
IDIOPATHIC PULMONARY FIBROSIS, 2017:
PATHOGENESIS AND NOVEL THERAPEUTIC TARGETS
Bruce D. Uhal Department of Physiology Michigan State University
East Lansing, Michigan

Disclosures
Paid Consultantships: last date:GlaxoSmithKline 2017Actelion Pharm. Ltd 2007

Definition:• a chronic progressive and “inevitably fatal*” lung disease
Idiopathic Pulmonary Fibrosis (IPF)
NORMAL IPF

Definition:• a chronic progressive and “inevitably fatal*” lung disease
*
Idiopathic Pulmonary Fibrosis (IPF)
NORMAL IPF
Recently, pirfenidone and nintedanib, 2 antifibrotic drugs, have been proven to be effective in slowing disease progression and are now approved as treatments in the US and Europe.

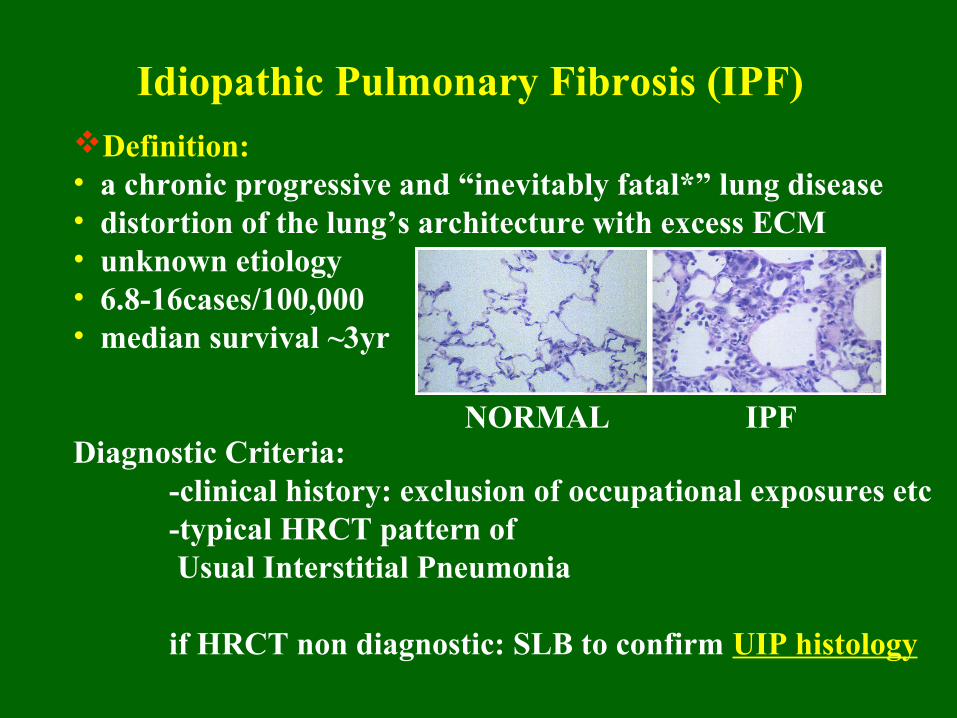
Definition:• a chronic progressive and “inevitably fatal*” lung disease • distortion of the lung’s architecture with excess ECM• unknown etiology• 6.8-16cases/100,000• median survival ~3yr
Diagnostic Criteria:clinical history: exclusion of occupational exposures etc
typical HRCT pattern of Usual Interstitial Pneumonia
if HRCT non diagnostic: SLB to confirm UIP histology
Idiopathic Pulmonary Fibrosis (IPF)
NORMAL IPF

Definition:• a chronic progressive and “inevitably fatal*” lung disease • distortion of the lung’s architecture with excess ECM• unknown etiology• 6.8-16cases/100,000• median survival ~3yr
Diagnostic Criteria:-clinical history: exclusion of occupational exposures etc-typical HRCT pattern of Usual Interstitial Pneumonia
if HRCT non diagnostic: SLB to confirm UIP histology
Idiopathic Pulmonary Fibrosis (IPF)
NORMAL IPF

Definition:• a chronic progressive and “inevitably fatal*” lung disease • distortion of the lung’s architecture with excess ECM• unknown etiology• 6.8-16cases/100,000• median survival ~3yr
Diagnostic Criteria:-clinical history: exclusion -typical HRCT pattern of Usual Interstitial Pneumonia:
if HRCT non diagnostic: SLB to confirm UIP histology
Idiopathic Pulmonary Fibrosis (IPF)
NORMAL IPF
Subpleural & basal reticular opacitiesTraction bronchiectasisHoneycomb changes (cystic airspaces thick walls 0.3-1.0cm)

Definition:• a chronic progressive and “inevitably fatal*” lung disease • distortion of the lung’s architecture with excess ECM• unknown etiology• 6.8-16cases/100,000• median survival ~3yr
Diagnostic Criteria:-clinical history: exclusion of occupational exposures etc-typical HRCT pattern of Usual Interstitial Pneumonia
if HRCT non diagnostic: SLB to confirm UIP histology
Idiopathic Pulmonary Fibrosis (IPF)
NORMAL IPF
Definition:• a chronic progressive and “inevitably fatal*” lung disease • distortion of the lung’s architecture with excess ECM• unknown etiology• 6.8-16cases/100,000• median survival ~3yr
Diagnostic Criteria:-clinical history: exclusion of occupational exposures etc-typical HRCT pattern of Usual Interstitial Pneumonia
if HRCT non diagnostic: SLB to confirm UIP histology
Idiopathic Pulmonary Fibrosis (IPF)
NORMAL IPF

Injury
Alveolitis
Derangements of Parenchyma
Loss of functionalalv.-capillary units
“Honeycomb Lung”
Pathogenesis of IPF-Traditional View:
IPF viewed as an“inflammatory disease”
From: Crystal, Ferrans and Basset, Ch7.8.1 The Lung:Scientific Foundations, 1991
Traditional View

Injury
Alveolitis
Derangements of Parenchyma
Loss of functionalalv.-capillary units
“Honeycomb Lung”
Pathogenesis of IPF-Traditional View:
IPF viewed as an“inflammatory disease”
From: Crystal, Ferrans and Basset, Ch7.8.1 The Lung:Scientific Foundations, 1991
Elephant in the room:
Antiiflammatory/Immunosuppressive Approaches do not work!
Traditional View

The failure of antiinflammatory/immunosuppressive clinical trials:
AJRCCM 190:867-878, 2014

The failure of antiinflammatory/immunosuppressive clinical trials:
“An Alarming Press Release”Wells AU et al.Eur.Resp.J.39:805-6, 2012
AJRCCM 190:867-878, 2014
“Triple Therapy” prednisone azathioprene +NAC

Arguments Against the “Inflammation Hypothesis”:Selm
Selman et al. Am J RespCrit Care Med 165:1205-8, 2002
Gauldie et al. Respir Res 2002; 3: 3-11. al.
• Anti-inflammatories/immunosuppressives don’t work
• Inflammation does not correlate with stage or outcome
• Inflammation is not required for the fibrotic response
• Inflammation is not a prominent histopathologic finding
SO, what IS critical in IPF?
IPF - Pathogenesis Theory

Arguments Against the “Inflammation Hypothesis”:Selm
Selman et al. Am J RespCrit Care Med 165:1205-8, 2002
Gauldie et al. Respir Res 2002; 3: 3-11. al.
• Anti-inflammatories/immunosuppressives don’t work
• Inflammation does not correlate with stage or outcome
• Inflammation is not required for the fibrotic response
• Inflammation is not a prominent histopathologic finding
SO, what IS critical in IPF?
IPF - Pathogenesis Theory
SO, what IS critical in IPF?

Histological Features of the IPF Lung:
F1000 Research 2016, 5(F1000 Faculty Rev):1046
Spatial heterogeneity: subpleural/paraseptal fibrosis vs. “spared” parenchyma
Temporal heterogeneity: active fibroblast foci, ECM deposition & paucity of inflammatory infiltrate vs. regions of normal lung histo

Histological Features of the IPF Lung:
F1000 Research 2016, 5(F1000 Faculty Rev):1046
Spatial heterogeneity: subpleural/paraseptal fibrosis vs. “spared” parenchyma
Temporal heterogeneity: active fibroblast foci, ECM deposition & paucity of inflammatory infiltrate vs. regions of normal lung histo
IPF
CTL
PICROSIRIUS RED
Uhal et al. AmJPhysiol275:L1192-9, 1998

Histological Features of the IPF Lung:
Annu Rev Pathol. 2014; 9:157-179
Key features of UIP: 1. fibroblastic foci -at the “edge” between fibrotic vs normal lung
-deposit collagens (myofibroblasts)
-Presence & number predict mortality in IPF! Nicholson et al. AJRCCM 166:173–177, 2002

Histological Features of the IPF Lung:
Annu Rev Pathol. 2014; 9:157-179
Key features of UIP: 1. fibroblastic foci -at the “edge” between fibrotic vs normal lung
-deposit collagens (myofibroblasts)
-Presence & number predict mortality in IPF! Nicholson et al. AJRCCM 166:173–177, 2002
Fibroblast Myofibroblast TGF-β1
collagen α−SMA

Histological Features of the IPF Lung:
Annu Rev Pathol. 2014; 9:157-179
Key features of UIP: 1. fibroblastic foci -at the “edge” between fibrotic vs normal lung
-deposit collagens (myofibroblasts)
-Presence & number predict mortality in IPF! Nicholson et al. AJRCCM 166:173–177, 2002
Fibroblast Myofibroblast TGF-β1
collagen α−SMA

Histological Features of the IPF Lung:
Annu Rev Pathol. 2014; 9:157-179
Key features of UIP: 1. fibroblastic foci -at the “edge” between fibrotic vs normal lung
-deposit collagens (myofibroblasts)
-Presence & number predict mortality in IPF! Nicholson et al. AJRCCM 166:173–177, 2002
2. “Reactive”-appearing epithelium -cuboidal
-primarily type II-like
-previously described as “hyperplastic”

Persistent and unrepaired epithelial damage (apoptosis)
Proliferation and accumulation of fibroblast/myofibroblasts
Thickening of alveolar wall by deposition of collagens I & III
Obliteration of the alveolar space.
Histological Features of the IPF Lung:
CTL
IPF
IPFISEL
The “Hyperplastic Alveolar Epithelium” is now known to be:dividing and dying (by apoptosis) simultaneously
Uhal et al. Alveolar epithelial cell death adjacent to underlying myofibroblasts in advanced fibrotic human lung. Am. J. Physiol. 275:L1192-L1199, 1998.

Lung Fibrogenesis Theory:
Early evidence for the “Severity of Epithelial Injury Hypothesis” lung explant studies – Witschi, Haschek, Adamson, Bowden 1979-1990
BHT, O2
epith. repair
Upshot: failure of reepithelialization fibrosis in the presence or the absence of blood

ANTIFIBROTIC FUNCTIONS OF THE EPITHELIUM:
Normal Alveolar Epithelium:
BM
III
Barrier~2,000Ohm
Surfactant surface T immunomod.Antioxidant Def.
AM
Soluble Factors Growth factors (e.g. EGF, FGFs) Growth inhibitors (PGE2)
Proteases uPA(degrade fibrin) MMPs (interstit. collagenases)

ANTIFIBROTIC FUNCTIONS OF THE EPITHELIUM :
Denuded Epithelium:
BM
capillary
BarrierCollapse
AM Proteases uPA = fibrinolysis MMPsint = collagen
fibrin
Lost/damaged type II cells = Surfactant surface T immunomod. Antioxidant Def.
EGF
PGE2
+
Upshot – Epith. death releases fibroblasts from inhibitions

Persistent and unrepaired epithelial damage (apoptosis)
Proliferation and accumulation of fibroblast/myofibroblasts
Thickening of alveolar wall by deposition of collagens I & III
Obliteration of the alveolar space.
Histological Features of the IPF Lung:
CTL
IPF
IPFISEL
The “Hyperplastic Alveolar Epithelium” is now known to be:dividing and dying (by apoptosis) simultaneously

Persistent and unrepaired epithelial damage (apoptosis)
Proliferation and accumulation of fibroblast/myofibroblasts
Thickening of alveolar wall by deposition of collagens I & III
Obliteration of the alveolar space.
Histological Features of the IPF Lung:
CTL
IPF
IPFISEL
The “Hyperplastic Alveolar Epithelium” is now known to be:dividing and dying (by apoptosis) simultaneously
But at the same time, Fibroblasts/myofibroblasts are Resistant to apoptosis:

Histological Features of the IPF Lung:
CTL
IPF
IPFISEL
Apoptosis in IPF Lung Biopsies:
TUNELChest 2005125:1005
ISELAm.J.Physiol. 1998275:L1192
BAX IHCChest 2005
125:1005
Little MF labeling=Resistance to apoptosis

Histological Features of the IPF Lung:
CTL
IPF
IPFISEL
Apoptosis in IPF Lung Biopsies:
TUNELChest 2005125:1005
ISELAm.J.Physiol. 1998275:L1192
BAX IHCChest 2005
125:1005
Little MF labeling=Resistance to apoptosis
Apoptosis high in the epithelium, But low in myofibroblast foci,
= “The Apoptosis Paradox” in IPF V. Thannickal

Persistent and unrepaired epithelial damage
Epithelial-Mesenchymal Transition (EMT) blasts
Thickening of alveolar wall by deposition of collagens I & III
Ob
literation of the alveolar space.
Mechanisms of fibrogenesis in IPF:
The “Hyperplastic Alveolar Epithelium” is now known to be:dividing and dying (by apoptosis)AND:Undergoing EMT (Epith-Mesenchymal Transition)

Persistent and unrepaired epithelial damage
Epithelial-Mesenchymal Transition (EMT) blasts
Thickening of alveolar wall by deposition of collagens I & III
Oblite
ration of the alveolar space.
Mechanisms of fibrogenesis in IPF:
The “Hyperplastic Alveolar Epithelium” is now known to be:dividing and dying (by apoptosis)AND:Undergoing EMT (Epith-Mesenchymal Transition)
Type II AEC Myofibroblast TGF-β1,
mutations collagen α−SMA

Persistent and unrepaired epithelial damage
Epithelial-Mesenchymal Transition (EMT) blasts
Epithelial “Activation” to secrete growth factors & cytokines I & III
O
bliteration of the alveolar space.
Mechanisms of fibrogenesis in IPF:
The “Hyperplastic Alveolar Epithelium” is now known to be:dividing and dying (by apoptosis)AND:Undergoing EMT (Epith-Mesenchymal Transition)
Type II AEC Myofibroblast TGF-β1,
mutations collagen α−SMA

MECHANISMS IF FIBROGENESIS IN IPF:
surviving “REACTIVE” Epithelium: (dying/proliferating??)
BM
capillary
Cytokines IL-1,6,8,10,11 GMCSF CCL2 CXCL12
Growth Factors TGF-β1 FGF’s, CTGF PDGF’s, IGF’s, TGF-α ET-1
+

MECHANISMS IF FIBROGENESIS IN IPF:
surviving “REACTIVE” Epithelium: (dying/proliferating??)
BM
capillary
Cytokines IL-1,6,8,10,11 GMCSF CCL2 CXCL12
Growth Factors TGF-β1 FGF’s, CTGF PDGF’s, IGF’s, TGF-α ET-1
+
recruit circulatingfibrocytes

Persistent and unrepaired epithelial damage
Epithelial-Mesenchymal Transition (EMT) blasts
Epithelial “Activation” to secrete growth factors & cytokines I & III
Entry & engraftment of circulating fibrocytes of t
he alveolar space.
Mechanisms of fibrogenesis in IPF:
The “Hyperplastic Alveolar Epithelium” is now known to be:-dividing and dying (by apoptosis)-undergoing EMT-secreting GFs/cytokines
Circulating fibrocytes

Persistent and unrepaired epithelial damage
Epithelial-Mesenchymal Transition (EMT) blasts
Epithelial “Activation” to secrete growth factors & cytokines I & III
Entry & engraftment of circulating fibrocytes
Genetic predispositions the alveolar space.
Mechanisms of fibrogenesis in IPF:
The “Hyperplastic Alveolar Epithelium” is now known to be:-dividing and dying (by apoptosis)-undergoing EMT-secreting GFs/cytokines
Circulating fibrocytes

Genetic Mutations Predisposing to Pulmonary Fibrosis (IPF-like)
Wolters P et al. AnnRev Pathol 9:157-179, 2014
Surfactant Protein C / A
Mucin 5B
Telomerase

Genetic Mutations Predisposing to Pulmonary Fibrosis (IPF-like)
Wolters P et al. AnnRev Pathol 9:157-179, 2014
Surfactant Protein C / A
Mucin 5B(elevated MUC5B protein)
-relation to IPF unclear
Telomerase(shortened telomeres)-increased apoptosis?

SP-C BRICHOS DOMAIN MUTATIONS:
Discovery:
Pedigree:Black = IPFSquare = males# = DNA seq
Proband Biospies
SP-C G100S mutation causes familial pulmonary fibrosis in Japanese kindred. Ono et al. ERJ 38:861-869, 2011.

SP-C BRICHOS DOMAIN MUTATIONS:
Cause disruption of protein folding and packaging into LBs
SP-C:
Made only by Type IIepithelial Cells
ESSENTIALfor normallung function
Lamellar Bodies:Fibrogenic non-fibrogenic
100S

SP-C BRICHOS DOMAIN MUTATIONS:Mechanisms of Toxicity:
1.UPR (Unfolded Protein Response) & ER Stress
2.Apoptosis of type II AECs & loss of antifibrotic functions
a
*Other activators of ER Stress: viruses, hyperoxia, hypoxia etc.3. EMT (Epithelial-Mesenchymal Transition)
(X-box BP-1)C/EBP-homol.PActivating TFs
Chaperones:
CHOP ATF-4,-6
Ubiquitin Proteasome System
Ono et al. ERJ 38:861-869, 2011 Lawson et al. AJP 294L1119, 2008Mulugeta et al. AJRCMB 32:521-530, 2005
Zhong et al. AJRCMB 45(3):498-509, 2011

SP-C BRICHOS DOMAIN MUTATIONS:Mechanisms of Toxicity:
1.UPR (Unfolded Protein Response) & ER Stress
2.Apoptosis of type II AECs & loss of antifibrotic functions
a
*Other activators of ER Stress: viruses, hyperoxia, hypoxia etc.3. EMT (Epithelial-Mesenchymal Transition)
(X-box BP-1)C/EBP-homol.PActivating TFs
Chaperones:
CHOP ATF-4,-6
Ubiquitin Proteasome System
Ono et al. ERJ 38:861-869, 2011 Lawson et al. AJP 294L1119, 2008Mulugeta et al. AJRCMB 32:521-530, 2005

SP-C BRICHOS DOMAIN MUTATIONS:Mechanisms of Toxicity:
1.UPR (Unfolded Protein Response) & ER Stress
2.Apoptosis of type II AECs & loss of antifibrotic functions
a
*Other activators of ER Stress: viruses, hyperoxia, hypoxia etc.3. EMT (Epithelial-Mesenchymal Transition)
(X-box BP-1)C/EBP-homol.PActivating TFs
Chaperones:
CHOP ATF-4,-6
Ubiquitin Proteasome System
Ono et al. ERJ 38:861-869, 2011 Lawson et al. AJP 294L1119, 2008Mulugeta et al. AJRCMB 32:521-530, 2005
Zhong et al. AJRCMB 45(3):498-509, 2011
Type II cell Myofibroblast ER Stress
collagen α−SMA

SP-C BRICHOS DOMAIN MUTATIONS:
Implications on Lung Fibrosis Pathogenesis:
1.SP-C is expressed only by type II alveolar epithelial cells
2.Fibrogenic SP-C mutants induce AEC apoptosis
3.Fibrogenic SP-C mutants also induce EMT4.“Activated” epithelia recruit circulating fibrocytes
5.The above strongly suggest that Epithelial Injury initiates and likely helps propogate fibrosis progression

SP-C BRICHOS DOMAIN MUTATIONS:
Implications on Lung Fibrosis Pathogenesis:
1.SP-C is expressed only by type II alveolar epithelial cells
2.Fibrogenic SP-C mutants induce AEC apoptosis
3.Fibrogenic SP-C mutants also induce EMT4.“Activated” epithelia recruit circulating fibrocytes
5.The above strongly suggest that Epithelial Injury initiates and likely helps propogate fibrosis progression
The “Witschi Hypothesis” ~ 1979a.k.a.“Severity of Epithelial Injury” theory
AJP:Lung 305:L906-L911, 2013

SP-C BRICHOS DOMAIN MUTATIONS:
Implications on Lung Fibrosis Pathogenesis:
1.SP-C is expressed only by type II alveolar epithelial cells
2.Fibrogenic SP-C mutants induce AEC apoptosis
3.Fibrogenic SP-C mutants also induce EMT4.“Activated” epithelia recruit circulating fibrocytes
5.The above strongly suggest that Epithelial Injury initiates and likely helps propogate fibrosis progression
The “Witschi Hypothesis” ~ 1979a.k.a.“Severity of Epithelial Injury” theory
AJP:Lung 305:L906-L911, 2013

SP-C BRICHOS DOMAIN MUTATIONS:
Implications on Lung Fibrosis Pathogenesis:
1.SP-C is expressed only by type II alveolar epithelial cells
2.Fibrogenic SP-C mutants induce AEC apoptosis
3.Fibrogenic SP-C mutants also induce EMT4.“Activated” epithelia recruit circulating fibrocytes
5.The above strongly suggest that Epithelial Injury initiates and likely helps propogate fibrosis progression
The “Witschi Hypothesis” ~ 1979a.k.a.“Severity of Epithelial Injury” theory
AJP:Lung 305:L906-L911, 2013

Pathophysiologic Stages of Idiopathic Pulmonary Fibrosis (IPF)
Summary of IPF Pathogenesis:
Epithelial Pathologic Cells: Mesenchymal Cells
telomere length?
From Wolters P et al. AnnRev Pathol 9:157-179, 2014
type II cell myofibroblast

Investigational Therapies for IPF, 2015From Ahluwalia et al. AJRCCM 190:867-868, 2014
Targets: Epithelial InjuryDrug: NAC
Matrix Accumulation
Immune LOXL2 mAB
ActivationIL-13 mABs
Vascular Leak
Fibroblast recruitment, Myofibroblast invasion, proliferation evolution
tyr kinase inhib,, antifibrotic. Integrin αvβ6mABLysoPA-R antagonist

TARGETING THE EPITHELIUM IN IPF:
Inducers of Apoptosis in Lung Epithelial CellsInducer Mediators . Chemotherapy, amiodarone caspases, Bcl-2 family, AT1RFas ligand caspases, Bcl-fam, AT1RTNF-α caspases, Bcl-fam, AT1RTGF-β1 caspases, EGR-1SP-C mutations ER stress, UPR, ATIR Eur Respir Rev 17: 109, 138–143, 2008 al Strategy – block or inhibit expressionCaspase inhibitors* Am.J.Physiol. 279:L143, 2000 HGF* Pediatric Res.56:336, 2004
p21 overexpression* Am.J.Physiol. 286:L727, 2004
AT1 receptor blockers* Am. J. Pathol. 163:2523, 2003 ACE-2/ANG1-7/mas activation * Am.J.Physiol. 279:L143, 2000
* In vivo confirmation (mice)
Blockers of Epithelial Apoptosis & Collagen Deposition
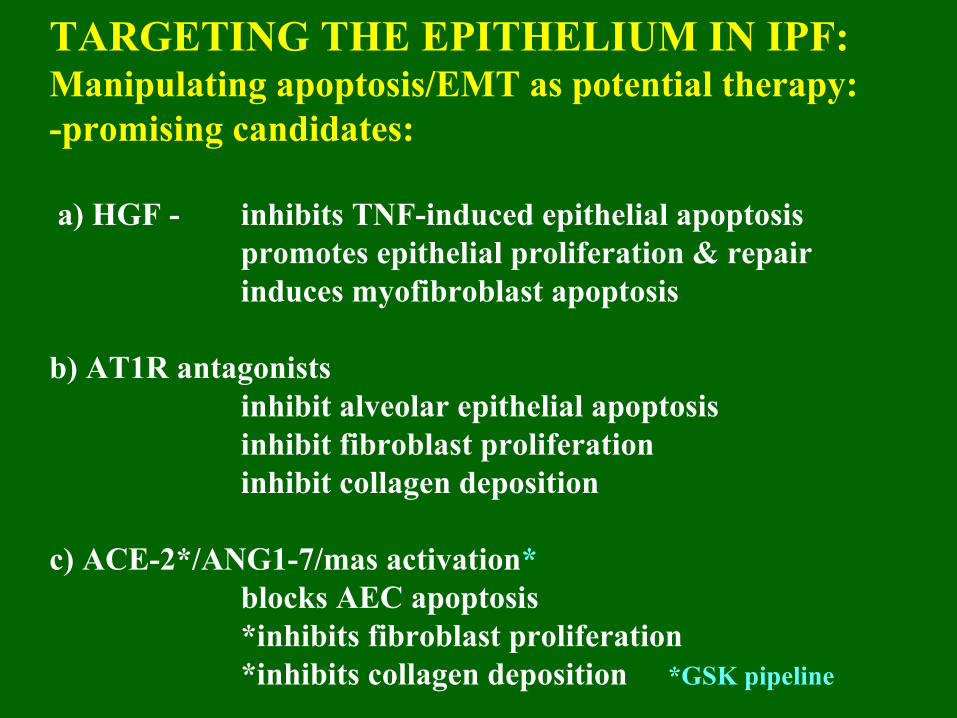
TARGETING THE EPITHELIUM IN IPF: Manipulating apoptosis/EMT as potential therapy:-promising candidates:
a) HGF - inhibits TNF-induced epithelial apoptosispromotes epithelial proliferation & repairinduces myofibroblast apoptosis
b) AT1R antagonistsinhibit alveolar epithelial apoptosisinhibit fibroblast proliferationinhibit collagen deposition
c) ACE-2*/ANG1-7/mas activation*blocks AEC apoptosis *inhibits fibroblast proliferation*inhibits collagen deposition *GSK pipeline

ACKNOWLEDGEMENTS
Collaborators:Dr. M. Molina-Molina BarcelonaDr. A. Xaubet Barcelona
Dr. Karen Friderici Michigan State
Dr. Yuehua Cui Michigan State
Dr. Xiaopeng Li U. Iowa
Dr. Amal Abdul-Hafez Michigan State
Funding: NIH, Am.Heart Assoc., Am.Physiol. Soc., IDIBAPS, SEPAR, SOCAP-FUCAP


Factors that Confer Resistance to Apoptosis in Lung Myofibroblasts/fibroblastsMolecule Basic Mechanism Mediators . IL-6 reduces FasL induction Stat3, Bcl-2
TGF-β1 blocks IL-1β induction iNOS, Bcl-2
Thrombin* blocks FasL induction PAR-1, PKC-ε , p21
IGF-1 blocks GF-withdrawal Akt, ERK phospho.
FIZZ1 blocks TNF-α induction ERK-1/2 phospo.(a.k.a. RELM-α, resistin-like molecule α)
Anti-α2β1* ligation of integrin PI3K, Akt, PKB integrin
Potential strategy- attempt blockade *human cells

Roles of ACE-2 in Lung Fibrosis
Angiotensinogen ANGI ANGII ACEchymase
ANG1-7
ACE-2
APOPTOSIS,FIBROSIS
ACE-2 SHOULD BE PROTECTIVE - IT IS!
AND, ACE-2 ISREDUCED
IN IPF
Am J Physiol 295(1):L178-L185, 2008
Tools to study ACE-2:Competitive inhibitor (DX600) ACE-2 siRNAs (mouse lung)

Mechanisms of Protection by ACE-2/ANG1-7:
Alveolar epithelial cells: fibroblasts, leukocytes:
Recommended

















