
Filariae
Filariasis is one of the five major parasitic
disease in China and also one of the six major
tropical diseases to which WHO devotes much
attention (malaria, shistosomiasis, filariasis, lei
shmaniasis, trypanosomiasis) . Wuchereria ba
ncrofti and Brugia malayi are found in China.

Eight Species of Filariae Parasitizing Humans_____________________________________________________________________________ Species Site of inhabitation Vector Pathogenesis Distribution_______________________________________________________________________ W. bancrofti lymphatic tissues mosquito lymphatic damage worldwide____________________________________________________________________ Brugia malayi lymphatic tissues mosquito lymphatic damage Asian_______________________________________________________________________ Brugia timori lymphatic tissues mosquito lymphatic damage Island of timor __
__________________________________________________________________ Onchocerca subcutaneous; eye black fly 蚋 river blindness Africa volvulus_______________________________________________________________________ Loa loa subcutaneous deer fly 斑虻 skin swellings Africa_______________________________________________________________________ Dipetalonema subcutaneous midge 库蠓 indefinite Africa streptocerca _______________________________________________________________________ Dipetalonema thoracic and midge 库蠓 indefinite Middle and perstans abdominal cavities South America_______________________________________________________________________ Mansonella peritoneal cavity midge 库蠓 indefinite South America ozzardi _______________________________________________________________________

I. Morphology
1. The adults are white and thread-like worms. T
he female is about 5-10 cm and the male 2.5-4 cm.
2. The microfilaria ranges from 177-296µm in len
gth. They are encased in a sheath. A large number
of body nuclei are seen in the stained specimen. A
nerve ring with no nuclei can be seen at the anterior
1/5 of the body. The morphological differences bet
ween bancroftian and malayan microfilariae are the
following:

Adult worm of filaria

Morphological Differences of Microfilariae between W. bancroti and B. malayi
________________________________________________________________
Species W. bancrofti B. malayi
________________________________________________________________
Appearance graceful, sweeping curves irregular, stiff curves
________________________________________________________________
Size larger 244-296× 7 µm smaller 177-230 × 6 µm ________________________________________________________________
Cephalic space shorter(1:1 or1:2) longer(2:1)
(length:width)
________________________________________________________________ Nuclei body nuclei equal sized, clearly unequal sized, coalescing,
defined, countable uncountable
________________________________________________________________
Terminal nuclei no two
________________________________________________________________

Microfilaria of W. bancrofti and B. malayi

Microfilaria of W. bancrofti

Anterior part and posterior part of bancroftian microfilaria

Microfilaria of W. bancrofti showing it’s appearance

Bancroftian microfilaria:body nuclei equal sized, clearly, defined, countable without cau
dal nucleus

Microfilaria of W. bancrofti

Microfilaria of B. malayi: the body nuclei is unequal sized, coalescing,uncountable. The cephalic space i
s longer with two caudal nuclei.

Microfilaria of B. malayi


II. Life Cycle: 1.Biohelminth: intermediate hosts(vector) are
mosquitoes, bancroftian filaria is transmitted by
Culex pipiens pallens in which the larval develop
ment takes 10-14 days, the development of malay
an filaria in Anopheles sinensis requires 6-6.5 da
ys;
2. Infective stage: filariform larva(L3);
3. Infective route: by skin( the wound bitten by
mosquito );

4. Site of inhabitation: lymphatic tissue;
5. Life span: 4-10 years;
6. Microfilariae may survive 1-3 months;
7. Viviparous;
8. Nocturnal periodicity: The microfilariae p
resent in the peripheral blood during dayt
ime is very low in density. The number of
microfilariae gradually increase from eve
ning to midnight.


Proboscis of a mosquito containing filariform larvae

A large number of 3rd stage larvae of a filarial sp emerging from the
proboscis of a mosquito.


III. Clinical manifestation
1. Acute stage:
The symptoms are due to allergic reaction. It be
gins with a chill followed by a high fever. It is c
alled filarial fever. The lymphangitis (淋巴管炎) , lymphadenitis(淋巴结炎) may occur, o
rchitis(睾丸炎) and inflammation of sperma
tic cord are only found in infection of W. bancr
ofti.

2. Chronic stage:
The manifestations are caused by lymphatic lesion.
(1) Elephantiasis: Lymph edema may occur in the limbs, scrotum, breast, vulva and etc.
(2) Chyluria only caused by W. bancrofti.
(3) Hydrocele is only found in infection of W. bancrofti.

A patient of elephantiasis

Elephantiasis of leg due to filariasis

Elephantiasis due to Brugia malayi. Pitting does not occur in this stage (solid edema)
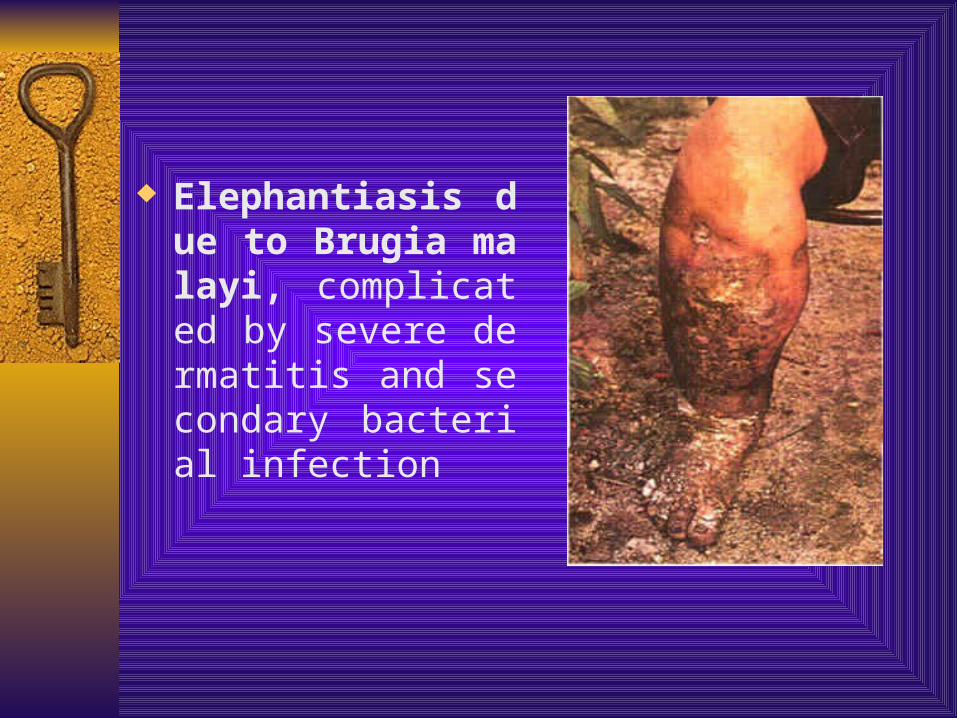
Elephantiasis due to Brugia malayi, complicated by severe dermatitis and secondary bacterial infection

This lady has elephantiasis of the right leg and edema in the left
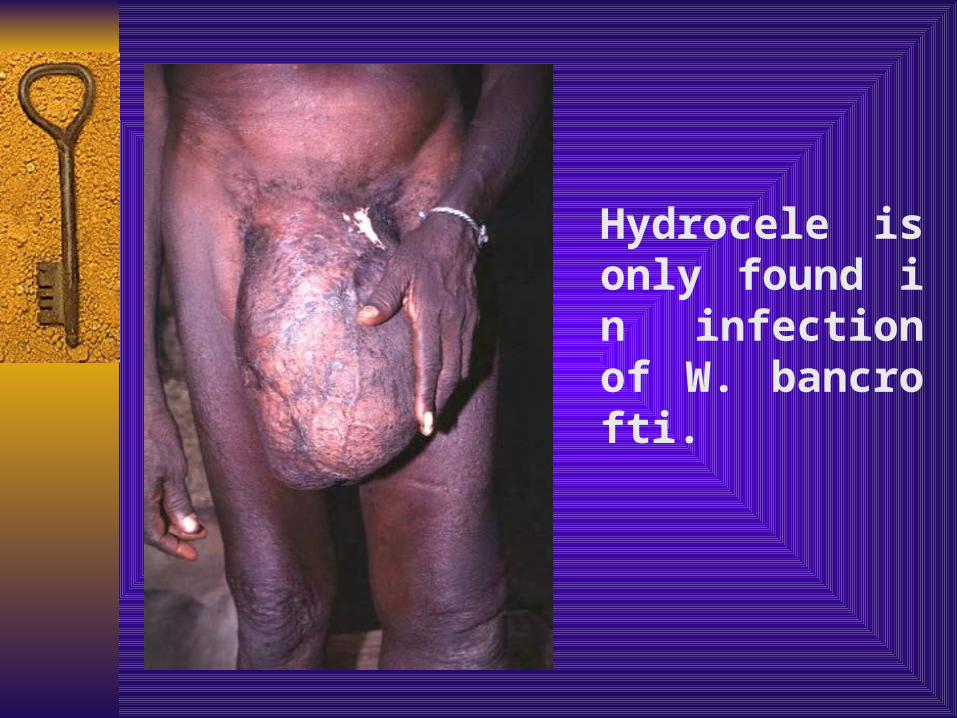
Hydrocele is only found in infection of W. bancrofti.

elephantiasis of the left leg and scrotum

IV. Diagnosis The diagnosis depends on the symptoms, sign
s and history of living in endemic areas, but the confirmative diagnosis depends on the demonstration of microfilariae.
1. First choice method is thick blood smear, taking blood at night from 9pm-2am.
2. Millipore membrane filtration is used for screening the patients or checking curative effect in the endemic areas with the low infective rate.
3. Fresh blood smear used for mass education.
4. Immunological tests are only made reference of the diagnosis.

V. Treatment and Prevention Elimination the source of infection and control mo
squitoes. 1. First choice drug is diethylcarbamazine ( DEC,
Hetrazan ). 2. DEC table salt (3:1000 ) are sold in endemic are
as. People take this salt over 6 months, resulting in an elimination or great reduction of microfilariae in the blood stream, for treating and preventing filariasis.
3. Remove the giant elephantiasis of the scrotum, chest and limbs.
4. Eradicate mosquito breeding place and control mosquitoes.It is important to protect people from mosquito biting for controlling filariasis.

VI. Epidemiology 1. Source of infection: The people harbor microfilariae i
n the blood stream. 2. Vector: Culex pipiens pallens, C. fatigans for W. banc
rofti, Anopheles sinensis, Anopheles anthropophagus transmitting B. malayi.
3. Distribution: Filariasis of W. bancrofti is world-wide distribution, while filariasis of B. malayi is in Asia. In China, W. bancrofti distributes in south of Yellow River 16 provinces and city, while B. malayi in south of Yellow River 13 provinces and city. B. malayi is not in Shandong, Hainan and Taiwan.
4. Reservoir host: W. bancrofti is no reservoir host, while cat, monkey may be the reservoir host of B. malayi.

Trichinella spiralis
T.spiralis is the smallest human nemato
de and a biohelminth. The adults and juv
eniles (larvae) live in the same host, but t
hey have to change a host to complete th
eir life cycle.They cause trichinosis, a zoo
nosis, which is spread by mammals kill e
ach other. Human infections result from
eating raw meat.

I. Morphology
1. Adults: ♂1.5mm, ♀3-4mm, both have a single set of reproductive organs and stichocytes surrounding the esophagus. The secretions of stichocytes are relative to digestion and pathogenesis.
2. Juvenile: 124×6 µm, one or more coil in a cyst in the skeletal muscle fibers. The cyst is about 0.25-0.5 ×0.21-0.42mm in size. This is infective stage. There are stichocytes around the esophagus.


Trichinella spiralis encysted larva

T. spralis – posterior end, male & female

II. Life cycle
1. Infective stage: juveniles in cyst
2. Site of inhabitation: adults in small intestine(mainl
y in duodenum and jejunum), juveniles in skeletal mu
scles
3. Route of infection: by mouth
4. Life span of female: 1-2 months
5. Final host and intermediate host: person
6. Reservoir host: pigs, cats, dogs, mice etc


swallowed by man digestive juice Juveniles in raw meat duodenum cysts rupture penetrate mucosa, develop and molt
Larvae free from the cysts ♂adults return to intestinal lumen ♀ die Mate give birth to portal vein ♂burrow into mucosa juveniles ♀ Liver R.H lungs L. H skeletal muscle cells

III. Clinical manifestation
The process of the pathogenesis may be divided into 3 stages:
1. Invading stage(about 1 week): The damage is mainly found in the intestine. In this stage, abdominal pain, nausea,vomiting,diarrhea and fever may occur.
2. Migrating stage of the juveniles(2-3weeks):The damage is mainly in the skeletal muscles. In this stage, muscular pain with high fever is main symptoms, especially in active muscles. Wandering juveniles may also cause pneumonitis, pleurisy, encephalitis, nephritis and myocarditis etc.
3. Encysted stage(4-16 weeks): In this stage, only muscular pain present without other symptoms.

IV. Diagnosis 1. Muscular biopsy; 2. Examination of left food and xeno
diagnosis; 3.Immunodiagnosis:(1) CPT(circumlarval precipitin test) (2) ELISA (3) IHA
V. Treatment: Albendazole and Mebendazole
VI. Epidemiology: Worldwide distribution. Lots of mammals can serve as reser
voir hosts. The spread of trichinosis is due to mammals killing each other. Humans get the infection by eating raw meat.
VII. Prevention 1. Quarantine of meat; 2. Avoid eating raw meat and feeding a
nimals on raw meat.
Recommended

![HOW FRANCE'S CAME, SA W AND CONQUERED CITYHOWFRANCE'SMARSHAL CAME, SAWAND CONQUERED CITY RICHMONDDOESITSELFPROUDIN] WARMTHOFFOCHDAY WELCOMEj City Declares Iialf-Holiday and Devotes](https://img.dokumen.tips/doc/110x75/5f46f2308c98510d5c7c493f/how-frances-came-sa-w-and-conquered-city-howfrancesmarshal-came-sawand-conquered.jpg)















