
Institutionalization of Patient Engagement and Consultation within the Structures and Systems of the Department of Health
Grace Marie V. Ku, MD, MPH, FPAFP, PhD1, 2, 3
Godofreda V. Dalmacion, MD, MSc, MHPEd, FPOGS2
Emmanuel Baja, MS, ScD2, 3
1Faculty of Medicine & Pharmacy, Vrije Universiteit Brussels, Belgium 2Department of Clinical Epidemiology, College of Medicine, University of the Philippines Manila 3Institute of Clinical Epidemiology, National Institutes of Health, University of the Philippines Manila Correspondence to: GMVKu at [email protected]; +639153615683

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 2
Table of Contents
LIST OF ABBREVIATIONS 4
EXECUTIVE SUMMARY 5
CHAPTER I: INTRODUCTION 7
GENERAL OBJECTIVE OF THE STUDY 8 DESIGN 8 METHODOLOGY 8
CHAPTER II: CONCEPTUAL FRAMEWORK 9
THE PATIENT ENGAGEMENT MODEL 9 SELF-EFFICACY, SELF-MOTIVATION AND SELF-CARE 10 THE MAJOR ROLES IN PATIENT ENGAGEMENT 11
CHAPTER III: METHODOLOGY 13
REVIEW OF LITERATURE ON PATIENT ENGAGEMENT IN OTHER COUNTRIES 13 KEY INFORMANT INTERVIEWS AND FOCUS GROUP DISCUSSIONS 14 NON-PARTICIPATORY OBSERVATION 15
CHAPTER IV: RESULTS 16
REVIEW OF LITERATURE 16 INTERVIEWS WITH THE DEPARTMENT OF HEALTH KEY PERSONNEL 35 CURRENT PRACTICES IN PATIENT ENGAGEMENT 35 CURRENT INITIATIVES TO INSTITUTIONALIZE PATIENT ENGAGEMENT 36 LIMITATIONS OF PATIENT ENGAGEMENT PRACTICES 36 PERCEPTIONS ON PATIENTS’ INVOLVEMENT 36 POTENTIALS FOR PATIENT ENGAGEMENT 37 PATIENT INTERVIEWS 39 DEMOGRAPHICS 39 FOCUS GROUP DISCUSSIONS 39 INDIVIDUAL PATIENT INTERVIEWS 41 RECOMMENDATIONS FROM PATIENTS’ GROUPS / PATIENTS 43 NON-PARTICIPATORY OBSERVATION 44 A PATIENT GROUP IN ACTION 44 A DEPARTMENT OF HEALTH – RETAINED HOSPITAL 44 LOCAL GOVERNMENT UNITS 45
CHAPTER V: DISCUSSION 46
THE CONTINUUM 48 CONSULTATION, ACTIVATION AND AROUSAL 49 INVOLVEMENT AND ADHERENCE 51 SHARED LEADERSHIP AND THE EUDAIMONIC PROJECT PHASE 52

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 3
PROPOSED ACTIVITIES IN THE DIFFERENT LEVELS OF THE ENGAGEMENT CONTINUUM TO PROMOTE AND SUSTAIN PATIENT ENGAGEMENT 53 LEVEL 0: INITIATION OF ENGAGEMENT PRIOR TO DIRECT CARE / INDIVIDUAL LEVEL 53 LEVEL 1: DIRECT PATIENT CARE / INDIVIDUAL LEVEL 56 LEVEL 2: ORGANIZATIONAL DESIGN AND GOVERNANCE LEVEL 57 LEVEL 3: POLICY-MAKING LEVEL 57
MONITORING AND EVALUATION 59
OUTPUT AND OUTCOME MEASURES 59 IMPACT ON UNIVERSAL ACCESS 59
QUO VADIS, DOH? 62
THE “PATIENT AFFAIRS UNIT” 62 VISION AND MISSIONS 62 FUNCTIONS 62 STAFF COMPLEMENT 63 A ROADMAP FOR OPERATIONALIZATION 65
CHAPTER VI: CONCLUSIONS & WAYS FORWARD 69
REFERENCES 71

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 4
LIST OF ABBREVIATIONS
BHFS Bureau of Health Facilities and Services
BHW Barangay Health Worker CSO Civil Society Organizations DAOP Diabetes Association of Pateros DOH Department of Health DPCB Disease Prevention and Control
Bureau FGD Focus Group Discussion HFDB Health Facility Development Bureau HHRDB Health Human Resources
Development Bureau HTA Health Technology Assessment IDI In-depth Interview KII Key Informant Interview LGU Local Government Unit MeTA Medicines Transparency Alliance NCPAM National Center for Pharmaceutical
Access and Management RHU Rural Health Unit UHC Universal Health Coverage

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 5
EXECUTIVE SUMMARY
Introduction Patient engagement has come to be considered the cornerstone of the health
care system revolution for its potential impact on health outcomes and on
reducing health care costs. Moves towards full patient engagement -
promoting and supporting active patient and public involvement in health
and healthcare to strengthen their influence on healthcare decisions, at both
the individual and collective levels – have been evident in most high-income
and some middle-income countries. In the Philippines, the call for patient
engagement in health and healthcare has become louder.
This study was conducted to devise strategies in institutionalizing
mechanisms within the DOH in order to mainstream patient engagement
and consultation in the public health sector. In order to do so, an attempt to
establish the current state of affairs of patient engagement in health and
health care in the Philippines was made and examples of successful
implementations of patient engagement in other countries were reviewed,
taking into consideration lessons learned, possible behavior change theories
that could be applied, and adapting these to the context of the Philippines.
Methodology This was a predominantly qualitative study that involved review of related
literature and pertinent documents and records; interviews with
patients/patients’ groups and key personnel at the Philippine Department of
Health; and non-participatory observation of a patient group in action, a
healthcare facility, and two local government units.
Results and Discussion
Patient engagement at the individual level involves a series of phases that
educates, arouses and activates patients to become capable of being involved
in their healthcare and make informed decisions about their health. The
same phases are evident for patients to become involved in a collective
manner and ultimately become partners with health organization
administrators and policy-makers in health and healthcare issues. In the
Philippines, there are no formal or structured patient engagement programs
in the public health sector. Patient education initiatives depend on local
government units and undertakings of the national government related to

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 6
patients and patients’ groups are mostly informative. Aside from sporadic
occurrences in the grassroots level, there are limited formal mechanisms by
which patients are involved and participate in decision-making, and there are
no regulatory mechanisms by which to enforce such.
The authors identify phases and levels of patient engagement, adapted from
patient engagement models of Barello and Graffigna (2015) and Carman et
al. (2013) and, applying current practices in other countries and adapting
these to the context of the Philippines, propose a roadmap for
operationalization to institutionalize patient and family engagement within
the structures and systems of the Department of Health. The roadmap
consists of seven strategies, namely: (1) education, empowerment and
enablement of patients and their families to be engaged in healthcare; (2)
preparation of direct care providers and health facility administrators for
patient engagement in healthcare; (3) creation of the First Line Care Team;
(4) monitoring and evaluation (including transparency and accountability);
(5) legislation and regulation; (6) partnership in health facility governance;
and (7) partnership in public policy (including research/production of
evidence for policy and HTA).
A separate unit in the DOH dedicated to patients’ affairs is recommended.
The mandate, functions and minimum staffing with corresponding basic
duties and responsibilities for this Patient Affairs Unit were identified.
While the DOH prepares for the official requisites towards the creation of
this unit, the Disease Prevention and Control Bureau may be designated to
initiate implementation of the first four strategies above, in coordination
with the Health Human Resources Bureau, the Bureau of Health Facilities
and Services and the Health Facilities Development Bureau, and in
collaboration with Local Government Units.
The DOH should introduce regulatory changes to institutionalize patient
engagement. Legislative changes have to be advocated by patients and
patients’ groups, together with their supporters such as the Medicines
Transparency Alliance.
Once the Patient Affairs Unit has been established with a full complement of
specific staff members, the seven strategies can be fully implemented.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 7
CHAPTER I
INTRODUCTION
Universal access to health and universal health coverage (UHC) imply that
all people and communities have access, without any kind of discrimination,
to comprehensive, appropriate and timely, quality health services based on
health as a fundamental human right. To achieve the goals set forth in UHC,
a multi-sectoral approach to address the social determinants of health and
promoting a society-wide commitment to foster health and well being is
required. Patient engagement is an indispensable ingredient in health service
delivery. Engagement means actively soliciting the experiences and values
these stakeholders bring to the table, and involving them throughout the
process. Patients, being the center of all health-related interventions, should
be rightfully at the center of the discussions. Unfortunately, the very
important patient perspective is often presented by researchers, policy
makers, disease-based organizations, and healthcare professionals, rather
than by the patients themselves.
In 2014, the Medicines Transparency Alliance (MeTA) Philippines, in
collaboration with the World Health Organization (WHO), commissioned a
research study entitled “Stakeholder Mapping and Development of a Framework for
the Engagement and Empowerment of Patient Organizations in the Philippines”. In the
study, there were 59 duly “licensed” patient organizations that were mapped
out which have varying mandates, structures, objectives and levels of
capacity. Gaps were identified in the areas of advocacy, communication and
information sharing, and provision of patient support and other services. In
spite of the encouraging number of patient organizations in the country,
there was no consolidated or umbrella organization that engages with the
Department of Health (DOH) and other stakeholders. Individual groups
consult or lobby on an ad hoc basis, oftentimes on specific disease-related
issues. Only a few relatively more organized groups supported by medical
societies or healthcare professionals are able to discuss their concerns with
other stakeholders, but the voice of the majority in this sector is largely
unheard. Although patient-centered care and patient safety is a national
priority and a core agenda of the DOH, there is no formal or institutional
mechanism within the current DOH structure to engage, consult and
collaborate with patients and patients’ organizations. To date, no organized

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 8
patient group, no agency inside the Department of Health or the Local
Government health facilities is directly connected with formally
incorporating patient engagement in the delivery of health care. Evidently
MeTA has identified the Department of Health to push forward patient
engagement by commissioning this study, which aims for the
institutionalization of Patient Engagement within the structures of the
Department of Health.
GENERAL OBJECTIVE OF THE STUDY This research was conducted to formulate institutional mechanisms within
the DOH in order to mainstream patient engagement and consultation in
the public health sector.
DESIGN Qualitative methods including focus group discussions, in-depth interviews
and key informant interviews; review of related literature, legislation and
documents; and observation of structures and activities considered as critical
to patient engagement were done.
METHODS Publications regarding examples/cases of effective patients’ engagement in
the public health sector as seen in other countries were reviewed; the current
practice within the DOH in sourcing patients’ insights and
recommendations, and integrating them in national policies and programs
were documented; patients experiences and opinions on patient engagement
up to the level of incorporation of their insights and recommendations in
DOH policies and activities were collected; and steps to formalize a regular
consultation process and a system to engage patient organizations in the
planning, execution and monitoring of key health policies and programs
were devised, identifying human, technical and other resources necessary to
support implementation of the proposed framework.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 9
CHAPTER II
CONCEPTUAL FRAMEWORK
THE PATIENT ENGAGEMENT MODEL
Barello and Graffigna (2015) define patient engagement as a processual
multi-level experience that results from conjoint cognitive (think), emotional
(feel) and conative (act) orientation of individuals towards their health
management. They also proposed a patient health engagement model to
illustrate the process of patient engagement (Figure 1).
Figure 1. The Patient Health Engagement Model. (Barello & Graffigna 2015)
In the “blackout” phase, patients fall into an initial state of emotional,
behavioral and cognitive blackout determined by a critical event that appears
unexpected and out of their control. It is deemed that the patient would be
in a “pre-contemplative” state and may be fully dependent on a paternalistic
model of medical care. In the subsequent phase of “arousal,” patients are
hyper-attentive for all symptoms their bodies produce. The patient may
enter the early contemplative stages wherein perceptions of self-efficacy
(Bandura 1977) in caring for the self may already be felt. Self-care may be
fully realized in the next phase as the patient adopts engagement. The
“adhesion” phase comes when patients have enough knowledge and
behavioral skills to effectively adhere to medical prescriptions and feel
sufficiently confident in their own emotional strength to cope with their
health condition. At this point, the patient may already be empowered
enough to veer away from the paternalistic model of medical care and move
“I am an ill body”

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 10
towards a collaborative model. Finally, the “eudaimonic project” phase
features patients that have fully come to terms with their health condition
and have accepted that the “patient” self is only one of their possible selves.
They are also able to recognize the internal resources needed to project
satisfactory life trajectories for their future. This final phase is also referred
to as the “full health engagement status” where, following the self-
determination theory (Ryan & Deci 2008), sustainable (autonomous)
motivation to adopt and adhere to self-care behavior has been stimulated
and developed.
Patient engagement – particularly of people with chronic conditions – has
come to be considered the cornerstone of the health care system revolution
for its potential impact on health outcomes and on reducing health care
costs (Barello et al. 2014). Involvement of the patient in caring for
him/herself entails more than promoting simple compliance to prescribed
medications and mere adherence to the therapeutic regimen (Delamater
2006). A collaborative approach (Wagner 1998) that takes into consideration
not only the biomedical aspects of the disease or the condition but also the
psychosocial aspects of the patient as a person may elicit better participation
of the person to be engaged for better (self-)care.
SELF-EFFICACY, SELF-MOTIVATION AND SELF-CARE
Corollary to Barello and Graffigna’s Patient Engagement Model and the
behavior change theories related to the different phases of patient
engagement, a local study on people with diabetes in Luzon (Ku & Kegels
2014a) demonstrated that the degree of self-efficacy and self-motivation that
the person possesses in order to be aroused and to adhere to health
engagement may depend on the types of attitudes, perceptions and beliefs,
and the level of knowledge and skills the person has. These internal factors
may be affected by the attitudes of and the information, education, skills
training, and other forms of support that come from the environment –
from the healthcare provider, the health service, and the community.
Whether these environmental factors are considered as motivators or de-
motivators will depend on the person. (Figure 2).

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 11
Figure 2. Internal and external influences that may affect self-care (from Ku & Kegels 2014a)
THE MAJOR ROLES IN PATIENT ENGAGEMENT
There are three groups that have major roles in patient engagement: the
engagee, the engagers, and the influencers.
In patient engagement in health, patients are logically thought of as the
engagees. It should be noted that patients, as engagees, are rational actors but
individual behavior can be affected by social, contextual and environmental
influences. Thus, for a person to be engaged, changes must be put in effect
at the individual, interpersonal and community levels. Engagement should
thus occur at the levels of (1) direct patient care, (2) the health care
organization / health system, and (3) policy-making. Consequently, engagers
should include the health care providers in the patient-doctor relationship,
and representatives from the health care organization, the health system, the
community, and the society. Fully engaged patients can also become
engagers themselves.
At the “direct patient care” level, engagement occurs focusing on the

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 12
individual. The patient is (a)“activated”; (b) assisted in setting goals for
health and self-care; (c) advised and supported for the “in-between”
moments when the person has to decide for any issues concerning the
condition without the immediate aid of a professional health care provider;
and (d) that arrangements have been made for follow-up, for consultations
with other health care professionals as needed, and referring the patient to
(support) groups (Ku & Kegels 2015). This individual focus becomes
collective in the other two levels. At the “health care organization/health
system level”, the patient would be involved in the organizational design and
governance of the health service or health system. At the community and
societal levels, the patient would be involved in policy-making. Carman et
al. (2013) illustrate the levels and continuum of engagement and the possible
factors that may influence engagement (Figure 3).
Figure 3. A multi-dimensional framework for patient and family engagement in health and healthcare (Carman et al. 2013)

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 13
CHAPTER III
METHODOLOGY
This was a predominantly qualitative study comprised of literature review,
qualitative interviews and, to a much lesser extent, non-participatory
observation. Scientific publications regarding experiences of other countries
on patient engagement were retrieved; interviews regarding patient
engagement among patients/patients’ groups in the Philippines and
officials/staff of the Philippine Department of Health were conducted; and
a patient group in action, a DOH-retained hospital and a municipality were
observed.
REVIEW OF LITERATURE ON PATIENT ENGAGEMENT
IN OTHER COUNTRIES
A scoping review of literature on the experiences of other countries
concerning patient engagement in the public health sector was done.
Attempts to retrieve information on the following were made: (1)
mechanisms by which a Principal Engager may support and promote
engagement at the community/societal level, the interpersonal level and at
the individual patient’s level; (2) the interactions between and within all
engagers, influencers and the engagee; (3) the processes of
implementation/operationalization; (4) the results of
implementation/operationalization; and (5) contributions of the engaged
patient either as an individual or as an organized group towards the
development of sound health policies and programs. At the
community/societal level and the health system/health service level,
healthcare providers, healthcare financiers, and support groups were deemed
as the engagers and influencers. At the interpersonal level, the healthcare
provider was considered as both an engager and an influencer, and family
and friends as influencers. Organizations with commercial interests in the
provision of health care and services are deemed as potential influencers.
Strategies delineated in the literature retrieved that could be applied in or
adapted to the context of the Philippines were noted.
Search for scientific publications were conducted using the PubMed database.
Keywords that were used were “patient engagement” and “health policies” OR
“patient participation” and “health policies”. Only publications published within

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 14
the past 10 years and written in the English language or with English
translation available were considered. Article sifting was done systematically.
Retrieved scientific publications were initially screened through the titles.
Abstracts of the chosen articles were retrieved and individually reviewed.
Full articles of the sifted abstracts were scrutinized and selected; only articles
that are relevant to this study’s objectives were included in the final
selection.
Philippine Department of Health documents (administrative orders,
programs, policies, etc.), which may refer to patient engagement, were also
reviewed. Information that were retrieved included: the types of AOs,
programs, activities and policies that were formulated / developed where
patients’ insights and recommendations were used; the specific patients’
insights and recommendations that were referred to; the degree to which
these insights and recommendations were used; and operationalization /
implementation and results if any.
KEY INFORMANT INTERVIEWS AND FOCUS GROUP
DISCUSSIONS
DOH officials/staff were interviewed regarding the extent of patient
involvement in the planning, execution and monitoring of key health
policies and programs and the strategies being utilized in gathering patients’
insights and recommendations. General open-ended questions on what
insights and recommendations from patients were considered in the
planning, execution and monitoring of key health policies and programs; the
degree to which these contributions were incorporated in the document; and
how these were collected were asked; questions specific to the
Bureau/Office were also asked.
Patients, either as individuals or as representatives of patients’ groups were
interviewed regarding their experiences of any involvement in the planning,
execution and monitoring of key health policies and programs. The
respondents were recruited from a list of patients’ groups in the Philippines
(MeTA 2014) and from snowballing. Individual patients (not belonging to
any patients’ groups in general) from sites in and outside Metro Manila were
likewise interviewed. Representation of as many (chronic)
diseases/conditions, of both sexes, of the different socio-economic strata,

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 15
etc. were sought. Additional criteria were: age of majority and willingness to
be interviewed.
The DOH interviews and patient FGDs were recorded in two separate
voice recorders and were later transcribed and translated to the English
language.
Proceedings of the individual patient interviews were noted by hand.
Thematic analyses of the qualitative data gathered from the KII/FGD were
done manually. Data from the DOH respondents were analyzed separately
from the data from the patient respondents.
Results of the analysis of the patients’ interviews were presented to the
patients / patients organization for feedback.
NON-PARTICIPATORY OBSERVATION
Activities of a local municipality-based patient organization (Diabetes
Association of Pateros), patient-engagement related activities and policies in
a DOH-retained provincial hospital (Bataan General Hospital) and any
undertakings that may influence or affect patient engagement in the City of
Balanga, Bataan and the municipality of Bangued, Abra were observed and
noted. Although this portion of the study was not in the protocol, it was
deemed that information gleaned might be useful and enrich the results
further.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 16
CHAPTER IV
RESULTS
REVIEW OF LITERATURE A total of 377 titles were retrieved from PubMed; of which 25 full articles
were reviewed. The process of systematically sifting retrieved articles is
illustrated in Figure 4.
Figure 4. Systematic sifting of articles reviewed.
Of the 25 articles that were reviewed, three were on shared decision making
either in the individual or the collective level; six were on organizational
design and governance in either facility- or community-based health
services; four on policy level; seven on research, guidelines development and
health technology assessment; and the remaining five covering two or more
of the aforementioned topics. Tables 1-5 summarize pertinent information
taken from the reviewed full articles.
Table 1. Shared Decision-making (Individual and Collective) 1. Changing the policy landscape: haemophilia patient involvement in healthcare decision-
making Author Brian O’Mahony, Alastair Kent, Segolene Ayme Year of publication 2014 Type of study Meta-analysis; narrative Location of study European Union Type/Level of engagement studied Knowledge management; individual patient,
policy Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Collaboration, networking

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 17
Results of implementation / operationalization
n/a
Problem(s) encountered / Limitations of the Study
n/a
Contributions of the engaged patient toward the development of sound health policies and programs
n/a
Plausible strategy (ies) for application / adaptation
All rare diseases face common challenges, so knowledge and expertise must be shared to improve the lives of affected patients [across the EU]. Collaboration can help to ensure that knowledge can be shared and resources combined as efficiently as possible, in order to tackle rare diseases effectively. Networking, registries and strong patient organisations are key success factors to achieving the goals of bridging the gap in provision of care and resources within each country.
2. Patient participation in collective healthcare decision making- the Dutch model Author van de Bovenkamp, Trappenburg and Grit
Year of publication 2009 Type of study Qualitative Location of study Netherlands Type/Level of engagement studied Not discussed in the article. Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Patient organizations are often asked to represent the interests of patients in formal decision-making (neo-corporatist model). Researchers asked actors who have had experiences with patient participation in decision-making processes.
Results of implementation / operationalization
Issues identified: (1) there are too many opportunities for participation and many patient organizations simply cannot cope with the demand, (2) Patient organizations have difficulty in contributing their perspective and have little bargaining power to support their position/experiential knowledge, (3) Professional employees and professional volunteers have different knowledge that could colour their input and that brings the issue of representativeness to the fore. The experiential knowledge patients were originally asked to contribute could paradoxically disappear in the background this way.
Problem(s) encountered / Limitations of the Study
Contributions of the engaged patient toward the development of sound health policies and programs
Not discussed in the article.
Plausible strategy (ies) for application / adaptation
One characteristic of neo-corporatism is that actors need to be recognized by the government to become part of the formal decision-making structure. Government therefore decides who is in and who is out. On the other end, when patient organizations focus on their professionalization

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 18
too much, they move away from the people they represent, which negatively affects their democratic potential. It is important to investigate further which subjects lend themselves to patient participation and which ones do not. The idea that patients should become an equal third party in every decision-making process concerning health care is not feasible in practice nor is it desirable when we look at the effects described. Forms of participation that rely on individual patients, such as focus groups, shadowing and training by patients, which have the advantage that they demand less of participants and are able to stay close to patient experiences, should also be considered.
3. An overview of patient involvement in healthcare decision-making: a situational analysis Author Chirk-Jenn Ng, Ping-Yein Lee, Yew-Kong Lee,
Boon-How Chew, Julia P Engkasan, Zarina-Ismail Irmi, Nik-Sherina Hanafi1 and Seng-Fah Tong
Year of publication 2013 Type of study Comprehensive literature review Location of study Malaysia Type/Level of engagement studied Direct patient care Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Not discussed in the article.
Results of implementation / operationalization
n/a
Problem(s) encountered / Limitations of the Study
n/a
Contributions of the engaged patient toward the development of sound health policies and programs
Incorporating teaching of SDM into undergraduate curriculum Incorporating a more structured SDM teaching into postgraduate curriculumP Incorporating SDM training into continuing professional development, including workshops on SDM and how to use patient decision aids Incorporating SDM in clinical practice guidelines Advocate the use of patient decision aids or other decision support tools in patient care Patient involvement in decision making as a quality indicator Payment/reimbursement for practices which implement SDM or use decision aids Baseline research on patient involvement in decision making at the national level Exploratory studies on the factors influencing decision making in a multi-cultural and multi-lingual context Developing and evaluating decision support interventions to help patients make informed decisions
Plausible strategy (ies) for application / adaptation

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 19
Develop and evaluate interventions to incorporate SDM in routine care Malaysian Medical Council should consider developing a national healthcare policy on SDM The Ministry of Health should improve on the existing patient health information system to make the content more accurate, user-friendly and accessible to the public Public health campaigns should target at empowering people to be more involved in their health care and making decisions about their health care
Table 2. Organizational design and governance of facility-based and community based health services
1. User engagement in the delivery and design of maternity services Author Nashita Patel, Daghni Rajasingam Year of publication 2013 Type of study Narrative Location of study UK (NHS) Type/Level of engagement studied Services in health facilities Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Empowering women through use of advocacy services; ‘Life course’, women centered approach to empowering women
Results of implementation / operationalization
n/a
Problem(s) encountered / Limitations of the Study
n/a
Contributions of the engaged patient toward the development of sound health policies and programs
Empowering these groups of women from ethnic minorities by the use of advocacy services may reduce some of the variation in the quality of care provided to them
Plausible strategy (ies) for application / adaptation
Established methods of user engagement have to be modified and culturally sensitive if service providers are to engage in a meaningful way with these groups of women. Innovative methods are required to re-educate doctors to enable shared-decision making. P
2. Involving users in service planning: A focus group approach Author Kelly A, Caldwell B, & Henshaw B
Year of publication 2006 Type of study Qualitative participatory research Location of study UK Type/Level of engagement studied Services in health facilities Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Involvement of service users in the possible reconfiguration of follow-up services for breast cancer patients at a North London hospital; focus group approach
Results of implementation / operationalization
Patients identified their needs such as the need for reassurance after the diagnosis of cancer, continuity of care, privacy and dignity and other elements of the Pexamination technique,

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 20
information and the detection of new symptoms, the opportunity to discuss feelings and worries
Problem(s) encountered / Limitations of the Study
Purely qualitative
Contributions of the engaged patient toward the development of sound health policies and programs
The qualitative approach provided the platform for the patients to tell their stories and provide valuable information about local services. The use of the focus group provided a valuable opportunity to explore also the thoughts and feelings of respondents in relation to breast care services in more depth than would have been feasible either in a questionnaire survey or through personal interviews.
Plausible strategy (ies) for application / adaptation
The focus group approach was an effective means of ascertaining the experiences and needs of service users.
3. Patient-and-public-involvement-models-and-muddles Author Forbat, Hubbard & Kearney Year of publication 2009 Type of study Qualitative Location of study UK Type/Level of engagement studied Services in health facilities Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Identified four models of engagement 1) Patient as consumer 2) Patient as citizen 3) Patient/ partner as partner 4) Patient as researcher Used method called Enabling Change collaborative work, where staff and people affected by cancer worked together to make changes to the service based on patient experiences and centralising patient involvement
Results of implementation / operationalization
Identified patient involvement concepts from perspective of service providers (some of which are worrisome according to the authors):
(1) Involvement is ‘patient satisfaction’, (2) Involvement is ‘day-to-day practice’, (3) Involvement is ‘making a difference to other’s care’, (4) Involvement is ‘getting a message across’
The range of ways of conceptualising involvement are used interchangeably within policy and practice without due recognition of the very different meanings and implications of public consultation, no evidence yet that health service providers are moving beyond the equation: involvement equals consultation.
Problem(s) encountered / Limitations of the Study
See above
Contributions of the engaged patient toward the development of sound health policies and programs
Not discussed in the article.
Plausible strategy (ies) for application / adaptation
One of the greatest barriers to truly integrating patient involvement into the health service, policy and research is the conceptual muddle with which

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 21
involvement is articulated, understood and actioned. There is a need for an urgent focus to underline the value in patients’ experiences informing services and research.
4. Patient empowerment as a component of health system reforms: rights, benefits and vested interests
Author Colombo, Moja, Gonzalez-Lorenzo, Liberati, Mosconi
Year of publication 2012 Type of study Narrative Location of study Italy Type/Level of engagement studied Not discussed in the article. Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Not discussed in the article.
Results of implementation / operationalization
Not discussed in the article.
Problem(s) encountered / Limitations of the Study
A paternalistic approach in health care still prevails in many countries, by professionals and patients. This is the first cultural obstacle to citizens’ and patients’ involvement, as health care operators often do not recognize patients and citizens as equal partners.
Contributions of the engaged patient toward the development of sound health policies and programs
Involving consumers in the development of information material for patients increases its relevance, reliability and understandability. Training programs targeted at citizens, patients and health professionals are needed in order to improve: (1) patients’ skills, in making informed decisions; (2) patients’ participation on advisory boards or in multidisciplinary working groups; and (3) health professionals’ skills in informing their patients and promoting shared decision-making. Full access to complete and reliable information is the key issue to allow and increase citizens’ and patients’ participation in health care decisions. A cultural change is still needed to spread these initiatives, to shift from expert- based medicine to shared decision-making. Improving citizens’ and patients’ health literacy is a fundamental condition to attain valuable benefits.
Plausible strategy (ies) for application / adaptation
5. A Model for Using Community-Based Participatory Research to Address the Diabetes Epidemic in East Harlem
Author Horowitz, Goldfinger, Pulichino, Arniella, & Lancaster
Year of publication 2008 Type of study Participatory research Location of study USA Type/Level of engagement studied Community-based health services Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Community engagement between clinicians, outreach workers, community leaders and researchers A conceptual model to describe the relationship

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 22
between individuals’ environments, medical care, and beliefs and behaviors, and how all of these elements affect nutrition, physical activity, and health outcomes including obesity and diabetes was created. A pilot of the HEAL (Healthy Eating, Active Lifestyles) program revealed that participants lost weight and maintained a 5% mean weight loss at 1 year follow-up.
Results of implementation / operationalization
Building trust through community outreach, and events. Then the coalition began to involve community members in research.
Problem(s) encountered / Limitations of the Study
Not discussed in the article.
Contributions of the engaged patient toward the development of sound health policies and programs
This model can be applied to other communities with low-income and low-literacy minority populations. Plausible strategy (ies) for application /
adaptation 6. ‘Pizza, patients and points of view’: Involving young people in the design of a post
registration module entitled the adolescent with cancer Author Fallon, Smith, Morgan, Stoner, Austin Year of publication 2008 Type of study Pilot exploratory study to develop “adolescents
with cancer” module Location of study UK Type/Level of engagement studied Not discussed in the article. Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Teenagers and young people with cancer from a major UK regional cancer centre were contacted by post and invited to attend a ‘Pizza, Patients and Points of View’ evening
Results of implementation / operationalization
The ‘post-it ideas storm’, and ‘diamond ranking’ identified and ranked the knowledge and qualities the participants felt adolescent cancer nurses should have.
Problem(s) encountered / Limitations of the Study
Involving users when they are young people can provoke anxiety including; the power balance between the facilitator and the young person might be seen as unequal or threatening, both facilitator and young person may feel vulnerable and the facilitator may feel unsure they have adequately developed communication skills necessary to engage young people in a meaningful way.
Contributions of the engaged patient toward the development of sound health policies and programs
There are benefits for both healthcare professionals and service users and carers to work in partnership in relation to health- care delivery and service planning: ensuring healthcare developments reflect service user and carers’ needs, reducing assumptions about user and carer’s views and needs, and improving communication between healthcare professionals and service users

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 23
Plausible strategy (ies) for application / adaptation
Activities used to elicit were the ‘post-it ideas storm’, ‘diamond ranking’ and ‘dot voting’ (Shephard & Treseder, 2002). Utilising the ‘spice it up’ framework (Shephard and Treseder, 2002) reduced the facilitators’ anxieties relating to engaging with young people in a meaningful way.
Table 3. Policy 1. Engaging Patients in Public Policy Advocacy
Author Charlotte W. Collins and Nuala S. Moore Year of publication 2014 Type of study Meta-analysis; narrative Location of study USA Type/Level of engagement studied Direct patient care; patient and community Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Engagement can be as simple as listening to patient stories about their conditions, struggles, and care, and respectfully asking them to repeat these stories to those who can make a difference. Ask them about the quality of their lives, including how the cost of care impacts them and their ability to work, socialize, and pay for other living expenses. P Invite patients to meetings and invite them to set up meetings for both groups. P Nominate a motivated patient to serve as a patient consumer representative on government regulatory panels, suchPas the FDA’s advisory committees.
Results of implementation / operationalization
n/a
Problem(s) encountered / Limitations of the Study
n/a
Contributions of the engaged patient toward the development of sound health policies and programs
Suggests that the patient plus the health care professional, along with a government-relations professional, are the “golden triad” of public policy change. Patients can convey authentic passion from their own stories about how a policy directly affects them or their community, a policy maker may define the parameters of a proposal byP a cost-benefit analysis or the ease of implementation. The government-relations professional completes the golden triad by adding insight into the policy-making process and by identifying potential tactics and barriers.
Plausible strategy (ies) for application / adaptation
2. Facts and figures about patient associations in the Netherlands between 2007 and 2009 Author Kamphuisa, Hekkerta, van Dongenb, Kool Year of publication 2012 Type of study Analysis of secondary data Location of study Netherlands Type/Level of engagement studied Policy Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Not discussed in the article.
Results of implementation / operationalization
Not discussed in the article.
Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 24
Problem(s) encountered / Limitations of the Study
Not discussed in the article.
Contributions of the engaged patient toward the development of sound health policies and programs
Not discussed in the article.
Plausible strategy (ies) for application / adaptation
Patient associations reduce information asymmetry by informing patients through several platforms such as social media.
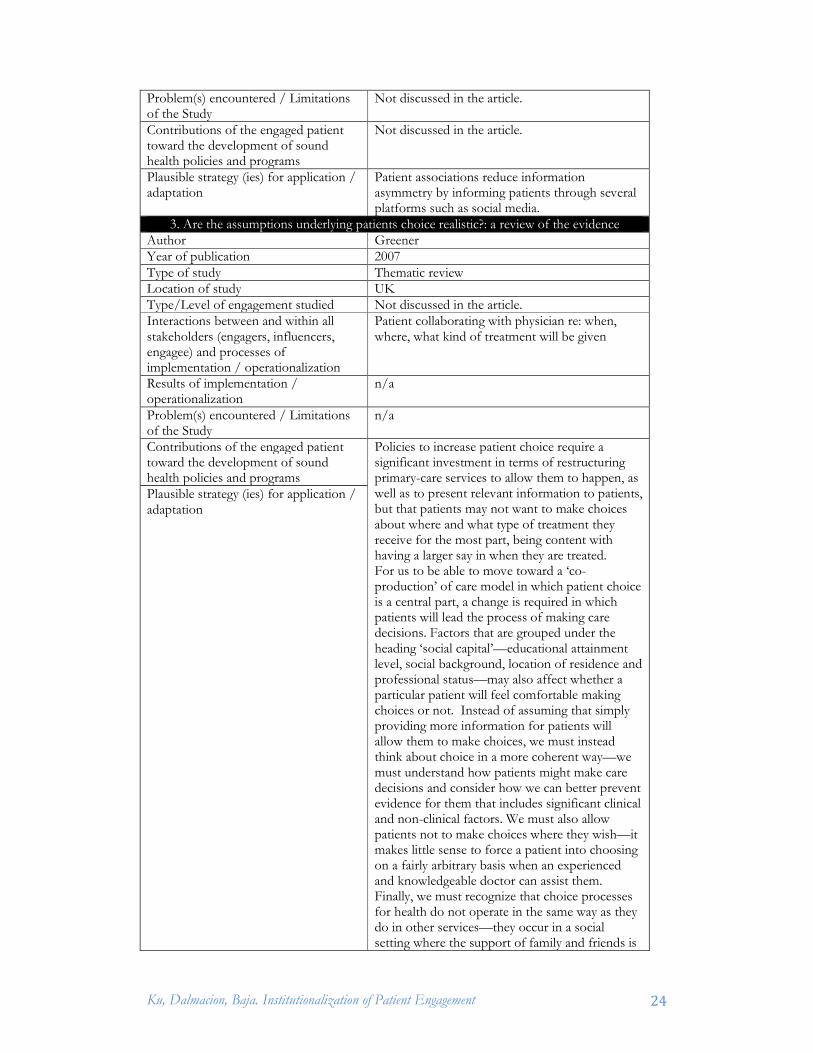
3. Are the assumptions underlying patients choice realistic?: a review of the evidence Author Greener Year of publication 2007 Type of study Thematic review Location of study UK Type/Level of engagement studied Not discussed in the article. Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Patient collaborating with physician re: when, where, what kind of treatment will be given
Results of implementation / operationalization
n/a
Problem(s) encountered / Limitations of the Study
n/a
Contributions of the engaged patient toward the development of sound health policies and programs
Policies to increase patient choice require a significant investment in terms of restructuring primary-care services to allow them to happen, as well as to present relevant information to patients, but that patients may not want to make choices about where and what type of treatment they receive for the most part, being content with having a larger say in when they are treated. For us to be able to move toward a ‘co-production’ of care model in which patient choice is a central part, a change is required in which patients will lead the process of making care decisions. Factors that are grouped under the heading ‘social capital’—educational attainment level, social background, location of residence and professional status—may also affect whether a particular patient will feel comfortable making choices or not. Instead of assuming that simply providing more information for patients will allow them to make choices, we must instead think about choice in a more coherent way—we must understand how patients might make care decisions and consider how we can better prevent evidence for them that includes significant clinical and non-clinical factors. We must also allow patients not to make choices where they wish—it makes little sense to force a patient into choosing on a fairly arbitrary basis when an experienced and knowledgeable doctor can assist them. Finally, we must recognize that choice processes for health do not operate in the same way as they do in other services—they occur in a social setting where the support of family and friends is
Plausible strategy (ies) for application / adaptation

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 25
crucial, and so, as a result, narrowing them to an individualistic process which does not take account these factors ignores the importance of individual support networks that are so crucial in welfare.
4. Tensions in public health policy: patient engagement, evidence-based public health and health inequalities
Author R Thomson, M Murtagh, F-M Khaw Year of publication 2005 Type of study Modeling Location of study UK Type/Level of engagement studied Not discussed in the article. Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Modeling of outcomes of shared decision making VS evidence-based guidelines for hypertension treatment
Results of implementation / operationalization
If only 50% (or 25%) of eligible patients agreed to treatment as a result of shared decision making, then 122 (or 183) strokes would occur that would otherwise have been prevented. In a typical UK general practice with 10 000 patients, this would represent an extra 12 (or 18) strokes over 5 years.
Problem(s) encountered / Limitations of the Study
Modeling only
Contributions of the engaged patient toward the development of sound health policies and programs
Engaging patients in treatment choices might therefore lead to fewer patients taking treatment, an increased incidence of stroke, and failure of health services to achieve targets for blood pressure control and disease reduction. Nonetheless, patients would have experienced greater involvement in decision making, less decisional conflict, greater satisfaction with their decision and, in those who decide to take treatment, potentially better levels of concordance and blood pressure control.
Plausible strategy (ies) for application / adaptation
There is a need to quantify the effects of patient engagement in treatment decisions and model the impact of these decisions on population health. There is also need for research that supports engagement that does not increase inequalities.
Table 4. Patient engagement in research, guidelines development and health technology assessment
1. Patient engagement in research: a systematic review Author Domecq, Prutsky, Elraiyah, Wang, Mohammed
Nabhan, Shippee, Brito, Boehmer, Hasan, Firwana, Erwin, Eton, Sloan, Montori, Asi, Dabrh and Murad
Year of publication 2014 Type of study Systematic literature review Location of study Not discussed in the article. Type/Level of engagement studied Not discussed in the article. Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of
Not discussed in the article.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 26
implementation / operationalization Results of implementation / operationalization
Some issues identified: patient engagement may become tokenistic (a false appearance of inclusiveness), resulting in a devaluated patients’ input. Another potential challenge described was “scope creep”; a theoretical concern that engaging patients in the research may include irrelevant community concerns and issues, which would make the research unfeasible.
Problem(s) encountered / Limitations of the Study
Not discussed in the article.
Contributions of the engaged patient toward the development of sound health policies and programs
Engaging patients in research improves patient enrollment and decrease attrition.
Plausible strategy (ies) for application / adaptation
Engaging patients in all research phases (preparatory, execution and translation) seems feasible in most cases. Patient engagement in healthcare research is likely feasible in many settings. However, this engagement comes at a cost and can become tokenistic. Research dedicated to identifying the best methods to achieve engagement is lacking and clearly needed.
2. Why we need community engagement in medical research Author Jessica K. Holzer, PhD1, Lauren Ellis, MA2, and
Maria W. Merritt, PhD Year of publication 2014 Type of study Participatory research Location of study California, North Carolina, Colorado
Type/Level of engagement studied Community engagement Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Employed locally appropriate trust-building activities such as hiring community members, working with community leaders and community-based organizations, considering the research participants’ practical needs, inquiring about factors affecting recruitment and retention, incorporating cultural practices into research protocols, and sharing results with community members Encouraging participation and promoting uptake of findings
Results of implementation / operationalization
Gains in recruitment and retention of African-American research participants
Problem(s) encountered / Limitations of the Study
Mistrust in research; Mistrust in health care system
Contributions of the engaged patient toward the development of sound health policies and programs
Value of engaging the community to medical research
Plausible strategy (ies) for application / adaptation
Applicable to all contexts, provided that researchers maintain context-specific situational awareness
3. The role of patient advocacy organisations in neuromuscular disease R&D Author Boon, BroekgaardenP Year of publication 2009 Type of study Not discussed in the article.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 27
Location of study Netherlands Type/Level of engagement studied Not discussed in the article. Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Not discussed in the article.
Results of implementation / operationalization
How the Dutch neuromuscular disease organisation (Vereniging Spierziekten Nederland, or VSN) communicated their needs in relation to biomedical innovations: (1) Management of expectations - aligning with scientific advisors and internalising the ability to assess scientific knowledge. Here it continuously kept track of scientific developments, annotated them, tried to clarify them, and reported about them using dis- claimers. They always left the choice to patients, and if they wanted to adopt a new therapy, they encouraged measurement of safety and efficacy data. (2) Active Case Building - VSN started to put issues on the policy agenda, such as the reimbursement of expensive drugs. They did a thorough synthesis of needs and preferences, which includes in some cases even producing full-blown consultations, reports and figures. (3) Network building - had an overview of the field and the problem at hand, and envisaged that some actors needed to be brought together in order to work on the problem. This mechanism largely concerns aligning other actors to achieve some longer-term solutions.
Problem(s) encountered / Limitations of the Study
Not discussed in the article.
Contributions of the engaged patient toward the development of sound health policies and programs
Not discussed in the article.
Plausible strategy (ies) for application / adaptation
Not discussed in the article.
4. User involvement, research and health inequalities: Developing new directions Author P. Beresford Year of publication 2007 Type of study Service user involvement in research Location of study n/a Type/Level of engagement studied Patients as engagees and as engagers
Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Researchers can include users in research, and at the same time, users can initiate the researches themselves.
Results of implementation / operationalization
n/a
Problem(s) encountered / Limitations of the Study
n/a
Contributions of the engaged patient toward the development of sound health policies and programs
n/a

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 28
Plausible strategy (ies) for application / adaptation
Health inequalities, with its concerns with disadvantage, social justice, social inclusion and equality seem a particularly suitable area to research in a participatory way, involving service users/participants and/or supporting and encouraging them to undertake their own research.
5. An international survey of the public engagement practices of health technology assessment organizations
Author Whitty Year of publication 2013 Type of study Web-based survey Location of study Australia Type/Level of engagement studied Not discussed in the article. Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Not discussed in the article.
Results of implementation / operationalization
Not discussed in the article.
Problem(s) encountered / Limitations of the Study
Challenges to engagement identified by respondents included the potential tension between social and scientific considerations, and practicalities around engaging patients and dissemination of information. Timeliness featured prominently, with respondents indicating a mismatch between the demand for timely HTA and the time required to undertake high-quality public engagement. A lack of expertise for undertaking qualitative research was identified as a challenge. While a majority of Health Technology Assessment (HTA) organization surveyed (67% of 39 responders) said that they engage in some form of public engagement, approximately half the organizations in the current survey reported being responsible for making decisions or recommendations. Findings of the survey appear to be that public engagement mechanisms used by HTA organizations predominantly occur via one- way transfer of information either from the HTA organization to the public (communication) or vice versa (consultation).
Contributions of the engaged patient toward the development of sound health policies and programs
Not discussed in the article.
Plausible strategy (ies) for application / adaptation
Some possible research questions: � Why do some HTA organisations report that
they do not undertake public engagement activity? Is this a philosophical position, or is a lack of engagement based on pragmatic barriers?
� Why and in what circumstances do organisations choose one engagement mechanism over another?

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 29
� Do different levels of HTA organisation use different public engagement mechanisms?
� To what extent do HTA organisations synthesise the literature on patient needs and perspectives or quantify patient or public preferences to inform HTA processes and decision-making?
� What are the potential role, benefits and disadvantages of novel approaches to public engagement, such as the use of social media?
� How can we synthesise the published literature and experiences from actual examples of public engagement in the HTA setting, to provide a more complete picture of development and activity in this area?
HTA organizations should be encouraged to publish narratives of their experiences with public engagement, to support the development of systematic yet pragmatic approaches and frameworks for doing so.
6. Patient-based health technology assessment: A vision of the future Author Bridges and Jones Year of publication 2007 Type of study HTA Location of study Not discussed in the article. Type/Level of engagement studied Individual patient Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Interaction between physician and patient mediated by HTA.
Results of implementation / operationalization
Not discussed in the article.
Problem(s) encountered / Limitations of the Study
Not discussed in the article.
Contributions of the engaged patient toward the development of sound health policies and programs
A patient-based HTA can promote the antecedents of empowerment by both informing patients about medicine and informing medicine about patients.
Plausible strategy (ies) for application / adaptation
HTA should be constructed in a way so that it is relevant to patients, and it must be respectful of the important role that physicians play in a shared decision-making environment. A patient-based HTA must be aware and respectful of patient preferences.
7. Reconsidering Patient Participation in Guideline Development Author van de Bovenkamp, & Trappenburg Year of publication 2008 Type of study Systematic literature review Location of study Type/Level of engagement studied Involvement in practice guidelines development. Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Not discussed in the article.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 30
Results of implementation / operationalization
When patients do participate, there is uncertainty amongst participants about the goals of participation and patients have difficulty following medical jargon and assessing technical medical literature. Several authors pointed out that as a consequence the patients gave little input.
Problem(s) encountered / Limitations of the Study
Not discussed in the article.
Contributions of the engaged patient toward the development of sound health policies and programs
Although the general consensus seems to be that patients should be involved in guideline development, the added value of their participation has yet to be established.
Plausible strategy (ies) for application / adaptation
Decision-making processes must be studied in different ways, for example by doing case studies, surveys, interviews and guideline analysis. A combination of methods should be used, including active participation, throughout the guideline development process. Most authors concluded that patient representatives should receive more guidance during the process. Patient participants ought to be trained, prepared and educated to fulfill their task. Attention in the guidelines for individual patient preferences can be accomplished by including a separate section or chapter on patient–physician communication.
Other conclusions Doctors and guideline development organisations did not always look forward to the idea that patients be involved in guideline development for patient care. Patients contribute most on the subject of patient education, although subsequently their contributions are not acted upon. Consumers should be involved in all stages of guideline development by using several methods at once, and supporting patients throughout the process. There is little evidence in support of the position of many authors that argue in favour of patient participation in guideline development because, supposedly, it increases the quality of the guidelines. Another difficulty that is encountered is the integration of patients’ experiential knowledge in an otherwise evidence-based guideline. Even if their involvement does not change the content of the guidelines much, it could make all parties in health care at least feel more like partners.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 31
Table 5. Multiple classifications (research, HTA, direct patient care, organizational design & governance, policy) 1. A review of literature about involving people affected by cancer in research, policy
and planning and practice Author Hubbard, Kidd, Donaghy, McDonald, & Kearney Year of publication 2007 Type of study Literature review Location of study n/a Type/Level of engagement studied Involving people affected by cancer in healthcare
research, policy and planning and practice Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
In research, people acted as advocates, strategists, advisors, reviewers and as participatory researchers. In policy and planning, people were involved in one-off involvement exercises and in longer-term partnerships. Men, those with rare cancers, children, and people who are socially deprived have been rarely involved.
Results of implementation / operationalization
n/a
Problem(s) encountered / Limitations of the Study
n/a
Contributions of the engaged patient toward the development of sound health policies and programs
n/a
Plausible strategy (ies) for application / adaptation
There needs to be a shift away from paternalism and a commitment made to sharing power and control. Healthcare professionals need to be encouraged to stop wanting to do things for patients, but to also want to do things with patients and their family care givers. Likewise, patients need to stop wanting things only to be done to them, but to also want to do things with healthcare professionals.
Other conclusions There is confusion around who is, and who should be, involved in research and policy and planning, and a lack of clarity of definitions when using the terms “user”, “patient”, “carer”, “public”, “consumer”, “advocate”, “stakeholder”, “survivor”. In the practice setting, it is clear that an individualised approach to involvement is required so that people affected by cancer can play an active, shared or passive role as, and, when they prefer. Thus, rather than advocating and implementing a ‘participation’ or ‘non-participation’ strategy for all patients, healthcare professionals need to adopt a flexible approach

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 32
2. Great expectations? Reflections on the future of patient and public involvement in the NHS
Author Ellins Year of publication 2011 Type of study Narrative Location of study UK Type/Level of engagement studied Individual Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Not discussed in the article.
Results of implementation / operationalization
Three key roles that patients can play in the healthcare system, all with the potential to improve the quality and outcomes of care: (1) evaluator, (2) consumer, (3) co-producer.
Problem(s) encountered / Limitations of the Study
Patient feedback tends to be used on an ad hoc and selective basis, rather than systematically or rigorously. Local services are most likely to respond to issues raised about the care environment, the provision of information and accessibility (eg opening times and appointment systems).
Contributions of the engaged patient toward the development of sound health policies and programs
Strategies to support patients have been established, although more tailored approaches that target the barriers to involvement that some groups are more likely to face are also required. Equally there needs to be a far greater focus on creating an environment conducive to patients evaluating services, making informed choices, and actively participating in their own care.
3. Theoretical directions for Pan emancipatory concept of patient and public involvement Author Gibson, Britten, & Lynch Year of publication 2012 Type of study Narrative Location of study UK Type/Level of engagement studied Individual with public partnership Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Not discussed in the article.
Results of implementation / operationalization
Proposed a framework for Patient and Public Involvement:
Problem(s) encountered / Limitations of the Study
Not discussed in the article.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 33
Contributions of the engaged patient toward the development of sound health policies and programs
People involved in establishing new involvement processes could use this framework to help identify the potential barriers and facilitators to the creation of any new engagement structures. The framework can also be used to map the diversity and fluidity of different patient and public involvement initiatives and groups. Effective engagement will always involve achieving at best a dynamic equilibrium between differing, sometimes contradictory points along the dimensions described in the framework (above). Professionals and lay people need to be able to participate from a position of equality, each acknowledging that there are complex questions of evidence and value in healthcare policy decisions. One of the aims of involvement may be to break down boundaries, share experience and build understanding. The government, together with its state ideological apparatuses, has to retreat and increase its trust in the citizenry of a democracy and its respect for their diverse cultures.
4. Patient and Citizen Participation in Health: The Need for Improved Ethical Support Author Laura Williamson Year of publication 2014 Type of study Meta-analysis; narrative Location of study n/a Type/Level of engagement studied Patient-centered approach, with individual patient
“making decisions for own health” Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
Contends that there must be public or community and private or individual patient engagement
Results of implementation / operationalization
n/a
Problem(s) encountered / Limitations of the Study
Narrative only
Contributions of the engaged patient toward the development of sound health policies and programs
n/a
5. What are the key ingredients for effective public involvement in health care improvement and policy decisions? A randomized trial process evaluation
Author Antoine Boivin, Pascale Lehoux, Jako Burgers,
And Richard Grol
Year of publication 2014 Type of study Randomized trial process evaluation Location of study Canada Type/Level of engagement studied All levels Interactions between and within all stakeholders (engagers, influencers, engagee) and processes of implementation / operationalization
The public members (1) attended a 1-day preparation meeting, (2) were consulted by vote on their local priorities for improvement, and (3) participated in a 2-day meeting to deliberate with professionals and reach agreement with them on local health care improvement priorities. The 2-

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 34
day meeting between public members and professionals included small-group deliberation, feedback of the public consultation results, and voting. In the control sites, the professionals among themselves prioritized quality indicators without public involvement (no participation of public members or feedback about the public consultation).
Results of implementation / operationalization
Priorities selected in intervention sites placed more emphasis on access to primary care, self-care support, patients’ participation in clinical decisions, and partnership with community organizations. Agreement between public representatives’ and professionals’ improvement priorities increased by 41% in favor of intervention sites. The intervention fostered mutual influence between patients’ and professionals’ priorities. Professionals’ choices moved toward indicators prioritized by the public (eg, access), and public representatives’ choices moved toward indicators prioritized by professionals (eg, self-care support).
Problem(s) encountered / Limitations of the Study
Limited because of the diversity of public involvement interventions and the influence of the sociopolitical contexts in which they are implemented
Contributions of the engaged patient toward the development of sound health policies and programs
The study showed how both technocratic (public credibility) and democratic process issues (their legitimacy to represent others) underlie the unfolding of a public involvement intervention and shape its impact on collective decisions. It also showed that public involvement interventions not only must give public participants enough information to understand the technical language used by professionals but also must support their ability to become a credible source of knowledge for professionals. Furthermore, it demonstrated that “giving a seat or two to patients” are unlikely to change health care and policy decisions.
Plausible strategy (ies) for application / adaptation
Engagers need to better distinguish statistical representativeness from representation roles in discussions about public legitimacy. They must also expand their notion of public members’ competence beyond members’ understanding of technical terms in order to support the development of a contributory public expertise.
No DOH documents explicitly stating consultation with or engagement of
patients during the formulation or crafting in any policies or activities were
found in our search.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 35
INTERVIEWS WITH THE DEPARTMENT OF
HEALTH KEY PERSONNEL
Representatives from five DOH bureaus/offices were interviewed. The
bureaus/offices were: (1) Health Policy Development & Planning Bureau;
(2) Health Facility Development Bureau; (3) Disease Prevention & Control
Bureau; (4) Human Health Resources Development Bureau; and (5)
Pharmaceutical Division. In-depth interviews of these key informants were
done. In two instances, there was more than one respondent per
bureau/office (HHRDB, HPDPB).
Contextual analysis of the interviews revealed the following findings
regarding current practices in patient engagement, current initiatives to
institutionalize patient engagement, limitations of patient engagement
practices, perceptions of the DOH on patient engagement, and potentials
for patient engagement.
Current Practices in Patient Engagement - Health Partners’ Meeting with civil society organizations (not
specifically patients’ groups) and academic institutions
- Joint Appraisal Committee and Joint Assessment and Planning
Initiatives
- Administrative documents and policies are drafted by the DOH, then
“nationwide” public consultations or dissemination forums are
conducted.
- Each bureau/office within the DOH craft its’ own policies and these
are funneled to DOH-HPDPB as a “finished product”.
- Engagement is more evident in a group of people with tuberculosis
(from the Lung Center of the Philippines) and disabled-people’s
organizations. However, programs for diseases/conditions that are
considered non-emergent are less or not prioritized.
- Advisory boards of hospitals are said to include one member from a
patients’ organizations (quality standards in hospitals)
- At present, patient engagement includes (and is somewhat limited to)
the use of patient satisfaction survey tools (patients are engaged as a
“service recipient” but not as a policy stakeholder).
- For the next cycle of budget preparation, the DOH will already be
required to include stakeholder consultation in its pre-planning

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 36
Current Initiatives to Institutionalize Patient Engagement - Adoption of the Mexico City Principle (disclosure of transparency
among pharmaceutical companies)
- AO 2007-0038 Development of Efficient National and Local Health
Systems: Engagement of stakeholders like LGU and Civil Society
Organizations (CSO).
Limitations of Patient Engagement Practices - Invited organizations to consultations and forum are not patient-
specific; rather, it is more of the CSOs who are more frequently
invited. Furthermore, whoever is invited to these
consultations/forums is at the discretion of DOH, and is usually
limited to those whose contact details are known to the Department
or are readily available.
- No concrete definition of “relevant” organizations to be invited to
the public consultations/fora
- DOH solicits “some” support from CSO in response to policies they
have created; but such consultations are mainly informative rather
than consultative
- There is no information system for patients and patient groups in the
DOH
- Some of the patients’ organizations have outdated websites and
contact numbers and thus are difficult to invite to policy
consultations
- DOH has no specific assigned office to receive patient inputs
- Patient groups are location-specific (inequity in patient
representation)
- Operations manuals for hospitals does not include consultations with
patients and patient groups
- Monitoring and evaluation of patient satisfaction survey results
beyond the facility as well as feedback to patients are vague
Perceptions on patients’ involvement - Perception that patients are too emotional, and might decide based
on emotions and “personally-related” experiences
- Perception that patients are not knowledgeable in the technical
process and technical concepts

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 37
Potentials for patient engagement - The need for patient engagement is recognized as this is required for
the next cycle of budget preparation
- Barangay Health Workers (BHWs) may play an important role as
patient engagers at the community level if they are trained to engage
and support people/patients
Interviews with representatives from the Department of Health revealed
that policies are usually crafted by the respective offices, bureaus, units and
the Health Policy Development and Planning Bureau (HPDPB) serves as a
“clearing house” for the “finished products”. The crafted policies are
introduced to the populace through nationwide “blitzes”, where members of
Civil Society Organizations, not necessarily of the patients’ groups’ variety,
are invited. When asked which specific patients’ groups have ever attended
any of these policy blitzes, the respondents replied that the most active ones
are those from the Lung Center of the Philippines and of people with
disabilities, which are based in Metro Manila. The DOH representatives
claim that it is difficult to invite patients’ groups as they do not have their
contact numbers, only a few patients’ groups have websites, and the contact
details listed in the said websites are oftentimes inaccurate. Neither does the
DOH have any office specifically for patients and patients’ groups –
whether to maintain a registry, to receive inputs, or to liaise between the
patients and the different offices of the Department, including the DOH-
related hospitals. With regard to specific processes in the crafting of policies
or program planning, the respondents replied that involvement of
patients/patients’ groups would depend on the office preparing the said
policy or program. However, patient participation in these activities are
vague; it is highly probable that they may only be included as a part of the
audience during information dissemination. The representatives, however,
are positive that involvement of and consultations with groups outside of
the DOH – civil society organizations generally and patients’ groups
specifically – will become a more common practice at the Department to
comply with the Department of Budget Management requirements. More
so, foreign aid specific for patient engagement activities will soon be
received by the DOH and thus they foresee an increased activity towards
inclusion and a more active participation of patients/patients’ groups in
DOH activities in the future.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 38
The DOH respondents recognize the significance of involving patients in
decision-making, in both individual and collective modes. The NCPAM has
initiated efforts to actively seek consultations specifically with
patients/patients’ groups regarding policies and regulations on medicine and
pharmaceutical companies in the Philippines. The NCPAM representative
agrees that patients’ experiences and reasonable preferences on health and
healthcare should be taken into consideration in making decisions that will
affect them. However, there is some trepidation among higher-level
personnel of the Department of Health. Apparently, some higher-level
administrators believe that certain health or healthcare experiences,
especially bad ones, may trigger emotional responses that may cloud the
patients’ judgment. Additionally, they apparently perceive that patients do
not have adequate knowledge and/or skills to follow deliberations of board
or committee meetings and non-familiarity with processes will only delay
planning and formulation of policies, projects, activities, etc.
Understandably, the thrust towards patient engagement will demand for
human resources in terms of additional manpower and supplementing the
knowledge and skills of pre-existing human resources for health. The DOH
respondents, especially representatives from the HHRDB, recognize the
need to train health care workers on patient engagement. They identify the
potential of barangay health workers (BHW) in community-based activities.
Although a common problem is the probable turn-over of BHWs with
every local government elections, they believe that equipping BHWs with
the knowledge and skills to engage patients and families in health may
increase their perceived self-efficacy and the possibility that, because of this
perceived expertise on the matter, they may still be motivated to carry on
such activities even if they will no longer be holding the position.
The DOH DPCP respondent echoed the same belief that patient
engagement in health and healthcare is essential. The respondent believes
that much of the initial work on engaging patients will be community-based
and is actually complementary to their health promotion and disease
prevention activities and signified willingness in taking on the (earlier steps)
in implementing patient engagement in health and healthcare in the
Philippines, should this be effected.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 39
Observations that prioritization of DOH projects may be whimsical was not
countered. Additionally, the observed lack of long-term monitoring and
evaluation of a number of implemented DOH programs and directives,
such as that of patients having representations in hospital boards, was
confirmed. Apparently, programs would be implemented and then left
behind, especially when top-level officials espouse new projects.
PATIENT INTERVIEWS
Demographics
Two focus group discussions were conducted among a total of 10 people
representing different patients’ groups. Separate individual interviews were
conducted in nine respondents. Majority of the respondents were patients
with chronic life-long conditions; two were parents of dependent patients
with chronic life-long conditions. Respondents came from Metro Manila
(City of Manila, Pasay City, Pateros, Caloocan City, Makati City, Quezon
City), Ilocos Norte (Batac City, Pagudpud), Bangued (Abra) and Cagayan de
Oro City. Ages ranged from 35 to 71 years. Educational attainment ranged
from college level (finished second year of college) to postgraduate (master’s
degree).
Focus Group Discussions
The following themes were identified from the focus group discussions with
patients’ groups:
Concepts.
- Patient engagement is thought of as a “fight”.
- Respondents believe patients should not be passive but rather should
be active co-participants in their care.
- It appears that the “engager” at the micro-level is the patient or a
concerned individual (immediate family, close friends).
- Patients are introduced to the patient organizations through informal
networks (health care provider, friends, fellow patients met in the
waiting area prior to clinical consultations). There are no formal
mechanisms to organize and integrate them.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 40
Barriers to patient engagement.
- Some patients lack (essential) knowledge on their condition, on health
care needs, on health services
- Decentralization
• Local Government Units (LGUs) are focused on other
diseases and do not seem to “follow” priorities and policies set
by higher-ups
• Health programs and services are dependent on the whims of
the local/regional chief executives)
• Change in local politicians may mean a change in frontline
health workers (and therefore the training for initial health
workers are put to waste)
- Burdens are on the private partners (in ‘Public-Private Partnerships’
PPP health projects)
- “Doctors as gods” mentality, meaning, whatever doctors say, patients
should follow (classical, paternalistic model of medical care rather
than collaborative or patient/person-centered). This may come from
the doctor themselves or may be the norm among patients.
Perception of DOH-level patient engagement.
- Top-down approach (patients are consulted only in the end when
there are already policies)
- Lack of support from the national level to stimulate patient
engagement at the individual level
The FGD participants were a mixture of people who are aware of, and
people who have not yet heard of the term “patient engagement”. Focusing
on the key word “engagement”, those who were not aware likened “patient
engagement” to “rules of engagement” (defined by NATO as directives to
military forces that define the circumstances, conditions, degree, and
manner in which the use of force, or actions which might be construed as
provocative, may be applied).
All of them agreed that they should “have a say” regarding their condition
and medical care; and, with the emotional upheaval upon learning of their or
their children’s/relatives’ condition and the lack of external resources for
formal support, were stimulated to explore on the conditions on their own.
None of the patients’ organizations to which the respondents belong to

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 41
were established through formal mechanisms: most of the groups were
organized by the patients themselves, who got to know each other in
doctors’ waiting rooms, while some groups were initiated by their
(attending) physicians.
The respondents recognize that, at present, they may be more enlightened
regarding their conditions as compared to the majority of patients in the
Philippines. Recounting the state of affairs before they attained this certain
level of enlightenment, the respondents reported that, then, they felt at a
loss regarding their diagnosis in terms of what it is, what to do, what health
services are needed and where to avail of these. Such lack of knowledge
could translate to dependence on the healthcare providers for medical
decisions. The paternalistic model of care, which is still being actively
practiced especially in rural areas, aggravates this situation further.
With regard to activities in the Department of Health, representatives of the
patients’ groups recount that the DOH does not involve them in the
crafting of policies or in the planning of activities. Rather, the DOH
presents to them the “finished product” and their comments and/or
suggestions are no longer considered. Although policies and directives
towards delivery of patient-centered care exist, the respondents observe that
these are not truly implemented especially in the grassroots level. The
respondents indicated that there seem to be no specific actions of the DOH
towards fostering patient engagement.
Individual patient interviews
The following themes were identified from the individual patient interviews:
Concept - Minimal awareness of patient engagement whether as (1) active caring
for oneself or (2) patient participation in crafting policies and
programs by the government
- Minimal awareness of the possibility of actively participating in one’s
healthcare; paternalistic and classical model of healthcare
- Personal need necessitated involvement in caring for oneself, which
was further catalyzed by family, friends (who have similar conditions)
and attending physicians

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 42
Barriers to patient engagement. - Social and economic factors
- Lack of awareness of how to participate further (beyond caring for
oneself)
- Lack of avenues to participate
Perception of DOH-level patient engagement.
- No activities whatsoever from DOH to engage patients
- Some activities in LGU engage townspeople and sometimes used as
avenue for local health services
The individual patient interviewees showed less awareness of patient
engagement and active participation in one’s health care. Concern and the
concomitant anxiety regarding their condition have prodded some of these
patients to “research” on their diagnosis. Such avenues being utilized for
their “research” include Internet searches, asking physicians or other
healthcare providers (may be their attending physicians, or friends or
relatives in the medical field), and talking with friends or neighbors who
have similar conditions and fellow patients in the doctors’ waiting rooms.
The patient interviewees feel uninformed regarding resources, if any, that
they could tap to enrich the information and education needed for their
condition and the care for their condition. Furthermore, they perceive that
such resources may not be free and would entail additional expenses on
their part.
The respondents are not aware of any specific DOH activities regarding
education and support for their condition and the care for their condition.
The perception of some of the patient respondents outside Metro Manila is
that DOH activities in their communities are mainly immunization
campaigns and care for under-fives, where public healthcare workers go to
their villages for specific immunizations of children and where BHWs
periodically visit households to weigh children less than five years of age.
In some LGUs (such as Batac City), a monthly People’s Day is held where
local government officials hold public consultations. Residents of the city
can declare their concerns, requests, etc., which may not necessarily be
health-related, during the assembly and the LGU officials address these
accordingly.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 43
Recommendations from patients’ groups / patients - Bottom-up approach; gathering of empirical data from grassroots to
know patient needs
- Provision of:
o avenues where patients can relay their
concerns/recommendations;
o feedback to patients from policy makers so patient can feel
that their voices are heard
- Health boards should have (an elected) member who is a patients or
part of a patient group
- Improvement of local health/patient registry
- Institutionalization of individual-centered health care
- Provision of genuine health care that also takes into consideration
issues in health care delivery
- Institutionalization of a “patient-centric” scorecard in hospitals
- Provision of training of health professionals in providing
psychosocial care
- Consideration of financial, spiritual, economic, and political
dimension of a disease
- Information dissemination to patients regarding their diseases
- Patients’ rights pamphlets and information dissemination in local
language
- Creative methods for information dissemination (using mass and
social media, text brigades, seminars while patients are on queue or in
the waiting area)
The respondents in both FGD and individual interviews feel that DOH
policies, directives, programs and activities are being formulated using a
“top-down” approach and thus do not necessarily reflect the true needs of
the populace and do not address the real situation at the front lines.
Respondents, particularly in the FGD, observe the lack of bidirectional
avenues in which patients’ feedbacks (whether these be concerns,
complaints, suggestions or recommendations) are relayed to the “top”
(managers, administrators, policy makers) and that the corresponding
responses and actions of the “top” are relayed back to the patients. These
observations were on the health facilities and the DOH levels. The
respondents feel that a lot needs to be done to improve health care delivery
including information dissemination and health promotion, the practice of

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 44
collaborative care, and recognition of the role of the patient in healthcare
decision-making. The patients suggest taking advantage of technology for
health promotion and patient education. They also demand for a shift of the
purely biomedical care practiced by healthcare workers to consider
psychosocial aspects, and for healthcare workers to listen attentively to and
have two-way communications with patients.
Although this is the initial thrust, the respondents believe that their
involvement in decision-making should not be limited only to self-care.
Patients should also be involved in the decision-making processes in health
and health care in the health services they belong to, in their LGU, and in
the national level. The creation of a patients’ registry could facilitate
communications between patients and the “top”.
NON-PARTICIPATORY OBSERVATION
A patient group in action The Diabetes Association of Pateros (DAOP) was formed through the
efforts of one of the municipal doctors, a diabetes specialist. Diabetes clinics
are held twice a week in one of the Barangay Health Stations of Pateros,
manned by the diabetes specialist and DAOP volunteers. Aside from clinical
consultations with the diabetes specialist, activities include blood glucose
testing, measurement of blood pressure, BMI and waist circumference, and
aerobic exercises. DAOP members, usually officers, actively attend
conferences and symposia for people with diabetes and disseminate lessons
learned during the twice-weekly consultations. People with diabetes from
Pateros pay a minimal membership fee in order to join. Financing is out-of-
pocket, especially as not all diabetes medications are available at the health
center pharmacy. Different pharmaceutical companies provide majority of
the diabetes care materials (diaries, leaflets, glucometers and glucose strips)
used by the group. The group seems to be active internally but is passive in
terms of involvement and participation outside their assemblage.
A Department of Health – retained hospital In the Bataan General Hospital, health promotion and patient education
towards self-management and patient engagement are actively fostered.
Leaflets on different conditions, on healthy lifestyle and smoking cessation
are readily available in strategic areas of the hospital. There is a health

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 45
promotion office manned by a health promotion nurse that offers
counseling to patients. One of the quality objectives of the hospital is “To
improve hospital services through customer’s active participation”.
Local government units The City of Balanga in Bataan province boasts itself as a healthy and smoke-
free local government unit. It has an interactive and responsive government.
The current administration involves its populace: consultative meetings are
the norm and the mayor and his board members hold office in different
barangays to be more accessible to the people. Governance is highly
inclusive and participative; for its smoke-free ordinance, senior citizens have
been given the power to monitor compliance and issue violation tickets in
cases of infringement. Other health-related activities of the city include,
among others: intensive health promotion, primary prevention and healthy
lifestyle advocacy (Balanga City Go4Health), nutrition programs in schools,
organic farming, and anti-alcohol and anti-illicit drugs campaigns.
In Bangued, Abra, a highly paternalistic type of medical care is observed.
Informal interviews revealed that, in a number of cases, particularly among
private practitioners, patients are not involved at all in the clinical
management of their condition. Beyond the provision of the diagnosis,
patients may no longer be given any other information including what
specific medicine they are given, which are dispensed unlabeled either by the
doctors themselves or through connected drugstores, wherein the doctor
writes the prescriptions in code so that only the connected drugstore can
interpret this.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 46
CHAPTER V
DISCUSSION
Similar to most low- and middle-income countries, the Philippines is faced
with the double burden of disease and has among its ranks, health care
workers trained and more accustomed to the delivery of acute and curative-
directed care. The emergence of chronic conditions more than two decades
ago has yet to shift the paradigm in the Philippines.
The “classical model of care” was defined by psychiatrist R.D. Laing (1971)
as a “set of procedures in which all doctors are trained”, the set of
procedures composed of collecting information on the chief complaint and
medical history, doing ancillary and laboratory tests as needed, arriving at a
diagnosis and prescribing treatment and providing the prognosis. It
concentrates on the concept of the disease, the importance of the diagnosis
and the identification of treatment options, which are likely to be successful.
The physician is traditionally viewed as the “expert”, is in an authoritarian
position, and is the dominant healthcare professional; the patient is expected
to “comply” with the physician’s prescription and advice; and the disease is
of major importance while other “external factors” (social, psychological)
may be given less attention. In contrast, a collaborative type of care gives
attention to the psychosocial aspects of the patient (De Ridder et al. 2008)
and involves, enables and engages the patient in caring for the condition
(WHO 1996); and eventually actively involves and engages the patient
towards more responsive health services and policies that reflect and
provide answers and solutions to the actual needs of these people.
In order for patient engagement to be institutionalized within the structures
and systems of the Department of Health, the DOH has to assume the role
of Principal Engager for patient engagement in the public health sector. The
Principal Engager would systematize and promote patient engagement at the
healthcare professional level (patient-doctor relationship/interpersonal
influence), at the healthcare service / healthcare organization level, and at
the community and societal level. As the Principal Engager, the DOH would
be the main mover for the engagers to assist the patient in attaining full
engagement, considering various behavior change theories for each of the
phases of patient engagement.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 47
Strategies that the Principal Engager needs to undertake and that will involve
the different engagers and influencers have to be formulated in order for the
patient to successfully traverse the different phases of engagement: to be
given appropriate information and support for a patient in the blackout phase
to be aroused and to contemplate engagement; to be provided the necessary
knowledge and skills and to stimulate perceived self-efficacy for them to move to
the adhesion phase; and to be given further reinforcements to attain full self-
determination to arrive at and sustain full health engagement status. Upon
attainment of the eudaimonic project phase, patients will then have the
capability of self-determining tailor-made and context-based disease
management and self-care strategies; furthermore, they may make more
meaningful contributions to health care and services.
The different phases of Barello and Graffigna’s (2015) Patient Health
Engagement Model correspond to the different stages of the continuum of
engagement presented in Carman et al.’s (2013) Multidimensional Framework
for Patient and Family Engagement in Health and Health Care, whether at the
individual level, the health organization/health system level, or the
community/societal level. The patient traverses the phases of patient
engagement for each level (Figure 5). It is assumed that before the patient
can make meaningful contributions at the health organization level, s/he, at
the least, has already been empowered and enabled with the knowledge and
skills for self-care and to make informed decisions regarding health care.
Similarly, before the patient can make meaningful contributions at the
policy-making level, the patient has already been activated and is or has been
involved in health organization design and governance.
Figure 5. Phases of patient engagement in the multidimensional engagement continuum

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 48
Thus, patients would undergo all the phases of engagement in each level
(Figure 6), and level-specific strategies have to be formulated to engage
patients, not only for them to accept that the “patient” self is only one of
their possible selves and to make well-informed decisions regarding their
care, but also towards sharing leadership in pertinent health service / health
system activities and in policy-making pursuits. Additionally, it may be
beneficial to initiate engagement even before the level of the patient-health
care provider consultation, either through community-based engagement
activities or wider engagement-dissemination campaigns. These may likewise
supplement and sustain the different levels and phases of engagement. A
level is thus added prior to the stated three levels of patient engagement in
the multidimensional engagement continuum (second row, Figure 6).
Figure 6. The multidimensional patient engagement continuum in the context of the Philippines
THE CONTINUUM In the current state of affairs of public health care in the Philippines, two-
way interactions between the recipients of care and the care providers are
still quite extra-ordinary. Consultations between the patient and provider are
mainly limited to the provision of biomedical care in the classical model; and
patient activation is at its minimum. Consultations between care recipients
and health service officials for health facility organizational design and
governance are usually in the form of patients’ satisfaction surveys done
merely to fulfill accreditation requirements. At policy-level, informative

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 49
rather than consultative meetings have been observed. Involvement and
shared leadership may be seen during consultations in Family Physician-led
health care services. In the Philippines, Family Medicine specialists are
trained in providing biopsychosocial care (Dionisio; Leopando & Olazo).
Involvement was noted in the Bataan General Hospital (organizational
design and governance) as well as in the City of Balanga (policy-making
level).
Consultation, activation and arousal
Activation of patients towards the arousal stage of patient engagement is
initiated in the earlier consultations with health care providers and
educators: whether in the initial visits of community-based health care
workers; in the first meetings with health care providers for specific
complaints or conditions; or in the introduction of patient representatives to
health boards and policy-making bodies. Activating patients, or informing
them regarding their condition and what needs to be done in caring for their
condition, prepares the patients to become better equipped for decision-
making in healthcare. It lays down the foundations of necessary knowledge
and skills towards the care for their condition that may motivate them
towards self-care. Furthermore, it may stimulate the patients’ perceptions of
appropriate health care needs and the corresponding services that patients
should be receiving from health facilities. Activating the patient on their
possible roles and functions as representatives in health boards or policy-
making bodies is the first step for them to be made aware on how to
become involved, and eventually become partners and share leadership in
health and healthcare governance and policy-making.
Activating the patient for self-care Ku and Kegels (2014b) conducted a study among patients with diabetes in a
hospital-based first line health service (the Veterans Memorial Medical
Center in Quezon City) and two local government health units (the RHUs
of Batac City and Pagudpud, Ilocos Norte) to evaluate diabetes knowledge,
attitudes, perceptions, and self-care practices and measure the Patients’
Assessment of Chronic Illness Care (PACIC). The PACIC, a 20-item
questionnaire designed by Glasgow et al. (2005), makes use of a 5-point
Likert scale with 1 (almost never) as the lowest and 5 (almost always) as the
highest rating and asks questions related to different aspects regarding
providing collaborative care: patient activation, delivery system design, goal

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 50
setting, problem solving, and follow-up/coordination. Overall PACIC rating
was low in the hospital-based facility (2.6) and was slightly above the
midpoint for the RHUs (3.2). Table 6 lists the PACIC ratings for Veterans
Memorial Medical Center (VMMC) and for the Batac City and Pagudpud
RHUs.
Table 6. Patients’ Assessment of Chronic Illness Care of people with diabetes consulting at two different
first line health services. (Adapted from Ku & Kegels 2014b).
Patients’ Assessment of Chronic Illness Care
Veterans Memorial Medical Center (n=350)
Batac City and Pagudpud RHUs (n=199)
Median (binomial interpolation of 95% confidence limits) Summary of overall score 2.6 (2.1-3.2) 3.2 (3.1-3.3) Patient activation 2.6 (1.6-3.6) 3.5 (3.4-3.7) Delivery system design 3.3 (2.5-4.0) 3.6 (3.4-3.8) Goal setting 2.6 (2.0-3.2) 3.1 (3.0-3.3) Problem solving 3.0 (2.7-3.2) 3.3 (3.1-3.5) Follow-up/coordination 2.1 (1.8-2.3) 3.0 (2.9-3.2)
The participants from the VMMC, who are being provided family medicine-
based first line health services, had significantly higher knowledge ratings
(mean VMMC=70.7%; mean RHU=58.7%; p<0.001); higher positive
attitudes (mean VMMC=3.7; mean RHU=3.3; p=0.002); and higher
perceived self-efficacy (mean VMMC=3.7; mean RHU=3.2; p<0.001) than
those from the RHUs. Self-care practices in terms of proportions of
participants utilizing health services (mean VMMC=78.8%; mean
RHU=37.0%; p<0.001), adherent to medications (mean VMMC=93.7%;
mean RHU 52.4%; p<0.001) and adherent to exercise (mean
VMMC=66.1%; mean RHU=32.2%; p<0.001) were also better among
those consulting at the VMMC. It appears so that the more knowledgeable
the patients are, the more “critical” they are of the care being provided
them, although the presence of culturally-competent healthcare workers in
the RHUs may also affect the assessment of care being delivered to them.
Interestingly, after arousing/activating the patients from the RHUs in a self-
management education and support project implemented by the same
researchers (Ku & Kegels 2015), statistically significant improvements were
noted in the PACIC ratings and in four of the five PACIC subscales one
year after full implementation (Table 7).

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 51
Table 7. Change in PACIC ratings one year after implementation of the First Line Diabetes Care (FiLDCare) Project in Batac City and Pagudpud (adapted from Ku & Kegels 2015) Patients’ Assessment of Chronic Illness
Care
Pre-implementation (n=164)
Post-implementation (n=164)
Wilcoxon’s signed-rank test p value
Median (binomial interpolation of 95% confidence limits)
Summary of overall score
3.2 (3.0-3.4) 3.5 (3.3-3.6) 0.009
Patient activation 3.3 (3.0-4.0) 3.7 (3.7-4.0) 0.026 Delivery system design
3.7 (3.3-3.7) 3.7 (3.3-4.0) 0.230
Goal setting 3.0 (3.0-3.0) 3.4 (3.2-3.6) 0.017 Problem solving 3.0 (3.0-3.2) 3.5 (3.2-3.8) <0.001 Follow-up/coordination
3.0 (3.0-3.0) 3.2 (3.0-3.6) <0.001
The education and skills development provided through the self-
management education and support activities of the project apparently
increased perceived self-efficacy to arouse and increase adherence of the
people with diabetes who participated. However, as explained by the
qualitative interviews conducted afterwards, the participants deemed that
improvements in the delivery system design were not addressed as the
RHUs were still not able to provide the needed laboratory tests and
medications (Ku & Kegels 2015).
Activating to arouse patients through a combination of direct health care
provider-based and community-based self-management education may be a
good strategy to apply in engaging patients.
Involvement and adherence
After having been activated and aroused, the patient moves from the
dormant listener to a participatory actor whose preferences and
recommendations are considered. In the individual level, this would equate
to a patient already equipped with enough knowledge and skills to adopt and
adhere to proper self-care. These knowledge and skills, complimented with
support and motivation from the external environment (the care providers,
the family, other members of the community) may increase a patient’s
perception of self-efficacy to to do the things needed to be done for their
condition.
In the cross-sectional study by Ku and Kegels (2014a) among people with
diabetes in Quezon City and Ilocos Norte, they were able to demonstrate

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 52
that a higher level of perceived self-efficacy positively contributed towards a
person with diabetes doing the things needed to be done for his/her
condition (i.e., adherence to medications, diet and exercise; foot care;
monitoring; follow-up).
Aside from the demonstrated effectiveness of activating patients towards
the arousal stage of patient engagement, the combination of direct health
care provider-based and community-based self-management education and
support increased perceived self-efficacy. Increasing self-efficacy may
stimulate the patient to progress to the next phase of engagement:
adherence.
With the provision of self-management education and support to patients,
and possibly proper health education and health promotion to other
members of the community, people may already be able to move from the
black-out phase to the arousal phase and, consequently to the adherence
phase and, finally, full patient engagement towards caring for one’s self.
Once patients have reached the adherence phase in caring for one’s self,
they may already be able to make meaningful contributions beyond the
individual and may already be ready to move towards the next level of the
continuum: the health organization. Actively encouraging involvement of
patients in the organizational design and governance of a health facility as
well as in policy-making may ensure that the healthcare environment that
will be created is well suited to the needs of the people. However, patients
will need to be educated on governance and policy-making for them to take
these roles.
Shared leadership and the Eudaimonic project phase
This phase of engagement is not yet evident in the Philippines as is the case
in low- and middle-income countries, and no publications on any local
studies regarding this subject was found even at the individual level. In high-
income countries such as the Netherlands, the United States of America,
Canada and the United Kingdom, involvement of patients as organized
groups in policy-level decision-making has been evident.
As stated by Collins and Moore (2014; Table 3.1, cfr page 23) the patient
plus the health care professional, along with a government-relations

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 53
professional, are the “golden triad” of public policy change. However, it
should be noted that constant and consistent equal participation in public
policy-making (in the neo-corporatist model) may lead these patient groups
to focus too much on professionalization, thereby moving them away from
the people they represent and negatively affecting their democratic potential
(van de Bovenkamp el al 2009; Table 1.2, cfr pp. 17-18).
PROPOSED ACTIVITIES IN THE DIFFERENT LEVELS OF THE ENGAGEMENT CONTINUUM TO PROMOTE AND SUSTAIN PATIENT ENGAGEMENT
Level 0: Initiation of engagement prior to direct care / individual level In the Philippines, routine annual medical examinations are unusual. The
standard practice is that people consult with medical professionals if and
when they feel symptoms. Community-based health promotion and
information dissemination activities may be helpful in activating and
arousing a patient in the blackout phase and recognizing the “I am an ill body”
phase of engagement. These activities may target those who are yet unaware
of any illness and those at risk.
Furthermore, those beyond the blackout phase may also benefit from
community-based activities to support advancement towards and to sustain
full engagement.
Level 0 activities at the local / LGU level
Community-based activities at the local level may be implementation of
local government policies, such as the case of Balanga City. Since the
enactment of the Local Government Code in 1991, the power, responsibility
and the resources for the performance of certain functions have been
transferred from the national to the local governments. This means that the
LGUs are autonomous, independent, and clearly perceived as a separate
level of government over which central authorities exercise little or no direct
control (de Guzman & Reforma, eds., 1993). Thus, Level 0 activities, at
present concentrating more on health promotion and health education
where these are being implemented, are sporadically rather than consistently
observed across all LGUs. The fact that LGUs have corporate status and
have the power to secure resources to perform their function could also
equate to inequity, where LGUs of higher economic status may have more

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 54
resources to expend towards such activities. Political will is likewise a major
determining factor for level 0 activities at the local level; as observed by
some of this study’s respondents, the whims of local government officials
strongly influence activities in the LGU.
The central government, through the DOH, should make attempts to
overcome inequities between LGUs in implementing Level 0 activities. The
DOH has to play an active role in motivating proper implementation and
ensuring continuity of implementation by consistently monitoring and
evaluating LGU Level 0 activities.
LGU Level 0 activities may include activation of the populace through
health promotion and activation of patients through specific health
education including self-management education, and provision of support
and motivation to local health workers to practice the principles of patient
engagement.
Level 0 activities at the DOH (central level)
The Department of Health can support local level 0 activities by producing
health promotion and behavior change materials (informative posters,
leaflets) that can be distributed in the community.
The DOH, through the Health Human Resources Development Bureau
(HHRDB) can provide training for local health care workers particularly
community-based health workers (BHWs), volunteers and “peers” regarding
patient education and support towards engagement. To augment the faculty,
the HHRDB can tap specific professional organizations and medical
specialty societies. Training of local healthcare workers is discussed further
in the succeeding section (Level 1 activities).
Educational and support materials, such as software programs, may be
produced and disseminated by the DOH to the local health care workers.
The Institute of Tropical Medicine in Belgium has interactive software that
was designed for European medics assigned in Africa
(http://www.kabisa.be/). The Kabisa software has educational and support
features: a trainee can learn diagnosing certain tropical conditions through a
certain presenting symptoms; and the software may suggest particular
clinical and/or laboratory tests to perform based on the data provided by

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 55
the user. Although this material is aimed to support physicians in clinical
decision-making, the concept may be used to support health care workers
and health educators in health promotion activities in the community and in
the provision of specific self-management education to patients.
On a wider, more general scale, the DOH, through the Disease Prevention
and Control Bureau (DPCB) can utilize mass and social media to increase
awareness and “advertise” patient engagement, in conjunction with the
health promotion and behavior change materials distributed locally.
According to Internet statistics
(http://www.internetworldstats.com/stats3.htm), there are more than 47
million Internet users and 30 million Facebook users in the Philippines
(43% and 27% respectively, 2015 Philippine population est). Maintaining a
pro-active and interactive Facebook page already has the potential of
reaching out to and contribute towards activating and arousing more than
one third of the Filipino population towards health engagement. On a more
ambitious scale, having and maintaining a website for patients akin to that of
the National Library of Medicine of the United States’ National Institutes of
Health (https://www.nlm.nih.gov/medlineplus/) may mean a wider reach
with more available materials for the populace. In addition to Internet-based
technologies, the use of mobile phones and short messaging systems can
also increase the reach of health promotion and education activities, as has
been demonstrated in a number of studies
(http://jhi.sagepub.com/content/15/1/17.short?rss=1&ssource=mfc). The
possibility of tapping print and broadcast media should likewise be explored.
Utilizing certain local artists and actors/actresses for health promotion
activities should be considered. For example, the phenomenon that is of Eat
Bulaga’s Kalye Serye (the main characters of which have been featured in the
2015 holiday issue of Readers’ Digest) may also be used to transmit good
health practices, aside from the good Christian values it promotes
(http://www.cbcpnews.com/cbcpnews/?p=65552). The use of mass and
social media should not be discounted. Studies have shown the considerable
degree of influence that these means of promotion and information
dissemination can have (Stern 2015). As was cited in the literature review,
involvement of patients in the preparation of the contents of the web
page/site, the text messages and print and broadcast media promotions is
recommended as this may equate to higher effectiveness.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 56
Level 1: Direct patient care / individual level The classical, paternalistic, purely biomedical care model that is still widely
practiced in the Philippines needs to be replaced with a model of care that
considers psychosocial aspects and involves patients in decision-making, and
eventually to equal participation and leadership. The Philippine Academy of
Family Physicians requires its members to have adequate training in the
biopsychosocial approach and conducts periodic training on active listening
skills and the biopsychosocial approach to its members, and to interested
general practitioners and rural physicians nationwide. However, training of
physicians alone will not suffice. A physician, particularly government
physicians who see between 50-100 patients per day in addition to attending
to administrative duties, may not have enough time to provide education
and counseling to patients. Redistribution of standardizable tasks may be
considered, especially in public health facilities. Training of other health care
workers (nurses, midwives, pharmacists, medical technologists), community-
based health workers as well as the creation of peer educators (people who
have certain conditions and deemed “experts” of their condition) may play a
large role in the activation of patients towards adherence, and in supporting
these patients towards the full engagement phase. As was mentioned in the
preceding section, the DOH can tap professional organizations and medical
specialty societies to augment the faculty. Additionally, the DOH can
establish training of trainers modules, identifying and providing intensive
training to regional, provincial and local trainers who can then disseminate
learnings in these levels and who can perform supportive supervision to the
health care workers.
A First Line Care Team composed of pre-existing formal and informal
healthcare workers (including volunteers and “peers”) may be created to
organize provision of self-care education and activate and support the
patient towards full engagement. Simply, this could be composed of the
rural health unit staff, with the doctor and/or the nurse providing the initial
education and activation and the midwives and barangay health
workers/volunteers/peers providing support. A framework delineating
possible tasks for each cadre may be prepared, together with algorithms of
the standardizable tasks for the less skilled members of the team. The
interactive software mimicking the principles of Kabisa may also be designed
to contain education and support materials for Level 1 activities.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 57
Training of the local formal and informal health care workers should thus
encompass community-based as well as direct patient-care based provision
of health promotion and education (Level 0 and Level 1 activities).
Level 2: Organizational design and governance level Akin to the Bataan General Hospital’s quality objective of patient
participation in the improvement of its health services, all hospitals should
be enjoined to practice a truly participatory type of governance, and not just
be required to submit regular reports on client satisfaction.
The inclusion of the “expert” or “fully-engaged patients” in organizational
governance may equate to some re-design of the health facility organization:
for example, patients may co-lead in hospital safety and quality
improvement activities as delineated in Figure 6; or may have seats in the
hospital board.
Inasmuch as the DOH is in the process of establishing a scorecard for its
retained hospitals, a patient-centric scorecard may be implemented. Such
patient-centered scorecards may likewise be implemented as part of DOH-
accreditation process(es) of any health facility with direct patient contact to
enforce implementation of patient engagement in general and participation
of patients, who should be at the least in the adherence phase of
engagement, in governance in particular. Patients in the latter phases of
engagement would have more expertise regarding their condition and the
care for their condition, and thus concerns on their credibility as a source of
knowledge regarding their condition may no longer be raised. However,
additional information on technical terms used may still need to be provided
(Boivin et al., 2014;Table 5.5, cfr pp. 33-34).
Level 3: Policy-making level Local Level
Coordination with and cooperation of local government units (LGU) for
involvement and shared decision-making with pertinent patients/patients’
groups need to be sought. Pro-active, participatory and health-oriented
LGUs, such as the City of Balanga, may be highlighted and endorsed
(through recognition, awards) for these to be emulated. Local level policy-
making that involves the community should be encouraged.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 58
National Level
National policies should be crafted based on evidence garnered from the
grassroots level; whether in the form of evidence-generating research or
participation of the people who will be primarily affected by the said
policies. Research may even be conducted by the patients themselves: as
demonstrated in the Netherlands, the Dutch neuromuscular organization
produced a synthesis of needs and preferences, which includes in some
cases even producing full-blown consultations, reports and figures to
communicate their needs in relation to biomedical innovations (Boon and
Broekgaarden 2009; Table 4.3, cfr pp.26-27). Additionally, as Bridges and
Jones (2007; Table 4.6, cfr p.29) have observed, a patient-based Health
Technology Assessment (HTA) can promote the antecedents of
empowerment by both informing patients about medicine and informing
medicine about patients. Such patient-generated research or evidence
gathered from patients should however be monitored for true
representativeness.
The previously mentioned “golden triad” can be utilized in policy
formulation, but safeguards must be in place to protect the patient
organizations from focusing on too much professionalization.
Additionally, safeguards should also be in place so that patients/patients’
organization may not be unduly influenced by stakeholders who may have
conflicting (financial) interests in upcoming policies and decisions where
patients are actively participating in. Patients/patients’ groups who are
involved in governance and policy-making may be approached by lobbyists
and sway them to their favor. The presence of pharmaceutical companies in
certain patients’ groups’ activities may be within the scope of their
“corporate social responsibility”, but their products are printed in the
materials that are distributed and the group members know the
pharmaceutical companies’ representatives and the companies they
represent. The patients involved in governance and policy-making thus may
consider that they owe pharmaceutical companies, which provide materials
and support to their activities, and may, in return, patronize the said
companies when making decisions.
In high-income countries, declarations of conflict(s) of interest are required
for people participating in said policy-or decision-making activities.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 59
However, such may not suffice in the Philippines. The value of the
contributions of pharmaceutical companies to patients’ groups is
recognized. However, it would be more preferable if the materials they
provide were de-identified. Furthermore, it would be more preferable that a
(central) distribution arm would collect materials from the pharmaceutical
companies and give these to the patients’ groups. This distributor thus
anonymizes the pharmaceutical companies and bars the possible links that
could be forged between the pharmaceutical companies and the patients’
groups. Such could also be a function of the DOH office, which will
undertake patient engagement.
MONITORING AND EVALUATION
Output and outcome measures Initial monitoring of patient engagement institutionalization may concern
intermediate (output and outcome) results of patient engagement, as
indicated in the level-based activities, i.e., number of healthcare workers
trained on patient engagement, number of health facilities implementing
patient engagement.
Impact on universal access Inasmuch as institutionalization of patient engagement aims to achieve the
goals set forth in UHC, the long-term indicator of the effectiveness of
institutionalization of patient engagement would be universal access to
health care. Effects of patient engagement on access to health care may be
evaluated making use of the framework proposed by Levesque et al. (2013)
(Figure 7) on patient-centered access to healthcare.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 60
Figure 7. Framework for patient-centered access to healthcare (Levesque et al. 2013)
In this framework, Levesque (2013) proposes that access is an interface
between the characteristics of persons, households, social and physical
environments and the characteristics of health systems, organizations and
providers. Thus there are provider-related factors (uppermost boxes),
process factors in which access is realized (boxes on arrow), and user-related
factors (lowermost boxes). Access is thus viewed as (1) the possibility to
identify healthcare needs, corresponding to the arousal phase of patient
engagement; (2) the possibility to seek and use healthcare services and reach
and obtain healthcare resources (corresponding to user-related factors boxes
2-4) and which may contribute towards a person achieving the adherence
phase of engagement; and (3) to be actually offered services appropriate to
the needs for care, which may influence full engagement. Correspondingly,
providers of care should have the following characteristics: (1)
approachability; (2) acceptability; (3) availability and accommodation; (4)
affordability; and (5) appropriateness. The process factors may also be used
as intermediate indicators.
However, the feasibility of using Levesque et al.’s framework as the
framework for monitoring and evaluation of effectiveness of patient
engagement in the Philippines needs to be explored. Furthermore, the
specific indicators for the process factors (perception of needs and desire
for healthcare, healthcare seeking, healthcare reaching and utilization, and

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 61
healthcare consequences) need to be studied if these are truly representative
in terms of universal access to health care in the Philippines.
Patients’ satisfaction surveys could be modified to measure patient-
dependent health care consequences (satisfaction, economic) and include
some elements of Glasgow’s PACIC, which could monitor patient
activation and provision of collaborative care in health facilities. Inclusion of
patient engagement measures in the patients’ satisfaction survey may also be
convenient for the health facilities in terms of collection and analysis.
Additionally, improvements in the current handling of patient satisfaction
surveys with regard to reporting and feedback have to be made. These
improvements may already have been addressed in the recently concluded
Client Satisfaction Study commissioned by the Health Facility Development
Bureau (HFDB) of the DOH through the Philippine Council for Health
Research and Development, where encoding of results was programmed to
be done electronically and results are transmitted to the DOH in real time.
Other measures, such as evaluating improvements in knowledge and skills
of patients can be utilized but could be resource-intensive.
Health care consequences on health may be measured individually through
clinical endpoints, and collectively through mortality and morbidity reports.
In high-income countries such as the United Kingdom where health
information systems have long been in place, the National Health Service
can monitor individual clinical endpoints such as laboratory results of
patients with chronic conditions to evaluate the performance of health
services. The DOH health information systems installed in the DOH-
retained hospitals has the capability of doing such. However, inasmuch as
not all electronic files are transmitted to the DOH, monitoring and
evaluation through clinical endpoints especially those based on laboratory
results may not be possible at the central level but only at the level of the
hospital.
Whether monitoring is done in the hospital or in the central level, human
resources dedicated to this activity are needed. In doing so, follow-up of
issues needing feedback to both the patients and the facilities involved, in
whatever circumstance (for example, handling of non-conformance or
extending recognition and praise), can be done without undue delay.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 62
QUO VADIS, DOH? With the suggested level-specific activities mentioned above to accompany
patients in their journey through the different phases of engagement and
possible monitoring and evaluation measures, where does the DOH start as
the principal engager? The logical first step would be for patient-specific
activities to be organized in a single unit in the DOH.
The “Patient Affairs Unit”
Vision and Missions It is envisioned that in the Philippines, patients and families will be fully
engaged in health care. The primary objective of the “Patient Affairs Unit”
would be to champion and safeguard patients by advancing patient and
family engagement in health care in the Philippines. This aim is envisioned
to be achieved by:
1. Promoting patient-centered care and shared decision-making
2. Fostering patient education, empowerment and enablement
3. Encouraging partnerships and shared leadership between patients,
health care providers, health care facility boards, and health policy
makers
Functions Functions of the “Patient Affairs Unit” would include but not limited to:
1. Coordination of all activities on patient engagement, such as
a. Patient engagement-related training of healthcare workers (in
cooperation with HHRDB)
b. Monitoring and evaluation of patient engagement activities in
all levels (in cooperation with HFDB, BHFS)
c. Enforcement of patient engagement activities in all levels in
coordination with pertinent DOH accreditation bodies.
d. Production of health promotion and education materials
2. Accreditation of patient organizations
3. Maintenance of a patient and patient organization registry
4. Central processing unit for patients’ feedbacks, whether positive or
negative
5. Reference center for recruitment of patients/patient organizations in
research, HTA, policy-making activities of the DOH
6. Monitoring of patient engagement in research, HTA, policy-making
activities of the DOH

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 63
7. Production and distribution of patient engagement materials for care
providers as well as for patients
8. Distribution of de-identified/anonymized pharmaceutical companies-
produced patient engagement materials and other patient care
materials to patients/patients’ groups
Staff Complement Ideally, this “Patient Affairs Unit” should be an independent/separate office
in the DOH. The fully working Unit where patient engagement activities
would already be completely developed and implemented would be
expected to have a minimum composition of the following key personnel
with their respective expected minimum duties and responsibilities:
1. Unit Chief
a. Oversees the day-to-day operations of the Unit
b. Reports to the Secretary of Health regarding activities of the
Unit
2. Monitoring and Evaluation Officer
a. Receives reports of the liaison officers (specific activity reports,
reports of client satisfaction surveys, reports of health
outcomes, and reports of patients’ feedbacks)
b. Collates and analyses reports
c. Make the necessary recommendations and appropriate actions,
including feedbacks to patients, DOH offices, LGUs and
health facilities based on report results
3. Liaison Officer, DOH (Internal)
a. Collaborates and coordinates with other DOH offices for Unit
functions where other DOH offices are involved
b. Monitoring and evaluation of the Unit’s activities where other
DOH offices are involved
c. Collaborates and coordinates with DOH-retained hospitals
d. Monitors and evaluates patient engagement activities in DOH-
retained hospitals
e. Monitors and evaluates client satisfaction survey results of
DOH-retained hospitals
f. Monitors and evaluates clinical endpoints, mortality and
morbidity reports of DOH-retained hospitals
4. Liaison Officer, Patients
a. Registry officer for patients’ groups

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 64
b. Coordinates with patients/patients’ groups
c. Monitors and evaluates levels of “involvement” and “partnership
and shared leadership” of patients/patients’ groups in research,
HTA and policy-making activities of the DOH
d. Receives feedbacks from patients/patients’ groups
e. Distribute materials to patients/patients’ groups (cfr functions
7 and 8,p. 63)
5. Liaison Officers, LGUs
a. Coordinate and collaborate with LGUs for community-based
and direct healthcare provider-based patient engagement
activities
b. Monitors and evaluates patient engagement activities in the
community and rural health unit/local government health units
c. Monitors and evaluates client satisfaction survey results of
local government health units
d. Monitors and evaluates clinical endpoints, mortality and
morbidity reports of local government health units
6. Liaison Officers, public hospitals
a. Coordinate and collaborate with public hospitals for patient
engagement activities
b. Monitors and evaluates patient engagement activities in public
hospitals
c. Monitors and evaluates client satisfaction survey results of
public hospitals
d. Monitors and evaluates clinical endpoints, mortality and
morbidity reports of public hospitals
7. Liaison Officers, private hospitals
a. Coordinate and collaborate with private hospitals for patient
engagement activities
b. Monitors and evaluates patient engagement activities in private
hospitals
c. Monitors and evaluates client satisfaction survey results of
private hospitals
d. Monitors and evaluates clinical endpoints, mortality and
morbidity reports of private hospitals
8. Information Technology and Media Officer
a. Maintains website/social media page(s) of the unit
b. Manages print and broadcast media activities of the Unit

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 65
c. Maintains telecommunications-based patient education and
support activities of the Unit
d. Manages and maintains software-based educational materials
of the Unit
e. Monitors and evaluates activities in social media page(s)
f. Monitors and evaluates print and broadcast media activities
g. Monitors telecommunications-based patient education and
support activities
h. Monitors and evaluates production and usage of software-
based educational materials
A roadmap for operationalization The following strategies are recommended to be implemented so that the
mandate of patient and family engagement in health care in the Philippines
is realized:
1. Education, empowerment and enablement of patients and their families
to be engaged in healthcare
2. Preparation of direct care providers and health facility administrators for
patient engagement in healthcare
3. Creation of the First Line Care Team
4. Monitoring and evaluation (including transparency and accountability)
5. Legislation and regulation
6. Partnership in health facility governance
7. Partnership in public policy (including research/production of evidence
for policy and HTA)
Early stages of implementation Although “units” do not necessarily require legislation for these to be
established in government agencies in the Philippines, the need for full-time
staff may be. However, a fully working “Patient Affairs Unit” is not a requisite
in the earlier stages of implementing patient and family engagement in the
Philippines. Priorities at this point would be: (1) education, empowerment
and enablement of patients and their families to be engaged in healthcare;
(2) preparation of direct care providers and health facility administrators for
patient engagement in healthcare together with (3) creation of the First Line
Care Team; (4) initial monitoring and evaluation, and making results
available for transparency and accountability; and (5) advocacy for
regulatory and legislative changes to establish patient and family engagement
in the Philippines.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 66
However, the fifth strategy is not solely for the DOH to undertake. The
DOH may put forth regulatory changes that, for example, will (a) require
patient and family engagement competencies for certification and
accreditation of health facilities and (b) provide incentives and penalties for
involving/not involving patients and families in organizational governance.
However, advocacy for legislative changes would be better forwarded with
patients/patients’ groups and their supporters (including MeTA) at the
forefront. Such legislation may include (a) provision of recognition and
rewards (such as PhilHealth reimbursements) for care that fully incorporate
patient and family engagement, (b) multi-sectoral support for patient and
family engagement activities, (c) provision for involvement and shared
leadership of patients/patients’ groups in public policy-making bodies, (d)
inclusion of patient engagement competencies education and training in
curricula of medical courses, (e) requiring patient and family engagement
competencies for board certification of medical and paramedical
professions, (f) inclusion of health promotion and activation towards
engagement in health and healthcare in elementary and high school
curricula, etc.
Although strategies 6 and 7 (partnerships in health facility governance and
policy-making) are not prioritized, these may also be implemented at this
stage, as there are already fully engaged patients/patients’ groups who have
the capacity to be involved and to become partners in governance and
policy making.
Patient and Provider Preparation
Much of the education, empowerment and enablement of patients and
families is foreseen to take place in the communities and during clinical
consultations with their healthcare providers. Inasmuch as this is so, patient
engagement activities of the DOH at this point may be performed by the
Disease Prevention and Control Bureau (DPCB) in coordination with
HHRDB, Bureau of Health Facilities and Services (BHFS) and HFDB.
Duties and responsibilities of DPCB 1. Coordinate and collaborate with HHRDB, BHFS and HFDB for
initial patient engagement activities.
2. Coordinate with LGUs.
3. Implement (agreed upon) patient engagement activities.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 67
4. Raise awareness of patient engagement through nationwide blitzes
and public announcements in broadcast and print media.
5. Create condition-specific educational materials (posters, leaflets) to
inform and educate patients and their families, translating medical
information (and medical jargon) to plain language and in dialects.
6. Maintain a website and/or social media page(s) where patients can
find materials on health and healthcare, including the condition-
specific educational materials above and can interact with the DOH.
7. Monitor and evaluate implemented patient engagement activities.
8. Make monitoring and evaluation results available for transparency
and accountability.
9. In coordination with HFDB, introduce measures of patient
engagement in the DOH Client Satisfaction Survey.
10. In coordination with HHRDB, (and possibly with medical specialty
societies), create a Patient Engagement education module for
healthcare workers and a Patient engagement education module for
patients and their families.
Duties and Responsibilities of HHRDB 1. Create and conduct training workshops for trainers of formal and
informal direct health care providers (physicians, nurses, midwives,
pharmacists, dentists, medical technologists, barangay health workers,
peer educators) on patient-centered care, self-management education
and support provision, shared decision-making, and the
biopsychosocial approach as delivered by a multidisciplinary team;
and on possible community resources (such as the Department of
Social Welfare and Development, possible existing patients’ groups,
community-based organizations) to facilitate partnerships outside of
the health facility to which the patients may be referred to for (self-
care) support (based on the contents of the Patient Engagement
education module for healthcare workers).
2. Knowledge management and preparation of educational and
decision-support materials (paper-based and/or interactive or non-
interactive software) that can be used by trainers for knowledge
transfer.
3. Monitor and evaluate effects of training (change in knowledge on
Patient Engagement; number of care providers trained; number of

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 68
care providers educating patients and families on patient engagement;
number of care providers practicing patient engagement)
Duties and Responsibilities of BHFS, HFDB
1. Coordinate and collaborate with respective health facilities for
training of care providers on patient engagement
2. Monitor and evaluate (initial) indicators* for patient engagement in
respective health facilities.
*initially could be (1) number of patients (and families) being
provided with education (based on the Patient Engagement education
module for patients and families) and (2) outcomes of the revised
Client Satisfaction Survey; eventually to include Levesque’s factors
(where applicable) and health outcomes.
Full implementation Eventually, after the activities on preparing the patient and the care
providers have been implemented, it is expected that a number patients will
move to the latter phases of Barello and Graffigna’s Patient Engagement
framework. At that point, the “Patient Affairs Unit” may have become fully
operational and some legislation may have been passed. Inasmuch as the
number of patients who are ready to be involved in governance will already
increase, full implementation of strategies 6 and 7 (partnership with health
facilities and eventually partnership in public policy) including monitoring
and evaluation of implementation of these strategies will be in order. The
education, empowerment and enablement of patients and their families to
be engaged in healthcare and preparation of direct care providers and health
facility administrators for patient engagement in healthcare activities will still
be continued. Monitoring and evaluation will be expanded to include other
outcomes and impacts of the patient engagement activities. Transparency
should be maintained.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 69
CHAPTER VI CONCLUSIONS & WAYS FORWARD
Engaging patients in their health care and within the structures and systems
of the Department of Health involves a number of phases and different
levels that the patient needs to undergo. Being the national agency for
health, the DOH shall act as the principal engager. This will entail assisting
and supporting the journey of a patient through the phases of black out;
arousal and activation regarding their condition; involvement in and
adherence to plans in maintaining their own health, and involvement as
advisers in health services design and governance, and policy-making; and
finally to full engagement status where the patient makes decisions in
partnership with the health care provider, the health service managers, and
the policy-makers. Initiating changes in the different levels of the continuum
and implementing interventions to progress through the different phases of
patient engagement is complex, and will involve numerous sectors and
actors who may have conflicting interests. The DOH must be prepared to
undertake such arduous task and should have mechanisms in place to
implement, monitor and ensure sustainability of the different patient-
engagement activities, at the same time putting safeguards in place to ensure
that the outputs of patient engagement activities reflect the needs of the
patients.
In this early stage, patients in the (near) full engagement status should
already be sought and be involved for patient engagement implementation:
be it in the planning of the different activities, the crafting of promotional
and behavior change materials, or the construction of initial policies for
patient engagement.
The DOH should take advantage of the impending implementation of the
scorecard and modify this into a patient-centric scorecard to stress the need
to deliver patient- and person-centered care and engage patients in the
organizational design and governance of health facilities.
Due to healthcare devolution, cooperation and coordination of local
government units should be sought and maintained. Encouragement of and
recognition of LGUs who advocate participatory governance may motivate

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 70
collaboration. In this way, patient engagement may be fully implemented in
the local government health units and in the communities.
Aside from creating a cadre of “peer educators” to activate co-patients, the
possibility of stimulating fully engaged patients as future engagers should
not be discounted; this could augment sustainability of patient engagement
in the Philippines.
Involvement of other sectors to support patient engagement is essential.
Possible contributions of LGUs, healthcare facilities, medical (specialty)
societies, and mass media have been identified. Other government agencies
such as the Department of Social Welfare and Development and the
Department of Education as well as the private sector can also play active
roles in patient and family engagement.
Advocacy for regulatory and legislative changes to establish patient and
family engagement in the Philippines should be prioritized; and vigilance
regarding full implementation and continuity of patient engagement
activities should be maintained.
The full effects of patient engagement on access to healthcare may only be
realized years after its implementation. However, intermediate and process
indicators may be able to indicate positive (or negative) results of
implementation.

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 71
REFERENCES
Adams SA, Van de Bovenkamp H, Robben P. Including citizens in
institutional reviews: expectations and experiences from the Dutch
Healthcare Inspectorate. Health Expect. 2013 Sep 24. doi:
10.1111/hex.12126. [Epub ahead of print] PMID: 24112128
[PubMed - as supplied by publisher]
Baker A. Patient involvement in a professional body: reflections and
commentary. J Health Organ Manag. 2007;21(4-5):460-9. PMID:
17933376 [PubMed - indexed for MEDLINE]
Bandura A. Self-efficacy: toward a unifying theory of behavior change.
Psychol Rev 1977;84:191-295.
Bandura A. Social cognitive theory. In R. Vasta (ed) Annals of child
development Vol. 6. Six theories of child development.
Greenwich,CT: JAI Press, 1989;1-60.
Barello S, Graffigna G 2015. Patient engagement in healthcare: pathways for
effective medical decision-making. Neuropsychological Trends 17.
Available from:
http://www.ledonline.it/NeuropsychologicalTrends/allegati/Neurop
sychologicalTrends_17_Barello.pdf
Barello S, Vegni E, Bosio AC 2014. The challenges of conceptualizing
patient engagement in healthcare: a lexicographic literature review. J
Participativ Med 6: e9.
Beresford P. User involvement, research and health inequalities: developing
new directions. Health Soc Care Community. 2007 Jul;15(4):306-12.
PMID: 17578391 [PubMed - indexed for MEDLINE]
Boivin A, Lehoux P, Burgers J, Grol R. What are the key ingredients for
effective public involvement in health careimprovement and policy
decisions? A randomized trial process evaluation. Milbank Q. 2014
Jun;92(2):319-50. doi: 10.1111/1468-0009.12060. PMCID:
PMC4089374 PMID: 24890250 [PubMed - indexed for MEDLINE]
Bridges JF, Jones C. Patient-based health technology assessment: a vision of
the future. Int J Technol Assess Health Care. 2007 Winter;23(1):30-5.
PMID: 17234014 [PubMed - indexed for MEDLINE]

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 72
Carman KL, Dardess P, Maurer M, Sofaer S, Adams K, Bechtel C, Sweeney
J 2013. Patient and family engagement: a framework for
understanding the elements and developing interventions and
policies. Health Affairs 32(2):223-31.
Chew-Graham C. Encouraging patient and public involvement in HEX.
Health Expect. 2014 Dec;17(6):753-4. doi: 10.1111/hex.12293.
PMID: 25345379 [PubMed - indexed for MEDLINE]
Collins CW, Moore NS. Engaging patients in public policy advocacy. Ann
Am Thorac Soc. 2014 Feb;11(2):260-3. doi:
10.1513/AnnalsATS.201311-398AR. PMID: 24575996 [PubMed -
indexed for MEDLINE]
Congress: changing the policy landscape: haemophilia patient involvement
in healthcare decision-making. Eur J Haematol Suppl. 2014
Jun;(74):1-8. doi: 10.1111/ejh.12316. PMID: 24801295 [PubMed -
indexed for MEDLINE]
De Ridder D, Geenen R, Kuijer R, van Middendoerp H 2008. Psychological
adjustments to chronic disease. Lancet 372: 246-255.
Delamater AM 2006. Improving patient adherence. Clinical Diabetes 24:71-7.
Gerber B, Stolley M, Thompson A, Sharp L, Fitzgibbon M, Mobile phone
text messaging to promote healthy behaviors and weight loss
maintenance: a feasibility study,
doi: 10.1177/1460458208099865Health Informatics Journal March
2009vol. 15 no. 1 17-25
Glasgow RE, Whitesides H, Nelson CC, King DK 2005. Use of the Patient
Assessment of Chronic Illness Care (PACIC) with diabetic patients.
Diabetes Care 28:2655-2661.
Graffigna G, Barello S, Wiederhold BK, Bosio AC, Riva G 2013. Positive
technology as a driver for health engagement. Studies in Health
Technology and Informatics 191:9-17.
Hogg CN. Patient and public involvement: what next for the NHS? Health
Expect. 2007 Jun;10(2):129-38. PMID: 17524006 [PubMed - indexed
for MEDLINE]

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 73
Holzer JK, Ellis L, Merritt MW. Why we need community engagement in
medical research. J Investig Med. 2014 Aug;62:851-5. doi:
10.1097/JIM.0000000000000097. PMCID: PMC4108547 [Available
on 2015-08-01] PMID: 24979468 [PubMed - indexed for
MEDLINE]
Horowitz CR, Goldfinger JZ, Muller SE, Pulichino RS, Vance TL, Arniella
G,Lancaster KJ. A model for using community-based participatory
research to address the diabetes epidemic in East Harlem. Mt Sinai J
Med. 2008 Jan-Feb;75(1):13-21. doi: 10.1002/msj.20017. PMCID:
PMC3236081 PMID: 18306238 [PubMed - indexed for MEDLINE]
Hubbard G, Kidd L, Donaghy E, McDonald C, Kearney N. A review of
literature about involving people affected by cancer in research, policy
and planning and practice. Patient Educ Couns. 2007 Jan;65(1):21-33.
Epub 2006 Jul 24. PMID: 16860517 [PubMed - indexed for
MEDLINE]
Hubbard G, Kidd L, Donaghy E.Involving people affected by cancer in
research: a review of literature. Eur J Cancer Care (Engl). 2008
May;17(3):233-44. doi: 10.1111/j.1365-2354.2007.00842.x. PMID:
18419626 [PubMed - indexed for MEDLINE]
Hui A, Stickley T. Mental health policy and mental health service user
perspectives on involvement: a discourse analysis. J Adv Nurs. 2007
Aug;59(4):416-26. PMID: 17635301 [PubMed - indexed for
MEDLINE]
Jin W, Irene H, Stan K, A review of the use of mobile phone text messaging
in clinical and healthy behaviour interventions. April 27, 2015,
doi:10.1177/1460458215577995. Health Informatics Journal April 27,
2015
Katherine E.S, Stephanie K.G, Ashley M.L, Lauren A.M., Recruitment and
retention in an SMS-based health education program: Lessons learned
from Text2BHealthy, doi: 10.1258/jtt.2010.100322J Telemed
Telecare January 2011 vol. 17 no. 1 41-48 Kelly L, Caldwell K, Henshaw L. Involving users in service planning: a focus
group approach. Eur J Oncol Nurs. 2006 Sep;10(4):283-93. Epub
2006 Apr 4. PMID: 16600685 [PubMed - indexed for MEDLINE]

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 74
Ku GMV, Kegels G 2014a. Knowledge, attitudes and perceptions of people
with type 2 diabetes as related toself-management practices: Results
of a cross-sectional study conducted in Luzon, Philippines. Chronic
Illness. Available from:
http://chi.sagepub.com/content/early/2014/06/04/1742395314538
291
Ku GMV, Kegels G 2014b. A cross-sectional study of the differences in
diabetes knowledge, attitudes, perceptions and self-care practices as
related to assessment of chronic illness care among people with
diabetes consulting in a family physician-led hospital-based first line
health service and local government health unit-based health centers
in the Philippines. Asia-Pacific Journal of Family Medicine 2014 13:14.
doi:10.1186/s12930-014-0014-z December 2014.
Ku GMV, Kegels G 2015. Implementing elements of a context-adapted
chronic care model to improve diabetes care: effects on assessment of
chronic illness care and glycaemic control among people with diabetes
enrolled to the First Line Diabetes Care (FiLDCare) Project in the
Northern Philippines. Primary Health Care Research & Development. Doi:
10.1017/S1463423614000553 First view 20 January 2015.
Laurance J, Henderson S, Howitt PJ, Matar M, Al Kuwari H, Edgman-
Levitan S, Darzi A. Patient engagement: four case studies that
highlight the potential for improvedhealth outcomes and reduced
costs. ). Health Aff (Millwood). 2014 Sep;33(9):1627-34. doi:
10.1377/hlthaff.2014.0375. PMID: 25201668 [PubMed - in process]
Levesque JF, Harris MF, Russel G 2013. Patient-centred access to health
care: conceptualizing acces at the interface of health systems and
populations. International Journal for Equity in Health 12:18. Available
from: http://www.equityhealthj.com/content/12/1/18
Lopes E, Street J, Carter D, Merlin T. Involving patients in health
technology funding decisions: stakeholder perspectives on processes
used in Australia. Health Expect. 2015 Feb 21. doi:
10.1111/hex.12356. [Epub ahead of print] PMID: 25703958
[PubMed - as supplied by publisher]

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 75
McNichol E. Involving patients with leg ulcers in developing innovations in
treatment and management strategies. Br J Community Nurs. 2014
Sep;Suppl:S27-8, S30-2. doi: 10.12968/bjcn.2014.19.Sup9.S27. PMID:
25192559 [PubMed - indexed for MEDLINE]
Medicines Transparency Alliance (MeTA) Philippines and the World Health
Organization (WHO) 2014. Stakeholder Mapping and Development
of a Framework for the Engagement and Empowerment of Patient
Organizations in the Philippines. (Unpublished).
Ng CJ, Lee PY, Lee YK, Chew BH, Engkasan JP, Irmi ZI, Hanafi NS, Tong
SF. An overview of patient involvement in healthcare decision-
making: a situational analysis of the Malaysian context. BMC Health
Serv Res. 2013 Oct 11;13:408. doi: 10.1186/1472-6963-13-408.
PMCID: PMC3852442 PMID: 24119237 [PubMed - indexed for
MEDLINE]
O'Mahony B, Kent A, Aymé S. Pfizer-sponsored satellite symposium at the
European Haemophilia Consortium (EHC)
Patel N, Rajasingam D. User engagement in the delivery and design of
maternity services. Best Pract Res Clin Obstet Gynaecol. 2013
Aug;27(4):597-608. doi: 10.1016/j.bpobgyn.2013.04.006. Epub 2013
Jun 12. PMID: 23768954 [PubMed - indexed for MEDLINE]
Ryan RM, Patrick H, Deci EL, Williams GC 2008. Facilitating health
behavior change and its maintenance: Interventions based on the
Self-Determination Theory. European Health Psychologist 10:2-5.
Shippee ND, Domecq Garces JP, Prutsky Lopez GJ, Wang Z, Elraiyah TA,
Nabhan M, Brito JP, Boehmer K, Hasan R, Firwana B, Erwin PJ,
Montori VM, Murad MH. Patient and service user engagement in
research: a systematic review and synthesized framework. Health
Expect. 2013 Jun 3. doi: 10.1111/hex.12090. [Epub ahead of print]
PMID: 23731468 [PubMed - as supplied by publisher]
Stern RJ 2015. Mass media campaigns to prevent chronic diseases –
powerful but underused tool. JAMA Intern Med. Published online 21
September 2015. Doi:10.1001/jamainternmed2015.5546

Ku, Dalmacion, Baja. Institutionalization of Patient Engagement 76
Thomson R, Murtagh M, Khaw FM. Tensions in public health policy:
patient engagement, evidence-based public health and health
inequalities. Qual Saf Health Care. 2005 Dec;14(6):398-400. PMCID:
PMC1744099 PMID: 16326781 [PubMed - indexed for MEDLINE]
Tomes N. The patient as a policy factor: a historical case study of the
consumer/survivor movement in mental health. Health Aff
(Millwood). 2006 May-Jun;25(3):720-9. PMID: 16684736 [PubMed -
indexed for MEDLINE]
Tritter JQ, Koivusalo M. Undermining patient and public engagement and
limiting its impact: the consequences of the Health and Social Care
Act 2012 on collective patient and public involvement. Health
Expect. 2013 Jun;16(2):115-8. doi: 10.1111/hex.12069. PMID:
23650917 [PubMed - indexed for MEDLINE]
Wagner, EH. Chronic disease management: what will it take to improve care
for chronic illness? Eff Clin Pract 1998;1(1): 2-4.
Williamson L. Patient and citizen participation in health: the need for
improved ethical support. Am J Bioeth. 2014;14(6):4-16. doi:
10.1080/15265161.2014.900139. PMCID: PMC4160284 PMID:
24809598 [PubMed - in process]
World Health Organization 1996. The Ljubljana charter on reforming health
care. BMJ 312: 1664-1665.
Recommended

















