
DOI: 10.1161/CIRCGENETICS.112.963660
1
Identification of the BCAR1-CFDP1-TMEM170A Locus as a Determinant of
Carotid Intima-Media Thickness and Coronary Artery Disease Risk
Running title: Gertow et al.; Genetic locus associated with cIMT and CAD
Karl Gertow, PhD1; Bengt Sennblad, PhD1; Rona J. Strawbridge, PhD1; John Öhrvik, PhD1;
Delilah Zabaneh, PhD2; Sonia Shah, MSc2; Fabrizio Veglia, PhD3; Cristiano Fava, MD, PhD4,5;
Maryam Kavousi, MD, MSc6,7; Stela McLachlan, PhD8; Mika Kivimäki, PhD9; Jennifer L.
Bolton, PhD8; Lasse Folkersen, PhD1,10; Bruna Gigante, MD, PhD11; Karin Leander, PhD11; Max
Vikström, BSc11; Malin Larsson, PhD1; Angela Silveira, PhD1; John Deanfield, MD, PhD12;
Benjamin F. Voight, PhD13,14; Pierre Fontanillas, PhD13,14; Maria Sabater-Lleal, PhD1; Gualtiero
I. Colombo, MD, PhD3; Meena Kumari, PhD9; Claudia Langenberg, PhD9,15; Nick J. Wareham,
MBBS, PhD15; André G. Uitterlinden, PhD6,7,16; Anders Gabrielsen, MD, PhD10; Ulf Hedin, MD,
PhD17; Anders Franco-Cereceda, MD, PhD17; Kristiina Nyyssönen, PhD18; Rainer Rauramaa,
MD, PhD19,20; Tomi-Pekka Tuomainen, MD, PhD18; Kai Savonen, MD, PhD19,20; Andries J.
Smit, MD, PhD21; Philippe Giral, MD, PhD22; Elmo Mannarino, MD, PhD23; Christine M.
Robertson, MBChB8; Philippa J. Talmud, PhD24; Bo Hedblad, MD, PhD4; Albert Hofman, MD,
PhD6,7; Jeanette Erdmann, PhD25*; Muredach P. Reilly, MBBCH, MSCE26,27*; Christopher J.
O’Donnell, MD, MPH28,29,30*; Martin Farrall, FRCPath31,32†; Robert Clarke, MD, PhD33†; Maria
Grazia Franzosi, PhD34†; Udo Seedorf, PhD35†; Ann-Christine Syvänen, PhD36; Göran K.
Hansson, MD, PhD10; Per Eriksson, PhD1; Nilesh J. Samani, MF, FRCP37,38*; Hugh Watkins,
FRCP31,32†; Jacqueline F. Price, MBChB8; Aroon D. Hingorani, MD, PhD9,39; Olle Melander,
MD, PhD4; Jacqueline C.M. Witteman, PhD6,7; Damiano Baldassarre, PhD3,40; Elena Tremoli
PhD3,40; Ulf de Faire, MD, PhD11; Steve E. Humphries, PhD24; Anders Hamsten, FRCP1
on behalf of the *CARDIoGRAM & †PROCARDIS consortiums
1Atherosclerosis Research Unit, 10Experimental Cardiovascular Rsrch Unit, Dept of Medicine, Solna, Karolinska Institutet, Karolinska Univ Hospital Solna, Stockholm, Sweden; 2Univ College London
Genetics Inst, 9Genetic Epidemiology Group, Dept of Epidemiology & Public Health, 24Cardiovascular Genetics, BHF Laboratories, Rayne Building, 39Centre for Clinical Pharmacology, Dept of Medicine,
Univ College London, London, UK; 3Centro Cardiologico Monzino, IRCCS, Milan, Italy; 4Clinical Rsrch
imäki, PhD ; Jenniffiffere
KaKKK riiiin n n n LeLeLeLeanananandededederrrr,,,, PPhPP DDDD11111
n Deaaaanfnfnfnfieieieieldldldld,,, MDMDMDMD,,,, PhPPP D
F a
o e
D n
n m
D e
MD PhD ; Philippe Giral MD PhD ; Elmo Mannarino MD PhD ; Christine
F. VoVoVoigighthth , PhPP DDD13111 ,14; Pierre Fontanillas, PhPhPhDD13,14; Maria a Sababaater-Lleal, PhD1; Gua
o,,, MMMD, PhD333; MeMMeenennaa a KuKuKummariririr ,, PPPhP DD9999;; CCClauuddia LLangngennnbeerg, PPPhDD9,9,99,1511515; NiNiNiN ckckckk JJJ. WaWW re
D1511 ;;;; AnAA dré ééé G.GGG UUUitteerrrlr indededed n,n,,, PPPPhDhDhDD6,,,,7,16; AnAnA dederssss GGGabababbrrir elelellseseen,n,n,n, MMMD,D,D, PPPPhDhh 11101 ; UUUlf HHHeH ddin
nders Franco-CeCeCeC rereeececececedadadaa, MDMDMDD, ,,, PhPhPhPhDDDD17; ; ; KrKrKrisiistititiinininina aa NyNyNyNyysysysssösösösöneneneen,n,n,n PPPPhDhDhDD18; ;;; Rainer Rauram
DDD19,20;;; TTTomomomi-i PePePekkkkaaa TuTuTuomomomaiainenenennn, MMMDDD, PPPhDhD181 ;;; KaKaKaii SaSaSavovovonenenennn, MMMDDD, PPPhDhD19,20;;; AnAnAndrdriei
MDMDMD PhPhPhDDD21111;; PhPhPhilililipipippepe GGGiririralalal MDMDMD PhPhPhDDD2222222;; ElElElmomo MMManannanariririnono MDMDMD PhPhPhDDD23232323;; ChChChriririststinininee by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
2
Center, Dept of Clinical Sciences, Lund Univ, Skåne Univ Hospital, Lund, Sweden; 5Division of Internal Medicine C, Dept of Medicine, Univ of Verona, Hospital "Policlinico G.B Rossi", Verona, Italy; 6Dept of Epidemiology, 16Dept of Internal Medicine, Erasmus University Medical Center; 7Netherlands Genomics Initiative - Sponsored Netherlands Consortium for Healthy Ageing, Rotterdam, The Netherlands; 8Centre
for Population Health Sciences, Univ of Edinburgh, Edinburgh, UK; 11Division of Cardiovascular Epidemiology, Inst of Environmental Medicine, 17Dept of Molecular Medicine & Surgery, Karolinska
Institutet, Stockholm, Sweden; 12Cardiothoracic Unit, Great Ormond Street Hospital, London, UK; 13Program in Medical & Population Genetics, Broad Institute, Cambridge, MA; 14Center for Human
Genetic Research & Diabetes Rsrch Center (Diabetes Unit), Massachusetts General Hospital, Boston, MA; 15MRC Epidemiology Unit, Inst of Metabolic Science, Univ of Cambridge, Addenbrooke's Hospital,
Cambridge, UK; 18Inst of Public Health & Clinical Nutrition, Univ of Eastern Finland; 19Kuopio Rsrch Inst of Exercise Medicine, Foundation for Rsrch in Health Exercise & Nutrition; 20Dept of Clinical
Physiology & Nuclear Medicine, Kuopio Univ Hospital, Kuopio, Finland; 21Dept of Medicine, Univ Medical Center Groningen, Groningen, the Netherlands; 22Assistance Publique - Hopitaux de Paris,
Service Endocrinologie-Metabolisme, Groupe Hôpitalier Pitie-Salpetriere, Unités de Prévention Cardiovasculaire, Paris, France; 23Internal Medicine, Angiology & Arteriosclerosis Diseases, Dept of
Clinical & Experimental Medicine, Univ of Perugia, Perugia, Italy; 25Universität zu Lübeck, Medizinische Klinik II, Lübeck, Germany; 26The Inst for Translational Medicine & Therapeutics,
27Cardiovascular Inst, Perelman School of Medicine, Univ of Pennsylvania, Philadelphia, PA; 28National Heart, Lung, and Blood Institute's Framingham Heart Study, Framingham, MA; 29Division of Intramural
Rsrch, NHLBI, Bethesda, MD; 30Cardiology Division, Dept of Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA; 31Dept of Cardiovascular Medicine, The Wellcome Trust
Centre for Human Genetics, 33Clinical Trial Service Unit, Univ of Oxford; 32Dept of Cardiovascular Medicine, Univ of Oxford, John Radcliffe Hospital, Headington, Oxford, UK; 34Dept of Cardiovascular
Rsrch, Istituto Mario Negri, Milan, Italy; 35Gesellschaft für Arterioskleroseforschung e.V., Leibniz-Institut für Arterioskleroseforschung an der Universität Münster (LIFA), Münster, Germany; 36Dept of
Medical Sciences, Molecular Medicine & Science for Life Laboratory, Uppsala Univ, Uppsala, Sweden; 37Dept of Cardiovascular Sciences, Univ of Leicester, 38Leicester NIHR Biomedical Rsrch Unit in
Cardiovascular Disease, Glenfield Hospital, Leicester, UK; 40Dipartimento di Scienze Farmacologiche e Biomolecolari, Univ of Milan, Milan, Italy
Corresponding author:
Karl Gertow, PhD
Atherosclerosis Research Unit
Karolinska University Hospital Solna
Center for Molecular Medicine, Building L8:03
S-171 76 Stockholm, Sweden
Tel: +46-8-51773201
Fax: +46-8-311298E
E-mail: [email protected]
Journal Subject Codes: [109] Clinical genetics
osclerosis Diseases, DeDDD pUnUnUnUniviviviverererersisisisitätätätät t t t zuzuzuzu LLLLüüüübebebebeckckckck,,,,üüü
Medicicicicinenenene &&&& ThThThThererererapapapapeueueueutitititiPhiladedededelplplplphihihih a,a,a,a, PPPPAAAA;;;; 2828828Na
29292929g, and Blood Institute s Framingham Heart Study Framingham MA; Division of IntraN ra mo cUtr ei w
o tular Disease, Glenfield Hospital, Leicester, UK; Dipartimento di Scienze Farmacolog
g, and Blood Institute s Framingham Heart Study, Framingham, MA; Division of IntraNHHLBLLBIII, BBBetetthhhesdsddaaa, MD; 30Cardiology Divisioioionn, Dept of Mededicinneee, Massachusetts Generarvrvvarararard Medicacac lll ScScScSchoohoolololol,,, BoBBB stststonononon, MAMAMAMA;;; 31DeDeDeD pt ofof Carrardidididiovoovovasssscuccuculalalar rr MeMeMeMediciciicinenenene, , ThTTT e ee WeWeWWelllllllcocococ mor HHHHumuu an Genetticccs, 3333 CCClinnnnicicical TTT irialll SServvvicce UUnnit, UUUninininivv vv oof OOOxforrd;;; 32DeDD pt ofofofo CararardiovvvaascUnnnivvv of Oxfofofordd, JJJohhn Radddclclifi fe HHooosppip taaall, Heaaddingngngtton,n, OOxfffoord, UUKKK; 34444DeDDD ppppttt oofo CaCardioiiovatitutoo MaMaMaMariririo NeNeNegrgrgri,ii MMMililili an, ItItItalalalalyyyy; 35GeGeGeG ssseselllllll schahahah ftftft ffffürürür AAAArtrtrterrereriiioi skskskklelelelerrrosososefefefforscscscschuhuhung eee VV.VV., LLLLeieieibr Arterioskleroseeeefofofof rsrsrschchchchunununng ggg annann ddddererer UUUUnininin veveveversrrsr itittätäät MMMMünününü sterererer (((LILILILIFAFAFAFA),),),), MMMMünününstststterererer, ,, Germany; 36Deiences, Moleculaaarrr MeMeMeM didd ciciciinenne &&&& ScScScS ieieiiencnce foffoforrr LiLLifefefe LLLabororratatorororyy, UpUpUpU pspssalalala a UnUnUnU iv, Uppsala, Sw
offf Cardiovasassascucucuculalalar rrr ScScSScieieieienccceseseses, ,, UnUnUnUniviiviv offff LLLeieieeicecceceststtsterererer, , , 383838LeLeLeL icicciceseesesteeer rr r NIININIHRHRHRHR BBBBioioiiomemememedididicacacacal ll RsRR rch Uniitululularar DDDisisiseaeasese, GlGlGlenenfififieleleldddd HoHoHosspipipitatall,l LLLeieieiceceststerer, UKUKUK;; 40404040DiDiDipapartrtimimimenentoto dddiii ScScScieieienznzee FaFaFarmrmacacololologog by guest on June 18, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
3
Abstract:
Background - Carotid intima-media thickness (cIMT) is a widely accepted marker of subclinical
atherosclerosis. To date, large-scale investigations of genetic determinants of cIMT are sparse.
Methods and Results - In order to identify cIMT-associated genes and genetic variants, a
discovery analysis using the Illumina 200K CardioMetabochip was conducted in 3,430 subjects
with detailed ultrasonographic determinations of cIMT from the IMPROVE study. Segment-
specific IMT measurements of common carotid (CC), bifurcation, and internal carotid arteries,
and composite IMT variables considering the whole carotid tree (IMTmean, IMTmax, and IMTmean-
max), were analysed. A replication stage investigating 42 single nucleotide polymorphisms
(SNPs) for association with CC-IMT was undertaken in five independent European cohorts (total
n=11,590). A locus on chromosome 16 (lead SNP rs4888378, intronic in CFDP1) was associated
with cIMT at significance levels passing multiple-testing correction at both stages (array-wide
significant discovery P=6.75x10-7 for IMTmax; replication P=7.24x10-6 for CC-IMT; adjustments
for sex, age and population substructure where applicable; minor allele frequency 0.43 and 0.41,
respectively). The protective minor allele was associated with lower carotid plaque score in a
replication cohort (P=0.04, n=2120), and lower coronary artery disease (CAD) risk in two case-
control studies of subjects with European ancestry (odds ratio [95%CI] 0.83 [0.77-0.90],
P=6.53x10-6; n=13,591, and 0.95 [0.92-0.98], P=1.83x10-4, n=82,297, respectively). Queries of
human biobank datasets (n=126-138) revealed associations of rs4888378 with nearby gene
expression in vascular tissues.
Conclusions - This study identified rs4888378 in the BCAR1-CFDP1-TMEM170A locus as a
novel genetic determinant of cIMT and CAD risk in individuals of European descent.
Key words: atherosclerosis; coronary artery disease; genetics; carotid intima-media thickness
p y p
enenenent ttt EuEuEuEurorororopepepepeanananan ccccohohohohorooo tssss
in CFFFFDPDPDPDP1111)))) wawawawas s s s asasasa so
w
d t
e and population substructure where applicable; minor allele frequency 0.43 and
y n
c
dies of subjects with European ancestry (odds ratio [95%CI] 0.83 [0.77-0.90],
at sisisisigngngnifififificicicanananceee llllevels passing multiple-teteteststing correction aatt t bobbb th stages (array-w
didididiscccovery P=6=6=6=6.7775x5x1010010 777-7 fofofoforr IMIMIMI TTTTmammax; rerrepliccaatiooonn PPPP=7==7.2.2224x44x10100-6-66-6 foooorr CCCCCCC -IMIMIMTTTT;;;; adadaddjujujujust
e aandndndnd ppopulllataa ioonnn suubbbstruuuctuture wwheheheh re aaapppp liicabllllee; mminnorr allelleee frrreqeqeqquencncncyy y 000.43 annd
y). The protectiiivevve minororor aallele e waww s s assssocicciatatedd wititith h looowewer cacaarororotid dd plppp aque score in
cohort ((P=0.04,4,4, n 2=22121220)0)0), ,, and dd lolll wer coronaryyy artery yy dididisease (C(C(C( ADADADAD) ) risk in two c
dddieieiess ofofof ssubububjejejectctss wiwiwithththth EEEururopopeaeann anancece tststryry ((((odododddsdsdsd rratattioioioi [[[[9595959 %C%C%C%CI]I]I]] 0000.8.8.883333 [0[0[0.7.7.777-7-7-0.0.0.909090],],],
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
4
Introduction
Carotid intima-media thickness (cIMT), as determined by high-resolution ultrasound techniques,
is a well-established marker of subclinical atherosclerosis and is widely used in epidemiological
studies and interventional trials.1, 2 It has been proposed as a surrogate marker for coronary
atherosclerosis, and has been shown to predict incident coronary and cerebrovascular events.3-5
Accordingly, cIMT constitutes an attractive quantitative intermediate disease phenotype for the
study of atherosclerosis-related cardiovascular disease. Genetic association studies of cIMT,
conducted in individuals free of manifest disease, may identify susceptibility genes and pathways
involved in the initiation and early phases of disease, which may be less readily discernible in
studies of late-stage and clinically manifest disease such as myocardial infarction (MI) and
stroke. Nevertheless, large-scale studies of genetic determinants of cIMT remain sparse.
To date, one meta-analysis of single-nucleotide polymorphism (SNP)-based genome-
wide association (GWA) studies of cIMT has been reported, which identified three regions (on
chromosome 8q23.1, 8q24, and 19q13) as being associated with common carotid IMT (CC-
IMT).6 In contrast, candidate gene studies of cIMT have provided inconsistent results,7 and two
genome-wide linkage scans only found regions with suggestive linkage to cIMT.8, 9 In the
present study, we performed a discovery genetic association analysis of cIMT in 3,430
participants of the Pan-European population-based IMPROVE study,10 using a custom
genotyping array (the Illumina CardioMetabochip, also referred to as the Metabochip). The
CardioMetabochip interrogates approximately 200,000 SNPs located in regions identified by
previous GWA studies of metabolic and cardiovascular traits and diseases. In a second stage, we
conducted replication studies in 11,590 participants from five independent population-based
cohorts. One robustly associated cIMT locus was subsequently tested in silico for association
tibilityyy genes and ppppataaa
ss re ddaddilililily didididiscerninininiblblblble
a
v
d
iation (GWA) studies of cIMT has been reported, which identified three regions
me 8q23 1 8q24 and 19q13) as being associated ith common carotid IMT (CC
ate-stststagagageee ananand clclclclini ically manifest diseaseee sussuch as myocardiiialalall infarction (MI) and ff
veeeerthhheless, largge--scalalalle sttttudududu ies ss oofo ggeneeetiic ddettermimiminanananannts oof cIMMMT reeemainininin spapaparseee.
date, ooonenenene metttaa-ananalallysysis offf sisisisingle-nnnucucucucleleleototttidididee popopolylylylymomomorppphihihihismsm ((((SNSNSNSNP)P)P)P)-babbb seed dd gegenonomm
iation ((GWA)) studididiies offf cIMTMTM hhhhas been repopp rted,,, hwhhhich hhh idididi entififififiedddd three regggions
88 2q233 11 88 2q244 dnd 1199q1313)) bb iei iiatedd ii hth itidd IMIMTT (C(CCC by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
5
with coronary artery disease (CAD) risk in two large independent GWA studies of CAD and
with mRNA expression of nearby genes in vascular tissues collected in two biobank
programmes.
Methods
Cohorts and Study Design
The first stage consisted of genetic association analysis of cIMT measurements in the IMPROVE
study (n=3,430).10 SNPs that passed an a priori threshold for statistical association (P<1x10-4 or
P<1x10-5 depending on cIMT phenotype) were then taken forward for replication in the
Whitehall-II study (WH-II, n=2,138),11, 12 the Edinburgh Artery Study (EAS, n=630),13 the
Rotterdam-I and Rotterdam-II studies (RS-I and RS-II, n=4,699 and n=1,980, respectively),14, 15
and the cardiovascular arm of the Malmö Diet and Cancer study (MDC, n=2,141),16, 17 with
subsequent evaluation of results by meta-analysis. Detailed descriptions of the discovery and
replication cohorts are given in online Supplemental Section S1 and in Supplemental Table 1.
A locus which reached significance levels passing correction for multiple testing at both the
discovery and replication stages was further tested for association with carotid plaque score in
the MDC study, with coronary artery calcium (CAC) score in the RS-I and RS-II studies, and for
association with CAD risk in PROCARDIS,18 a large European CAD case-control study to
which additional controls were added from the Wellcome Trust Case-Control Consortium
(WTCCC), in total 5,710 cases and 7,881 controls, and in CARDIoGRAM,19 a large CAD case-
control GWA study meta-analysis consortium comprising 22,233 CAD cases and 64,762
controls of European descent. In addition to replication in independent cohorts, complementary
internal validation by bootstrap analyses was undertaken in IMPROVE in order to corroborate
findings from the discovery stage in relation to IMT phenotypes which were not available in the
(
repllllicicicicatatatatioioioion n n n inininin tttthehehehe
31313II study (WH II n=2 138) the Edinburgh Artery Study (EAS n=630) the
)
d h
evaluation of results by meta-analysis. Detailed descriptions of the discovery an
cohorts are given in online pp Supplemental Tab
II studydydy (((WHWHWH-IIII,II n=2,138), the Edinbururgh Artery Study y y (EAS, n=630), the
I annnd Rotterdadadammm-IIIIIIII ssstuttudidididiesese ((((RSRSRSR --I and ddd RRS--III, nn=4=4=4,6,66999999 aandndnd nn=1== ,99998080808 , rererespsps ececectititivevevelylll )
diooovavavvascscscculululu arararar aaarmrmrmm oooff f thhhhee MaMaMaM lmlmlmlmö öö DiDiDiDietetett aaaandndnd CCCCanananncececec r rr ststststudududdy y (M(M(MMDCDCDCDC,,,, n=n==2,2,2,2 14141441)1)1),,,1116, 17 wiwiwitht
evaluation of rrrresesesesulululltststst bbbby yyy mememeetatatat -a-aa-anananan lylylyysisisisis.s.s DDDetetettaiaiaia llel d ddd dedededescscscscririptptpttioioioi nsnsnsn ooof fff ththththe discovery an
cocohohortrtss araree gigivevenn iniin oonlnllininee SuSuSuS pppplelelemementnttalalal SSSSecectitititionon SSSS1111 aanddnd iiinn SuSuSuS pppplelelel mementntalalal TTTaaba
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
6
replication cohorts. The replicated cIMT locus was also tested for association with mRNA
expression of nearby genes in vascular tissues collected in the Advanced Study of Aortic
Pathology (ASAP) and the Biobank of Karolinska Endarterectomies (BiKE) studies,20 in order to
explore potential mechanisms underlying the observed cIMT and CAD associations.
Genotyping and Quality Control
A description of the genotyping technologies used for the discovery and replication cohorts
along with quality control (QC) criteria is provided in Supplemental Section S2 and
Supplemental Table 1. Genotyping in IMPROVE, WH-II, EAS and MDC was performed using
the Illumina 200K CardioMetabochip, whereas the RS-I and RS-II studies were genotyped using
the Ilumina HumanHap550 array and imputed to the 1000Genomes CEU Caucasian reference
panel.19 The CardioMetabochip is a custom Illumina iSelect genotyping array that captures DNA
variation at regions identified by meta-analyses of GWA studies for diseases and traits relevant
to metabolic and atherosclerotic/cardiovascular endpoints, comprising approximately 200,000
SNPs. In IMPROVE, individual level exclusion criteria were call rates <0.95, results of identity
by state (IBS) estimations (e.g. unverified cryptic relatedness), verified relatedness, estimated
inbreeding (excessive homozygosity), discrepancy between recorded and genotype-determined
sex, outliers in multi-dimensional scaling (MDS) analysis (Supplemental Section S2 and
Supplemental Figure 1), and self-reported non-Caucasian ethnicity. Exclusion criteria for SNPs
were genotype call rates <0.90, deviation from Hardy-Weinberg equilibrium (P<5x10-7) and
minor allele frequency (MAF) <0.005. Following QC procedures, 3,430 individuals and 127,830
autosomal SNPs were included in the discovery association analysis in IMPROVE.
Ultrasonographic Measurements
The carotid ultrasound protocol applied in IMPROVE and the precision of the ultrasonographic
MDC was performmmmedeee
dies were genotytytypepepepedddd
a n
e CardioMetaboch is a custom Illumina iSelect genoty ng array that captures
t v
c and atherosclerotic/cardiovascular endpoints, comprising approximately 200,0
MPROVE i di id l l l l i i i ll 0 95 l f id
a HuuumamamanHnHnHapapap555550000 array and imputed to thehehehe 111000Genomes CCCEUEEE Caucasian referen
e CCCardioMetabobobochhhipppp is aaa a custststomomm IIllumumminaa iiSelelelececcct t t t ggennnottypiingngg aaarrrray tttthahahahat caaapturuures
t regioioioi nsnsnsns iiidded ntttifififiiiei d dd bbby metatata-analysysseees off f GWGWGWGWA AA sttstst dududieieies fofofor dididiseasessss aaand tttraitititi s relell v
ccc aaandndd aaaththt erere osososclclc erere otototicicc/c/c/carara didid ovovovasasascucuculalaarr enene dpdpdpoioio ntntts,s,s, cccomomo prprp isissiningg g apapapprprp oxoxo imimatatatelele yy y 202000,0,0,000
MPROVE i di id l l l l i i i ll 0 95 l f id by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
7
measurements have been reported.10 In brief, measurements were made of the mean and
maximum IMT of the common carotid at the 1st cm proximal to the bifurcation (CC-1st cm-
IMTmean and CC-1st cm-IMTmax) and in a segment excluding the 1st cm proximal to the
bifurcation (CC-IMTmean and CC-IMTmax), of the bifurcation (Bif-IMTmean and Bif-IMTmax), and
of the internal carotid arteries (ICA-IMTmean and ICA-IMTmax). Composite IMT variables
considering the whole carotid tree were derived from the segment-specific measurements:
IMTmean, IMTmax, and IMTmean-max (the average of IMT maxima recorded at the different
segments).10 Measures of common carotid IMT were available in all replication cohorts, and in
addition, Bif-IMTmax was measured and a 6-level carotid plaque score was generated in the
MDC cohort (Supplemental Section S1 and Supplemental Table 1).
Statistical Analyses of the Discovery and Replication Cohorts
All cIMT variables were logarithmically transformed prior to statistical analysis due to skewed
distributions. Association analysis was performed using linear regression, adjusting for age and
sex, under the assumption of additive genetic effects using PLINK version 1.07.21 For
IMPROVE, the first three MDS dimensions (based on CardioMetabochip genotype data) were
used to adjust for identified population substructure (Supplemental Section S2 and
Supplemental Figure 1). The a priori threshold for array-wide statistical significance was
established as P<8.39x10-7 through estimation of the total number of uncorrelated SNPs on the
CardioMetabochip (Supplemental Section S3). Selection of index SNPs for replication from
candidate SNPs that obtained an a priori level for statistical association in the discovery analysis
(set to P<10-4 for segment-specific IMT measurements and P<10-5 for composite IMT variables)
was performed by the PLINK clump procedure. A linkage disequilibrium (LD) threshold of r2
>0.8 within a physical distance of 500 kilobases (kb) was used in the clump procedure.
eplication cohorts,,,, anaaa
was gggeneratttt ddded in nnn ththththe
r
A
variables were logarithmically transformed prior to statistical analysis due to skew
n e
the ass mption of additi e genetic effects sing PLINK ersion 1 07 21 For
rt ((((SuSuSupppppplelelememmm ntntnttal Section S1 and Supppplelelemmental Table 1).).).
AnAnAnA ala yses of thheee DDissscovvvveere y anaanddd RRepppliicattioon CoCoCoohohohh rttts
variablblbbleseseses wweree llologagaga iririthththmicacacalllllllly trannnsffsfsforororo memeddd pprioioiorrrr totoo ssstatititisststs icicii llalal anaalylylylysisisiis dudud ee totot sskkkew
ns. Association analyllyl siis was pepp rfffformed dd usinii g gg linear regggressioiii n,,, adjdjdjd ustinggg for aggge
theh ptiio fof ddddiitii iti fefffect iin PLPLININKK iio 11 0707 2121 FFor by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
8
Power calculations for the replication studies indicated that it would be justifiable to take
up to 50 uncorrelated SNPs forward to replication (Supplemental Section S4).
The replication stage comprised two approaches. The first approach involved meta-analysis of
the replication cohorts, both separately from and jointly with IMPROVE, using a fixed-effect
model with inverse variance weighting as applied in Metal (version 25 March 2011).22 Pooled
regression coefficients with corresponding 95% confidence intervals (CI) and P-values were
calculated. Two IMT phenotypes were studied in the replication stage. Primarily, 39 SNPs
associated with CC-IMT variables (CC-1st cm-IMTmean, CC-1st cm-IMTmax, CC-IMTmean, and/or
CC-IMTmax) and 3 SNPs associated with composite IMT variables (IMTmean, IMTmax, and/or
IMTmean-max) in IMPROVE were examined in relation to CC-IMT in the WH-II, EAS, MDC, RS-
I and RS-II cohorts (total n=11,590). Additionally, 26 SNPs associated with Bif-IMT in
IMPROVE were investigated in relation to Bif-IMT in the MDC cohort (n=1,690).
Given that the composite IMT-measures were unique to IMPROVE and thereby not
assessable by conventional replication in independent cohorts, we applied nonparametric
bootstrap re-sampling to perform internal validation. 23In brief, this method uses a weighted
average over bootstrap replicates of the difference between the effect size estimated from the
observations in the bootstrap sample and the one estimated from the observations not in the
bootstrap sample to estimate the over-estimation of the effect sizes of the most significant SNPs
(Supplemental Section S5).
Secondary Analyses
Regional plots of associations from the original discovery analysis and adjusted analysis where
the lead SNP was included as a covariate in the regression model were generated using
LocusZoom (http://csg.sph.umich.edu/locuszoom/). Secondary analyses to assess potential
MTmax, CC-IMTmeanananan,,, , a
MTmean, IMIMIMIMTTTTmax, anananandddd/
x C
en that the composite IMT-measures were unique to IMPROVE and thereby not
b con entional replication in independent cohorts e applied nonparametric
x) innnn IIIMPMPMPMPROROROROVEVEVEE were examined in relatiiiionoon to CC-IMT in thththhe WH-II, EAS, MDC
ccoc hhhorts (totall nnn=11,,,5990000))).) Addddddid tttioonallllyy, 2626 SNPNPNPs s s s aassooocciateeded wwwitititthhh h Biiiif-f-f-IMMI TTT T innn
wereee ininininvvvev stigigi tatatededd iiinn relatititionononon to BiBiBiB ffff I-IIIMTMTMTT iiinn thhheeee MDMDMDMDCCC coococohohohh ttrtrt (n==11,11 6966690))). fffff
en that the compopp iisiite IIIMTMMT-measures were uniquqq e to IIMPMPMPROROROOVEVEVE and therebyy not
bbb iti lal lili iti ii iindde dnd t hhort lpliiedd et iri by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
9
pleiotropy and possible confounders were performed by investigating genotype associations with
biochemical and clinical parameters (including 13 variables reflecting established cardiovascular
risk factors: waist circumference, systolic and diastolic blood pressure, pulse pressure,
hypertension, LDL-cholesterol, HDL-cholesterol, triglycerides, blood glucose, diabetes, C-
reactive protein, statin treatment, and cumulative life-time smoking expressed as a 5-level
categorical variable according to never-smoker status and quartiles of pack-years), and by further
adjustments of the original model (adjusted for sex, age and MDS) using PASW Statistics
version 18.
CAD Case-Control Studies
To determine whether a locus robustly associated with cIMT is also implicated in the
pathogenesis of clinically manifest CAD, we explored the lead SNP identified at the level of
array-wide statistical significance in relation to cIMT (rs4888378) for associations with CAD in
the PROCARDIS and CARDIoGRAM case-control studies.18, 19 Design features and details of
genotyping, QC and statistical analyses are provided in online Supplemental Sections S1 and
S6.
Association with Coronary Artery Calcium Score
Associations of the lead SNP with CAC score measured by a C-150 Imatron scanner in RS-I 24
and a 16- or 64-slice MDCT scanner in RS-II25 was evaluated by fixed-effect model meta-
analysis with inverse variance weighting using Metal.22
Expression Quantitative Trait Locus (eQTL) Studies
In silico analyses of genotype-gene expression level associations were conducted in the ASAP
and BiKE data sets. Details of design features and methods for ASAP and BiKE have been
reported.20 In ASAP, mRNA extracted from biopsies of ascending thoracic aorta intima-media
n
is of clinical manifest CAD, we ex ored the lead SNP identified at the level o
A
A l
QC and statistical anal ses are pro ided in online S pplemental Sections S1 a
ne wwwheheheethththhererer a lllocococus robustly associated wwwititii h h cIMT is also iiimpmm licated in the
iss oooof clinicallyy mmmannififififest t t t CCAC D,DDD wwwee exxxpploreded thehehe llleeaee dd d SNSSNP idddeeenttit fffif ed aaaat tt thhheee levevvel o
statiiiistststicicicicalalala siggniniifififificacancncee in rrrelelelelation nn tototo ccccIMIMIMMTTT (r(r(( s4s4s48888888883383837888))) fffoforr asassociciciciatatatiiioi nss wititith hhh CCCA
ARDIS and CARDRRDIoII GRGRGRRAMAMAMM case-contr lloll studidd es.1818181 , 19191919 DDe isiigngg fffeatures and detail
QCQC dd statiis iti ll lal iiddedd iin lnliine SSupplleme tnt lal SSectitions S1S1 a by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
10
(n=138), aortic adventitia (n=133), mammary artery (n=89), heart (n=127), and liver (n=211)
from patients undergoing aortic valve surgery20 was analysed with Affymetrix ST 1.0 Exon
arrays. In BiKE, RNA extracted from human plaque tissue (n=126) and peripheral blood
mononuclear cells (PBMC; n=96) obtained from patients referred for surgical treatment of severe
carotid artery stenosis, was analysed with Affymetrix HG-U133 plus 2.0 Genechip arrays.20
Robust Multichip Average (RMA) normalization was performed as implemented in the
Affymetrix Power Tools 1.10.2 package apt-probeset-summarize and processed gene expression
data was returned in a log2-scale.20 For both studies, blood-derived DNA had been genotyped
with Illumina 610w-Quad BeadArrays. Genotype-gene expression associations were investigated
using an additive model. 20
Results
Discovery Analysis
A total of 3,430 subjects (54 to 79 years of age, 48% males) from the IMPROVE study were
included in the discovery analysis. Basic characteristics of IMPROVE study participants are
shown in Supplemental Table 1. Since MDS analysis revealed significant population
substructure in IMPROVE (Supplemental Figure 1), adjustment for the first three MDS
dimensions, in addition to age and sex, was performed in all SNP association analyses with
cIMT measures. Associations with segment-specific mean and maximum IMT were investigated
as well as composite IMT variables reflecting the whole carotid tree (Figure 1 and
Supplemental Figure 2 a-k). One locus on chromosome 16 (lead SNP rs4888378, MAF=0.43,
P=6.75x10-7, beta [SE]= -0.019 [0.004] versus IMTMax for the minor A allele) passed the array-
wide significance threshold of P<8.39x10-7 (Figure 1). Rs4888378 is located in the last 3’ intron
of the CFDP1 gene (encoding cranio-facial development protein-1). A Q-Q plot of observed
NA had been genooootytytytyp
ociattttioiii ns were invevevevest
d 20
A
,430 subjects (54 to 79 years of age, 48% males) from the IMPROVE study wer
dditiiiiveveve mmmodododdeleee . 2020200
Analysis
,4,43030 ssububjejecttctss (5(5(54 44 totot 779 99 yeyeararss offof aagege,, 48488% %% mamaleles))s) ffroromm thhthee IMIMIMPRPRROVOVOVEEE ststududyy wewer
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
11
versus expected P-values from the analysis of IMTmax is presented as an insert in Figure 1. The
genomic inflation factor (lambda) in the analysis of IMTmax was 1.05, indicating an adequate
correction of population substructure by the MDS-adjustment.
SNPs associated with any of the 4 CC-IMT measures at P<1x10-4 (a set of 46 SNPs) or
any composite IMT measure at P<1x10-5 (a set of 4 SNPs) were considered as candidates for
replication with respect to CC-IMT in independent cohorts (i.e a total of 50 SNPs). From these,
index SNPs were selected using the PLINK clump procedure, performed once for each set of
candidate SNPs, resulting in 39 index SNPs selected among the 46 SNPs that were associated
with CC-IMT measures at P<1x10-4 (designated CC-IMT SNPs, Supplemental Table 2) and 3
index SNPs selected among the 4 SNPs that were associated with composite IMT measures at
P<1x10-5 (Table 1) (designated composite IMT SNPs). Similarly, 26 index SNPs associated with
either of the 2 Bif-IMT measures (designated Bif-IMT SNPs) were generated from 52 candidate
SNPs associated at P<1x10-4 (not shown). For SNPs that passed the initial significance criteria
for more than one cIMT variable of the same category (CC-IMT, Bif-IMT, or composite IMT,
respectively), the most significant association was considered for the clump procedure.
Replication and Internal Validation
A replication stage investigating associations with CC-IMT of the identified 39 CC-IMT SNPs
and 3 composite IMT SNPs was undertaken in five independent population-based cohorts from
Sweden, the United Kingdom, and the Netherlands (total n=11,590). Basic characteristics of
participants in the replication cohorts are shown in Supplemental Table 1. In the replication
meta-analysis of the CC-IMT SNPs, no SNP was significantly associated with CC-IMT
(Bonferroni correction for 42 independent tests P<0.0012; lowest observed P=0.007;
Supplemental Table 2). In contrast, the association of the composite IMT SNP rs4888378 with
NPs that were assocccciaiaiai t
pleme tntttallll TTTaT blblblb e 2222)))) a
s s
T e
e d
c t
an one cIMT ariable of the same categor (CC IMT Bif IMT or composite IM
s seeelelelelectcttctedededed aaamomomonngn the 4 SNPs that were asasasassoociated with compmpmposite IMT measures
Taaaabbblb e 1) (desiggnnnateeddd d compmmm osssititite IMMTTT SSNPsPs). SSSimimimiili aarlyyy,, 26 innndexexex SNPNPNPNPs ss asasassoccciaate
e 2 BiBBiBiffff-IMIMMIMT memeasasurureses (((deded sisiisiggggnatededed BBBBifififi -ff IMMMIMTT TT SNSNSNNPsPPsPs))) wewereerere ggeneneeratttedededed ffffrom m 5255252 ccanand
ciated at P<1x10000-444 ((((not hhshown)n)). FFFor SNSNSNS PsPP thhhah t papp ssedddd thheh iii iniii iitiialll sigigii nificance crit
a IcIMTMT iiablbl fof thhe te ((CCCC IMIMTT BBifif IMIMTT iit IMIM by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
12
CC-IMT (P=7.24x10-6; Table 1) passed Bonferroni correction in meta-analysis of the replication
cohorts (i.e. P<0.0012). This index SNP also achieved array-wide significance in combined
meta-analysis of IMPROVE and replication cohorts (P=3.51x10-7). The associations of
rs4888378 with CC-IMT in all individual cohorts and in the meta-analyses are illustrated in
Figure 2. The two other composite IMT SNPs that were selected at the P<1x10-5 level reached
nominal significance in the replication cohorts (Table 1). None of the Bif-IMT index SNPs were
significantly associated with Bif-IMT in the MDC cohort after Bonferroni correction for 26
independent tests (all P>0.0019). The internal validation of the 3 composite IMT SNPs by non-
parametric double bootstrap confirmed significant associations with composite IMT (bootstrap
beta with 98.33% confidence intervals to account for analysis of 3 independent SNPs: -0.0094 [-
0.0200, -0.0034] for rs4888378, -0.0083 [-0.0166, -0.0035] for rs1001861, and 0.0056 [0.0018,
0.0131] for rs200991; Supplemental Figure 3).
Secondary Analyses in the Discovery Cohort
The replicated lead SNP rs4888378 in the chromosome 16 locus was evaluated in greater detail
in the IMPROVE cohort. Regional association plots for IMTmax (Figure 3) indicated the
presence of only one single association signal (rs4888378 in the IMPROVE cohort), centered
over the 3’ end of the CFDP1 gene. Potential pleiotropy and possible confounders were assessed
by investigating associations of rs4888378 with biochemical and clinical parameters. To the best
of our knowledge, rs4888378 was included on the CardioMetabochip due to previous
associations with systolic blood pressure. However, in IMPROVE this association was not
confirmed (P=0.12). Cumulative life-time smoking (pack-year categories) was found to differ
between genotype groups (Kruskal-Wallis P=0.0067). Adjustment for pack-year categories, in
addition to age, sex, the first three MDS dimensions, and 12 additional variables reflecting
posite IMT SNPs bybybyby n
ompositititite IMIMIMIMTT TT (b((b(boooooooottttst
8 0
003 for rs4888378, -0.0083 0.0166, -0.003 for rs1001861, and 0.0056 0.0
ated lead SNP rs4888378 in the chromosome 16 loc s as e al ated in greater d
8.33%3%3% cococonfnfnfnfidenenence intervals to account fofofoforrr analysis of 3 indededeependent SNPs: -0.00
0003034] for rs48888837878788, -00-0.00.0083333 [-000.0166666, -00.0003335]5]5] fffoor rrrs11001818186111,, and ddd 000.0 00055565 [000.0 0
rs2000009909099191919 ; SuSuS pppppplelelememementalalal FFFFiiigi ure ee 3333)).
Analysyy es in the DiDiiscovery yy CoC hhhort
at ded ll dd SNSNPP 48488888373788 iin thhe hhr 1616 ll ll at ded ii te dd by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.112.963660
13
established cardiovascular risk factors (see Methods) did not have a major impact on the original
cIMT association of rs4888378 (P=2.7x10-6 for IMTMax), indicating that this association signal is
not mediated by established cardiovascular risk factors.
Investigation of rs4888378 in relation to segment-specific IMT measurements in
IMPROVE showed that rs4888378 was most strongly associated with Bif-IMT (P=1.13x10-5 for
Bif-IMTmax), whereas the weakest association was seen with CC-IMT (P-values for the 4 CC-
IMT variables ranging from 0.010 to 0.038), the ICA-IMT association being intermediate
(Supplemental Table 3).
Association with Other Cardiovascular Phenotypes
The lead SNP rs4888378 in the chromosome 16 locus was further investigated for associations
with carotid plaque score in the MDC study, with CAC score in the Rotterdam studies, and with
CAD risk in PROCARDIS and CARDIoGRAM. Since the association of rs4888378 with CC-
IMT was consistent across the investigated cohorts (Table 1, Figure 2), no significant between-
cohort heterogeneity was expected with respect to associations with other related cardiovascular
phenotypes. Accordingly, fixed-effects (rather than random-effects) models were considered
appropriate for meta-analyses of the CAC score in the Rotterdam studies and of CAD in
CARDIoGRAM. The minor A allele of rs4888378 (which was associated with thinner IMT) was
weakly associated with a lower carotid plaque score (beta [SE]=-0.046 [0.023], P=0.04, n=2120)
in the MDC study and showed a tendency towards lower CAC score in meta-analysis of RS-I
and RS-II (beta [SE]=-0.11 [0.06], P=0.06, n=2,948). Furthermore, the thinner-IMT allele was
associated with decreased risk for CAD and MI in PROCARDIS and CARDIoGRAM (odds
ratio [95%CI] 0.83 [0.77-0.90] for all CAD and 0.84 [0.77-0.91] for MI in PROCARDIS, and
0.95 [0.92-0.98] for all CAD and 0.96 [0.93-0.99] for MI in CARDIoGRAM) (Figure 4).
NP rs4888378 in the chromosome 16 locus was further investigated for associati
d plaque score in the MDC stu , with CAC score in the Rotterdam studies, and
n C
o w
rogeneit as e pected ith respect to associations ith other related cardio as
NP rrrs4s4s4888888888383383787878 iiiinn n the chromosome 16 locucucuss was further invevevestigated for associati
d plllaque scoree innn thehehee MDCDCDD stutut dyyy, witthh CACA sscocooorererer in thhe RoRoRotteere dddad m ststtudddieieiei s, annd
n PRRRROCOCOCOCARARARA DIDIDISSSS ananddd CACC RDRDRDDIIIoIoGRRRRAMAMAMAM. SiSiSiincncee thththeeee assssssos ciciciatatatatioionn ofo rs4s4s4s4888888883337878788 wititithhh C
onsistent across thehh iiiinves itiigagg ted ddd cohoh rts (((TaT blbb e 1,11,1 FFFigiigi ure 2222),)),) no signgg ificant betw
ieit tedd ii hth ct t iciatiio iithh othhe llatedd drdiio by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
14
Association with Expression in Target Tissues
Global gene expression data from five different tissues (aortic intima-media, aortic adventitia,
mammary artery intima-media, PBMC, and carotid plaque) were used to link individual genes to
the cIMT-associated locus discovered in this study. We investigated associations between
genotype and expression levels of all genes located within ±200 kb of the lead SNP rs4888378.
A total of 9 genes were contained within this region, 8 of which were captured by the microarray
analysis (Supplemental Figure 4). The most significant allele-specific difference in gene
expression level according to rs4888378 genotype was observed for TMEM170A
(transmembrane protein 170a) (in aortic intima-media, P=0.000569, n=138, and adventitia,
P=0.000576, n=133, respectively; Figure 5) Two more genes were differentially expressed at
nominally significant levels, BCAR1 (breast cancer anti-estrogen resistance-1) in carotid plaque,
P=0.00749, n=126, and LDHD (lactate dehydrogenase D) in aortic intima-media and adventitia,
P=0.0459, n=138, and P=0.00836, n=133, respectively (Figure 5). However, strictly considering
multiple testing of 8 genes in 7 different tissues, a P-value of <0.00089 should be held
statistically significant; this threshold was reached only for TMEM170A. No significant genotype
association was observed with expression levels of CFDP1 (lowest observed P=0.0693, n=133,
for aortic adventitia; Supplemental Figure 4).
Discussion
In this study, we investigated genetic determinants of cIMT, a widely accepted marker of
subclinical atherosclerosis, applying a two-stage discovery and replication study design
involving more than 15,000 subjects. We identified a novel locus on chromosome 16 (lead SNP
rs4888378), the minor allele of which was associated with thinner cIMT and decreased risk of
CAD in subjects of European ancestry. The association with CAD was stronger in PROCARDIS
MEM170A
=138888, and ddd dadddventtttititititiaiaiaia,
6 d
s
, n
n d
sting of 8 genes in 7 different tiss es a P al e of <0 00089 sho ld be held
6, nnn=1=1=133333333, rereresppeecectively; Figure 5) Two mmomorre genes were dddifififffefff rentially expressed
siiiigngngnnificant leveellls, BCBCCARRRR111 (brrrreeassst cannnccer ananti-esesestrtrtrtrogogoo ennn rresisstaaancncnceee-1) inininin cararrotiiddid pl
, n=12112126666, aand LDLDLDL HDHDHDH (((lall ctttatatateeee ddddehyyydrdrdrogogogogennasasee DDD)))) iiiin aaaortititicccc inini tititimma-mememmedidididia ananddd d adddadveven
n=138, ,, and P=000 0.0008080808363636,,, n=11131 3,3,3 respepp ctiiivi lelly yy (((Figugg re 55).).) HoHH wever,,, strictly yy consid
iti ff 88 iin 77 ddififffe nt tiis a PP lal ff 0<0 0000008989 hho lldd bbe hheldld by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
15
than in CARDIoGRAM, which may reflect the fact that PROCARDIS recruited cases from
CAD-enriched families, thereby potentially enhancing the impact of genetic risk factors. We
also identified allele-specific differences in the expression of nearby genes in vascular tissues
according to rs4888378 genotype. Thus, investigation of genetic determinants of cIMT resulted
in discovery of a novel CAD risk locus and novel candidate CAD susceptibility genes that merit
further investigation.
A recent meta-analysis of SNP-based GWA studies of cIMT conducted by the CHARGE
consortium discovered three regions associated with CC-IMT.6 In IMPROVE, the lead SNPs for
the three IMT-associated loci identified by CHARGE were associated with cIMT , albeit at
significance levels that did not qualify for inclusion in the replication stage of our study
(investigated directly or by proxy; data not shown). The fact that our lead SNP rs4888378 was
not identified by the CHARGE consortium may reflect differences in study design and IMT
phenotyping. Specifically, rs4888378 was selected for replication in our study based on its
association with composite IMT, and among individual segments rs4888378 proved to be most
strongly associated with Bif-IMT; neither of these IMT phenotypes were analysed by the
CHARGE consortium.
It is noteworthy that established CAD loci19, 26, 27 neither appeared as major determinants
of cIMT in the current study, nor in the study reported by the CHARGE consortium.6 Thus it
appears that the impact of these loci that confer risk of clinically manifest CAD may not be as
strong in early subclinical atherosclerosis.
Our results suggest that the observed associations may be due to an influence of
rs4888378, or linked variants, on the expression of nearby gene(s) in the arterial wall. The
expression of CFDP1, the gene harbouring rs4888378 in its last 3’ intron, showed no allele-
PROVE, the lead SNSNSNSNP
with hhh cIIIIMTMTMTMT , alblll eieieieittt t at
e
ed direct or proxy; data not shown The fact that our lead SNP rs4888378 w
ed by the CHARGE consortium may reflect differences in study design and IMT
ith composite IMT and among indi id al segments rs4888378 pro ed to be m
e levevevelelelsss thththt atatat didididd not qualify for inclusion nn inin the replicationn stststage of our study
edd d dddirectly or bybyby prroxxxy; dadadad ta nnnot shhownwwn). TThe fffacaccctt tt thththattt oour llleeead dd SSSNS PP rsss488888888 373737378 w
ed bbbby y ththththeee e CHCHCHARARARRGEGEGE cconsooortrtrtrtiiiium mamamay yyy reflflflflecect ttt dididifffffffferrrenenenceeessss inn sstttutudy ddddeesesign n anand ddd IMIMIMT
g.gg Spepp cifically,y,y, r 4s4448888888 8383833787878 was s lellecteddd d fofff r replp icatioiii n iiini our studydydd based on its
ii hth isite IIMTMT dd iindidi iidd lal nt 48488888373788 ded t bbe by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
16
specific association with rs4888378. The biological role of TMEM170A, the expression of which
showed the strongest association with rs4888378, is currently unknown. In silico sequence
analysis predicts that the TMEM170A protein consists of an extracellular N-terminal part, three
transmembrane helices, and a short cytoplasmic C-terminal tail (MEMSAT-SVM;
http://bioinf.cs.ucl.ac.uk). In contrast to TMEM170A, BCAR1 (also known as p130CAS) has been
extensively studied and ascribed important roles in processes such as cellular adhesion,
migration and proliferation/survival e.g. in vascular smooth muscle cells (VSMC) 28, 29, and thus
has a biologically plausible role in atherogenesis. In silico analysis of the genomic sequence
surrounding rs4888378 predicts that rs4888378 may influence the binding of transcription
factors (YY1 and NF-1; TESS software, http://www.cbil.upenn.edu/cgi-bin/tess/tess). YY1 is
expressed in human carotid atherosclerotic lesions and has experimentally been ascribed roles in
VSMC injury responses and neointima formation.30, 31 Accordingly, it is tempting to speculate
that one mechanism underlying the association between rs4888378 and cIMT and CAD risk
would be influence of rs4888378 on YY1-regulated transcription of BCAR1 in VSMC, with
downstream effects on VSMC function. The BCAR1 locus is further indicated by the discovery
stage composite IMT index SNP rs100861 which maps close to the BCAR1 gene. Interestingly,
another intronic SNP in the CFDP1 locus has been associated with markers of chronic
obstructive pulmonary disease (COPD).32 This SNP (rs2865531) is in strong LD with rs4888378
(r2=0.967 in the HapMap CEU reference panel; not present on the CardioMetabochip). The
BCAR1-CFDP1-TMEM170A locus is thus implicated in both atherosclerotic cardiovascular
disease and COPD, two pathologies which both have strong inflammatory components and
involve tissue remodeling including dysregulation of SMC phenotype and function, and that
exhibit pronounced co-morbidity.33
the genomic sequeeeencnnn
ding offff ttttranscripipipi tititiionononon
Y 1
n o
u l
echanism underlying the association between rs4888378 and cIMT and CAD risk
nfl ence of rs4888378 on YY1 reg lated transcription of BCAR1 in VSMC ith
Y1 aaandndndn NNNNF-FF-111; TETETETESS software, http://wwwww.cbc il.upenn.edu/cccgiggg -bin/tess/tess). YY1
nnn huuumu an carottiddd athththherosssscclc erotootiici leesiooonns andnd hhhaas eexee pperrrimmenntaaallyyy bbbbeennn n aaascrcrcriiibi edededd ro
ury resesespopopoponnnsess aa ddndnd nneoeoiiintimimmaaaa fffformmmattatatioioioionnn.3030300,,, 31131 AAAcccccccororordiididinggglyylyly, iiittt iiisis tempmpmmptitititingg tttoo spspececulu
echanism underlyllyl inii g gg hthhhe associatiioi n bbebb tween rs4888888888883737373 8888 and ddd IcIMTMTMT and CAD risk
nffll ff 48488888373788 YYY1Y1 llat ded t iip iti ff BCBCARAR11 ii VSVSMCMC iith by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
17
A major strength of the current study is the extensive and thoroughly standardised
ultrasound examination performed in the discovery cohort (IMPROVE). The fact that SNPs
selected for replication based on their association with composite IMT variables performed better
at the replication stage than those selected based on their associations with CC-IMT, suggests
that these composite variables are of particular value. However, some limitations of the present
study should also be considered. Differences in ultrasonographic protocols exist between the
participating cohorts. For example, CC-IMT was not measured in exactly the same way in all
cohorts. Furthermore, recruitment protocols differed between studies. Whereas the IMPROVE
study recruited high-risk individuals (with at least three established vascular risk factors), the
WH-II study recruited healthy subjects, and the MDC, EAS and Rotterdam studies enrolled
population-based subjects. These between-cohort differences may have obscured associations
that remain undetected in the present study.
Conclusions
This study identified rs4888378 in the BCAR1-CFDP1-TMEM170A locus on chromosome 16 as
a novel genetic determinant of cIMT and CAD risk in individuals of European ancestry. Further
investigations, including experimental studies, are needed to fully clarify the biological
mechanisms underlying the current findings.
Acknowledgments: The authors fully acknowledge the thousands of study participants who volunteered their time to help advance science and the scores of research staff and scientists who have made this research possible. The Edinburgh Artery Study would particularly like to acknowledge all EAS staff and participants. The authors representing the Rotterdam Study are very grateful to the participants and staff from the Rotterdam Study, the participating general practitioners and the pharmacists. Whitehall-II genotyping was in part supported by a MRC-GSK pilot programme grant (ID 85374). David Altshuler, Sekar Kathiresan and "The Pfizer Broad-Massachusetts General Hospital-Broad Genetics Collaboration" are acknowledged for supporting the genotyping in the Malmö Diet and Cancer Study. Members, sources of funding, and
Whereas the IMPRRRROOOO
scular riisii k kkk ffffacttttors)s)s)s), th
d d
- o
n
n
dy rrrecececrururuititititedededd heeeealalalalthy subjects, and the MDDDC,CC EAS and Rotteerdrrr am studies enrolled
-bbbbassssed subjectss. Thhheh sse bbbbeteetweeeeen-cooohooortt diffffereencncccesesese mayaay havveee obobbssscuredededed aaassssociaiaiai tio
undeddedeteteteectctctc ed iiinn thhththe e prprese enttt ststststudy.
nnnss
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
18
disclosures of the CARDIoGRAM consortium are listed in Supplemental Section S7. Members of the PROCARDIS consortium are listed in Supplemental Section S8. Members of the writing group and affiliations by participating study are listed in Supplementary Section S9.
Funding Sources:The IMPROVE study was supported by the European Commission (Contract number: QLG1-CT-2002-00896), the Swedish Heart-Lung Foundation, the Swedish Research Council (projects 8691 and 0593), Knut and Alice Wallenberg Foundation, the Torsten and Ragnar Söderberg Foundation, the Swedish Foundation for Strategic Research, the Stockholm County Council (project 562183), the Strategic Cardiovascular and Diabetes Programmes of Karolinska Institutet and Stockholm County Council, Academy of Finland (Grant #110413), Ministry of Education and Culture of Finland, the City of Kuopio, the British Heart Foundation (RG2008/014) and the Italian Ministry of Health (Ricerca Corrente). The UCL Genetics Institute supported D.Z., and S.S., and. S.E.H was supported by the BHF (RG2008/08). The Rotterdam Study was funded by the Erasmus Medical Center and Erasmus University, Rotterdam, Netherlands Organization for the Health Research and Development (ZonMw), the Research Institute for Diseases in the Elderly (RIDE), the Ministry of Education, Culture and Science, the Ministry for Health, Welfare and Sports, the European Commission (DG XII), and the Municipality of Rotterdam. The Rotterdam GWA study was funded by the Netherlands Organisation of Scientific Research (NWO, De Nederlandse Organisatie voor Wetenschappelijk Onderzoek) Investments (number 175.010.2005.011, 911-03-012), the Research Institute for Diseases in the Elderly (014-93-015; RIDE2) and the Netherlands Genomics Initiative (NGI)/Netherlands Consortium for Healthy Aging (NCHA) project number 050-060-810. The present work was further supported by an NWO grant (vici, 918-76-619). The Whitehall-IIStudy was supported by the Medical Research Council, the British Heart Foundation, and the US National Institutes of Health (R01HL36310). S.E.H and P.J.T were supported by BHF RG005/014. The Malmö Diet and Cancer Study was supported by the Swedish Research Council, the Swedish Heart-Lung Foundation and the European Research Council (ERC-StG-282255). The Edinburgh Artery Study was financed by the British Heart Foundation and the Chief Scientist Office of the Scottish Executive Health Department. The ASAP Study was supported by the Swedish Research Council (12660), the Swedish Heart-Lung Foundation (20090541), the European Commission (FAD, Health F2 2008 200647) and a donation from Fredrik Lundberg. The BiKE Study was funded by the Swedish Heart-Lung Foundation, the Swedish Research Council, the European Commission (AtheroRemo (FP7-HEALTH-2007-A-201668), the AFA Foundation, and the Torsten and Ragnar Söderberg Foundation. PROCARDIS was supported by the European Community Sixth Framework Program (LSHM-CT- 2007-037273), AstraZeneca, the British Heart Foundation, the Wellcome Trust (Contract No. 090532/Z/09/Z), the Swedish Research Council, the Knut and Alice Wallenberg Foundation, the Swedish Heart-Lung Foundation, the Torsten and Ragnar Söderberg Foundation, the Strategic Cardiovascular Program of Karolinska Institutet and Stockholm County Council, the Foundation for Strategic Research and the Stockholm County Council. M.F and H.W. are supported by the British Heart Foundation Centre of Research Excellence. M S-L is a recipient of a Marie Curie Intra European Fellowship within the 7th Framework Programme of the European Union (PIEF-GA-2009-252361).
Conflict of Interest Disclosures: Stela McLachlan reports stock ownership interest in Pfizer. Mika Kivimäki reports receiving research grant support from NHLBI (R01HL36310; principal
ZoZoZoZonMnMnMnMw)w)w)), ,,, ththththe e e ReReReReseseseseararararccccn, Culululultutututurererere aaaandndndnd SSSScicicic enenenenccceceDG XIIIIII ),),),), aaandndnd ttthehehehe
ty of Rotterdam. The Rotterdam GWA study was funded by the Netherlandson of Scientific Research (NWO, De Nederlandse Organisatie voor Wetenschapp) Investments (number 175.010.2005.011, 911-03-012), the Research Institute fo
nherlands Consortium for Healt A ng NCHA pr ect number 050-060-810. Tr Isupported by the Medical Research Council, the British Heart Foundation, and t
n4
ty of Rotterdam. The Rotterdam GWA study was funded byyy the Netherlands on ooof ff f SScientnntntiifi iccc RRResearch (NWO, De Neddderrlandse Orggganaa isatattiiie voor Wetenschapp) IIInvnvnvestmentss (((nunnumbmbmbbereer 1757575.0.0.001010100.2.2.200000005.5.5.5 0100 1, 91111-000-033-3-3-0111012)2)2)2 , thththhee Reesesesesearaararchchchch IInnsnstititit tutututettete fo thththeee e Elderly (010114-999333-0111155;5 RIDE2EE2) annndd thhe Neeeththhthererererlaandddss Geenoomimimiics Innnin ttit aaatiive
herrrlalalalandndnds CooCoonnnsorororrtitt ummumm forrr HHHeaeaeaealtltltl hyhyhyy AAAgigigigingngng (((NCNCN HAHAHAH ))) prprprrojojojecececcttt t nuunumbmbmberererer 05050500-0606060-8101101 . Trk was further sssupuuppopp rteddd bby yy an NWO ggraaantn (vici,,, 919 8-76-619919).)) The Whitehall-Isupported by ththththe ee e MeMMeMedididiicacacac ll ReReReReseseseeararaarchchchh CCCCououououncncncilililil, ,, the eee BrBrBrBrititititisiiish hh HeHeHeH ararara t tt FoFoFoFouuundation, and t
nssstitititutututetetesss ofofof HHHeaeaealtltlthhh (R(R(R010101HLHLHL3636363131310)0)0). SSS.EEE.HHH anananddd PPP.JJJ.TTT wewewererere sssupupuppopoportrtrtededed bbbyyy BHBHBHFFF 4. The Maalmlmmöö DiDiDiDietett aaandndd Cananancecer rr StStStudududyyy wwwasass supupppopoportrttedededed bbby yy thththhe ee SwSwSwwededede isisisish hhh ReR searchh
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
19
investigator). John Deanfield reports receiving research grant support from the British Heart Foundation and Medical Research Foundation, and honoraria payment and payment for speaker’s bureau appointments (Novartis, Roche, Merck, Danone, Pfizer). Benjamin Voight reports receiving research grant support from NIH (A GWAS for early onset myocardial infarction; post-doc) and an industry grant (Toward therapeutical markers for MI in a T2D background; post-doc). Meena Kumari reports receiving research grant support from the British Heart Foundation (PG1041133124260, RG1081008), NIH (AG13196), Medical Research Council, and NHLBI (HL36310). Anders Gabrielsen was employed by Bayer after completion of the study. Ulf Hedin reports consultant relationship with Cardoz AB. Kristiina Nyyssönen reports receiving research grant support from the Academy of Finland for the IMPROVE study (Grant #110413). Philippe Giral reports receiving Hospital Clinical Research Programme (PHRC) research grant support, awarded by the French Health Ministry. Robert Clarke reports receiving research grant support from the British Heart Foundation. Maria Grazia Franzosi reports receiving research grant support from the European Commission 6th Framework Programme as collaborator in the PROCARDIS project. Aroon D. Hingorani reports receiving research grant report from the British Foundation. Damiano Baldassarre reports receiving research grant support from the European Commission (Contract number: QLG1-CT-2002-00896) for the IMPROVE study. Elena Tremoli reports receiving research grant support from the European Commission (Contract number: QLG1-CT-2002-00896) for the IMPROVE study. Steve E. Humphries reports receiving research grant support from the British Heart Foundation (RG2008/08, programme and project grants on cardiovascular genetics) and European Commission 7th Framework Programme on diabetes, and discloses speakers' bureau appointment payment (Genzyme meeting on FH, Amsterdam November 2011) and one consultant/advisory board relationship (Store Gene, a CHD-risk genetic testing University College London spin-off company).
References:
1. Simon A, Megnien JL, Chironi G. The value of carotid intima-media thickness for predicting cardiovascular risk. Arterioscler Thromb Vasc Biol. 2010;30:182-185.
2. Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, et al. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the american society of echocardiography carotid intima-media thickness task force. Endorsed by the society for vascular medicine. J Am Soc Echocardiogr.2008;21:93-111.
3. Amato M, Montorsi P, Ravani A, Oldani E, Galli S, Ravagnani PM, et al. Carotid intima-media thickness by b-mode ultrasound as surrogate of coronary atherosclerosis: Correlation with quantitative coronary angiography and coronary intravascular ultrasound findings. Eur Heart J.2007;28:2094-2101.
4. Lorenz MW, Markus HS, Bots ML, Rosvall M, Sitzer M. Prediction of clinical cardiovascular events with carotid intima-media thickness: A systematic review and meta-analysis. Circulation.2007;115:459-467.
ngorani reports rececececeiviiirrrre eee rerererepopopoportrtrtrtsss s rerererececececeivivivivinnnngggg ber: QLQLQLQLG1G1G1G1-CTCTCTCT-222000000002222-arch ggggrarararantntntnt ssssupupupuppopopoportrtrtrt fffro
C yumphries reports receiving research grant support from the British Heart Founda
o nGenzyme meeting on FH, Amsterdam November 2011) and one consultant/advisionship (Store Gene, a CHD-risk genetic testing University College London spin
Commmmimimimissssssioioion nn (CCCCoono tract number: QLG1-CTCTCT-2-- 002-00896) foror ttthe IMPROVE studyummmmppphp ries repepepepororrortsttt rececececeieieivivvv ngngng rrrresesese eaeaeaearcrcrch hhh grgrgrg antt ssupppporororort t t t fromomomom ttthehehe BBBBritiiiishshshsh HHHHeartrttrt FFFouououundnnn a8888, ppprp ogrammee aaand ppprojjececece t grrraantss on caardioiovascscululularr geneeneticcsss) aaandnnn Eurururu opopopeaaan
on 777thtt Frameeewowow rrrk PProoogramaammee oonnn ddiabbbeetess, aanddd dddiscsclosesses spsppeaaakekersrsrs' buuurerereaauu appppooinGenzyyymemememe meeetititingngng oonn FHFF , AmAmAmAmsterdaddadammmm NNoNovevembmbmberererer 2220101010 1)1)1) aandndd oonne ccccononono sultttanant/t/t/addad ivivisionship (Store GeGGeG nenenee,, a a a CHCHCHC D-D-D-D-riririsksksksk gggenenenenetete icicic ttesesesstititit nngn UUUUninininivevevev rsrsrssitititity y y CoCoCoC lllllllegegegege London spin
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
20
5. van der Meer IM, Bots ML, Hofman A, del Sol AI, van der Kuip DA, Witteman JC. Predictive value of noninvasive measures of atherosclerosis for incident myocardial infarction: The rotterdam study. Circulation. 2004;109:1089-1094.
6. Bis JC, Kavousi M, Franceschini N, Isaacs A, Abecasis GR, Schminke U, et al. Meta-analysis of genome-wide association studies from the charge consortium identifies common variants associated with carotid intima media thickness and plaque. Nat Genet. 2011;43:940-947.
7. Paternoster L, Martinez-Gonzalez NA, Charleton R, Chung M, Lewis S, Sudlow CL. Genetic effects on carotid intima-media thickness: Systematic assessment and meta-analyses of candidate gene polymorphisms studied in more than 5000 subjects. Circ Cardiovasc Genet. 2010;3:15-21.
8. Fox CS, Cupples LA, Chazaro I, Polak JF, Wolf PA, D'Agostino RB, et al. Genomewide linkage analysis for internal carotid artery intimal medial thickness: Evidence for linkage to chromosome 12. Am J Hum Genet. 2004;74:253-261.
9. Wang D, Yang H, Quinones MJ, Bulnes-Enriquez I, Jimenez X, De La Rosa R, et al. Agenome-wide scan for carotid artery intima-media thickness: The mexican-american coronary artery disease family study. Stroke. 2005;36:540-545.
10. Baldassarre D, Nyyssonen K, Rauramaa R, de Faire U, Hamsten A, Smit AJ, et al. Cross-sectional analysis of baseline data to identify the major determinants of carotid intima-media thickness in a european population: The improve study. Eur Heart J. 2010;31:614-622.
11. Kivimaki M, Lawlor DA, Smith GD, Kumari M, Donald A, Britton A, et al. Does high c-reactive protein concentration increase atherosclerosis? The whitehall ii study. PLoS One.2008;3:e3013.
12. Marmot M, Brunner E. Cohort profile: The whitehall ii study. Int J Epidemiol. 2005;34:251-256.
13. Lee AJ, Mowbray PI, Lowe GD, Rumley A, Fowkes FG, Allan PL. Blood viscosity and elevated carotid intima-media thickness in men and women: The edinburgh artery study. Circulation. 1998;97:1467-1473.
14. Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE. Common carotid intima-media thickness and risk of stroke and myocardial infarction: The rotterdam study. Circulation.1997;96:1432-1437.
15. Hofman A, van Duijn CM, Franco OH, Ikram MA, Janssen HL, Klaver CC, et al. The rotterdam study: 2012 objectives and design update. Eur J Epidemiol. 2011;26:657-686.
16. Berglund G, Elmstahl S, Janzon L, Larsson SA. The malmo diet and cancer study. Design and feasibility. J Intern Med. 1993;233:45-51.
La RoRRR sa RRRR, etttt alll. AAAAican amamamamerererericicccanananan ccccororororonoo a
a
s sn dn
ko13
ase ffffamamamilililly y stststudddyy.y Stroke. 2005;36:540-54445.55.
saaaarre ee D, Nyysssonnenn KKKK, RaRaRaR uramaamaaa R, dee Faiaire UUU, , ,, HaHaHammmstten A,A,A, SSSmimmm t AJAJAJAJ, ett aaal. CrCrCrosnalalalyyyysiss s of bbbasaa eeliiine daata ttto o idenentifyfyfy thhehe majajoor dddeeterrmminannannts ofoff cararrotoo iddd iiinntn imimima-memm dn a eurururopopopopeeean popopupupulalal tiititiono : ThThThhee imprprprovovovoveee e sttttuddudy. EuEuEuur HeHeHeH arrrttt JJJJ. 2020200101 ;3;3;3;31:1:1:66616 4-44 62626222.22 JJJJ
ki M, ,, Lawlor DDDA,A,AA SSSS imiii hhth GGGGD,D,D, KKKumari i M,M,M, DDDonald ddd A,A,AA BBriitton AAAA, ,, et al. Does higgh oootein conccenenenentrtrtrt atattatioioioion n n n iniinincrcrcrreaeaeaeaseseese aaaathththererererosossosclcclclererrerososososisisis???? ThThhTheeee whhwhwhitititehhhehalaalall ll iiiiiiii ssstutuutudydyddy. . PLPPLPLoS One.1313 by guest on June 18, 2018
http://circgenetics.ahajournals.org/D
ownloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
21
17. Hedblad B, Nilsson P, Janzon L, Berglund G. Relation between insulin resistance and carotid intima-media thickness and stenosis in non-diabetic subjects. Results from a cross-sectional study in malmo, sweden. Diabet Med. 2000;17:299-307.
18. Farrall M, Green FR, Peden JF, Olsson PG, Clarke R, Hellenius ML, et al. Genome-wide mapping of susceptibility to coronary artery disease identifies a novel replicated locus on chromosome 17. PLoS Genet. 2006;2:e72.
19. Schunkert H, Konig IR, Kathiresan S, Reilly MP, Assimes TL, Holm H, et al. Large-scale association analysis identifies 13 new susceptibility loci for coronary artery disease. Nat Genet.2011;43:333-338.
20. Folkersen L, van't Hooft F, Chernogubova E, Agardh HE, Hansson GK, Hedin U, et al.Association of genetic risk variants with expression of proximal genes identifies novel susceptibility genes for cardiovascular disease. Circ Cardiovasc Genet. 2010;3:365-373.
21. Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MA, Bender D, et al. Plink: A tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet.2007;81:559-575.
22. Willer CJ, Li Y, Abecasis GR. Metal: Fast and efficient meta-analysis of genomewide association scans. Bioinformatics. 2010;26:2190-2191.
23. Ioannidis JP, Thomas G, Daly MJ. Validating, augmenting and refining genome-wide association signals. Nat Rev Genet. 2009;10:318-329.
24. Vliegenthart R, Oudkerk M, Hofman A, Oei HH, van Dijck W, van Rooij FJ, et al. Coronary calcification improves cardiovascular risk prediction in the elderly. Circulation. 2005;112:572-577.
25. Odink AE, van der Lugt A, Hofman A, Hunink MG, Breteler MM, Krestin GP, et al. Risk factors for coronary, aortic arch and carotid calcification; the rotterdam study. J Hum Hypertens.2010;24:86-92.
26. The Coronary Artery Disease (C4D) Genetics Consortium. A genome-wide association study in europeans and south asians identifies five new loci for coronary artery disease. Nat Genet.2011;43:339-344.
27. Malarstig A, Hamsten A. Genetics of atherothrombosis and thrombophilia. Curr Atheroscler Rep. 2010;12:159-166.
28. Tang DD. P130 crk-associated substrate (cas) in vascular smooth muscle. J Cardiovasc Pharmacol Ther. 2009;14:89-98.
29. Tikhmyanova N, Little JL, Golemis EA. Cas proteins in normal and pathological cell growth control. Cell Mol Life Sci. 2010;67:1025-1048.
t. 2010;3:365-373. . . .
der D,DDD etttt allll. PlPlPlPliniii k:k:k:k: AAAA tses AmAmAmAm JJJJ HHHHumumumum GGGGeenenenet
C
d
nthart R O dkerk M Hofman A Oei HH an Dijck W an Rooij FJ et al Cor
9-5757575.55.
CCCCJJ, Li Y, Abecacaasis GGRGRG . MeMMM taaal:l:l: FFFaast anaand eeffficiiienennt t t t memmm taaa--analllyyysisss ooof geeeennnomemem wiiiiddded scccananns. Bioiiinfnn ororrmaatiiics. 2020202 10;2;2;2; 6::::2212 90000--219911.
dis JP, Thomas GGGG,, DaDaDaDalylylyy MMMJ.JJ. VVVValalallididididatatattininining,g,g, aaauguguggmememem nttttininini g g g g ananana d ddd rererer fififiinininingngngg ggggenome-wide signgg als. Nat Rev GeGG net. 20202000909090 ;1;111000:0 3313 88-88 32323299.9
nthhart RR OO dkdk kk MM HH fof AA OO iei HHHH DDijij kck WW RRo ioijj FJFJ et ll CCo by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
22
30. Santiago FS, Ishii H, Shafi S, Khurana R, Kanellakis P, Bhindi R, et al. Yin yang-1 inhibits vascular smooth muscle cell growth and intimal thickening by repressing p21waf1/cip1 transcription and p21waf1/cip1-cdk4-cyclin d1 assembly. Circ Res. 2007;101:146-155.
31. Santiago FS, Lowe HC, Bobryshev YV, Khachigian LM. Induction of the transcriptional repressor yin yang-1 by vascular cell injury. Autocrine/paracrine role of endogenous fibroblast growth factor-2. J Biol Chem. 2001;276:41143-41149.
32. Soler Artigas M, Loth DW, Wain LV, Gharib SA, Obeidat M, Tang W, et al. Genome-wide association and large-scale follow up identifies 16 new loci influencing lung function. Nat Genet.2011;43:1082–1090.
33. Maclay JD, McAllister DA, Macnee W. Cardiovascular risk in chronic obstructive pulmonary disease. Respirology. 2007;12:634-641.
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
23
Table 1. Loci selected for replication based on association with composite IMT variables in the discovery analysis (P<1x10-5)
Composite IMT Discovery
(n=3,428-3,429)
CCA-IMT Discovery
(n=3,427-3,429)
CCA-IMT Replication
(n=11,585-11,587)
SNP Nearest gene Chr Pos
Alleles
effect/other Freq Beta SE P Beta SE P Freq Beta SE P
Heterogeneity
I2 Pheterogeneity
rs4888378 CFDP1 16 73889542 A/G 0.43 -0.0192 0.0038 6.75E-07 -0.0071 0.0028 0.010 0.41 -0.0045 0.0010 7.24E-06 0 0.784
rs1001861 BCAR1 16 73863956 G/A 0.35 -0.0178 0.0040 7.16E-06 -0.0064 0.0028 0.025 0.37 -0.0033 0.0011 0.002 0 0.835
rs200991 HIST1H2BN 6 27923473 A/C 0.12 0.0136 0.0030 8.83E-06 0.0087 0.0028 0.002 0.16 0.0032 0.0013 0.015 41.6 0.144
Discovery and replication meta-analysis P-values and beta-coefficients for the effect allele (minor allele in the discovery cohort) are shown after adjustments for sex, age, and population substructure when applicable (multi-dimensional scaling in the IMPROVE discovery cohort only). Observations are sorted according to discovery P-value. Chr: chromosome, Freq: frequency. SE: standard error. Between-cohort heterogeneity is described by I2 in percent and Q-test P-values. Chromosome positions are given according to NCBI Build 36.
SEEEE P P P P FrFrFrFreqeqeqeq
0028 0000 001010 0000 000 410.43 0.0192 0.0038 6.75E 07 0.0071 0.0028 0.010 0.41
7
6
s c
0.43 0.0192 0.0038 6.75E 07 0.0071 0.0028 0.010 0.41
0.35 -000.017878788 00.00 00000 40404040 7.166EEE-066 -0.0.0.0.000000644 0.00002228 0.020202025 0..37
0.12 0...0101010 36363636 0.00 0000000030303030 8.8.8.8.83838383EEEE--06060 0....0000000087878787 0.0.0.0.000000028282828 0.000 002 0.16
sss and betetetetaaaa----cocococoefefefeffififif cicicicienenenentstststs fffforororor tttthehehehe eeeeffffffffecececect ttt alalallleleleelelelele ((((mimimiminonononor rrr alalalallelelelelelelele iiiin nnn the dissc
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCGENETICS.112.963660
24
Figure Legends:
Figure 1. Manhattan plot of the association P-values for IMTmax in the IMPROVE study,
adjusted for sex, age and population substructure (multi-dimensional scaling). SNPs are plotted
with their P-values (as -log10 values) as a function of genomic position (NCBI Build 36). The
red line indicates the threshold for array-wide significance (P=8.39x10-7). The lead SNP
rs4888378 is colored in green. Insert: Quantile-quantile (Q-Q) plot for associations with IMTmax
in IMPROVE, adjusted for sex, age, and population substructure. The expected distribution of
the P-values under the null distribution is given by the diagonal, and the empirical distribution of
the observed P-values is given by the open black circles. The lead SNP rs4888378 is colored in
green. The genomic inflation factor lambda equals 1.05.
Figure 2. Plot showing the associations of the minor allele of rs4888378 with common carotid
IMT (CC-IMT) in the discovery and replication cohorts separately, and meta-analysis of the
discovery and replication cohorts combined. Effect size (beta with 95% confidence intervals),
sample size, and minor allele frequency (MAF) of rs4888378 are given.
Figure 3. Regional plots of the genomic region containing the lead SNP rs4888378 (± 500
kilobases). SNPs are plotted with their P-values for the association with IMTmax (as -log10
values) as a function of genomic position (NCBI Build 36). Estimated recombination rates (from
the HapMap project) are plotted to reflect the local LD structure. The lead SNP rs4888378 is
shown as a diamond, and all other SNPs as circles. Correlations between a given SNP and
expected distributtttioioioion
he empipipii iiriical lll didididistriririribubububut
e e
Plot showing the associations of the minor allele of rs4888378 with common caro
MT) in the disco er and replication cohorts separatel and meta anal sis of th
ed PPP-v-v-valalala ueueuess s is gggiviii en by the open black ciriririrclcles. The lead SNPNPNPP rs4888378 is colore
gggennnnomic inflaatititioon faaactoooorrr r llal mbmbmbm daaa eequuualls 1.005.
Plot showing gg the asso iciiatioii ns of fff hhthe miiinor llalllelll le off f rs4848488888888837373778888 wiiii hthh common caro
MTMMT)) iin thhe ddiis dnd lili iti hoh ts at lel dnd eta lal iis ff hth by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCGENETICS.112.963660
25
rs4888378 are indicated according to a color scheme based on pairwise r2-values from HapMap
(CEU reference panel). A. Original associations from the discovery analysis. B. Secondary
analysis where discovery associations are adjusted for the effect of rs4888378.
Figure 4. Associations of rs4888378 with coronary artery disease (CAD) and myocardial
infarction (MI). Forest plot of odds ratios with 95% confidence interval for the association of the
rs4888378 minor allele with CAD phenotypes in PROCARDIS with additional controls from the
Wellcome Trust Case-Control Consortium (adjusted for age, gender, country, and relatedness)
and in CARDIoGRAM (meta-analysis of 12 CAD and 10 MI case-control studies, respectively,
adjusted for age, gender, the genomic inflation (lambda), and taking into account the uncertainty
of imputed genotypes). Relative study size is reflected by plotted box size.
Figure 5. Associations of rs4888378 with nearby gene expression in human target tissues.
Robust Multichip Average (RMA)-normalized expression levels of TMEM170A and LDHD in
aortic intima-media and adventitia and BCAR1 in carotid plaque according to rs4888378
genotype are shown. Additive model P values are given.
countryy, and relateeeedndndndne
ntrol sttutt didididies, respececececttttiv
r age, gender, the genomic inflation (lambda), and taking into account the uncert
A
ltichip A erage (RMA) normali ed e pression le els ofd TMEM170A and LDHD
r agegege,, gegegendndnddeeer, ththththe genomic inflation (lammmbdbdbb a), and taking iiintntntto account the uncert
gggennnnotypes). RRellatiivi eee studududu y sisisisizze iss refflecteedd byyy pppplolol ttteddd boxx sssizee.e
Associations of rs484848888888 3737373 8 88 withhh nearbbbby yy gegg ne expppressiiioi n iinii hhhhuman targegg t tissues.
lll iti hchiip AA ((RMRMA)A) lalii ded iio lle lls ffdd TMTMEMEM17170A0A dnd LDLDHDHD by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

-0.02
-0.015
-0.01
-0.005
0
0.005
0.01
0.015
0.02
IMPROVE n=3427MAF=0.43
WH-II n=2138MAF=0.41
MDC n=2140MAF=0.40
RS-I n=4699MAF=0.41
RS-II n=1980MAF=0.42
EAS n=630MAF=0.40
Replication n=11587MAF=0.41
Combined n=15014MAF=0.41
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

Tremoli, Ulf de Faire, Steve E. Humphries and Anders HamstenAroon D. Hingorani, Olle Melander, Jacqueline C.M. Witteman, Damiano Baldassarre, Elena
Syvänen, Göran K. Hansson, Per Eriksson, Nilesh J. Samani, Hugh Watkins, Jacqueline F. Price,J. O'Donnell, Martin Farrall, Robert Clarke, Maria Grazia Franzosi, Udo Seedorf, Ann-Christine
Philippa J. Talmud, Bo Hedblad, Albert Hofman, Jeanette Erdmann, Muredach P. Reilly, ChristopherTuomainen, Kai Savonen, Andries J. Smit, Philippe Giral, Elmo Mannarino, Christine M. Robertson,
Tomi-PekkaGabrielsen, Ulf Hedin, Anders Franco-Cereceda, Kristiina Nyyssönen, Rainer Rauramaa, Colombo, Meena Kumari, Claudia Langenberg, Nick J. Wareham, André G. Uitterlinden, AndersSilveira, John Deanfield, Benjamin F. Voight, Pierre Fontanillas, Maria Sabater-Lleal, Gualtiero I. Bolton, Lasse Folkersen, Bruna Gigante, Karin Leander, Max Vikström, Malin Larsson, AngelaFabrizio Veglia, Cristiano Fava, Maryam Kavousi, Stela McLachlan, Mika Kivimäki, Jennifer L. Karl Gertow, Bengt Sennblad, Rona J. Strawbridge, John Öhrvik, Delilah Zabaneh, Sonia Shah,
Intima-Media Thickness and Coronary Artery Disease Risk Locus as a Determinant of CarotidBCAR1-CFDP1-TMEM170AIdentification of the
Print ISSN: 1942-325X. Online ISSN: 1942-3268 Copyright © 2012 American Heart Association, Inc. All rights reserved.
TX 75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas,Circulation: Cardiovascular Genetics
published online November 14, 2012;Circ Cardiovasc Genet.
http://circgenetics.ahajournals.org/content/early/2012/11/14/CIRCGENETICS.112.963660World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circgenetics.ahajournals.org/content/suppl/2012/11/14/CIRCGENETICS.112.963660.DC1Data Supplement (unedited) at:
http://circgenetics.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Genetics Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further information aboutnot the Editorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center,Circulation: Cardiovascular Genetics Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 18, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

SUPPLEMENTAL MATERIAL
Identification of the BCAR1-CFDP1-TMEM170A locus as a determinant of
carotid intima-media thickness and coronary artery disease risk
Karl Gertow, PhD; Bengt Sennblad, PhD; Rona J. Strawbridge, PhD; John Öhrvik, PhD; Delilah
Zabaneh, PhD; Sonia Shah, MSc; Fabrizio Veglia, PhD; Cristiano Fava, MD, PhD; Maryam Kavousi,
MD, MSc; Stela McLachlan, PhD; Mika Kivimäki, PhD; Jennifer L. Bolton, PhD; Lasse Folkersen,
PhD; Bruna Gigante, MD, PhD; Karin Leander, PhD; Max Vikström, BSc; Malin Larsson, PhD;
Angela Silveira, PhD; John Deanfield, MD, PhD; Benjamin F. Voight, PhD; Pierre Fontanillas, PhD;
Maria Sabater-Lleal, PhD; Gualtiero I. Colombo, MD, PhD; Meena Kumari, PhD; Claudia
Langenberg, PhD; Nick J. Wareham, MBBS, PhD; André G. Uitterlinden, MD, PhD; Anders
Gabrielsen, MD, PhD; Ulf Hedin, MD, PhD; Anders Franco-Cereceda, MD, PhD; Kristiina
Nyyssönen, PhD; Rainer Rauramaa, MD, PhD; Tomi-Pekka Tuomainen, MD, PhD; Kai Savonen,
MD, PhD; Andries J. Smit, MD, PhD; Philippe Giral, MD, PhD; Elmo Mannarino, MD, PhD;
Christine M. Robertson, MBChB; Philippa J. Talmud, PhD; Bo Hedblad, MD, PhD; Albert Hofman,
MD, PhD; Jeanette Erdmann, PhD*; Muredach P. Reilly, MBBCH, MSCE*; Christopher J.
O’Donnell, MD, MPH*; Martin Farrall, FRCPath†; Robert Clarke, MD, PhD
†; Maria Grazia Franzosi,
PhD†; Udo Seedorf, PhD
†; Ann-Christine Syvänen, PhD; Göran K. Hansson, MD, PhD; Per Eriksson,
PhD; Nilesh J. Samani, MF, FRCP*; Hugh Watkins, FRCP†; Jacqueline F. Price, MBChB; Aroon D.
Hingorani, MD, PhD; Olle Melander, MD, PhD; Jacqueline C.M. Witteman, PhD; Damiano
Baldassarre, PhD; Elena Tremoli PhD; Ulf de Faire, MD, PhD; Steve E. Humphries, PhD; Anders
Hamsten, FRCP
*On behalf of the CARDIoGRAM consortium
†On behalf of the PROCARDIS consortium

CONTENTS
1. SUPPLEMENTAL SECTION S1: COHORT DESCRIPTIONS
2. SUPPLEMENTAL SECTION S2: GENETIC QUALITY CONTROL PROCEDURES IN
THE DISCOVERY COHORT (IMPROVE)
3. SUPPLEMENTAL SECTION S3: ESTABLISHMENT OF THRESHOLD FOR ARRAY-
WIDE STATISTICAL SIGNIFICANCE
4. SUPPLEMENTAL SECTION S4: POWER CALCULATIONS
5. SUPPLEMENTAL SECTION S5: BOOTSTRAPPING PROCEDURE
6. SUPPLEMENTAL SECTION S6: ASSOCIATION TESTING IN CAD CASE-CONTROL
STUDIES
7. SUPPLEMENTAL SECTION S7: CARDIoGRAM MEMBERS, AFFILIATIONS,
FUNDING AND DISCLOSURES
8. SUPPLEMENTAL SECTION S8: PROCARDIS MEMBERS AND AFFILIATIONS
9. SUPPLEMENTAL SECTION S9: WRITING GROUP, STUDY AND INSTITUTIONAL
AFFILIATIONS
10. SUPPLEMENTAL TABLES 1-3
11. SUPPLEMENTAL FIGURE LEGENDS 1-4
12. SUPPLEMENTAL FIGURES 1-4

SUPPLEMENTAL SECTION S1: COHORT DESCRIPTIONS
IMPROVE: The IMPROVE study1 was designed to evaluate the capacity of cross-sectional carotid
intima-media thickness (cIMT) and cIMT progression as predictors of incident vascular events in
European subjects at high risk for cardiovascular disease. The IMPROVE study enrolled 3,711
individuals (age range 54 to 79 years, 48% men) with at least three vascular risk factors but
asymptomatic for cardiovascular diseases, and free of any conditions that might limit longevity (e.g.
cancer) during 2004 and 2005. Subjects were recruited from 7 centres in 5 countries across Europe:
1,050 from two centres in Kuopio, Finland, 501 from Paris, France, 553 from Milan, Italy, 542 from
Perugia, Italy, 532 from Groningen, the Netherlands and 533 from Stockholm, Sweden. Among these,
the common carotid artery could not be properly visualized by ultrasonography in 8 subjects; hence
3,703 individuals were considered. Measurements of mean and maximum IMT of the common carotid
(CC), bifurcation (Bif), and internal carotid arteries (ICA) were obtained. IMT of the CC was
measured at two levels; at the 1st cm proximal to the bifurcation (CC-1
st cm), and in a segment
excluding the 1st cm proximal to the bifurcation (CC-IMT). Composite IMT variables considering the
whole carotid tree (IMTmean, IMTmax, and IMTmean-max [the average of IMT maxima recorded at the
different segments]) were derived from the segment-specific measurements.1 Details of the
ultrasonographic protocol have been described.1
Malmö Diet and Cancer (MDC) study: MDC is a population-based prospective study.2 Between
1991 and 1996, women aged 45 to 73 years and men aged 46 to 73 years residing in Malmö
(approximately 250,000 habitants), Sweden, were invited by mail and by newspaper advertisement to
participate in the study. In all, 28,449 persons from an eligible population of 74,000 participated. The
participants were asked to complete a questionnaire at home, which included lifestyle factors,
medication and previous and current diseases. Measurement of IMT in the distal part of common
carotid artery (mean) and at the bifurcation (max) level was obtained along with detection of carotid
plaques (summarized in a plaque scoring system on a 0-6 scale).3 Ultrasound measurements (along
with measurements of other cardiovascular risk factors) were performed in a random subsample

referred to as the MDC-CVA (n=6,103). Genotyping with the CardioMetabochip was performed in
2,143 non-diabetic participants in the MDC-CVA subset.
Edinburgh Artery Study (EAS): EAS was designed to explore the epidemiology of peripheral
arterial disease in a general population sample. The EAS study enrolled 1,592 men and women (age
range 55 to 74 years), selected in 1988 at random from 10 general practices spread across the city of
Edinburgh, Scotland. Surviving participants were invited to attend a five-year follow-up examination
involving measurements of cIMT. Valid measurements of cIMT and quality-controlled
CardioMetabochip genotyping data were available for 630 subjects for the present study.
Measurement of cIMT was made for both the right and left common carotid arteries 2 cm proximal to
the bifurcation.4
Whitehall-II (WH-II): WH-II recruited 10,308 men and women between 1985 and 1989 from 20
London-based civil service departments.5 Clinical measurements were taken at 5-year intervals.
Currently, clinical data is available from 4 phases (phase 1: 1985-1988, phase 3: 1991-1993, phase
5:1997-1999 and phase 7: 2003-2004). Carotid ultrasound measurements were made at Phase 7 (2003–
2004). cIMT was measured in the right and left common carotid arteries. Longitudinal images of the
CC artery, triggered on the R-wave of the ECG, were magnified and recorded in DICOM format as a
cine loop, on the hard drive of the ultrasound machine for later analysis. The CC-IMT was measured
at its thickest part 1 cm proximal to the bifurcation. The overall coefficient of variation for repeated
measures of cIMT was 4.7% (n=89).6 A total number of 2,138 subjects were included in the present
study.
Rotterdam study-I and Rotterdam study-II (RS-I and RS-II): The Rotterdam Study is a
prospective population-based cohort study aimed at investigating the determinants of chronic diseases
among participants aged 55 years and older.7 Briefly, residents of Ommoord, a district of
Rotterdamthe Netherlands, 55 years of age or older, were asked to participate, of whom 7983
participated (RS-I). The baseline examination was conducted in 1990-1993 and consisted of a home
interview and research centre visit for blood sampling. In 1999, inhabitants who turned 55 years of age
or had moved into the study district since the start of the study participated (RS-II). Ultrasonography
of the common carotid artery of the left and right carotid arteries was performed with a 7.5-MHz
linear-array transducer (ATL UltraMark IV). The maximal cIMT, summarized as the mean of the
maximal measurements from the near and far walls on both the left and right sides, was used for
analysis.8 A total of 4699 subjects from RS-I and 1980 subjects from RS-II had both genotyping and
IMT measurements available and were included in the current study.9
PROCARDIS: The PROCARDIS cohort has been described elsewhere.10
In brief, cases were
included if a diagnosis of coronary artery disease (CAD) was made before the age of 66 years and a
sibling also was diagnosed with CAD before 66 years. Control subjects were defined as being free
from symptoms of CAD up to the age of 66 years and without siblings diagnosed with CAD before 66
years. Subjects were genotyped on the Illumina 1M or 610K genotyping arrays, and imputation was
made using the MACH2 software. Standard quality control procedures were performed.11
PROCARDIS control subjects were supplemented with control subjects from the WTCCC, which has
been described previously.12
Genotyping, imputation and quality control procedures of WTCCC
subjects were comparable with those of PROCARDIS.
CARDIoGRAM: The CARDIoGRAM CAD genome-wide association study (GWAS) meta-analysis
consortium has been described elsewhere.13
In brief, CARDIoGRAM combined GWAS data from 14
CAD case-control studies providing a discovery sample size of 22,233 cases and 64,762 controls.
Only subjects reporting European ancestry were included. Genotyping in individual discovery GWAS
was carried out on Affymetrix or Illumina platforms and approximately 2.3 million imputed genotypes
were generated using the MACH, IMPUTE or BIMBAM algorithms, which has been described
previously.13
Quality control was performed at individual sites and centrally.13
REFERENCES
1. Baldassarre D, Nyyssonen K, Rauramaa R, de Faire U, Hamsten A, Smit AJ, et al. Cross-
sectional analysis of baseline data to identify the major determinants of carotid intima-media
thickness in a european population: The improve study. Eur Heart J. 2010;31:614-622.

2. Berglund G, Elmstahl S, Janzon L, Larsson SA. The malmo diet and cancer study. Design and
feasibility. J Intern Med. 1993;233:45-51.
3. Hedblad B, Nilsson P, Janzon L, Berglund G. Relation between insulin resistance and carotid
intima-media thickness and stenosis in non-diabetic subjects. Results from a cross-sectional
study in malmo, sweden. Diabet Med. 2000;17:299-307.
4. Lee AJ, Mowbray PI, Lowe GD, Rumley A, Fowkes FG, Allan PL. Blood viscosity and
elevated carotid intima-media thickness in men and women: The edinburgh artery study.
Circulation. 1998;97:1467-1473.
5. Marmot M, Brunner E. Cohort profile: The whitehall ii study. Int J Epidemiol. 2005;34:251-
256.
6. Kivimaki M, Lawlor DA, Smith GD, Kumari M, Donald A, Britton A, et al. Does high c-
reactive protein concentration increase atherosclerosis? The whitehall ii study. PLoS One.
2008;3:e3013.
7. Hofman A, van Duijn CM, Franco OH, Ikram MA, Janssen HL, Klaver CC, et al. The
rotterdam study: 2012 objectives and design update. Eur J Epidemiol. 2011;26:657-686.
8. Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE. Common carotid intima-media
thickness and risk of stroke and myocardial infarction: The rotterdam study. Circulation.
1997;96:1432-1437.
9. Bis JC, Kavousi M, Franceschini N, Isaacs A, Abecasis GR, Schminke U, et al. Meta-analysis
of genome-wide association studies from the charge consortium identifies common variants
associated with carotid intima media thickness and plaque. Nat Genet. 2011;43:940-947.
10. Farrall M, Green FR, Peden JF, Olsson PG, Clarke R, Hellenius ML, et al. Genome-wide
mapping of susceptibility to coronary artery disease identifies a novel replicated locus on
chromosome 17. PLoS Genet. 2006;2:e72.
11. Strawbridge RJ, Dupuis J, Prokopenko I, Barker A, Ahlqvist E, Rybin D, et al. Genome-wide
association identifies nine common variants associated with fasting proinsulin levels and
provides new insights into the pathophysiology of type 2 diabetes. Diabetes. 2011;60:2624-
2634.

12. The Coronary Artery Disease (C4D) Genetics Consortium. A genome-wide association study
in europeans and south asians identifies five new loci for coronary artery disease. Nat Genet.
2011;43:339-344.
13. Schunkert H, Konig IR, Kathiresan S, Reilly MP, Assimes TL, Holm H, et al. Large-scale
association analysis identifies 13 new susceptibility loci for coronary artery disease. Nat
Genet. 2011;43:333-338.

SUPPLEMENTAL SECTION S2: GENETIC QUALITY CONTROL PROCEDURES IN THE
DISCOVERY COHORT (IMPROVE)
The IMPROVE study, enrolled 3,711 subjects in five different European countries, 3,615 of which had
both phenotype and CardioMetabochip genotype data available. Individual level quality control (QC)
exclusion criteria were call rates <0.95, results of identity by state (IBS) estimations (e.g. unverified
cryptic relatedness), verified relatedness, estimated inbreeding (excessive homozygosity), and
discrepancy between recorded and genotype-determined sex, resulting in 140 exclusions. Multi-
dimensional scaling (MDS) analysis and calculation of the genomic inflation factor lambda was
performed to evaluate population substructure, using PLINK 1.07.1 MDS analysis was performed
using largely uncorrelated CardioMetabochip SNPs obtained by applying a filter of pair-wise
correlation of r2<0.5 within a 50 SNP window, iteratively shifted 5 SNPs along the sequence, which
revealed significant population substructure (Supplemental Figure 1). An additional 45 individuals
were excluded based on results of the MDS analysis or self-reported non-Caucasian ethnicity. In order
to adjust for the identified population substructure, the first three MDS dimensions were included as
covariates in subsequent association analyses. QC exclusion criteria for SNPs were genotype call rates
<0.90, highly significant deviation from Hardy-Weinberg equilibrium (P<5x10-7
) and minor allele
frequency (MAF) <0.005. Following QC procedures, 3,430 individuals and 127,830 autosomal SNPs
were included in the association analysis.
REFERENCES
1. Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MA, Bender D, et al. Plink: A tool set
for whole-genome association and population-based linkage analyses. Am J Hum Genet.
2007;81:559-575.

SUPPLEMENTAL SECTION S3: ESTABLISHMENT OF THRESHOLD FOR ARRAY-WIDE
STATISTICAL SIGNIFICANCE
The a priori threshold for array-wide statistical significance was established as P<8.39x10-7
through
approximation of the total number of uncorrelated SNPs on the CardioMetabochip with the number of
principal components explaining >99.5% of the total SNP variation according to methods proposed by
Gao et al,1, 2
using a block size of 8,192 SNPs. This number was then used for a standard Bonferroni
correction to set the threshold for array-wide significance for a two-sided test at the 5% level.
REFERENCES
1. Gao X, Becker LC, Becker DM, Starmer JD, Province MA. Avoiding the high bonferroni
penalty in genome-wide association studies. Genet Epidemiol. 2010;34:100-105.
2. Gao X, Starmer J, Martin ER. A multiple testing correction method for genetic association
studies using correlated single nucleotide polymorphisms. Genet Epidemiol. 2008;32:361-369.

SUPPLEMENTAL SECTION S4: POWER CALCULATIONS
Power calculations for the replication studies were performed using the Genetic Power Calculator.1
The 90th percentile of the carotid intima-media thickness (cIMT) variable was used as a threshold to
group participants into cases (above the 90th percentile) and controls (at and below the 90
th percentile).
With upwards of 11,000 subjects available in the five replication cohorts, we assigned 1,100 cases.
Furthermore, we assumed a minor allele frequency (MAF) of at least 0.05 and that the proportion of
the cIMT variance attributable to a specific locus would be at least 0. 16%. Based on these conditions
and setting the experimental error rate to at most 5% and the minimum power 80% (to detect a SNP in
the replication studies contributing at least 0.16% of the variation in cIMT), it would be justifiable to
take up to 50 uncorrelated SNPs forward to replication.
REFERENCES
1. Purcell S, Cherny SS, Sham PC. Genetic power calculator: Design of linkage and association
genetic mapping studies of complex traits. Bioinformatics. 2003;19:149-150.

SUPPLEMENTAL SECTION S5: BOOTSTRAPPING PROCEDURE
Given that the composite IMT-measures were unique to IMPROVE and thereby not assessable by
conventional replication in independent cohorts, nonparametric bootstrap re-sampling was applied to
perform internal validation. While this approach cannot evaluate the generality of the results in terms
of population-specificity, it allows adjustment for the effect known as the winner’s curse, i.e. a bias
towards over-estimation of effect sizes among the most significant SNPs.1 A modified version of the
double bootstrap re-sampling method (BR-squared) proposed by Sun et al 2 was used. This method
uses a weighted average over bootstrap replicates of the difference between the effect size estimated
from the observations in the bootstrap sample and the one estimated from the observations not in the
bootstrap sample to estimate the over-estimation. The difference was adjusted for the negative
correlation between the two effect sizes (disjoint events). Since the bias correction in this context may
be large, the standard deviation of the original effect size can be a poor estimate of the bias-corrected
effect size. To resolve this, we performed a double bootstrap. In the outer bootstrap we draw B2
samples from the original sample. The bias corrected effect size was computed by drawing B1 inner
bootstrap samples from each of the B2 samples. The limits of an approximate (1-α)100% confidence
interval (CI) for the bias corrected effect size is then given by the B2*α/2 and the B2*(1- α/2) ordered
bias-corrected effect sizes. A (1-α)100% CI not covering zero corresponds to rejecting the null
hypothesis at significance level α. In case of multiple testing α was adjusted using the Bonferroni
correction. First, results from the meta-analysis of the CC-IMT SNPs in the replication cohorts alone
were compared with the outcome of a bootstrap validation of the same CC-IMT SNPs in IMPROVE
(Supplemental Figure 3a). The agreement between the two approaches was good in terms of both
estimates of effect sizes and their confidence intervals when corrected for sample size (Supplemental
Figure 3a), indicating good performance of the bootstrap approach in adjusting for the winner’s curse
effect. Subsequent bootstrap validation of the 3 composite IMT index SNPs confirmed significant
effects of these SNPs on composite IMT, with similar deflation of effect size estimates as those
observed for the CC-IMT SNPs, indicating an adjustment for the winner’s curse effect similar to that
for the CC-IMT SNPs (Supplemental Figure 3b).

REFERENCES
1. Ioannidis JP, Thomas G, Daly MJ. Validating, augmenting and refining genome-wide
association signals. Nat Rev Genet. 2009;10:318-329.
2. Sun L, Dimitromanolakis A, Faye LL, Paterson AD, Waggott D, Group TDER, et al. Br-
squared: A practical solution to the winner's curse in genome-wide scans. Human genetics.
2011.

SUPPLEMENTAL SECTION S6: ASSOCIATION TESTING IN CAD CASE-CONTROL
STUDIES
In PROCARDIS, associations between the SNP and all CAD (n=13,591), and MI only (n=12,472)
were tested by logistic regression analysis assuming an additive model of allelic association and
adjusting for age, gender, country and relatedness using STATA version 11. In CARDIoGRAM,
associations between rs4888378 and all CAD (n=82,297), and MI only (n=52,226) were tested by
meta-analysis of cohort-specific associations using a fixed-effect model with inverse variance
weighting. In each CARDIoGRAM cohort analyzed (12 cohorts for CAD and 10 cohorts for MI),
associations were tested by logistic regression analysis assuming an additive model of allelic
association and adjusting for age, gender, genomic inflation (lambda), and taking into account the
uncertainty of imputed genotypes.1
REFERENCES
1. Schunkert H, Konig IR, Kathiresan S, Reilly MP, Assimes TL, Holm H, et al. Large-scale
association analysis identifies 13 new susceptibility loci for coronary artery disease. Nat
Genet. 2011;43:333-338.

SUPPLEMENTAL SECTION S7: CARDIoGRAM MEMBERS, AFFILIATIONS, FUNDING
AND DISCLOSURES
The CARDIoGRAM Consortium
Executive Committee: Sekar Kathiresan1,2,3
, Muredach P. Reilly4, Nilesh J. Samani
5,6, Heribert
Schunkert7
Executive Secretary: Jeanette Erdmann7
Steering Committee: Themistocles L. Assimes8, Eric Boerwinkle
9, Jeanette Erdmann
7,79 Alistair
Hall10
, Christian Hengstenberg11
, Sekar Kathiresan1,2,3
, Inke R. König12
, Reijo Laaksonen13
, Ruth
McPherson14
, Muredach P. Reilly4, Nilesh J. Samani
5,6, Heribert Schunkert
7,79, John R. Thompson
15,
Unnur Thorsteinsdottir16,17
, Andreas Ziegler12
Statisticians: Inke R. König12
(chair), John R. Thompson15
(chair), Devin Absher18
, Li Chen19
, L.
Adrienne Cupples20,21
, Eran Halperin22
, Mingyao Li23
, Kiran Musunuru1,2,3
, Michael Preuss12,7
, Arne
Schillert12
, Gudmar Thorleifsson16
, Benjamin F. Voight2,3,24
, George A. Wells25
Writing group: Themistocles L. Assimes8, Panos Deloukas
26, Jeanette Erdmann
7,79, Hilma Holm
16,
Sekar Kathiresan1,2,3
, Inke R. König12
, Ruth McPherson14
, Muredach P. Reilly4, Robert Roberts
14,
Nilesh J. Samani5,6
, Heribert Schunkert7,79
, Alexandre F. R. Stewart14
ADVANCE: Devin Absher18
, Themistocles L. Assimes8, Stephen Fortmann
8, Alan Go
27, Mark
Hlatky8, Carlos Iribarren
27, Joshua Knowles
8, Richard Myers
18, Thomas Quertermous
8, Steven
Sidney27
, Neil Risch28
, Hua Tang29
CADomics: Stefan Blankenberg30
, Tanja Zeller30
, Arne Schillert12
, Philipp Wild30
, Andreas Ziegler12
,
Renate Schnabel30
, Christoph Sinning30
, Karl Lackner31
, Laurence Tiret32
, Viviane Nicaud32
, Francois
Cambien32
, Christoph Bickel30
, Hans J. Rupprecht30
, Claire Perret32
, Carole Proust32
, Thomas Münzel30
CHARGE: Maja Barbalic33
, Joshua Bis34
, Eric Boerwinkle9, Ida Yii-Der Chen
35, L. Adrienne
Cupples20,21
, Abbas Dehghan36
, Serkalem Demissie-Banjaw37,21
, Aaron Folsom38
, Nicole Glazer39
,

Vilmundur Gudnason40,41
, Tamara Harris42
, Susan Heckbert43
, Daniel Levy21
, Thomas Lumley44
,
Kristin Marciante45
, Alanna Morrison46
, Christopher J. O´Donnell47
, Bruce M. Psaty48
, Kenneth Rice49
,
Jerome I. Rotter35
, David S. Siscovick50
, Nicholas Smith43
, Albert Smith40,41
, Kent D. Taylor35
,
Cornelia van Duijn36
, Kelly Volcik46
, Jaqueline Whitteman36
, Vasan Ramachandran51
, Albert
Hofman36
, Andre Uitterlinden52,36
deCODE: Solveig Gretarsdottir16
, Jeffrey R. Gulcher16
, Hilma Holm16
, Augustine Kong16
, Kari
Stefansson16,17
, Gudmundur Thorgeirsson53,17
, Karl Andersen53,17
, Gudmar Thorleifsson16
, Unnur
Thorsteinsdottir16,17
GERMIFS I and II: Jeanette Erdmann7,79
, Marcus Fischer11
, Anika Grosshennig12,7
, Christian
Hengstenberg11
, Inke R. König12
, Wolfgang Lieb54
, Patrick Linsel-Nitschke7, Michael Preuss
12,7, Klaus
Stark11
, Stefan Schreiber55
, H.-Erich Wichmann56,58,59
, Andreas Ziegler12
, Heribert Schunkert7,79
GERMIFS III (KORA): Zouhair Aherrahrou7,79
, Petra Bruse7,79
, Angela Doering56
, Jeanette
Erdmann7,79
, Christian Hengstenberg11
, Thomas Illig56
, Norman Klopp56
, Inke R. König12
, Patrick
Diemert7, Christina Loley
12,7, Anja Medack
7,79, Christina Meisinger
56, Thomas Meitinger
57,60, Janja
Nahrstedt12,7
, Annette Peters56
, Michael Preuss12,7
, Klaus Stark11
, Arnika K. Wagner7, H.-Erich
Wichmann56,58,59
, Christina Willenborg,7,79
, Andreas Ziegler12
, Heribert Schunkert7,79
LURIC/AtheroRemo: Bernhard O. Böhm61
, Harald Dobnig62
, Tanja B. Grammer63
, Eran Halperin22
,
Michael M. Hoffmann64
, Marcus Kleber65
, Reijo Laaksonen13
, Winfried März63,66,67
, Andreas
Meinitzer66
, Bernhard R. Winkelmann68
, Stefan Pilz62
, Wilfried Renner66
, Hubert Scharnagl66
, Tatjana
Stojakovic66
, Andreas Tomaschitz62
, Karl Winkler64
MIGen: Benjamin F. Voight2,3,24
, Kiran Musunuru1,2,3
, Candace Guiducci3, Noel Burtt
3, Stacey B.
Gabriel3, David S. Siscovick
50, Christopher J. O’Donnell
47, Roberto Elosua
69, Leena Peltonen
49,
Veikko Salomaa70
, Stephen M. Schwartz50
, Olle Melander26
, David Altshuler71,3
, Sekar Kathiresan1,2,3
OHGS: Alexandre F. R. Stewart14
, Li Chen19
, Sonny Dandona14
, George A. Wells25
, Olga Jarinova14
,
Ruth McPherson14
, Robert Roberts14

PennCATH/MedStar: Muredach P. Reilly4, Mingyao Li
23, Liming Qu
23, Robert Wilensky
4, William
Matthai4, Hakon H. Hakonarson
72, Joe Devaney
73, Mary Susan Burnett
73, Augusto D. Pichard
73,
Kenneth M. Kent73
, Lowell Satler73
, Joseph M. Lindsay73
, Ron Waksman73
, Christopher W. Knouff74
,
Dawn M. Waterworth74
, Max C. Walker74
, Vincent Mooser74
, Stephen E. Epstein73
, Daniel J. Rader75,4
WTCCC: Nilesh J. Samani5,6
, John R. Thompson15
, Peter S. Braund5, Christopher P. Nelson
5,
Benjamin J. Wright76
, Anthony J. Balmforth77
, Stephen G. Ball78
, Alistair S. Hall10
, Wellcome Trust
Case Control Consortium
Affiliations
1 Cardiovascular Research Center and Cardiology Division, Massachusetts General Hospital, Boston,
MA, USA; 2 Center for Human Genetic Research, Massachusetts General Hospital, Boston, MA,
USA; 3 Program in Medical and Population Genetics, Broad Institute of Harvard and Massachusetts
Institute of Technology (MIT), Cambridge, MA, USA; 4 The Cardiovascular Institute, University of
Pennsylvania, Philadelphia, PA, USA; 5 Department of Cardiovascular Sciences, University of
Leicester, Glenfield Hospital, Leicester, UK; 6 Leicester National Institute for Health Research
Biomedical Research Unit in Cardiovascular Disease, Glenfield Hospital, Leicester, LE3 9QP, UK; 7
Medizinische Klinik II, Universität zu Lübeck, Lübeck, Germany; 8 Department of Medicine,
Stanford University School of Medicine, Stanford, CA, USA; 9 University of Texas Health Science
Center, Human Genetics Center and Institute of Molecular Medicine, Houston, TX, USA; 10 Division
of Cardiovascular and Neuronal Remodelling, Multidisciplinary Cardiovascular Research Centre,
Leeds Institute of Genetics, Health and Therapeutics, University of Leeds, UK; 11 Klinik und
Poliklinik für Innere Medizin II, Universität Regensburg, Regensburg, Germany; 12 Institut für
Medizinische Biometrie und Statistik, Universität zu Lübeck, Lübeck, Germany; 13 Science Center,
Tampere University Hospital, Tampere, Finland; 14 The John & Jennifer Ruddy Canadian
Cardiovascular Genetics Centre, University of Ottawa Heart Institute, Ottawa, Canada; 15 Department
of Health Sciences, University of Leicester, Leicester, UK; 16 deCODE Genetics, 101 Reykjavik,
Iceland; 17 University of Iceland, Faculty of Medicine, 101 Reykjavik, Iceland; 18 Hudson Alpha

Institute, Huntsville, Alabama, USA; 19 Cardiovascular Research Methods Centre, University of
Ottawa Heart Institute, 40 Ruskin Street, Ottawa, Ontario, Canada, K1Y 4W7; 20 Department of
Biostatistics, Boston University School of Public Health, Boston, MA USA; 21 National Heart, Lung
and Blood Institute's Framingham Heart Study, Framingham, MA, USA; 22 The Blavatnik School of
Computer Science and the Department of Molecular Microbiology and Biotechnology, Tel-Aviv
University, Tel-Aviv, Israel, and the International Computer Science Institute, Berkeley, CA, USA; 23
Biostatistics and Epidemiology, University of Pennsylvania, Philadelphia, PA, USA; 24 Department
of Medicine, Harvard Medical School, Boston, MA, USA; 25 Research Methods, Univ Ottawa Heart
Inst; 26 Department of Clinical Sciences, Hypertension and Cardiovascular Diseases, Scania
University Hospital, Lund University, Malmö, Sweden; 27 Division of Research, Kaiser Permanente,
Oakland, CA, USA; 28 Institute for Human Genetics, University of California, San Francisco, San
Francisco, CA, USA; 29 Dept Cardiovascular Medicine, Cleveland Clinic; 30 Medizinische Klinik
und Poliklinik, Johannes-Gutenberg Universität Mainz, Universitätsmedizin, Mainz, Germany; 31
Institut für Klinische Chemie und Laboratoriumsmediizin, Johannes-Gutenberg Universität Mainz,
Universitätsmedizin, Mainz, Germany; 32 INSERM UMRS 937, Pierre and Marie Curie University
(UPMC, Paris 6) and Medical School, Paris, France; 33 University of Texas Health Science Center,
Human Genetics Center, Houston, TX, USA; 34 Cardiovascular Health Resarch Unit and Department
of Medicine, University of Washington, Seattle, WA USA; 35 Cedars-Sinai Medical Center, Medical
Genetics Institute, Los Angeles, CA, USA; 36 Erasmus Medical Center, Department of Epidemiology,
Rotterdam, The Netherlands; 37 Boston University, School of Public Health, Boston, MA, USA; 38
University of Minnesota School of Public Health, Division of Epidemiology and Community Health,
School of Public Health (A.R.F.), Minneapolis, MN, USA; 39 University of Washington,
Cardiovascular Health Research Unit and Department of Medicine, Seattle, WA, USA; 40 Icelandic
Heart Association, Kopavogur Iceland; 41 University of Iceland, Reykjavik, Iceland; 42 Laboratory of
Epidemiology, Demography, and Biometry, Intramural Research Program, National Institute on
Aging, National Institutes of Health, Bethesda MD, USA; 43 University of Washington, Department
of Epidemiology, Seattle, WA, USA; 44 University of Washington, Department of Biostatistics,
Seattle, WA, USA; 45 University of Washington, Department of Internal Medicine, Seattle, WA,

USA; 46 University of Texas, School of Public Health, Houston, TX, USA; 47 National Heart, Lung
and Blood Institute, Framingham Heart Study, Framingham, MA and Cardiology Division,
Massachusetts General Hospital, Boston, MA, USA; 48 Center for Health Studies, Group Health,
Departments of Medicine, Epidemiology, and Health Services, Seattle, WA, USA; 49 The Wellcome
Trust Sanger Institute, The Wellcome Trust Genome Campus, Hinxton, Cambridge, UK; 50
Cardiovascular Health Research Unit, Departments of Medicine and Epidemiology, University of
Washington, Seattle; 51 Boston University Medical Center, Boston, MA, USA; 52 Department of
Internal Medicine, Erasmus Medical Center, Rotterdam, The Netherlands; 53 Department of Medicine,
Landspitali University Hospital, 101 Reykjavik, Iceland; 54 Boston University School of Medicine,
Framingham Heart Study, Framingham, MA, USA; 55 Institut für Klinische Molekularbiologie,
Christian-Albrechts Universität, Kiel, Germany; 56 Institute of Epidemiology, Helmholtz Zentrum
München – German Research Center for Environmental Health, Neuherberg, Germany; 57 Institut für
Humangenetik, Helmholtz Zentrum München, Deutsches Forschungszentrum für Umwelt und
Gesundheit, Neuherberg, Germany; 58 Institute of Medical Information Science, Biometry and
Epidemiology, Ludwig-Maximilians-Universität München, Germany; 59 Klinikum Grosshadern,
Munich, Germany; 60 Institut für Humangenetik, Technische Universität München, Germany; 61
Division of Endocrinology and Diabetes, Graduate School of Molecular Endocrinology and Diabetes,
University of Ulm, Ulm, Germany; 62 Division of Endocrinology, Department of Medicine, Medical
University of Graz, Austria; 63 Synlab Center of Laboratory Diagnostics Heidelberg, Heidelberg,
Germany; 64 Division of Clinical Chemistry, Department of Medicine, Albert Ludwigs University,
Freiburg, Germany; 65 LURIC non profit LLC, Freiburg, Germany; 66 Clinical Institute of Medical
and Chemical Laboratory Diagnostics, Medical University Graz, Austria; 67 Institute of Public Health,
Social and Preventive Medicine, Medical Faculty Manneim, University of Heidelberg, Germany; 68
Cardiology Group Frankfurt-Sachsenhausen, Frankfurt, Germany; 69 Cardiovascular Epidemiology
and Genetics Group, Institut Municipal d’Investigació Mèdica, Barcelona; Ciber Epidemiología y
Salud Pública (CIBERSP), Spain; 70 Chronic Disease Epidemiology and Prevention Unit, Department
of Chronic Disease Prevention, National Institute for Health and Welfare, Helsinki, Finland; 71
Department of Molecular Biology and Center for Human Genetic Research, Massachusetts General

Hospital, Harvard Medical School, Boston, USA; 72 The Center for Applied Genomics, Children’s
Hospital of Philadelphia, Philadelphia, Pennsylvania, USA; 73 Cardiovascular Research Institute,
Medstar Health Research Institute, Washington Hospital Center, Washington, DC 20010, USA; 74
Genetics Division and Drug Discovery, GlaxoSmithKline, King of Prussia, Pennsylvania 19406, USA;
75 The Institute for Translational Medicine and Therapeutics, School of Medicine, University of
Pennsylvania, Philadelphia, PA, USA; 76 Department of Cardiovascular Surgery, University of
Leicester, Leicester, UK; 77 Division of Cardiovascular and Diabetes Research, Multidisciplinary
Cardiovascular Research Centre, Leeds Institute of Genetics, Health and Therapeutics, University of
Leeds, Leeds, LS2 9JT, UK; 78 LIGHT Research Institute, Faculty of Medicine and Health,
University of Leeds, Leeds, UK; 79 Nordic Center for Cardiovascular Research (NCCR), Lübeck,
Germany.
Sources of Funding
The ADVANCE study was supported by a grant from the Reynold's Foundation and NHLBI grant
HL087647.
Genetic analyses of CADomics were supported by a research grant from Boehringer Ingelheim.
Recruitment and analysis of the CADomics cohort was supported by grants from Boehringer
Ingelheim and PHILIPS medical Systems, by the Government of Rheinland-Pfalz in the context of the
“Stiftung Rheinland-Pfalz für Innovation”, the research program “Wissen schafft Zukunft” and by the
Johannes-Gutenberg University of Mainz in the context of the “Schwerpunkt Vaskuläre Prävention”
and the “MAIFOR grant 2001”, by grants from the Fondation de France, the French Ministry of
Research, and the Institut National de la Santé et de la Recherche Médicale.
The deCODE CAD/MI Study was sponsored by NIH grant, National Heart, Lung and Blood Institute
R01HL089650-02.
The German MI Family Studies (GerMIFS I-III (KORA)) were supported by the Deutsche
Forschungsgemeinschaft and the German Federal Ministry of Education and Research (BMBF) in the
context of the German National Genome Research Network (NGFN-2 and NGFN-plus), the EU

funded integrated project Cardiogenics (LSHM-CT-2006-037593), and the bi-national BMBF/ANR
funded project CARDomics (01KU0908A).
LURIC has received funding from the EU framework 6 funded Integrated Project “Bloodomics”
(LSHM-CT-2004-503485), the EU framework 7 funded Integrated Project AtheroRemo (HEALTH-
F2-2008-201668) and from Sanofi/Aventis, Roche, Dade Behring/Siemens, and AstraZeneca.
The MIGen study was funded by the US National Institutes of Health (NIH) and National Heart,
Lung, and Blood Institute’s STAMPEED genomics research program through R01 HL087676. Ron
Do from the MIGen study is supported by a Canada Graduate Doctoral Scholarship from the Canadian
Institutes of Health Research.
Recruitment of PennCATH was supported by the Cardiovascular Institute of the University of
Pennsylvania. Recruitment of the MedStar sample was supported in part by the MedStar Research
Institute and the Washington Hospital Center and a research grant from GlaxoSmithKline. Genotyping
of PennCATH and Medstar was performed at the Center for Applied Genomics at the Children’s
Hospital of Philadelphia and supported by GlaxoSmithKline through an Alternate Drug Discovery
Initiative research alliance award (M. P. R. and D. J. R.) with the University of Pennsylvania School
of Medicine.
The Ottawa Heart Genomic Study was supported by CIHR #MOP--82810 (R. R.), CFI #11966 (R.
R.), HSFO #NA6001 (R. McP.), CIHR #MOP172605 (R. McP.), CIHR #MOP77682 (A. F. R. S.).
The WTCCC Study was funded by the Wellcome Trust. Recruitment of cases for the WTCCC Study
was carried out by the British Heart Foundation (BHF) Family Heart Study Research Group and
supported by the BHF and the UK Medical Research Council. N. J. S. and S. G. B. hold chairs funded
by the British Heart Foundation. N. J. S. and A.H.G are also supported by the Leicester NIHR
Biomedical Research Unit in Cardiovascular Disease and the work described in this paper is part of
the research portfolio of the Leicester NIHR Biomedical Research Unit.

The Age, Gene/Environment Susceptibility Reykjavik Study has been funded by NIH contract
N01-AG-12100, the NIA Intramural Research Program, Hjartavernd (the Icelandic Heart Association),
and the Althingi (the Icelandic Parliament).
The Cleveland Clinic GeneBank study was supported by NIH grants P01 HL098055, P01HL076491-
06, R01DK080732, P01HL087018, and 1RO1HL103931-01.
The collection of clinical and sociodemographic data in the Dortmund Health Study was supported
by the German Migraine- & Headache Society (DMKG) and by unrestricted grants of equal share
from Astra Zeneca, Berlin Chemie, Boots Healthcare, Glaxo-Smith-Kline, McNeil Pharma (former
Woelm Pharma), MSD Sharp & Dohme and Pfizer to the University of Muenster. Blood collection
was done through funds from the Institute of Epidemiology and Social Medicine, University of
Muenster.
The EPIC-Norfolk study is supported by the Medical Research Council UK and Cancer Research
UK.
The EpiDREAM study is supported by the Canadian Institutes for Health Research, Heart and Stroke
Foundation of Ontario, Sanofi-Aventis, GlaxoSmithKline and King Pharmaceuticals.
Funding for Andrew Lotery from the LEEDS study was provided by the T.F.C. Frost charity and the
Macular Disease Society.
The Rotterdam Study is supported by the Erasmus Medical Center and Erasmus University
Rotterdam; the Netherlands Organization for Scientific Research; the Netherlands Organization for
Health Research and Development (ZonMw); the Research Institute for Diseases in the Elderly; The
Netherlands Heart Foundation; the Ministry of Education, Culture and Science; the Ministry of Health
Welfare and Sports; the European Commission (DG XII); and the Municipality of Rotterdam. Support
for genotyping was provided by the Netherlands Organization for Scientific Research (NWO)
(175.010.2005.011, 911.03.012), the Netherlands Genomics Initiative (NGI)/ NWO project nr. 050-
060-810 and Research Institute for Diseases in the Elderly (RIDE). This study is further supported by
a grant from NWO (Vici, 918-76-619).
The SAS study was funded by the British Heart Foundation.
The Swedish Research Council, the Swedish Heart & Lung Foundation and the Stockholm County
Council (ALF) supported the SHEEP study.
SMILE was funded by the Netherlands Heart foundation (NHS 92345). Dr Rosendaal is a recipient of
the Spinoza Award of the Netherlands Organisation for Scientific Research (NWO) which was used
for part of this work.
The Verona Heart Study was funded by grants from the Italian Ministry of University and Research,
the Veneto Region, and the Cariverona Foundation, Verona.
The Atherosclerosis Risk in Communities Study is carried out as a collaborative study supported by
National Heart, Lung, and Blood Institute contracts N01-HC-55015, N01-HC-55016, N01-HC-55018,
N01-HC-55019, N01-HC-55020, N01-HC-55021, and N01-HC-55022. The authors thank the staff
and participants of the ARIC study for their important contributions.
The KORA (Kooperative Gesundheitsforschung in der Region Augsburg) research platform was
initiated and financed by the Helmholtz Zentrum München - National Research Center for
Environmental Health, which is funded by the German Federal Ministry of Education, Science,
Research and Technology and by the State of Bavaria. Part of this work was financed by the German
National Genome Research Network (NGFN-2 and NGFNPlus) and within the Munich Center of
Health Sciences (MC Health) as part of LMUinnovativ.
Work described in this paper is part of the research portfolio supported by the Leicester NIHR
Biomedical Research Unit in Cardiovascular Disease.
This work forms part of the research themes contributing to the translational research portfolio of
Barts and the London Cardiovascular Biomedical Research Unit which is supported and funded by the
National Institute of Health Research.
Disclosures
Dr Absher reports receiving an NIH research grant for the ADVANCE study. Dr Assimes reports
receiving an NIH research grant for the ADVANCE study. Dr Blankenberg reports receiving research
grants from NGFNplus for Atherogenomics and from BMBF for CADomics. Dr Boerwinkle received
research support from NIH/National Human Genome Research Institute (NHGRI), GWA for gene-
environment interaction effects influencing CGD; NIH/NHLBI, Molecular epidemiology of essential
hypertension; NIH/NHLBI, Genome-wide association for loci influencing coronary heart disease;
NIH/NHLBI, Genetics of hypertension-associated treatment; NIH/NHLBI, Modeling DNA diversity
in reverse cholesterol transport; NIH/NHLBI, 20-year changes in fitness and cardiovascular disease
risk; NIH/NHLBI, Genetic epidemiology of sodium-lithium countertransport; NIH/National Institute
of General Medical Sciences (NIGMS), Pharmacogenomic evaluation of antihypertensive responses;
NIH/NIGMS, Genomic approaches to common chronic disease; NIH/NHLBI, Genes of the CYP450-
derived eicosanoids in subclinical atherosclerosis; NIH/NHGRI-University of North Carolina, Chapel
Hill, Genetic epidemiology of causal variants across the life course; and NIH/NHLBI, Building on
GWAS for NHLBI-diseases: the CHARGE consortium. Dr Cupples reports receiving research grants
from NIH/NHLBI, The Framingham Heart Study; NIH/NHLBI, Genome-wide association study of
cardiac structure and function; NIH/NHLBI, Functional evaluation of GWAS loci for cardiovascular
intermediate phenotypes; and NIH/NHLBI, Building on GWAS for NHLBI-diseases: the CHARGE
consortium. Dr Halperin reports receiving research grants from NIH, subcontract Genome-wide
association study of Non Hodgkin’s lymphoma; ISF, Efficient design and analysis of disease
association studies; EU, consultant AtheroRemo; NSF, Methods for sequencing based associations;
BSF, Searching for causal genetic variants in breast cancer and honoraria from Scripps Institute,
UCLA. Dr Halperin also reports ownership interest in Navigenics. Dr Hengstenberg reports receiving
research grants for EU Cardiogenics. Dr Holm reports receiving a research grant from NIH; providing
expert witness consultation for the district court of Reykjavik; serving as member of the editorial
board for decodeme, a service provided by deCODE Genetics; and employment with deCODE
Genetics. Dr Li reports receiving research grant R01HG004517 and other research support in the form

of coinvestigator on several NIH-funded grants and receiving honoraria from National Cancer Institute
Division of Cancer Epidemiology and Genetics. Dr McPherson reports receiving research grants from
Heart & Stroke Funds Ontario, CIHR, and CFI. Dr Rader reports receiving research grant support
from GlaxoSmithKline. Dr Roberts reports receiving research grants from the Cystic Fibrosis
Foundation, NIH, and Cancer Immunology and Hematology Branch; membership on the speakers
bureau for AstraZeneca; receiving honoraria from Several; and serving as consultant/advisory board
member for Celera. Dr Stewart reports receiving research grant support from CIHR, Genome-wide
scan to identify coronary artery disease genes, and CIHR, Genetic basis of salt-sensitive hypertension
in humans; other research support from CFI: Infrastructure support; and honoraria from the Institute
for Biomedical Sciences, Academia Sinica, Taipei, Taiwan. Dr Thorleifsson is an employee of
deCODE Genetics. Dr Thorsteinsdottir reports receiving research grants from NIH and EU; serving as
an expert witness for a US trial; having stock options at deCODE Genetics; and having employment
with deCODE Genetics. Dr Kathiresan reports receiving research grants from Pfizer, Discovery of
type 2 diabetes genes, and Alnylam, Function of new lipid genes, and serving as consultant/advisory
board member for DAIICHI SANKYO Merck. Dr Reilly reports receiving research grant support from
GlaxoSmithKline. Dr Schunkert reports receiving research grants from the EU, project Cardiogenics;
NGFN, project Atherogenomics; and CADnet BMBF. M. Preuss, L. Chen, and Drs König, Thompson,
Erdmann, Hall, Laaksonen, März, Musunuru, Nelson, Burnett, Epstein, O’Donnell, Quertermous,
Schillert, Stefansson, Voight, Wells, Ziegler, and Samani have no conflicts to disclose. Genotyping of
PennCATH and MedStar was supported by Glaxo-SmithKline. Dawn M. Waterworth, Max C.
Walker, and Vincent Mooser are employees of GlaxoSmithKline. PennCath/MedStar investigators
acknowledge the support of Eliot Ohlstein, Dan Burns and Allen Roses at GlaxoSmithKline.

SUPPLEMENTAL SECTION S8: PROCARDIS MEMBERS AND AFFILIATIONS
The PROCARDIS Consortium
Project Steering Committee: Hugh Watkins (chair) 1,2
, Anders Hamsten3, Rory Collins
4, Udo
Seedorf5, Maria Grazia Franzosi
6, Jörg Hager
7, Fiona Green
8, Michael Parker
9, Jose Manuel Soria
10,
Elena Tremoli11,12
, Johan Björkegren13
, Anna Walentinsson14
, Carla Finocchiaro15
Department of Cardiovascular Medicine, University of Oxford: Anuj Goel1, Martin Farral
1,2,
Shapour Jalilzadeh1, Theodosios Kyriakou
1, Halit Ongen
1, John F Peden
1, Hugh Watkins
1,2
Atherosclerosis Research Unit, Department of Medicine, Solna, Karolinska Institutet: Per
Eriksson3, Lasse Folkersen
3, Anders Hamsten
3, Mai-Lis Hellénius
3, Ferdinand vant Hooft
3, Jacob
Lagercrantz3, Anders Mälarstig
3, Maria Sabater-Lleal
3, Bengt Sennblad
3, Angela Silveira
3, Rona
Strawbridge3, John Öhrvik
3
Clinical Trial Service Unit, University of Oxford: Robert Clarke4, Rory Collins
4, Jemma C
Hopewell4, Pamela Linksted
4, Sarah Parish
4
Leibniz-Institut für Arterioskleroseforschung an der Universität Münster: Gerd Assmann5,
Stephan Rust5, Udo Seedorf
5
Department of Cardiovascular Research, Istituto Mario Negri: Simona Barlera6, Maria Grazia
Franzosi6, Gianni Tognoni
6
Centre National de Genotypage: Marc Delepine7, Jörg Hager
7, Simon Heath
7, Mark Lathrop
7
Division of Biomedical Sciences, University of Surrey: Fiona Green8
The Ethox Centre, University of Oxford: Paula Boddington9, Michael Parker
9
Institut de Recerca del Hospital de la Santa Creu I Sant Pau: Alfonso Buil10
, Jose Manuel Soria10
,
Juan Carlos Souto10

Centro Cardiologico Monzino and Dipartimento di Scienze Farmacologiche e Biomolecolari,
University of Milan: Cristina Banfi11,12
, Elena Tremoli11,12
Clinical Gene Networks AB: Johan Björkegren13
, Josefin Skogsberg13
, Jesper Tegnér13
CV Genetics and Molecular Biology, AstraZeneca R&D: Per G Olsson14
, Gunnar O Olsson14
, Anna
Walentinsson14
CF consulting S.r.l: Serena Cogoni15
, Carla Finocchiaro15
, Tessa Gronchi15
Affiliations
1 Department of Cardiovascular Medicine, The Wellcome Trust Centre for Human Genetics,
University of Oxford, Oxford, United Kingdom; 2 Department of Cardiovascular Medicine, University
of Oxford, John Radcliffe Hospital, Headington, Oxford, United Kingdom; 3 Atherosclerosis Research
Unit, Department of Medicine, Solna, Karolinska Institutet, Karolinska University Hospital Solna,
Stockholm, Sweden; 4 Clinical Trial Service Unit, University of Oxford, United Kingdom; 5 Leibniz-
Institut für Arterioskleroseforschung an der Universität Münster, Münster, Germany; 6 Department of
Cardiovascular Research, Istituto Mario Negri, Milan, Italy; 7 Centre National de Genotypage,
Institut Genomique, Commisariat L’Energie Atomique, Evry,France; 8 Division of Biomedical
Sciences, Faculty of Health and Medical Sciences, University of Surrey, Surrey, United Kingdom; 9
The Ethox Centre, Institute of Health Sciences, University of Oxford, Oxford, United Kingdom; 10
Institut de Recerca del Hospital de la Santa Creu I Sant Pau, Barcelona, Spain; 11 Centro Cardiologico
Monzino, IRCCS, Milan, Italy; 12 Dipartimento di Scienze Farmacologiche e Biomolecolari,
University of Milan, Milan, Italy; 13 Clinical Gene Networks AB, Stockholm, Sweden; 14 CV
Genetics and Molecular Biology , AstraZeneca R&D, Mölndal, Sweden; 15 CF consulting S.r.l,
Milan, Italy.

SUPPLEMENTAL SECTION S9: WRITING GROUP, STUDY AND INSTITUTIONAL
AFFILIATIONS
Writing Group: Karl Gertow1, Bengt Sennblad
1, Rona J. Strawbridge
1, John Öhrvik
1, Delilah
Zabaneh2, Sonia Shah
2, Fabrizio Veglia
3, Cristiano Fava
4,5, Bruna Gigante
11, Karin Leander
11, Max
Vikström11
, Gualtiero I. Colombo3, Jacqueline F. Price
8, Olle Melander
4, Damiano Baldassarre
3,40,
Elena Tremoli3,40
, Ulf de Faire11
, Steve E. Humphries24
, Anders Hamsten1 (chair)
The following is a list of study and institutional affiliations:
IMPROVE: 1 Atherosclerosis Research Unit (K.G., B.S., R.J.S., J.Ö., M.L., A.S., M.S-L.,
A.Hamsten), Department of Medicine, Solna, Karolinska Institutet, Karolinska University Hospital
Solna, Stockholm, Sweden; 11 Division of Cardiovascular Epidemiology (B.G., K.L., M.V., U.de F.),
Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden; 36 Department of
Medical Sciences (A-C.S.), Uppsala University, Sweden; 2 University College London Genetics
Institute (D.Z., S.S.), University College London, London, United Kingdom; 24 Cardiovascular
Genetics (S.E.H.), BHF Laboratories, Rayne Building, University College London, London, United
Kingdom; 3 Centro Cardiologico Monzino, IRCCS, (F.V., G.I.C., D.B., E.T.), and 40 Dipartimento di
Scienze Farmacologiche e Biomolecolari (D.B., E.T.), University of Milan, Milan, Italy; 18 Institute
of Public Health and Clinical Nutrition (K.N., T-P.T.), University of Eastern Finland, Kuopio,
Finland; 19 Kuopio Research Institute of Exercise Medicine (R.R., K.S.), Foundation for Research in
Health Exercise and Nutrition, Kuopio, Finland; 20 Department of Clinical Physiology and Nuclear
Medicine (R.R., K.S.), Kuopio University Hospital, Kuopio, Finland; 21 Department of Medicine
(A.J.S.), University Medical Center Groningen, Groningen, the Netherlands; 22 Assistance Publique -
Hopitaux de Paris (P.G.), Service Endocrinologie-Metabolisme, Groupe Hôpitalier Pitie-Salpetriere,
Unités de Prévention Cardiovasculaire, Paris, France; 23 Internal Medicine (E.M.), Angiology and
Arteriosclerosis Diseases, Department of Clinical and Experimental Medicine, University of Perugia,
Perugia, Italy.
Rotterdam Study: 6 Department of Epidemiology (M.Kavousi, A.G.U., A.Hofman, J.C.M.W.),
Erasmus University Medical Center, Rotterdam, The Netherlands; 16 Department of Internal Medicine
(A.G.U), Erasmus University Medical Center, Rotterdam, The Netherlands; 7 Netherlands Genomics
Initiative - Sponsored Netherlands Consortium for Healthy Ageing (M.Kavousi, A.G.U, A.Hofman,
J.C.M.W.), Rotterdam, The Netherlands.
Whitehall-II: 2 University College London Genetics Institute (D.Z., S.S.), University College
London, London, United Kingdom; 12 Cardiothoracic Unit (J.D.), Great Ormond Street Hospital,
London, United Kingdom; 9 Genetic Epidemiology Group (M.Kivimäki., M.Kumari, C.L., A.D.H.),
Department of Epidemiology and Public Health, University College London, London, United
Kingdom; 15 MRC Epidemiology Unit (C.L., N.J.W), Institute of Metabolic Science, University of
Cambridge, Addenbrooke's Hospital, Cambridge, United Kingdom; 39 Centre for Clinical
Pharmacology (A.D.H.), Department of Medicine, University College London, London, United
Kingdom; 24 Cardiovascular Genetics (P.J.T., S.E.H.), BHF Laboratories, Rayne Building, University
College London, London, United Kingdom.
Malmö Diet and Cancer Study: 4 Clinical Research Center (C.F., B.H., O.M.), Department of
Clinical Sciences, Lund University, Skåne University Hospital, Lund, Sweden; 5 Division of Internal
Medicine C (C.F.), Department of Medicine, University of Verona, Hospital "Policlinico G.B Rossi",
Verona, Italy; 13 Program in Medical and Population Genetics (B.F.V., P.F.), Broad Institute,
Cambridge, Massachusetts 02142, USA; 14 Center for Human Genetic Research and Diabetes
Research Center (Diabetes Unit) (B.F.V., P.F.), Massachusetts General Hospital, Boston,
Massachusetts 02114, USA.
Edinburgh Artery Study: 8 Centre for Population Health Sciences (S.M., J.L.B., C.M.R., J.F.P),
University of Edinburgh, Edinburgh, United Kingdom.
Advanced Study of Aortic Pathology: 1 Atherosclerosis Research Unit (L.F., P.E.), Department of
Medicine Solna, Karolinska Institutet, Karolinska University Hospital Solna, Stockholm, Sweden; 17

Cardiothoracic Surgery Unit (A.F-C.), Department of Molecular Medicine and Surgery, Karolinska
Institutet, Stockholm, Sweden.
Biobank of Karolinska Endarterectomies: 10 Experimental Cardiovascular Research Unit (L.F.,
A.G., G.K.H.), Department of Medicine Solna, Karolinska Institutet, Karolinska University Hospital,
Stockholm, Sweden; 17 Cardiothoracic Surgery Unit (U.H.), Department of Molecular Medicine and
Surgery, Karolinska Institutet, Stockholm, Sweden.
Precocious Coronary Artery Disease Study: 31 Department of Cardiovascular Medicine (M.F.,
H.W.), The Wellcome Trust Centre for Human Genetics, University of Oxford, Oxford, United
Kingdom; 32 Department of Cardiovascular Medicine (M.F., H.W.), University of Oxford, John
Radcliffe Hospital, Headington, Oxford, United Kingdom; 33 Clinical Trial Service Unit (R.C.),
University of Oxford, United Kingdom; 34 Department of Cardiovascular Research (M.G.F.), Istituto
Mario Negri, Milan, Italy; 35 Gesellschaft für Arterioskleroseforschung e.V. (U.S.), Leibniz-Institut
für Arterioskleroseforschung an der Universität Münster (LIFA), Münster, Germany. Names and
affiliations for all members of the PROCARDIS consortium are provided in Supplemental Section S8.
Coronary Artery Disease Genome Wide Replication and Meta-Analysis Consortium: 25
Universität zu Lübeck, Medizinische Klinik II (J.E.), Lübeck, Germany; 26 The Institute for
Translational Medicine and Therapeutics (M.P.R.), School of Medicine, University of Pennsylvania,
Philadelphia, PA, USA; 27 The Cardiovascular Institute (M.P.R.), University of Pennsylvania,
Philadelphia, PA, USA; 28 National Heart, Lung, and Blood Institute's (NHBLI’s) Framingham Heart
Study (C.J.O), Framingham, Mass, USA; 29 Division of Intramural Research (C.J.O.), NHLBI,
Bethesda, USA; 30 Cardiology Division (C.J.O.), Department of Medicine, Massachusetts General
Hospital, Harvard Medical School, Boston, Mass, USA; 37 Department of Cardiovascular Sciences
(N.J.S.), University of Leicester, Glenfield Hospital, Leicester, United Kingdom; 38 Leicester NIHR
Biomedical Research Unit in Cardiovascular Disease (N.J.S.), Glenfield Hospital, Leicester, United
Kingdom. Names and affiliations for all members of the CARDIoGRAM consortium are provided in
Supplemental Section S7.

SUPPLEMENTAL TABLES 1-3

Supplemental Table 1. Description of the discovery and replication cohorts, genotyping technologies, and quality control criteria
IMPROVE Whitehall-II Edinburgh Artery Study (EAS) Malmö Diet and Cancer (Cardiovascular arm) Rotterdam Study-I Rotterdam Study-II
Prospective Prospective Prospective Prospective Prospective Prospective
European European European (Scotland) Swedish European European
N (%M) 3430 (48) 2138 (77) 630 (46) 2143 (49) 4699 (41) 1980 (46)
Age (years) 64.2 (5.4) 60.74 (5.9) 69.75 (5.68) 57.4 (6.0) 68.9 (8.70) 64.7 (7.9)
BMI kg/m2 mean (sd) 27.2 (4.3) 26.55 (4.11) 26.31 (4.06) 25.1 (3.4) 26.3 (3.6) 27.3 (4.2)
SBP mmHg mean (sd) 142.0 (18.5) 126.82 (15.8) 147.48 (24.13) 139.9 (18.6) 138.9 (22.1) 143.0 (21.2)
DBP mmHg mean (sd) 82.0 (9.7) 73.95 (10.2) 82.19 (12.41) 82.2 (9.5) 73.6 (11.4) 79.0 (11.0)
Current smokers % 14.9 7.4 18.25 25.6 23.4 19.6
Lipid-lowering therapy % 49.5 10.7 N/A 1.8 2.6 12.4
Anti-hypertensive therapy % 56.8 22 20.95 59.4 17.8 21.8
Diabetes % 26.7 1.5 4.6 0 10 10.6
HDL-Chol mmol/L mean (sd) 1.26 (0.36) 1.57 (0.44) 1.45 (0.38) - at baseline 1.39 (0.36) 1.34 (0.36) 1.37 (0.37)
LDL-Chol mmol/L mean (sd) 3.55 (1.00) 3.47 (2.42) 5.36 (1.21) - at baseline 4.13 (0.95) TBC TBC
Total-Chol mmol/L mean (sd) 5.50 (1.13) 5.7 (0.98) 7.11 (1.3) - at baseline 6.08 (1.04) 6.63 (1.21) 5.78 (0.99)
Triglycerides mmol/L mean (sd) 1.59 (1.24) 1.35 (0.84) 1.53 (0.88) - at baseline 1.23 (0.57) - 1.60 (0.88)
Fasting glucose mmol/L mean (sd) 5.92 (1.65) 5.38 (0.9) 5.78 (1.38) - at baseline 4.78 (0.33) 6.89 (2.59) - not fasting 6.0 (1.7)
Common carotid baseline IMT variable(s) CC-IMTmean, CC-IMTmax, CC 1st cm-IMTmean, CC 1st cm-IMTmax CC-IMTmean CC-IMTmean CC-IMTmean (right only) CC-IMTmax CC-IMTmax
Bifurcation baseline IMT variable(s) Bif-IMTmean, Bif-IMTmax - - Bif-IMTmax (right only) - -
Composite baseline IMT variable(s) IMTmean, IMTmax, IMTmean-max - - Plaque score (right only) - -
IMT variable transformation(s) log10 log10 log10 log10 ln (recalculated to log10 for meta-analysis) ln (recalculated to log10 for meta-analysis)
IMT units mm mm mm mm mm mm
Genotyping centre Uppsala , Sweden UCL Genomics and Cambridge Edinburgh Clinical Research Facility- Genetics Core Broad Institute of Harvard and MIT Erasmus MC Rotterdam Erasmus MC Rotterdam
Genotyping platform Illumina CardioMetabochip Illumina CardioMetabochip Illumina CardioMetabochip Illumina CardioMetabochip Illumina HumanHap 550 Illumina HumanHap 550
Genotype calling algorithm GeneCall Illumina GenomeStudio GeneCall BIRDSEED (modified for Illumina Intensity Data) Illumina BeadStudio Illumina BeadStudio
Pre-imputation quality control - - - - MAF>0.01, Call rate>0.98, HWE p>1x10-6
MAF>0.01, Call rate>0.98, HWE p>1x10-6
Imputation software - - - - Mach (v1.0.1.5) Mach (v1.0.1.5)
Call rate criteria ≥95% ≥90% ≥95% ≥95% ≥97.5% ≥97.5%
Exclusion criteria
relatedness (confirmed or cryptic), reported non-European descent,
outliers identified by multi-dimensional scaling, estimated inbreeding
(excessive homozygosity), mismatch between recorded and genotype-
determined sex
cryptic relatedness, outliers
determined by multidimensional
scaling, mismatch between
recorded and genotype-
determined sex
cryptic relatedness, outliers determined by
multidimensional scaling, mismatch between recorded
and genotype-determined sex
excess or deficient homozygosity, excess low-level
identity by descent (IBD) sharing (PIHAT>0.1,
pairwise close kinship (PIHAT>0.2), outliers
identified in principal components space
excess autosomal heterozygosity >0.336
(~FDR<0.1%), mismatch between recorded and
genotype-determined sex, outliers identified by
identity by state (IBS) clustering analysis (>3
standard deviations from population mean), first
or second degree relatives using IBS
probabilities>97%
excess autosomal heterozygosity >0.336
(~FDR<0.1%), mismatch between recorded and
genotype-determined sex, outliers identified by
identity by state (IBS) clustering analysis (>3
standard deviations from population mean), first
or second degree relatives using IBS
probabilities>97%
N SNPs after quality control filtering 127,998 (127,830 autosomal SNPs included in discovery analysis) 131,007 125,888 179,195 530,683 495,478
Call rate criteria ≥90% ≥98% ≥90% ≥95% ≥90% ≥90%
Hardy-Weinberg equilibrium (HWE) criteria* p>5x10-7
p>5x10-7
p>5x10-7
p>1x10-6
p>5x10-5
p>5x10-5
Minor allele frequency (MAF) criteria* ≥0.005 ≥0.005 ≥0.005 ≥0.01 >0.01 >0.01
Adjustments population substructure (multi-dimensional scaling), age, sex age and sex age and sex age and sex age and sex age and sex
Analysis method linear regression linear regression linear regression linear regression linear regression linear regression
Genetic model additive additive additive additive additive additive
Software for analysis plink (version 1.07) plink (version 1.07) plink (version v1.07) plink (version 1.07) R using ProbABEL software (version 1.1) R using ProbABEL software (version 1.1)
Cohort reference (PMID) 19952003 15576467 9576427 8429286 21877163 21877163
Website - - - - http://rotterdamstudy.com/index.html http://rotterdamstudy.com/index.html
Cohort
Study type
Ethnicity
Genotyping
Characteristics
*For the meta-analysis in the current study, HWE and MAF filters were applied centrally.
IMT variables
Sample quality control
References
Imputation
SNP quality control
Analysis

Supplemental Table 2. Loci selected for replication based on association with CC-IMT in the discovery analysis (P<1x10-4
)
Discovery Replication
SNP
Nearest
gene Chr Pos
Alleles
effect/other Freq Beta SE n P Freq Beta SE n P
Heterogeneity
I2 Pheterogeneity
rs4901536 SAMD4A 14 54270284 T/C 0.29 0.013 0.0026 3429 9.97E-07
0.29 -0.0018 0.0011 11586 0.096 0 0.509
rs11256141 GATA3 10 9366107 C/T 0.17 0.0113 0.0024 3429 3.21E-06
0.17 0 0.0013 11583 1.000 38.2 0.167
rs17624670 NRG1 8 32245916 A/G 0.22 0.0128 0.0028 3427 5.62E-06
0.20 0.0004 0.0012 11587 0.732 44.9 0.123
rs11897302 OSR1 2 19637880 C/T 0.15 -0.0116 0.0026 3429 7.78E-06
0.13 0.0004 0.0015 11501 0.769 4.6 0.381
rs2925663 UBXN2B 8 59424423 T/C 0.13 0.011 0.0025 3427 1.07E-05
0.13 0.0002 0.0015 11587 0.888 0 0.952
rs4061073 SSBP3 1 54469331 G/A 0.28 0.0082 0.0019 3427 1.31E-05
0.31 -0.0013 0.0011 11585 0.228 0 0.512
chr18:55963125†‡ PMAIP1 18 55963125 T/C 0.007 0.0623 0.0143 3429 1.38E-05
0.0005 0.0018 0.0667 2768 0.978 0 0.985
rs11850769 BRMS1L 14 35492026 G/A 0.06 0.022 0.0051 3429 1.48E-05
0.06 -0.0027 0.0024 11586 0.257 0 0.775
rs2013056 RUNX1T1 8 93537351 T/C 0.15 0.0165 0.0038 3427 1.63E-05
0.13 0.0031 0.0014 11587 0.033 12.1 0.336
rs2972481 LSAMP 3 117048396 A/G 0.08 0.0186 0.0044 3428 2.07E-05
0.07 0.0006 0.0019 11586 0.750 44.3 0.127
rs17145627 GATA3 10 9336846 A/G 0.14 0.0111 0.0026 3429 2.20E-05
0.14 0.0016 0.0015 11585 0.268 0 0.624
rs4145320 TMEM26 10 62693320 A/G 0.49 -0.0101 0.0024 3423 2.36E-05
0.46 -0.0009 0.0010 11575 0.353 14.6 0.321
rs12453442 HLF 17 50745420 A/G 0.16 0.0158 0.0037 3427 2.39E-05
0.18 0.0012 0.0013 11583 0.348 19.0 0.293
rs13260097 FAM84B 8 127730309 A/G 0.11 -0.0113 0.0027 3427 2.55E-05
0.11 0.0021 0.0019 11587 0.280 0 0.506
rs2584681 PHB 17 44884745 A/G 0.25 -0.013 0.0031 3426 2.66E-05
0.28 -0.0013 0.0012 11587 0.261 0 0.570
chr6:119186493† C6orf204 6 119186493 A/G 0.16 -0.0133 0.0032 3429 3.07E-05
0.19 0.0006 0.0021 4907 0.758 0 0.790
rs7296372 KIAA0528 12 22517338 C/T 0.09 0.0136 0.0033 3429 3.36E-05
0.10 -0.0001 0.0016 11510 0.968 34.9 0.189
rs4723264§ BBS9 7 33164040 G/A 0.02 0.0303 0.0074 3429 3.94E-05
NA NA NA NA NA NA NA
rs12579259 IPO8 12 30395202 A/C 0.13 0.01 0.0025 3421 4.67E-05
0.12 0.0015 0.0015 11580 0.339 0 0.803
rs17164583 OR2A5 7 143370870 T/C 0.19 0.0088 0.0022 3426 4.88E-05
0.18 0.0026 0.0013 11512 0.041 0 0.509
rs1155530 FHIT 3 59702842 A/G 0.22 0.0087 0.0022 3429 4.97E-05
0.22 -0.0007 0.0012 11587 0.559 0 0.427
rs2551968 CCNYL1 2 208244781 A/C 0.45 -0.0096 0.0024 3429 4.98E-05
0.46 -0.0015 0.0010 11586 0.144 12.4 0.335
rs6491467 DOCK9 13 98349266 G/A 0.11 0.0152 0.0038 3429 5.58E-05
0.12 0.0033 0.0016 11587 0.037 0 0.956
rs4791906 GLP2R 17 9736177 T/C 0.35 -0.01 0.0025 3428 5.65E-05
0.35 0.0013 0.0010 11587 0.213 0 0.802
chr20:39103884† TOP1 20 39103884 G/A 0.02 0.0237 0.0059 3427 5.74E-05
0.02 -0.0034 0.0070 4908 0.623 14.2 0.312
rs11863148 RBFOX1 16 7065902 T/G 0.23 -0.0132 0.0033 3423 5.74E-05
0.25 0.0019 0.0011 11585 0.094 18.2 0.299
chr11:47233666* NR1H3 11 47233666 T/C 0.38 0.0111 0.0028 3422 6.29E-05
0.37 0.0025 0.0010 11564 0.016 9.1 0.355
rs2613235* CDH17 8 95262411 T/A 0.27 -0.0108 0.0027 3429 6.55E-05
0.22 -0.0014 0.0012 11584 0.249 27.2 0.240
rs6659255 SERINC2 1 31642256 T/C 0.13 -0.011 0.0028 3429 7.20E-05
0.12 0.0003 0.0015 11588 0.823 57.0 0.054
rs2304977 KIAA0753 17 6454053 A/G 0.35 0.0111 0.0028 3427 7.30E-05
0.38 0.0014 0.0010 11586 0.168 35.1 0.188
rs1040691 FSCB 14 43711385 C/T 0.26 -0.0106 0.0027 3429 7.61E-05
0.26 -0.0003 0.0011 11588 0.759 56.9 0.054
rs4801882 SIGLEC5 19 56818865 A/G 0.44 0.0067 0.0017 3427 7.88E-05
0.45 -0.0003 0.0010 11587 0.762 0.5 0.404
rs9295957 HCG27 6 31265572 A/G 0.18 -0.014 0.0036 3427 8.27E-05
0.21 0.0010 0.0012 11586 0.425 19.0 0.293
rs8085514 HRH4 18 20447234 T/C 0.42 0.0108 0.0027 3427 9.00E-05
0.40 -0.0013 0.0010 11588 0.204 0 0.740
rs10171653 EML6 2 54981105 A/G 0.18 0.0086 0.0022 3427 9.23E-05
0.17 0.0036 0.0013 11499 0.007 9.0 0.355
chr17:61664923† APOH 17 61664923 A/G 0.009 0.0577 0.0147 3427 9.24E-05
0.008 0.0006 0.0091 4908 0.949 0 0.737
rs10757269 CDKN2BAS 9 22062264 A/G 0.49 0.0072 0.0018 3411 9.41E-05
0.54 -0.0020 0.0010 11458 0.044 0 0.952
rs10763757 SVIL 10 30119539 T/C 0.35 -0.0076 0.0019 3426 9.57E-05
0.36 -0.0010 0.0010 11586 0.316 0 0.744
rs1655217 TLE3 15 68339357 A/G 0.29 -0.0078 0.002 3428 9.68E-05 0.32 -0.0009 0.0011 11586 0.424 0 0.436

Supplemental Table 2 Footnote:
Discovery and replication meta-analysis P-values and beta-coefficients for the effect allele (minor allele in the discovery cohort) are shown after adjustments
for sex, age, and population substructure when applicable (multi-dimensional scaling in the IMPROVE discovery cohort only). Observations are sorted
according to discovery P-value. Chr: chromosome, Freq: frequency. SE: standard error. Between-cohort heterogeneity is described by I2 in percent and Q-test
P-values. Chromosome positions are given according to NCBI Build 36. *In the Rotterdam-I and Rotterdam-II studies, rs2157 was used as proxy for
rs2613235 and rs749067 for chr11:47233666. †The SNPs chr6:119186493, chr17:61664923, chr18:55963125, and chr20:39103884 were not imputed in the
Rotterdam-I and Rotterdam-II studies and therefore lost from analysis in these cohorts. ‡The rare SNP chr18:55963125 failed the general minor allele
frequency cut-off in the replication cohorts, however the association result is given for completeness. §The low-frequency SNP rs4723264 was only detected
in the discovery cohort.

Supplemental Table 3. Association of rs4888378 with individual segment-specific IMT phenotypes in IMPROVE
Results are shown from linear regression analysis using an additive model, adjusted for sex, age, and population substructure (multi-dimensional scaling). SE:
standard error. CC-IMTmean: mean IMT of the common carotid excluding the 1st cm proximal to the bifurcation, CC-IMTmax: maximum IMT of the common
carotid excluding the 1st cm proximal to the bifurcation, CC-1
st cm-IMTmean: mean IMT of the 1
st cm of the common carotid proximal to the bifurcation, CC-1
st
cm-IMTmax: maximum IMT of the 1st cm of the common carotid proximal to the bifurcation, Bif-IMTmean: mean IMT of the bifurcation, Bif-IMTmax: maximum
IMT of the bifurcation, ICA-IMTmean: mean IMT of the internal carotid artery, ICA-IMTmax: maximum IMT of the internal carotid artery.
IMT phenotype Beta SE n P
CC-IMTmean -0.0043 0.0017 3427 0.013
CC-IMTmax -0.0071 0.0028 3427 0.010
CC-1st cm-IMTmean -0.0039 0.0019 3429 0.038
CC-1st cm-IMTmax -0.0061 0.0024 3429 0.013
Bif-IMTmean -0.0129 0.0033 3409 1.02E-04
Bif-IMTmax -0.0174 0.0040 3409 1.13E-05
ICA-IMTmean -0.0115 0.0034 3397 8.18E-04
ICA-IMTmax -0.0160 0.0045 3397 3.71E-04

SUPPLEMENTAL FIGURE LEGENDS 1-4

Supplemental Figure 1. Plots of results from multi-dimensional scaling (MDS) analysis of the
CardioMetaboChip genotypes in IMPROVE after exclusion of 45 individuals who reported non-
Caucasian ethnicity or who were outliers in the MDS analysis. MDS analysis was performed using
n=83,856 SNPs obtained by applying a sequential filter of pairwise correlation of r2<0.5 within a
window size of 50 SNPs, and with 5 SNPs overlap between windows, as implemented by the indep-
pairwise function in PLINK. The first three dimensions used for adjustment in association analysis are
plotted. A color scheme according to recruitment centre is applied.
Supplemental Figure 2. Manhattan plots of the association P-values for segment-specific and
composite carotid IMT variables in the IMPROVE study, adjusted for sex, age and population
substructure (multi-dimensional scaling). SNPs are plotted with their P-values (as -log10 values) as a
function of genomic position (NCBI Build 36). The red line indicates the threshold for array-wide
significance (P=8.39x10-7
). The lead SNP rs4888378 is plotted with a larger symbol and colored in
green. Segment-specific variables: CC-IMTmean: mean IMT of the common carotid excluding the 1st
cm proximal to the bifurcation, CC-IMTmax: maximum IMT of the common carotid excluding the 1st
cm proximal to the bifurcation, CC-1st cm-IMTmean: mean IMT of the 1
st cm of the common carotid
proximal to the bifurcation, CC-1st cm-IMTmax: maximum IMT of the 1
st cm of the common carotid
proximal to the bifurcation, Bif-IMTmean: mean IMT of the bifurcation, Bif-IMTmax: maximum IMT of
the bifurcation, ICA-IMTmean: mean IMT of the internal carotid artery, ICA-IMTmax: maximum IMT of
the internal carotid artery. Composite IMT variables: IMTmean: over-all mean of segment-specific
IMT means, IMTmax: over-all maximum of segment-specific IMT maxima, IMTmean-max: mean of the
segment-specific IMT maxima.
Supplemental Figure 3. A. Comparison of results from replication meta-analysis and bootstrap
analysis. Effect sizes (beta with 95% confidence intervals) of associations with common carotid IMT
(CC-IMT) are shown for SNPs that reached P<0.05 in the replication meta-analysis. The bootstrap
confidence intervals are adjusted for sample size (i.e. simulating an equal sample size as that of the
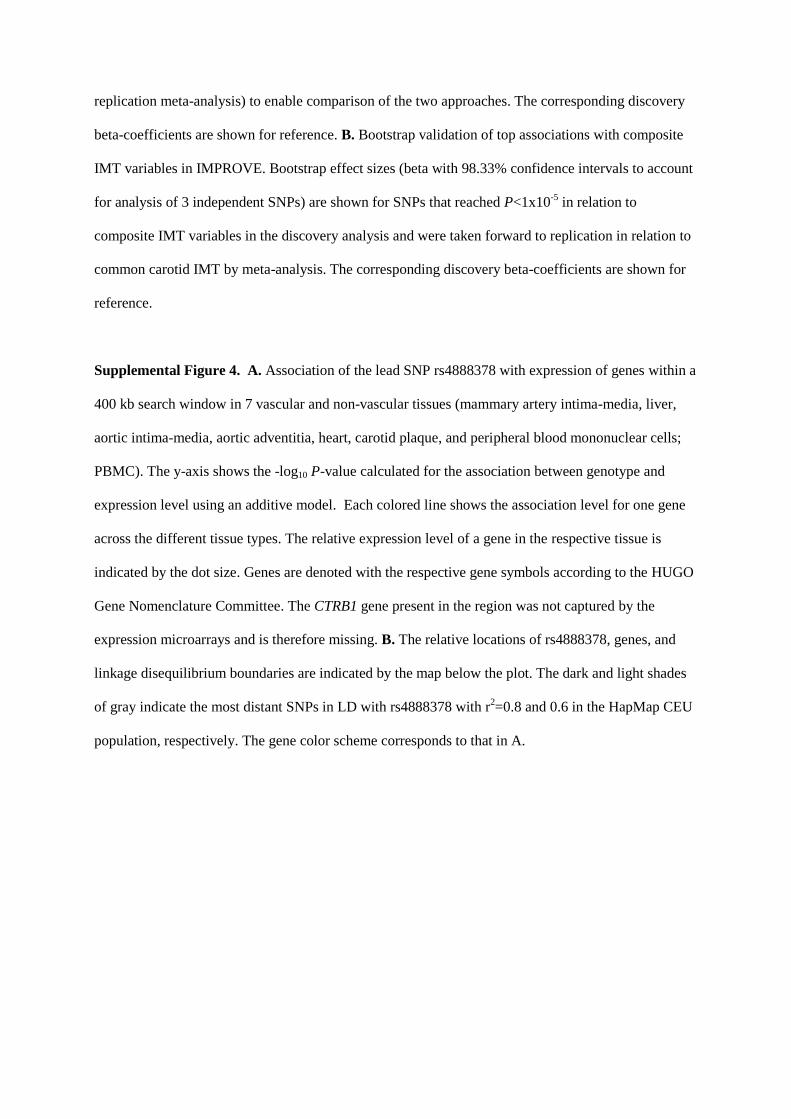
replication meta-analysis) to enable comparison of the two approaches. The corresponding discovery
beta-coefficients are shown for reference. B. Bootstrap validation of top associations with composite
IMT variables in IMPROVE. Bootstrap effect sizes (beta with 98.33% confidence intervals to account
for analysis of 3 independent SNPs) are shown for SNPs that reached P<1x10-5
in relation to
composite IMT variables in the discovery analysis and were taken forward to replication in relation to
common carotid IMT by meta-analysis. The corresponding discovery beta-coefficients are shown for
reference.
Supplemental Figure 4. A. Association of the lead SNP rs4888378 with expression of genes within a
400 kb search window in 7 vascular and non-vascular tissues (mammary artery intima-media, liver,
aortic intima-media, aortic adventitia, heart, carotid plaque, and peripheral blood mononuclear cells;
PBMC). The y-axis shows the -log10 P-value calculated for the association between genotype and
expression level using an additive model. Each colored line shows the association level for one gene
across the different tissue types. The relative expression level of a gene in the respective tissue is
indicated by the dot size. Genes are denoted with the respective gene symbols according to the HUGO
Gene Nomenclature Committee. The CTRB1 gene present in the region was not captured by the
expression microarrays and is therefore missing. B. The relative locations of rs4888378, genes, and
linkage disequilibrium boundaries are indicated by the map below the plot. The dark and light shades
of gray indicate the most distant SNPs in LD with rs4888378 with r2=0.8 and 0.6 in the HapMap CEU
population, respectively. The gene color scheme corresponds to that in A.

SUPPLEMENTAL FIGURES 1-4
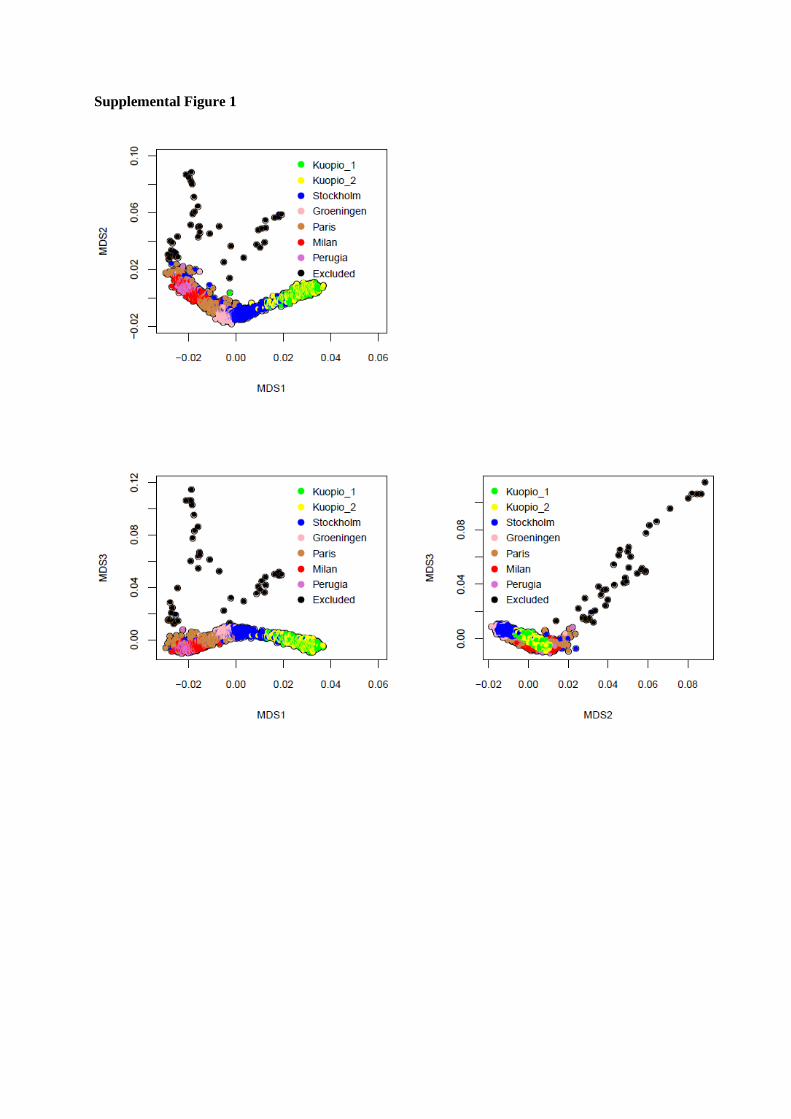
Supplemental Figure 1

Supplemental Figure 2

Supplemental Figure 3

Supplemental Figure 4

Recommended

















