Dr. Senendra Raj UpretiDirector
Child Health Division, Department of Health Services
Community Based
Newborn Care
ProgramNepal
CB-NCP

2
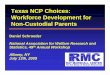
Trends in Child Mortality in Nepal
46 5039
33 33
16
102
79
64
48 46
32
153
118
91
6154
38
0
20
40
60
80
100
120
140
160
180
1991 1996 2001 2006 2011 2015
Neonatal mortalityInfant Mortality
U5 mortality
Marked decline in infant and child mortality
Source: NDHS, NHSP

Source: Pradhan YV et al. 2012. Newborn survival in Nepal: a decade of change and future implications. Health Policy and Planning 27(Suppl. 3):iii57–iii71.Data source: Nepal mortality estimates (Liu et al. 2012). Note: Severe infection includes sepsis, meningitis, pneumonia and tetanus.
3 causes account for 90% of all newborn
deaths
Causes of Neonatal mortality

Community Based Newborn Care Program (CB-NCP)
As an approach to reduce newborn mortality in Nepal

When was policy and programme change achieved?
Pivotal milestone for newborn survival involving multiple champions, partners
and wide ownership
Source: Pradhan YV et al. 2012. Newborn survival in Nepal: a decade of change and future implications. Health Policy and Planning 27(Suppl. 3):iii57–iii71.
Background and Context of CB NCP

Underlying key principles of CB-NCP
• Reaching mothers and newborns early is critical to reducing mortality.
• Mothers need to be identified when they become pregnant and followed up through delivery and post-natal period.
• Community volunteers can be trained to deliver an essential package of newborn interventions, including use of antimicrobials and the management of birth asphyxia .
• The health system at all levels needs to support community based efforts, to ensure newborn care practices improved.

Policy and strategy adoption
• Formation of a technical working group and sub-committees under the leadership of the DoHS and MoHP to collect and review data, synthesize recommendations and develop methods .
• Policy to allow FCHVs to classify and treat sick newborns
with the first dose of co-trimoxazole. • Policies on incentives for FCHVs, mothers and facility
workers to support ANC, delivery and early PNC practices
These policy adoption reflect a strong national commitment

1. Behavior Change and Communication (BCC)2. Promotion of institutional delivery and clean delivery
practices in case of home deliveries 3. Postnatal home visit for newborn4. Case management of Possible Severe Bacterial Infection
(PSBI)5. Management and care of low birth weight newborns6. Prevention and management of hypothermia 7. Recognition and management of birth asphyxia
The Female Community Health Volunteer (FCHV) is identified as pivotal for implementation of CB-NCP.
Seven Interventions included in CB-NCP

Implementation Phases of CB-NCP
Phase I (pilot): 10 districtsPhase II (scale up)—34 districts “covered”,
5 districts- trainings ongoing
Chlorhexidine included in the CB NCP package
Assessment of CB NCP pilot districts : completed May 2012

Source: Pradhan YV et al. 2012. Newborn survival in Nepal: a decade of change and future implications. Health Policy and Planning 27(Suppl. 3):iii57–iii71.Data source: Nepal mortality estimates (Liu et al. 2012). Note: Severe infection includes sepsis, meningitis, pneumonia and tetanus.

Learning from CB NCP
• FCHV role in complication management much smaller than expected
• Enhanced co ordination across divisions (FHD, CHD, MD, LMD, NHTC, NHEICC) required for smoother implementation of peripheral level neonatal (and maternal) services
• Streamline MNCH within the Department of Health Services

Steps forward: Revision of CB NCP
• Increase focus on quality of care and effective coverage for newborn and maternal complications at peripheral health facilities
• Increase the focus on FCHV counseling/ health education during pregnancy and post-natally. (In areas with difficult access to health facility care, ensure program support for an FCHV role in newborn sepsis management)
• Use a flexible, micro-planning approach to determine inputs and service-delivery
• Ensure seamless integration across the range of maternal-newborn services delivered at the primary health care/ community level

Challenges• Funding Gaps
• Wide disparities by socio-economic status in NMR
• Collaboration with private and other non health sector. Eg education, environment
• Capacity for rapid scale up of Newborn Programs across the country to meet the NHSP target
• Quality and infrastructure of referral centres
• Institutional delivery still low in some communities.

Source: Pradhan YV et al. 2012. Newborn survival in Nepal: a decade of change and future implications. Health Policy and Planning 27(Suppl. 3):iii57–iii71. Data source: (Pitt et al. 2010) with special analysis done by C. Pitt Note: All values are in constant 2008 USD. MNCH donor projects with reference to newborn health include MNCH donor disbursements that mention the word ‘newborn’ or relevant search terms in titles or project descriptions. The OECD database does not systematically capture funding from emerging donor states, foundations, non-governmental organizations or faith-based groups.
Changes in official development assistance for MNCH in Nepal
Only 8% of official development assistance for MNCH mentioned newborns in 2008
Child health donor projects with no
reference to newborn terms in the search
fields
Maternal health donor projects with
no reference to newborn terms in the
search fields
MNCH donor projects with reference to
newborn terms in the search fields

Opportunities
• Newborn program is the governments priority program
• Increasing interest of EDPs and partners, thus increased funding
• Implementation and scale up plan developed for Newborn interventions: IMCI/NCP 5 year costed Multi year plan
• HRH strategy endorsed by the government
• Experience and learning from our community based maternal, newborn and child health programs

Dr. Kiran RegmiDirector Family health Division
Innovation in Reducing Neonatal Death in Nepal: Chlorhexidine (CHX) a Simple Intervention

Innovation in Reducing Neonatal Death in Nepal: CHX a simple intervention > Overview
Child mortalityCauses of neonatal deathChlorhexidine a simple intervention in reducing
neonatal deathMilestones of Chlorhexidine in NepalEvidence that Chlorhexidine is effective for cord careChlorhexidine application Nepal policyChlorhexidine implementation approach in NepalKey to Program Success in NepalLesson learnt/ challenges
17

Source: NDHS&NHSP*18
Marked decline in infant and child mortality
Less improvement with neonatal mortality and no change from 2006-2011
Innovation in Reducing Neonatal Death in Nepal: CHX a simple intervention > Child mortality status

Innovation in Reducing Neonatal Death in Nepal: CHX a simple intervention > Causes of neonatal death

20
Innovation in Reducing Neonatal Death in Nepal > CHX a simple invention

Innovation in Reducing Neonatal Death Nepal > CHX a simple intervention

22
Innovation in Reducing Neonatal Death in Nepal > CHX a simple intervention

Innovation in Reducing Neonatal Death in Nepal: CHX a simple intervention > Milestones

Innovation in Reducing Neonatal Death in Nepal: CHX a simple intervention > Milestones

Innovation in Reducing Neonatal Death in Nepal: CHX a simple intervention > Milestones

An estimated 1 in 6 neonatal deaths could be averted with Chlorhexidine cord care.
A simple technology with potential to prevent 500,000 global neonatal deaths annually.
Soure : Hodgins et.al(2013)
Application of Chlorhexidine in freshly cut umbilical cord stump can reduce neonatal mortality by 23%
68% reduction in serious infection Source: Mullany (2011).
Innovation in Reducing Neonatal Death in Nepal: CHX a simple intervention> Evidence > Literature

Study Characteristic Nepal Bangladesh Pakistan
Overall NMR (at time of study)
39/1000 36/1000 30/1000
% of births at home (at time of study)
92% 88% 80%
Total sample size 15,123 29,790 9,741
Primary outcomes Neonatal mortalityOmphalitis
Neonatal mortalityOmphalitis
Neonatal mortality Omphalitis
Comparison group Dry cord care Dry cord care Dry cord care
Frequency of application Days 1,2,3,4,6,8,10 a. First 24 hoursb. Daily for 7 days
Daily for 14 days
Intervention provider Project staff Project staff TBA and care taker
Product form used Water-based liquid Water-based liquid Water-based liquid27
Innovation in Reducing Neonatal in Nepal: Chlorhexidine a simple intervention > Evidence > Research Community based
RCT

24 hours post applicationa. 4.6% (15 of 327) of cultures were positive in the gel group b. 10.7% (35 of 326) in the aqueous groupc. The absolute difference in rates (gel minus aqueous) was 6.1%
(95% CI: 10.2%, 2.1%)
The gel formulation was not inferior to aqueous and gel reduced bacterial colonization to a greater degree
28
Innovation in Reducing Neonatal in Nepal: Chlorhexidine a simple intervention > Evidence > Research Community based RCT > Result

29
Innovation in Reducing Neonatal in Nepal: Chlorhexidine a simple intervention > Evidence > Research Community based RCT >
Recommendations
7.1% Chlorhexidine digluconate is safe for neonatal umbilical cord careAll RCTs showed sufficient evidence to recommend 7.1% Chlorhexidine digluconate for umbilical cord care to reduce neonatal mortalityAll studies recommended for the application of Chlorhexidine as early as possible, specifically within 24 hours of birth

Application of Chlorhexidine to each newborn irrespective of facility and home birth
Single dose resume immediate after cord cutting as a part of essential newborn care followed by clean and dry cord care practices
CHX integrate with essential newborn careScaling up Ensuring sustainabilityCommunity targeted implementation approach
30
Innovation in Reducing Neonatal in Nepal: Chlorhexidine a simple intervention > Nepal policy

31
Chlorhexidine integration into
ongoing programs
Innovation in Reducing Neonatal in Nepal: Chlorhexidine a simple intervention > Nepal policy >
Integration

Completed and Active Districts: 41Planned: Entire Country (75 districts)
Innovation in Reducing Neonatal in Nepal: Chlorhexidine a simple intervention > Nepal policy >
Scale up

Implementation approach
FCHVs distributes CHX to pregnant mother at 8th month of pregnancy after counseling
Orientation to service providers of all level
Orientation to FCHVs
Chlorhexidine orientation to stakeholders and staff of DPHO/DHO
Service delivery at hospital and peripheral health facility
Availability of service at
home birth
Monitoring and quality assurance

34
Government leadership since inception of the programSupply is ensured through the government logistics supply normsLocal manufacturer (Lomus Pharmaceutical) producing a good-quality product - 3 gram of 7.1% Chlorhexidine digluconate gel tube - Nepali brand name KawachCurrent price is Rs.18 ($0.23) for GovernmentPictorial instruction inside boxPartners and professional organisation involvement since beginning to scaling upNepal – member of global Chlorhexidine working groupEnsuring sustainability
Innovation in Reducing Neonatal in Nepal: Chlorhexidine a simple intervention > Key to success

Chlorhexidine added in Essential Drug List of NepalChlorhexidine cord care is a part of an essential newborn careGovernment of Nepal included Chlorhexidine procurement in multi-year procurement planIncluded in routine health information system for recording and reporting
Innovation in Reducing Neonatal in Nepal: Chlorhexidine a simple intervention > Key to success >
Sustainability

Rapid scale up is possible through the existing government health system in NepalTraditional harmful practices of cord care can be replaced
Innovation in Reducing Neonatal in Nepal: Chlorhexidine a simple intervention > Lesson learnt

Source : NDHS, 2011
Innovation in Reducing Neonatal in Nepal: Chlorhexidine a simple intervention > Challenges

WHO position (1998) understood to be against antiseptic useProgram shifting for cord care may create confusion in service provider & recipientIntegrating program at different level i.e. LMIS, HMIS and other essential newborn care related programs
Innovation in Reducing Neonatal in Nepal: Chlorhexidine a simple intervention > Challenges

References:
39
Hodgins S, Pradhan YV, Khanal L, Upretti S, KC NP. Chlorhexidine for umbilical cord care: game-changer for newborn survival? Glob Health Sci Pract. 2013;1(1):5-10. http://dx.doi.org/10.9745/GHSP-D-12-00014
Mullany , L(2011) Chlorhexidine Cord Cleansing. Summary and Meta Analysis of South Asian Trials
Ministry of Health and Population (MOHP) [Nepal], New ERA, and ICF International Inc. 2012. Nepal Demographic and Health Survey 2011. Kathmandu, Nepal: Ministry of Health and Population, New ERA, and ICF International, Calverton, Maryland.

Thank you
Recommended