
Re-evaluate for exit-site or occult tunnel infection, intraabdominal
abscess, catheter colonization etc
Peritonitis with exit-site or tunnel infection consider catheter
removal**Duration of therapy: 21 days
No clinical improvement by 5 days on appropriate antibiotics, remove
catheter
ISPD 2010
ISPD 2010

Staphylococcus aureus on culture
Continue gram-positive coverage based on sensitivities*Stop gram-negative coverage, assess exit site again
If methicillin resistant, adjust coverage to vancomycin or teicoplanin**Add rifampin 600 mg/day orally (in single or split dose) for 5 to 7 days (450 mg/day if BW < 50
kg)
Assess clinical improvement , repeat dialysis effluent cell count and culture at days 3-5- Symptoms resolved
- Bags clear
Clinical improvement- Continue antibiotics
- Duration of therapy 21 days
No clinical improvement- Re-culture & evaluate
Re-evaluate for exit-site or occult tunnel infection, intraabdominal
abscess, catheter colonization etc
Peritonitis with exit-site or tunnel infection may prove to be
refractory**** and the catheter must be removed.
Allow a minimum rest period of 3 weeks before re-initiating PD*****
No clinical improvement by 5 days on appropriate antibiotics, remove
catheter
ISPD 2010

Enterococcus/Streptococcus on culture
Discontinue starting antibiotics*Start continuous ampicillin 125 mg/L each bag;
consider adding aminoglycoside for enterococcus**
If ampicillin resistant, start vancomycin;If vancomycin resistant enterococcus, consider quinupristin/dalfopristin, daptomycin, or
linezolid
Assess clinical improvement, repeat dialysis effluent cell count and culture at days 3-5- Symptoms resolved
- Bags clear
Clinical improvement- Continue antibiotics; duration of therapy:
14 days (streptococcus)21 days (enterococcus)
No clinical improvement- Re-culture & evaluate
Re-evaluate for exit-site or occult tunnel infection, intraabdominal
abscess, catheter colonization etc
Peritonitis with exit-site or tunnel infection consider catheter
removal***Duration of therapy: 21 days
No clinical improvement by 5 days on appropriate antibiotics, remove
catheter
ISPD 2010
ISPD 2010

Culture negative on day 1 & 2
Infection resolvingPatient improvement clinically
Infection not resolvingSpecial culture technique for unusual causes (e.g. viral,
mycoplasma, mycobacteria, legionella). Consider fungi
Continue initial therapy for 14 days
Now culture positive Still culture negative
Continue initial therapy
Day 3: Culture still negativeClinical assessment
Repeat PD Fluid white cell count and differential
Adjust therapy according to sensitivity patterns
Duration of therapy based on organism identified
Clinical improvement
Continue antibiotic
Duration of therapy: 14 days
No clinical improvement after 5 days
Remove catheter*
Continue antibiotics for at
least 14 days
ISPD 2010

Pseudomonas species on culture
Without catheter infection(exit-site/tunnel)
With catheter infection(exit-site/tunnel) current or
prior to peritonitisGive 2 different antibiotics acting in
different ways that organism is sensitive to eg oral quinolone,
ceftazidime, cefapime, tobramycin, piperacillin
Assess clinical improvement, repeat dialysis effluent cell count
and culture at days 3-5: - Symptoms resolved
- Bags clear
Catheter removal*
Continue oral and/or systemic antibiotics for at least two weeks
No clinical improvement
- Re-culture & evaluate- Consider changing
antibiotics
No clinical improvementby 5 days on
appropriate antibiotics, remove catheter
Clinical improvement
- Continue antibiotics; - duration of therapy: 21
days
ISPD 2010

Single gram-negative organism on cultureon culture*
OtherE. coli proteus, klebsiellaetc
Stenotrophomonas
Adjust antibiotics to sensitivity pattern Cephalosporin (ceftazidime
or cefepime) may be indicated
Treat with 2 drugs with differing mechanisms based on sensitivity
pattern (trimethoprim / sulphamethoxazole is preferred)
Assess clinical improvement , repeat dialysis effluent cell count
and culture at days 3-5: - Symptoms resolved
- Bags clear
Assess clinical improvement at days 3-5: - Symptoms resolved
- Bags clear
Clinical improvement- Continue antibiotics;
- Minimum 21 day treatment
Clinical improvement- Continue antibiotics:
21- 28 days treatment
No clinical improvement by 5
days on appropriate antibiotics - remove
catheter
ISPD 2010

Polymicrobial peritonitis: days 1-3
Multiple gram-negative organisms or mixed gram negative/gram
positive- consider GI problem
Multiple gram-positive organisms- Touch contamination
- Consider catheter infection
Change therapy to metronidazole in conjunction with ampicillin,
ceftazidime or aminoglycoside
Continue therapy based on sensitivities
Obtain urgent surgical assessment
Duration of therapy
minimum 21 days based on
clinical response
In case of laparotomy indicating intraabdominal pathology/abscess,
remove catheter*
Continue antibiotics – 14 days
With exit site or tunnel infection, remove
catheter*
Without exit site or tunnel
infection – continue
antibiotics
ISPD 2010

The Commette feels that the minimum of therapy for peritonitis is 2 weeks, athough for more severe infections, 3 weeks is reccomendedOpinion
After initiation of antibiotic treatment clinical improvement shoud be present in the first 72 hours

Fungal peritonitis
Fungal peritonitis is a serious complication leading to death in 25% or more episodes ,should be strongly suspected after recent antibiotic treatment for bacterial peritonitis.
Catheter removal is indicated immediately after fungi are identified by microscopy or cultureEVIDENCE
ISPD 2010

PERITONITIS DUE TO MYCOBACTERIA Mycobacteria are an infrequent cause of peritonitis but can be difficult to diagnose. When under clinical consideration, special attention must be paid to culture techniques. Treatment requires multiple drugs EVIDENCEThey can be caused by Mycobacterium tuberculosis or non-tuberculosis mycobacteria, such as M. fortuitum, M. avium, M. abscessus and M. chelonei
ISPD 2010

Terminology of peritonitisTerminology for peritonitis
• Recurrent: An episode that occurs within 4 weeks of completation of therapy for a prior episode but with a different organism
• Relapsing: An episode that occurs within 4 weeks of completation of therapy for a prior episode with the same organism or one sterile episode
• Repeat: An episode that occurs after 4 weeks of completation of therapy for a prior episode with the same organism
• Refractory: Failure of the effluent to clear after 5 days of appropriate antibiotics
• Catheter-related peritonitis: Peritonitis in conjunction with exit-site or tunnel infection with the same organism or one site sterile
When calculating peritonitis rates, Relapsing episodes should not be counted as another peritonitis; while recurrent and repeat should be counted
ISPD 2010

\Indications for catheter removal:• Relapsing peritonitis• Refractory peritonitis• Fungal peritonitis• Refractory catheter infectionsThe focus shoul be on preservation of the
peritoneum rather than saving peritoneal catheter
Opinion
ISPD 2010

Catheter reinsertion
A minimum period of 2-3 weeks between catheter removal and reinsertion of a new catheter is raccomanded, although some would reccomend later reinsertion in case of fungin peritonitis
ISPD 2010

REFRACTORY PERITONITISRefractory peritonitis, defined as failure to respond to appropriate antibiotics within 5 days, should be managed by removal of the catheter to protect the peritoneal membrane for future use
ISPD 2010

OUTCOMES EVALUATION• Collect data to include• Date of culture, organism identified, drug therapy used• Date infection resolved• Recurrent organisms, date of drug therapy• Method of interim renal replacement therapy• Date of catheter removal• Date of new catheter reinsertion• Documentation of contributing factors
– Break in technique, patient factors, exit-site infections, tunnel infections
• Date of re-education/training• Enter data into catheter management database
ISPD 2010
Recommended