
Hindawi Publishing CorporationJournal of Aging ResearchVolume 2012, Article ID 306818, 30 pagesdoi:10.1155/2012/306818
Review Article
Flexibility Training and Functional Ability in Older Adults:A Systematic Review
Liza Stathokostas,1 Robert M. D. Little,1 A. A. Vandervoort,2 and Donald H. Paterson1
1 Canadian Centre for Activity and Aging, School of Kinesiology, The University of Western Ontario, London, 3M Centre 2225,ON, Canada N6A 3K7
2 School of Physical Therapy, Elborn College 1400, The University of Western Ontario, London, ON, Canada N6A 3K7
Correspondence should be addressed to Liza Stathokostas, [email protected]
Received 9 July 2012; Accepted 11 September 2012
Academic Editor: Wojtek Chodzko-Zajko
Copyright © 2012 Liza Stathokostas et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Background. As indicated in a recent systematic review relating to Canada’s Physical Activity Guidelines for Older Adults,exercise interventions in older adults can maintain or improve functional abilities. Less is known about the role of flexibilityin the maintenance or improvement of functional abilities, and there currently does not exist a synthesis of the literaturesupporting a consensus on flexibility training prescription. Purpose. To systematically review the effects of flexibility-specifictraining interventions on measures of functional outcomes in healthy older adults over the age of 65 years. Methods. Five electronicdatabases were searched for intervention studies involving concepts related to aging, flexibility, functional outcomes, and traininginterventions. After evaluating the articles for relevance, 22 studies were considered. Results. The results suggested that whileflexibility-specific interventions may have effects on range of motion (ROM) outcomes, there is conflicting information regardingboth the relationship between flexibility interventions and functional outcomes or daily functioning. Conclusions. Due to thewide range of intervention protocols, body parts studied, and functional measurements, conclusive recommendations regardingflexibility training for older adults or the validity of flexibility training interventions as supplements to other forms of exercise, oras significant positive influences on functional ability, require further investigation.
1. Introduction
As indicated in a recent systematic review relating toCanada’s Physical Activity Guidelines for Older Adults,exercise interventions (comprised of aerobic and strengthtraining) in older adults can maintain or improve functionalabilities [1]. Less is known about the role of flexibility inthe maintenance or improvement of functional abilities.While joint flexibility may decrease with age, with thepotential to affect normal daily function, older adults domaintain the ability to improve flexibility through stretchingexercises [1]. The 2009 American College of Sports Medicine(ACSM) position statement “Exercise and Physical Activityfor Older Adults” [2] noted there is a lack of studiesof the effects of range of motion exercises on flexibilityoutcomes in older populations and a lack of consensusregarding the prescription of stretching exercises for olderadults. Despite the lack of a synthesis of the literature to
support the recommendation of the inclusion of a flexibilitycomponent to older adult exercise programs, many olderadult activity programs place a considerable emphasis onflexibility. Stretching exercises are used extensively in therehabilitation context wherein injury or disease may haveresulted in a restricted range of motion specific to givenjoints, and the goal is to regain “normal” range of motion[3]. However, the present paper is focused not on stretchingexercise for rehabilitation purposes but for the role offlexibility in general exercise prescription for older adults.
In light of the significant benefits of an exercise programfor an aging population, it is important to provide evidence-based prescription for older adult exercise programs andhighlight areas of research requiring further investigation inorder to maximize these benefits. The goal of a flexibilityprogram is to improve range of motion in the major muscle-tendon groups in accordance with individualized goals [4].For the majority of the aging population, the goals may not

2 Journal of Aging Research
be related to athletic performance, but rather performance offunctional abilities in activities of daily living. Nevertheless,there is relatively little research on the potential benefits offlexibility-specific training interventions for this populationin that context. Despite the lack of research and no “knownhealth benefits” [5], again, there is still a tendency in theliterature to mention flexibility training as a presumed“component of fitness” and beneficial adjunct to other formsof exercise. Therefore, the purpose of this systematic reviewis to investigate the functional outcomes of flexibility specifictraining in older adults.
2. Methods
2.1. The Literature Search and Inclusion Criteria. A searchstrategy was developed, where all reasonable expressionsof the concepts of aging, flexibility, functional outcomes,and training interventions were considered (see Appendixfor a sample search strategy). A comprehensive electronicliterature search was conducted on five online databases:PubMed (NCBI; 1950-), Embase (OVID; 1974-), CINAHL(OVID & EBSCO; 1982-), Scopus (1823-), and SportDis-cus (EBSCO; 1800-). The literature was searched up toJanuary 2011. The final inclusion criteria for this paperwere (1) an original research article, (2) human subjects,(3) an intervention study, (4) flexibility training was anindependent intervention or was used as a control, (5) agedpopulation (mean age ≥ 65 years), and (6) the populationwas healthy but allowing for arthritis, osteoarthritis, andthose residing in assisted living (based on age and risk,not diseases or other medical conditions). For this paper,healthy was operationally defined as community-dwellingand assisted living with the health and function and cognitiveability to participate in light physical activity interventionsand complete physical function measures. Interventionstargeting specific chronic conditions (aside from arthritisand osteoarthritis) were excluded from review. Despite theiruse in flexibility training, tai chi- and yoga-based studieswere excluded from this paper because by nature they includestrength components. The electronic search yielded 4037citations. The citations and applicable electronic versionsof the article (where available) were downloaded to anonline research management system (RefWorks, Bethesda,MD, USA).
2.2. Screening. Two reviewers independently (RL, LS) eval-uated the articles for relevance using standard systematicreview methodology leading to further consideration of 22articles.
Two reviewers independently completed standardizeddata extraction forms for each level of screening. Three levelsof screening were utilized. Level 1 screening was based onarticle titles, Level 2 was based on the title and abstract, andLevel 3 was a full text screening. The articles that progressedthrough to Level 3 were retrieved electronically or manuallyvia the Canadian interlibrary system and were printedfrom electronic copy. Any cross-referenced articles from thereference section of Level 3 articles were hand-screened.
Disagreements regarding inclusion were resolved throughdiscussion with a third reviewer (DP).
2.3. Data Extraction. Data from the included studies wereextracted (Table 1) and organized by the target musclegroups of the flexibility interventions. Two reviewers com-pleted standardized data extraction forms. One reviewerperformed the data extraction for each paper assigned tothem and the extraction was verified by another reviewer.The reviewers were not blinded to the journal or the authornames when extracting information from the articles.
2.4. Level of Evidence. The approach used to establish thelevel and grade of evidence was consistent with Lau et al.[6] which provide predefined and objective criteria. Thus,the strength of the evidence was assessed for flexibilityinterventions and functional outcomes in older adults withrespect to general recommendations and appropriate dose.
2.5. Quality Assessment. Quality assessment of the includedstudies was also performed (Table 1). The Downs and Black[7] scale was selected to assess the quality of each study as it isappropriate to evaluate nonrandomized investigations, and itcontained the highest number of relevant items for the needsof this paper. However, as not all items were relevant to thevarious study types included in this paper, a modified versionof the checklist was employed for each of RCTs (randomizedcontrol trials), and non-RCTs study types. Thus, the qualityof each study was also established similar to the method ofGorber et al. [8] to include the most relevant componentsof the scoring tool. Therefore, a modified version of theDowns and Black checklist was used with the final checklistconsisting of 22 items with a maximum score of 24 points forthe studies of a RCT design; 22 items for non-RCT designswith a maximum score of 23; experimental single groupinterventions had a maximum score of 18 from 18 items;experimental single-group and single-session studies werebased on 14 items for a maximum score of 14. Higher scoresreflected a superior quality of investigation.
2.6. Integration of Findings. Due to the heterogeneity acrossstudy populations, methods used, and outcomes assessed, weconducted a narrative synthesis of the results.
3. Results
3.1. Description of Studies. The initial search yielded 4037articles. Twenty-two articles were ultimately included aftermeeting Level 3 inclusion criteria (Figure 1). Of the final 22articles, 18 were from electronic database searching, and 4were found by hand searching. Quality assessment indicatedthat the RCT studies (n = 13) were of good quality with anaverage score of 18 out of 24. The non-RCT studies (n = 6)had an average score of 14 out 23. An average score of 12out of 18 was assessed for the experimental single-groupstudies (n = 3). Fourteen articles were conducted in theUnited States [10–12, 14, 15, 17, 18, 20, 22, 25–29], whilethe remainder of the studies were from Japan [19], Brazil

Journal of Aging Research 3
Ta
ble
1:Ta
ble-
Flex
ibili
tytr
ain
ing
stu
dies
exam
inin
gth
ere
lati
onsh
ipbe
twee
nfl
exib
ility
and
fun
ctio
nal
abili
ties
inol
der
adu
lts.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Bar
rett
and
Smer
dely
,20
02[9
].A
ust
ralia
.R
CT
(sin
gle-
blin
ded,
asse
ssor
).Fo
cus
Maj
orm
usc
legr
oups
.
Tode
term
ine
wh
eth
era
resi
stan
cetr
ain
ing
prog
ram
cou
ldim
prov
est
ren
gth
,m
obili
ty,a
nd
qual
ity
oflif
eof
com
mu
nit
y-dw
ellin
gel
derl
yp
eopl
eve
rsu
sfl
exib
ility
con
trol
grou
p.
n=
40.
Age
:67
yr.
10m
ales
,30
fem
ales
.E
xper
imen
tal
n=
20.
Age
:64±
3yr
.5
mal
e,15
fem
ale.
Con
trol
n=
20A
ge:7
0±
3yr
.5
mal
e,15
fem
ale.
Incl
usi
oncr
iter
ia>
60yr
,hea
lthy
.
Pre
post
10w
ks.
Bot
hgr
oups
atte
nde
dcl
ass
1h
r,tw
ice
wk−
1,1
0w
ks.
Inte
rven
tion
5m
inw
arm
-up
incl
udi
ng
stre
tch
ing,
8–10
resi
stan
ceex
erci
ses
(∼45
min
)w
ith
free
wei
ghts
for
both
upp
eran
dlo
wer
limbs
,fol
low
edby
5m
inof
stre
tch
ing.
Con
trol
Stre
tch
ing
ofm
ajor
mu
scle
grou
ps(2
5m
in)
ligh
tca
rdio
vasc
ula
r(2
0m
in)
and
low
inte
nsi
tyst
ren
gth
enin
g(1
5m
in).
Ass
essm
ent
Isom
etri
cst
ren
gth
bila
tera
llyw
ith
han
ddy
nam
omet
er:b
icep
s,qu
ads;
tim
eto
stan
dan
dsi
t5
tim
esfo
rle
gst
ren
gth
.B
alan
ce:F
un
ctio
nal
reac
hte
stan
dst
epte
st.
Qu
alit
yof
Life
:SF3
6H
ealt
h.
Surv
eyse
lf-r
epor
ted.
An
alys
isIn
depe
nde
nt
sam
ple
t-te
sts.
Gen
der:
Ch
i-sq
uar
ete
sts.
Bon
ferr
onia
dju
stm
ent.
Pro
gres
sive
resi
stan
cetr
ain
ing
grou
pim
prov
edsi
gnifi
can
tly
inal
lphy
sica
lm
easu
rem
ents
.Fl
exib
ility
grou
pim
prov
edsi
gnifi
can
tly
insi
t-to
-sta
nd
(9.6
%fr
om10
.2to
9.2
s)an
dst
epte
st(2
3.5%
from
17to
20st
eps)
only
.P
rogr
essi
vere
sist
ance
trai
nin
gh
ada
grea
ter
effec
tth
anfl
exib
ility
trai
nin
gon
quad
rice
psst
ren
gth
,lef
tbi
ceps
stre
ngt
h,f
un
ctio
nal
reac
hte
stan
dst
epte
st.
Nei
ther
grou
pim
prov
edsi
gnifi
can
tly
inan
ysu
bsca
leof
qual
ity
oflif
e.
Pro
gres
sive
hig
hin
ten
sity
resi
stan
cetr
ain
ing
prod
uce
sgr
eate
rst
ren
gth
,bal
ance
,an
dga
itim
prov
emen
tsth
ana
non
spec
ific
flex
ibili
tygr
oup.
13/1
8

4 Journal of Aging Research
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Kle
inet
al.2
002
[10]
.U
SA.
Pro
spec
tive
two-
stag
ein
terv
enti
on.
Focu
sM
ajor
mu
scle
grou
ps.
Toex
amin
eth
eim
pact
ofP
NF
onph
ysic
alfu
nct
ion
inan
assi
sted
-liv
ing
popu
lati
onby
asse
ssin
gR
OM
and
isom
etri
cst
ren
gth
.
n=
14.
Age
:87±
6.5
yr.
Mal
e=
2.Fe
mal
e=
12.
Incl
usi
oncr
iter
ia≥6
5yr
,no
neu
rolo
gica
lor
cogn
itiv
eim
pair
men
ts,r
esti
ng
BP<
160/
100
mm
Hg,
no
limit
ing
card
iore
spir
ator
yco
ndi
tion
orre
cen
tsu
rger
yLi
vin
gin
assi
sted
-liv
ing
faci
lity,
frai
l.
Bas
elin
e(T
1),p
retr
ain
ing
(T2,
5w
ks),
post
trai
nin
g(T
3,10
wks
).P
re-t
rain
ing
1w
k−1
visi
tw
ith
trai
ner
toin
crea
sera
ppor
tan
din
tere
stin
part
icip
atio
n.
Trai
nin
gp
rogr
am40
–60
min
,2w
k−1W
arm
-up,
cool
dow
n,a
nd
flex
ibili
ty(s
ingl
ese
t15
–20
min
,lat
er2-
3se
ts)
Flex
ibili
ty:8
exer
cise
su
sin
gpa
ssiv
eco
ntr
act-
rela
xP
NF
tech
niq
ue
(6s
isom
etri
cco
ntr
acti
onth
enpa
ssiv
est
retc
hh
eld
for
20s
then
20s
rest
).H
amst
rin
gs,g
lute
als,
shin
s,ca
lves
and
back
).A
sses
smen
tsIs
omet
ric
stre
ngt
h(d
ynam
omet
er),
flex
ibili
ty(b
ubb
lein
clin
omet
erfo
rsh
ould
ers,
hip
s,an
dan
kles
,si
t-an
d-re
ach
for
spin
e,fu
nct
ion
al-r
each
for
shou
lder
).M
obili
ty:g
et-u
p-an
d-go
test
,5-
sit-
to-s
tan
d.A
nal
ysis
List
wis
ere
pea
ted
mea
sure
s,u
niv
aria
teA
NO
VA
,pai
red
t-te
sts,
and
Bon
ferr
onia
dju
stm
ent
n=
11St
atis
tica
llysi
gnifi
can
tdi
ffer
ence
sin
6of
18va
riab
les:
sit-
to-s
tan
dde
crea
sed
sign
ifica
ntl
yfr
om9.
33to
7.91
s(P=
0.42
).N
och
ange
inba
lan
ce,g
etu
pan
dgo
,si
ngl
ele
gst
and.
An
kle-
flex
ion
RO
Mde
crea
sed
(im
prov
ed)
from
26.2
5to
20.2
7◦
(P=
0.00
9).
Shou
lder
-flex
ion
RO
Min
crea
sed
from
163.
8to
177.
6◦(P=
0.01
6)N
och
ange
inh
ipfl
exio
n,h
ipex
ten
sion
,an
kle
exte
nsi
on,
fun
ctio
nal
reac
h,a
nd
sit-
and-
reac
h.
Sign
ifica
nt
incr
ease
sin
stre
ngt
hfo
rh
ipex
ten
sion
and
ankl
efl
exio
n/e
xten
sion
.N
och
ange
inh
ipfl
exio
n,s
hou
lder
exte
nsi
on,a
nd
shou
lder
flex
ion
stre
ngt
h
PN
Ffl
exib
ility
trai
nin
gca
nim
prov
eR
OM
,iso
met
ric
stre
ngt
h,a
nd
sele
cted
phys
ical
-fu
nct
ion
task
sin
assi
sted
-liv
ing
olde
rad
ult
s.B
ecau
seth
etr
ain
ing
peri
odw
assh
ort,
10w
eeks
,th
ere
sult
ssu
gges
tth
atco
nti
nu
edtr
ain
ing
mig
ht
hav
ea
grea
ter
impa
cton
phys
ical
fun
ctio
nan
dth
eab
ility
top
erfo
rmro
uti
ne
daily
acti
viti
es.
13/1
8

Journal of Aging Research 5
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Bro
wn
etal
.200
0[1
1].
USA
.R
CT.
Focu
sM
ajor
mu
scle
grou
ps.
Toex
amin
eeff
ects
oflo
w-i
nte
nsi
tyex
erci
seon
fact
ors
asso
ciat
edw
ith
frai
lty
(gai
t,fl
exib
ility
,str
engt
h,
bala
nce
,sen
sati
on,
resp
onse
tim
e,an
dco
ordi
nat
ion
)ve
rsu
sfl
exib
ility
con
trol
grou
p.
n=
87.
Age
:83±
4yr
.E
xper
imen
talg
rou
p(e
xer)
n=
48.
Mal
e=
20,
Fem
ale=
28.
Age
:83±4
yr.
Con
trol
grou
p(h
ome)
n=
39.
Mal
e=
17,
fem
ale=
22.
Age
:83±4
yr.
Ch
arac
teri
stic
sSe
den
tary
,ove
r78
yrs,
livin
gin
depe
nde
ntl
ybu
tw
ith
diffi
cult
y.In
clu
sion
crit
eria
Med
ical
scre
enin
g,ph
ysic
alpe
rfor
man
cete
st(P
PT
)fo
rfr
ailt
y:17
<sc
ore<
32.
Pre
-pos
t3
mo
Inte
rven
tion
exer
22lo
win
ten
sity
stre
ngt
han
dfl
exib
ility
exer
cise
for
upp
eran
dlo
wer
body
3x/w
eek
for
tota
lof3
6se
ssio
ns
(∼3
mo)
HO
ME
9u
pper
and
low
erbo
dyfl
exib
ility
exer
cise
s.C
ondu
cted
ath
ome
(sel
f-re
port
),op
tion
topa
rtic
ipat
eon
site
1w
k−1.
Ass
essm
ents
Stre
ngth
:phy
sica
lper
form
ance
test
,iso
kin
etic
dyn
amom
eter
(kn
eefl
exor
s/ex
ten
sors
,an
kle
flex
ors/
exte
nso
rs),
and
han
d-h
eld
dyn
amom
eter
(upp
erex
trem
itie
s)R
OM
:gon
iom
etry
(sh
ould
ers,
hip
s,kn
ees,
ankl
es,a
nd
tru
nk)
.B
alan
ce:s
tati
c(R
ombe
rgte
st),
dyn
amic
(bal
ance
bean
,obs
tacl
eco
urs
e,an
dga
itsp
eed)
,an
dw
eigh
t-sh
ift
(Ber
gba
lan
cete
st).
Gai
t:pr
essu
re-s
ensi
tive
foot
swit
ches
.C
oord
inat
ion:
Pu
rdu
ep
egbo
ard.
Spee
dof
resp
onse
:red
ligh
tto
gree
nlig
ht,
step
pin
gon
brak
ean
dga
spe
dals
.Se
nsat
ion:
Sem
mes
-Wei
nst
ein
mon
ofila
men
ts.
An
alys
is2×
2A
NO
VA
;pai
red
t-te
sts
for
EX
ER
grou
pon
ly
Phy
sica
lper
form
ance
test
Sign
ifica
nt
impr
ovem
ents
inP
PT
scor
esfr
om29±
4to
31±
4;u
nch
ange
din
con
trol
grou
p);
impr
ovem
ents
wer
ein
chai
rri
se,
putt
ing
on/t
akin
goff
coat
,pic
kin
gu
ppe
nny
,an
dR
ombe
rgte
st.
Stre
ngt
hSi
gnifi
can
tin
crea
ses
inkn
eefl
exor
and
exte
nso
rst
ren
gth
(9%
chan
geve
rsu
s−1%
inco
ntr
ol)
and
shou
lder
abdu
ctor
s.R
ange
ofm
otio
nFl
exib
ility
incr
ease
din
all
mea
sure
men
tsan
din
both
grou
ps.
Bal
ance
Sign
ifica
nt
impr
ovem
ents
inE
XE
Rgr
oup
for
obst
acle
cou
rse,
full-
tan
dem
ofR
ombe
rg,B
erg
bala
nce
test
,an
don
e-lim
bst
andi
ng
tim
e.N
osi
gnifi
can
tch
ange
sin
con
trol
grou
pG
ait
Sign
ifica
nt
chan
gein
pref
erre
dw
alki
ng
cade
nce
inE
XE
Rgr
oup.
Coo
rdin
atio
nD
iffer
ence
betw
een
grou
psw
as“a
lmos
tsi
gnifi
can
t.”R
esp
onse
tim
eU
nch
ange
din
both
grou
ps.
Sen
sati
onN
oap
pare
nt
diff
eren
ces.
Th
eco
ntr
olgr
oup
lost
asm
alla
mou
nt
ofst
ren
gth
and
bala
nce
inju
st3
mon
ths,
even
thou
ghfl
exib
ility
impr
oved
.T
hes
ere
sult
ssu
gges
tth
atth
em
ore
com
preh
ensi
veth
eex
erci
sein
terv
enti
on,t
he
grea
ter
the
likel
ysc
ope
ofim
prov
emen
tin
frai
lty.
14/2
4

6 Journal of Aging Research
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Kin
get
al.2
000
[12]
.U
SA.
RC
T.Fo
cus
Maj
orm
usc
legr
oups
.
Toev
alu
ate
the
effec
tsof
two
diff
eren
tco
mm
un
ity-
base
dph
ysic
alac
tivi
tyre
gim
ens—
onon
eye
arph
ysic
alpe
rfor
man
ceou
tcom
es,
per
ceiv
edfu
nct
ion
ing
and
wel
l-be
ing
ina
sam
ple
ofco
mm
un
ity-
dwel
ling,
sede
nta
ryw
omen
and
men
.
n=
103
Age
:70±
4yr
Mal
es=
36,f
emal
es=
67 Incl
usi
oncr
iter
ia>
65yr
s,ab
sen
ceof
card
iova
scu
lar
dise
ase
orst
roke
,reg
ula
rly
acti
ven
om
ore
than
2x/w
eek
duri
ng
the
prec
edin
g6
mo,
free
ofm
usc
ulo
skel
etal
prob
lem
sth
atw
ould
prev
ent
part
icip
atio
nin
mod
erat
ele
vels
ofph
ysic
alac
tivi
ty.
Pre
-pos
t12
mon
th,6
mon
thin
teri
mas
sess
men
t2
exer
cise
clas
ses/
wee
kan
dh
ome
exer
cise
atle
ast
2w
k−1.
Cla
sses
one
hou
r,h
ome
exer
cise
built
up
to40
min
sess
ion
s.E
xper
imen
talg
rou
p(fi
tan
dfi
rm)
Pro
gres
sive
mod
erat
e-in
ten
sity
endu
ran
cean
dst
ren
gth
enin
gex
erci
ses.
5–10
min
war
m-u
p,40
–45
min
aero
bic
and
stre
ngt
htr
ain
ing
circ
uit
,5–1
0m
inco
ol-d
own
;ta
rget
hea
rtra
te60
–75%
HR
R.
Con
trol
grou
p(s
tret
chan
dfl
ex)
Stre
tch
ing
and
flex
ibili
tyex
erci
ses.
5–10
min
war
m-u
p,40
min
stre
tch
ing
sect
ion
,5–1
0m
inre
laxa
tion
exer
cise
s.St
retc
hin
gfo
rn
eck,
shou
lder
s,ba
ck,c
hes
t,w
aist
,ham
stri
ngs
,ca
lves
,an
dh
ands
.A
sses
smen
tsFu
ncti
onal
capa
city
/end
uran
ce:
Gra
ded
trea
dmill
exer
cise
test
(GX
T).
Stre
ngth
and
flexi
bilit
y:u
pper
body
stre
ngt
h(l
ift
and
reac
hta
sk),
low
erbo
dyst
ren
gth
(sit
tost
and)
,an
dfl
exib
ility
(sit
and
reac
hw
/Acc
ufl
ex1
sit
and
reac
hbo
x.Se
lf-ra
ted
phys
ical
perf
orm
ance
:ase
lf-e
ffica
cyqu
esti
onn
aire
.Pe
rcei
ved
func
tion
ing
and
wel
l-be
ing:
scal
esfr
omth
eM
edic
alO
utc
omes
Stu
dy(M
OS)
incl
.ph
ysic
alfu
nct
ion
ing,
bodi
lypa
in,
emot
ion
alw
ell-
bein
g,
(val
ues
repo
rted
sepa
rate
lyfo
rm
enan
dw
omen
for
each
grou
p).
Fun
ctio
nal
cap
acit
y/en
du
ran
ceSu
bmax
HR
:Fit
&Fi
rmh
adsi
gnifi
can
tly
grea
ter
impr
ovem
ent
vers
us
Stre
tch
&Fl
exSt
ren
gth
and
flex
ibil
ity
Lif
tan
dre
ach
task
:Fit
&Fi
rmh
adsi
gnifi
can
tly
grea
ter
upp
erbo
dyst
ren
gth
than
Stre
tch
&Fl
ex.
Sit-
to-s
tan
d:N
osi
gnifi
can
tre
sult
s.Si
t-an
d-re
ach
:Men
assi
gned
toSt
retc
h&
Flex
had
sign
ifica
ntl
ygr
eate
rin
crea
ses
than
men
inFi
t&
Firm
.No
stat
isti
cald
iffer
ence
inw
omen
,bu
ttr
end
for
grea
ter
impr
ovem
ent
for
wom
enin
Fit
&Fi
rmve
rsu
s.St
retc
h&
Flex
.Wom
enin
Fit
&Fi
rmh
adsi
gnifi
can
tly
grea
ter
incr
ease
sin
flex
ibili
tyat
12m
oth
anm
en.
Self
-rat
edp
hysi
calp
erfo
rman
ceSi
gnifi
can
tly
grea
ter
incr
ease
sin
wal
kin
gdi
stan
cean
dse
lf-e
ffica
cyfo
rh
eavy
lifti
ng
inFi
t&
Firm
than
inSt
retc
h&
Flex
.P
erce
ived
fun
ctio
nin
gan
dw
ell-
bei
ng
On
lypa
insc
ale
had
sign
ifica
ntl
ygr
eate
reff
ects
for
Stre
tch
&Fl
ex(a
lso
stat
isti
cally
sign
ifica
nt
wit
hin
grou
p)th
anFi
t&
Firm
.
Com
mu
nit
y-ba
sed
phys
ical
acti
vity
regi
men
sfo
cusi
ng
onm
oder
ate-
inte
nsi
tyen
dura
nce
and
stre
ngt
hen
ing
exer
cise
sor
flex
ibili
tyex
erci
ses
can
bede
liver
edth
rou
gha
com
bin
atio
nof
form
ats
that
resu
ltin
impr
ovem
ents
inim
port
ant
fun
ctio
nal
and
qual
ity
oflif
eou
tcom
es.
21/2
4

Journal of Aging Research 7
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
ener
gy/f
atig
ue,
slee
ppr
oble
ms,
sen
seof
mas
tery
,an
dse
lf-e
stee
m.
An
alys
isA
NO
VA
,AN
CO
VA
,MA
NC
OV
A,
Tuke
y’s
stu
den
tize
dra
nge
test
,an
dle
ast-
squ
ares
mea
ns
proc
edu
re.
Laz
owsk
iet
al.1
999
[13]
.C
anad
a.R
CT.
Focu
sM
ajor
mu
scle
grou
ps.
Toev
alu
ate
grou
pex
erci
sepr
ogra
ms
inlo
ng-
term
care
vers
us.
flex
ibili
tyco
ntr
olgr
oup.
n=
68.
Age
:80±
0.9
yr.
11m
ale,
57fe
mal
e.Fu
nct
ion
alFi
tnes
sfo
rlo
ng-
term
care
prog
ram
(FFL
TC
)gr
oup
n=
36.
7m
ale,
29fe
mal
e.R
ange
ofm
otio
n(R
OM
)gr
oup
n=
32.
2m
ale,
30fe
mal
e.R
esid
ents
offi
velo
ng-
term
care
inst
itu
tion
s(>
3m
onth
)In
clu
sion
crit
eria
No
rece
nt
card
iova
scu
lar
even
ts,
un
con
trol
led
hig
hB
P,re
cen
tfr
actu
re,t
otal
blin
dnes
s,or
deaf
nes
s.A
bilit
yto
stan
dw
ith
min
imal
assi
stan
ce.
Wal
kin
gde
vice
san
dw
hee
lch
airs
allo
wed
.
Pre
-pos
t4
mo
Inte
rven
tion
FFLT
Cgr
oup
45m
in,3
wk−
1
war
mu
p/st
retc
hin
g(5
min
),w
alki
ng
(15
min
),pr
ogre
ssiv
eu
pper
and
low
erbo
dyst
ren
gth
enin
g(1
0m
in),
bala
nce
,an
dco
oldo
wn
stre
tch
ing
(5m
in).
Con
trol
grou
pSe
ated
ran
geof
mot
ion
grou
pvo
cale
xerc
ises
,wor
d/m
emor
yga
mes
,ran
geof
mot
ion
exer
cise
s(fi
nge
rs,h
ands
,arm
s,kn
ees,
ankl
es),
and
rela
xati
onex
erci
ses.
Ass
essm
ents
Mob
ility
-tim
edu
p-an
d-go
(TU
G).
Fun
ctio
nal
bala
nce
-Ber
gSc
ale.
Stai
rcl
imbi
ng
pow
er.
Fun
ctio
nal
abili
ty-f
un
ctio
nal
inde
pen
den
cem
easu
re(F
IM).
Flex
ibili
ty-M
odifi
edsi
tan
dre
ach
test
.sh
ould
erfl
exio
n.
Isom
etri
cst
ren
gth
:elb
owfl
exio
n,
shou
lder
abdu
ctio
n,k
nee
exte
nsi
on,h
ipab
duct
ion
/add
uct
ion
.gr
ipst
ren
gth
.Is
oton
icSt
ren
gth
:kn
eeex
ten
sors
.
86%
and
79%
com
plia
nce
RO
Msc
ored
low
eron
seve
ral
mea
sure
sat
base
line.
Con
side
rabl
eva
riab
ility
wit
hin
all
con
diti
ons
onal
lmea
sure
s.FF
LTC
led
tosi
gnifi
can
tim
prov
emen
tsin
mob
ility
,bal
ance
,fl
exib
ility
,an
dva
riou
sm
easu
res
ofst
ren
gth
.Fu
nct
ion
alca
paci
tyw
asu
nch
ange
din
the
FFLT
Cgr
oup
and
decr
ease
din
the
RO
Mgr
oup.
No
chan
gein
grip
stre
ngt
h,g
ait
spee
dan
dst
air-
clim
bin
gpo
wer
for
eith
er,g
rou
p.R
OM
(con
trol
).In
crea
sed
TU
Gti
me.
No
chan
gein
bala
nce
orlo
wer
body
flex
ibili
ty.
Non
-sig
nifi
can
t3.
5%ch
ange
insh
ould
erfl
exio
nR
OM
.21
%in
crea
sein
shou
lder
abdu
ctio
nst
ren
gth
.D
eclin
ein
isot
onic
leg
and
hip
stre
ngt
h.
Th
eFF
LTC
issu
itab
lefo
rlo
ng-
term
care
resi
den
ts,
feas
ible
for
staff
tode
liver
,an
dlo
w-c
ost.
Mos
tim
port
antl
y,fu
nct
ion
alou
tcom
escl
earl
ysu
per
ior
tose
ated
RO
Mpr
ogra
m.
RO
Mm
ayim
prov
esh
ould
er-a
bdu
ctio
nst
ren
gth
,bu
tw
illn
otpr
even
tde
clin
esin
low
erbo
dyst
ren
gth
,m
obili
ty,a
nd
bala
nce
.
21/2
4

8 Journal of Aging Research
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Stan
zian
oet
al.2
009
[14]
.U
SA.
RC
T.Fo
cus
Maj
orm
usc
legr
oups
.
Toex
amin
eim
pact
ofan
acti
ve-
assi
sted
(AA
)fl
exib
ility
prog
ram
onR
OM
and
fun
ctio
nal
perf
orm
ance
vari
able
sin
olde
rpe
rson
sliv
ing
ina
resi
den
tial
reti
rem
ent
com
mu
nit
y(R
RC
).
n=
17.
Age
:88±
5.4
yr.
Exp
erim
enta
lgro
up
n=
8.90±
4.5
yr.
1m
ale,
7fe
mal
e.C
ontr
olgr
oup
n=
9.88±
6.2
yr.
3m
ale,
6fe
mal
e.In
clu
sion
crit
eria
Livi
ng
inan
RR
C,a
bilit
yto
sit
upr
igh
tin
ach
air
for
30m
in(n
oak
ath
isia
,n
euro
logi
cal,
oros
teop
orot
iclim
itat
ion
s).
Pre
-pos
t8
wks
2w
k−1
Exp
erim
enta
lgro
up
10st
retc
hes
:bac
ksc
ratc
h(s
hou
lder
flex
ion
/abd
uct
ion
),st
andi
ng
thig
h(h
iphy
pere
xten
sion
),si
delu
nge
(hip
abdu
ctio
n),
over
hea
dba
ck(s
hou
lder
hyp
erfl
exio
n),
over
hea
dsi
de(l
ater
altr
un
kfl
exio
n),
cros
sch
est
(hor
izon
tals
hou
lder
addu
ctio
n),
seat
edtr
un
ktw
ist
(tru
nk
rota
tion
),se
ated
ham
stri
ng
(tru
nk/
hip
flex
ion
),an
dse
ated
calf
(dor
sifl
exio
n).
10re
peti
tion
s,4-
5s
each
.C
ontr
olgr
oup
Art
san
dcr
afts
clas
sw
ith
limit
edph
ysic
alex
erti
on.
Ass
essm
ent
Con
duct
ed1
wk
befo
rean
daf
ter
trai
nin
gpe
riod
.Fl
exib
ility
:ba
cksc
ratc
hte
st(B
S).
Mod
ified
chai
rsi
tan
dre
ach
test
(SR
).Su
pin
ekn
eeex
ten
sion
test
(KE
).M
odifi
edto
talb
ody
rota
tion
test
(BR
).St
ren
gth
/pow
er:
30-s
ecch
air
stan
d(C
S).
Mod
ified
ram
ppo
wer
test
(MR
PT
).30
-sec
arm
curl
(AC
).G
allo
nju
gsh
elft
est
(GJS
T).
Mob
ility
:50
-foo
tga
itsp
eed
test
(GS)
.8-
foot
tim
edu
pan
dgo
(UG
).A
nal
ysis
AN
CO
VA
n=
13Fl
exib
ilit
ySi
gnifi
can
tin
crea
ses
inR
OM
mad
eby
exp
erim
enta
lgro
up
for
all
mea
sure
sbu
tle
ftsi
deB
San
dri
ght
side
SR.
Con
trol
grou
psh
owed
no
chan
gein
any
flex
ibili
tym
easu
rebu
ta
sign
ifica
nt
loss
inR
OM
for
righ
t-si
dekn
eeex
ten
sion
.Fu
nct
ion
alit
yE
xper
imen
talg
rou
psi
gnifi
can
tly
impr
oved
CS
and
MR
PT,
wh
ileco
ntr
olh
adsi
gnifi
can
tde
clin
es.
Exp
erim
enta
lgro
up
sign
ifica
ntl
yim
prov
edin
AC
and
the
GJS
T,w
hile
con
trol
had
no
chan
ge.
Exp
erim
enta
lgro
up
redu
ced
tim
eta
ken
toco
mpl
ete
the
UG
and
GS.
Eig
ht
wee
ksof
AA
stre
tch
ing
may
bean
effec
tive
inte
rven
tion
for
impr
ovin
gR
OM
,mob
ility
,an
dfu
nct
ion
alp
ower
for
olde
rpe
rson
sliv
ing
ina
RR
C.
Dat
apr
ovid
ecl
ear
link
betw
een
flex
ibili
tyan
dfu
nct
ion
alpe
rfor
man
cein
olde
rp
erso
ns
and
supp
ort
the
incl
usi
onof
flex
ibili
tytr
ain
ing
inin
terv
enti
ons
desi
gned
toin
crea
sein
depe
nde
nce
inol
der
pers
ons.
16/2
4

Journal of Aging Research 9
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Raa
bet
al.1
988
[15]
.U
SA.
Non
-RC
T.Fo
cus
Maj
orm
usc
legr
oups
.
Exa
min
eth
eab
ility
ofw
eigh
ted
and
non
wei
ghte
dex
erci
ses
toin
crea
sefl
exib
ility
inol
der
adu
lts
inth
eh
ip,s
hou
lder
,w
rist
,an
kle,
and
nec
k.
n=
46.
Fem
ale.
Exp
erim
enta
lgro
ups
Exe
rcis
e(n
ow
eigh
ts,
EN
).n=
16.
70±
3.9
yr.
Exe
rcis
e(w
ith
wei
ghts
,EW
).n=
17.
70±
3.2
yr.
Con
trol
grou
pN
oex
erci
se.
n=
1371±
8.1
yr.
Hea
lthy
,act
ive
olde
rad
ult
s.
Pre
-pos
t25
wks
.E
xerc
ise
pro
gram
60m
in,3
days
/wee
k;5–
10m
intr
eadm
illw
arm
-up;
10m
inae
robi
csat
65%
HR
max
;25
–30
min
wh
ole
body
stre
ngt
han
dfl
exib
ility
exer
cise
s;10
–15
mon
cool
-dow
n.
Exe
rcis
esin
volv
edac
tive
and
pass
ive
stre
tch
ing
hel
dfo
r20
s,sl
owci
rclin
gm
otio
ns
for
RO
M,
and
repe
titi
vem
ovem
ents
for
exam
ple,
leg
curl
s.E
Wh
adgr
adu
alin
trod
uct
ion
ofw
rist
and
ankl
ew
eigh
ts.
Ass
essm
ents
Shou
lder
flex
ion
and
abdu
ctio
n.
Nec
kro
tati
on.
Wri
stfl
exio
n/e
xten
sion
.A
nkl
efl
exio
n/e
xten
sion
.H
ipfl
exio
n.
An
alys
isTw
o-w
ayA
NO
VA
,Du
nn
-pla
nn
edco
mpa
riso
ns
wit
htw
oco
ntr
asts
,on
e-an
dtw
o-ta
iled
t-te
sts.
Flex
ibili
tyim
prov
edsi
gnifi
can
tly
for
exer
cise
grou
psin
ankl
epl
anta
rfl
exio
n,s
hou
lder
flex
ion
abdu
ctio
n,
and
cerv
ical
rota
tion
toth
ele
ft.
Hip
flex
ion
(refl
ecti
ng
ham
stri
ng
flex
ibili
ty)
incr
ease
dfo
ral
lgro
ups
,w
ith
no
betw
een
-gro
ups
diff
eren
ces.
Th
eex
erci
sew
ith
no
wei
ghts
grou
psh
adn
earl
y2.
5xgr
eate
rin
crea
sein
RO
Mth
anex
erci
sew
ith
wei
ghts
for
shou
lder
abdu
ctio
n.N
oot
her
flex
ibili
tyco
mpa
riso
ns
inth
eex
erci
segr
oups
wer
esi
gnifi
can
t.N
ofu
nct
ion
alou
tcom
es.
Exe
rcis
eca
nin
crea
sefl
exib
ility
inh
ealt
hy,o
lder
wom
enby
impr
ovin
gsh
ould
erfl
exio
nan
dab
duct
ion
,an
kle
plan
tar
flex
ion
,an
dce
rvic
alro
tati
on.
For
shou
lder
abdu
ctio
n,a
non
wei
ghte
dex
erci
sepr
ogra
mca
npr
odu
cegr
eate
rfl
exib
ility
gain
sin
olde
rad
ult
sth
ana
wei
ghte
dex
erci
sepr
ogra
m,a
nd
shou
ldbe
con
side
red
iffl
exib
ility
isth
epr
imar
ygo
al.
13/2
3

10 Journal of Aging Research
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Bir
det
al.2
009
[16]
.A
ust
ralia
.R
ando
miz
edC
ross
over
.Tr
ia.l.
Focu
sM
ajor
mu
scle
grou
ps.
Tode
term
ine
the
effec
tof
com
mu
nit
y-ba
sed
resi
stan
ce-
vers
us
flex
ibili
ty-t
rain
ing
prog
ram
son
bala
nce
and
rela
ted
mea
sure
s.
n=
32.
Age
:mea
n67
yr.
Mal
es=
18,
Fem
ales
=14
.Se
den
tary
.In
clu
sion
crit
eria
No
his
tory
ofst
roke
orot
her
neu
rolo
gica
ldi
seas
eor
curr
ent
diab
etes
,ca
rdio
vasc
ula
rdi
seas
e,or
un
con
trol
led
hype
rten
sion
.No
use
ofw
alki
ng
aids
.
Pre
-pos
t16
wks
,4w
kw
ash
out,
16w
ks(c
ross
over
).In
terv
enti
onB
oth
grou
psh
ad3
sess
ion
s. wk−
1
for
16w
ks,t
hen
4w
kw
ash
out,
then
swit
ched
toot
her
grou
pfo
r16
wks
.R
esis
tan
cetr
ain
ing
(RT
)2-
3se
tsof
10–1
2re
ps.
Flex
ibil
ity
trai
nin
g(F
T)
40–4
5m
inw
ith
16–2
0st
retc
hes
;tw
ost
retc
hes
for
each
of:
ham
stri
ngs
,qu
adri
ceps
,bac
k,an
dch
est.
Ass
essm
ents
Bal
ance
,for
cepl
ate.
Tim
edu
p-an
d-go
.10
tim
essi
t-to
-sta
nd.
Step
test
.Lo
wer
limb
stre
ngt
h(r
igh
tan
dle
ftkn
ee-fl
exio
nan
dex
ten
sion
)w
ith
anis
okin
etic
dyn
amom
eter
.A
nal
ysis
Rep
eate
dm
easu
res
AN
OV
A
Low
erlim
bst
ren
gth
incr
ease
dsi
gnifi
can
tly
inth
eR
Tgr
oup,
but
not
inth
efl
exib
ility
grou
pan
dth
ere
was
asi
gnifi
can
tdi
ffer
ence
betw
een
the
two
grou
ps.
Sign
ifica
nt
impr
ovem
ents
wer
ese
enin
both
grou
psfo
rti
med
up-
and-
go,
10ti
mes
sit-
to-s
tan
d,an
dst
epte
st.
Sign
ifica
nt
impr
ovem
ents
inm
edia
l-la
tera
lsw
ayra
nge
wer
ese
enin
the
flex
ibili
tygr
oup
only
.Si
gnifi
can
tde
crea
ses
insw
ayve
loci
tyw
ere
seen
inbo
thco
ndi
tion
s.
Sign
ifica
nt
impr
ovem
ents
inba
lan
cep
erfo
rman
cew
ere
ach
ieve
dw
ith
both
resi
stan
ce-t
rain
ing
and
stan
din
gfl
exib
ility
-tra
inin
gpr
ogra
ms
inh
ealt
hyu
ntr
ain
edol
der
adu
lts.
Flex
ibili
typr
ogra
mdi
din
corp
orat
eso
me
degr
eeof
bala
nce
trai
nin
gin
the
nat
ure
ofth
efl
exib
ility
task
s.
19/2
4

Journal of Aging Research 11
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Swan
ket
al.2
003
[17]
.U
SA.
Non
-RC
T.Fo
cus
Maj
orm
usc
legr
oups
.
Tode
term
ine
the
effec
tsof
addi
ng
mod
est
han
dan
dan
kle
wei
ghts
tow
hol
e-bo
dyst
retc
hin
gex
erci
seon
RO
M.
n=
43.
Age
:55–
83yr
.B
ody
Rec
all(
BR
).n=
18.
68±
5.6
yr;8
mal
e,10
fem
ale.
BR
+W
eigh
ts.
n=
14.
68±
3.1
yr.
4m
ale,
10fe
mal
e.C
ontr
ol.
n=
11.
69±
6.5
yr.
1m
ale,
10fe
mal
e.Pa
rtic
ipan
tsof
body
reca
llol
der
adu
ltlo
win
ten
sity
flex
ibili
typr
ogra
m.
Incl
usi
oncr
iter
iaN
oov
ert
dise
ase
oran
yse
vere
lylim
itin
gor
thop
aedi
cpr
oble
ms
Pre
-pos
t10
wks
.In
terv
enti
onSu
perv
ised
.B
R=
pain
-fre
e,sm
ooth
,rhy
thm
icw
hol
e-bo
dym
ovem
ents
.Tr
ain
ing
grou
p1
(BR
)60
min
ute
s,3
wk−
1.
Trai
nin
ggr
oup
2(B
R+
W)
60m
inu
tes,
3w
k−1w
ith
grad
ual
prog
ress
ion
ofan
kle
wei
ghts
and
ban
dex
erci
ses.
Con
trol
grou
pN
ode
scri
ptio
n.A
sses
smen
tR
OM
(gon
iom
eter
)fo
rn
eck
(lef
tan
dri
ght
rota
tion
),h
ip(fl
exio
nan
dex
ten
sion
),sh
ould
er(fl
exio
nan
dab
duct
ion
),kn
ee(e
xten
sion
and
flex
ion
),an
dan
kle
(pla
nta
ran
ddo
rsifl
exio
n).
An
alys
isA
NC
OV
A,L
even
e’s
test
ofeq
ual
ity.
Tuke
yH
ones
tly
Sign
ifica
nt
Diff
eren
cete
st,
P=≤
0.01
.
(pre
valu
esn
otgi
ven
).Si
gnifi
can
tdi
ffer
ence
sfo
un
dfo
r6
of10
RO
Mm
easu
res:
cerv
ical
rota
tion
(lef
tan
dri
ght)
,hip
exte
nsi
on,a
nkl
efl
exio
n/e
xten
sion
and
shou
lder
flex
ion
,for
both
BR
and
BR
+W
inco
mpa
riso
nto
con
trol
BR
+W
show
edsi
gnifi
can
tly
grea
ter
incr
ease
sin
4of
6m
easu
res
that
show
edsi
gnifi
can
tch
ange
:cer
vica
lro
tati
on(l
eft
and
righ
t),h
ipex
ten
sion
,an
dan
kle
dors
iflex
ion
vers
us
BR
.
Fou
nd
that
the
addi
tion
ofw
eigh
tsen
han
ced
effec
tive
nes
sof
stre
tch
ing
exer
cise
.It
islik
ely
that
apo
siti
veeff
ect
was
not
edfo
r2
reas
ons:
incr
ease
dre
sist
ance
duri
ng
exer
cise
mov
emen
tan
dex
erci
ses
wer
ep
erfo
rmed
thro
ugh
full
RO
M.
Itse
ems
plau
sibl
eto
hypo
thes
ize
that
grea
ter
effec
tsw
ould
besh
own
byad
diti
onof
wei
ghts
tost
retc
hin
gro
uti
nes
for
nu
rsin
gh
ome
clie
nts
orfr
ee-l
ivin
g,ot
her
wis
ese
den
tary
elde
rly.
14/2
3

12 Journal of Aging Research
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Ale
xan
der
etal
.200
1[1
8].
USA
.N
on-R
CT.
Focu
sM
ajor
mu
scle
grou
ps.
(1)
An
alyz
eth
ebi
omec
han
ics
ofri
sepe
rfor
man
cedu
rin
gch
air-
rise
task
sw
ith
vary
ing
task
dem
and
inm
ore
disa
bled
olde
rad
ult
s.(2
)To
dete
rmin
ew
het
her
ast
ren
gth
-tra
inin
gpr
ogra
mm
igh
tim
prov
ech
air-
rise
succ
ess
and
alte
rch
air-
rise
stra
tegy
vers
us.
flex
ibili
tyco
ntr
ol.
n=
30(fi
nal
).Tr
ain
ing
Gro
up.
n=
16.
Age
:82±
6.0
yr.
4m
ale,
12fe
mal
e.C
ontr
olgr
oup.
n=
14.
Age
:84±
7.4
yr.
2m
ale,
12fe
mal
e.R
esid
ents
oflo
cal
hou
sin
gfa
cilit
y.In
clu
sion
crit
eria
>65
yr.
No
low
erex
trem
ity
hem
iple
gia
oram
puta
tion
s,bl
indn
ess,
acu
tein
flam
mat
ory
orin
fect
iou
sill
nes
s,an
dn
ode
men
tia.
Mu
stco
mpl
ete
the
easi
est
chai
r-ri
seta
sk.
Can
not
becu
rren
tly
invo
lved
info
rmal
exer
cise
.
Pre
-pos
t12
wks
.In
terv
enti
onR
esis
tan
cetr
ain
ing
1h
our/
day,
3da
ys. w
k−1
usi
ng
Hyd
raFi
tnes
shy
drau
liceq
uip
men
tfo
rlo
wer
body
exer
cise
.Als
ow
eigh
ted
chai
rri
sean
dw
eigh
ted
ankl
efl
exio
n/e
xten
sion
.C
ontr
olgr
oup
Part
icip
ated
inse
ries
ofse
ated
nec
k,tr
un
k,ar
m,l
eg,a
nd
foot
flex
ibili
tyex
erci
ses.
Ass
essm
ent
Seve
nch
air
rise
task
s,bi
omec
han
ics
ofta
sks
H=
usi
ng
han
dsN
H=
wit
hou
tu
sin
gh
ands
60/1
00/1
40ar
ese
ath
eigh
tsas
%of
floo
rto
knee
hei
ghts
).A
nal
ysis
Two-
way
AN
OV
A,r
epea
ted
mea
sure
sA
NO
VA
wit
hpa
irw
ise
post
hoc
com
pari
son
s(F
ish
er’s
PL
SD).
On
lytr
ain
ing
grou
pim
prov
edab
ility
toco
mpl
ete
the
mos
tdi
fficu
ltta
sks.
Con
trol
sm
ain
tain
edp
erfo
rman
ces
inge
ner
al,o
ne
ortw
ode
clin
ed.
On
lysi
gnifi
can
tde
crea
sew
asin
tota
lri
seti
me
for
both
grou
psat
H-1
00.
Cen
tre
ofP
ress
ure
(CO
P)
incr
ease
dsi
gnifi
can
tly
inbo
thgr
oups
inal
lta
sks
but
H-1
40(h
igh
est
seat
hei
ght)
.K
nee
torq
ues
incr
ease
dfo
rbo
thgr
oups
sign
ifica
ntl
yfo
rH
-100
,H-6
0,N
H-1
00,a
nd
NH
-100
-F.
Mea
nh
ipto
rqu
esin
crea
sed
sign
ifica
ntl
yin
con
trol
san
dde
crea
sed
sign
ifica
ntl
yin
trai
nin
ggr
oup
inH
-60.
Subt
le,y
etsi
gnifi
can
tch
ange
sca
nbe
dem
onst
rate
din
chai
r-ri
sep
erfo
rman
ceas
are
sult
ofco
ntr
olle
d,sh
ort-
term
resi
stan
cetr
ain
ing
prog
ram
.
15/2
3

Journal of Aging Research 13
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Take
shim
aet
al.2
007
[19]
.Ja
pan
.N
on-R
CT.
Focu
sM
ajor
mu
scle
grou
ps.
Toco
mpa
reth
eeff
ects
ofa
wal
kin
g-ba
sed
aero
bic
prog
ram
,aba
nd-
base
dre
sist
ance
prog
ram
,ast
retc
hin
g-fl
exib
ility
prog
ram
,a
cust
omiz
edba
lan
cepr
ogra
m,
and
aTa
iCh
ipr
ogra
mon
fun
ctio
nal
fitn
ess
ina
grou
pof
com
mu
nit
yol
der
adu
lts.
n=
117.
73±
6yr
.64
mal
e,49
fem
ale.
Aer
obic
(AE
R).
n=
13.
Res
ista
nce
(RE
S).
n=
17.
Bal
ance
(BA
L).
n=
15.F
lexi
bilit
y(F
LE
X).
n=
16.
TaiC
hi(
T-C
HI,
Yan
gSt
yle)
.n=
31.
Con
trol
(CO
N).
n=
25.
Hea
lthy
sede
nta
ry.
Incl
usi
oncr
iter
iaN
om
eds
for
hyp
erte
nsi
on,H
RT.
No
CH
D,n
ore
gula
rph
ysic
alac
tivi
ty.
Pre
-pos
t12
wks
.In
terv
enti
onSu
perv
ised
2da
ysw
k−1
(RE
S,B
AL
,FL
EX
,T-C
HI)
3da
ysp
erw
k(A
ER
).A
llh
ad10
–15
min
war
m-u
p60
–70
min
ofsp
ecifi
cex
erci
se:
AE
R-O
utd
oor
wal
kin
gR
ES-
Pro
gres
sive
elas
tic
ban
dex
erci
ses
for
allm
ajor
mu
scle
grou
psB
AL-
Eye
sop
en/c
lose
d,ex
erci
seon
floo
r,on
foam
mat
sFL
EX
-15
stat
icst
retc
hes
for
upp
eran
dlo
wer
body
(15–
20s
each
).T
-CH
I-st
anda
rdiz
ed24
form
s.A
sses
smen
tsFu
nct
ion
alFi
tnes
s.30
sar
mcu
rlte
st.
30s
chai
rst
and
tim
e.8
Ftti
med
up-
and-
go.
back
scra
tch
test
.ch
air
sit
and
reac
hte
st.
12m
inw
alk
test
.A
nal
ysis
AN
OV
A.
Wilk
’scr
iter
ion
.K
olom
ogor
ov-S
mir
nov
test
.
Impr
ovem
ent
inca
rdio
resp
irat
ory
fitn
ess
(12
min
wal
k)w
aslim
ited
toA
ER
(16%
)R
ES,
BA
L,an
dT
-CH
I,re
sult
edin
impr
ovem
ents
inu
pper
and
low
erbo
dyst
ren
gth
and
bala
nce
/agi
lity.
RE
Ssh
owed
grea
test
upp
erbo
dyst
ren
gth
impr
ovem
ent
(31%
).B
AL
show
edgr
eate
stlo
wer
body
stre
ngt
him
prov
emen
t(4
0%).
Bal
ance
/agi
lity
was
sim
ilar
acro
ssR
ES,
BA
L,a
nd
T-C
HI
(10%
).Fu
nct
ion
alre
ach
,sim
ilar
impr
ovem
ents
for
AE
R(1
3%),
BA
L(1
6%),
RE
S(1
5%).
No
sign
ifica
nt
chan
ges
inei
ther
FLE
Xor
CO
Non
any
mea
sure
.
Itis
reco
mm
ende
dth
atol
der
adu
lts
part
icip
ate
ina
wel
l-ro
un
ded
exer
cise
prog
ram
vs.s
ingl
em
ode.
RE
S,B
AL
,an
dTA
IC
HI
cros
sdo
mai
ns
not
spec
ifica
llyta
rget
edin
thei
rde
sign
.A
ER
nec
essi
tate
sae
robi
c-sp
ecifi
cac
tivi
tyto
impr
ove
card
iore
spir
ator
yfi
tnes
s.W
ith
FLE
X,l
ack
ofim
prov
emen
tsu
gges
tsth
atfu
rth
erst
udy
isn
eede
dto
expl
ore
the
effec
tof
flex
ibili
tyex
erci
setr
ain
ing
inol
der
adu
lts.
18/2
3

14 Journal of Aging Research
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Eri
ckso
net
al.2
011
[20]
.U
SA.
RC
T.Fo
cus
Maj
orm
usc
legr
oups
.
Toev
alu
ate
wh
eth
er1
year
ofex
erci
setr
ain
ing
incr
ease
sth
esi
zeof
the
hip
poca
mpu
san
dim
prov
essp
atia
lmem
ory
usi
ng
mod
erat
e-in
ten
sity
aero
bic
exer
cise
vers
us
ast
retc
hin
gan
dto
nin
gex
erci
sepr
ogra
m.
n=
120.
Exp
erim
enta
l(ex
p).
n=
60.
Age
:68
yr.
16m
ale,
44fe
mal
e.C
ontr
ol(c
on).
n=
60.A
ge:6
6yr
.24
mal
e,46
fem
ale.
Com
mu
nit
y-dw
ellin
g,se
den
tary
.In
clu
sion
crit
eria
Age
d55
–80
yr,n
ode
men
tia,
hea
lthy
less
than
30m
in.o
fPA
inla
st6
mo.
Bot
hE
XP
and
CO
Ngr
oups
incl
ude
dsa
me
5m
inof
stre
tch
ing,
both
befo
rean
daf
ter
exer
cise
.P
rogr
amla
sted
1ye
ar.
Aer
obic
exer
cise
con
dit
ion
(EX
P)
Pro
gres
sed
from
wal
kin
g10
min
at50
–60%
HR
Rm
axto
40m
inat
60–7
5%H
RR
max
byw
eek
7,th
enm
ain
tain
edu
nti
lpro
gram
fin
ish
ed.
Stre
tch
ing
and
ton
ing
con
trol
con
dit
ion
(CO
N)
4m
usc
leto
nin
gex
erci
ses,
2ba
lan
ceex
erci
ses,
one
yoga
sequ
ence
,an
don
eex
erci
seof
choi
ce.T
old
toex
erci
seat
RP
Eof
13–1
5on
20pt
Bor
gsc
ale.
Ass
essm
ents
VO
2m
axM
RI
for
hip
poca
mpa
lvol
um
e.C
ompu
ter-
base
dsp
atia
lmem
ory
task
.A
nal
ysis
Rep
eate
dm
easu
res
AN
OV
A.
t-te
sts.
EX
Pgr
oup
VO
2m
axin
crea
sed
7.78
%w
hile
CO
Nin
crea
sed
1.11
%.
EX
Pgr
oup
had
sign
ifica
nt
grou
p×
tim
ein
tera
ctio
nfo
rin
crea
sed
hip
poca
mpu
ssi
ze(l
eft
+2.
12%
,ri
ght
+1.
97%
),w
hile
CO
Ngr
oup
decl
ined
(lef
t−1
.4%
,rig
ht−1
.43%
).
Gre
ater
incr
ease
sin
aero
bic
fitn
ess
wer
eas
soci
ated
wit
hgr
eate
rin
crea
sed
inh
ippo
cam
palv
olu
me,
sugg
esti
ng
that
larg
erch
ange
sin
fitn
ess
tran
slat
eto
larg
erch
ange
sin
volu
me.
Hig
her
aero
bic
fitn
ess
leve
lsat
base
line
wer
eas
soci
ated
wit
hbe
tter
spat
ialm
emor
y.A
erob
icex
erci
se-i
ndu
ced
incr
ease
sin
BD
NF
are
sele
ctiv
ely
rela
ted
toth
ech
ange
sin
ante
rior
hip
poca
mpa
lvol
um
e.Lo
ssof
hip
poca
mpa
lvol
um
ein
late
adu
lth
ood
isn
otin
evit
able
and
can
bere
vers
edw
ith
mod
erat
e-in
ten
sity
exer
cise
.
19/2
4

Journal of Aging Research 15
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Cec
elie
tal
.200
9[2
1].
Turk
ey.
Non
-RC
T.Fo
cus
Maj
orm
usc
legr
oups
.
Tode
term
ine
ifpe
rfor
min
gre
gula
rR
OM
exer
cise
sh
ada
ben
efici
aleff
ect
onth
eba
lan
ce,
fun
ctio
nal
acti
vity
,an
dfl
exib
ility
ofel
derl
ysu
bjec
ts.
n=
46.
Age
:73
yr.
3m
ales
,43
fem
ales
.G
rou
p1.
n=
25.
Age
:74±
5.15
yr.
21fe
mal
e;3
mal
es.
Res
th
ome
resi
den
ts.
Gro
up
2(c
ontr
ol).
n=
21.
Age
:72±
4.13
yr.
Fem
ale.
Inpa
tien
tcl
inic
pati
ents
,an
dse
den
tary
hou
sew
ives
.In
clu
sion
crit
eria>
65yr
.A
ble
toam
bula
tew
ith
out
assi
stiv
ede
vice
.In
depe
nde
nt
inac
tivi
ties
ofda
ilyliv
ing.
Pre
-pos
t;4
mon
th.
Inte
rven
tion
Supe
rvis
edR
OM
exer
cise
s.Su
pin
epo
siti
onw
ith
10re
peti
tion
sof
each
upp
eran
dlo
wer
extr
emit
yjo
ints
.3
wk−
1,2
0m
in.
Flex
ibil
ity
Late
ralt
run
kfl
exio
n(r
igh
tan
dle
ft)
dist
ance
betw
een
mid
dle
fin
ger
atre
stan
din
max
late
ralfl
exio
n.
An
teri
ortr
un
kfl
exio
n:d
ista
nce
from
mid
dle
fin
ger
tip
toth
egr
oun
d.B
alan
ceSh
arpe
ned
Rom
berg
(SR
)te
st.
On
e-le
gged
stan
cete
st(O
LST
).B
oth
test
sp
erfo
rmed
wit
hey
esop
enth
encl
osed
.Fu
nct
ion
alac
tivi
ty.
30m
Wal
kin
gT
ime.
Fun
ctio
nal
reac
hte
st.
An
alys
isM
ann
-Wh
itn
eyU
test
.
Sign
ifica
nt
incr
ease
inG
rou
p1
vers
us
2in
left
(10.
76to
13.3
2cm
,P=
0.03
5)an
dri
ght
(10.
47to
12.8
8cm
,P=
0.44
)la
tera
lflex
ion
.No
chan
gein
ante
rior
flex
ion
(8.6
6to
8.24
cm)
30m
wal
kti
me
decr
ease
dsi
gnifi
can
tly
from
28.1
4to
20s
(P=
0.00
1)in
Gro
up
1.Fu
nct
ion
alre
ach
incr
ease
dsi
gnifi
can
tly
from
15.9
5to
19.6
cm(P=.0
14).
No
sign
ifica
nt
diff
eren
cein
bala
nce
test
s.
Au
thor
sst
ated
that
part
icip
atin
gin
daily
flex
ibili
tygr
oup
exer
cise
incr
ease
sR
OM
and
cau
ses
som
eim
prov
emen
tin
bala
nce
.W
hen
com
pare
dto
ara
ndo
mly
sele
cted
hos
pita
lap
plie
dgr
oup,
the
rest
hom
egr
oup
has
bett
erba
lan
ce,
tru
nk
flex
ibili
tyan
dfu
nct
ion
alab
ility
.
11.5
/23

16 Journal of Aging Research
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Ch
rist
ian
sen
2008
[22]
.U
SA.
RC
T.Fo
cus
Hip
san
dan
kles
.
Toex
amin
eth
eeff
ects
ofa
hip
and
ankl
est
atic
stre
tch
ing
prog
ram
onfr
eely
chos
enga
itsp
eed
ofh
ealt
hy,
com
mu
nit
y-dw
ellin
gol
der
peop
len
otac
tive
inex
erci
se.
n=
37.
Age
:72±
4.7
yr.
Inte
rven
tion
Gro
up
.n=
18.A
ge:7
2±
4.7
yr.
3m
ale,
15fe
mal
e.C
ontr
olgr
oup.
n=
19.
Age
:72±
5.0
yr.
5m
ale,
14fe
mal
e.In
depe
nde
ntl
yliv
ing.
Incl
usi
oncr
iter
iaIn
desi
red
age
ran
ge,
hea
lthy
,no
join
tor
mu
scu
losk
elet
alpa
inth
atlim
ited
mov
emen
tin
past
mon
th,n
odi
agn
osed
gait
orba
lan
cedi
sord
er,n
ofa
llsh
isto
ry,h
asn
otpa
rtic
ipat
edin
form
alex
erci
sedu
rin
gth
epr
evio
us
6m
onth
,an
dh
asn
otu
sed
anas
sist
ive
devi
cefo
rw
alki
ng.
Pre
-pos
t8
wee
ks.
Inte
rven
tion
grou
pH
ipan
dan
kle
stre
tch
ing.
2st
atic
stre
tch
esh
eld
for
45se
con
dsan
dre
pea
ted
3ti
mes
alte
rnat
ing
side
s;to
tal9
min
ute
s(5
40s)
/ses
sion
.St
retc
hes
are
stan
din
gca
lfst
retc
han
dst
andi
ng
hip
flex
orst
retc
h.
Con
trol
grou
pE
nsu
red
no
chan
ges
incu
rren
tph
ysic
alac
tivi
ty.
Ass
essm
ents
Pass
ive
RO
M:g
onio
met
ric
mea
sure
men
tsof
hip
(hip
exte
nsi
onba
sed
onT
hom
aste
stpo
siti
on)
and
ankl
e.G
ait:
shoe
son
;tw
ow
alki
ng
spee
ds.
An
alys
isIn
depe
nde
nt
tte
sts
orch
i-sq
uar
ete
sts,
ICC
mod
el2
and
form
1,2-
fact
orre
pea
ted
mea
sure
sA
NO
VA
,sep
arat
ere
pea
ted-
mea
sure
sA
NO
VA
,pa
ired
tte
sts,
and
Bon
ferr
oni
adju
stm
ent.
85%
com
plia
nce
Gai
t:si
gnifi
can
tin
crea
sein
free
ly-c
hos
enga
itsp
eed
for
inte
rven
tion
grou
p(1
.23
to1.
30m
s−1,+
0.7m
s−1,a
nd
P=
0.01
6)ve
rsu
s.co
ntr
ol(n
och
ange
).jo
intm
otio
n:pe
akh
ipex
ten
sion
and
knee
flex
ion
incr
ease
dsi
gnifi
can
tly
(59.
7to
66.5◦ )
inin
terv
enti
ongr
oup,
wit
hn
och
ange
inco
ntr
ol(5
6.2
to56
.1◦ )
.Si
gnifi
can
tin
crea
sein
inte
rven
tion
grou
p(7
.8to
11.3◦ )
for
pass
ive
dors
iflex
ion
,wit
hn
och
ange
inco
ntr
ol.
Oth
er:N
osi
gnifi
can
tch
ange
sin
stri
dele
ngt
hor
join
tan
gula
rdi
spla
cem
ent.
Evid
ence
ispr
ovid
edfr
omth
ere
sult
sth
atjo
int
mot
ion
isa
mod
ifiab
leim
pair
men
tth
atca
nbe
effec
tive
lyta
rget
edfo
rol
der
peo
ple
wit
hsi
mpl
e,st
atic
stre
tch
ing
hom
e-ba
sed
inte
rven
tion
.
19/2
4

Journal of Aging Research 17
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Cri
stop
olis
kiet
al.
2009
[23]
.B
razi
l.R
CT.
Focu
sH
ips
and
ankl
es.
Tode
term
ine
wh
eth
era
4w
ksu
per
vise
dst
retc
hin
gpr
ogra
mfo
rlo
wer
limbs
alte
rsga
itki
nem
atic
sin
aged
popu
lati
on.
n=
28.
Fem
ale.
Exp
erim
enta
lGro
up.
n=
12.
Age
:66±
4.2
y.r
Con
trol
Gro
up.
n=
8.A
ge:6
5±
2.9
yr.
Ch
arac
teri
stic
sC
omm
un
ity
dwel
ling.
Incl
usi
oncr
iter
iaH
ealt
hy,n
oga
itpe
rfor
man
celim
itat
ion
s.
Pre
-pos
t4
wks
.In
terv
enti
onE
xper
imen
talg
rou
p.3
sess
ion
s. wk−
1.
Supe
rvis
ed.
5m
inw
alki
ng
war
m-u
p.H
ipex
ten
sor/
flex
orm
usc
les,
ankl
epl
anta
rfl
exor
mu
scle
s.St
atic
stre
tch
es,6
0s
each
,4ti
mes
.C
ontr
oln
oac
tivi
ty.
Ass
essm
ent
Stat
icR
OM
ofh
ipex
ten
sion
and
flex
ion
and
ankl
edo
rsifl
exio
nby
phot
ogra
phy.
Gai
tp
erfo
rman
ceA
nal
ysis
Rep
eate
dm
easu
res
AN
OV
A,
un
ivar
iate
anal
ysis
,pos
th
ocSc
heff
e.
Stat
icra
nge
ofm
otio
nch
ange
dsi
gnifi
can
tly
(P<
0.05
)in
both
hip
and
ankl
ejo
ints
for
the
expe
rim
enta
lgr
oup,
no
chan
gein
the
con
trol
grou
p.H
ipex
ten
sion
(73
to91
◦ ).
Hip
un
iart
icu
lar
flex
ors
(6.3
to2.
0◦).
Hip
biar
ticu
lar
flex
ors
(7.0
to2.
7◦).
Pla
nta
rfl
exor
ampl
itu
de(3
9to
48◦ )
.E
xper
imen
talg
rou
psh
owed
incr
ease
dst
eple
ngt
h,h
igh
erve
loci
ty,
and
redu
ced
dou
ble
supp
ort
tim
eaf
ter-
trai
nin
g.
Supe
rvis
edst
retc
hin
gpr
ogra
mis
effec
tive
toal
ter
an
um
ber
ofga
itva
riab
les.
Age
dpa
rtic
ipan
tsdi
spla
yed
gait
para
met
ers
wh
ich
wer
esi
mila
rto
thos
eof
you
ng
adu
lts.
17/2
4

18 Journal of Aging Research
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Bat
ista
etal
.200
9[2
4].
Bra
zil.
Exp
erim
enta
l(P
re-p
ost
wit
hin
subj
ects
).Fo
cus
Ham
stri
ngs
.
Tode
term
ine
ifan
acti
vest
retc
hin
gpr
ogra
min
crea
ses
knee
-flex
orto
rqu
ean
dfl
exib
ility
,an
tago
nis
tic
torq
ue,
and
fun
ctio
nal
mob
ility
inol
der
adu
lts,
and
wh
eth
erth
epo
ssib
lead
apta
tion
sre
mai
naf
ter
inte
rven
tion
.
n=
12.
Sex:
fem
ale.
Age
:68±
6.4
yr.
Part
icip
ants
inge
riat
ric
revi
taliz
atio
npr
ogra
mfo
rat
leas
t12
mon
th.
Incl
usi
oncr
iter
ia>
60–8
0yr
s,n
ova
scu
lar,
infl
amm
ator
yor
low
er-l
imb
mu
scu
losk
elet
aldi
sord
ers.
No
un
con
trol
led
hyp
erte
nsi
onFl
exib
ility
defi
cit≥2
0◦.
4w
ksw
ith
out
stre
tch
ing
(A1)
follo
wed
by4
wks
ofst
retc
hin
gin
terv
enti
on(B
),fo
llow
edby
4w
eeks
wit
hou
tst
retc
hin
g(A
2).
Part
icip
ants
wer
eow
nco
ntr
ols
(A1)
.Fl
exib
ilit
yin
terv
enti
on(B
)2
wk−
1;4
wks
.St
andi
ng
infr
ont
ofta
ble,
ther
apis
tal
ign
edsp
ine
wit
hba
r,pa
rtic
ipan
tfl
exed
knee
san
dtr
un
ku
nti
lhan
dsre
ach
edta
ble.
Th
enex
ten
dkn
eean
dti
ltp
elvi
san
teri
orly
tom
axpa
inle
sste
nsi
onH
eld
for
60s,
retu
rned
tost
andi
ng
for
30s.
Rep
eate
d7
tim
es(7×
60=
420
s).
Ass
essm
ents
Kn
eeex
ten
sion
RO
Mde
fici
t(g
onio
met
er).
Isok
inet
icto
rqu
eof
knee
flex
ors
and
exte
nso
rs.
Tim
edU
p-an
d-G
o(T
UG
),fu
nct
ion
alca
paci
ty.
An
alys
isR
epea
ted
one-
way
anal
ysis
ofva
rian
ce.
Stu
den
t’sN
ewm
an-K
euls
test
.
Sign
ifica
nt
decr
ease
inkn
eeex
ten
sion
defi
cit
afte
rin
terv
enti
on(2
4.1◦
to14
.1◦ ,
P=
0.00
01),
but
not
com
plet
ely
mai
nta
ined
afte
r4
wks
(18.
8◦).
TU
Gp
erfo
rman
ceim
prov
ed(8
.4to
7.2
s,P<
0.05
)an
dre
mai
ned
aten
dof
prog
ram
(7.6
s).
Sign
ifica
nt
incr
ease
inco
nce
ntr
ican
dec
cen
tric
torq
ue
ofkn
eefl
exor
san
dex
ten
sors
.
Th
ekn
eefl
exor
stre
tch
ing
prog
ram
was
effec
tive
inin
crea
sin
gth
efl
exib
ility
ofth
ism
usc
legr
oup,
incr
easi
ng
knee
-flex
oran
dex
ten
sor
torq
ue
and
impr
ovin
gfu
nct
ion
alm
obili
tyin
olde
rad
ult
s.M
ost
impr
ovem
ents
last
edat
leas
t4
wks
afte
rth
est
retc
hin
gce
ased
.Th
ein
crea
sein
knee
RO
Mis
prob
ably
are
sult
ofad
apta
tion
inth
eco
nn
ecti
veti
ssu
eca
use
daf
ter
the
knee
-flex
orpr
ogra
m.
13/1
8

Journal of Aging Research 19
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Joh
nso
net
al.2
007
[25]
.U
SA.
Exp
erim
enta
l(P
re-p
ost
wit
hin
subj
ects
).Fo
cus
Cal
ves.
Toin
vest
igat
eth
eeff
ects
ofa
stat
icca
lfM
TU
stre
tch
ing
prog
ram
onan
kle
dors
iflex
ion
RO
Min
hea
lthy
adu
ltw
omen
65ye
ars
and
olde
r.
n=
13.
Age
:84±
4.7
yr.
Fem
ale.
Incl
usi
oncr
iter
ia>
65yr
,hea
lthy
.N
oev
iden
ceof
low
erex
trem
ity
dysf
un
ctio
n(a
sses
sed
byvi
sual
obse
rvat
ion
ofga
it).
Less
than
10◦
ofpa
ssiv
ean
kle
dors
iflex
ion
RO
M.
Fun
ctio
nal
lyin
depe
nde
nt.
Pre
-pos
t,6
wks
.N
oco
ntr
olgr
oup.
Inte
rven
tion
Supe
rvis
edst
retc
hin
gof
left
and
righ
tca
lfm
usc
lete
ndo
nu
nit
(MT
U).
Stan
din
gw
ith
shoe
son
,pla
ced
one
foot
infr
ont
ofot
her
inco
mfo
rtab
lest
eppi
ng
stan
cew
ith
han
dson
chai
r.Le
aned
forw
ard
onfr
ont
leg
un
til
stre
tch
felt
inre
arle
g.H
eld
for
60s
and
rep
eate
d4x
/leg
,on
ceda
ily,5
days
wk−
1fo
r6
wks
.A
sses
smen
tPa
ssiv
ean
kle
dors
iflex
ion
RO
Mby
gon
iom
etry
.M
easu
red
prio
rto
stre
tch
ing
prot
ocol
and
3da
ysaf
ter-
prot
ocol
.Po
stte
stin
gre
sear
cher
blin
dto
pret
esti
ng
data
.A
nal
ysis
Pair
edt-
test
.
Dor
sifl
exio
nR
OM
incr
ease
dsi
gnifi
can
tly
from
−11.
1◦to
1.2◦
(P<
0.00
1).
A6-
wk
stre
tch
ing
prot
ocol
sign
ifica
ntl
yim
prov
edan
kle
dors
iflex
ion
RO
Min
elde
rly
fem
ales
.Th
eR
OM
impr
ovem
ents
wer
em
ain
tain
ed3
days
afte
rth
ela
stda
y.W
ere
able
tode
mon
stra
tea
last
ing,
orpl
asti
cch
ange
inca
lfM
TU
pass
ive
RO
M.
10/1
8
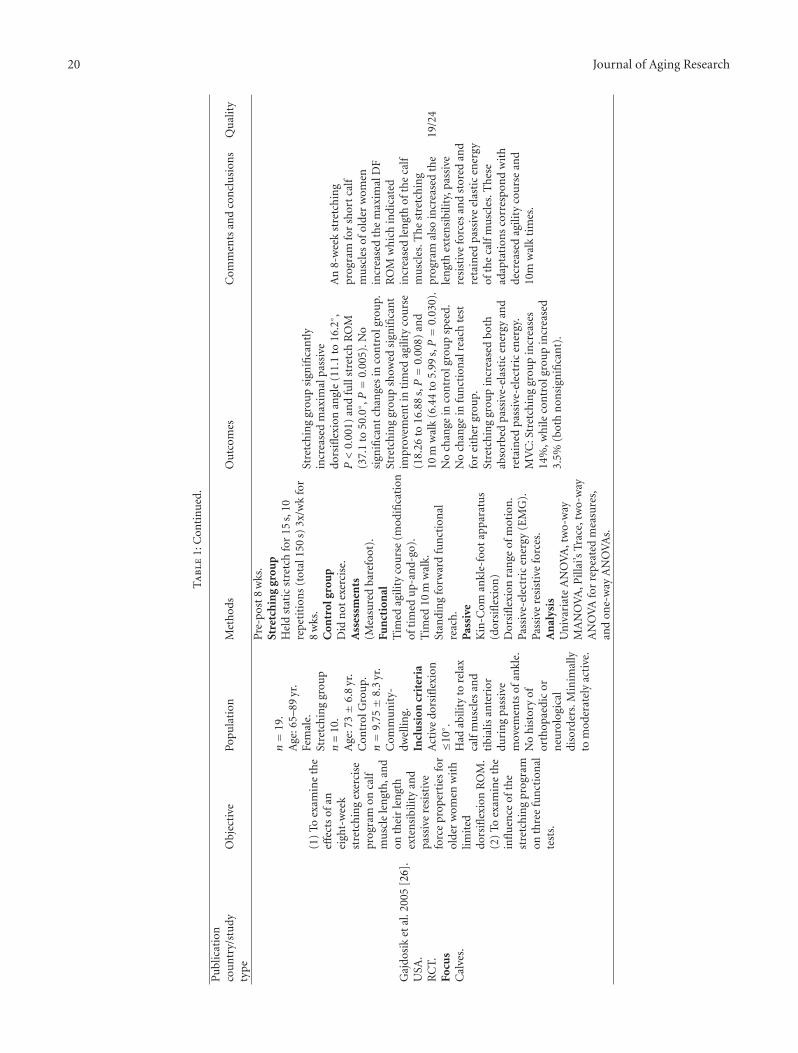
20 Journal of Aging Research
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Gaj
dosi
ket
al.2
005
[26]
.U
SA.
RC
T.Fo
cus
Cal
ves.
(1)
Toex
amin
eth
eeff
ects
ofan
eigh
t-w
eek
stre
tch
ing
exer
cise
prog
ram
onca
lfm
usc
lele
ngt
h,a
nd
onth
eir
len
gth
exte
nsi
bilit
yan
dpa
ssiv
ere
sist
ive
forc
epr
oper
ties
for
olde
rw
omen
wit
hlim
ited
dors
iflex
ion
RO
M.
(2)
Toex
amin
eth
ein
flu
ence
ofth
est
retc
hin
gpr
ogra
mon
thre
efu
nct
ion
alte
sts.
n=
19.
Age
:65–
89yr
.Fe
mal
e.St
retc
hin
ggr
oup
n=
10.
Age
:73±
6.8
yr.
Con
trol
Gro
up.
n=
9.75±
8.3
yr.
Com
mu
nit
y-dw
ellin
g.In
clu
sion
crit
eria
Act
ive
dors
iflex
ion
≤10◦
.H
adab
ility
tore
lax
calf
mu
scle
san
dti
bial
isan
teri
ordu
rin
gpa
ssiv
em
ovem
ents
ofan
kle.
No
his
tory
ofor
thop
aedi
cor
neu
rolo
gica
ldi
sord
ers.
Min
imal
lyto
mod
erat
ely
acti
ve.
Pre
-pos
t8
wks
.St
retc
hin
ggr
oup
Hel
dst
atic
stre
tch
for
15s,
10re
pet
itio
ns
(tot
al15
0s)
3x/w
kfo
r8
wks
.C
ontr
olgr
oup
Did
not
exer
cise
.A
sses
smen
ts(M
easu
red
bare
foot
).Fu
nct
ion
alT
imed
agili
tyco
urs
e(m
odifi
cati
onof
tim
edu
p-an
d-go
).T
imed
10m
wal
k.St
andi
ng
forw
ard
fun
ctio
nal
reac
h.
Pas
sive
Kin
-Com
ankl
e-fo
otap
para
tus
(dor
sifl
exio
n)
Dor
sifl
exio
nra
nge
ofm
otio
n.
Pass
ive-
elec
tric
ener
gy(E
MG
).Pa
ssiv
ere
sist
ive
forc
es.
An
alys
isU
niv
aria
teA
NO
VA
,tw
o-w
ayM
AN
OV
A,P
illai
’sTr
ace,
two-
way
AN
OV
Afo
rre
pea
ted
mea
sure
s,an
don
e-w
ayA
NO
VA
s.
Stre
tch
ing
grou
psi
gnifi
can
tly
incr
ease
dm
axim
alpa
ssiv
edo
rsifl
exio
nan
gle
(11.
1to
16.2◦ ,
P<
0.00
1)an
dfu
llst
retc
hR
OM
(37.
1to
50.0◦ ,P=
0.00
5).N
osi
gnifi
can
tch
ange
sin
con
trol
grou
p.St
retc
hin
ggr
oup
show
edsi
gnifi
can
tim
prov
emen
tin
tim
edag
ility
cou
rse
(18.
26to
16.8
8s,P=
0.00
8)an
d10
mw
alk
(6.4
4to
5.99
s,P=
0.03
0).
No
chan
gein
con
trol
grou
psp
eed.
No
chan
gein
fun
ctio
nal
reac
hte
stfo
rei
ther
grou
p.St
retc
hin
ggr
oup
incr
ease
dbo
thab
sorb
edpa
ssiv
e-el
asti
cen
ergy
and
reta
ined
pass
ive-
elec
tric
ener
gy.
MV
C:S
tret
chin
ggr
oup
incr
ease
s14
%,w
hile
con
trol
grou
pin
crea
sed
3.5%
(bot
hn
onsi
gnifi
can
t).
An
8-w
eek
stre
tch
ing
prog
ram
for
shor
tca
lfm
usc
les
ofol
der
wom
enin
crea
sed
the
max
imal
DF
RO
Mw
hic
hin
dica
ted
incr
ease
dle
ngt
hof
the
calf
mu
scle
s.T
he
stre
tch
ing
prog
ram
also
incr
ease
dth
ele
ngt
hex
ten
sibi
lity,
pass
ive
resi
stiv
efo
rces
and
stor
edan
dre
tain
edpa
ssiv
eel
asti
cen
ergy
ofth
eca
lfm
usc
les.
Th
ese
adap
tati
ons
corr
esp
ond
wit
hde
crea
sed
agili
tyco
urs
ean
d10
mw
alk
tim
es.
19/2
4

Journal of Aging Research 21
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Pett
yet
al.1
999
[27]
.U
SA.
Tim
e-se
ries
,qu
asi-
expe
rim
enta
l.Fo
cus
Cal
ves.
(1)
Toex
amin
eth
ere
lati
onsh
ipbe
twee
nm
axim
um
ankl
edo
rsifl
exio
nR
OM
and
anin
divi
dual
’sab
ility
tom
ove
the
tru
nk
post
erio
rly
wit
hfi
xed
BO
S.(2
)To
exam
ine
inte
rven
tion
desi
gned
toin
crea
sega
stro
cnem
ius
len
gth
onm
axim
alan
kle
DF
RO
Man
dth
eab
ility
tom
ove
post
erio
rly
wit
hfi
xed
BO
S.(3
)To
exam
ine
the
con
trib
uti
ons
ofm
axim
um
ankl
eD
FR
OM
,age
,an
dh
eigh
tto
perf
orm
ance
ofvo
litio
nal
post
erio
rtr
un
km
ovem
ent.
n=
7.82±
4.5
yr.
4m
ale,
3fe
mal
e.Fr
omau
dien
ceat
reti
rem
ent
com
mu
nit
yle
ctu
re.
Exc
lusi
oncr
iter
iaA
nycu
rren
tn
euro
logi
cal
sym
ptom
s,ta
kin
gan
ym
edic
atio
ns
that
mig
ht
affec
tba
lan
ce,
any
visu
alpr
oble
ms
inte
rfer
ing
wit
hda
ilyfu
nct
ion
,sig
nifi
can
tpa
indu
rin
gba
ckw
ard
lean
test
.In
clu
sion
crit
eria
>65
yr,n
ogr
eate
rth
an0◦
ankl
eD
FR
OM
,at
leas
t90
◦of
shou
lder
flex
ion
and
0◦of
elbo
wex
ten
sion
,ab
ility
tost
and
wit
hou
tex
tern
alsu
ppor
tfo
r2
min
and
per
form
Bac
kwar
dLe
anTe
stpr
oper
ly,
and
not
curr
entl
yre
ceiv
ing
phys
ical
ther
apy.
Inte
rven
tion
4w
kst
retc
hin
gpr
ogra
m:
gast
rocs
stre
tch
ing
in“s
tep-
stan
din
g”po
siti
on;p
oin
tof
stre
tch
hel
dfo
r30
sfo
llow
edby
15s
rest
;4re
peti
tion
spe
rbo
dypa
rt,r
epea
ted
twic
ep
erda
y.A
sses
smen
tsM
axim
alan
kle
dors
iflex
ion
(kn
eeex
ten
ded)
.B
ackw
ard
Lean
Test
(bar
efoo
t).
An
alys
isPe
arso
npr
odu
ctm
omen
t.co
rrel
atio
nco
effici
ent.
Pair
edt
test
.M
ult
iple
regr
essi
onan
alys
is.
Mea
npr
etes
tD
FR
OM
:−5.
9◦±
2.5◦
incr
ease
dto
0.5◦±
2.9◦
(sig
nifi
can
tm
ean
chan
geof
6.4◦±
2.2◦
)B
ackw
ard
Lean
pre-
test
:5.2±
3.5
cmin
crea
sed
to9.
3±
3.6
cm(s
ign
ifica
nt
mea
nch
ange
of4.
1±
2.2
cm).
Th
eB
ackw
ard
Lean
test
prov
edu
sefu
lfor
asse
ssin
gch
ange
sin
dyn
amic
post
ura
lco
ntr
olin
apo
ster
ior
dire
ctio
n.
Th
ep
osit
ive
corr
elat
ion
betw
een
max
imal
ankl
eD
FR
OM
and
dist
ance
ofpo
ster
ior
hor
izon
talt
run
kex
curs
ion
duri
ng
Bac
kwar
dLe
anm
aybe
rela
ted
toth
ebi
omec
han
ical
requ
irem
ents
ofth
eB
Lte
st.
Subj
ects
wh
op
erfo
rmed
anex
erci
sepr
ogra
mde
sign
edto
len
gth
enth
ega
stro
csol
eus
mu
scle
sde
mon
stra
ted
incr
ease
dra
nge
ofm
axim
alan
kle
DF
wit
hkn
eeex
ten
ded
and
impr
oved
abili
tyto
lean
back
war
dw
hile
mai
nta
inin
ga
stat
ion
ary
BO
S.T
he
sign
ifica
nt
incr
ease
inD
FR
OM
from
pret
est
topo
stte
stsu
ppor
tsth
eeffi
cacy
ofth
est
retc
hin
gpr
otoc
ol.
Asi
gnifi
can
tre
lati
onsh
ipex
ists
betw
een
the
degr
eeof
avai
labl
em
axim
alan
kle
DF
RO
Mw
ith
the
knee
sex
ten
ded
and
the
hor
izon
tal
dist
ance
anin
divi
dual
isab
leto
mov
eth
etr
un
kpo
ster
iorl
yw
hile
mai
nta
inin
ga
fixe
dB
OS.

22 Journal of Aging Research
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Ker
riga
net
al.2
003
[28]
.U
SA.
Dou
ble-
blin
dR
CT.
Focu
sH
ipfl
exor
s.
Tote
stth
eeff
ect
ofa
hip
flex
orst
retc
hin
gpr
ogra
mon
age-
rela
ted
gait
chan
ges
abou
tth
ean
kle.
n=
96.
Mal
es=
30.
Fem
ales
=66
.Tr
eatm
ent.
n=
47.
15m
ale,
32w
omen
.C
ontr
ol.
n=
49.
15m
en,3
4w
omen
.In
clu
sion
crit
eria
≥65
yrs
old,
hea
lthy
.
Pre
-pos
t10
wks
.P
roto
col
Hom
eex
erci
ses.
Bot
hgr
oups
perf
orm
edw
arm
-up
and
cool
-dow
n;3
0s
stre
tch
esal
tern
atin
glim
bsfo
r4
sets
/8st
retc
hes
into
tal.
2xpe
rda
y(a
ppro
xim
atel
y5
min
).Tr
eatm
entg
rou
pH
ipst
retc
hin
gex
erci
se.
Con
trol
grou
pD
elto
idst
retc
hin
gex
erci
se.
Ass
essm
ent
Stat
ich
ipex
ten
sion
ran
ge,
gon
iom
eter
.Pe
lvic
and
bila
tera
llo
wer
-ext
rem
ity
join
tm
otio
nan
djo
int
kin
emat
ics.
An
alys
isU
npa
ired
and
pair
edt
test
s,pa
ired
Stu
den
tt
test
s,an
dB
onfe
rron
iad
just
men
t.
On
lyp
eak
ankl
edo
rsifl
exio
nan
dpl
anta
rfl
exio
ndu
rin
gsw
ing
incr
ease
dsi
gnifi
can
tly
wit
htr
eatm
ent.
Tren
dfo
rin
crea
sed
inst
atic
peak
hip
exte
nsi
on(6
.1to
7.7◦
,P=
0.32
).N
om
ajor
chan
ges
wit
hco
ntr
olgr
oup.
Bot
hgr
oups
had
sim
ilar
min
orin
crea
ses
inco
mfo
rtab
lew
alki
ng
spee
d.
Ten
den
cyto
war
da
redu
ctio
nin
ante
rior
pelv
icti
ltim
plie
sth
atm
odes
tim
prov
emen
tin
hip
exte
nsi
onra
nge
allo
wed
for
asl
igh
tde
crea
sein
ante
rior
pelv
icti
lt.T
hes
efi
ndi
ngs
supp
ort
the
hypo
thes
isth
atan
incr
ease
inpe
lvic
tilt
inth
eel
derl
yis
aco
mpe
nsa
tion
for
hip
con
trac
ture
rath
erth
ana
com
pen
sati
onor
adi
rect
resu
ltof
anot
her
impa
irm
ent.
Impr
ovem
ent
inp
eak
ankl
epl
anta
rfl
exio
nw
ith
hip
stre
tch
ing
and
atr
end
tow
ard
impr
oved
ankl
epl
anta
rfl
exor
pow
erat
com
fort
able
wal
kin
gsp
eed
wer
efo
un
d.T
hes
ere
sult
ssu
gges
tth
atth
ese
outc
omes
inth
eel
derl
ym
aybe
seco
nda
ryto
prox
imal
impa
irm
ent
rath
erth
anto
impa
irm
ent
atth
ean
kle
oran
kle
mu
scu
latu
rep
erse
.
17/2
4

Journal of Aging Research 23
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Rid
er&
Dal
y19
91[2
9].
USA
.R
CT.
Focu
sTr
un
k.
Tode
term
ine
ifa
flex
ibili
tytr
ain
ing
prog
ram
cou
ldpo
siti
vely
infl
uen
ceth
esp
inal
mob
ility
ofol
der
adu
lts
and
beco
ndu
cted
insu
cha
way
asto
faci
litat
eth
ead
opti
onof
such
apr
ogra
mby
the
part
icip
ants
aspa
rtof
thei
rw
eekl
yex
erci
sero
uti
ne.
n=
20.
Fem
ales
.E
xper
imen
talg
rou
p.n=
10.
Con
trol
grou
p.n=
10.A
ge:m
ean
72yr
.In
clu
sion
crit
eria
No
orth
opae
dic
con
diti
ons
for
exam
ple,
mod
erat
eto
seve
reba
ckpa
in,n
oos
teop
oros
isor
any
spin
alde
con
diti
onin
gdi
sord
ers.
Pre
-pos
t10
wks
.E
xper
imen
talg
rou
pSu
perv
ised
flex
ibili
tyex
erci
ses
(sit
and
reac
h,k
nee
tuck
,pel
vic
lift,
and
back
exte
nsi
on)
3ti
mes
each
,h
eld
for
10s
each
3da
ysw
k−1.
Con
trol
grou
pC
onti
nu
edcu
rren
tex
erci
sepr
ogra
mw
ith
out
flex
ibili
tytr
ain
ing.
Ass
essm
ents
Spin
alfl
exio
n(s
itan
dre
ach
)Sp
inal
exte
nsi
on.
An
alys
isR
epea
ted
mea
sure
sA
NO
VA
.
Exp
erim
enta
lgro
up
show
edsi
gnifi
can
tim
prov
emen
t(P
<0.
05)
pre
topo
stfo
rbo
thsp
inal
flex
ion
(28.
36cm
to32
.57
cm)
and
spin
alex
ten
sion
(17.
87cm
to25
.04
cm).
Th
ere
isa
mea
nin
gfu
lpo
siti
veas
soci
atio
nbe
twee
nre
gula
rfl
exib
ility
trai
nin
gan
dsp
inal
mob
ility
inol
der
popu
lati
onst
udi
esan
dm
ayre
duce
the
pot
enti
alfo
rag
e-re
late
dsp
inal
deco
ndi
tion
ing.
14/2
4

24 Journal of Aging Research
Ta
ble
1:C
onti
nu
ed.
Pu
blic
atio
nco
un
try/
stu
dyty
pe
Obj
ecti
vePo
pula
tion
Met
hod
sO
utc
omes
Com
men
tsan
dco
ncl
usi
ons
Qu
alit
y
Wen
get
al.2
009
[30]
.Ta
iwan
.R
CT
(blin
das
sign
men
t).
Focu
sT
hig
hs.
Toco
mpa
reth
eeff
ects
ofva
riou
sst
retc
hin
gte
chn
iqu
eson
the
outc
omes
ofis
okin
etic
exer
cise
inpa
tien
tsw
ith
knee
oste
oart
hri
tis
(OA
).
n=
132.
n=
33in
each
of4
grou
ps.
Age
:64±
7.5
yr.
Mal
es=
26,F
emal
es=
106.
Incl
usi
oncr
iter
iaB
ilate
rial
mod
erat
ekn
eeO
A(A
ltm
anG
rade
II).
No
hip
join
tO
Aor
any
oth
erh
ippr
oble
ms
wit
hR
OM
limit
atio
ns.
Pre
-pos
t8
wks
.In
terv
enti
onis
okin
etic
exer
cise
3xw
k−1
for
8w
ksat
incr
easi
ng
dose
s.A
ctiv
e-as
sist
edqu
adri
ceps
and
bice
psfe
mor
is,h
oldi
ng
end-
poin
tfo
r30
s,re
pea
t10
x(1
0m
in).
PN
F:H
R(h
old-
rela
x),C
R(c
ontr
act-
rela
x),C
RA
C(c
ontr
act-
rela
xag
onis
tco
ntr
act)
,H
RA
C(h
old-
rela
xag
onis
tco
ntr
act)
.G
rou
p1:
isok
inet
icm
usc
ula
rst
ren
gth
enin
g.G
rou
p2:
bila
tera
lkn
eest
atic
stre
tch
ing
befo
reis
okin
etic
exer
cise
.G
rou
p3:
PN
Fbe
fore
isok
inet
icex
erci
se.
Gro
up
4(c
ontr
ol):
war
m-u
pon
ly.
All
grou
psre
ceiv
ed10
min
(15
min
inco
ntr
ol)
hot
pack
san
dpa
ssiv
eR
OM
onst
atio
nar
ybi
ke.
Ass
essm
ent
RO
M:g
onio
met
erch
ange
sin
knee
acti
veas
sist
edR
OM
(flex
ion
and
exte
nsi
on).
Pain
:VA
Ssc
ale.
Dis
abili
ty:L
equ
esn
e’s
inde
x(L
I).
MP
T:fl
exio
nan
dex
ten
sion
wit
his
okin
etic
dyn
amom
eter
An
alys
isW
eigh
ted
kapp
ast
atis
tics
,Pai
red
tte
sts,
one-
way
AN
OV
Aw
ith
Tuke
y’s
test
,an
dD
un
net
t’ste
st.
n=
124.
Follo
w-u
pn=
111.
RO
M:s
ign
ifica
ntl
yin
crea
sed
ingr
oups
IIan
dII
I.Pa
in:d
ecre
ased
sign
ifica
ntl
yin
all
grou
ps,b
ut
incr
ease
din
con
trol
.G
reat
erde
crea
ses
inII
and
grea
test
inII
I.D
isab
ility
:ave
rage
LIsc
ores
decr
ease
dsi
gnifi
can
tly
inal
lgro
ups
,gr
eate
stin
III.
MP
T:a
vera
geat
60◦ /
seco
nd
incr
ease
dsi
gnifi
can
tly
inal
lm
easu
rem
ents
for
grou
psII
and
III.
All
grou
psin
crea
sed
sign
ifica
ntl
ym
ore
than
con
trol
.
Stre
tch
ing
ther
apy
isre
com
men
ded
asan
adju
van
ttr
eatm
ent
tois
okin
etic
exer
cise
for
pati
ents
wit
hkn
eeO
A.
PN
Fis
mor
eeff
ecti
veth
anst
atic
stre
tch
ing
exer
cise
.
13/2
4
Yr:
year
;hr:
hou
r;w
k:w
eek;
wks
:wee
ks;m
in:m
inu
tes;
s:se
con
ds;m
:met
ers;
RO
M:r
ange
ofm
otio
n;x
:tim
es;m
o:m
onth
s;pt
:poi
nt;
HR
R:h
eart
rate
rese
rve;
cm:c
enti
met
ers.

Journal of Aging Research 25
Electronic database search
Level 1 screening: title
Level 2 screening: title
Level 3 screening: full text
Final full text articles
10: not original article69: no intervention studied280: no flexibility intervention
5: subjects not healthy1: study not in english
32: flexibility not focus of intervention or control protocol6: no flexibility intervention2: not original article
Hand searching of referencesRelevant database articles
4: single-session studies
and abstract
n = 4037
n = 4037
n = 436
n = 62
n = 18
n = 22
n = 4
Excluded or duplicates (n = 3601)
Excluded (n = 374)
9: subjects not >65 yr
Excluded (n = 44)
+
Figure 1: Article Screening Flow Chart.
[23, 24], Turkey [21], Australia [9, 16], Taiwan [30], andCanada [13].
3.2. Population. The mean sample age was 74.1 years,ranging from 64 years [30] to 88.8 years [14]. Seven studiesincluded populations that were ≥80 years of age [10, 11, 13,14, 18, 25, 27]. The number of participants in the articlesof this paper ranged from 7 [27] to 132 [30]. There were atotal of 1127 participants, 841 of whom were female (75%),while 286 were male. Six studies were female only [15, 23–26, 29]. Twenty studies were based on community-dwellingpopulations, and two studies involved individuals residing inassisted-living facilities [10, 13].
3.3. Outcome Measures. Outcomes were measured usingflexibility measurements, physical ability tests, and question-naires. One study also used brain imaging for the purposesof identifying changes in hippocampal volume with training[20]. A common outcome measure was simply whetherthere was a change in range of motion usually assessed bygoniometry [15, 17, 20, 24–28, 30]. The inclusion of thesestudies in the review (although they reported no “functionaloutcome”) was to provide the data for the purpose ofdetermining whether older adults would, in fact, improverange of motion about different joints with various flexibilityexercise programs. Functional outcomes were operationallydefined as tests or measures designed to reflect abilities forvarious levels of daily activities and potentially related tomaintenance of independence of older adults. In general,
these tests assessed ability in a function that involved morethan a single fitness component (e.g., not just a strengthmeasure of a weight that could be lifted, but rather aperformance that may involve strength and power as wellas balance and agility). The most commonly used tests offunctional outcome were gait and various walking speeds[11, 13, 14, 19, 21, 22, 26], the sit-and-reach test [10, 12–14,19, 29], the sit-to-stand test [9, 12, 14, 16, 18, 19], functionalreach test [9, 10, 21, 26], step test [9, 16], timed up-and-go(TUG) [10, 13, 14, 16, 19, 24, 26], and Romberg test [11,21]. Other functional outcome measures were Berg balancescale [13], questionnaires [9, 12], peg board [11], red-light-green-light [11], Lequesne’s index of disability [30], thephysical performance test (PPT) [11], and the gallon jugshelf test [14]. Gait and walking speed proved to be morepositively affected by flexibility training than other outcomemeasures [14, 19, 21, 22, 26], although this was not entirelyconsistent [11, 13]. Several studies showed increases inflexibility-related outcomes, but lacked significant changes inother more applicable and generic measures of functionality.Only one study followed up on outcome maintenance afterthe postintervention measurements. This study found thatknee torque and timed up-and-go showed improvementscompared to the control group, which persisted for fourweeks after intervention [24].
In the sub-group containing eight studies of the very old(≥80 years), frail, and assisted-living populations [10, 11, 13,14, 18, 21, 25, 27], there were significant improvements seenin functional reach [21], sit-to-stand [10, 14] and 30 m walktimes [21], but no changes in the PPT [11] and mixed resultsfor flexibility, strength, balance, and TUG tests. As comparedto studies on less aged independently-living populations,the outcomes results of this sub-group were similar, exceptthat the more aged/dependent group had less consistentflexibility outcomes; there were some neutral outcomes andsome negative changes following flexibility training.
Six out of the 22 studies included several functionaloutcome measures and were considered most relevant tothis paper [11–14, 16, 19], and are individually reviewedherein. Four of the six conducted randomized control trials(RCT) [11–14], and only two studies reported sample sizesless than 68 participants. Brown et al. [11] conducted a 12-week RCT (n = 87), wherein the flexibility trained groupdemonstrated only flexibility measure improvements and nochange in functional outcomes. The measures included werevery practical and included the chair stand, picking up apenny, putting on and taking off a coat, and the Rombergbalance test. However, it should be noted that this studyalso showed minor strength and balance losses. In a oneyear RCT, King et al. [12], similarly, showed no change inmost functional outcomes in the flexibility trained group.Functional measures included lift-and-reach, sit-to-stand,sit-and-reach, self-rated physical performance, self-efficacyfor physical performance scale, and perceived functioningand well-being. There were only significant increases for thesit-and-reach test in men only (10.4 to 11.9 inches) anddecreases in self-rated daily bodily pain scores (by 7.3% forwomen and 9.4% for men). Lazowski et al. [13] conducted

26 Journal of Aging Research
a 16-week RCT (n = 68). Timed up-and-go increased(worsened) from 27 to 33 seconds, and no changes wereseen in any other functional measures or in the sit-and-reach test. Additional functional measures included strengthtests, Berg balance scale, self-paced and fast-paced walk tests,stair-climbing, and the functional independence measurefor functional capacity. Stanziano et al. [14] employed an8-week RCT (n = 17), where the experimental flexibilitygroup significantly improved in every measure: chair standrepetitions (11 to 13), modified ramp power (69 W to 86 W),arm curl repetitions (12.9 to 18.8), gallon jug shelf test(13.4 to 11.5 seconds), 8 foot timed up-and-go (8.7 to 7.6seconds), and 50 foot gait speed (13.9 to 12.3 seconds). Thestudy by Bird et al. [16] was a 32-week randomized cross-over design (n = 32) with 16 weeks spent in the flexibilitygroup. Four functional outcomes improved significantly forthe flexibility group: TUG (7.6 to 6.6 seconds), sit-to-stand(22.6 to 18.0 seconds), step test (13.5 to 17.6 steps), andmediolateral sway range (eyes open: 4.16 to 2.97 cm; eyesclosed: 6.87 to 5.64 cm). Strength was also tested, with noimprovement by the flexibility group. In a 12-week non-RCT(n = 117), Takeshima et al. [19] reported no improvementsfor the flexibility trained group in the 12-minute walk, armcurls, chair stand, TUG, functional reach, back scratch, andsit-and-reach. These six studies exemplify the mixed resultsof the functional outcome measures in this paper. Theyserve as a strong representation of the lack of consistencyof functional outcomes in the literature and therefore, anyspecific recommendation regarding type or frequency ofstretching exercises is premature.
Overall, seven of 22 studies demonstrated mostly positivefunctional outcomes [9, 10, 14, 16, 21, 23, 29], whilesix reported mostly negative functional results, that is, noimprovement in variables [11–13, 18, 19, 22]. Ten studiesshowed no functional outcome measures [15, 17, 20, 24–30]and only reported changes in flexibility and ROM (althoughthey purported to relate flexibility to function, and wereincluded for their results related to the ability of older adultsto improve flexibility). There were no obvious differencesbetween the characteristics of the studies with positive,negative, or no functional outcomes.
3.4. Intervention Characteristics. Twelve studies used flexibil-ity training as the sole intervention [10, 11, 14, 17, 21–27,29], four studies used flexibility training as a significant partof an intervention protocol [15, 16, 19, 30], five studies usedflexibility as a control group to compare with various otherexercise interventions [9, 11–13, 18, 20], and four studiesutilized flexibility exercises along with strength or aerobicexercise in the intervention protocol but in the controlgroup, the entire exercise protocol was flexibility exercises[9, 11, 13, 20]. The types of flexibility training methodsvaried from simple static stretches (19 studies) to differentproprioceptive neuromuscular facilitation (PNF) techniques(1 study). Passive static stretching was the most commonmethod used [9, 11–13, 16, 18–29], while passive staticstretching with added weights was used once [17], active-assisted (AA) was used twice [14, 30], active and passive
were used in conjunction once [15], contract-relax (CR)PNF was used once [30], contract-relax-agonist contract(CRAC) PNF was used once [30], and hold-relax-agonistcontract (HRAC) PNF was used once as well [30]. One studycompared multiple methods with each other [30]. Active-assisted stretching had positive and sometimes significantimprovements in several outcome measures as comparedto the inactive control group, but less significant than theimprovements seen with the PNF techniques [30]. Weightedflexibility exercises were similar to nonweighted exercises inone study [15], but significantly better than nonweightedexercises in another [17].
Thirteen studies involved whole body flexibility training[9–21], two focused on hips and calves [22, 23], one focusedon hamstrings [24], three focused on calves [25–27], onefocused on hip flexors [28], one focused on the trunk[29], and one study focused on the quadriceps muscles[30]. Whole body flexibility training showed some minor tosignificant increases in outcomes; however, most increaseswere seen in ROM and flexibility measures, per se, andnot in other functional outcome measures. These resultswere consistent with the overall effects of specific isolatedstretching interventions on outcome measures for the relatedspecific body parts.
The mean length of the included studies was 14.2 weeks,ranging from 4 weeks to one year [12, 20]. Results didnot differ significantly throughout the range of interventiondurations. In the three studies of at least 25 weeks in duration[12, 15, 20], no functional outcome measures were improvedother than flexibility and ROM. In the four studies withdurations of 6 weeks or less [23–25, 27] TUG improvedfrom 8.4 to 7.2 seconds [24], walking velocity increased 1.07to 1.22 m/s [23], and flexibility and ROM were improvedoverall.
The mean frequency was 4-exercise sessions per week,ranging from the lowest frequency of twice per week [9, 10,12, 22, 24] to 14x/week [27, 28]. Two studies did not reportexercise frequency [20, 22]. Some results from these studiesinclude a TUG time decrease from 8.4 to 7.2 seconds [24] anda no-change [10], sit-to-stand time decreased from 10.2 to9.2 seconds [9] and 9.3 to 7.9 seconds [10] and a no-change[12], a step test increased in reps from 16.5 to 20.2 [9], andan increase in freely chosen gait speed from 1.23 to 1.30 m/s[22]. The 5x/week and 14x/week studies did not includefunctional outcomes similar to the twice weekly studies. The3x/week studies included results such as an improved TUGtime from 7.6 to 6.6 seconds [16] and a worsening time from26.8 to 33.0 seconds [13], a functional reach improvementof 16.0 to 19.6 cm [21] and two no-changes [19, 26], a sit-to-stand improvement of 22.6 to 18.0 seconds [16], a steptest improvement of 13.5 to 17.6 repetitions [16], a 10 mwalk time improvement from 6.44 to 5.99 seconds [26], anda 30 m walk time improvement from 28.1 to 20.0 seconds[21]. Although limited in number, these results show thatthe frequency of the flexibility training interventions had nonoticeable differences compare with 2 and 3 times per week.
The mean flexibility exercise session time was 32 minutes,ranging from 30 seconds [29] to 85 minutes [19].

Journal of Aging Research 27
4. Discussion
There are currently scientific discussions regarding the utilityof stretching exercises which are regularly recommended andconducted as a part of preexercise protocols to reduce injuryand increase performance. Earlier reviews of stretching andflexibility have questioned their value in terms of injury pre-vention, delayed onset of muscle soreness, and improvementof performance [31, 32]. In fact, what occurs physiologicallywith stretching remains unknown [32]. Due to equivocalevidence thus far, the current American College of SportsMedicine’s guidelines for exercise testing and prescription[33] recommended the removal of static stretching as partof a warm-up routine for strength and power activities.Additionally, based on available evidence, the 2011 ACSMposition statement for guidance on prescribing exercise sug-gests performing flexibility after cardiorespiratory enduranceor resistance exercise for general fitness programs. Thisposition stand highlighted the need for further researchto ascertain the effects of various flexibility prescriptionsfor various activities and performance goals. From thepresent review, there is not enough consistent evidence tomake recommendations for any specific prescriptions oftype, frequency, duration, or length of program related toflexibility training; particularly no specific recommendationscan be made regarding the program or dose response offlexibility training to the focus of the present study, thetransfer of flexibility gains to functions of daily life, orability to live independently. A recent systematic review of106 articles relating the effects of pre-exercise acute-passivestatic stretching on maximal muscle performance provided74 methodologically sound studies providing 104 findings[34]. This paper showed that 50% of the 104 findingsreported significant reductions in task performances, andthe authors concluded that static muscle stretches totalingless than 45 s can be used in pre-exercise protocols withoutsignificant decrement to strength, power or speed type tasks;thus a conclusion was to recommend stretches held for atmaximum 45 s to avoid loss of strength. Shrier [35] hadalso previously reported the potential negative acute effectsof stretching on performance, but additionally reviewed theliterature regarding regular stretching on performance whichindicates that regular stretching improves force, jump height,and speed performance. Both reviews recommend furthersynthesis of the literature with respect to the effects of otherforms of stretching on various performance measures.
The difficulties of the ability of this paper to providea consensus on flexibility training prescription for healthyolder adults include the lack of well-conducted studiesfocused on flexibility in older adults and the lack ofconsistency in the flexibility protocols employed, functionaloutcomes measured, and functional results observed. Assuch, according to the criteria used to assess level of evidence,to recommend stretching/flexibility exercises as a routinecomponent of an exercise program for older adults toenhance health or functional abilities is Level 4, GradeC. The more influential studies in this paper (based onfocused flexibility protocols with clear functional outcomesand relatively large sample sizes) [11–14, 16, 19] showed very
comparable effects to the overall outcomes of the 26 studies,namely, an ambivalence in the value of flexibility training onfunctional outcomes that may be related to maintenance ofindependence in daily activities of older adults. Of these sixstudies, 5 were RCTs with an average quality assessment scoreof 18 out of 24. Only two of the six showed improvement inflexibility and functional outcomes ([14] 16/24; [16] 19/24).
In the sub-group (≥80 years), frail, and assisted-livingpopulations there were significant improvements seen infunctional reach, sit-to-stand, and 30 m walk times, butno changes in the PPT, and mixed results were observedfor flexibility, strength, balance, and TUG tests. This sub-group was similarly ambivalent in the role of flexibilitytraining with functional outcomes to the rest of the studypopulations, although this group had less consistency inthe flexibility-related outcome measures. Frequency andduration differences between studies showed no noticeabledifferences in outcomes. When different muscle groupswere targeted, the flexibility outcomes were expectedly fairlybody-part specific. Regarding the different flexibility trainingmethods, active-assisted (AA) stretching had positive andsometimes significant improvements in several outcomemeasures as compared to the inactive control group, butless significant than the improvements seen with the PNFtechniques. Weighted flexibility exercises were similar tononweighted exercises in one study, but significantly betterthan nonweighted exercises in another. One study showedACR-PNF to be much more effective than CR-PNF and staticstretching for both ROM and EMG activity. The overallresults point to PNF stretching being more effective thannon-PNF techniques for improving flexibility outcomes, butnot necessarily functional outcome measures.
While flexibility training interventions synthesized inthe present paper have been shown to increase flexibilityand joint ROM, no consistent increases in functional out-comes have been observed. Therefore, future studies shouldconsider the relationship that increased flexibility and jointROM have with functional outcomes to determine if theincreased flexibility is beneficial and worthwhile in termsof maintaining or increasing functional capacity for healthyolder adults. More research is also needed regarding the rela-tionships between outcome variables (i.e., how one variablesuch as functional reach would relate to another variable suchas the timed up-and-go) and on the relationships betweenoutcome measures and quality of life through self-reportedfunctioning/quality of life questionnaires to best determinethe applicability of the outcome measures.
Older adults are less concerned with high performancebenefits from increased flexibility and more focused on beingsafely active and safely performing activities of daily living[36]. Injury and fall prevention are also common motivesfor recommending flexibility programs to older adults.The 2011 ACSM position statement notes that flexibilitytraining may enhance postural stability and balance whencombined with resistance training; however, no consistentlink has been shown between regular flexibility exercise anda reduction of musculoskeletal injuries or delayed onset ofmuscle soreness [4]. However, despite the growing literaturedescribing the relationship of flexibility to injury risk in
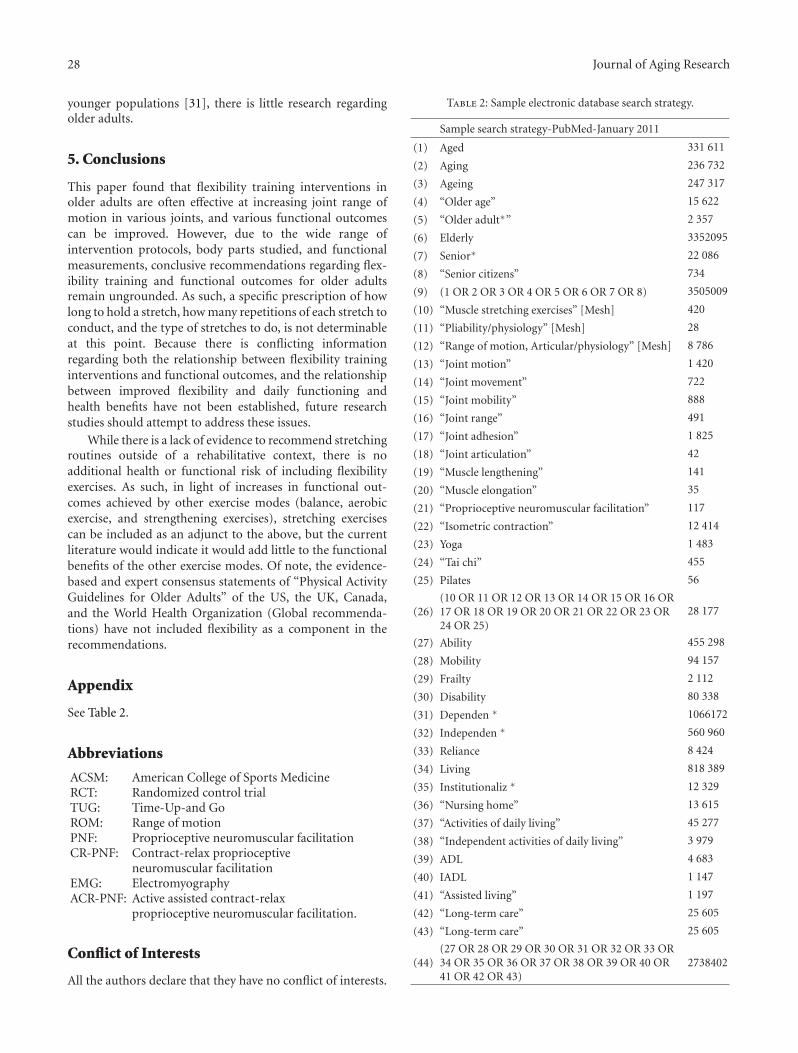
28 Journal of Aging Research
younger populations [31], there is little research regardingolder adults.
5. Conclusions
This paper found that flexibility training interventions inolder adults are often effective at increasing joint range ofmotion in various joints, and various functional outcomescan be improved. However, due to the wide range ofintervention protocols, body parts studied, and functionalmeasurements, conclusive recommendations regarding flex-ibility training and functional outcomes for older adultsremain ungrounded. As such, a specific prescription of howlong to hold a stretch, how many repetitions of each stretch toconduct, and the type of stretches to do, is not determinableat this point. Because there is conflicting informationregarding both the relationship between flexibility traininginterventions and functional outcomes, and the relationshipbetween improved flexibility and daily functioning andhealth benefits have not been established, future researchstudies should attempt to address these issues.
While there is a lack of evidence to recommend stretchingroutines outside of a rehabilitative context, there is noadditional health or functional risk of including flexibilityexercises. As such, in light of increases in functional out-comes achieved by other exercise modes (balance, aerobicexercise, and strengthening exercises), stretching exercisescan be included as an adjunct to the above, but the currentliterature would indicate it would add little to the functionalbenefits of the other exercise modes. Of note, the evidence-based and expert consensus statements of “Physical ActivityGuidelines for Older Adults” of the US, the UK, Canada,and the World Health Organization (Global recommenda-tions) have not included flexibility as a component in therecommendations.
Appendix
See Table 2.
Abbreviations
ACSM: American College of Sports MedicineRCT: Randomized control trialTUG: Time-Up-and GoROM: Range of motionPNF: Proprioceptive neuromuscular facilitationCR-PNF: Contract-relax proprioceptive
neuromuscular facilitationEMG: ElectromyographyACR-PNF: Active assisted contract-relax
proprioceptive neuromuscular facilitation.
Conflict of Interests
All the authors declare that they have no conflict of interests.
Table 2: Sample electronic database search strategy.
Sample search strategy-PubMed-January 2011
(1) Aged 331 611
(2) Aging 236 732
(3) Ageing 247 317
(4) “Older age” 15 622
(5) “Older adult∗” 2 357
(6) Elderly 3352095
(7) Senior∗ 22 086
(8) “Senior citizens” 734
(9) (1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8) 3505009
(10) “Muscle stretching exercises” [Mesh] 420
(11) “Pliability/physiology” [Mesh] 28
(12) “Range of motion, Articular/physiology” [Mesh] 8 786
(13) “Joint motion” 1 420
(14) “Joint movement” 722
(15) “Joint mobility” 888
(16) “Joint range” 491
(17) “Joint adhesion” 1 825
(18) “Joint articulation” 42
(19) “Muscle lengthening” 141
(20) “Muscle elongation” 35
(21) “Proprioceptive neuromuscular facilitation” 117
(22) “Isometric contraction” 12 414
(23) Yoga 1 483
(24) “Tai chi” 455
(25) Pilates 56
(26)(10 OR 11 OR 12 OR 13 OR 14 OR 15 OR 16 OR17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR24 OR 25)
28 177
(27) Ability 455 298
(28) Mobility 94 157
(29) Frailty 2 112
(30) Disability 80 338
(31) Dependen ∗ 1066172
(32) Independen ∗ 560 960
(33) Reliance 8 424
(34) Living 818 389
(35) Institutionaliz ∗ 12 329
(36) “Nursing home” 13 615
(37) “Activities of daily living” 45 277
(38) “Independent activities of daily living” 3 979
(39) ADL 4 683
(40) IADL 1 147
(41) “Assisted living” 1 197
(42) “Long-term care” 25 605
(43) “Long-term care” 25 605
(44)(27 OR 28 OR 29 OR 30 OR 31 OR 32 OR 33 OR34 OR 35 OR 36 OR 37 OR 38 OR 39 OR 40 OR41 OR 42 OR 43)
2738402

Journal of Aging Research 29
Table 2: Continued.
Sample search strategy-PubMed-January 2011
(45) Control 2295628
(46) Treatment 6813000
(47) Modality 165 777
(48) Adjunct 25 544
(49) Component 289 484
(50) Group 1741947
(51) Subset 76 495
(52) Subset 446
(53) Subgroup 55 099
(54) Subgroup 2 358
(55) “Exercise” [Mesh] 52 144
(56) “Exercise prescription” 772
(57) “Exercise program∗” 3 376
(58) “Exercise treatment” 240
(59) “Exercise therapy” 20 527
(60) Activity 1731305
(61) “Physical activity” 37 516
(62) “Physical therapy” 38 673
(63) “Fitness program∗” 277
(64) Dance 2 274
(65) “Rhythmic exercise” 86
(66)(45 OR 46 OR 47 OR 48 OR 49 OR 50 OR 51 OR52 OR 53 OR 54 OR 55 OR 56 OR 57 OR 58 OR59 OR 60 OR 61 OR 62 OR 63 OR 64 OR 65)
9 702261
(67) (9 AND 26 AND 44 AND 66) 2 401(67 NOT child NOT children NOT cognit∗ NOT“alzheimer disease”
434
NOT depression NOT anxiety NOT post-surg∗
NOT postsurg∗
NOT surgery NOT surgical NOT cardiac NOTfracture∗ NOT arthroplasty
(68)NOT diabetes NOT diabetic NOT cancer NOTstroke NOT Parkinson∗
NOT “multiple sclerosis” NOT sclerosis NOTstenosis NOT memoryNOT mental NOT coronary NOT cerebral NOTdystrophy NOT polio
NOT fibromyalgia)
Authors’ Contributions
All authors have made substantial contributions to theconception and design of the present systematic review.L. Stathokostas coordinated the conduct of the systematicreview. L. Stathokostas and R. M. D. Little were involvedin the acquisition and analysis of data. All authors wereresponsible for the interpretation of data. All authors havebeen involved in drafting the paper. All authors read andapproved the final manuscript for publication.
Disclosure
D. H. P. Paterson is the research director of the Cana-dian Centre for Activity and Aging and is responsible for
evidence-based development of exercise programs for olderadults. Recently, DH was a coauthor of a systematic reviewwhich resulted in the modification and update of Canada’sPhysical Activity Guidelines for Older Adults submitted toIJBNPA in 2010. This paper showed that exercise inter-ventions in older adults are effective in maintaining orimproving functional abilities. However, it was identified thatless is known about the role of flexibility in the maintenanceor improvement of functional abilities. As such, the presentpaper was undertaken.
Acknowledgment
The authors gratefully acknowledge the assistance of MarisaSurmacz, Health Sciences librarian, University of WesternOntario.
References
[1] D. H. Paterson and D. E. R. Warburton, “Physical activityand functional limitations in older adults: a systematic reviewrelated to Canada’s Physical Activity Guidelines,” InternationalJournal of Behavioral Nutrition and Physical Activity, vol. 7,article 38, 2010.
[2] W. J. Chodzko-Zajko, D. N. Proctor, M. A. Fiatarone Singh etal., “Exercise and physical activity for older adults,” Medicineand Science in Sports and Exercise, vol. 41, no. 7, pp. 1510–1530, 2009.
[3] K. P. Speer, Injury Prevention and Rehabilitation for ActiveOlder Adults, Human Kinetics, Champaign, Ill, USA, 2005.
[4] C. E. Garber, B. Blissmer, M. R. Deschenes et al., “Quantityand quality of exercise for developing and maintainingcardiorespiratory, musculoskeletal, and neuromotor fitness inapparently healthy adults: guidance for prescribing exercise,”Medicine and Science in Sports and Exercise, vol. 43, no. 7, pp.1334–1359, 2011.
[5] U.S. Department of Health and Human Services. 2008 PhysicalActivity Guidelines for Americans. 29–34. 2008.
[6] D. C. Lau, J. D. Douketis, K. M. Morrison, I. M. Hramiak,A. M. Sharma, and E. Ur, “2006 Canadian clinical practiceguidelines on the management and prevention of obesity inadults and children,” Canadian Medical Association Journal,vol. 176, no. 8, pp. S1–S13, 2007.
[7] S. H. Downs and N. Black, “The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions,” Journal of Epidemiology and CommunityHealth, vol. 52, no. 6, pp. 377–384, 1998.
[8] S. C. Gorber, M. Tremblay, D. Moher, and B. Gorber, “Acomparison of direct versus self-report measures for assessingheight, weight and body mass index: a systematic review,”Obesity Reviews, vol. 8, no. 4, pp. 307–326, 2007.
[9] C. Barrett and P. Smerdely, “A comparison of community-based resistance exercise and flexibility exercise for seniors,”Australian Journal of Physiotherapy, vol. 48, no. 3, pp. 215–219,2002.
[10] D. A. Klein, W. J. Stone, W. T. Phillips, J. Gangi, and S.Hartman, “PNF training and physical function in assisted-living older adults,” Journal of Aging and Physical Activity, vol.10, no. 4, pp. 476–488, 2002.
[11] M. Brown, D. R. Sinacore, A. A. Ehsani, E. F. Binder, J.O. Holloszy, and W. M. Kohrt, “Low-intensity exercise as a
30 Journal of Aging Research
modifier of physical frailty in older adults,” Archives of PhysicalMedicine and Rehabilitation, vol. 81, no. 7, pp. 960–965, 2000.
[12] A. C. King, L. A. Pruitt, W. Phillips, R. Oka, A. Rodenburg, andW. L. Haskell, “Comparative effects of two physical activityprograms on measured and perceived physical functioningand other health-related quality of life outcomes in olderadults,” Journals of Gerontology Series A, vol. 55, no. 2, pp.M74–M83, 2000.
[13] D. A. Lazowski, N. A. Ecclestone, A. M. Myers et al., “Arandomized outcome evaluation of group exercise programsin long-term care institutions,” Journals of Gerontology SeriesA, vol. 54, no. 12, pp. M621–M628, 1999.
[14] D. C. Stanziano, B. A. Roos, A. C. Perry, S. Lai, and J. F.Signorile, “The effects of an active-assisted stretching programon functional performance in elderly persons: a pilot study,”Clinical Interventions in Aging, vol. 4, no. 1, pp. 115–120, 2009.
[15] D. M. Raab, J. C. Agre, M. McAdam, and E. L. Smith,“Light resistance and stretching exercise in elderly women:effect upon flexibility,” Archives of Physical Medicine andRehabilitation, vol. 69, no. 4, pp. 268–272, 1988.
[16] M. L. Bird, K. Hill, M. Ball, and A. D. Williams, “Effectsof resistance- and flexibility-exercise interventions on balanceand related measures in older adults,” Journal of Aging andPhysical Activity, vol. 17, no. 4, pp. 444–454, 2009.
[17] A. M. Swank, D. C. Funk, M. P. Durham, and S. Roberts,“Adding weights to stretching exercise increases passive rangeof motion for healthy elderly,” The Journal of Strength andConditioning Research, vol. 17, no. 2, pp. 374–378, 2003.
[18] N. B. Alexander, M. M. Gross, J. L. Medell, and M. R.Hofmeyer, “Effects of functional ability and training on chair-rise biomechanics in older adults,” Journals of GerontologySeries A, vol. 56, no. 9, pp. M538–M547, 2001.
[19] N. Takeshima, N. L. Rogers, M. E. Rogers, M. M. Islam, D.Koizumi, and S. Lee, “Functional fitness gain varies in olderadults depending on exercise mode,” Medicine and Science inSports and Exercise, vol. 39, no. 11, pp. 2036–2043, 2007.
[20] K. I. Erickson, M. W. Voss, R. S. Prakash et al., “Exercise train-ing increases size of hippocampus and improves memory,”Proceedings of the National Academy of Sciences of the UnitedStates of America, vol. 108, no. 7, pp. 3017–3022, 2011.
[21] E. Ceceli, F. Gokoglu, M. Koybasi, O. Cicek, and Z. R.Yorgancioglu, “The comparison of balance, functional activity,and flexibility between active and sedentary elderly,” Topics inGeriatric Rehabilitation, vol. 25, no. 3, pp. 198–202, 2009.
[22] C. L. Christiansen, “The effects of hip and ankle stretching ongait function of older people,” Archives of Physical Medicineand Rehabilitation, vol. 89, no. 8, pp. 1421–1428, 2008.
[23] F. Cristopoliski, J. A. Barela, N. Leite, N. E. Fowler, and A. L.F. Rodacki, “Stretching exercise program improves gait in theelderly,” Gerontology, vol. 55, no. 6, pp. 614–620, 2009.
[24] L. H. Batista, A. C. Vilar, J. J. De Almeida Ferreira, J. R.Rebelatto, and T. F. Salvini, “Active stretching improves flex-ibility, joint torque, and functional mobility in older women,”American Journal of Physical Medicine and Rehabilitation, vol.88, no. 10, pp. 815–822, 2009.
[25] E. G. Johnson, B. D. Bradley, K. R. Witkowski et al., “Effectof a static calf muscle-tendon unit stretching program onankle dorsiflexion range of motion of older women,” Journalof Geriatric Physical Therapy, vol. 30, no. 2, pp. 49–52, 2007.
[26] R. L. Gajdosik, D. W. Vander Linden, P. J. McNair, A. K.Williams, and T. J. Riggin, “Effects of an eight-week stretchingprogram on the passive-elastic properties and function of thecalf muscles of older women,” Clinical Biomechanics, vol. 20,no. 9, pp. 973–983, 2005.
[27] J. F. Petty, V. S. Mercer, and M. T. Gross, “Relationship betweenmaximum ankle dorsiflexion range of motion and maximalposterior horizontal excursion in standing,” Issues on Aging,vol. 23, no. 3, pp. 7–14, 1999.
[28] D. C. Kerrigan, A. Xenopoulos-Oddsson, M. J. Sullivan, J.J. Lelas, and P. O. Riley, “Effect of a hip flexor—stretchingprogram on gait in the elderly,” Archives of Physical Medicineand Rehabilitation, vol. 84, no. 1, pp. 1–6, 2003.
[29] R. A. Rider and J. Daly, “Effects of flexibility training onenhancing spinal mobility in older women,” Journal of SportsMedicine and Physical Fitness, vol. 31, no. 2, pp. 213–217, 1991.
[30] M. C. Weng, C. L. Lee, C. H. Chen et al., “Effects of differentstretching techniques on the outcomes of isokinetic exercisein patients with knee osteoarthritis,” Kaohsiung Journal ofMedical Sciences, vol. 25, no. 6, pp. 306–315, 2009.
[31] S. B. Thacker, J. Gilchrist, D. F. Stroup, and C. D. Kimsey, “Theimpact of stretching on sports injury risk: a systematic reviewof the literature,” Medicine and Science in Sports and Exercise,vol. 36, no. 3, pp. 371–378, 2004.
[32] J. L. Leibesman and E. Cafarelli, “Physiology of range ofmotion in human joints: a critical review,” Critical Reviews inPhysical and Rehabilitation Medicine, vol. 6, no. 2, pp. 131–160,1994.
[33] ACSM, ACSM’s Resource Manual for Guidelines for ExerciseTesting and Prescription, Lippincott, Williams & Wilkins,Philidelphia, Pa, USA, 8 edition, 2010.
[34] A. D. Kay and A. J. Blazevich, “Effect of acute static stretch onmaximal muscle performance: a systematic review,” Medicine& Science in Sports & Exercise, vol. 44, pp. 154–164, 2012.
[35] I. Shrier, “Does stretching improve performance? A systematicand critical review of the literature,” Clinical Journal of SportMedicine, vol. 14, no. 5, pp. 267–273, 2004.
[36] P. Estabrooks and A. V. Carron, “The conceptualization andeffect of control beliefs on exercise attendance in the elderly,”Journal of Aging and Health, vol. 10, no. 4, pp. 441–457, 1998.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com
Recommended

















