3D microtomography characterization of dental implantology bone substitutes used in-vivo.
Rossella Bedini a, Deborah Meleo b, Raffaella Peccic
Technology and Health Department, Istituto Superiore di Sanità (ISS), Rome, Italy
[email protected], [email protected], [email protected],
*corresponding author: Rossella Bedini, Technology and Health Department, Istituto Superiore di Sanità (ISS), v.le Regina Elena 299, 00161, Rome, Italy. Phone number: +39 06 49902725, e-mail
address: [email protected]
Keywords: biomaterials, bone substitutes, 3D microtomography characterization, dental implantology
Abstract
After a short introduction to bone substitute biomaterials and X-ray microtomography, this article
describes a research work carried out for in-vitro characterization of bone substitute biomaterials as
well as for in-vivo investigation of human bone grafted with biomaterials.
Three different bone substitute biomaterials have been analyzed in-vitro by means of 3D
microtomographic technique, while human bone samples grafted with bone substitute biomaterials
are investigated by 3D microtomography and histological techniques.
3D images of bone substitutes and human bone samples with biomaterials have been obtained,
together with morphometric parameters, by microtomography .
2D histological images have also been obtained by traditional technique only for human bone
samples with biomaterials. Compared to traditional histological analysis, 3D microtomography
shows better results for investigating bone tissue and bone substitute biomaterial, and in a short
time.
Nevertheless, histological analysis remains the best technique for the observation of soft tissue and
blood vessels.
Introduction
The increasing knowledge of implantology and the mechanisms of bone neo-formation require a
continuous update in order to reach those objectives that until a few years ago were considered
impossible to achieve.
The restoration of skeletal segments, lost for various reasons (traumas, infectious, neo-plastic or
congenital diseases) has led to the development of several techniques for the bone reconstruction of
maxilla and mandible for dental implant-prosthetics.
The choice among these techniques could be motivated by many factors such as the location and
extension of the defect, the anatomy of the site to be treated, the condition of site hard and soft
tissues, the rehabilitation needs of the patient and, last but not least, the preferences of the
implantologist [1].
Most of these different reconstructive techniques and methods are based on the use of various
grafting materials which differ in their osteogenic, osteoconductive and osteoinductive properties.
Therefore, the choice must depend on a good knowledge of the properties of each material [1].
In 1991, during the Second International Consensus Conference in Chester, biomaterials have been
defined as materials for which is expected an interface with biological systems to evaluate, treat,
improve or replace every kind of tissue, organs or functions of the human body. This definition
identifies biomaterials not according to their properties, but considering their intended use [2].
Bone material substitutes are instead defined according to their origin into autologous, homologous,
heterologous and artificial bone [1] as follow:
Key Engineering Materials Vol. 541 (2013) pp 97-113© (2013) Trans Tech Publications, Switzerlanddoi:10.4028/www.scientific.net/KEM.541.97
All rights reserved. No part of contents of this paper may be reproduced or transmitted in any form or by any means without the written permission of TTP,www.ttp.net. (ID: 193.205.224.194-26/11/12,08:26:15)

- Autologous (Autograft) when the transfer of bone tissue is done from a donor site to a
recipient site in the same individual
- Homologous (Allograft) when the transfer of bone tissue, properly treated, takes place
between individuals of the same species (i.e. bone bank)
- Heterologous (Xenograft) when the transfer of bone tissue, properly treated, takes place
between individuals of different species (i.e. bovine bone)
- Alloplastic graft when synthetic materials (i.e. hydroxyapatite, bio-glass, tricalcium
phosphate, resorbable polymers, etc.) are used.
In this study bone material substitutes used as scaffolds will be analyzed as osteconductor
biomaterials used to verify the possible applications of microtomographic techniques as an aid in
clinical practice applied in both bone tissue regeneration and tissue engineering.
Nowadays, tissue engineering aims to reconstruct biological tissues by culturing cells extracted
from the patient on artificial scaffolds. The scaffolds are made of biomaterials that allow cell
proliferation both in-vitro and in-vivo. After implantation, scaffolds can be reabsorbed through
metabolic processes or stay on site and continue to provide a mechanical support. These features
pave the way for replacing biological tissues and represent the basis of regenerative medicine [3-
10].
Biomaterials science is a relatively young discipline, still experiencing a steady growth in
developing new materials and testing new techniques. To investigate in this direction, innovative
methodologies like X-rays microtomography have been used in order to study bone tissue and
biomaterials as well as the interactions that occur both in-vivo and in-vitro, between biomaterial
substitutes and cellular components of biological tissues [3-6, 9].
Tissue Engineering started being considered a multidisciplinary research area in 1995, aiming at
tissue regeneration and restoring functions of different organs through cells implantation or tissue
growth outside the body, or stimulating cells to proliferate inside an implanted matrix. The
development of tissue engineering has been largely due to the improvement of materials’ design,
with the creation of three-dimensional scaffolds with a bio-mimetic approach, and also due to the
growing expectations of cell cultures in laboratory and to the molecular biology techniques with the
use of genes and growth factors [2,5,6]. Two different paths could be followed:
a. Tissue engineering – progenitor cells and/or bioactive molecules are seeded on three-
dimensional modified and absorbable materials (scaffolds). The engineered constructs grow
outside the body imitating natural tissues behaviour and then they are re-implanted in the
patient and usually absorbed and replaced by vital tissues with vascular and nervous support.
Clinical applications for cartilage, skin and blood vessels are already available.
b. In situ tissue regeneration – this approach involves the use of materials loaded with bioactive
molecules to stimulate local repair through mechanisms of cell adhesion and activation of
progenitor cells. The bioactive implanted materials then release bioactive molecules at a
controlled speed, activating in this way cells and their interactions. Cells, in their turn,
produce growth factors that stimulate the proliferation of other cells and their assembly into
in-situ tissues [11, 12].
The in-depth knowledge about the processes of deposition and re-modelling of bone tissue represent
the basis of tissue engineering. Biological, chemical and mechanical signals regulate and order a
sequence of events that are the starting point of bone repair, such as the production of granulation
tissue, differentiation of osteocompetent cells, formation, mineralization and re-modelling of the
intercellular matrix. At the end, a very solid tissue is formed, apparently unchangeable but with a
continuous and dynamic evolution due to biochemical stimuli (growth factors, cytokines,
hormones) and to mechanical forces applied to the bone [1, 2, 11].
98 Bone and Biomaterials for Bone Tissue Engineering

The goal of bone tissue engineering is to put together all these components: a three-dimensional
support (scaffold) that must allow the adhesion and the function of osteocompetent cells in response
to biochemical stimuli, and in presence of an adequate vascular supply [3-6, 13].
A scaffold must be able to mimic the stromal support of bone tissue and therefore will have pores
and interconnections with diameter size in the range of 100-300 microns in order to allow the
migration and proliferation of bone cells, vascular structures and osteoid matrix. A process of
degradation might occur at the same time as bone regeneration in-situ, providing mechanical
stability, necessary condition for the restoration of function, without producing toxic substances or
altering the local pH, etc…[13, 14].
There are natural materials which are generally easy to find, prepare and model in required formats
and composition, with mechanical and structural properties very similar to human bone tissue. In
the specific, there are hydroxyapatites (HA) of animal (bovine, equine, swine, corals) or plant
(seaweed) origin properly treated from an antigenic point of view to reduce the inflammatory
response of the receiving site.
The homologous bank bone tissue (from cadaver or living donor) has been also widely used in its
various formulations (DFDBA, Demineralized Freeze-Dried Bone Allograft; FDBA, Freeze-Dried
Bone Allograft) although the risk of spreading infectious diseases vectors is still affecting the use.
At the same time, synthetic materials are ever more used since their structural and architectural
features can be checked during the production phase. These are mainly bio-glass and ceramic
materials such as hydroxyapatite (HA), calcium phosphate (CP) and tricalcium phosphate (TCP),
which have the same structure of bone mineralized component and a partially or totally modulating
porosity. The main disadvantages of these substances are their reabsorbility, as degradation time
can require years, and mechanical properties, due to fragility of ceramics which are unable to bear
heavy loads and impacts [13-15].
Polymers represent another branch of the synthetic material industry. These substances can be
highly modulated from a chemical point of view, are mouldable, and have a known degradation
time. Composites may be particle-loaded polymers, fibres, ceramic/carbon tubes also in nanoscale
(<100 microns) and, as hybrids, they have excellent physical and mechanical properties [15].
Osteoinductive properties of synthetic scaffolds can be further improved thanks to the
implementation of bio-mimetic surfaces, that is promoting the engraftment of the host cells and
their functionality as they’ve been treated with the addition of binding peptide sequences able to
interact with specific cell integrins [15].
Combining the three components scaffolds/cells/factors, some authors identify three possible
solutions in terms of bone regeneration and bone tissue engineering, i.e. cell-free systems, cell
systems and factor and gene therapies [15].
In matrix-based approaches, the chemical-structural features of scaffolds play a dominant role in
the healing process. The three-dimensional support must fill the defect properly, undergo
mechanical stresses and promote access, adhesion and proliferation of osteocompetent cells and
neo-formed vascular structures [3-8, 10, 15].
In cell systems, scaffolds are filled with cells harvested from the donor site, placed on these 3D
supports and induced to proliferate and differentiate in an osteogenetic way, with the goal of
transplanting them in the donor body. Whereas, the use of exogenous cells with no antigenic
potential is still under investigation [10, 15].
In the end, the factor-based or gene therapies, are considered the most innovative resource in this
field, supporting the introduction of an osteoinductive stimulus within the scaffold-cell system.
Growth factors (Bone Demineralized Matrix – DBM- and Bone Morphogenetic Proteins – BMP-),
synthetic factors or extracted from the patient (i.e. platelets) or other human subjects are still under
investigation but have been already applied in clinical practice and seems to induce a fast
regeneration, although it is difficult to bind them to transport molecules and regulate their release
and half-life, with the consequent high risk of pathogen transmission [9, 15].
Key Engineering Materials Vol. 541 99

X-ray microtomography (microCT) is a miniaturized form of computerized axial tomography
(CAT) able to investigate in a non-destructive, non-invasive and three-dimensional way small
radiopaque objects with a high resolution of a few microns.
This innovative technology, compared to conventional optic and electronic techniques, allows the
investigation of a sample avoiding cuts, covers or special chemical treatments.
Traditional techniques usually provide only bi-dimensional images while modern microscopy main
objective is to obtain a three-dimensional visualization of the samples, although the information
about their three-dimensional structure may be obtained by combining images of the surface of
several thin slices. Such information may not be reliable, as the methods of cutting or preparation
with destructive techniques can drastically alter the sample structure.
It is also true that many objects can’t be studied in this way due to the impossibility of being cut or
the risk of being damaged during the cutting phase [8, 16-27].
According to the shape and width of the incident beam of X-rays, there are two different geometries
in performing a tomographic investigations:
- Fan-beam geometry, when the X-ray beam is collimated to obtain a fan shaped beam that
affects a linear detector, which means that during the investigation, for each rotation angle,
slice to slice sample projections are acquired. The scanners that use such technology are
called single-row, but as effective as they could be, they’re now considered quite outdated
and very little used due to the long acquisition times required.
- Cone-beam geometry, where X-ray beam has the shape of a cone and a bi-dimensional
detector is used, allowing the simultaneous acquisition of several layers, reducing scan time
and radiation dose. 1998 witnessed the launch on the market of the latest generation of TC
multi-layers machines (multi-slice) with multi-row detectors [19, 24, 25].
Therefore, X-ray microtmography allows to investigate on objects without any preparation or
alteration; to obtain 3D images with different magnification in a non-invasive and non-destructive
way; to provide internal structure measurement of morphometric and ultrastructure parameters [19,
20, 22].
As a matter of fact, this methodology is widely used not only in medical and dental applications, but
also in biomedical engineering, material science, biology, electronics, geology, archeology and in
oil and semiconductor industry [4, 24, 25].
Computed tomography is based essentially on the execution of two different processes:
- acquisition of images and projection data;
- reconstruction of images using specific algorithms.
As an X-ray beam reduces its density while crossing a material, it will be then collected by means
of a system of detectors able to transform its intensity in an electric signal of corresponding value.
This electrical signal is proportional to the intensity of the outgoing beam, but also correlated to the
attenuation coefficient of the material it got through.
Considering that the more attenuated an X-ray beam, the more dense the structures it passes
through, a density map of the object can be acquired. A very thin and collimated X-ray beam, after
passing through a sample, reaches a detector providing a measure of the attenuation occurred
during the whole process. The sample is then rotated to get as many projections as the angles of
rotation are [19, 24, 25].
Image reconstruction phase requires the use of particular algorithms that allows to obtain, from the
composition of provided projections, a bi-dimensional image of the sample, called slice, composed
of a grid of pixels (picture elements) whose light intensity depends on the properties of attenuation
of X-rays within the corresponding voxel (volume element of the object).
After superimposing subsequent slices by means of a dedicated software, it is possible to obtain a
three-dimensional reconstruction of the entire sample and the complete visualization of its internal
and external structures. Therefore, this 3D image can be cut along any axis by means of the
previously used software, then inside explored and measured without any alteration [24, 25].
100 Bone and Biomaterials for Bone Tissue Engineering

In the end, we can briefly summarize the most important possibilities that this technology offers:
- evaluation of the structural properties of a material;
- morphological and morphometric analysis;
- objects’ porosity measurement;
- characterization of multiphase materials, identification and quantification of the defects of a
material such as cracks, craters and fissures;
- study of the behavior of materials subjected to different types of stress [4, 20, 24, 25, 28, 29]
Materials &Methods
Experimental study
This experimental study analyzed samples of tricalcium phosphate (TCP Bioset, Tiradix Srl,
Vimercate, MB, Italy), de-hydrated and de-antigenated equine bone (Bio-Gen, Biotek Srl, Milano,
Italy), re-absorbable nano-hydroxyapatite (Apagen Resorb 400, Gruppo Stomygen Srl, Roma,
Italy), and also a block of banked human iliac crest bone, de-hydrated and de-antigenated.
The study was divided in two phases:
- Pre-clinical/in-vitro study, in which the previously mentioned biomaterials have been
analyzed by means of microtomography before clinical application, in a sufficiently large
volumetric formulation (<3-4 mm) to allow reliable measurements;
- Clinical/in-vivo study, where the same biomaterials have been used in thinner formulations
inside primary bone defects (post-extraction sites) on voluntary patients.
Among the selected biomaterials listed above, only the re-absorbable nano-hydroxyapatite hasn’t
been analyzed by means of microtomography in pre-clinical in-vitro study, because it lacks
adequate dimensional formulation to allow a reliable pre-implantation morphometric evaluation.
A microtomographic analysis on a block of banked human iliac crest bone has been also carried out
in pre-clinical/in vitro study, to obtain reference images and morphometric parameters.
The microtomography analysis has been carried out by means of SkyScan 1072 system (SkyScan,
Kartuizersweg 3B, 2550 Kontich, Belgium), featuring a cone beam technology instrument, an
image reconstruction software (NRecon V1.6.3, Kartuizersweg 3B, 2550 Kontich, Belgium) and a
processing software of morphometric parameters (CT-Analyser V1.9, Kartuizersweg 3B, 2550
Kontich, Belgium).
Pre-clinical in-vitro study
This phase should be performed before application in a human model to assess, by means of
microtomographic analysis, to what extent pre-implant morphometric characteristics of a scaffold
may affect the osteoconductive properties of the graft.
To allow a reliable microtomographic morphometric analysis in pre-clinical study, some of the
osteo-conductor biomaterials mentioned above have been selected in a sufficiently large
formulation, more than 3-4 mm, in shape of block or particulate, as available on the market
Pre-clinical in-vitro study materials and methods
Samples of tricalcium phosphate, de-hydrated and de-antigenated equine bone and bank de-
hydrated and banked de-antigenated human cancellous iliac bone have been subjected to
microtomographic scanning and analysis.
The tricalcium phosphate sample has been provided in pellet form of about 3 mm diameter, the
equine bone was shaped as a block of 10x10x0 mm, and the human bone as a block of 9x15x10
mm.
Biomaterial samples used in different sizes in this study were scanned according to different
parameters, as follows:
- Tricalcium phospate at 3,66 µm pixel size, corresponding to 80X magnification;
- Equine bone at 13,32 µm pixel size, corresponding to 22X magnification;
- Human iliac crest bone at 16,3 µm pixel size, corresponding to 18X magnification.
Key Engineering Materials Vol. 541 101

Before scanning, a block of biomaterial sample was placed on a rotating stub inside the instrument,
a correct display of the sample has been assessed by observing the pc monitor to fit image inside the
limits, and to define the operating parameters that must be defined beforehand. These parameters
are:
- Voltage, 100 kV
- Current, 98mA
- Filter, 1mm aluminum
- Rotatiton Step, 0,45°
- Rotation Angle, 180°
- Frame averaging, 2 frames
- Amount of axial slices, about 800
- Slice thickness, 10 micron
The rotation angle chosen is not 360° because, with a full rotation, the same data would be acquired
twice, introducing artifacts reconstruction.
At the end of microtomographic data acquisition, bi-dimensional images are obtained for each
sample and, by means of a specific software (NRecon V1.6.3, Kartuizersweg 3B, 2550 Kontich,
Belgium) cross sections are then reconstructed.
For every cross section, a Region Of Interest (ROI) is chosen where a process of binarization called
tresholding is made in order to process data necessary to 3D image reconstruction.
Morphometric parameters are calculated by means of Ct_analyser software while three-dimensional
images are generated starting from 2D images by 3D_creator.
Pre-clinical in-vitro study results
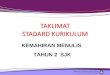
For every analyzed sample, hundreds of slices have been produced and three-dimensional images
have been obtained by means of 3D_creator processing software (Fig. 1)
Fig. 1 - 3D reconstruction image of tricalcium phosphate (a), equine bone (b) and human iliac crest
bone (c).
Table 1 shows the morphometric parameters obtained by means of CT_analyser software for each
material used in this study.
The morphometric parameters shown in Table 1 are:
− BV/TV (Bone Volume Fraction, in %) which represents the volume percentage,
− BS/BV (Specific Bone Surface, in mm-1
) the examined specific surface,
− Porosity (in %) that represents the percentage of voids compared to total volume,
− Tb.Th (Trabecular Thickness, in µm) that represents the thickness of bone trabeculae
− Tb.Sp (Trabecular Separation, in µm-1
) indicating the distance between each trabecula.
102 Bone and Biomaterials for Bone Tissue Engineering

Table 1. Morphometric parameter values obtained for each materials by microtomographic analysis
Parameters Tricalcium Phosphate Equine Bone Human bone
BV/TV [%] 70.36 26.44 27.38
BS/BV [mm-1
] 11.20 16.47 16.77
Porosity [%] 29.64 73.56 72.62
TbTh [µm] 265.05 220.01 206.83
TbSp [µm] 284.49 602.93 640.58
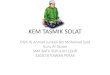
After in-vitro microtomography processing, negative 3-D images for each sample have been
obtained for an easy displaying of the interconnectivity of biomaterial and bone structures (Fig. 2)
Fig. 2 - Tricalcium phosphate (a), equine bone (b) and human iliac crest bone (c) 3D images.
Positive images are on top and negative ones are at bottom.
Pre-clinical in-vitro study discussion
The results obtained in this step of the study are not aiming at assessing the best biomaterial or
scaffold, but shall be used for a better structural knowledge of tested samples, suggesting to
clinicians how to choose the most suitable bone substitute for biomedical application.
The importance of the three-dimensional structure of an osteoconductive matrix in the formation of
a new bone is well known. An ideal scaffold should have specific features, such as high porosity, a
large surface area for cell adhesion, pores sufficiently large with wide interconnectivity to allow the
penetration of newly formed vascular structures.
Indeed, grafting is followed by a complex processes of cell proliferation, migration, and
differentiation, leading to bone formation. The presence of a three-dimensional osteocondutcive
matrix featuring structural characteristics very similar to human bone tissue makes the regenerative
process considerably easier. A high porosity contributes to the invasion of the graft by progenitor
cells, so the higher percentage content of pores, the larger the migration of mesenchymal cells and
osteoblasts to the recipient site. Moreover, high porosity and high ratio of surface area of contact-
Key Engineering Materials Vol. 541 103

volume (i.e. in presence of a large number of small pores) can promote cell adhesion. At the same
time, it is also true that large pores with extensive interconnections among them, contribute to
osteogenesis allowing an adequate blood supply and trophism of the graft.
Some authors [3-7] have shown that to improve osteogenesis a pore size of between 100 and 300
microns is required, but it is also quite evident that relatively large pores can influence the
mechanical strength of bone substitute materials.
This is essential in some types of applications of biomaterials because, in the early phases of the
integration process, the graft must also play as a support in complex skeletal segment that is going
to replace or repair and, therefore, must be able to support also loads, even if limited.
As regards the mechanical properties of a graft, trabecular dimensions and thicknesses also play a
decisive role.
There must be a compromise between all these aspects which are essential for an optimal
performance in the graft recipient site.
In the light of the results obtained so far, equine tissue represents the bone substitute material most
similar to the human bone. Sufficient porosity and an adequate value of specific surface and
trabecular separation allow the entry and migration of newly formed bone tissue inside the scaffold.
At the same time, the percentage volume and trabecular thickness grant equine bone mechanichal
properties comparable to those of human bone tissue.
On the other hand, results obtained for tricalcium phosphate show that this biomaterial is more
compact and full compared to equine bone, and also characterized by lower porosity and lower
trabecular separation, with a little space available for osteogenetic cell colonization and newly
formed vessels. Moreover, lower porosity together with higher value of trabecular thickness and
volume percentage express an increased mechanical strength.
The same results are observed from the analysis of 3-D reconstruction images obtained from the
biomaterials used (Fig. 1 and 2). In particular, we focused on the concept of Interconnectivity
(Connectivity Density) through the processing of the images in negative.
This parameter expresses the presence of spaces of communication and connection among pores
that are of fundamental importance for the migration of cells and fluids inside a scaffold. It is worth
mentioning that the synthesis product (tricalcium phosphate) has a poor internal interconnection,
compared to the other biomaterials [30-34] .
Clinical in-vivo study
In this second phase, the re-absorbable synthetic nano-hydroxyapatite and biomaterials analyzed in
the pre-clinical in-vitro study without human iliac cancellous bone have been used in smaller
compositions than the ones previously analyzed, to be implanted in a human model of primary bone
defect as post-extraction site.
During this in-vivo study, biomaterials have been chosen in chips or granules formulation with
different dimensional values:
- Beta- TCP in granules of 0.5-1 mm diameter;
- Hydroxyapatite equine cancellous in chips of 0.5 mm diameter;
- Re-absorbable synthetic Nano-hydroxyapatite in micro-granules of 400 µm diameter.
Samples of regenerated bone tissue extracted four months after first surgery were analyzed by
means of microtomographic and histological tests and the results have been compared with the
others obtained from similar evaluations carried out on samples taken from control sites, i.e.
extraction sockets healed only with blood clot in the same patient.
The main purpose of this study is to show the possible applications of microtomography in
morphometric characterization of normal human bone tissue and provide a further contribution in
the development of this technique in the study of the properties of the bone grafted with different
types of biomaterials [35].
104 Bone and Biomaterials for Bone Tissue Engineering

Clinical in-vivo study materials and methods
The study has been performed on 3 patients, aged 18-30 and in good health, who needed surgical
bilateral extraction of third lower molars totally enclosed.
With each of them, an informed consent has been discussed and signed in accordance with the
Declaration of Heliski to justify their participation in the research project. Moreover, the experiment
was approved by the Ethics Committee of the Sapienza University of Rome (Policlinico hospital
Umberto I in Rome, Rif.2134/28.04.2011).
Ortopantomography and intraoral pre-surgery examination confirmed the presence of total inclusion
of the lower octaves, bone or bone-lining, in order to obtain a closure of the flaps after surgery and
then protecting the grafts after avulsion.
In each patient the post-extraction site of one side was sutured and healed by means of clot
formation (control site), while the other (test site) was grafted with one of the osteconductors
biomaterials chosen for this study.
Each bone substitute has been compacted inside the after extraction alveolus, protected on the
surface by the application of a collagen sponge (Condress, Abiogen, Pharma) and the flaps were
then closed and sutured into their original position.
At sixteen weeks after avulsion, follow-up has been performed on patients with grafted and non-
grafted sites.
After raising a small flap of line-shaped muco-periosteum, specimens were extracted with steel
surgical trephine drill of 3 mm internal diameter (DRILL-300, FMD S.r.l. Medical Devices, Rome,
Italy), mounted on contra-angle handpiece and under abundant cooling, thus obtaining samples with
a height of about 5 mm (carrot sample) which were immediately placed in formalin and sent to
microtomographic and histologic analysis.
Before microtomographic scanning, each bone sample has been washed with physiological solution
and fixed on its stub in the instrument. After scanning, each carrot sample was again plunged in
sterile physiological solution for about ten minutes to facilitate rehydration and subsequently in
formalin for storage and sending to histological analysis.
For each control and test sample, morphometric values have been calculated while bi-dimensional
and three-dimensional images were produced with the same methodology adopted in the first phase
of this experimental investigation (pre-clinical in-vitro study).
In order to allow the superimposition of the qualitative and quantitative results, all samples were
scanned with the same following parameters:
- Magnification 95X, equivalent to 3.1 microns
- Rotation angle, 180°
- Rotation step, 45°
- Power source 100 KV- 98 microA
- Filter, 1 mm Al.
Three-dimensional images have been obtained by means of 3D_creator software, then coloured to
distinguish inside the extracted tissues the differences between each stage of mineralization and
highlight the residual particles of biomaterial.
It is well known that in radiology an object is displayed with different levels of gray corresponding
to a different coefficient of X-rays absorption that represents the structures that constitute the
sample.
Three density ranges have been chosen, each identified by a color, in order to highlight the
radiopaque structure of a single sample like the newly formed bone tissue in different stages of
mineralization and the biomaterials used.
After a careful study of the reconstruction software characteristics of the samples obtained, a range
of density has been set up to investigate the samples described above, allowing a proper
reconstruction and representation of a more advanced stage of calcification.
Key Engineering Materials Vol. 541 105

After obtaining the various images related to different stages of bone mineralization and
biomaterial, assigning each a different color, it’s possible to visualize the entire sample by
superimposing each image using a function that allows to overlap in transparency every single
structure.
For the different stages of bone mineralization, yellow area indicates a poor calcific component,
orange area an average mineralization while red area highly calcified structures (see an example on
Fig. 3).
Fig. 3 – Example of 3D image of a sample where yellow area indicates a poor calcific component,
orange area an average mineralization while red area highly calcified structures
For histological analysis, samples have been embedded in resin and treated according to traditional
techniques (no-decalcified samples; hematoxylin and eosin staining; 100X magnification).
Clinical in-vivo study results
For each sample, through microtomographic analysis and the subsequent reconstruction using a
dedicated software, hundreds of two-dimensional images have been obtained and collected in an X-
ray single image. By means of another displaying software, by scrolling images, it is possible to
observe any slice of the sample, selecting a specific line.
For each sample, histomorphometric parameters acquired by the software CT_Analyser are shown
in Table 2.
As in the pre-clinical phase, this table shows histomorphometric parameters such as BV/TV (Bone
Volume Fraction, in %), BS/BV(Bone Specific Surface, expressed in 1/mm), Porosity ( expressed
in %), Tb.Th (Trabecular Thickness, in mm) and Tb.Sp (Trabecular Separation).
Table 2 - Histomorphometric parameters obtained for test and control samples
Product Tricalcium Phosphate Equine Bone Resorbable nanoHA
sample test control test control test control
BV/TV (%) 17.77 61.31 15.07 31.69 54.25 52.07
BS/BV (mm-1
) 61.96 37.85 52.25 28.30 50.84 43.47
Porosity (%) 82.23 38.69 84.93 68.31 45.75 47.93
Tb.Th. (µm) 136.13 83.36 112.18 61.10 64.25 141.24
Tb.Sp. (µm) 331.41 117.00 462.20 141.81 73.82 95.96
106 Bone and Biomaterials for Bone Tissue Engineering

By means of 3D_creator software, 3D colored images have been reconstructed, where each color
indicates a density value of reference for a better view of analyzed human bone and biomaterials.
In the following pairs of images, the one on the left side represent always the 3D reconstruction of
the entire sample, while the one the right shows only one slice (Fig. 4 – 6).
Fig. 4. 3D reconstruction image of test sample with tricalcium phosphate (a) and a slice of the same
sample (b); control sample (c) and a slice of the same sample (d).
Fig. 5. 3D reconstruction image of test sample with equine bone (a) and a slice of the same sample
(b); control sample (c) and a slice of the same sample (d).
Key Engineering Materials Vol. 541 107

Fig. 6. 3D reconstruction image of test sample with resorbable nanoHA (a) and a slice of the same
sample (b); control sample (c) and a slice of the same sample (d).
By means of histological investigation, images shown in Fig.7 - 9 have been obtained for each
human bone sample, with and without tricalcium phosphate, equine bone, and re-absorbable
nanohydroxyapatite, to complete the analysis within this clinical trial and to confirm what already
observed in terms of qualitative and quantitative analysis by microtomographic analysis.
Fig. 7 - Histological image of test (sx) and control (dx) bone sample with tricalcium phosphate
(100x, H&E). CT = Connettive Tissue; Sc = residual Scaffold; NB = New Bone; BV= Blood
Vessels
108 Bone and Biomaterials for Bone Tissue Engineering

Fig. 8 - Histological image of test (sx) and control (dx) bone sample with equine bone (100x, H&E).
CT = Connettive Tissue; Sc = residual Scaffold; NB = New Bone; BV= Blood Vessels
Fig. 9 - Histological image of test (sx) and control (dx) bone sample with resorbable nanoHA (100x,
H&E). CT = Connettive Tissue; Sc = residual Scaffold; NB = New Bone; BV= Blood Vessels.
Clinical in-vivo study discussion
In this clinical study, an approach with simple models of experimental evaluation has been used, in
which a post-extraction bone defect has been selected as a grafting site for the different
biomaterials analysed. Using a split-mouth design, the post-extraction contra-lateral site, serving as
a control, was allowed to heal with simple clot.
As regards the quantitative evaluation emerging from morphometric data, it is clear that all test
samples have shown: a) a lower performance in the presence of a greater volume of non-
mineralized tissue, due to higher porosity; b) a smaller volume percentage and a greater trabecular
separation compared to control samples. This results in a lower or at least slown down new bone
formation inside the grafted bone defects.
By observing 3D microtomographic images colored as already mentioned in this article (Fig. 4),
qualitative considerations can be drawn to confirm the results of the analysis of morphometric
parameters.
Key Engineering Materials Vol. 541 109

The 3D reconstruction images of the test samples show a high presence of non-colored spaces,
probably due to non-mineralized tissue, such as fibrous connective tissue, vascular structures,
empty spaces. At the same interval of time, samples healed only with blood clot show a greater
formation of bone tissue, with widespread areas of mineralization.
This may lead to the conclusion that a biomaterial slows down the bone formation process.
Comparing the images obtained for test and control samples, it is interesting to observe that
microtomographic analysis can identify residual biomaterial particles in the grafted bone tissue; this
is more evident for very radiopaque bone-substitutes such as equine bone and tricalcium phosphate,
while becomes quite undetectable in re-absorbable nano-hydroxyapatite, due to its formulation in a
fine powder, which does not allow a clear display and probably also promotes a more rapid
reabsorption.
The analysis of histological images shows that histology is only able to confirm the presence of a
micro-CT undetectable biomaterial like reabsorbable nano-hydroxyapatite ( low radiopacity and
powder formulation) used in test samples.
It should be pointed out that only histological images are able to detect the presence of different
types of non-calcified tissues such as fibrous connective tissue, vascular structures, adipose tissue
and empty spaces that are non colored in 3D microtomographic images.
Conclusions
The results of this experimental investigation confirm the possible applications of X-ray
microtomography to provide a further contribution in the development of alternative approaches to
optics and electronics traditional microscopy, for microstructural characterization of human bone
and regenerated human bone after implantation of osteoconductive biomaterials [36].
In the in-vitro study, results have shown morphometric parameter values obtained by
microtomography analysis for human, equine and TCP bone substitute biomaterials. Comparing the
performance of these biomaterials it is possible to observe that equine bone values are more similar
to those of human bone.
In the clinical study, morphometric parameter values of test and control sample for each bone
substitute biomaterial used in-vivo are very different for TCP and equine bone, and very similar for
resorbable nanoHA. 3D microtomography images obtained in this study during the bone healing
process clearly highlight differently calcified areas, that is displaying poor calcification, average
mineralization and highly calcified structures. Bone substitute biomaterials are also detectable along
any dimension, by sample slicing through processing and reconstruction software. Differently,
histological processing is made on a single slide obtained by random sampling.
Moreover, the possibility of observing and comparing the scaffolds used as bone substitutes, has
allowed the biomedical field to consider the microtomographic technique a very important aid in the
choice of the ideal bone substitute for clinical applications [29, 34]. So far, this technique has also
been considered very useful in design and structural optimization of scaffolds with ideal and
predetermined osteoconductive characteristics. These features are able to completely overcome the
use of autologous bone, now considered the gold standard in bone regeneration, but patients need a
second surgery for removal of autologous bone, resulting in increased possibility of infections.
The use of microtomographic instrumentation allows structural observations of grafting
biomaterials without any treatment, alteration or damaging of samples. Through this system and a
dedicated reconstruction software, it is possible to obtain three- dimensional images and analyze
inside microstructure of a sample by slicing it in every direction. For each slice it is possible to
make further magnification without losing image quality.
In biomaterials industry, microtomography can contribute to the implementation of scaffolds with
ideal structural characteristics, studying their behavior and that of bone tissue subjected to different
types of stresses, from mechanical to chemical and thermal ones [36].
110 Bone and Biomaterials for Bone Tissue Engineering

In tissue engineering, microtomography may contribute to the design of a three-dimensional
biocompatible matrix for growing autologous ex-vivo cells for the repair of injuries and
regeneration of tissues. This technique has recently spread making it possible monitoring and
characterizing newly-formed bone tissue both in-vivo and ex-vivo, resulting from the combination
of progenitors cells, bio-molecules and biomaterials which act as osteoconductors [12, 36].
Acknowledgments
The authors wish to thank Alessandra Ceccarini for the linguistic review, and Prof. G. Soda of
Sapienza, University of Rome, Experimental Medicine Dept., for the technical support of
histological analysis.
References
[1] M. Chiapasco, E. Romeo, La riabilitazione implantoprotesica nei casi complessi, first ed.,
UTET, Milano, 2002.
[2] C.A. Vacanti, A.G. Mikos, Tissue Engineering, Mary Ann Liebert Inc., Larchmont (NY), 1995.
[3] A. Papadimitropoulos, M. Mastrogiacomo, F. Peyrin, E. Molinari, V.S. Komlev, F.
Rustichelli, R. Cancedda, Kinetics of in vivo bone deposition by bone marrow stromal cells
within a resorbable porous calcium phosphate scaffold: an X-ray computed microtomography
study, Biotechnol. Bioeng. 98(1) (2007) 271-281.
[4] J.R. Jones, G. Poologasundarampillai, R.C. Atwood, D. Bernard, P.D. Lee, Non-destructive
quantitative 3D analysis for the optimisation of tissue scaffolds, Biomaterials. 28(7) (2007)
1404-1413.
[5] H.G. van Lenthe, H. Hagenmuller, M. Bohner, S.J. Hollister, L. Meinel, R. Muller,
Nondestructive micro-computed tomography for biological imaging and quantification of
scaffold-bone interaction in vivo, Biomaterials. 28 (2007) 2479-2490.
[6] R. Cancedda, A. Cedola, A. Giuliani, V. Komlev, S. Lagomarsino, M. Mastrogiacomo, F.
Peyrin, F. Rustichelli, Bulk and interface investigations of scaffolds and tissue-engineered
bones by X-ray microtomography and X-ray microdiffraction, Biomaterials. 28(15) (2007)
2505-2524. Epub 2007 Jan 16. Review.
[7] S. Lin-Gibson, J.A. Cooper, F.A. Landis, M.T. Cicerone, Systematic investigation of porogen
size and content on scaffold morphometric parameters and properties, Biomacromolecules. 8(5)
(2007) 1511-1518.
[8] A. Basillais, S. Bensamoun, C. Chappard, B. Brunet-Imbault, G. Lemineur, B. Ilharreborde,
M.C. Ho Ba Tho, C.L. Benhamou, Three-dimensional characterization of cortical bone
microstructure by microcomputed tomography: validation with ultrasonic and microscopic
measurements, J. Orthop. Sci. 12(2) (2007)141-148.
[9] C.M. Cowan, T. Aghaloo, Y.F. Chou, B. Walder, X. Zhang, C. Soo, K. Ting, B. Wu, MicroCT
evaluation of three-dimensional mineralization in response to BMP-2 doses in vitro and in
critical sized rat calvarial defects, Tissue. Eng. 13(3) (2007) 501-512.
[10] V.S. Komlev, F. Peyrin, M. Mastrogiacomo, A. Cedola, A. Papadimitropoulos, F. Rustichelli, R.
Cancedda, Kinetics of in vivo bone deposition by bone marrow stromal cells into porous
calcium phosphate scaffolds: an X-ray computed microtomography study, Tissue. Eng. 12(12)
(2006) 3449-3458.
[11] N.L. Lumelsky, Commentary: engineering of tissue healing and regeneration. Tissue. Eng. 13
(2007) 1393-1398.
Key Engineering Materials Vol. 541 111

[12] Barbetta A, Bedini R, Pecci R, Dentini M. Role of X-ray microtomography in tissue
engineering. Ann Ist Super Sanita. 48(1) (2012) 10-8.
[13] L.E. Freed, F. Guilak, X.E. Guo, M.L. Gray, R. Tranquillo, J.W. Holmes, M. Radisic, M.V.
Sefton, D. Kaplan, G. Vunjak-Novakovic, Advanced tools for tissue engineering: scaffolds,
bioreactors and signaling, Tissue. Eng. 12 (2006) 3285-3305.
[14] D.W. Hutmacher, Scaffolds in tissue engineering bone and cartilage, Biomaterials. 21 (2000)
2529-2543.
[15] K.J.L. Burg, S. Porter, J.F. Kellam, Biomaterial development for bone tissue engineering,
Biomaterials. 21 (2000) 2347-2359.
[16] R. Müller, H. Van Campenhout, B. Van Damme, G. Van Der Perre, J. Dequeker, T. Hildebrand,
P. Rüegsegger, Morphometric analysis of human bone biopsies: a quantitative structural
comparison of histological sections and micro-computed tomography, Bone. 23(1) (1998) 59-
66.
[17] A. Sasov, D. Van Dyck, Desktop X-ray microscopy and microtomography, .J Microsc. 191(2)
(1998) 151-158.
[18] P.F. Gielkens, J. Schortinghuis, J.R. de Jong, M.C. Huysmans, M.B. Leeuwen, G.M.
Raghoebar, R.R. Bos, B. Stegenga, A comparison of micro-CT, microradiography and
histomorphometry in bone research, Arch. Oral. Biol. 53(6) (2008) 558-66.
[19] M. Kachelrieb, Micro-CT, Handb. Exp. Pharmacol. 185(1) (2008) 23-52. Review.
[20] M. Stauber, R. Müller, Micro-computed tomography: a method for the non-destructive
evaluation of the three-dimensional structure of biological specimens, Methods. Mol. Biol. 455
(2008) 273-292.
[21] Y.S. Park, K.Y. Yi, I.S. Lee, Y.C. Jung, Correlation between microtomography and
histomorphometry for assessment of implant osseointegration, Clin. Oral. Implants. Res. 16(2)
(2005)156-160. Erratum in: Clin Oral Implants Res. 2005.
[22] P.F. Gielkens, J. Schortinghuis, J.R. de Jong, M.C. Huysmans, M.B. Leeuwen, G.M.
Raghoebar, R.R. Bos, B. Stegenga, A comparison of micro-CT, microradiography and
histomorphometry in bone research, Arch. Oral. Biol. 53(6) (2008) 558-66.
[23] D. Chappard, N. Reatailleau-Gaborit, E. Legrand, M.F. Baslè, M. Audran, Comparison insight
bone measurements by histomorphometry and microCT, J. Bone. Miner. Res. 20 (2005) 1177-
1184.
[24] R. Bedini, R. Pecci, P. Ioppolo, D. Meleo, A. Bianco, P. Casti, Proposta di valutazione
microtomografica di alcuni sostituti ossei, Istituto Superiore di Sanità, Roma, 2009. (Rapporti
Istisan 09/10).
[25] R. Bedini, P. Ioppolo, R. Pecci, P. Filippini, S. Chiazza, A. Bianco, G. Columbro, Osservazioni
di osso equino al microscopio elettronico a scansione e alla microtomografia 3D, Istituto
Superiore di Sanità, Roma, 2005. (Rapporti Istisan 05/37).
[26] R. Bedini, D. Meleo, R. Pecci, L. Pacifici, The use of microtmography in bone tissue and
biomaterial three-dimensional analisys, Ann. Ist. Super. Sanità. 45(2) (2009) 178-184.
[27] S.Y. Tang, D. Vashishth, A non-invasive in vitro technique for the three-dimensional
quantification of microdamage in trabecular bone, Bone. 40(5) (2007) 1259-1264.
[28] G. Kerckhofs, J. Schrooten, T. van Cleynenbreugel, S.V. Lomov, M. Wevers, Validation of x-
ray microfocus computed tomography as an imaging tool for porous structures, Rev. Sci.
Instrum. 79(1) (2008) 013711.
112 Bone and Biomaterials for Bone Tissue Engineering

[29] Bedini R, Meleo D, Pecci R, Pacifici L. The use of microtomography in bone tissue and
biomaterial three-dimensional analysis. Ann Ist Super Sanita. 45(2) (2009) 178-84.
[30] Rossella Bedini, Pietro Ioppolo, Raffaella Pecci, Franco Marinozzi, Fabiano Bini, Elisa Pepe,
Andrea Marinozzi. Misura delle caratteristiche di tessuto osseo in condizioni patologiche
tramite analisi microtomografica: primi risultati. Rapporti ISTISAN. 7 (2009) 1- 37.
[31] Lehmann G, Palmero P, Cacciotti I, Pecci R, Campagnolo L, Bedini R, Siracusa G, Bianco A,
Camaioni A, Montanaro L. Design, production and biocompatibility of nanostructured porous
HAp and Si-HAp ceramics as three-dimensional scaffolds for stem cell culture and
differentiation. CERAMICS-SILIKATY. 54 (2) (2010) 90-96.
[32] R Bedini, F Marinozzi, R Pecci, L Angeloni, F Zuppante, F Bini, A Marinozzi. Analisi
microtomografica del tessuto osseo trabecolare: influenza della soglia di binarizzazione sul
calcolo dei parametri istomorfometrici. Rapporti ISTISAN. 15 (2010) 1- 49.
[33] Bernardo E, Colombo P, Cacciotti I, Bianco A, Bedini R, Pecci R, Pardun K, Treccani L,
Rezwan K. Porous wollastonite–hydroxyapatite bioceramics from a preceramic polymer and
micro- or nano-sized fillers. Journal of the European Ceramic Society. 32(2) (2012) 399-408.
[34] Meleo D, Bedini R, Pecci R, Mangione F, Pacifici L. Microtomographic and morphometric
characterization of a bioceramic bone substitute in dental implantology. Ann Ist Super Sanita.
48(1) (2012) 59-64.
[35] Marinozzi F, Marinozzi A, Bini F, Zuppante F, Pecci R, Bedini R. Variability of morphometric
parameters of human trabecular tissue from coxo-arthritis and osteoporotic samples. Ann Ist
Super Sanita. 48(1) (2012) 19-25.
[36] Bedini R. A new technology in biomedical engineering analysis: the 3Dimensional
microtomography. Preface. Ann Ist Super Sanita. 48(1) (2012) 7-9.
Key Engineering Materials Vol. 541 113
Recommended