325
JOURNAL OF ENDOUROLOGYVolume 16, Number 6, August 2002© Mary Ann Liebert, Inc.
TECHNIQUES IN ENDOUROLOGY
Laparoscopic Antegrade Continence Enema (Malone)Procedure: Description and Illustration of Technique*
EDWARD KARPMAN, M.D., SAKTI DAS, M.D., and ERIC A. KURZROCK, M.D., FAAP
ABSTRACT
The antegrade continence enema (ACE Malone) procedure has improved the lives of many patients who strug-gle with intractable forms of constipation. We describe a laparoscopic approach to this technique and reviewthe literature.
INTRODUCTION
THE MANAGEMENT OF CHRONIC CONSTIPATIONand encopresis in patients with neurogenic bowel and other
colonic motility disorders has traditionally relied on laxatives,enemas, digital stimulation, and manual disimpaction. Evenwith the strictest of regimens and the most diligent patients, en-copresis, constipation, or both often persist.
In 1990, Malone and associates first described the antegradecontinence enema (ACE) procedure using the appendix.1 Sev-eral modifications have been described since. This operationhas improved the lives of many patients who struggle with in-tractable forms of constipation. Complete resolution of fecalsoiling has been reported in as many as 95% of patients.2 Pa-tient satisfaction with the ACE procedure is very high, and therisk of complications is low.3
More recently, laparoscopic ACE (LACE) has been reported.The LACE may offer the advantages of a shorter hospital stay,faster recovery, less postoperative pain, and better cosmesis.Minimizing postoperative ileus is especially important in thesepatients with bowel motility problems. Success with this ap-proach relies on proper patient selection and appropriate plan-ning and performance of the laparoscopic surgery.
TECHNIQUE
Patient Selection
The ideal candidate for LACE is one who suffers from in-tractable constipation or encopresis and has failed multiple
bowel evacuation regimens. For those requiring assistance, areliable caretaker is paramount. Preferably, the patient’s fecalsoiling should be the result of neurogenic bowel or poor distalrectal or anal competence. Prior abdominal surgery may be arelative contraindication.
Patient Preparation
The patient is prepared with mild laxatives 3 days prior tosurgery and a full mechanical bowel preparation the day beforesurgery. Broad-spectrum antibiotics are given perioperatively.The patient is induced with a general anesthetic, and an oro-gastric tube and Foley catheter are placed. The table is tilted tothe patient’s left and with the head down.
Port Placement
An inverted-V incision is made in the umbilicus to raise aflap for subsequent stomal construction. A 5-mm trocar is in-serted directly beneath the skin flap and secured in place withtwo fascial sutures. After the pneumoperitoneum has been es-tablished and the camera inserted, two additional 3.5- or 5-mmtrocars are placed lateral to the rectus muscle at the level of theumbilicus.
Localization and Mobilization of Appendix
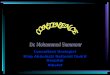
The appendix is mobilized out of the right lower quadrantusing grasping forceps. Adhesions may obscure the appendix,especially in children with a ventriculoperitoneal shunt. The tipof the appendix is grasped and stretched to demonstrate itslength and caliber (Fig. 1A). The mesentery and vasculature are
Department of Urology, Children’s Hospital, University of California Davis School of Medicine, Sacramento, California.* A video illustrating certain steps in this technique is included with the issue and is available online at www.liebertpub.com/end/video.

inspected. Often, separate arteries may be evident supplying theproximal and distal appendix (Fig. 1B). To straighten a longappendix for catheterization, the distal artery may be sacrificed(Fig. 1C). The pneumoperitoneum will distort the apparentproximity of the cecum to the abdominal wall. Release of thepneumoperitoneum will reveal the appendiceal redundancy(Fig. 2).
Usually, only 1 to 2 cm of intra-abdominal appendix is re-quired for prevention of stomal leakage. Appendiceal coapta-tion and the cecoappendiceal sphincter will provide adequateresistance.3 We make every attempt to position the stoma in theumbilicus. If necessary, the right side of the colon can be mo-bilized along the line of Toldt. If the appendix still does notreach the umbilicus, the stoma can be created in the right up-per or lower quadrant.
Creation of Anastomosis
After adequate mobilization of the appendix, the camera isswitched to the left port. The appendix is clamped with grasp-ing forceps and brought out through the umbilical wound afterthe port is removed. The pneumoperitoneum is released, andthe appendix is divided at the level of the skin. Prior to com-plete division of the appendix, the appendicular artery is lig-
ated at skin level with absorbable suture. The appendix is in-tubated with an 8F feeding tube and spatulated on the antime-senteric border. The umbilical V-flap is sewn into the spatula-tion, and the stoma is matured with absorbable suture.
Postoperative Care
An appendiceal catheter is left in situ for approximately threeweeks (Fig. 3). The catheter is removed in clinic, and the pa-tient is instructed on catheterization and enema technique. Westart at a volume of 250 mL and instruct the patients to increasethe volume gradually until they are able to evacuate all of theircolonic contents in one sitting. This usually requires a volumeof 500 to 1000 ml. Placement of the enema and complete evac-uation of the colon can take as long as an hour. In general, en-emas are placed daily, but some patients are satisfied withevery-other-day enemas.
ROLE IN UROLOGIC PRACTICE
The ACE procedure has undergone many revisions since itsinception in 1990. The original description by Malone and as-sociates utilized appendiceal reversal, whereas more recent se-
KARPMAN ET AL.326
A B
C
FIG. 1. Mobilization and preparation of appendix. (A) Tip ofappendix being grasped. (B) Uncoiling of appendix and iden-tification of arteries (d 5 distal artery; p 5 proximal artery;tip 5 tip of appendix). (C) Division of distal artery (d).

ries use in situ appendix with or without cecal plication. Theknowledge that use of the appendix in situ without plication re-sults in low rates of stomal leakage opened the door for the lap-aroscopic approach. Cromie and colleagues4 published the firstreport of LACE in dogs. The results of clinical series arepromising,5–8 but more controlled studies comparing LACEwith open surgery need to be done.
The indications for surgery and proper patient selection arecritical. Previously reported series have shown better successin patients with spina bifida and those with distal rectal andanal incompetence than in patients with chronic constipationfor other reasons.9 Children under the age of 5 years may notbe able to remain on the toilet for the time required to evacu-ate all of the colonic contents. Finally, the dedication of the pa-tient or caretaker must be scrutinized. People who are poorlycompliant with a regular bowel regimen will not be successfulin remaining clean and dry after LACE.10
Many modifications to the ACE Malone procedure have been
described. These include cecal plication, appendix reversal, for-mation of a cecal tube using the Boari principle, formation ofan intestinal conduit using the Monti principle, and split ap-pendix surgery.11–14 We perform an in situ anastomosis of theappendix to the abdominal wall without any plication. Previ-ously, it had been suspected that stomal leakage would be morefrequent without plication. Studies have shown this not to betrue, with a reported leakage rate of only 6.7% with LACE8
compared with 6.6% with open ACE.15 We believe appendicealcoaptation and the preservation of the ceco-appendiceal sphinc-ter create adequate outlet resistance.
Some authors recommend forming the stoma on the rightlower abdomen.1,7 This approach requires less cecal mobiliza-tion and manipulation, theoretically reducing the risk of com-plications. We and others recommend using the umbilicus be-cause of the cosmetically appealing results.11,16 The umbilicallocation does not increase the risk of stomal stenosis for ACEor urinary diversion.16 We attempt to minimize stenosis by us-ing an inverted-V incision to inlay into the spatulated appen-dix. Other options include a VQZ incision or Y appendi-coplasty.10,17
The rate of stomal stenosis has been reported to be about30% with either laparoscopic or open ACE.8 The majority ofpatients are managed initially with dilatation. How many ofthese patients ultimately require surgical revision is unknown.
We begin using the ACE 3 weeks after surgery and recom-mend tap water because of its effectiveness and simplicity. Inthe Southhampton study, the most common washout regimenused was a phosphate enema,9,10 but this product has been re-ported as the cause of pain in 58% of the patients in the initial3 months of using the ACE. To overcome this problem, the au-thors reported using a liquorice root recipe. Other options in-clude Fletcher’s arachis-oil retention enema, saline, and warmtap water enemas.10,18 Fatal hypernatremia has been reportedas a result of using home-made saline solutions for colonicwashouts.19 Our clinical nurse specialist is closely involved inmonitoring the patient’s progress. Close postoperative follow-up is paramount to long-term success.
LAPAROSCOPIC ACE MALONE 327
FIG. 3. Well-concealed umbilical stoma intubated with cath-eter.
A B
FIG. 2. Effect of pneumoperitoneum on relation of cecum to abdominal wall. (A) Extension of appendix (arrow) with pneu-moperitoneum (t 5 right trocar). (B) Extension of appendix after pneumoperitoneum is released.

CONCLUSIONS
The management of fecal soiling and constipation has beenrevolutionized by the description of the ACE procedure by Ma-lone and associates. The LACE procedure provides an appeal-ing option. The rates of stomal leakage and stenosis are com-parable after open and laparoscopic ACE. We believe that withtime, the advantages of laparoscopy, such as shortened hospi-tal stay, superior cosmesis, and greater patient satisfaction, willbecome evident with LACE, as with so many other operations.
REFERENCES
1. Malone PS, Ransley PG, Kiely EM. Preliminary report: The ante-grade continence enema. Lancet 1990;336:1217–1218.
2. Levitt MA, Soffer SZ, Pena A. Continent appendicostomy in thebowel management of fecally incontinent children. J Pediatr Surg1997;32:1630–1633.
3. English SF, Pisters LL, McGuire EJ. The use of the appendix as acontinent catheterizable stoma. J Urol 1998;159:747–749.
4. Cromie WJ, Goldfischer ER, Kim JH. Laparoscopic creation of acontinent cecal tube for antegrade colonic irrigation. Urology 1996;47:905–907.
5. Van Savage JG, Yohannes P. Laparoscopic antegrade continenceenema in situ appendix procedure for refractory constipation andoverflow fecal incontinence in children with spina bifida. J Urol2000;164:1084–1087.
6. Webb HW, Barraza MA, Crump JM. Laparoscopic appendicos-tomy for management of fecal incontinence. J Pediatr Surg 1997;32:457–458.
7. Robertson RW, Lynch AC, Beasley SW, Morreau PN. Early ex-perience with the laparoscopic ACE procedure. Aust NZ J Surg1999;69:308–310.
8. Lynch AC, Beasley SW, Robertson RW, Morreau PN. Compari-son of results of laparoscopic and open antegrade continence en-ema procedures. Pediatr Surg Int 1999;15:343–346.
9. Curry JI, Osborne A, Malone PS. The MACE procedure: Experi-ence in the United Kingdom. J Pediatr Surg 1999;34:338–340.
10. Malone PS, Curry JI, Osborne A. The antegrade continence enemaprocedure: Why, when and how? World J Urol 1998;16:274–278.
11. Wedderburn A, Lee RS, Denny A, Steinbrecher HA, Koyle MA,Malone PS. Synchronous bladder reconstruction and antegradecontinence enema. J Urol 2001;165:2392–2393.
12. Sugarman ID, Malone PS, Terry TR, Koyle MA. Transverselytubularized ileal segments for the Mitrofanoff or Malone antegradecolonic enema procedures: The Monti principle. Br J Urol 1998;81:253–256.
13. Goepel M, Sperling H, Stohrer M, Otto T, Rubben H. Managementof neurogenic fecal incontinence in myelodysplastic children by amodified continent appendiceal stoma and antegrade colonic en-ema. Urology 1997;49:758–761.
14. Hensle TW, Reiley EA, Chang DT. The Malone antegrade conti-nence enema procedure in the management of patients with spinabifida. J Am Coll Surg 1998;186:669–674.
15. Graf JL, Strear C, Bratton B, Housley HT, Jennings RW, HarrisonMR, Albanese CT. The antegrade continence enema procedure: Areview of the literature. J Pediatr Surg 1998;33:1294–1296.
16. Glassman DT, Docimo SG. Concealed umbilical stoma: Long-termevaluation of stomal stenosis. J Urol 2001;166:1028–1030.
17. Tam PK. Y-appendicoplasty: A technique to minimize stomal com-plications in antegrade continence enema. J Pediatr Surg 1999;34:1733–1735.
18. Yerkes EB, Rink RC, King S, Cain MP, Kaefer M, Casale AJ. Tapwater and the Malone antegrade continence enema: A safe combi-nation? J Urol 2001;166:1476–1478.
19. Schreiber CK, Stone AR. Fatal hypernatremia associated with theantegrade continence enema procedure. J Urol 1999;162:1433; dis-cussion 1433–1434.
Address reprint requests to:Eric A. Kurzrock, M.D., FAAP
4860 Y St., Suite 3500Sacramento, CA 95817
E-mail: [email protected]
EDITORIAL COMMENT
The authors describe their technique of performing the Mal-one ACE operation laparoscopically. The figures show beauti-fully the simplicity of this procedure.
Many readers may wonder why urologists, and not generalsurgeons, should perform the ACE. Neurogenic bowel patientsroutinely consult urologists for their bladder problems. In mostcases, their bowel care is administered by rehabilitation medi-cine physicians. The ACE procedure may offer a tremendousimprovement in these patients’ quality of life and may be com-bined with a urinary procedure if needed. Urologists who arecomfortable with urinary diversion procedures can easily per-form the ACE. And, as the authors show, the laparoscopic ACEmay be readily performed.
I would like to emphasize several points the authors make.First, patient selection is critical (article reference 11).1,2 Stomalstenosis occurs in about a third of patients. We have found thatreoperation rates may be as high as 80% (unpublished data),but patients remain enthusiastic about the improved quality oflife from this procedure. Thus, patient motivation must be as-sessed critically.
Second, the authors perform an in situ anastomosis, bring-ing a V-shaped skin flap into the stomal anastomosis. We per-form the open procedure similarly. Complication rates arehigher when appendiceal reversal is performed. There is no ev-idence that tunneling the appendix in a submucosal trough inthe cecal tenia provides better stomal continence than the sim-pler in situ anastomosis without plication.
Third, the authors wait 3 weeks before using the ACE. Weroutinely start using the ACE at 1 week, when the catheter isremoved and patients begin daily catheterization and enema ad-ministration. As the authors describe, we use tap water and in-crease volumes sequentially.
The ACE procedure can truly make an enormous and positivedifference to these patients’ lives. I would encourage urologiststo consider offering this option to appropriately selected patients.
Joel M.H. Teichman, M.D., FRCSCThe University of Texas Health Science Center
San Antonio, Texas
REFERENCES
1. Gerharz EW, Vik V, Webb G, Leaver R, Shah PJ, Woodhouse CRJ:The value of the MACE (Malone antegrade colonic enema) proce-dure in adult patients. J Am Coll Surg 1997;185:544–547.
2. Teichman JMH, Harris JM, Currie DM, Barber DB: Malone ante-grade continence enema for adults with neurogenic bowel disease.J Urol 1998;160:1278–1281.
KARPMAN ET AL.328
Recommended