Hunt for Ambulatory Metrics in the Pediatric Neurosciences
Gerald Grant, MDAssociate Professor
Department of NeurosurgeryStanford University
Neurosafe 2017

Brain & Behavior QAPI (Quality Assurance/Performance Improvement)
2
Ensure an effective, ongoing data-driven quality assessment and performance improvement program as recommended by the Centers for Medicare and Medicaid (CMS). The QAPI will monitor and evaluate clinical outcomes and facilitate improvements of identified systems issues that impact quality, safety and effectiveness.
The team will provide a multidisciplinary approach for improving outcomes and processes within the Institute of Medicine’s six domains of quality (safe, effective, efficient, timely, patient and family-centered, and equitable), guided by the Packard Quality Management System (PQMS).
Develop and monitor process and outcome measuresDevelop improvement initiatives based on outcome/process measures, opportunities surfaced in the daily management system, and goals deployed through the hospital.Report results and lessons learned from initiatives on a regular basis
Vice President, Procedures and DiagnosticsTransplant, Brain & Behavior, Surgical Sub-specialtiesVice President Medical AffairsVice President Patient Care Services & CNO
Neuroscience QAPI Chairs:Med Director Stroke ProgramMedical Director Neuro-critical careCNS Neurosciences
Core Team, including Chairs
Division Chief of Pediatric NeurosurgeryDivision Chief of Child NeurologyNeuro RadiologyClinical Nurse Specialist- Pediatric Intensive Care UnitSurgical TechnicianOR Nurse LeadNeurologistNP Neurosurgery Peer Review MD LeaderMedical Director(s)Patient Safety Representative Professional Practice Evaluation Program ManagerFamily Advisor
Purpose Scope
Responsibilities
Members
Sponsorship

Guideline to Identify and Track Actionable Metrics
➢ Discuss CY 2016 dashboard metrics value add towards Quality, Safety, Affordability or Innovation
➢ Review metrics from other pediatric transplant centers
➢ Identify measurable/meaningful metrics for CY 2017 (US News and world Report)
➢ Incorporate evidence based benchmarks for the selected metrics
➢ Identify metric owners for continuous improvement
➢ Transplant quality team will send out under performing metrics data to the metric owners 2 weeks prior to the quality council meeting
➢ Metric owner to present interventions for underperforming metrics
➢ Track the implemented intervention for sustainability

Regulatory Update- Successful CMS Transplant Survey
• Opportunities for improvement for the quality committee:
✓Collaboration with Patient Experience Department to receive real time feedback on transplant patients.
✓Identify measurable interventions for improvement and timely implementation of the measures.
✓Monitor sustainability of the identified interventions.
✓Utilize separate template for reviewable events.

PICU Model of Care
Transition to Specialty Care Teams

Specialty Care Team Goals
1. Increase depth of knowledge for specialized care
2. Improve competencies and quality of care
3.Elevate and maintain consistency in quality
4.Strengthen collaborative environment for program development
Sub-specialty or service-line defined goals and objectives
Annual education & training
Participation in QAPI, PIPS, PPEC and other programmatic meetings
Dissemination of care improvements and education to general PICU
Specialty Care Teams
Specialty Care Team Members
PCCM faculty liaison or program director
PICU nurse practitioner
RN core team – 10-15 PICU nurses per team
PICU leadership representative
Specialty Care Teams
• ECMO• ENT/Complex Airway• Neurocritical Care• Pulmonary Chronic Care• Pulmonary Hypertension
• Renal Replacement Therapy• Solid Organ Transplant• Stem Cell Transplant • Trauma

Patient Levels of Care
PICU IMCU Acute Care
Staffing 1:1 or 1:2 1:3 1:4
Frequency of intervention
q1 to q2 q2 to q4 q4 to q8
Level of complexity
Continuous mechanical support (ventilators, CRRT, ECMO)
Mature tracheostomies, stable NIPPV, HD/mechanical PD
Continuous invasive monitoring
Non-invasive intermittent monitoring
Multi-organdysfunction
Single-organdysfunction
Critical devices No critical devices





Leadership Initiative: Quality and Safety in Pediatric Neurosurgery
EpilepsyBrain TumorsConcussionChiari I

Leadership Initiative: Quality and Safety in Pediatric Neurosurgery
EpilepsyBrain TumorsConcussionCraniosynostosisHydrocephalusChiari I

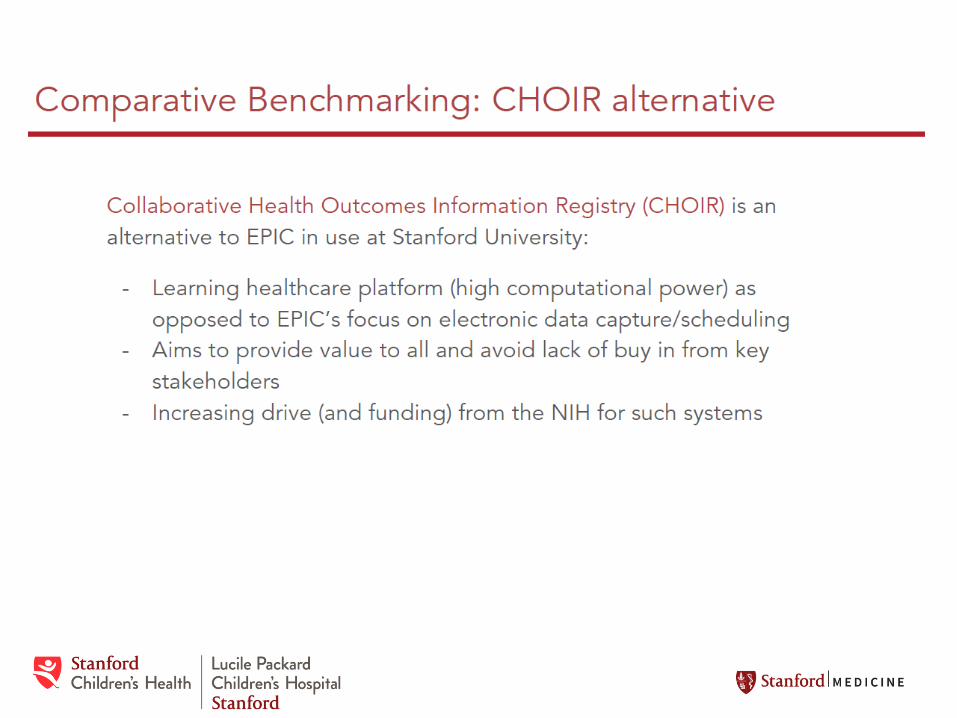
Chiari I MalformationWho Needs Surgery?
Cerebellar Tonsil Position
Smith et al, JNS Peds, 2013

Mission : To provide the highest quality of neurosurgical care to the children we treat
1) We will develop, validate, and incorporate disease-specific patient based instruments in the ambulatory setting.
1) These instruments will be disease specific.
1) Seamless integration of quality metrics into our daily workflow.
1) Improve patient care and outcomes.
1) Lead to a national collaborative multi-institutional effort focusing on quality outcome metrics in pediatric neurosurgery
1) Collaboration between Neurosurgery, Stanford Healthcare, Stanford Children’s Health, Center for Health Policy, and Center for Quality and Clinical Effectiveness
Challenges
New territory. First of its kind
Database: Redcap vs. pCHOIR
Chiari I natural history is not defined
Operationalize this concert
Getting buy in from patients and staff!
Education
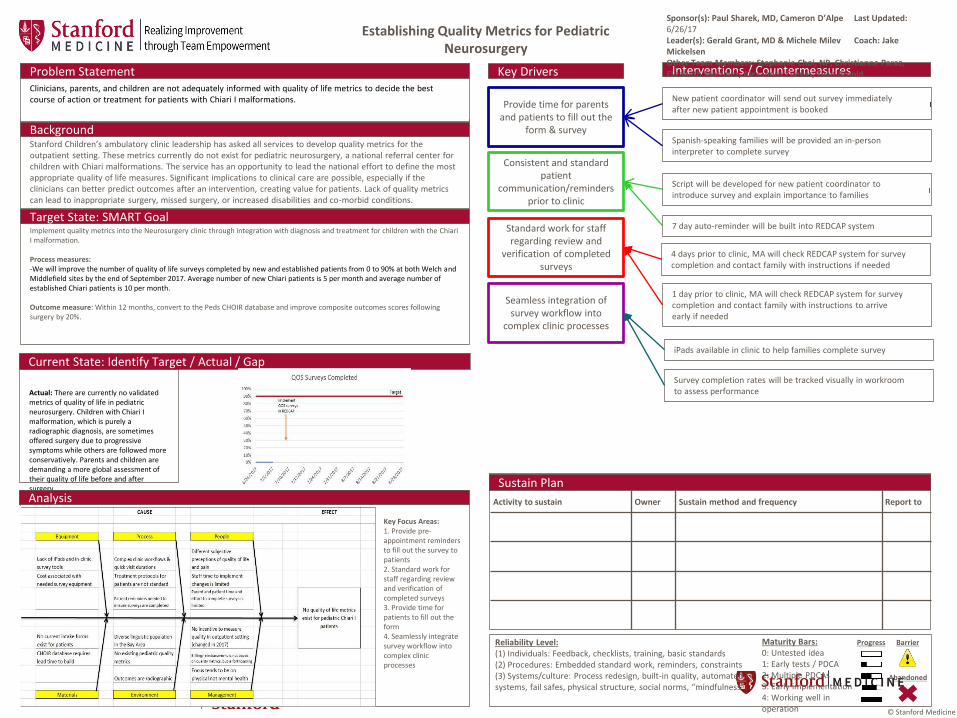
Stanford Children’s ambulatory clinic leadership has asked all services to develop quality metrics for the outpatient setting. These metrics currently do not exist for pediatric neurosurgery, a national referral center for children with Chiari malformations. The service has an opportunity to lead the national effort to define the most appropriate quality of life measures. Significant implications to clinical care are possible, especially if the clinicians can better predict outcomes after an intervention, creating value for patients. Lack of quality metrics can lead to inappropriate surgery, missed surgery, or increased disabilities and co-morbid conditions.
Background
Implement quality metrics into the Neurosurgery clinic through integration with diagnosis and treatment for children with the Chiari I malformation.
Process measures:-We will improve the number of quality of life surveys completed by new and established patients from 0 to 90% at both Welch andMiddlefield sites by the end of September 2017. Average number of new Chiari patients is 5 per month and average number of established Chiari patients is 10 per month.
Outcome measure: Within 12 months, convert to the Peds CHOIR database and improve composite outcomes scores following surgery by 20%.
Target State: SMART Goal
Actual: There are currently no validated metrics of quality of life in pediatric neurosurgery. Children with Chiari I malformation, which is purely a radiographic diagnosis, are sometimes offered surgery due to progressive symptoms while others are followed more conservatively. Parents and children are demanding a more global assessment of their quality of life before and after surgery.
Current State: Identify Target / Actual / Gap
Analysis
Key Drivers
Provide time for parents and patients to fill out the
form & survey
Consistent and standard patient
communication/reminders prior to clinic
Standard work for staff regarding review and
verification of completed surveys
Seamless integration of survey workflow into
complex clinic processes
New patient coordinator will send out survey immediately after new patient appointment is booked
Spanish-speaking families will be provided an in-person interpreter to complete survey
Script will be developed for new patient coordinator to introduce survey and explain importance to families
Sustain Plan
Clinicians, parents, and children are not adequately informed with quality of life metrics to decide the best course of action or treatment for patients with Chiari I malformations.
Problem Statement
Establishing Quality Metrics for Pediatric Neurosurgery
Interventions / Countermeasures
Activity to sustain Owner Sustain method and frequency Report to
Maturity Bars:0: Untested idea1: Early tests / PDCA2: Multiple PDCAs3: Early implementation4: Working well in operation
Reliability Level:(1) Individuals: Feedback, checklists, training, basic standards(2) Procedures: Embedded standard work, reminders, constraints(3) Systems/culture: Process redesign, built-in quality, automated systems, fail safes, physical structure, social norms, “mindfulness”
Progress
Abandoned
Barrier
Sponsor(s): Paul Sharek, MD, Cameron D’Alpe Last Updated: 6/26/17Leader(s): Gerald Grant, MD & Michele Milev Coach: Jake MickelsenOther Team Members: Stephanie Choi, NP, Christianne Paraz, Elizabeth Martinez, Alexandra Cuevas, Evan Arnold
© Stanford Medicine
Key Focus Areas:1. Provide pre-appointment reminders to fill out the survey to patients 2. Standard work for staff regarding review and verification of completed surveys3. Provide time for patients to fill out the form4. Seamlessly integrate survey workflow into complex clinic processes
4 days prior to clinic, MA will check REDCAP system for survey completion and contact family with instructions if needed
1 day prior to clinic, MA will check REDCAP system for survey completion and contact family with instructions to arrive early if needed
iPads available in clinic to help families complete survey
Survey completion rates will be tracked visually in workroom to assess performance
7 day auto-reminder will be built into REDCAP system

Chiari Intake Form

Survey Process Map

Performance improvement in a complex health careenvironment depends on the cooperation of diverseindividuals and groups, allocation of time and resources,and use of effective improvement methods.








Challenges
New territory. First of its kind
Database: Redcap vs. pCHOIR
Chari I natural history is not defined
Operationalize this concept with seamless integration into workflow
Getting buy in from patients and staff!
Education

Recommended