GallstonesGallstones
Mrs. Kirsty Cattle MRCSMrs. Kirsty Cattle MRCS
SHOSHO

GeneralGeneral Ian Aird said “Good pathology makes Ian Aird said “Good pathology makes
mighty surgeons proud.”mighty surgeons proud.” Incidence – common (17% at time of death)Incidence – common (17% at time of death) Age – any age, mostly 40sAge – any age, mostly 40s Aetiology – bile constituents, infective, bile Aetiology – bile constituents, infective, bile
stasisstasis Sex ratio – female>maleSex ratio – female>male Geography – Western dietGeography – Western diet Predisposing factors – “fat, fair, fertile, Predisposing factors – “fat, fair, fertile,
flatulant, forties” flatulant, forties” Macroscopy – cholesterol, mixed (90%), pigmentMacroscopy – cholesterol, mixed (90%), pigment Microscopy – histology of gallbladder wallMicroscopy – histology of gallbladder wall SpreadSpread PrognosisPrognosis

AnatomyAnatomy

PresentationPresentation
Asymptomatic (85-90%)Asymptomatic (85-90%) Biliary colicBiliary colic CholecystitisCholecystitis Obstructive jaundiceObstructive jaundice Ascending cholangitisAscending cholangitis PancreatitisPancreatitis Rarities:Rarities:
Gallstone ileus, Mucocoele, Perforation, Gallstone ileus, Mucocoele, Perforation, Mirizzi’s syndrome, CarcinomaMirizzi’s syndrome, Carcinoma

Biliary colicBiliary colic
Definition: colicky abdominal pain Definition: colicky abdominal pain due to the presence of gallstones in due to the presence of gallstones in gall bladdergall bladder
InvestigationsInvestigations Normal blood resultsNormal blood results USS: gallstones within thin-walled gall USS: gallstones within thin-walled gall
bladder, no CBD dilatationbladder, no CBD dilatation ManagementManagement
SymptomaticSymptomatic CholecystectomyCholecystectomy

CholecystitisCholecystitis
Definition: constant abdominal pain Definition: constant abdominal pain and tenderness due to an infected and tenderness due to an infected gall bladdergall bladder
InvestigationsInvestigations Raised WBC, Normal LFTsRaised WBC, Normal LFTs USS: gallstones within thick-walled gall USS: gallstones within thick-walled gall
bladder, no CBD dilatationbladder, no CBD dilatation ManagementManagement
SymptomaticSymptomatic CholecystectomyCholecystectomy

JaundiceJaundice
Definition: obstructive jaundice due Definition: obstructive jaundice due to CBD stoneto CBD stone
InvestigationsInvestigations Raised LFTs: Alk Phos > ALT, Raised LFTs: Alk Phos > ALT, USS: gallstones, CBD dilatation USS: gallstones, CBD dilatation ± ± CBD CBD
stonestone ManagementManagement
ERCPERCP CholecystectomyCholecystectomy

Ascending cholangitisAscending cholangitis
Surgical emergencySurgical emergency Definition: jaundice, rigors, RUQ tendernessDefinition: jaundice, rigors, RUQ tenderness InvestigationsInvestigations
Raised WBC, raised LFTsRaised WBC, raised LFTs USS: gallstones, CBD dilatation USS: gallstones, CBD dilatation ± ± CBD stoneCBD stone
ManagementManagement Urgent resuscitation, iv Antibiotics (e.g. Urgent resuscitation, iv Antibiotics (e.g.
Ciprofloxacin)Ciprofloxacin) Urgent ERCPUrgent ERCP CholecystectomyCholecystectomy

Acute PancreatitisAcute Pancreatitis
DefinitionDefinition acute inflammation of the pancreas, acute inflammation of the pancreas,
primarily due to intracellular activation primarily due to intracellular activation of trypsinogen to trypsin.of trypsinogen to trypsin.
PresentationPresentation Epigastric pain, radiating to back, nausea Epigastric pain, radiating to back, nausea
± ± vomiting, dehydration, renal failurevomiting, dehydration, renal failure InvestigationsInvestigations
Amylase >3x normal rangeAmylase >3x normal range Scoring of severityScoring of severity

Causes of Acute Causes of Acute PancreatitisPancreatitis
Obstruction:Obstruction: Gallstones (30-70%)Gallstones (30-70%) Ampullary or pancreatic Ampullary or pancreatic
tumours (3%)tumours (3%) Congenital abnormalities Congenital abnormalities
(5%)(5%) Sphincter of Oddi Sphincter of Oddi
hypertension (1-2%)hypertension (1-2%) AscariasisAscariasis
Drugs/Toxins:Drugs/Toxins: Alcohol (30-70%)Alcohol (30-70%) Azathioprine, 6-Azathioprine, 6-
mercaptopurine, some mercaptopurine, some antibiotics antibiotics (metronidazole, (metronidazole, tetracycline), Htetracycline), H22 blockers, othersblockers, others
Iatrogenic/Trauma:Iatrogenic/Trauma: ERCPERCP Cardiopulmonary bypassCardiopulmonary bypass Blunt abdominal traumaBlunt abdominal trauma
Metabolic:Metabolic: Hypertriglyceridaemia Hypertriglyceridaemia
(2%)(2%) Hypercalcaemia, Hypercalcaemia,
hyperparathyroidism hyperparathyroidism (rare)(rare)
Infection:Infection: AIDS, secondary AIDS, secondary
infectioninfection Mumps, Coxsackie virus, Mumps, Coxsackie virus,
hepatitis A, B and Chepatitis A, B and C Idiopathic (10%)Idiopathic (10%)

Modified Glasgow ScoreModified Glasgow Score
Indication of severity of pancreatitisIndication of severity of pancreatitis Factors:Factors:
Age > 55Age > 55 PaO2 < 8.0 kPaPaO2 < 8.0 kPa WBC > 15WBC > 15 Calcium < 2 mmol/lCalcium < 2 mmol/l Glucose > 10Glucose > 10 Albumin < 32Albumin < 32 Urea > 16Urea > 16 LDH > 600LDH > 600
A score of 3 or more indicates severe A score of 3 or more indicates severe pancreatitis and requires anaesthetic input pancreatitis and requires anaesthetic input regarding HDU careregarding HDU care
Compete score on admission and 48 hours Compete score on admission and 48 hours laterlater

ManagementManagement Supportive – analgesia, iv rehydration, Supportive – analgesia, iv rehydration,
catheterise, fluid balance, NBM (catheterise, fluid balance, NBM (± NG ± NG tube). Consider Antibiotics.tube). Consider Antibiotics.
Observe for complications:Observe for complications: Systemic: cardiovascular, pulmonary, renal, Systemic: cardiovascular, pulmonary, renal,
haematological, metabolic, neurological, haematological, metabolic, neurological, gastrointestinalgastrointestinal
Local: fluid collections, pseudocyst, necrosis, Local: fluid collections, pseudocyst, necrosis, ascites, infection, pseudoaneurysmascites, infection, pseudoaneurysm
Establish and remove cause:Establish and remove cause: ERCP, CholecystectomyERCP, Cholecystectomy Strongly advise patient to stop drinking alcoholStrongly advise patient to stop drinking alcohol

RaritiesRarities
Gallstone ileus:Gallstone ileus: Large gallstone erodes through gall Large gallstone erodes through gall
bladder wall into neighbouring bladder wall into neighbouring duodenum, passes along small bowel duodenum, passes along small bowel until it lodges and causes small bowel until it lodges and causes small bowel obstructionobstruction
AXR: distended loops of small bowel, AXR: distended loops of small bowel, typically to terminal ileum, with air in typically to terminal ileum, with air in biliary treebiliary tree


RaritiesRarities
Mucocoele:Mucocoele: Gallstone lodges in neck of gall bladder, Gallstone lodges in neck of gall bladder,
preventing drainage of mucous.preventing drainage of mucous. May become infected, causing May become infected, causing
empyemaempyema Require drainage and later Require drainage and later
cholecystectomycholecystectomy PerforationPerforation CarcinomaCarcinoma

Mirizzi’s syndrome:Mirizzi’s syndrome: In 1948, P. L. Mirizzi described an unusual presentation of In 1948, P. L. Mirizzi described an unusual presentation of
gallstones which, when lodged in either the cystic duct or gallstones which, when lodged in either the cystic duct or the Hartmann pouch of the gallbladder, externally the Hartmann pouch of the gallbladder, externally compressed the common hepatic duct (CHD), causing compressed the common hepatic duct (CHD), causing symptoms of obstructive jaundice (Mirizzi, 1948). symptoms of obstructive jaundice (Mirizzi, 1948).
Pathophysiology: Pathophysiology: Impaction of a large gallstone (or Impaction of a large gallstone (or multiple small gallstones) in the Hartmann pouch or cystic multiple small gallstones) in the Hartmann pouch or cystic duct results in the Mirizzi syndrome in 2 ways: (1) Chronic duct results in the Mirizzi syndrome in 2 ways: (1) Chronic and/or acute inflammatory changes lead to contraction of and/or acute inflammatory changes lead to contraction of the gallbladder, which then fuses with and causes the gallbladder, which then fuses with and causes secondary stenosis of the CHD, or (2) large impacted secondary stenosis of the CHD, or (2) large impacted stones lead to cholecystocholedochal fistula formation stones lead to cholecystocholedochal fistula formation secondary to direct pressure necrosis of the adjacent duct secondary to direct pressure necrosis of the adjacent duct walls. Increasingly, these phenomena are seen not as walls. Increasingly, these phenomena are seen not as distinct and separate steps but as part of a continuum distinct and separate steps but as part of a continuum (Pemberton, 1997; Hazzan, 1999). (Pemberton, 1997; Hazzan, 1999).

Laparoscopic Laparoscopic cholecystectomycholecystectomy

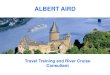
This is a case of a 42 year old male with a previous history of This is a case of a 42 year old male with a previous history of abdominal pain for 6 months. He was admitted to the abdominal pain for 6 months. He was admitted to the hospital with nausea but vomiting or fever. An ultrasound hospital with nausea but vomiting or fever. An ultrasound study showed gallstones with some thickening of the study showed gallstones with some thickening of the gallbladder wall. The diagnosis of cholecystitis was made gallbladder wall. The diagnosis of cholecystitis was made and the patient was scheduled to undergo a laparoscopic and the patient was scheduled to undergo a laparoscopic cholecystectomy. This picture shows the omentum partially cholecystectomy. This picture shows the omentum partially covering the gallbladder in its normal position.covering the gallbladder in its normal position.

Due to significant distention of the gallbladder, a Due to significant distention of the gallbladder, a needle is used to drain some bile so grasper clamps needle is used to drain some bile so grasper clamps can be applied for dissection and manipulation.can be applied for dissection and manipulation.

The Hartmann'a pouch is rectracted laterally and upward, The Hartmann'a pouch is rectracted laterally and upward, exposing the triangle of Calot where the cystic artery can exposing the triangle of Calot where the cystic artery can be identified branching off the right hepatic artery.be identified branching off the right hepatic artery.

A short cystic duct is dissected free using a "right A short cystic duct is dissected free using a "right angle" clamp.angle" clamp.

Clips are applied to the cystic duct away from Clips are applied to the cystic duct away from the common bile duct.the common bile duct.

The cystic duct is transected using scissors.The cystic duct is transected using scissors.

Same technique is used with the cystic artery Same technique is used with the cystic artery which is dissected free using a "right angle" which is dissected free using a "right angle" clamp and will be divided between clips.clamp and will be divided between clips.

Hook electrocautery is used to dissect the Hook electrocautery is used to dissect the gallbladder off the liver bed.gallbladder off the liver bed.

The gallbladder is now free and will be placed The gallbladder is now free and will be placed into a Pleatman sac for retreival.into a Pleatman sac for retreival.

This picture shows the body of the gallbladder, This picture shows the body of the gallbladder, that becomes distended during removal. Caution that becomes distended during removal. Caution must be used to avoid rupture while pulling.must be used to avoid rupture while pulling.

Thank youThank you
Questions?Questions?
Recommended