Graves’ and Thyroid Disease: The Journey
CHASE LAY MD
ENT – OCULOPLASTICS – SKULL BASE
Cupertino, CA

Grave’s Disease
Surgical Considerations

The Thyroid & Grave’s
Thyroid hormone is critical for regulating mood, weight, and mental and physical energy levels.
If the body makes too much thyroid hormone, the condition is called hyperthyroidism. (An underactive thyroid leads to hypothyroidism.)
Graves disease is the most common cause of hyperthyroidism.
Caused by an abnormal immune system response that causes the thyroid gland to produce too much thyroid hormones.
Body actually produces antibodies that activate thyroid hormone production

Grave’s Eye Disease - Inflammation
Signs & Symptoms
Anxiety
Breast enlargement in men (possible)
Double vision
Eyeballs that stick out (exophthalmos)
Eye irritation and tearing
Frequent bowel movements
Heat intolerance
Increased appetite
Menstrual irregularities in women
Muscle weakness
Nervousness
Rapid or irregular heartbeat (palpitations or arrhythmia)
Restlessness and difficulty sleeping
Tremor
Weight loss (rarely, weight gain)

Testing for Graves Simple blood test
TSH, T3, T4
TSH receptor antibody; Thyroid stimulating immunoglobulin or “TSI”
Ultrasound of the neck if thyroid is enlarged or mass felt

Surgical Grave’s Disease Hyperthyroidism or progressing eye disease in patients
who can’t be treated with radioactive iodine therapy
Rapidly worsening Thyroid Eye Disease
Enlarged thyroid or Goiter causing difficulty breathing or swallowing
Women interested in becoming pregnant
Nodule in a patient with Grave’s or a family history of thyroid cancer
Suspicious thyroid nodules Change of malignancy in thyroid nodules is
double in context of Graves

Thyroid nodules are common Can be found in 5% of the
general population
Mostly benign
Can be observed if there are no risk factors
www.mythyroid.com

Detecting Thyroid Nodules
Physical Exam
Ultrasound
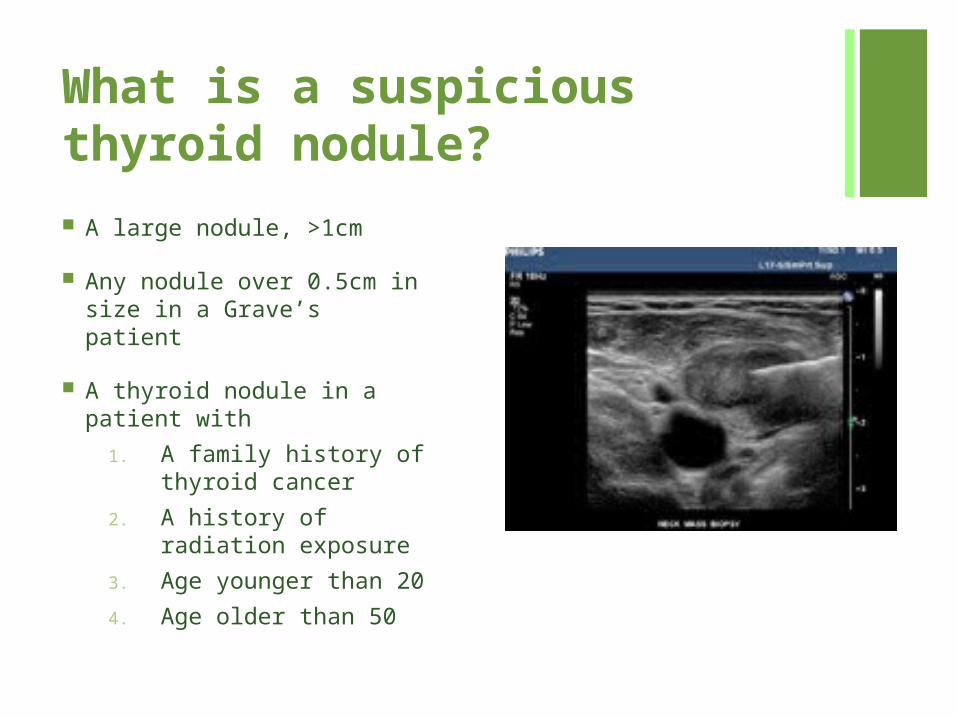
What is a suspicious thyroid nodule?
A large nodule, >1cm
Any nodule over 0.5cm in size in a Grave’s patient
A thyroid nodule in a patient with
1. A family history of thyroid cancer
2. A history of radiation exposure
3. Age younger than 20
4. Age older than 50

Surgery & Risks General anesthesia
Small incision in the lower neck
Hoarse voice
Vocal cord weakness
Visible incision
Bleeding
Low Calcium (Total thyroidectomy)

After Surgery Small incision – Quick healing
Typically stay in the hospital overnight
Back to work in a 2 to 6 days. Complications with nerve
weakness, post-operative bleeding, or calcium regulation may delay return to work.

Surgical Treatment of Eye Disease

Marty Feldman

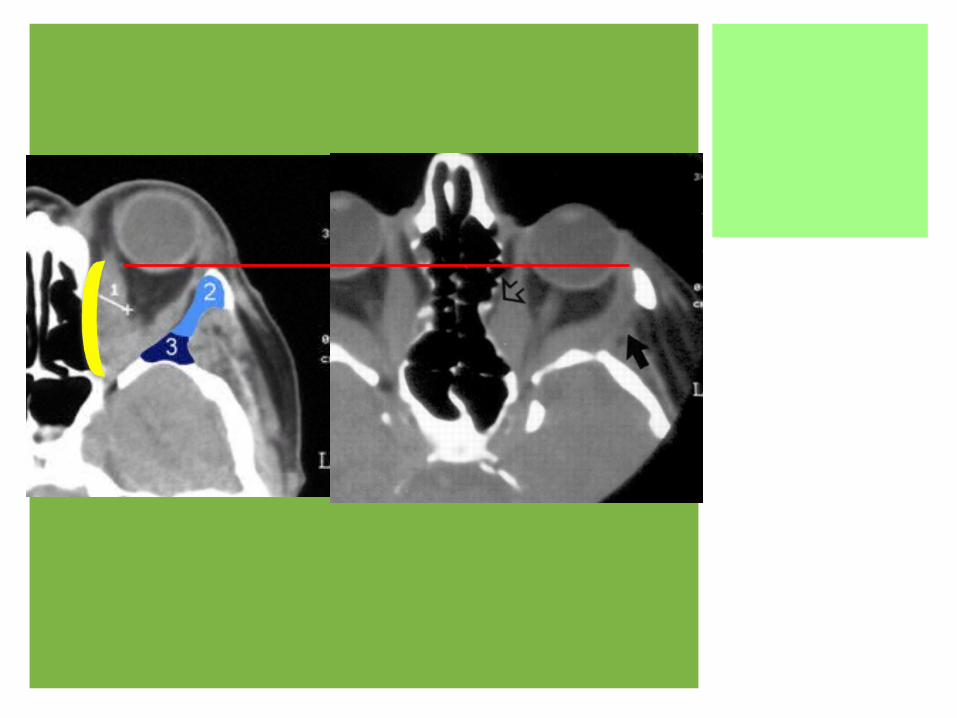
Grave’s Eye Disease - Inflammation

Combination of compression of the optic nerve and inflammation of the nerve

Orbital Decompression &Fat Removal Performed both endoscopically and
externally
Surgical treatment to save or restore vision
Should be thought of as a medical necessity
Additional corrective surgeries are often required
Typically outpatient procedures



Endoscopic Decompression
Extended or Advanced Sinus Surgery




External Decompression



Risks of Decompression Surgeries
CSF leak during endoscopic surgery
Diplopia or Double Vision (often pre-existing)
Bleeding
Infection
Eyelid retraction or drooping

Droopy eyelid repaired


Thank you for your time
Recommended