Dr. S. Nishan Silva(MBBS)


Parts and regions of the lower limb
Gluteal region - between iliac crest superiorly and gluteal fold inferiorly
Thigh - between hip and kneeknee - joint between leg and
thighLeg - between knee and footAnkleFoot

Frolich, Human Anatomy, Lower LImb
Joints of Lower Limb
Hip (femur + acetabulum) Ball + socket Multiaxial Synovial
Knee (femur + patella) Plane Gliding of patella Synovial
Knee (femur + tibia) Hinge Biaxial Synovial

Frolich, Human Anatomy, Lower LImb
Joints of Lower Limb
Proximal Tibia + Fibula Plane Gliding Synovial
Distal Tibia + Fibula Slight “give” Fibrous
Ankle (Tibia/Fibula + Talus) Hinge Uniaxial Synovial
pg 218

Frolich, Human Anatomy, Lower LImb
Lower Limb MovementsHip
Flexion/extensionAbduction/adductionLateral/medial rotation
KneeFlexion/extension
AnkleDorsiflexion/
plantarflexionInversion/eversion
ToesFlexion/extension
Bending on posterior side is flexion (except hip)
Bending on anterior sided is extension (except hip)

Surface anatomy of lower limb
Gluteal region and thighanterior superior and inferior iliac spines
tubercle of iliac crestischial tuberositygreater trochanterpubic tuberclepubic crestsuperior border of pubic symphysis

Frolich, Human Anatomy, Lower LImb
Surface Anatomy: Posterior Pelvis
Iliac crestGluteus maximus = cheeksNatal/gluteal cleft = crackGluteal folds = bottom of
cheek
pg 789

12-9
Surface Anatomy of the Lower Limb Gluteus maximus muscle Gluteus medius muscle Gluteal cleft Gluteal fold Ischeal tuberosity Greater trochanter

Nelaton’s line
a line drawn from the anterior superior lilac spine to the ischial tuberosity, passing over or near the top of the greater trochanter. The trochanter can be felt superior to this line in a person which a dislocated hip or a fractured femoral neck.

Hip - AnatomyMultiaxial ball & socket jointAcetabulum
1/2 sphereFemoral head
2/3 sphereStrong ligaments & capsuleMaximally stable

AnatomyForcesStanding - 0.3 times body weightStanding on 1 leg - 2.5 times body weightWalking - 1.3 to 5.8 times body weightWalking up stairs - 3 times body weightRunning - 4.5+ times body weight

•Flexion and Extension
•Abduction and Adduction
•External Rotation and Internal Rotation.

Bony AnatomyFemur
Femoral HeadFemoral NeckGreater TrochanterLesser TrochanterIntertrochanteric
CrestIntertrochanteric
LineGluteal Tuberosity




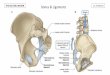
Bony AnatomyPelvic Girdle
Acetabulum3 bones fused
together Ilium
Iliac fossa Iliac Crest ASIS AIIS PSIS PIIS Gluteal Lines Greater Sciatic Notch
Lateral View

Bony AnatomyIlium
Iliac fossaIliac CrestIliac TuberosityASISAIISPSISPIISGluteal Lines
Medial View

Bony AnatomyIliumIshium
Ramus of ishiumIshial tuberosityIshial spineLessor Sciatic Notch

Bony AnatomyIliumIshiumPubis
Superior Ramus of Pubis
Inferior Ramus of Pubis
Pubic CrestPubic TuberclePectinSymphyseal Surface


AnatomyLigaments
Iliofemoral ligament (Y ligament of Bigelow) Reinforces anterior joint
capsule (limits hyperextension)
Keeps us uprightPubofemoral ligament
Limits abduction & hyperextension
Inguinal ligament Runs from ASIS to pubic
symphysis Superior border of
femoral triangle

Anatomical Components:1. Articular Capsule2. Acetabular labrum3. Ligaments:
IliofemoralIliofemoral PubofemoralPubofemoral IschiofemoralIschiofemoral Ligament of the head of the femurLigament of the head of the femur Transverse ligament of the acetabulum Transverse ligament of the acetabulum
Added

Anterior view

Posterior view

Medial view with acetabular floor
removed

Anterior view with capsule removed

Ligamentous and Cartilogenous Structures for the Hip and Pelvic Girdle
Sacroiliac JointSacrotuberousSacrospinousFunction of these
two ligamentsIliolumbar Interosseous
Sacroiliac

Ligamentous and Cartilogenous Structures for the Hip and Pelvic Girdle
Sacroiliac JointSacrotuberousSacrospinousFunction of these
two ligamentsIliolumbar Interosseous
Sacroiliac

Ligamentous and Cartilogenous Structures for the Hip and Pelvic Girdle
Sacroiliac JointSacrotuberousSacrospinousFunction of these
two ligamentsIliolumbar Interosseous
SacroiliacDorsal Sacroiliac

Ligamentous and Cartilogenous Structures for the Hip and Pelvic Girdle
Sacroiliac JointHip Joint
CapsuleThree thickenings
of the capsule Iliofemoral Pubofemoral Ishiofemoral
Ligamentum TeresInguinal

Ligamentous and Cartilogenous Structures for the Hip and Pelvic Girdle
Sacroiliac JointHip Joint
CapsuleThree thickenings
of the capsule Iliofemoral Pubofemoral Ishiofemoral
Ligamentum TeresInguinal

Ligamentous and Cartilogenous Structures for the Hip and Pelvic Girdle
Sacroiliac JointHip Joint
CapsuleThree thickenings
of the capsule Iliofemoral Pubofemoral Ishiofemoral
Ligamentum TeresInguinal






AP HIP
ACETABLUMFEMORAL HEAD
GREATERTROCHANTER
LESSER TROCHANTER
FEMORAL NECK
CORTICAL BONE
MEDULLARY BONE
FOVEA CAPITIS

CORONAL MRI
RT. HIP

Coxa vara (abnormally decreased angle of inclination, it occurs in fractures of the neck of the femur and slipping of the femoral epiphysis )
Coxa valga (abnormally increased angle of inclination, in cases of congenital dislocation of the hip)
Normal angle of inclination 1250-1300

Coxa VaraCoxa Valga
ANGLE OF INCLINATION

Articulations of the Hip and PelvisPubic Symphysis
Interpubic diskSome movement

Articulations of the Hip and PelvisPubic SymphysisSacroiliac Joints

Articulations of the Hip and PelvisPubic SymphysisSacroiliac JointsHip Joints

Ligamentous and Cartilogenous Structures for the Hip and Pelvic Girdle
Sacroiliac JointHip Joint
CapsuleThree thickenings
of the capsule Iliofemoral Pubofemoral Ishiofemoral
Ligamentum TeresInguinal

ButtockSupericialGluteus MaximusGluteus Medius – reverse actionGluteus MinimusTensor Fascia Latae – iliotibial band,
functional considerations“Gower’s” SignPositive Trendelenburg

Gluteus Maximus


Gluteus Medius and Minimus

G Med., G Min, TFL




Trendelenburg

Deep Buttocks“External Rotators of the Hip”Small Muscles Mostly attach near or on greater trochanterExcellent mechanical advantage for 1)
producing external rotation and 2) to help maintain stability of the hip
All but one innervated by named nerves specific to one or two of them
The exception is the obturator externus – innervated by posterior brach of obturator n.

Deep ButtockMuscles:PiriformisSuperior GemellusObturator InternusInferior GemellusQuadratus FemorisObturator Externus

Deep Muscles of Buttocks

Hip MusclesAnterior
Rectus FemorisSartoriusIliopsoas Muscle
Group Iliacus Psoas Major

Hip MusclesAnterior
Rectus FemorisSartoriusIliopsoas Muscle
Group Iliacus Psoas Major

Hip MusclesPosterior
SemimembranosusSemitendinosusBiceps FemorisGluteus Maximus

Hip MusclesMedial
Adductor BrevisAdductor LongusAdductor MagnusPectineusGracilus

Hip MusclesLateral
Gluteus MediusGluteus MinimusTensor Fascia LataSix Intrinsic External
Rotators Periformis Quadratus Femoris Obturator Internus Obturator Externus Gemellua Superior Gemellus Inferior

Hip MusclesLateral
Gluteus MediusGluteus MinimusTensor Fascia LataSix Intrinsic External
Rotators Periformis Quadratus Femoris Obturator Internus Obturator Externus Gemellua Superior Gemellus Inferior

Femoral Triangle
BordersSuperiorLateralMedialPosteriorAnterior
Structures

Movements of the PelvisForward and Backward TiltLeft and right Lateral TiltLeft and Right Rotation

Kinematics of the Hip JointPelvic-on-Femoral Osteokinematics:
Abduction and Adduction in the Frontal PlaneRight lateral tilt and left lateral tilt

The Hip and Pelvic GirdleA. General Structure & FunctionB. Structure & Function of Specific JointsC. Muscular ConsiderationsD. Specific Functional ConsiderationsE. Common Injuries

Muscular Considerations: Sagittal Plane Pelvic Motion1. Pelvic-on-Femoral Flexion: Anterior Pelvic Tilt
Force coupleHip flexors Lower trunk extensors

Muscular Considerations: Sagittal Plane Pelvic Motion1. Pelvic-on-Femoral Flexion: Posterior Pelvic Tilt
Force coupleHip extensors Lower trunk flexors

Muscular Considerations: Overall Function of the Hip Flexors2. Femoral-on-Pelvic Hip Flexion
synergy between hip flexors and abdominal muscles

Muscular Considerations: Extensors
Pelvic-on-Femoral
Hip Extension

Muscular Considerations: Hip AdductorsHip AdductionPelvic Action?Muscles being
utilized?

Primary Movements of the Pelvis as Performed in a Standing Position
Pelvis Spinal Joints Hip Joints
Forward Tilt Hyperextension Slight Flexion
Backward Tilt Slight Flexion Complete Ext.
Lateral Tilt Left Slight Lateral Flexion RT
R = ADD
L= ABD
Rotation Left Rotation RT R = Slight ER
L= Slight IR

Movements of the Pelvis Secondary to those of the SpineSpine Pelvis
Flexion Posterior Tilt
Hyperextension Anterior Tilt
Lateral Flex Left Lateral Tilt Left
Rotation Left Rotation Left

Frolich, Human Anatomy, Lower LImb
Lumbar plexus (femoral nerve)
Sacral plexus (sciatic nerve)
With leg out to side like quadruped, lumbar-anterior, sacral-posterior makes sense




AP PELVIC ARTERIOGRAM1. ABDOMINAL
AORTA
2. COMMON ILLIAC ARTERY
3. INTERNAL ILLIAC ARTERY
4. EXTERNAL ILLIAC ARTERY
5. COMMON FEMORAL ARTERY
6. LUMBAR ARTERY
1
4
6
2
3
5

External iliac arteryInguinal ligamentCommon femoral arteryProfunda femoris
arterySuperficial femoral
artery
477
Anterior Thigh

Common femoral art
Profunda femoris art
Superficial femoral art

Frolich, Human Anatomy, Lower LImb
Internal Iliac Cranial + Caudal Gluteals= gluteals Internal Pudendal = perineum, external
genitalia Obturator = adductor muscles
External Iliac Femoral = lower limb
• Deep femoral = adductors, hamstrings, quadriceps
Popliteal (continuation of femoral) • Geniculars = knee• Anterior Tibial = ant. leg muscles, further
branches to feet• Posterior Tibial = flexor muscles, plantar
arch, branches to toes


Blood Supply to Femoral Head
1. Artery of Ligamentum Teres• Most important in children.• Its contribution decreases with age,
and is probably insignificant in elderly patients.

Blood Supply to Femoral Head
2. Ascending Cervical Branches Arise from ring at base of neck. Ring is formed by branches of medial and lateral
circumflex femoral arteries. Penetrate capsule near its femoral attachment
and ascend along neck. Perforate bone just distal to articular cartilage. Highly susceptible to injury with hip dislocation.


Common InjuriesDislocation-femoral head moves out of the
acetabulum-usually it goes posterior into
notch-position typically flexion,
adduction, and internal rotation-common mechanism: knee to
dashboard during traffic collision-signs and symptoms: extreme
pain, obvious deformity, unwilling to move the extremity

Hip Dislocation: Mechanism of Injury
Almost always due to high-energy trauma.Most commonly involve unrestrained
occupants in MVAs.Can also occur in pedestrian-MVAs, falls
from heights, industrial accidents and sporting injuries.


COMMON INJURIESHip Fracture-most frequently occurs through the femoral
neck-a direct blow to the lateral hip-signs and symptoms: pain, swelling, and loss
of function-the involved leg will appear shortened and will
be externally rotated


INTERTROCHANTERIC FRACTURE

COMMON INJURIESAvascular Necrosis of the Femoral Head-blood supply to the femur head is severed or is
occluded for a prolonged period of time.-this is a common complication following hip
dislocations, fractures, and chronic synovitis and often necessitates a hip replacement


POST OPERATIVE REPAIR

COMMON INJURIESPiriformis Syndrome-sciatic nerve through piriformis-pressure on the sciatic nerve due to muscle
spasm, trigger points, or tightness causing posterior thigh pain
-other signs and symptoms: pain, limited ROM, pt tenderness deep to the gluteals



COMMON INJURIESTrochanteric Bursitis-cause is abnormal friction or irritation of
the bursa between the IT band and greater trochanter, direct blow, or improper biomechanics
-usually a sport such as running-signs and symptoms: local pain, swelling,
pt tenderness, and crepitus over the greater trochanter
-patient may complain of hip snapping



COMMON INJURIESIschial Bursitis-lies over the ischial tuberosity-may become painful and inflamed with
excessive friction-signs and symptoms: pain with sitting, pt
tenderness over ischial tuberosity, pain w/ passive hip flexion and active/resistive hip extension
-often difficult to differentiate from proximal hamstring tendinitis




COMMON INJURIESHip Joint Sprain-less common-excessive forcible exertion of the extremity
that stretch or tear the surrounding ligaments
-signs and symptoms: pain and decrease ROM

COMMON INJURIESHip Joint Strains-resulting from overstretching or from a rapid,
forceful contraction of the muscle-explosive starts and slipping of the foot during
cutting are common mechanisms for hip flexor and adductor strains
-these injuries frequently occur during the beginning of practice and preseason training
-signs and symptoms: pain, pt tenderness, muscle spasm, swelling, ecchymosis , and decreased ROM

COMMON INJURIESLegg-Calve-Perthes Disease-characterized by avascular necrosis of the
proximal femoral epiphysis-a chronic condition that develops slowly in
children-more often in males than in females-signs and symptoms: pain in the hip or groin
that radiates to the knee, limping, decreased ROM, and hip flexor tightness may be noted
-physician should be consulted to rule out serious pathologies such as this



COMMON INJURIESChronic Synovitis-inflammatory process at the hip that is
characterized by chronic irritation and excess secretion of synovial fluid within the capsule
-this condition is very difficult to detect-may lead to avascular necrosis of the femoral
head

ORIF
Hemi
THR

Hips
The End


Recommended