Ethics, Virtue and Professionalism—An Overview
Howard Brody, MD, PhD
Center for Ethics & Humanities
Michigan State University
Main Topics
• What is ethics all about?• What sorts of conversations produce
ideally ethical behavior?• What’s the relationship between ethics
and professionalism (virtue)?• What tensions characterize the effort to
become an ethical and virtuous physician?
Ethics
• “Deliberation and explicit arguments to justify particular actions”
• “Principles governing ideal human character”
• Focus on reasons why an action is right or wrong
• For practical purposes, ethics = morals– Lo, p. 5
Ethical dilemmas not resolved by:
• Emotional reactions to case
• Personal moral values
• Claims of conscience
• Claims of rights– Lo, pp. 3-5
• Law
• Appeals to particular religious teachings
Model for Ideal Ethical Conversation
• Based on experience with hospital (institutional) ethics committees
• Currently, most widely recommended practical method for dealing with ethical concerns and disputes in health care settings
How Does a Good Hospital Ethics Committee Try To Resolve an Ethical Case
Dilemma?
Productive Moral Conversation
• Includes people of diverse backgrounds (personal and professional)– Diversity eagerly sought, not merely
tolerated
• Lays as many ethical considerations as possible on the table– No decision reached until the “quiet people”
have spoken up
Productive Moral Conversation (II)
• Ethical considerations are critically weighed for pertinence to case at hand
• Often reason by analogy: have we been successful with similar cases in past?
• Appeals to rules and principles (e.g., patient autonomy) are tools of inquiry, not rigid formulas
Productive Moral Conversation (III)
• Basic moral value, respect for others modeled in process as well as in outcome– Ideas others put on table are critically
challenged and questioned– Questioning is done without suggesting
disrespect for the person who holds differing moral views
– The person who disagrees with you is your best resource in discovering moral truth
Integrity Preserving Compromise
• Commonly used process for resolving moral disputes in pluralistic settings
• Distinguishes two senses of compromise:– Giving up my moral integrity by abandoning
my core moral values– Agreeing to a practical course of action that
coheres only in part with my deeply held moral values
Integrity Preserving Compromise (II)
• Recognizes that in real world we cannot simply “fire” those with differing views
• Recognizes that we value high-quality patient care, which requires that many people of diverse moral backgrounds all agree to cooperate
• Values of civil discourse, cooperation, mutual respect as important as values on what should be done
Example from Course
• How should Ob-Gyn residency programs handle training in abortion techniques?
• We will not have a debate on whether abortion is right or wrong
• We will discuss how residents and faculty with diverse views on the morality of abortion could agree upon an acceptable policy
Professionalism and Ethics– The Same or
Different?
Professionalism
• Competence
• Honesty
• Compassion
• Respect for Others
• Professional Responsibility
• Social Responsibility
Ethics and Virtue
• The CHM list of professional behaviors describes a set of virtues of the good (student) physician
• How does virtue fit in with ethics?
Two Ethical Questions
• What ought to be done in this situation, all things considered?– “Snapshot ethics”– Main focus of HM 546 ethics module
• How ought I live a life of moral excellence in my chosen profession?– “Video ethics”– Main focus of professionalism curriculum
What Are Virtues?
• Excellences in human behavior
• Represent core moral values
• One tries to live a life so that one’s daily behavior exemplifies those core values
• “Obituary test” (inherently biographical view)
Example: Compassion
• Core personal and professional value (defines ideal physician)
• What would the ideally compassionate physician do in this situation?
• How would the ideally compassionate physician go about living a life with medicine as a chosen career?
A Famous Musician
• “If I don’t practice for one day, I know it. If I don’t practice for two days, the critics know it. If I don’t practice for three days, the audience knows it.”
• “Fine discernment” and virtue
Fine Discernment
• Virtue ideally involves doing the right thing, in the right way, for the right reasons, with the right attitude
• Like becoming a music virtuoso, achieving optimal virtue is a life long project
• Irony: The more virtuous one is, the better one can detect even slight lapses
Compassion
• Response to the fellow human who is suffering• Beginner: “Oh, don’t worry, it can’t be that
bad”• Responds to my discomfort at other’s suffering• Challenge: To appropriately be present with
the suffering person, appropriately vulnerable to their suffering, while remaining whole oneself– Requires extensive experience and practice
Compassion, cont.
• Conscious and unconscious elements• Conscious: wish to reflect carefully on what
compassion is and why it is important (e.g., why not “sympathy”?)
• Unconscious: I wish in the future to respond automatically to a new situations as a compassionate person would– Goal: To be compassionate even when I’m having a
bad day
Important Concepts
• Ethics
• Virtue
• Integrity (= wholeness)
“Three-Legged Stool”
• Proposed model to describe typical moral tensions that arise in trying to live a life of integrity in medicine
A Traditional Argument
• The physician’s professional and social responsibility is solely and completely determined by one ethical role– serving as a single-minded advocate for each individual patient
The Virtuous Physician
Individual patient advocacy
Medicine’s Future
• Resources will be limited and some system of rationing will be needed
• Physicians will increasingly be held accountable for how they spend other people’s money
Newer Argument
• Physicians cannot be completely ethical merely by being advocates for individual patients; they must advocate for all patients collectively by concerning themselves with the prudent allocation of limited resources
The Tension: The Physician as--
Loyal patientadvocate
Prudent allocator of limitedresources
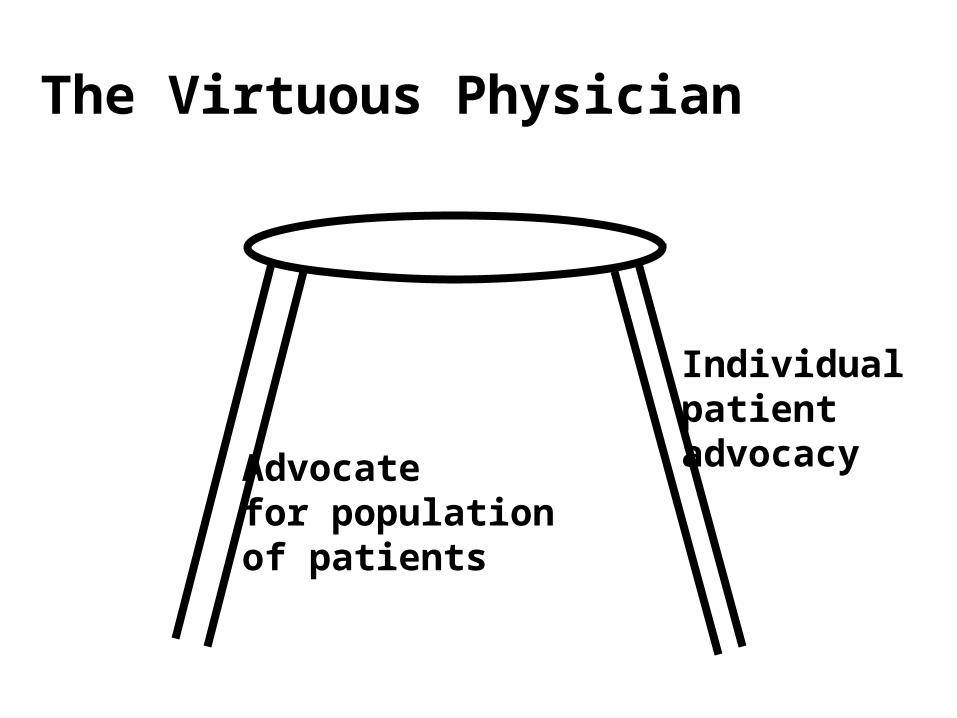
The Virtuous Physician
Individual patient advocacyAdvocate
for populationof patients
Example: Time Spent with Each Patient
• Complaint: Managed care forces the physician to rush patients through too quickly
• Does the managed care contract require limitations of time per visit?
• Or must the physician see more patients faster if he/she wishes to maintain a certain level of income?
[I]f the providers can somehow insistupon driving Cadillacs, then a given[health care] budget set aside bysociety…will make available topatients fewer real health servicesthan would be available if providerscould be induced somehow to makedo with Chevrolets.
--U. Reinhardt, Milbank Q 1987
Patient Advocacy?
• Suppose your patient needs another $60K to be able to afford a liver transplant
• Suppose you have $60K set aside as a college fund for your 12-year-old
• Are you obligated to give your patient this $60K?– How do one- and two-legged stool models
answer this question?
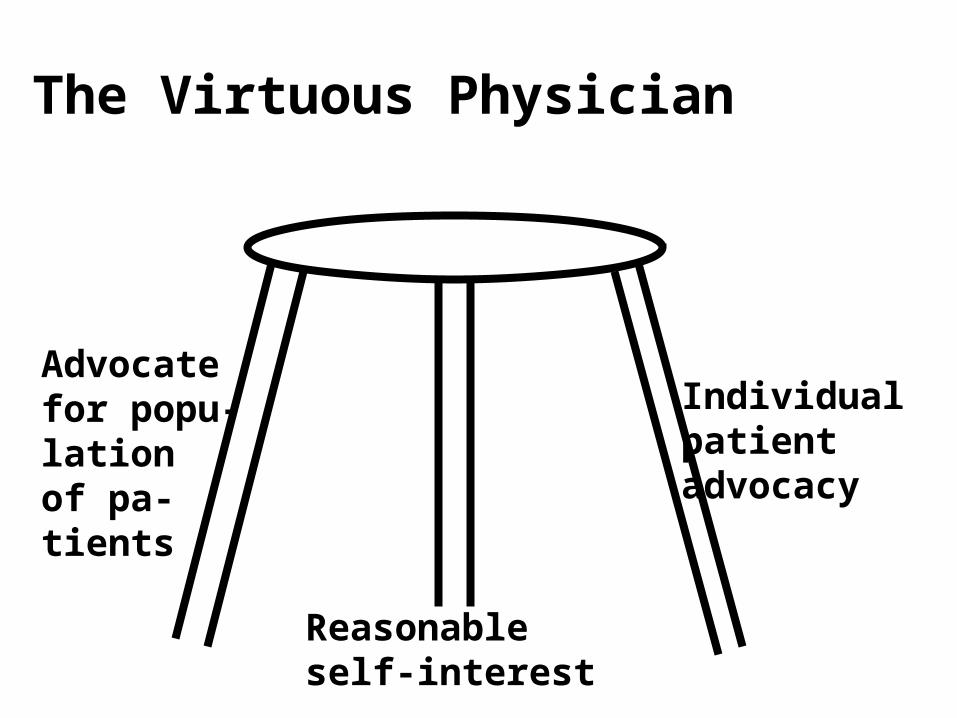
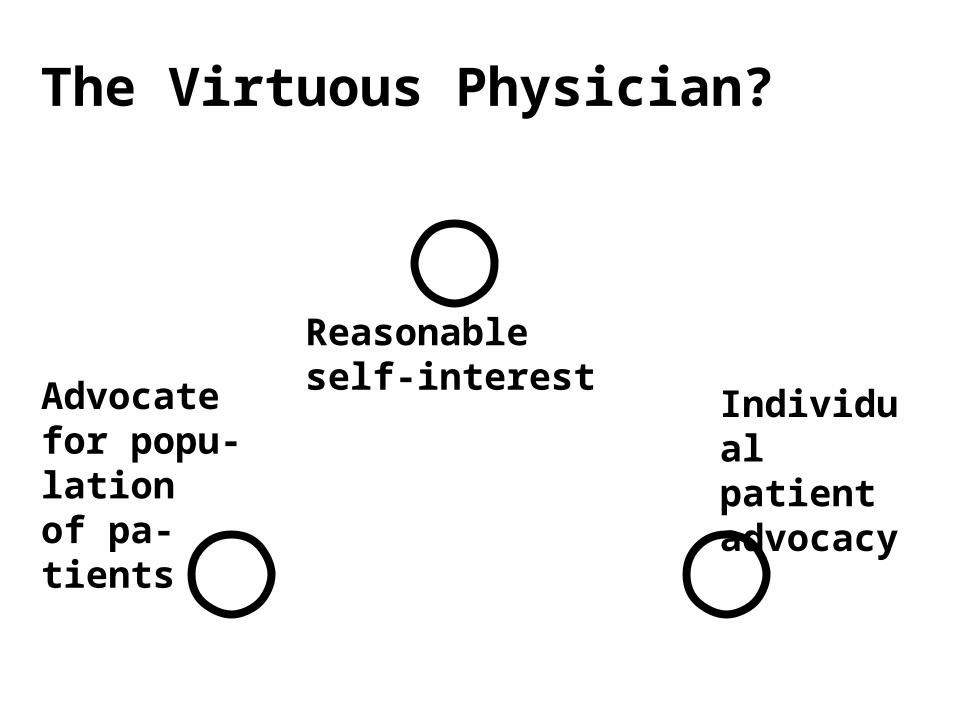
The Virtuous Physician
Advocatefor popu-lationof pa-tients
Individual patient advocacy
Reasonableself-interest
“Three-Legged Stool”
• Argues that to live a whole life, one has to consider one’s own personal interests as being in some sort of reasonable balance with competing interests
• Ignoring these tensions seems to portray medical ethics in an unrealistic light (“Sunday sermon”)
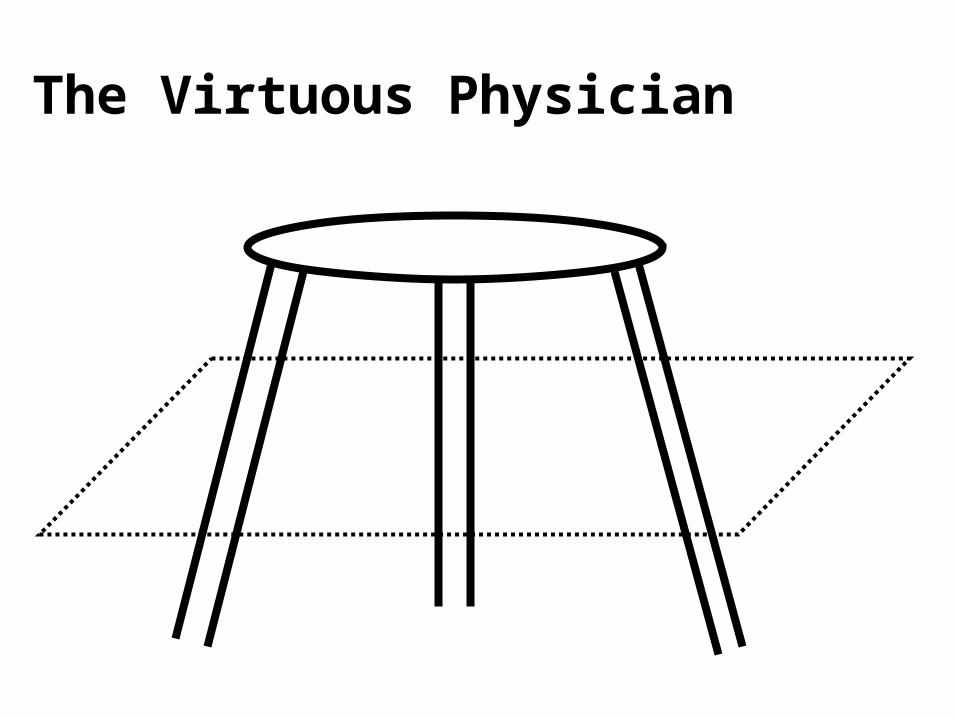
The Virtuous Physician
The Virtuous Physician?
Advocatefor popu-lationof pa-tients
Individual patient advocacy
Reasonableself-interest
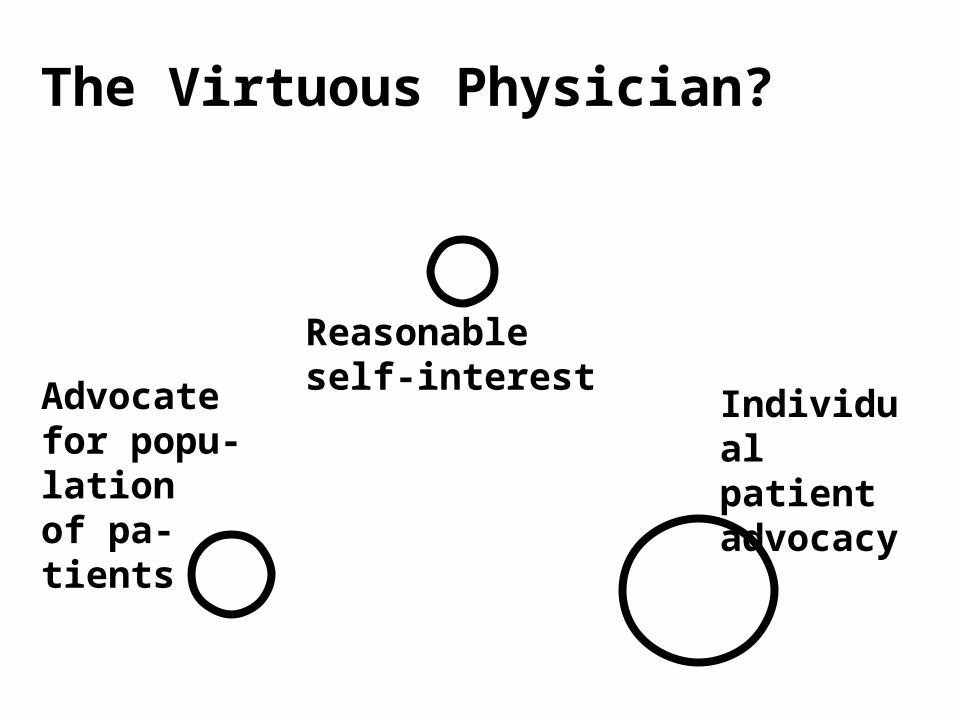
The Virtuous Physician?
Advocatefor popu-lationof pa-tients
Individual patient advocacy
Reasonableself-interest
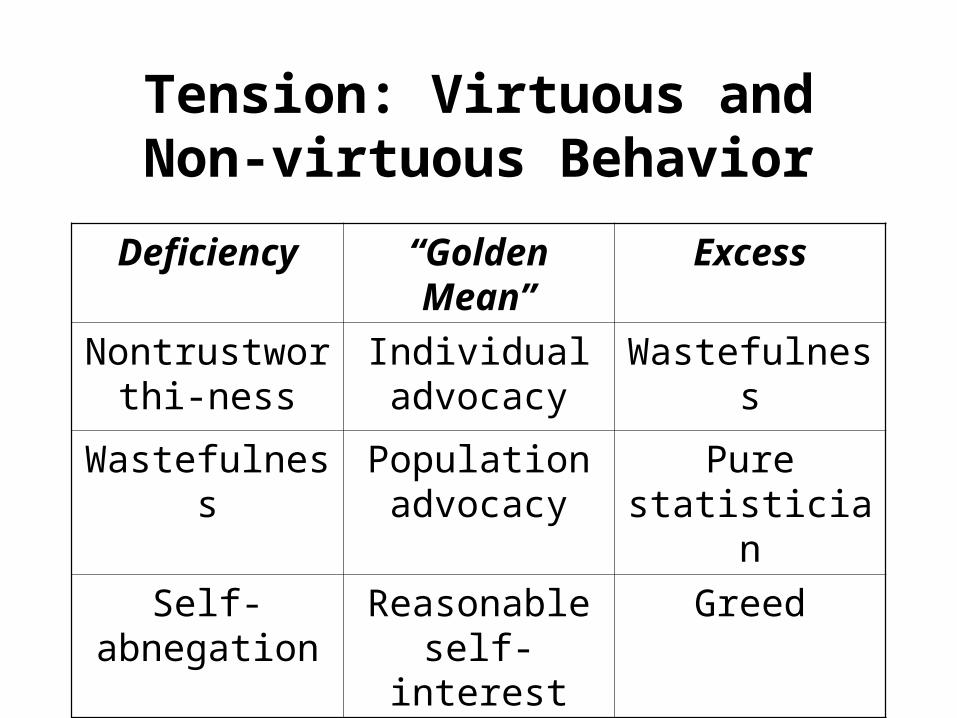
Tension: Virtuous and Non-virtuous Behavior
Deficiency “Golden Mean” Excess
Nontrustworthi-ness
Individual advocacy
Wastefulness
Wastefulness Population advocacy
Pure statistician
Self-abnegation Reasonable self-interest
Greed
“Three-Legged Stool”
• The ideally virtuous physician strives throughout a professional life to balance these tensions:– Among the three competing values (“legs)”– Against the pulls on each “leg” to move away
from the “golden mean”
Recommended

















