
Drugs for Bone and soft tissue infections

Principles of antimicrobial therapy
Drug
HostMicrobe

Name of the diseaseEtiological agent (s)Signs and symptoms Treatment (drug of choice and one alternative drug)

Skin Normal Flora
• Mostly gram-positive bacteria– staphylococci– micrococci– corynebacteria (diphtheroids)– Propionibacterium acnes
• Vigorous washing reduces but does not completely eliminate
• Sweat glands and hair follicles help to reestablish bacterial flora
S. aureus

impetigo
Ecthyma
Cellulitis
Panniculitis
Necrotizing fasciitis
Erysipelas

Folliculitis: infection of hair follicle (S. aureus)
Impetigo (S. pyogenes, S. aureus)
Furuncle: deep inflammatory nodule usually developing from folliculitis (S. aureus)
Carbuncle: more extensive than a furuncle with involvement of the subcutaneous fat (S. aureus)

1.2.
3.
4.5.

Skin and soft tissue
IDSA 2005

• better oral absorption (53.7% and 32.9%, respectively)
• slower (renal and extra-renal) elimination (T1/2 : 46 and 32 min, respectively).
• high risk of cholestatic hepatitis
PhenoxymethylpenicillinCloxacillin Dicloxacillin
Flucloxacillin
PHP 32
Similar profile : • Comparable bioavailability after oral
administration dicloxacillin /cloxacillin (48.8% and 36.9%)
• The elimination rate was similar the urinary recovery of active dicloxacillin was higher in young subjects and that the non-renal
clearance was higher in elderly volunteers.- Dicloxacillin: risk of thrombophlebitis
- (NSW advisory, 2000)

Cloxacillin Dicloxacillin Oxacillin FlucloxacillinR: ClR1: H
R: ClR1: Cl
R: HR: H
R: ClR1: F
Bioavailability % 6.0 3.1 6.9 5.3Protein binding % 94.7 96.9 93.1% 94.7Cost 28.50 na 212/vial 32.35Indications (Need) Staphylococcal skin infections and cellulitis
Pneumonia (adjunct) / Osteomyelitis, septic arthritis Septicaemia / Empirical treatment for endocarditis Surgical prophylaxis

Cellulitis: extending subcutaneous tissues (S. aureus, S. pyogenes, anaerobes)
Erysipelas: (S. pyogenes)
Staphylococcal Toxic Shock Syndrome: (S. aureus)
Scalded skin syndrome (S. aureus)

Common Antibiotics for skin and soft tissue infections

Nafcillin• resistant to inactivation by the enzyme penicillinase (beta-
lactamase).• relatively acid-stable and have reasonable bioavailability.• The peak OX levels in serum were at least twice the peak NAF
level, but the half-life of NAF in the serum (2.1 hours) was about twice that of OX (1.1 hours).
• Nafcillin is associated with neutropenia; oxacillin can cause hepatitis


Soft Tissue Infections• Myositis
– infection of skeletal muscle (rare)– S. aureus, S. pyogenes (rare), mixed organism

Soft Tissue Infections• Necrotizing fasciitis
– “flesh-eating disease”– sever infection involving the
subcutaneous soft tissue, particularly the superficial and deep fascia
– predisposing conditions: diabetes, abdominal surgery, perineal infection, trauma
– organisms: S. pyogenes, C. perfringens, mixed aerobic and anaerobic bacteria
– treatment surgical debridement, antibiotics, + immunoglobulins


Gas gangrenerapidly progressive, life-threatening, toxemic infection of skeletal muscle due to clostridia

Antibiotics for MRSA

Why are MRSA important?
MRSA: Strains that are oxacillin and methicillin resistant, historically termed methicillin-resistant S. aureus (MRSA), are resistant to all ß-lactam agents, including cephalosporins and carbapenems.
• Pathogenicity. MRSA have many virulence factors that enable them to cause disease in normal hosts.
• Limited treatment options.Vancomycin and two newer antimicrobial agents, linezolid and daptomycin, are among the drugs that are used for treatment of severe healthcare-associated MRSA infections.
• MRSA are transmissible.CDC

Linezolid :Initiation Factors
30S ribosome
mRNA50S
ribosome
30S + mRNA
fMet - tRNA
Elongation Factors
70S Initiation Complex
Peptide Product
Elongation
AminoglycosidesMacrolides Streptogramins
Linezolid blocks formation of the
initiation complex
Prevents bacterial protein synthesis by binding to the 23S ribosomal RNA of 50S subunit

LinezolidUse:• Works against aerobic gram-positive organisms• Infections caused by MRSA/VREPdynamics:• Linezolid is administered by intravenous infusion or orally
(100% oral bioavailability)• have significant penetration into bone, fat, muscle, and
hematoma fluid • metabolism is non-enzymatic and does not involve CYP450;
Non-renal clearance accounts for 65% of an administered linezolid dosage (no adjustment in renal failure)
•

Safety of Linezolid
• common adverse events in children are diarrhea, vomiting, loose
stools, and nausea• Toxicity: Duration-dependent bone marrow suppression,
Thrombocytopenia is the most common manifestation, • non-selective inhibitor of monoamine oxidase (MAO)
=neuropathy, and optic neuritis serotonin-syndrome may occur when coadministered with other serotonergic drugs (eg, selective serotonin reuptake inhibitors); lactic acidosis

Daptomycin
• Daptomycin is a lipopeptide class antibiotic that disrupts cell membrane function via calcium-
dependent binding, resulting in bactericidal activity in a concentration-dependent fashion.
It is a naturally-occurring compound found in the soil microbe Streptomyces roseosporus.

Lipopeptides• treatment of complicated skin
and soft tissue infections due to gram-positive bacteria (but not anaerobes)
• Bacteriocidal against multidrug-resistant, gram-positive bacteria
• Methicillin-resistant Staphylococcus aureus
• Vancomycin-resistant enterococci
• Glycopeptide-intermediate and -resistant S. aureus.
• Penicillin-resistant Streptococcus pneumoniae

Daptomycin
• Post antibiotic effect• Once daily dosing• ElevationsAdv events:
in creatinine phosphokinase (CPK), rarely treatment limitingmuscle pain or weakness; daptomycin-induced eosinophilic pneumonia have been described
Excreted mainly through kidneys





Types of bone/joint infections
• Arthritis (infective/septic)• Osteomyelitis• Prosthetic bone and joint infections

BacteriaAcute Septic
ArthritisProsthetic
Joint InfectionSeptic Bursitis Osteomyelitis
Staphylococcus aureus +++ +++ +++ +++
Coag negative Staph +++
Hemolytic Streptococcus ++ ++ ++ ++
Other Streptococci + + +
Skin anaerobes + +++ +
Gram-negative cocci + +
Hemophylus influenza + + +
Gram-negative anaerobes + ++ + +
Pseudomonas aeruginosa + + +
Salmonella + + +
Intestinal anaerobes +
Mycobacteria + +

Bone Infections
• Septic arthritis– infection of joint spaces– hematogenous or contiguous– S. aureus, Streptococcus spp., Gram-negative bacilli
• Osteomyelitis– infection of the bone– hematogenous or contiguous– S. aureus, S. pyogenes, H. influenzae, Gram-negative bacilli

RISK FACTORS / Manifestations Trauma Diabetes Hemodialysis SplenectomyAdvanced age
Immune function
Poor circulation
Pain Swelling, redness,
warmth Purulent exudate Systemic
Fever Chills Nausea Malaise
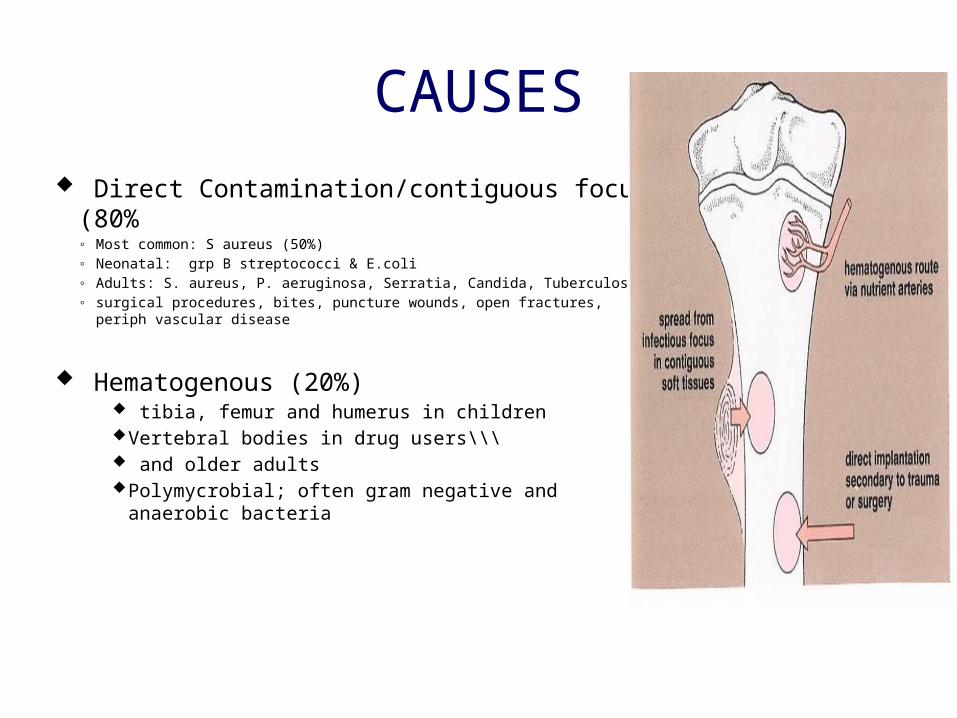
CAUSES Direct Contamination/contiguous focus (80%
◦ Most common: S aureus (50%)◦ Neonatal: grp B streptococci & E.coli◦ Adults: S. aureus, P. aeruginosa, Serratia, Candida, Tuberculosis◦ surgical procedures, bites, puncture wounds, open fractures, periph vascular
disease
Hematogenous (20%) tibia, femur and humerus in children Vertebral bodies in drug users\\\ and older adults Polymycrobial; often gram negative and anaerobic
bacteria

Gonococcal ArthritisTenosynovitis, dermatitis, polyarthralgia syndrome
Typically seen in young adults Acute illness with fever, chills,
malaise. Tenosynovitis Generalized arthralgia Dermatitis: pustular or
vesicopustular Monoarticular or
Pauciarticular◦Large joint involvement (knees, wrists, ankles)
Most patients are afebrile Signs of disseminated
infection are rare

DIAGNOSTIC STUDIES
MRI CT Bone Scan Ultrasound Labs:
Sed Rate WBC’s Cultures

Initial empirical antibiotic choice in suspected septic arthritis
Patient group Antibiotic choice
No risk factors for atypical organisms Penicillin 3-4 u IV q 8 (pen sensitive)Nafcillin or oxacillin 2 g IV q 4hFlucloxacillin 2 g qds i.v. Local policy may be to
add gentamicin i.v.If penicillin allergic, clindamycin 450–600 mg qds i.v. or 2nd or 3rd generation cephalosporin (Cefazolin 1 g q 8)
High risk of Gram-negative sepsis (elderly, frail, recurrent UTI, and recent abdominal surgery)
2nd or 3rd generation cephalosporin eg cefuroxime 1.5 g tds i.v. Local policy may be to add flucloxacillin i.v. to 3rd generation cephalosporin. Discuss allergic patients with microbiology—Gram stain may influence antibiotic choice
MRSA risk (known MRSA, recent inpatient, nursing home resident, leg ulcers or catheters, or other risk factors determined locally)
Vancomycin i.v. plus 2nd or 3rd generation cephalosporin i.v.
Suspected gonococcus or meningococcus Ceftriaxone i.v. or similar dependent on local policy or resistance
Pseudomonas Extended B lactam: Piperacillin 3-4g Ivq 4-6h; Ceftazidime 2 g IV q 12h

• Duration of treatment– Hematogenous 4-6 weeks– Contiguous focus 2 wks after debridement– Chronic 4-6 wks

Diabetic foot infection


Management
• Surgical debridement (may not be necessary in children)
• Antibiotics for 4-6 weeks (at least 2wks IV)– multiple courses may be necessary
Rheumatology 2006 45(8):1039-1041;

Septic ArthritisEpidemiology Risk factors
Elderly or very young
Underlying chronic illness
Increased incidence with warmer climates and poorer socioeconomic status
1:10,000 annual incidence in Northern European children
Age > 80 years
Comorbid conditions (especially diabetes)
Joint damage from arthritis
Prosthetic joint
Skin & extraarticular infection
Immune suppression (malignancy or treatment)
Cirrhosis
Chronic renal failure and hemodialysis
IV drug abuse
Prior antibiotic use

1. Hematogenous
2. Dissemination from osteomyelitis
3. Spread from adjacent soft tissue infection
4. Diagnostic or therapeutic measures
5. Penetrating damage by puncture or cutting.
Pathogenesis
• No previous joint disease or illness in 54%
• 72% of infections were hematogenous in origin
• Staph aureus 37%
• Strep pyogenes 16%
• Neisseria gonorrhea 12%Clinical Features
• Joint swelling and pain
• Pain with range of motion, immobility
• Fever
• Signs of sepsis
• Distribution usually monoarticular
• Large joints most often involved

Septic ArthritisJoints affected (non-gonococcal)
Joint Adults % Children %
Knee 55 40
Hip 11 28
Ankle 8 14
Shoulder 8 4
Wrist 7 3
Elbow 6 11
Others 5 3
Multiple joints (12) (7)

Septic ArthritisNatural History
0 1 2 3 4 5 6 7 8
Time (days)
Experimental bacterial arthritis induced
Maximal acute arthritis symptoms
Chronic or irreversible changes
• Temp < 38.3 in 14/40
• WBC < 15K in 13/38
• ESR < 30 in 4/36
• Synovial fluid WBC < 50K in 8/22

Classification of Joint Effusions
Type Features WBC/mm3
Normal Clear, colorless, Viscous<200<25% PMNs
Non-Inflammatory Clear, Yellow, viscous200-2000<25% PMNs
InflammatoryCloudy, Yellow, WateryGlucose may be low
2000-100,000>50% PMNs
SepticPurulentGlucose very low
80,000>90% PMNs

Septic ArthritisAdults versus Children
Adults % Children %
Gram positive cocci
Staph aureus 35 27
Strep (pyogenes, pneumonia, viridans) 10 16
Gram negative cocci
Neisseria (meningitidis and gonorrhea) 50 8
Hemophilus influenzae <1 40
Gram negative bacilli
E. coli, Salmonella and Pseudomonas sp. 5 9
Mycobacteria and Fungi <1 <1

Rheumatology 2006;45:1039–1041

Viral Arthritis
Inflammatory polyarthritis, similar to early RA
Duration usually < 1 month, self limited illness
Not destructive to joint
Prodromal symptoms◦ Fever
◦ Rash
Supportive Treatment (NSAIDs, Analgesics)
Definite Possible
Hepatitis (B & C) Rubella Parvovirus Mumps Arbovirus Variola
Vaccinia Varicella Rubeola Echo EBV Adenovirus
No Antibiotic treatment !!!

Suspected MRSA

Drugs for MRSAIDSA, 2011


a. Name of the diseaseb. Etiological agent (s)
c. Treatment (drug of choice)
d. Alternative drug)
1.
2.
3.
Recommended

















