Hypertensive EMERGENCY5 TAKE HOME POINTS

1EMERGENCY= Severe SYMPTOMATIC elevation in BP WITH evidence of end organ damage
Brain (seizures, increased ICP)Kidneys (renal insufficiency)Eyes (papilledema, retinal hemorrhage, exudates)Heart (heart failure)
URGENCY= Severe elevation in BP WITHOUT severesymptoms or evidence of end organ damage
Definitions

2Most common type of hypertensive emergency
Severe BP elevation with cerebral edema +neurological sx of lethargy and/or seizures
Pathophysiology: cerebrovascular endotheliumbreaks down secondary to failure of cerebral autoregulation
AMS/seizures occurred in 50% of 110 patientsin one retrospective series*. 27% had hypertensive retinopathy and 13% had LV hypertrophy
Hypertensive encephalopathy
*Deal JE et al. Arch Dis Child. 1992

3Etiologies
Renovascular dz(thromboembolism from
umbilical a. catheterization)
Congenital renal anomalies
Renal vein thrombosis
Coarctation of aorta
BPD
glomerulonephritis
renovascular disease
endocrine disease(pheochromocytoma,
neuroblastoma,excess exogenous
glucocorticoids)
renal parenchymal dz
preeclampsia
drugs(cocaine, amphetamines)
Chandar J et al. Pediatr Nephrol. 2012

4Approach
Confirm marked BP elevation
Rapid assessment of severity of disease
Exclusion of other causes of severe HTN for which rapid reduction of BP might be harmful
(intracranial injury, mass lesion, coarct, drugs)
Emergent antihypertensive therapy

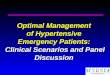
5Management
No large clinical trials evaluating management of HTN emergencies in kids
Goal: lower BP promptly by no more than 25% within 8 hours of treatment
For HTN emergency: bolus dose IV hydralazine or labetolol followed by nicardipine or labetolol ggt

5

5Management
DRUG DOSE ONSET DURATION MECH
Labetolol
Nicardipine
Hydralazine
Bolus: 0.2-1 mg/kg (max 40 mg/dose)
Infusion: 0.25-3 mg/kg/hr
2-5 mins
2-5 mins
10 min
alpha/beta adrenergic
blocker2-6 hr
30 min-4 hr
4-6 hoursDirect
vasodilator0.2-0.6 mg/kg
(max 20 mg)
Ca channel blocker
0.5-4 mcg/kg/min
Recommended