HIV Treatment Update
Anton Pozniak
Consultant Physician,
Director of HIV Services
Chelsea and Westminster Hospital, London

Guidelines
Nuke sparing
Nukes
Efavirenz placement as the gold standard ARV
Role of PIs
STRs
Switching
Second Line
Choosing the best Regimen
Evolution of Better Treatments DHHS panel criteria for regimen selection
Preferred regimens (studied in RCTs)
– Optimal and durable virologic efficacy
– Favourable tolerability and toxicity profiles
– Ease of use
DHHS Guidelines for the Use of Antiretroviral
Agents in HIV-1-Infected Adults and Adolescents.
March 27, 2012. Available at:
http://www.aidsinfo.nih.gov/Guidelines

Summary of key randomized clinical trials in ARV-naïve patients
1. Molina J-M, et al. Lancet 2011;478: 238–246; 2. Cohen CJ, et al. Lancet 2011; 378:229–237; 3. Daar E, et al. Ann Intern Med 2011;154:445–456; 4. Ortiz R, et al. AIDS 2008;22:1389–1397; 5. Lennox JL, et al. Lancet 2009;374:796−806; 6. Riddler SA, et al. N Engl J Med 2006;358:2095−2106; 7. Molina J-M, et al. Lancet 2008;372:646–655
EFV vs.
NNRTI 2NN, ECHO1,
THRIVE2
vs. PI ACTG 52023
ACTG
51426
vs. INI
STARTMRK5
ATV/r vs.
NNRTI ACTG 52023
vs. PI
CASTle
ACTG5257
DRV/r vs. PI
ARTEMIS4
ACTG5257
RAL vs.
NNRTI STARTMRK5
NNRTI = non-nucleoside reverse transcriptase inhibitor; PI = protease inhibitor; INI = integrase inhibitor.
EVG/c vs.
NNRTI QUAD102
vs. PI
QUAD103
DTG vs.
NNRTI Single
vs. INI
Spring
vs. PI
Flamingo
vs. INI
QUAD103
vs. INI
Spring
vs.
PI / NRTI
ACTG5257 NEAT001
vs. INI
ACTG5257
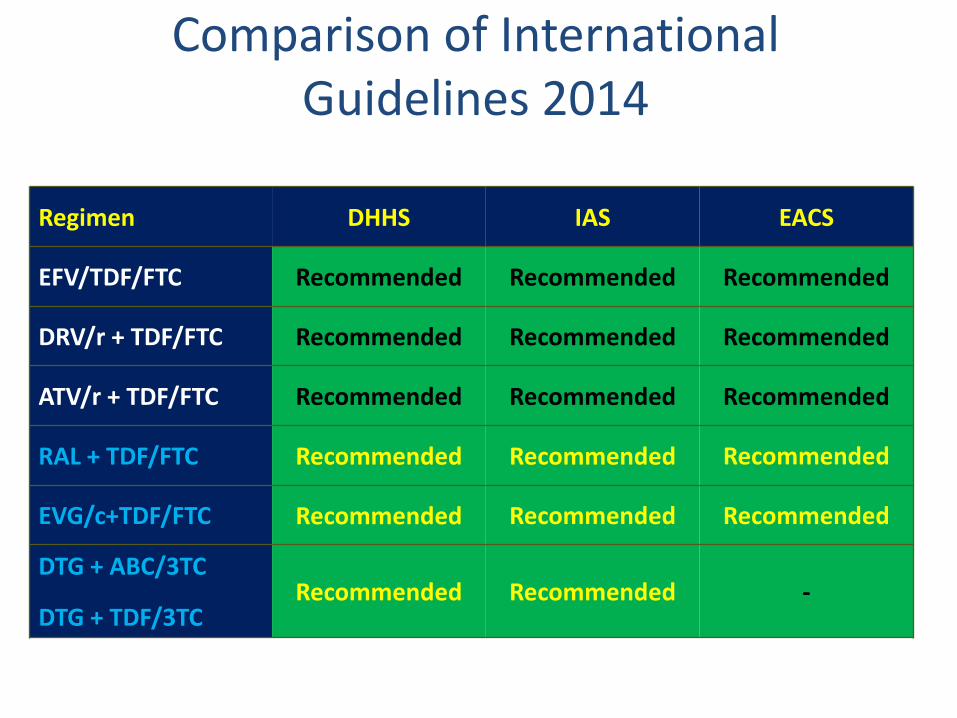
Comparison of International
Guidelines 2014 Regimen DHHS IAS EACS
EFV/TDF/FTC Recommended Recommended Recommended
DRV/r + TDF/FTC Recommended Recommended Recommended
ATV/r + TDF/FTC Recommended Recommended Recommended
RAL + TDF/FTC Recommended Recommended Recommended
EVG/c+TDF/FTC Recommended Recommended Recommended
DTG + ABC/3TC
DTG + TDF/3TC Recommended Recommended -
US Department of Health and Human Services Guidelines; Revised January 10, 2011 Available at: http://aidsinfo.nih.gov/contentfiles/AdultandAdolescentGL.pdf; Thompson MA, et al. JAMA 2010;304(3):321-333; www.eacs.eu.
DO WE STILL NEED NUKES?
TOLERABILITY AND TOXICITY
NUKES ASSOCIATED WITH
CVS, RENAL AND BONE PROBLEMS

NRTI-sparing regimens 7 randomised trials of PI/r + RAL versus PI/r + 2NRTIs
HIV RNA <50 copies/mL (switch = failure endpoint)
Overall, in 7 randomised trials of 1266 patients, PI/r + raltegravir showed HIV RNA suppression rates 10% lower than PI/r + 2NRTIs (p=0.008). However there was evidence for heterogeneity between the trials (p=0.03).
Favours 3-drug treatment
Favours 2-drug treatment
If we still need Nukes
We need to sort out the ABC CV question
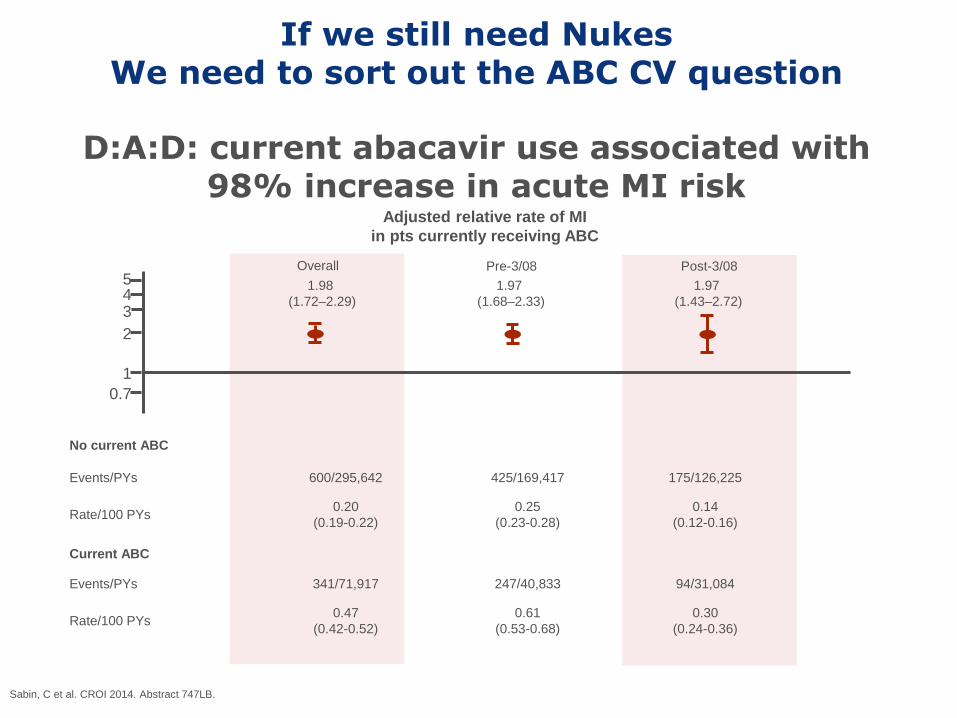
D:A:D: current abacavir use associated with 98% increase in acute MI risk
Sabin, C et al. CROI 2014. Abstract 747LB.
5 4 3
2
1
0.7
Adjusted relative rate of MI
in pts currently receiving ABC
Overall Pre-3/08 Post-3/08
1.98
(1.72–2.29)
1.97
(1.68–2.33)
1.97
(1.43–2.72)
No current ABC
Events/PYs 600/295,642 425/169,417 175/126,225
Rate/100 PYs 0.20
(0.19-0.22)
0.25
(0.23-0.28)
0.14
(0.12-0.16)
Current ABC
Events/PYs 341/71,917 247/40,833 94/31,084
Rate/100 PYs 0.47
(0.42-0.52)
0.61
(0.53-0.68)
0.30
(0.24-0.36)
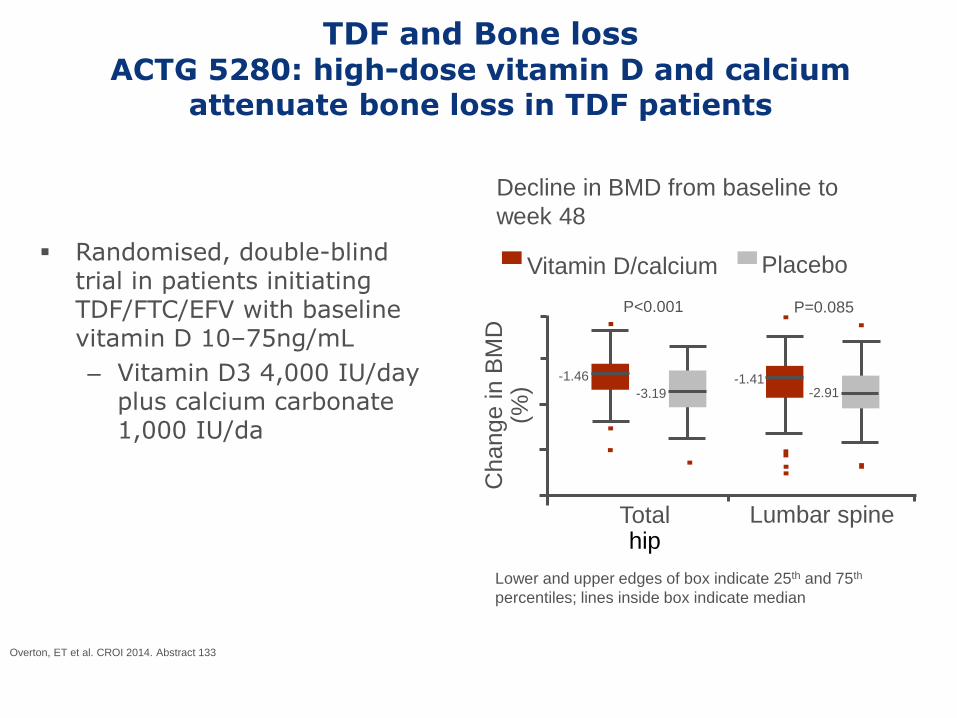
TDF and Bone loss ACTG 5280: high-dose vitamin D and calcium
attenuate bone loss in TDF patients
Randomised, double-blind trial in patients initiating TDF/FTC/EFV with baseline vitamin D 10–75ng/mL
– Vitamin D3 4,000 IU/day plus calcium carbonate 1,000 IU/da
Decline in BMD from baseline to
week 48
Overton, ET et al. CROI 2014. Abstract 133
Lower and upper edges of box indicate 25th and 75th
percentiles; lines inside box indicate median
5
0
-5
-10
-15 Total
hip Lumbar spine
-1.46
-3.19 -1.41
-2.91
P<0.001 P=0.085
Change in B
MD
(%
)
Placebo Vitamin D/calcium

IS IT TIME TO MOVE ON FROM EFAVIRENZ?
Why is EFV no longer so gold?
Has been ‘beaten’ by the integrase inhibitors
Non-inferior to other STRs (Stribild ▼ and Eviplera ▼) – But the latter have less toxicity
Baseline resistance increased in MSM
NNRTI resistance develops in about half of the failures
The toxicity is not acceptable now?
PI, important points to consider
and indication are outlined at the
end of this presentation
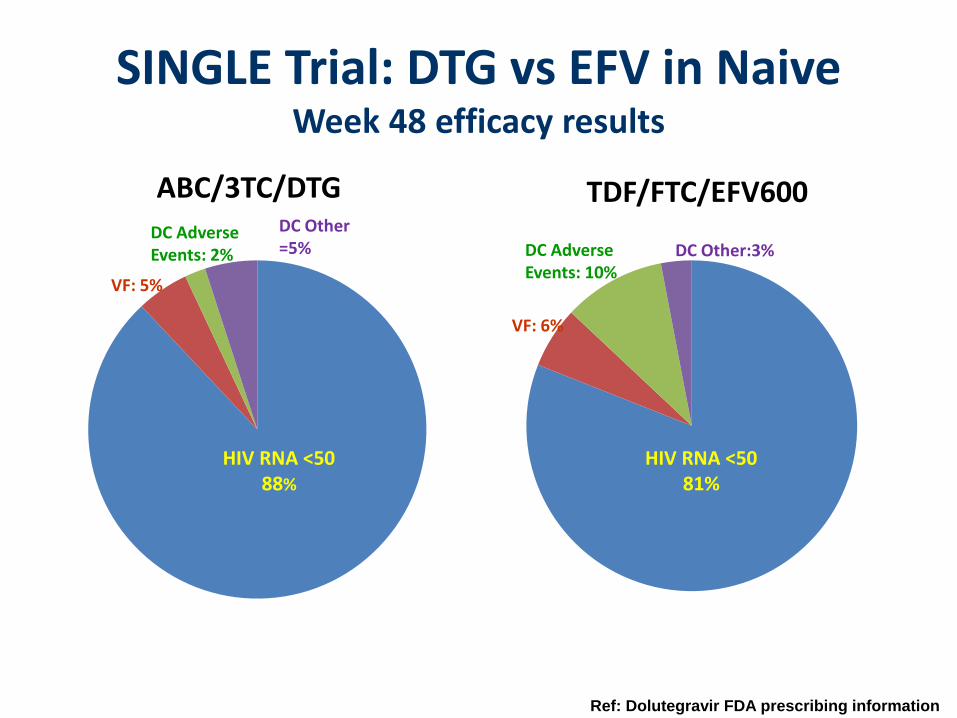
SINGLE Trial: DTG vs EFV in Naive Week 48 efficacy results
ABC/3TC/DTG TDF/FTC/EFV600
Ref: Dolutegravir FDA prescribing information
HIV RNA <50 88%
HIV RNA <50 81%
VF: 5%
VF: 6%
DC Adverse Events: 2% DC Adverse
Events: 10%
DC Other =5% DC Other:3%
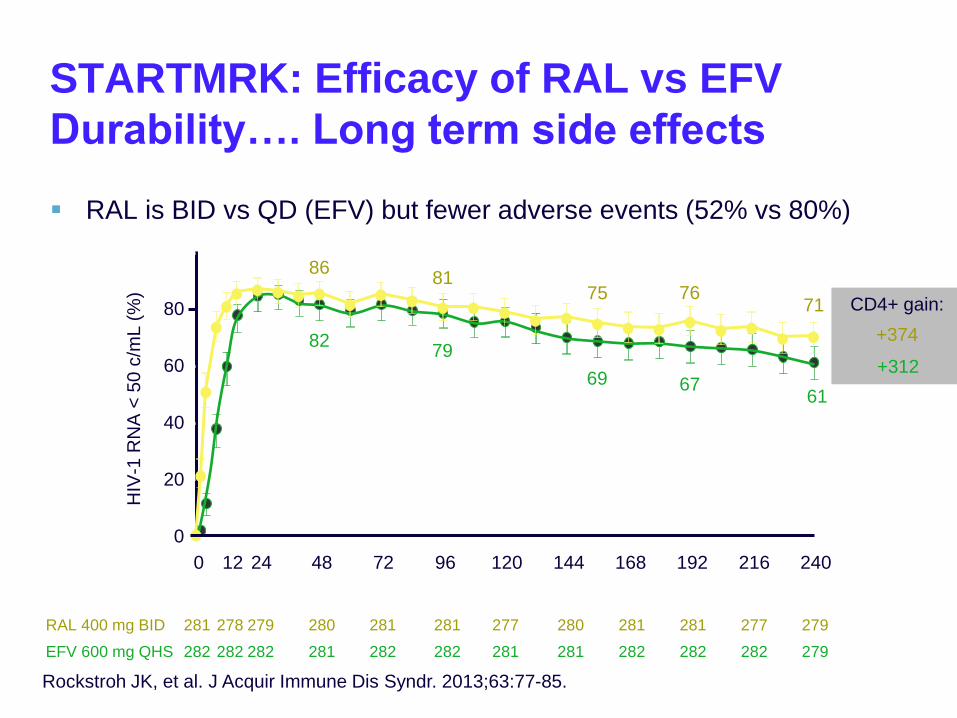
STARTMRK: Efficacy of RAL vs EFV
Durability…. Long term side effects
RAL is BID vs QD (EFV) but fewer adverse events (52% vs 80%)
Rockstroh JK, et al. J Acquir Immune Dis Syndr. 2013;63:77-85.
ITT, NC = F
281 278 279 280 281 281 277 280 281 281 277 279
282 282 282 281 282 282 281 281 282 282 282 279
RAL 400 mg BID
EFV 600 mg QHS
Pts at Risk, n
0 12 24 48 72 96 120 144 168 192 216 240 Wks
0
20
40
60
80
100
HIV
-1 R
NA
< 5
0 c
/mL
(%
)
86
82
81
79
75
69
76
67
71
61
CD4+ gain:
+374
+312
Efavirenz tolerability But do the neuropsychiatric symptoms matter?
In the short-term – For the majority of patients probably not…
In the long-term if neuropsychiatric symptoms persist – Then…?
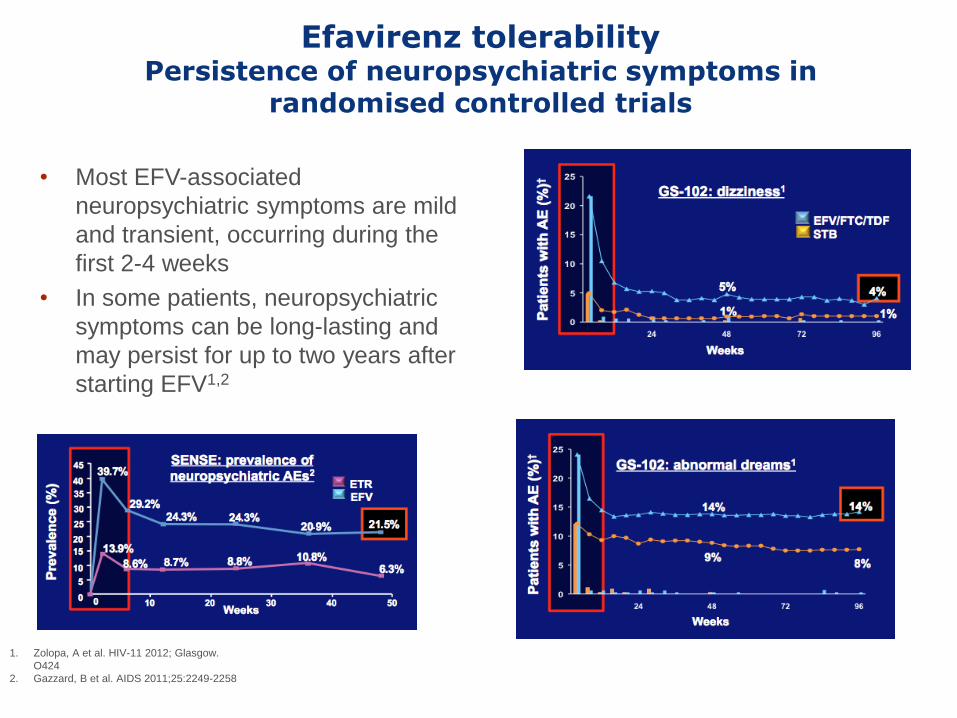
Efavirenz tolerability Persistence of neuropsychiatric symptoms in
randomised controlled trials
1. Zolopa, A et al. HIV-11 2012; Glasgow.
O424
2. Gazzard, B et al. AIDS 2011;25:2249-2258
• Most EFV-associated
neuropsychiatric symptoms are mild
and transient, occurring during the
first 2-4 weeks
• In some patients, neuropsychiatric
symptoms can be long-lasting and
may persist for up to two years after
starting EFV1,2
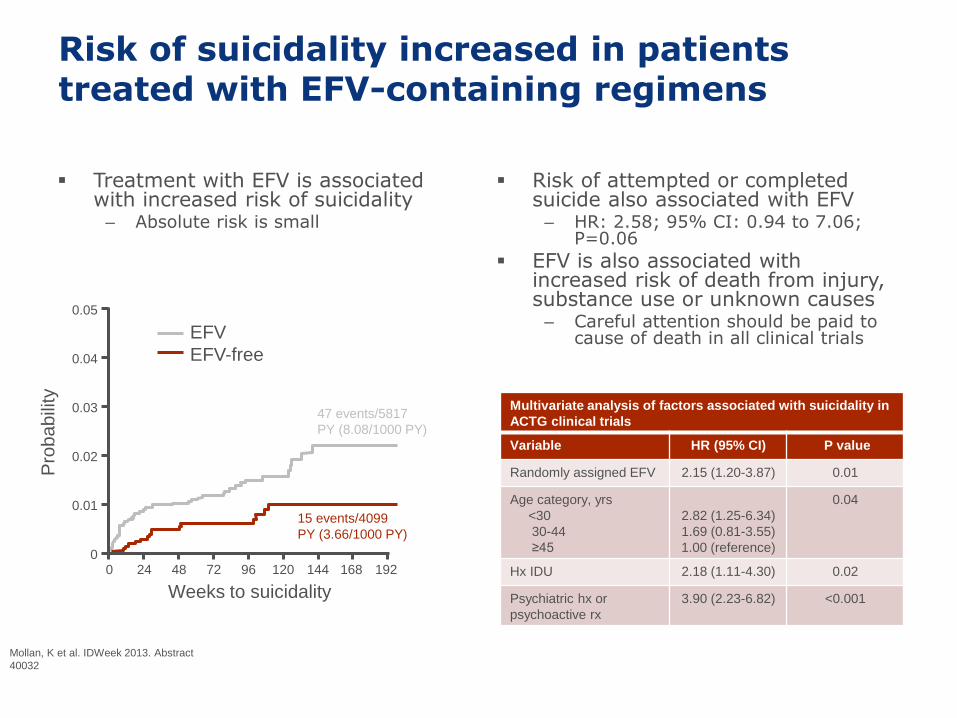
Risk of suicidality increased in patients treated with EFV-containing regimens
Treatment with EFV is associated with increased risk of suicidality – Absolute risk is small
Risk of attempted or completed suicide also associated with EFV – HR: 2.58; 95% CI: 0.94 to 7.06;
P=0.06
EFV is also associated with increased risk of death from injury, substance use or unknown causes – Careful attention should be paid to
cause of death in all clinical trials
HR: 2.28 (95% CI 1.27-4.10; P = .006)
47 events/5817
PY (8.08/1000 PY)
15 events/4099
PY (3.66/1000 PY)
Mollan, K et al. IDWeek 2013. Abstract
40032
EFV
EFV-free
0.05
0.04
0.03
0.02
0.01
0
Pro
babili
ty
192 0 24 48 72 96 120 144 168
Weeks to suicidality
Multivariate analysis of factors associated with suicidality in
ACTG clinical trials
Variable HR (95% CI) P value
Randomly assigned EFV 2.15 (1.20-3.87) 0.01
Age category, yrs
<30
30-44
≥45
2.82 (1.25-6.34)
1.69 (0.81-3.55)
1.00 (reference)
0.04
Hx IDU 2.18 (1.11-4.30) 0.02
Psychiatric hx or
psychoactive rx
3.90 (2.23-6.82) <0.001
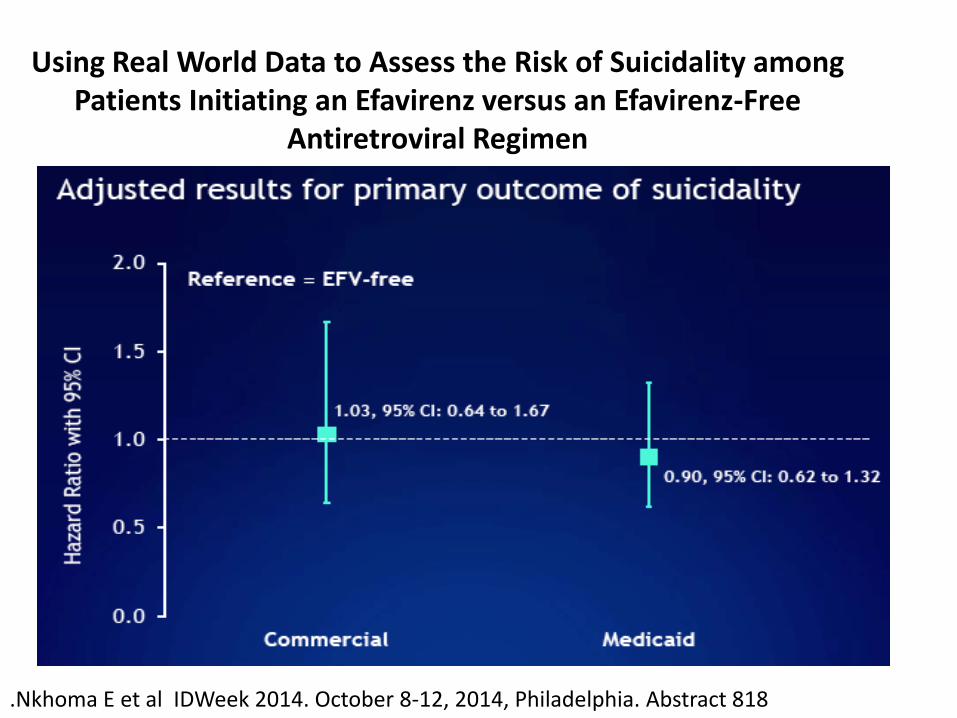
Using Real World Data to Assess the Risk of Suicidality among Patients Initiating an Efavirenz versus an Efavirenz-Free
Antiretroviral Regimen
.Nkhoma E et al IDWeek 2014. October 8-12, 2014, Philadelphia. Abstract 818
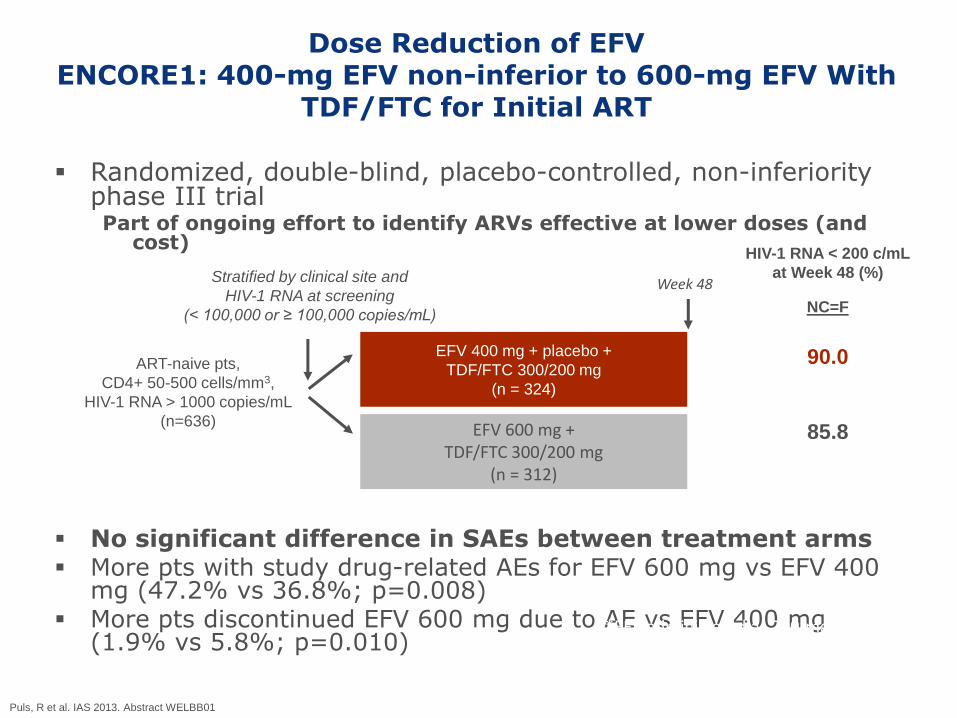
Dose Reduction of EFV ENCORE1: 400-mg EFV non-inferior to 600-mg EFV With
TDF/FTC for Initial ART
Randomized, double-blind, placebo-controlled, non-inferiority phase III trial Part of ongoing effort to identify ARVs effective at lower doses (and
cost)
No significant difference in SAEs between treatment arms More pts with study drug-related AEs for EFV 600 mg vs EFV 400
mg (47.2% vs 36.8%; p=0.008) More pts discontinued EFV 600 mg due to AE vs EFV 400 mg
(1.9% vs 5.8%; p=0.010)
Puls, R et al. IAS 2013. Abstract WELBB01
EFV 400 mg + placebo +
TDF/FTC 300/200 mg
(n = 324)
EFV 600 mg + TDF/FTC 300/200 mg
(n = 312)
ART-naive pts,
CD4+ 50-500 cells/mm3,
HIV-1 RNA > 1000 copies/mL
(n=636)
Week 48 Stratified by clinical site and
HIV-1 RNA at screening
(< 100,000 or ≥ 100,000 copies/mL)
*EFV administered as 200-mg tablets.
HIV-1 RNA < 200 c/mL
at Week 48 (%)
NC=F
90.0
85.8

Starting another NNRTI
STaR Study Multicenter, international, randomized, open-label, Phase 3b, 96-week study
RPV/FTC/TDF
STR
EFV/FTC/TDF
STR
ARV-naive HIV-1 RNA ≥2500 c/mL Sensitivity to EFV, FTC, RPV, TDF (N=786)
Stratified by HIV RNA (≤ or >100,000 c/mL)
n=394
n=392
96 Weeks
Primary endpoint: Efficacy of the 2 STRs by proportion with HIV-1 RNA <50 c/mL at
Week 48 (Snapshot analysis); non-inferiority margin of 12%
Secondary endpoints: Safety and efficacy of the 2 STRs by proportion with
HIV-1 RNA <50 c/mL at Week 96 (Snapshot analysis)
Change in CD4 cell count at Weeks 48 and 96
Genotype/phenotype resistance at time of virologic failure
48 Weeks
Primary Endpoint
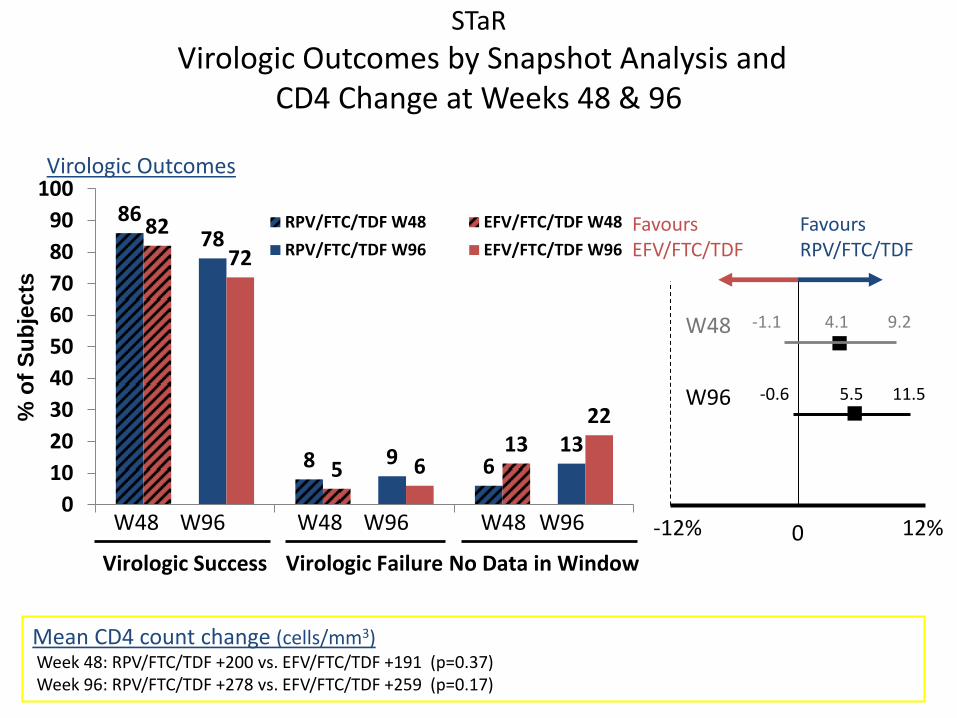
STaR
Virologic Outcomes by Snapshot Analysis and CD4 Change at Weeks 48 & 96
86
8 6
82
5 13
78
9 13
72
6
22
0
10
20
30
40
50
60
70
80
90
100
Virologic Success Virologic Failure No Data in Window
RPV/FTC/TDF W48 EFV/FTC/TDF W48
RPV/FTC/TDF W96 EFV/FTC/TDF W96
4.1 -1.1 9.2
W48 W96 W48 W96 W48 W96
-0.6 5.5 11.5 W96
W48
0 -12% 12%
Mean CD4 count change (cells/mm3) Week 48: RPV/FTC/TDF +200 vs. EFV/FTC/TDF +191 (p=0.37) Week 96: RPV/FTC/TDF +278 vs. EFV/FTC/TDF +259 (p=0.17)
Favours EFV/FTC/TDF
Favours RPV/FTC/TDF
Virologic Outcomes
% o
f S
ub
jec
ts
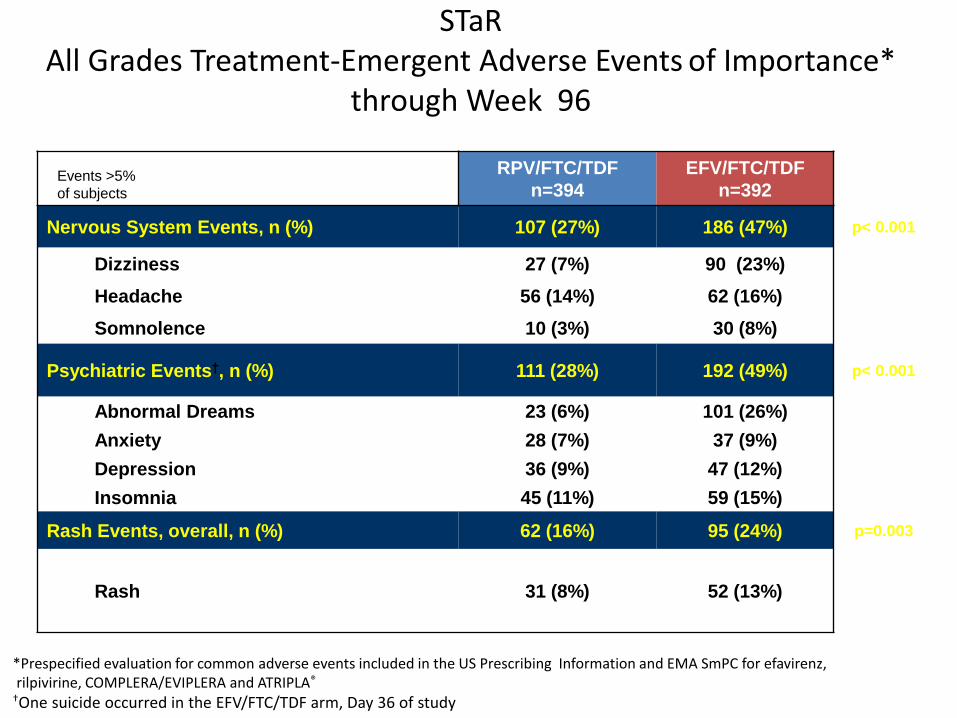
STaR All Grades Treatment-Emergent Adverse Events of Importance*
through Week 96
*Prespecified evaluation for common adverse events included in the US Prescribing Information and EMA SmPC for efavirenz, rilpivirine, COMPLERA/EVIPLERA and ATRIPLA®
†One suicide occurred in the EFV/FTC/TDF arm, Day 36 of study
RPV/FTC/TDF
n=394
EFV/FTC/TDF
n=392
Nervous System Events, n (%) 107 (27%) 186 (47%) p< 0.001
Dizziness 27 (7%) 90 (23%)
Headache 56 (14%) 62 (16%)
Somnolence 10 (3%) 30 (8%)
Psychiatric Events†, n (%) 111 (28%) 192 (49%) p< 0.001
Abnormal Dreams 23 (6%) 101 (26%)
Anxiety 28 (7%) 37 (9%)
Depression 36 (9%) 47 (12%)
Insomnia 45 (11%) 59 (15%)
Rash Events, overall, n (%) 62 (16%) 95 (24%) p=0.003
Rash 31 (8%) 52 (13%)
Events >5%
of subjects
Role for PI/r as first line therapy
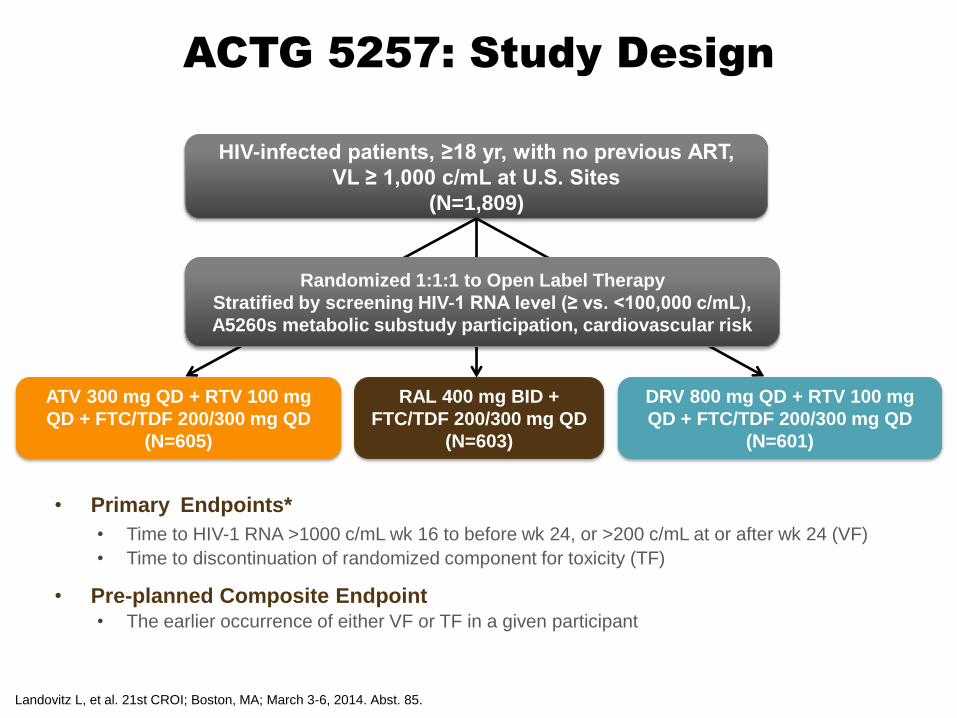
ACTG 5257: Study Design
• Primary Endpoints*
• Time to HIV-1 RNA >1000 c/mL wk 16 to before wk 24, or >200 c/mL at or after wk 24 (VF)
• Time to discontinuation of randomized component for toxicity (TF)
• Pre-planned Composite Endpoint • The earlier occurrence of either VF or TF in a given participant
Landovitz L, et al. 21st CROI; Boston, MA; March 3-6, 2014. Abst. 85.
HIV-infected patients, ≥18 yr, with no previous ART,
VL ≥ 1,000 c/mL at U.S. Sites
(N=1,809)
ATV 300 mg QD + RTV 100 mg
QD + FTC/TDF 200/300 mg QD
(N=605)
RAL 400 mg BID +
FTC/TDF 200/300 mg QD
(N=603)
DRV 800 mg QD + RTV 100 mg
QD + FTC/TDF 200/300 mg QD
(N=601)
Randomized 1:1:1 to Open Label Therapy
Stratified by screening HIV-1 RNA level (≥ vs. <100,000 c/mL),
A5260s metabolic substudy participation, cardiovascular risk
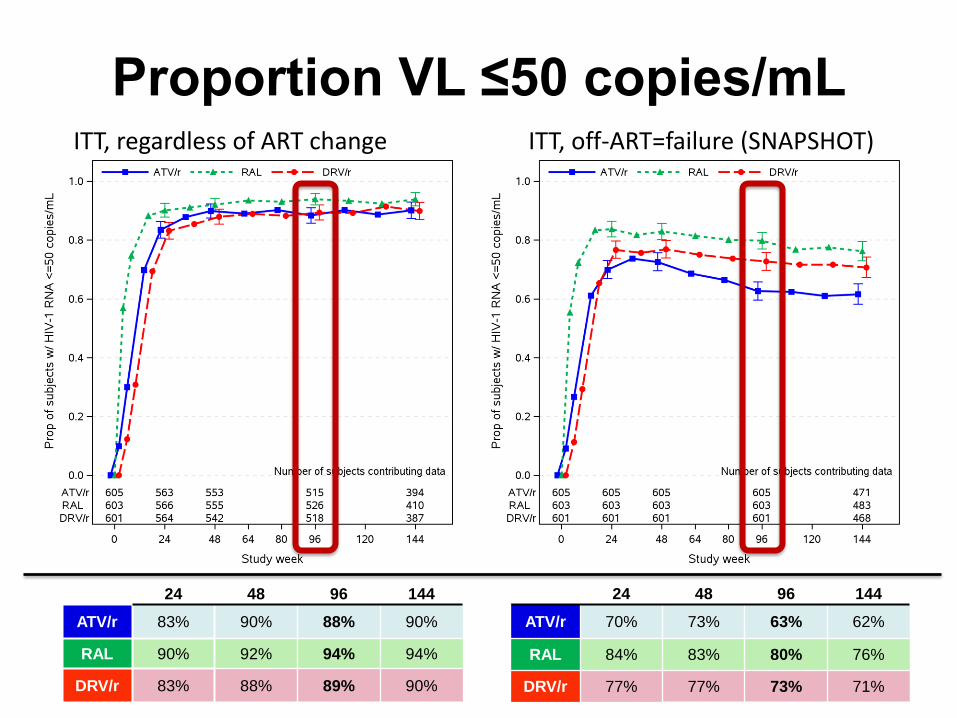
Proportion VL ≤50 copies/mL ITT, regardless of ART change ITT, off-ART=failure (SNAPSHOT)
24 48 96 144
ATV/r 83% 90% 88% 90%
RAL 90% 92% 94% 94%
DRV/r 83% 88% 89% 90%
24 48 96 144
ATV/r 70% 73% 63% 62%
RAL 84% 83% 80% 76%
DRV/r 77% 77% 73% 71%
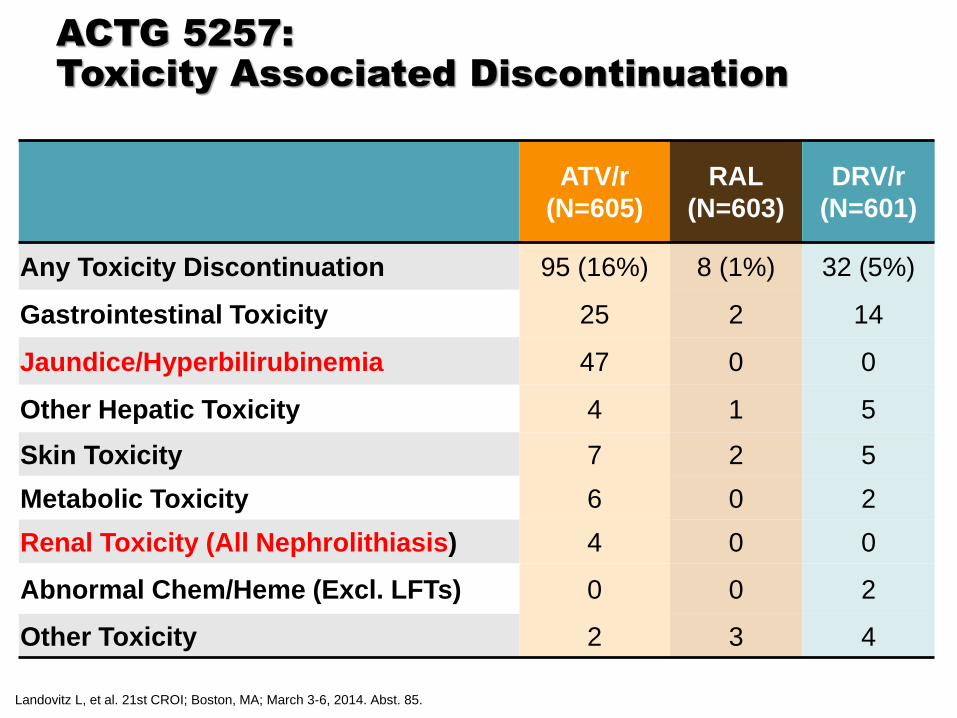
ACTG 5257:
Toxicity Associated Discontinuation
ATV/r
(N=605)
RAL
(N=603)
DRV/r
(N=601)
Any Toxicity Discontinuation 95 (16%) 8 (1%) 32 (5%)
Gastrointestinal Toxicity 25 2 14
Jaundice/Hyperbilirubinemia 47 0 0
Other Hepatic Toxicity 4 1 5
Skin Toxicity 7 2 5
Metabolic Toxicity 6 0 2
Renal Toxicity (All Nephrolithiasis) 4 0 0
Abnormal Chem/Heme (Excl. LFTs) 0 0 2
Other Toxicity 2 3 4
Landovitz L, et al. 21st CROI; Boston, MA; March 3-6, 2014. Abst. 85.

0 TDF+FTC
1 RAL
0 RAL+FTC
0 RAL+FTC+TDF
1 TDF+FTC
1 RAL
0 RAL+FTC
0 RAL+FTC+TDF
Resistance to Study Agents None to boosted PIs
75/94 VF
Available
RAL
99/115 VF
Available
9 Any Resistance
(1.5%)
18 Any Resistance
(3%)
4 Any Resistance
(<1%)
2 TDF 0 TDF 0 TDF
5 FTC 7 FTC 3 FTC
0 TDF+FTC
ATV/r DRV/r
295 Virologic Failures 1 Baseline Missing
56 VF Failed to Amplify
1809 Participants
1 RAL
7 RAL+FTC
3 RAL+FTC+TDF
65/85 VF
Available
Which Patient for Boosted PIs?
Considerations in Favor
• Effective across HIV-1 RNA, CD4+ strata[1,2]
• Few CNS adverse events[1,2]
• Little/no emergence of resistance at VF[1,2]
• Preferred agents in pregnancy3
• Low risk for new resistance to develop in those with transmitted resistance or those with poor adherence
Considerations Against
• No coformulations with NRTIs (yet)
• Variable lipid effects[1,2]
• Concerns about renal function (greatest concern when ATV/RTV combined with TDF)[1,4]
• Drug–drug interactions with other drugs metabolized by CYP system[5,6]
• Hyperbilirubinemia with ATV[1,5]
1. Molina JM, et al. Lancet. 2008;372:646-655. 2. Ortiz R, et al. AIDS. 2008;22:1389-1397. 3. DHHS Perinatal Guidelines. July 2012. 4. Mocroft A, et al. AIDS. 2010;24:1667-1678. 5. Atazanavir [package insert]. 6. Darunavir [package insert].
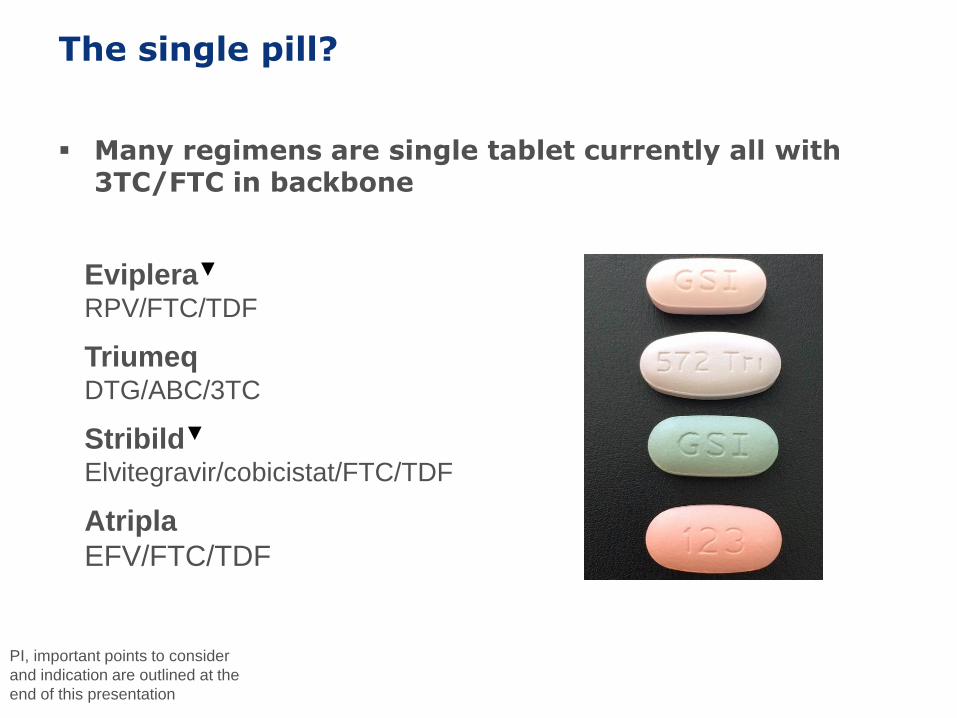
The single pill?
Many regimens are single tablet currently all with 3TC/FTC in backbone
PI, important points to consider
and indication are outlined at the
end of this presentation
Atripla
EFV/FTC/TDF
Eviplera▼ RPV/FTC/TDF
Stribild▼
Elvitegravir/cobicistat/FTC/TDF
Triumeq DTG/ABC/3TC

29
More STRs on the Way!
30
31
FDCs/STRs-issues not for everyone
Cannot adjust the doses – Important in renal disease and with DDIs
Some may be too big to make
Co-packaging vs single pill
Does differing half lives matter if you stop?
All have FTC/3TC at present
STR cross resistance – 184V is a multidrug resistant mutation to all current and proposed
STR!
Where is the data re significant difference
Patented so more expensive

What about
Switches Due to Toxicity
27%
14%
12%12%
9%
8%
18% CNSSE
GI
CVDRisk
Hepatotoxicity
Metabolic
RenalToxicity
Other
Boyle A et al, HIV11 2012, Oral 312.
•923 regimens switched over 18 months affecting 12% (n=722/6211) •Predicted annual switch rate of 8%
•Half switches for toxicity

Many switch options if undetectable
• Need a reason to switch!
• Must check treatment history and prior resistance tests
Recent trials
• PI/r to rilpivirine plus TDF/ FTC
• PI/r to Stribild
• NNRTI to Stribild

SECOND-LINE TREATMENT SWITCH FOR VIROLOGICAL
FAILURE
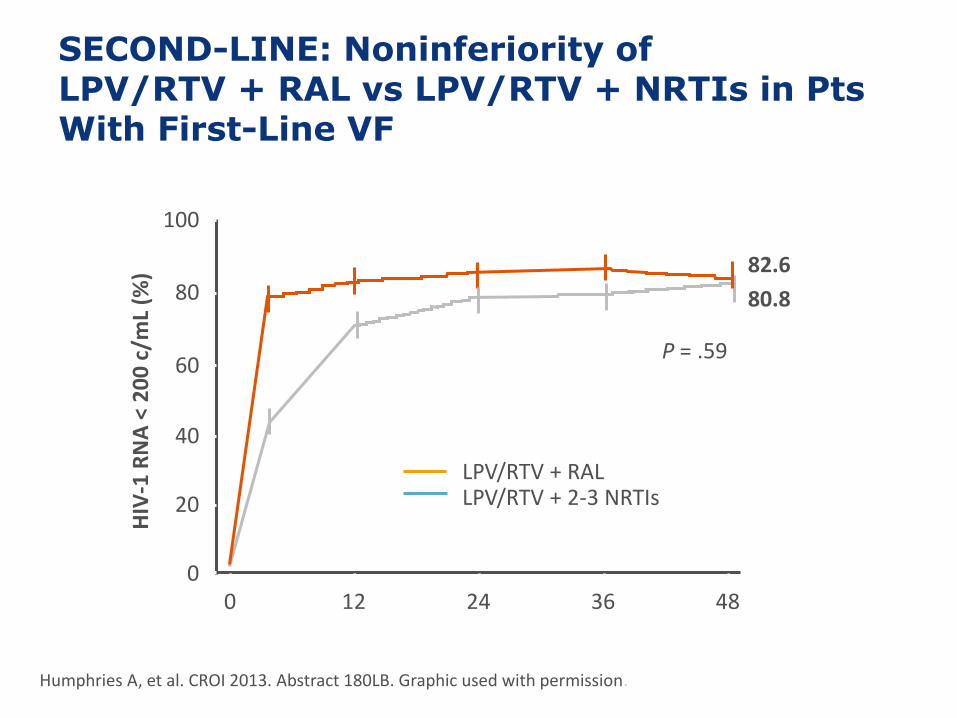
SECOND-LINE: Noninferiority of LPV/RTV + RAL vs LPV/RTV + NRTIs in Pts With First-Line VF
0
20
40
80
100
Wk
LPV/RTV + RAL LPV/RTV + 2-3 NRTIs
60
0 12 24 36 48
HIV
-1 R
NA
< 2
00
c/m
L (%
) 82.6
80.8
P = .59
Humphries A, et al. CROI 2013. Abstract 180LB. Graphic used with permission.
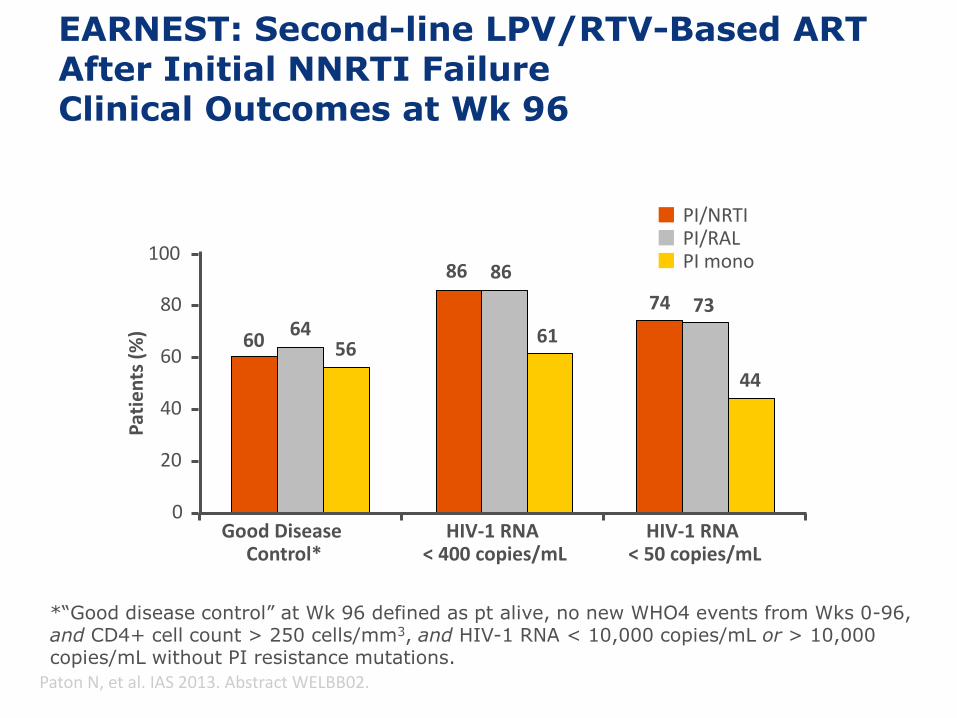
EARNEST: Second-line LPV/RTV-Based ART After Initial NNRTI Failure Clinical Outcomes at Wk 96
*“Good disease control” at Wk 96 defined as pt alive, no new WHO4 events from Wks 0-96, and CD4+ cell count > 250 cells/mm3, and HIV-1 RNA < 10,000 copies/mL or > 10,000 copies/mL without PI resistance mutations.
Paton N, et al. IAS 2013. Abstract WELBB02.
100
80
60
40
20
0 Good Disease
Control* HIV-1 RNA
< 400 copies/mL HIV-1 RNA
< 50 copies/mL
60 64
56
86 86
61
74 73
44
PI/NRTI PI/RAL PI mono
Pat
ien
ts (
%)
Conclusion
Modern HAART is highly effective but.....
Need to maintain lifelong well tolerated therapy
is Efavirenz going to remain first line treatment of choice
What will be the role of PI/r and integrase?
STRs are becoming a standard of care in Naives
Switching because of toxicity is common
Second Line therapy –can you move to a second regimen without resistance testing
38
Recommended

















