Gestational diabetes
Dr. Garamvölgyi ZoltánI. Sz. Szülészeti és Nőgyógyászati Klinika,
Budapest

Definition
„At first during the pregnancy identified or developed the glucose-intolerance.”
(Diabetes Care Volume 30 Supplement 1, January 2007, p S42–S47)
Unnoted to the definition:
The method of the therapy (diet or insulin)
Existed IGT before or after the pregnancy

Prevalence•
Prevalence 6-8% (USA: 3-10%) 2000-3000 cases/year
Ethnics:
caucasian: 1,5-2 %
asian: 5-8 %
afroamerican: 5-8 %
hispan: 5-8 %
Higher prevalence :
Obesitas
Typ. 2. diabetes mellitus
Ogden CL et al. (2006) Prevalence of overweight and obesity in the United States, 1999-2004.
JAMA 295: 1549-1555
Mokdad AH et al. (2003) Prevalence of obesity, diabetes, and obesity-related health risk factors,
2001. JAMA 289: 76-79
Rosenberg TJ et al. (2005) Maternal obesity and diabetes as risk factors for adverse pregnancy
outcomes: differences among 4 racial/ethnic groups. Am J Public Health 95: 1545-1551
diabetes and pregnancy:
90 % GDM
8 % Typ. 2. DM
2 % Typ. 1. DM

Pathomechanism. of GDM
Pregnancy has got „diabetogen” effect
Insulinresistance (developing and increasing) (Progesteron, Östrogen, hPL, GH, TSH, kortizol, prolactin)
glucosetolerance and insulinsensitivity
insulinsecretion
bodyweight (fatty tissue)

GDM: β-cell dysfunction
• Autoimmunity(<10 %)
• Β-cell apoptosis(oxidative stress?)
IR
• Insulin signal pathway
Cause:- PCOS/obesity- GLUT4
- PPAR-γ expression ↓- Membrán glikoprotein-1
overexpression
+

Pregnancy
I. trimester Lipogenesis
LPL-activity
TG-level
II-III. trimester Lipolysis
HSL activity
Insulin-effect
FFA
Visceral obesity

Pregnancy
CRH
Sympathetic nervous system activity
Catecholemines Β-adrenoreceptors
II-III. trimester

I. trimester: extended anabolism fat tissue insulin sensitivity
II. trimester: katabolism, insulin sensitivity (30-60%) IR, insulin level (2-3x)Aminoacids lipids (lipolysis, keton, FFA, TG, cholesterol level incr.) Fasting bl.gl. pprandial bl.glucose
HbA1C and frustosamin: lower level in normal pregnancies than in non pregnants(hemodilution)
GDM: early ins.answ.delayed pprandial hyperglycaemia
hepatic gl.production reduced fasting pl. gl.level incr.

Pregnancy
IR o Diabetogen hormones
o Citokines
o Insulin signal cascade damaged
Chr. Β-cell damage/dysfunction Relative abscence of the insulin
(hormonal effect) >

PregnancyPlacental hormones
Insulin sensitivity of the mother
Fetal Source of Energy
GDM:
Accelerated macrophage infiltration
o musculoskeletal tissue
o fatty tissue
Citokines
o lipidperoxidation of the placenta
o oxidised LDL
Cytotoxical damage of the trophoblast
VEGF,eNOS
Placental angiogenesis and vascularisation
Fetal
Glucose
o uptake
o conversation to FFA

Abortus
spontaneusMaternal Chr. Subclinical inflammation
Embryo/fetus?
Habitualis ab.: 40-80 % of PCOS!
LH: effect on to the implantation (non PCOS vs PCOS= 12-15% vs 30-50%)
Uterinal factor: perifollicular bloodcirculation worse
Folliculus gene expression (androgen effect)
IGF-1: Y IGF-1 rec. downregulation
(morula’s gl.uptake decreases before the implantation)
GLUT-4 (cc. decr.)
IGFBP-1(cc.decr.) implantation/adhesion get worse

PCOS: else metab./endocrin. disorders
CRH-ACTH-kortizol axis activated
Hyperreninaemia/hyperaldosteronismus
PRL 2-3X
PAI-1/fibrinogen incr.
Hyperuricaemia/homociszteinaemia
Ferritin cc. Incr. (storage of iron incr.)
NAD(P)H-oxidase aktiv.Szuperoxid freeradical incr.
obesity
Musculature: gl.uptake decr.
Liver: inz.metab.decr.IR
GI tr.:Iron uptake incr.

Pedersen- hypothesis
Maternal plasma glucose:
Facilitied transplacental transmission

Obesity
GDM risk 20%
Hyperglycaemia
Hyperlipidaemia
Peripherial ins.sensitivity
Postprandial TG-level
Fuel mediated teratogenesis
I.trimester
Birth weight

Obesity
Glucose uptake of the muscle
Glycogen synthesis
LPL-activity hyperlipidaemia
Fatty tissue accumulates
-the musculoskeletal
-the live
Macrophag-infiltration
Of the fatty tissue
Proinflammatoric citokines

Obesity
LDL oxidised
Fibrinogen
PAI-1 (endothelium/liver)
enhance its production:
o bacterial lipopolisacharid
o IL-1, IL-6
o TNF-α
o TG
o thrombin
o lipoprotein-A
Thr.-aggregation:
-macrophages
-monocytes
-thrombocytes

Maternal morbidity
Urogenital infection
Hypertension
(in GDM 10%,
preeclampsia [12% vs. 8%])

Maternal morbidity
Detect GDM Hypertension Insulintherapy
I. Trimester 18,46 % 33,85 %
24-28. weeks 5,88 % 7,06 %
Diabetes mellitus diagnosed during early pregnancyJose L. Bartha, AJOG
Volume 182, Issue 2, Pages 346-350 (February 2000)

Maternal morbidity
Preeclampsia Fasting bl.glucose< 5,9 mmol/l
7,8 %
Fasting bl.glucose> 5,9 mmol/l
13,8 %
Yogev Y, Xenakis EM, Langer O. The association between preeclampsia and the
severity of gestational diabetes: the impact of glycemic control. Am J Obstet
Gynecol. Nov 2004;191(5):1655-60.

Fetal morbidity
Miscarrieges (1-2 % vs. 4-8 %, cardiovascular, malformation of the neurological system (neurol tube defect), Caudal Regression Syndrom, HbA1C-level before the conception. HbA1C <6,5%-min. 3 month, HBA1C<8,5%:3,4%, >8,5%: 22,4%!!!)
IUGR (Growth restiction: Typ.1. diabetes, hypertonia)
Growth acceleration (90th percentile, fetal insulin, central deposition of subcut. fat, 15-40 %, excessive rate of neonatal morbidity, offsprings and IGT)

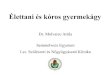
Antero-posterior radiographic view showing:
omissing ribs,
oabsent lumbosacral vertebrae,
ohypoplastic pelvis
o"frog-like" position of the lower extremities
Caudal regression syndrome
Sacral agenesia
Frequency: 1:60.000 diabetical females
Diabetes mellitus!
Non GDM

Macrosomy
Postprandial average
glucose value
Macrosomy (prevalence)
> 120 mg/dl (6,5 mmol/l) 20 %
> 160 mg/dl (8,9 mmol/l) 35 %
Birth weight> 4000g: 23 % (GDM) vs. 8 % (non diabetic) p < 0.001
Casey B, Lucas M, McIntire D et al. Pregnancy outcomes in women with gestational diabetes
compared with the general obstetric population. Obstet. Gynecol. 90, 869-873 (1997).
Abdominal circumference of the abdomen (AC) > 95 percentile:
macrosomy 90 %
In case of macrosomy increases AC und TG-levels after the 24th gest.week
(statistician significancy).
Shoulder distocia (0.3-0.5 % vs. 1-2 %)

Neonatal complications
Polycythemia
(Htc>65 %, 5-10 %, fetal erythropoietin Oxygen tension
ischemia, Infarction)
Hypoglycemia (Insulintherapy, Labour)
Hypocalcemia (< 7 mg/100 ml,
Hypoparathyreoidismus?)
Hyperbilirubinemia (prematurity, polycythaemia)
IRDS (Typ. 1. IDDM, prevalence decreased sice 1970.)

Screening and diagnosis
OGTT and different methods
Diagnostic
methods
Carpenter-
Coustan
(100g)
ADA
(100g)
WHO
(75g)
WHO
(75g)
IGT
Fasting
Plasma glucose
5,3 mmol/l 5,8 mmol/l 5,3 mmol/l 5,6-6,9
mmol/l
(IFG)
1 hour 10 mmol/l 10 mmol/l
2 hours 8,6 mmol/l 9,1 mmol/l 7,8 mmol/l 7,8 mmol/l
3 hours 7,8 mmol/l 8 mmol/l
Two steps pregnant pregnant One step
pregnant non pregnant
7,8 mmol/l (80%) vs. 7,2 mmol/l (90%) O’Sullivan és Mahan
(1964.)

Screening and diagnosis
Selective Screening (ADA)
82 % sensitivity
35% less screennig
procedure
At high risk patients
Universal Screening (WHO)
More diagnosis (35-47%)
Prompt diagnosis
Decreased morbidity
Increased sensitivity
Low risk
24-28. week
High risk
(I.Trimester)
OGTT
(ADA)
>7,8 mmol/l
OGTT
(ADA)
Low risk (no
Screening)
Middle risk
24-28. week
High risk
(I.Trimester)
OGTT
(WHO)
50g.GCT
O’Sullivan,
1973.

Screening and diagnosis
high risk patients:
Relatives suffered by diabetes mellitus
In the history
-IGT, GDM
-Eclampsia, premature labour, intrauterine death,
macrosomy, miscarrieges, malformations, hypertonia
BMI > 30 kg/m2
Age > 35 years
twins
Glucosuria
American Diabetes Association: Gestational diabetes mellitus
Diabetes Care 2004; 27 Suppl1.: S88-S90.

ADA, 1999. 2steps (selective) screening and diagnosis
50 g, 1 hour bl.sugar
≥7,8 mmol/l >11 mmol/l
GDM: No OGTT!3 hours GTT (100g)
National Diabetes Data Group (NDDG)
hour Bl.sugar (mmol/l)
0 5,8
1 10,6
2 9,2
3 8,1
≥2 values=GDM
3 hours OGTT
(100g)
IV.GDM Workshop
2 hours
OGTT (75g)
hour Bl.sugar (mmol/l) Bl.sugar (mmol/l)
0 5,3 5,3
1 10,0 10,0
2 8,6 8,6
3 7,8

Prospective, multicentrical study 2000-2006. 23316 females, 9 countries
Fasting bl.sug.+ 75 g OGTT, 24-32.weeks: 1hr, 2hrs + random pl.glucose
(34-37.weeks)
Til the postpartum 6th weeks followed up
Inhomogen ethnicitiy:
48% white, non hispan
12% black, non hispan
29% asian
8% hispan
3% others
Hyperglycemia and adverse pregnancy outcome (HAPO),
Pasadena, California

ADA: 75 gr. OGTT: 2 path.values = diagnosis
IADSG: 1 path.value = diagnosis
16,1 % GDM!!!
ADA, 2007: 57 million americans, 19% of the adult population has got prediabetes
1., pl. sugar level is a predictive value
2., multinational study
3., international consensus
4., I.trimester: fasting pl.sugar: <4,4 mmol/l (80 mg/dl) OGTT not recommended
5., universal screening (75 gr.OGTT)
HbA1C?
n= 21064 terhes
mean±SD: 4,79±0,4
Pregnancy outcome:
pl. sugar. vs.HbA1C:
pl. sugar has got sign. correlation (exepted: PE, prenatal labour)
IADSG

International Association of Diabetes and Pregnancy Study Groups (IADPSG)
2008. 75 g OGTT
Pl.glucose mmol/l
fasting 5,1
1 hr 10,0
2 hrs 8,5
fasting plasma bl.sugar ≥7 mmol/l
HbA1C ≥6.5%
Random plasma bl.sugar ≥11,1 mmol/l
GDM=≥1 value
Manifest diabetes

International Association of Diabetes and Pregnancy Study Groups (IADPSG)
2008.
At the time of the recognition of the
pregnancy at every pregnant womens
fasting pl.sugar
HbA1C
random pl.sugar
diabetes Fasting pl.sugar:
5,1-7,0 mmol/l
<5,1mmol/l
GDM
OGTT,75g:
24-28. weeks
Bl.sugar mmol/l
fasting 5,1
1 hr 10,0
2 hrs 8,5
GDM=≥1 value
Flow diagram of the screening and diagnosing of the GDM:

Clinical care of diabetic pregnancies
HbA1C (every 3 months) + fructosamin (oedema, proteins!, thyreoid
disorders)
Blood sugar levels from a capillary device 6-8 times/day
Ophthalmologic evaluation
Kidney –and liverfunction
24-h urine collection for protein and creatinin
NST
Ultrasonogram (AFI, Doppler-examination)
Fetal echocardiography (fasting plasma glucose >6,9 mmol/l, insulin dependent)

Attention at the preconceptional care:
preprand. vérc.: 3.5-5.5 mmol/lpostprand.vérc: 5-8 mmol/l + no acetonurie/glucosurie
NB: fasting bl.sugar >5.8 mmol/L: Danger of the IU death: til the 32th weeks(between the 32-36th weeks the most common)
Pregestational diabetes
Pregnancy is contraindicated:
proliferative retinopathy Advanced nephropathy severe ischaemic heartdisease HbA1C> 10%ketoacidosis during early pregnancy >40 yrs old + 2 childrenteenager girl + not planed pregnancy

Therapy
Goal: achieving euglycemia without glucosuria and
ketonuria
Metabolic control before and during pregnancy
Self-monitoring

Therapy
Dietary therapy
(total of 6 feedings, distribution, dietitian)
Insulin therapy
(increasing insulin resistance and fetal demand for
glucose, risk for hypoglycemia, timing)
Oral hypoglycemic agents
(risk of teratogenesis and hypoglycemia)

Self-monitoring :
(blood sugar measurement with capillary blood)
Fasting: 3,3-4,4 mmol/l Prepr: 3,3-5,5 mmol/l postp. 4-7 mmol/l (1ó)
3,5-6 mmol/l (2ó)
(Total weight gain < 8 kg/pregnancy)
mean. bl.sugar/day: 3,5-5 mmol/l
fructosamin: 170-220 umol/L HbA1C: 4,5-5,6 % (HbA1C <6%)
No glucosurie

Insulin therapy
When should begin?(nedded in 20-25 % of all cases)
Bloodsugar level ACOG
(American College of Obstetricians
and Gynecologists)
ADA
(American
Diabetes
Association)
WHO
(World Health
Organization)
Fasting >5,3 mmol/l > 5,9 mmol/l > 5,3 mmol/l
1. hour 7,2-7,8 mmol/l > 8,6 mmol/l
2. hours > 6,5 mmol/l > 7,2 mmol/l > 6,7 mmol/l
>7,0 mmol/l

Insulin demand
ITDM:
0-12. weeks: reduced (10%) 12-36. weeks: continually increasing(50%)>36. week: slow decreasing of the demand of the insulin.
IITDM:
Major rate the insulin resistance: III. trimester: 1,5-2 E/tskg
(90% need insulin therapy!)

7 mmol/l pp bl.sugar values:16-20 E Insulin (8-4-6 E)
>10 mmol/l pp. bl. sugar.:
(Fasting hyperglycaemia! Enhanced demand of insulin)
12-8-10 E + bedtime: 6-8 E basis (NPH-typ) insulin +
min 6 x meats/day
In case of major rate of insulin resistance:
5x or more times shortact (rapid) insulin:
6-12-17-22-3 hour(dose ratio: 5-3-4-2-1)
Time of the meats:
6:15-9:00-12:15-14:45-17:15-19:45-22:15
30-20-50-20-40-20-15 gr.
Before the mean meats: Actrapid H or Humulin R
Ultrarapid effect-insulin (Lispro, Aspart):
Need meats with great amount of the CH (not propriate in pregnancy)
Ultrarapid insulin analogs only in cases of insulin-pump (Not started at first during
pregnancy!)
Insulin therapy

Insulin therapy
Insulinanalogs and GDM
Changed structure of insulin:
Teratogenic effect?
High GF1 rec. affinity
Lispro + Aspart : not contraindicated
Glargin: cc.+malformatio 5-6x
Levemir: no datas+ „off label use”
Ultrarapid To hinder
Pp.bloodsugar
increasing
Humalog
Novorapid
Long effect Maternal
Hypoglycemia
Lantus (glargin)
Levemir
(detemir)
mixed Novomix 30
Humalog Mix 25

Insulin therapy:
Insulin analogs are differed to each other in structure of the aminoacids(better absorption, less risk of hypoglycaemia)
Human insulinLess immunogen activity, the insulin-antibodies do not cross the placenta
Before bedtime blood sugar measure obligated!Every 1-2 weeks diabetological controll.
HbA1C:In the I. trimester usableII. and III. trimester: routine-like usage not recommended(rather the pp. bl.sugar! (NICE))
Risk of the hypoglycaemia: vomiting make it severe (exp. between 10-15th weeks) I.TDM>II.TDM (NICE): <3,5 mmol/l.

Oral medicaments
name Medicament
-group
Effect Crossable to
placenta
I.
Trimester
Hypoglycemia +Insulin Lact.
Glyburide Szulfanilurea
II.Generation
Insulin
secretion
(Pancreas)
slightly (T1/2 ,
binding to
proteins)
no yes yes yes
Metformin Biguanoid Glucose
secretion
(Liver)
Glucose
uptake
(tissues)
highly yes
(PCOS!)
no yes
(30%)
no

Sulfanilurea, Glibenclamide (Glyburide)Enhanced insulin secretion. Risk of hypoglycaemia and weight gain!
Chlorpropamide and tolbutamide: no malformations, But neonatal icterus and hypoglycaemia. Minimum transmission through the placenta
Randomised controlled study(Langet et al, A comparison of glyburide and insulin in women with gestational diabetes mellitus. N. Engl. J. Med. 2000, 343: 1134-8.): NS: neonatal outcomes.
Metformin
Hepatic glucose production reducedEnhanced glucose uptake of the peripherial tissuesFFA cc. decreased, IR reduced.Entirely transmitted through the placentaMIG study: metformin vs insulin: after 20th weeks prefered the metformin (?)NICE ajánlás:NICE. Diabetes and pregnancy. Management of diabetes and its complications from pre-
conception to the postnatal period. London, 2008.

Management of the labour
GDM normal p
Induced labour 38,6 % 10,8 % <0,001
Cesarian section 34 % 20 % <0,001
Peled Y, Perri T, Cen R et al. Gestational diabetes mellitus - implications of
different treatment protocols. J. Pediatr. Endocrinol. Metab. 17(6), 847-852 (2004).

Intrapartum management of diabetic deliveries
Goal: maternal euglycemia during labour (4-7 mmol/l)
Insulin- glucose- potassium combinated infusion
Capillary glucose levels monitoring
Fetal heart rate monitoring
(intrauterine asphyxia)

Postpartum
Insulin?
Diet
Reclassification
contraception
Lactation

Postpartum
reclassification
170 g Diatery th.
6 weeks after the delivery
OGTT (WHO)
Normal OGTT Pathological OGTT
Repeat of OGTT after ½-1 year IFG IGT DM
World Health Organization (1999)
Definition, diagnosis and classification of diabetes mellitus and its complications.
Baranyi Éva

Late effect of the GDM
GDM + LGA Child
10-16 years:
overweight
Hypertension
Dyslipidemia
IGT (19,3 %)
Mother
IGT/DM (15 %)
recurrency of GDM (30-69 %)
Evans E, Patry R. Management of gestational diabetes mellitus and pharmacists'role in patient
education. Am. J. Health Syst. Pharm. 61, 1460-1465 (2004).
McKinney PA, Parslow R, Gurney KA, Law GR, Bodansky HJ, Williams R. Perinatal and neonatal
determinants of childhood type 1 diabetes. A case-control study in Yorkshire, U.K.
Diabetes Care. Jun 1999;22(6):928-32.
Recommended