
DIGITAL HEALTH TECHNOLOGY wellness
patient-centred care
Dr Gareth Kantor
Private Practice Anaesthetist
Hon Lecturer, University of Cape Town
Assistant Professor, Case Western Reserve University, Cleveland, OH, USA
Clinical Consultant – Discovery Health, Insight

Disclosures
Paid Consultant to Insight, Discovery
No commercial interests in technologies
Opinions are my own

vanishing hospitals
wearable and implantable sensors
predict heart attacks
Artifical Intelligence diagnosis of....
remote diagnosis of infections
http://techonomy.com/2016/11/at-techonomy-2016-a-vision-of-disrupted-healthcare/
unlimited advances
Dr. Eric Topol

“DIGITAL HEALTH”

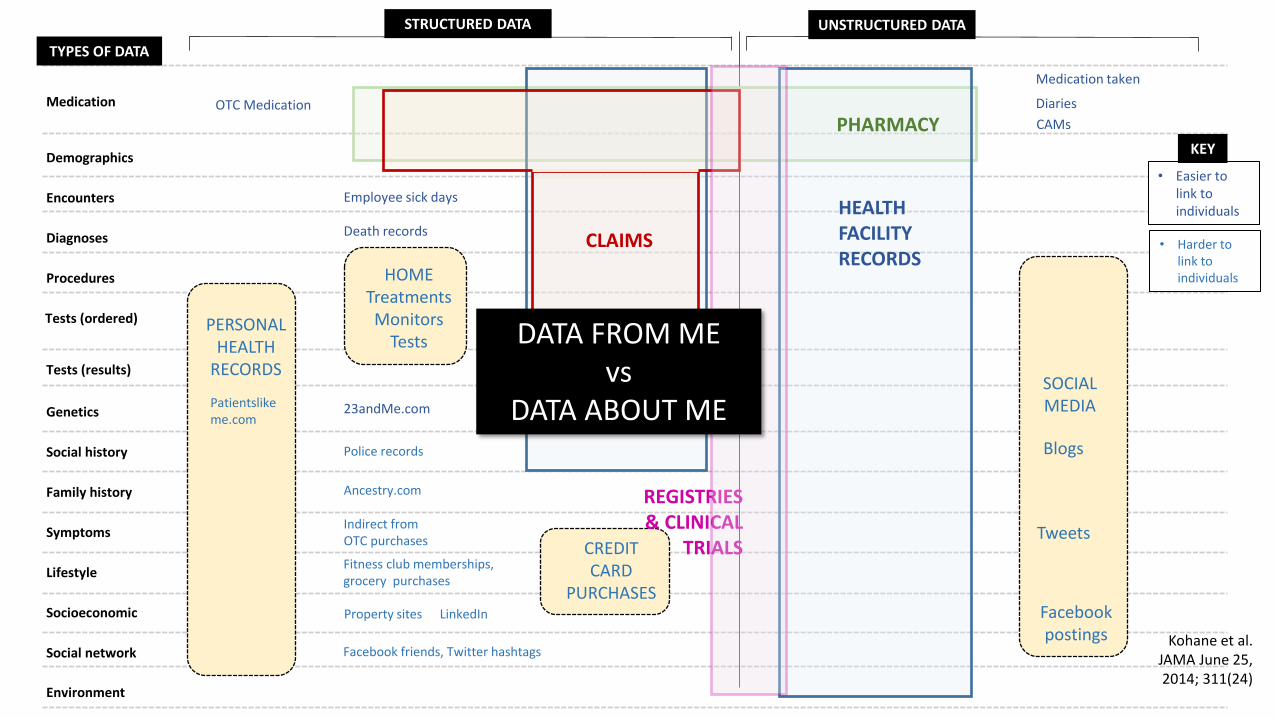
TYPES OF DATA
Medication
Demographics
Encounters
Diagnoses
Procedures
Tests (ordered)
Tests (results)
Genetics
Social history
Family history
Symptoms
Lifestyle
Socioeconomic
Social network
Environment
STRUCTURED DATA UNSTRUCTURED DATA
Medication filled
Medication instructions
Allergies
Out-of-pocket expenses
Chief complaint
Differential diagnosis
DIGITAL NOTES
REPORTS
PHYSICAL EXAMINATIONS
PAPER NOTES
TRACINGS IMAGES
Medication prescribed
Dose Route
NAPPI ATC
HL7
Visit type and time
SNOMED ICD-10
CPT RPL
LOINC
ECG
Lab values, vital signs
SNPs, NGS
Tobacco/alcohol use
Pathology
Radiology
HEALTH FACILITY RECORDS
PHARMACY
CLAIMS
REGISTRIES & CLINICAL
TRIALS
• Easier to link to individuals
KEY
Kohane et al. JAMA June 25, 2014; 311(24)

HEALTH FACILITY RECORDS
PHARMACY
REGISTRIES & CLINICAL
TRIALS
CLAIMS
MUCH MORE DATA
HEALTH FACILITY RECORDS
80-90% unstructured

TYPES OF DATA
Medication
Demographics
Encounters
Diagnoses
Procedures
Tests (ordered)
Tests (results)
Genetics
Social history
Family history
Symptoms
Lifestyle
Socioeconomic
Social network
Environment
CREDIT CARD
PURCHASES
STRUCTURED DATA UNSTRUCTURED DATA
OTC Medication
Medication taken
Diaries
CAMs
Police records
Ancestry.com
Indirect from OTC purchases
Fitness club memberships, grocery purchases
Property sites LinkedIn
Facebook friends, Twitter hashtags
23andMe.com
Employee sick days
Death records
• Easier to link to individuals
KEY
• Harder to link to individuals
Kohane et al. JAMA June 25, 2014; 311(24)
PERSONAL HEALTH
RECORDS
Patientslikeme.com
HOME Treatments Monitors
Tests
SOCIAL MEDIA
Blogs
Tweets
Facebook postings
HEALTH FACILITY RECORDS
PHARMACY
REGISTRIES & CLINICAL
TRIALS
CLAIMS
HEALTH FACILITY RECORDS


Doctor “Old”
Medicine Patient
Doctor Evidence-based
MEDICINE Patient
“Evidence” science: what works (population level)

https://www.cbinsights.com/blog/digital-health-medicine-market-map-company-list/


13 Topol E. Individualized Medicine from Prewomb to Tomb. Cell 157 (2014): 241–253

Adapted from: Melanie Swan, MS Futures Group
Genome
Microbiome
Transcriptome
Metabolome
Proteome
Exposome
Personal Health History
Family Health History
Lab Tests
Demographics
Questionnaires
Apps
Devices / Sensors
Images
Traditional Data Quantified Self ‘Omics
>165,000 apps (2015)
INTERNET OF THINGS
IMSHealth 2015

“Discover the right app from a curated, evidence-based selection and immediately ‘prescribe’ it directly to a patient’s mobile device.”

“Your phone will be the repository of your medical record, the means by which you collaborate with your provider, and the vehicle for submission of data to your care team.”
The desktop is dead. The phone is the future.
John Halamka, CIO, Beth Israel Deaconess Medical Center
DIY cellphone. David Mellis MIT

Cell 163, 1079–1094, November 19, 2015

Dietary Interventions Induce Consistent
Alterations to the Gut Microbiota Composition
High Interpersonal Variability in the
Postprandial Glycemic Response to the Same Meal
Cell 163, 1079–1094, November 19, 2015

“approaches that grade
dietary ingredients as
universally ‘good’ or ‘bad’
based on their average
PPGR in the population may
have limited utility for an
individual.”
Cell 163, 1079–1094, November 19, 2015

MEDICAL GRADE DEVICES
(FDA-approved)
AbStats
Proteus
AliveCor
GENERAL WELLNESS DEVICES
Fitbit
Apple Watch

PERSONAL SMOKING
CESSATION THERAPY

‘P4 MEDICINE’
predictive
preventive
personalized
participatory
“technoscientific holism”
each person’s whole life process is quantifiable and
controllable
‘the medicalization of health and life itself’
Med Health Care and Philos (2016) 19:307–323
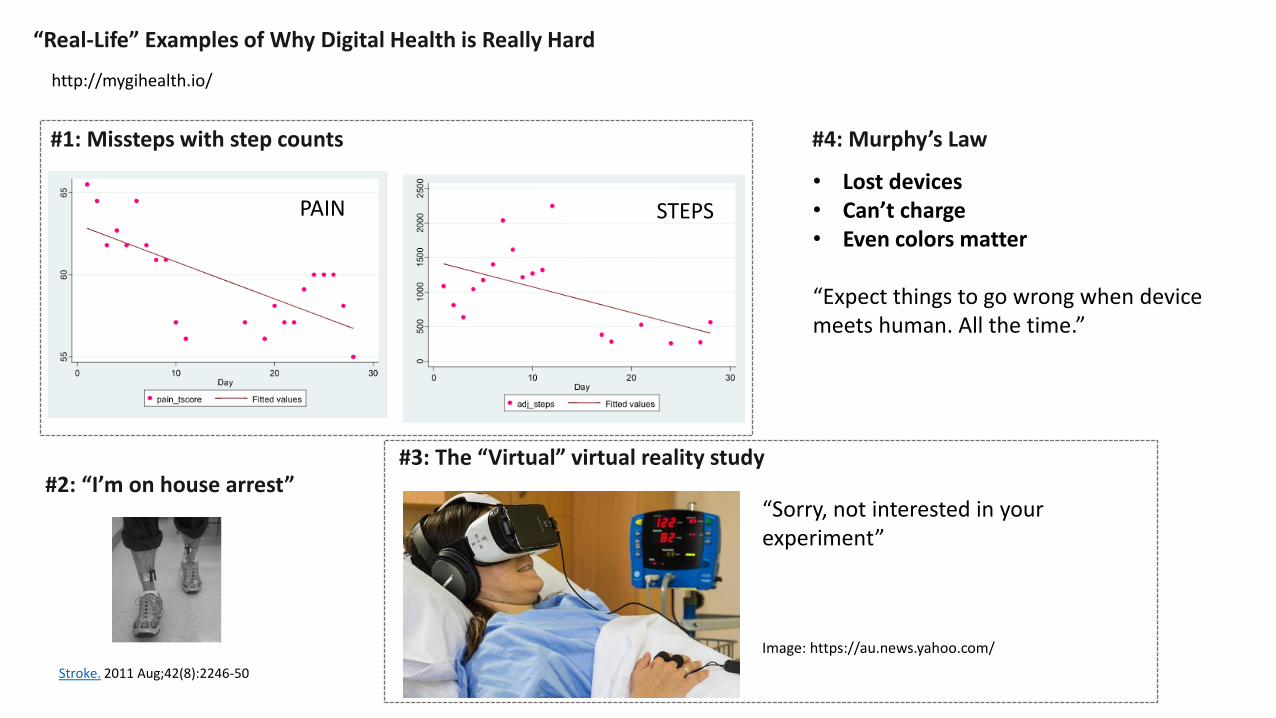
http://mygihealth.io/
“Real-Life” Examples of Why Digital Health is Really Hard
#1: Missteps with step counts
#2: “I’m on house arrest” #3: The “Virtual” virtual reality study
#4: Murphy’s Law
“Sorry, not interested in your experiment” Image: https://au.news.yahoo.com/
• Lost devices • Can’t charge • Even colors matter
“Expect things to go wrong when device meets human. All the time.”
STEPS PAIN
Stroke. 2011 Aug;42(8):2246-50

Top 10 Reasons Doctors Fear Digital Health
1. TIME
2. LIABILITY
9. EVIDENCE
4. COST
5. GENERATION GAP
6. SECURITY
7. WRONG PROBLEM
8. HYPE
3. BEHAVIOUR
Dr. Brennan Spiegel

“there are not large short-term increases or decreases in health care costs or utilization associated with monitoring chronic health conditions using mobile health or digital medicine technologies” Bloss et al. (2016). PeerJ 4:e1554; DOI 10.7717/peerj.1554

10. VALUE
Five themes in 2016: 1. Beyond step counting 2. Better design
3. Smart clothing 4. Advancing sensor technology 5. Reimbursement constraints
Wearables Weekly
Gillian Christie

https://www.youtube.com/watch?v=cFyd2Xdx-L8
Ezekiel Emanuel. Techo-Skeptic: Being Realistic About How Technology Will Improve Healthcare.
Engage Get data Transmit
data
Use data in a healthcare
system
Enable sustained behavior change
Behavior change leads
to health improvement
Improvement saves money

eHealth has unique capability to solve the challenges of making the health system safe, effective and sustainable
Enrico Coiera
“e-HEALTH EXCEPTIONALISM”
eHealth is indeed powerful but just like any other system intervention, it faces huge system barriers

Start with the problem we want to solve rather
than the technology we want to build
Enrico Coiera

• 6% of public hospitals and clinics met 70% pass mark - Office of Health Standards Compliance
• State sector: R35 – 49 billion owed / claimed
• R650K obstetrics premiums
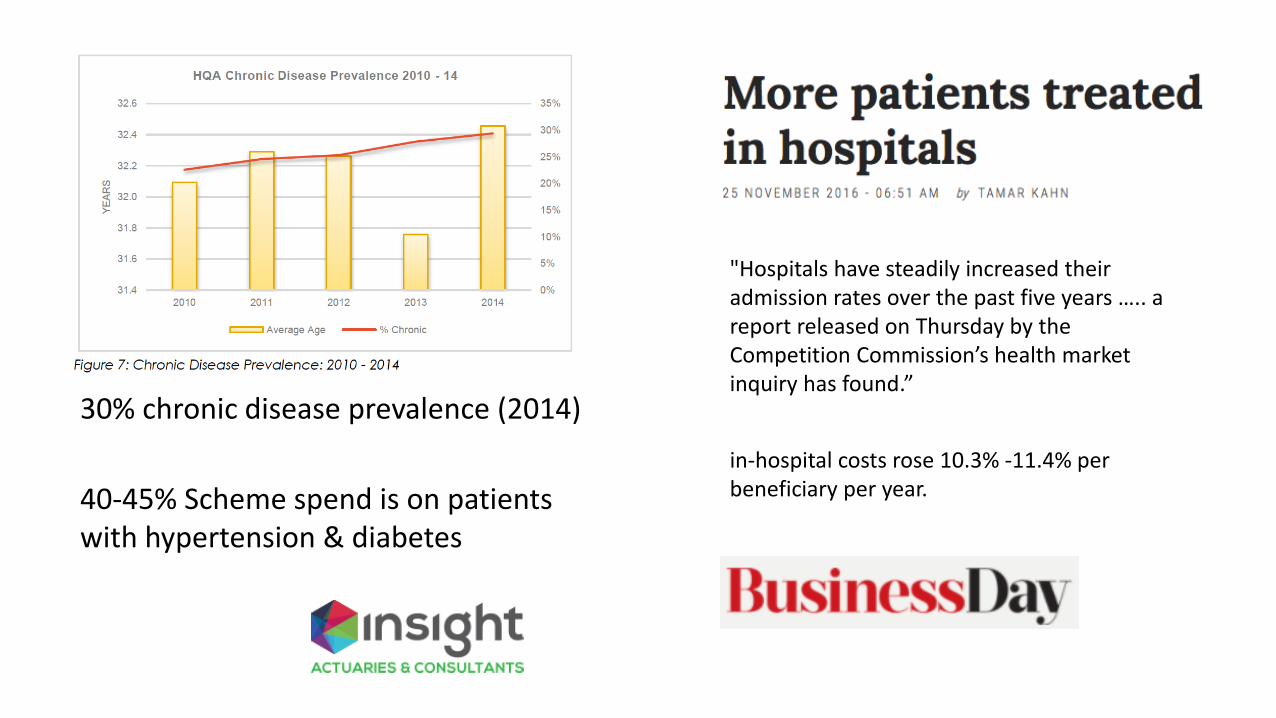
30% chronic disease prevalence (2014)
40-45% Scheme spend is on patients with hypertension & diabetes
"Hospitals have steadily increased their admission rates over the past five years ….. a report released on Thursday by the Competition Commission’s health market inquiry has found.”
in-hospital costs rose 10.3% -11.4% per beneficiary per year.

Best Care at Lower Cost: The path to continuously learning health care in America. National Academies Press

Time and motion study of ~150 primary care encounters (doctor-patient)
Christian Terwiesch , Wharton School . The efficiency of primary care http://www.youtube.com/watch?v=q9nw9IzFjBA#t=843

Status quo
EXTENDER DOCTOR
ONSITE
REMOTELY
150 episodes categorised by experienced primary care doctors viewing the videotapes
Christian Terwiesch, Wharton School . The efficiency of primary care http://www.youtube.com/watch?v=q9nw9IzFjBA#t=843

Status quo Extender onsite
e.g. discuss weight loss
Emails and follow-up calls
e.g. do you want to come in for your follow-up appointment or talk on the
phone?
Extender calls
e.g. do you need refills
EXTENDER DOCTOR
ONSITE
REMOTELY
Christian Terwiesch, Wharton School . The efficiency of primary care http://www.youtube.com/watch?v=q9nw9IzFjBA#t=843

Status quo Extender onsite
e.g. discuss weight loss
Emails and follow-up calls
e.g. do you want to come in for your follow-up appointment or talk on the
phone?
Extender calls
e.g. do you need refills?
EXTENDER DOCTOR
ONSITE
REMOTELY
19% 3%
59% 18%
22%
78%
78% 21%
Christian Terwiesch , Wharton School . The efficiency of primary care http://www.youtube.com/watch?v=q9nw9IzFjBA#t=843


• 27.0% direct clinical face time • 49.2% time EHR and desk work
• 1 hr clinical face time : 2 hr EHR/desk work • 1-2 hours personal time each night
computer/clerical work

Registrars
13-16%
“The finding that concerned us most was the small amount of time spent with patients.”
Medical Registrars
42-45%
20%
“spent surprisingly little time with patients” …this amount of time was less than we predicted and hoped it would be.”
J Gen Intern Med. 2013;28(8):1042-1047
Czernik. JAMA June 14, 2016 315(22)
N Engl J Med 1961;264(9):439-443
1959 1988 2012 Medical Registrars
40% with computer
12%
“spent a minority of time directly caring for patients … which may affect the quality of the patient-physician relationship and the quality of care delivered.”
Context
Time clerking
Time with patients

Primary care is incredibly inefficient for patients!
Christian Terwiesch , Wharton School . The efficiency of primary care http://www.youtube.com/watch?v=q9nw9IzFjBA#t=843
4h


PATIENTS
Opened at least one note > 80%
Better understanding of health and medical conditions Taking better care of themselves Doing better with taking meds Feeling more in control
> 2/3
Shared a note with someone else ~ 20%
Availability of notes would influence choice of providers
> 85%
Confused, worried, or offended by what they read
1-8%
PHYSICIANS
More time answering patient questions outside of visits
3%
More time writing or editing notes 11%
Email volume No change
Changed the way they wrote about cancer, mental health, substance misuse, or obesity
~ 20%
Opted to continue 99%
BMJ February 10, 2015;350:g7785 NEJM 2014; 370:6-8
TYPES OF DATA
Medication
Demographics
Encounters
Diagnoses
Procedures
Tests (ordered)
Tests (results)
Genetics
Social history
Family history
Symptoms
Lifestyle
Socioeconomic
Social network
Environment
CREDIT CARD
PURCHASES
STRUCTURED DATA UNSTRUCTURED DATA
OTC Medication
Medication taken
Diaries
CAMs
Police records
Ancestry.com
Indirect from OTC purchases
Fitness club memberships, grocery purchases
Property sites LinkedIn
Facebook friends, Twitter hashtags
23andMe.com
Employee sick days
Death records
• Easier to link to individuals
KEY
• Harder to link to individuals
Kohane et al. JAMA June 25, 2014; 311(24)
PERSONAL HEALTH
RECORDS
Patientslikeme.com
HOME Treatments Monitors
Tests
SOCIAL MEDIA
Blogs
Tweets
Facebook postings
HEALTH FACILITY RECORDS
PHARMACY
REGISTRIES & CLINICAL
TRIALS
CLAIMS
HEALTH FACILITY RECORDS
DATA FROM ME vs
DATA ABOUT ME

Patient
Experience
Social
Media
Functional &
Quality Life
Measures
Patient-reported
Outcomes
Measures
Special Purpose
Surveys
Real-time
Assessment
(SMS)

Doctor PRECISION MEDICINE Person
Phenotype Genotype
Evidence
Decision Support
still evidence-based
• social/behavioural • engagement/activation
• human • computer
Preferences Values Goals
Care System


Framework for Clinical Excellence

• Solve real problems
• Avoid blind faith in data, big or small
• FOCUS ON.. • Flow • Teams
• PARTNERSHIP • People
“Just because e-Health is hard does not mean we can ignore it”.
Enrico Coiera
Image: Healthcare IT News

I understand all aspects of my care.
My doctors communicate with each other about my care.
My care system shares and receives information to improve care for me and others.
I can easily access information about health care that is valuable to me.
CARE SYSTEM
PUBLIC
Image: www.dreamstime.com


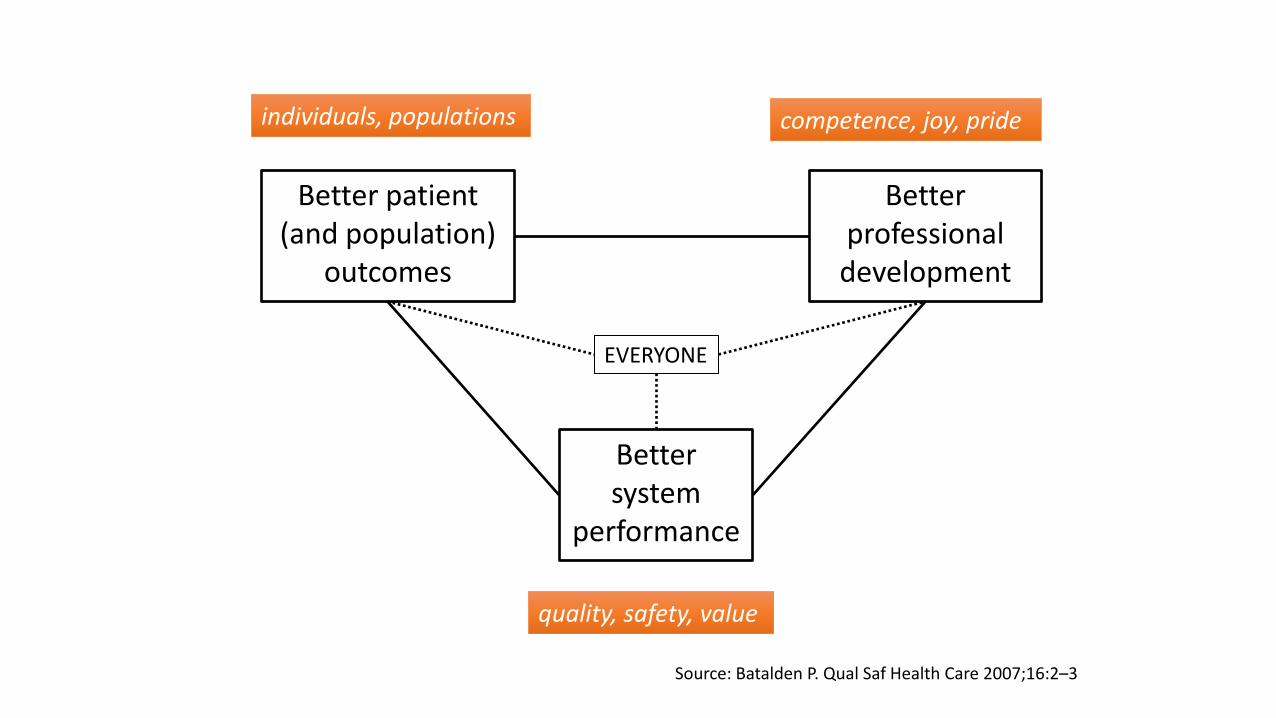
quality, safety, value
competence, joy, pride individuals, populations
Adapted from: Batalden P. Qual Saf Health Care 2007;16:2–3
Better patient (and population)
outcomes
Better system
performance
Better professional development ?
? ?

Framework for Clinical Excellence



TYPES OF DATA
Medication
Demographics
Encounters
Diagnoses
Procedures
Tests (ordered)
Tests (results)
Genetics
Social history
Family history
Symptoms
Lifestyle
Socioeconomic
Social network
Environment
CREDIT CARD
PURCHASES
STRUCTURED DATA UNSTRUCTURED DATA
OTC Medication
Medication taken
Diaries
CAMs
Medication filled
Police records
Ancestry.com
Indirect from OTC purchases
Fitness club memberships, grocery purchases
Property sites LinkedIn
Facebook friends, Twitter hashtags
23andMe.com
Employee sick days
Death records
Medication instructions
Allergies
Out-of-pocket expenses
Chief complaint
Differential diagnosis
DIGITAL NOTES
REPORTS
PHYSICAL EXAMINATIONS
PAPER NOTES
TRACINGS IMAGES
Medication prescribed
Dose Route
NAPPI ATC
HL7
Visit type and time
SNOMED ICD-10
CPT RPL
LOINC
ECG
Lab values, vital signs
SNPs, NGS
Tobacco/alcohol use
Pathology
Radiology
HEALTH FACILITY RECORDS
PHARMACY
CLAIMS
REGISTRIES & CLINICAL
TRIALS
• Easier to link to individuals
KEY
• Harder to link to individuals
Kohane et al. JAMA June 25, 2014; 311(24)
PERSONAL HEALTH
RECORDS
Patientslikeme.com
HOME Treatments Monitors
Tests
SOCIAL MEDIA
Blogs
Tweets
Facebook postings
DATA FROM ME vs
DATA ABOUT ME

GOOGLE GLASS
DIGITAL PAPER DIGITAL PEN
VOICE RECOGNITION
NATURAL LANGUAGE PROCESSING
MEDICAL SCRIBE
CONCEPT ENGINE-DRIVEN INTERFACE

In 1959, Payson et al lamented that the
intern was spending “barely enough time
with his patient to establish an
acquaintance, much less a relation.”
For the first time, these moments of indirect care can
become opportunities for patient education and shared
decision-making.
While some may worry that this will lead to less eye
contact and further harm to the patient-physician
relationship, there are data that show that, used
effectively, computers can improve patient-physician
communication.
The EHR allows us an
unprecedented opportunity: the
ability to take some of that
“indirect patient care,” work
previously done trapped in
radiology reading rooms and
hovering over charts at nursing
stations, and move it to the
bedside.
Czernik, Z. JAMA June 14, 2016 Volume 315, Number 22
In an observational study of outpatient
visits, Frankel and colleagues7 found that physicians were
able to use computer screens to share information
visually, clarify assessments, and engage patients
effectively. Based on his earlier data as
well as the work of others, Frankel8 recently proposed a
standardized practice for enriching patient-physician
communication using the computer.
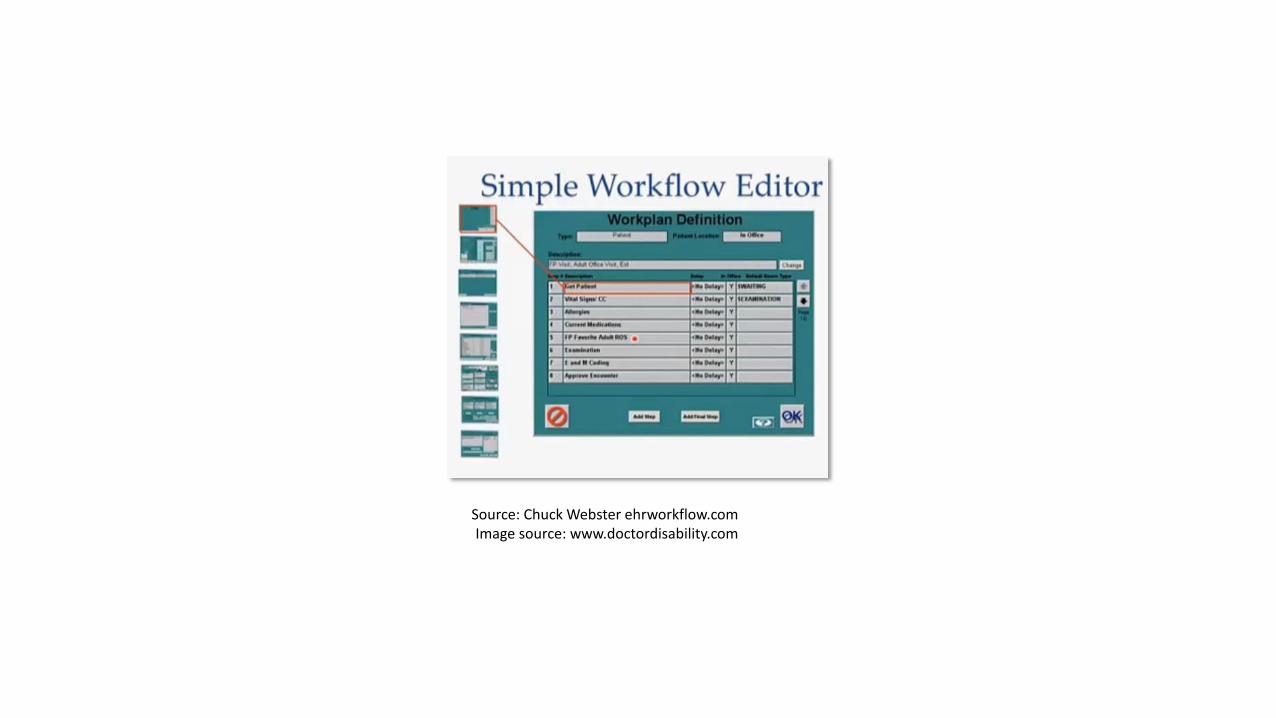
Source: Chuck Webster ehrworkflow.com Image source: www.doctordisability.com



• $$$ oWho pays vs. who benefits
oVolume-based payment (FFS)
• Value (process improvement)
• Leadership
• Design (usability)
• Interoperability
• Evidence
• “Ethics”
quality, safety, value
competence, joy, pride individuals, populations
Source: Batalden P. Qual Saf Health Care 2007;16:2–3
Better patient (and population)
outcomes
Better system
performance
Better professional development
EVERYONE

PATIENT DATA
PRACTICE DATA
Ownership Access
Control of access
“CARE SYSTEM”
etc

• 12 month study at 3 sites - urban and rural • 105 primary care physicians and >19 000 patients
BMJ February 10, 2015;350:g7785 NEJM 2014; 370:6-8
After a visit, secure message to the patient: the note is available
Patient can log in to secure portal and read the note
Before the next scheduled visit, message encourages patient to review the note
0
2 000
4 000
6 000
8 000
10 000
12 000
14 000
16 000
100
700
1 3
00
1 9
00
2 5
00
3 1
00
3 7
00
4 3
00
4 9
00
5 5
00
6 1
00
6 7
00
7 3
00
7 9
00
8 5
00
9 1
00
9 7
00
10 3
00
10 9
00
11 5
00
12 1
00
12 7
00
13 3
00
13 9
00
14 5
00
15 1
00
15 7
00
16 3
00
16 9
00
17 5
00
18 1
00
18 7
00
19 3
00
19 9
00
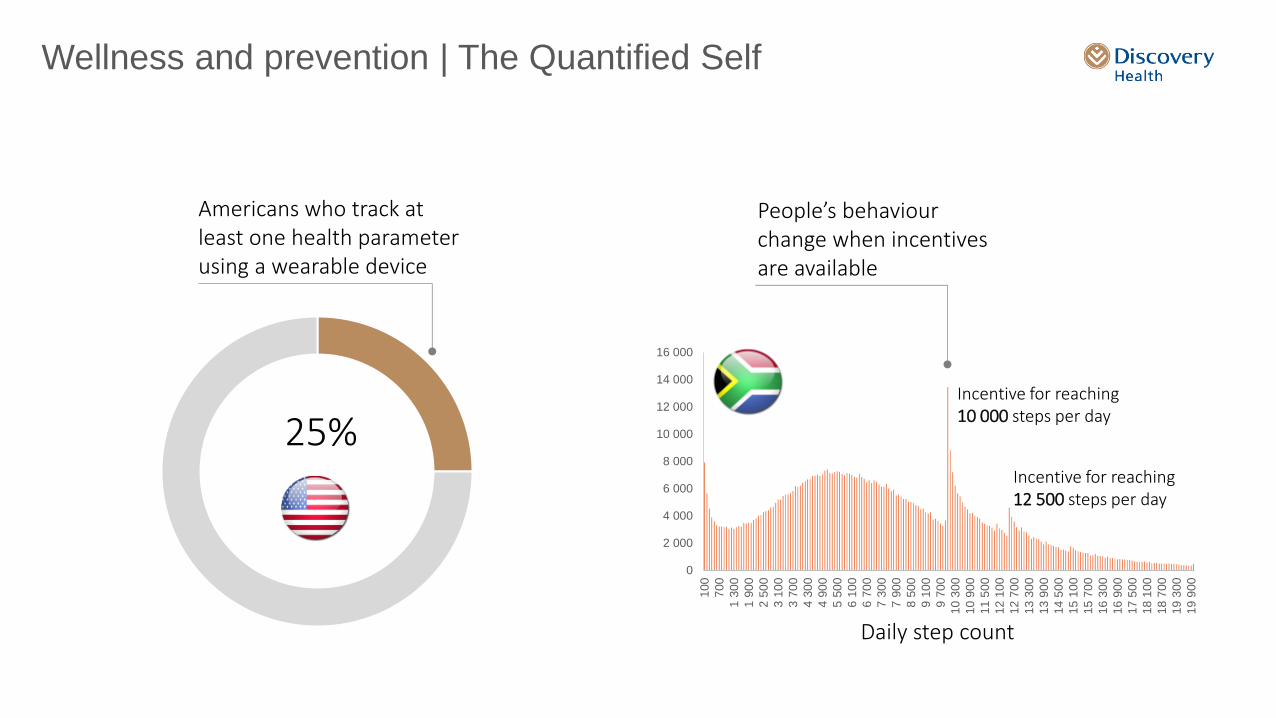
Wellness and prevention | The Quantified Self
Americans who track at least one health parameter using a wearable device
25%
People’s behaviour change when incentives are available
Daily step count
Incentive for reaching 10 000 steps per day
Incentive for reaching 12 500 steps per day

Management of chronic conditions
No technological intervention With technological intervention
Contact with the health system is limited to a doctor’s visit 3 or 4 times per year
Portable or wearable bio-sensors can capture biometric data between provider visits and over extended time periods for review and action by patients, their doctors and health care teams
Range of measurements potentially available:
• blood pressure • heart rate and rhythm • heart rate variability • cardiac output • stroke volume • respiratory rate • oxygen saturation and
air flow • sleep pattern
• galvanic skin response • body temperature • intraocular pressure • blood glucose • brain waves • intracranial pressure • muscle movements • falls

Electronic Health Records can help us work smarter, not harder
What we really need is not technology that replaces doctors, but technology enabled health systems that enhance quality, alter the cost curve, support practitioners and do not get in the way of the human touch
Medication history Telemetric Glucose
Monitoring Treatment timeline Episode of care

Technology exposes us to an exciting new world
It can either be seen as a…
Threat
Opportunity

Source: Brent James. Health Affairs June 2011;30(6)
1,400 clinical processes !
• Administrative systems contain 50-60% of the data needed for process improvement
e-Health → health system transformation
non condition-specific
condition-specific
related to service quality
administrative processes
104 key processes ~ 95% of clinical care

“The health care system is perfectly designed to achieve exactly the results it gets”.
Source: Paul Batalden

“Patient-Centred Medical Home”
• Continuous healing relationship • Whole person orientation
• Family and community context • Comprehensive care
Family Medicine Core Values
Practice Organisation
Health Information Technology
Quality Measures
Patient Experience
Health Information Technology
• Full patient data in electronic health records + scripting, lab results, etc
• Support coordinated care with individualised care plans
• Clinician/patient structured email interactions
• Population segmentation & management
Adapted for SA from
CLINICAL LEADERSHIP

“Patient Engagement”
Increase patient access to their health information
Enable patients to take action with their information
Shift attitudes to support patient-doctor partnership
Source: Office of the National Coordinator for Health IT
Action
Attitudes
Access

e-Health is difficult
•Complex interventions in a complex system
•What works locally may not work everywhere
•Quickly obsolete (needs change)
Source: Enrico Coiera

Not technical, sociotechnical
“The biggest information repository in most organisations [is in] the heads of those who work there….the largest communication network is the web of conversations that binds them”
Enrico Coiera

Environmental sensors can quantify and track exposure to radiation, air pollution, pollen count, pesticides in food, and other important threats to health
Sensors worn by newborns in socks or clothing can wirelessly alert parents to changes in sleep, heart rate, or breathing
Sensors that measure breath compounds such as nitric oxide or organic chemicals may enable the measurement of lung function or the diagnosis of certain cancers
Nanochips embedded in the bloodstream can potentially monitor the appearance of tumour DNA, immune activation, or genomic signals that may indicate a heart attack or stroke
A smartphone’s microphone can be used to quantify components of lung function, analyze voice quality to gauge mood or make the diagnosis of Parkinson’s disease or schizophrenia

“At once it struck me what quality went to form a Man of Achievement . . . when a man is capable of being in uncertainties, mysteries, doubts, without any irritable reaching after fact and reason.” — John Keats, December 18171
“As we move further into the 21st century, it seems clear that technology will perform the routine tasks of medicine for which algorithms can be developed. Our value as physicians will lie in the gray-scale space, where we will have to support patients who are living with uncertainty — work that is essential to strong and meaningful doctor–patient relationship”

Registrars
13-16%
<10 mins
“The finding that concerned us most was the small amount of time spent with patients.”
Medical Registrars
42-45%
20%
17-28 mins
3.5 mins
“spent surprisingly little time with patients” …this amount of time was less than we predicted and hoped it would be.”
2012 Context Medical Registrars
Time clerking 40% with computer
Time with patients 12%
Admission 10-24 mins
Follow-up in hospital 7.7 mins
“interns … spent a minority of time directly caring for patients … which may affect the quality of the patient-physician relationship and the quality of care delivered.”
J Gen Intern Med. 2013;28(8):1042-1047 Czernik. JAMA June 14, 2016 315(22)
N Engl J Med 1961;264(9):439-443
1959 1988

My speculation is that this technology and system adaptation will allow for a 5x5 improvement across healthcare. • 5x reduction in doctor work, enabling doctors to focus on patient care, research,
or new things not yet imagined. • 5x increase in research, as medicine shifts do being more data-driven and all
patients’ data is online (in a secure, anonymized way) to be used for studies. • 5x lower error rate since the majority of conditions will have computer systems
guiding them towards the correct results by default. • 5x faster diagnosis due to the advent of consumer-driven systems (diagnosis
from your home) as well as fast and sophisticated hardware and software systems replacing the current back-and-forth and communication between all the various entities of the healthcare system (not just your physician, but your nurses, PCP’s, insurers, etc…).
• And lastly, I speculate that healthcare will be 5x cheaper, although this will require a very conscious effort in ensuring we do not promote technological systems that just add on and increase the cost of care.
http://www.khoslaventures.com/wp-content/uploads/20-Percent-Doctor-Included.pdf
Recommended













![InfoWell Patient Portal: A Case of Patient-Centred Design [05 Cr2 1100 Chan]](https://img.dokumen.tips/doc/110x75/5549359cb4c905054d8b469d/infowell-patient-portal-a-case-of-patient-centred-design-05-cr2-1100-chan.jpg)




