December 2010
Patrick Farley, MD (Neuroradiology Fellow) andThomas Bouldin, MD (Neuropathologist)
Clinical Neuroradiology–Neuropathology Conference
CLINICAL HISTORY: 59-year-old man with history of altered mental status and hearing loss.
Case #1

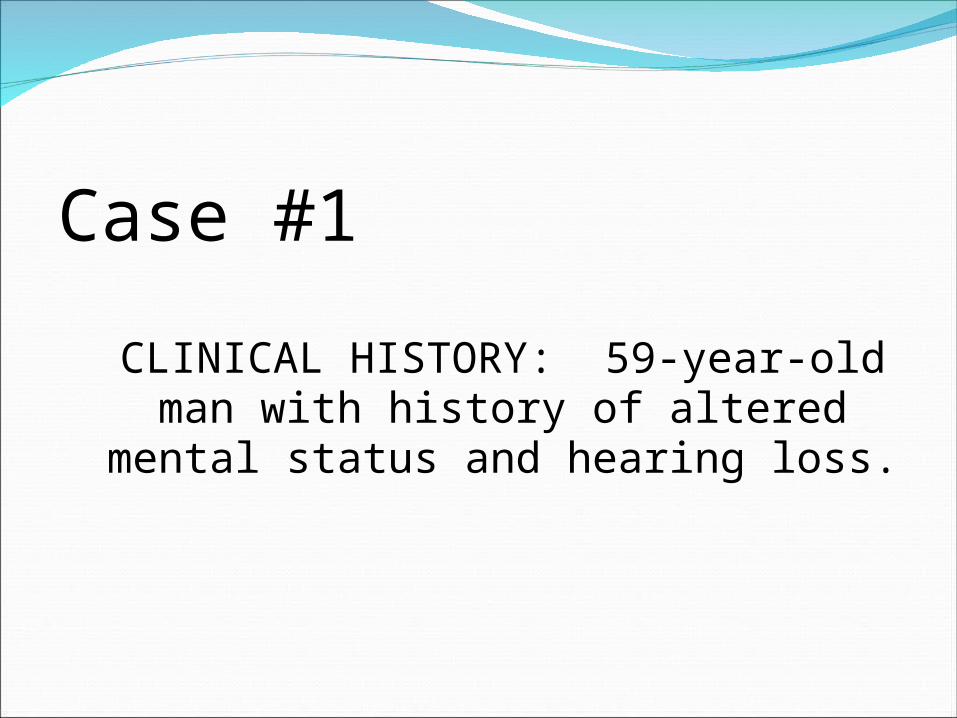
Differential diagnosis Infectious Meningitis
Neoplastic Meningitis
Breast, lung most common extracranial sources
Most common primary brain tumors are GBM, medulloblastoma, pineal tumors, and choroid plexus tumors
Neurosarcoidosis
Lacy leptomeningeal enhancement
May have ventricular or dural-based enhancing masses
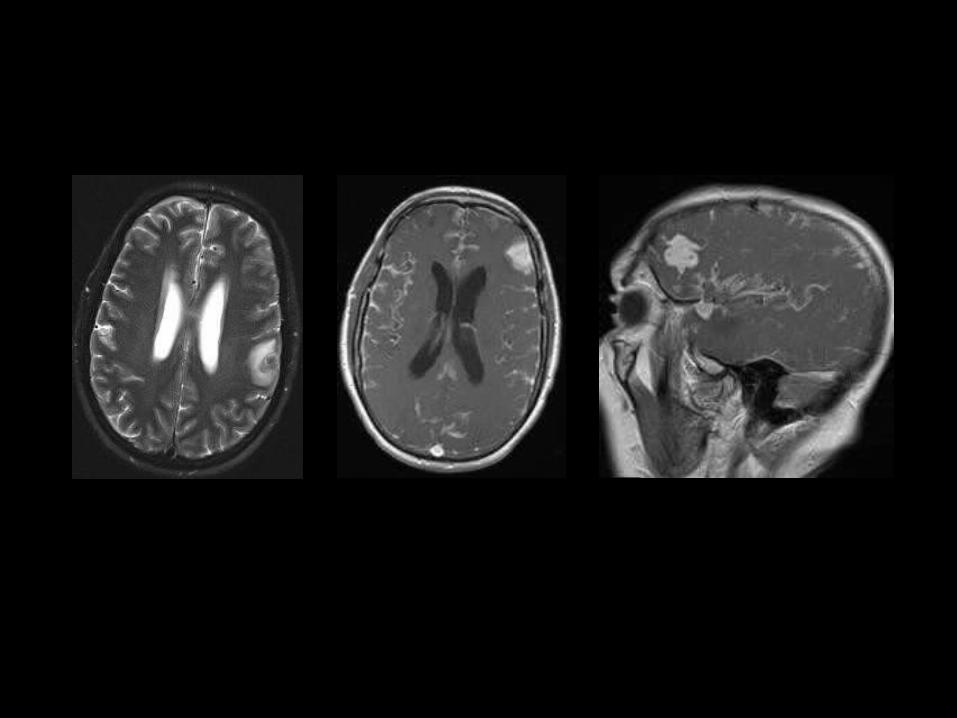
Brain biopsy revealed a poorly differentiated neoplasm within the leptomeninges and around several intracortical blood vessels. The immunophenotype of the neoplastic cells was consistent with a melanoma. The histologic features do not permit distinction between metastatic melanoma (common) and primary leptomeningeal melanoma (rare).
Case #2
CLINICAL HISTORY: 21-year-old postpartum woman with a sellar mass.


Adenoma
Pituitary hyperplasia
25–50% of females 18–35 years old have upwardly convex pituitary
Usually < 10 mm unless pregnant, lactating
Aneurysm
Usually eccentric, not directly suprasellar
Pituitary gland visible and identified as separate from mass
Flow-related artifacts on MRI are common
Meningioma
Pituitary gland may be visible and identified as SEPARATE from mass

Differential Diagnosis (continued) Metastasis
Lymphocytic hypophysitis
Can mimic adenoma clinically and on imaging studies
May show zones of very low T2 signal peripherally
Most common in peripartum female
Craniopharyngioma
Ca++, cysts more common, Children > adults
Rim/nodular > solid enhancement
May be indistinguishable from Rathke cleft cyst
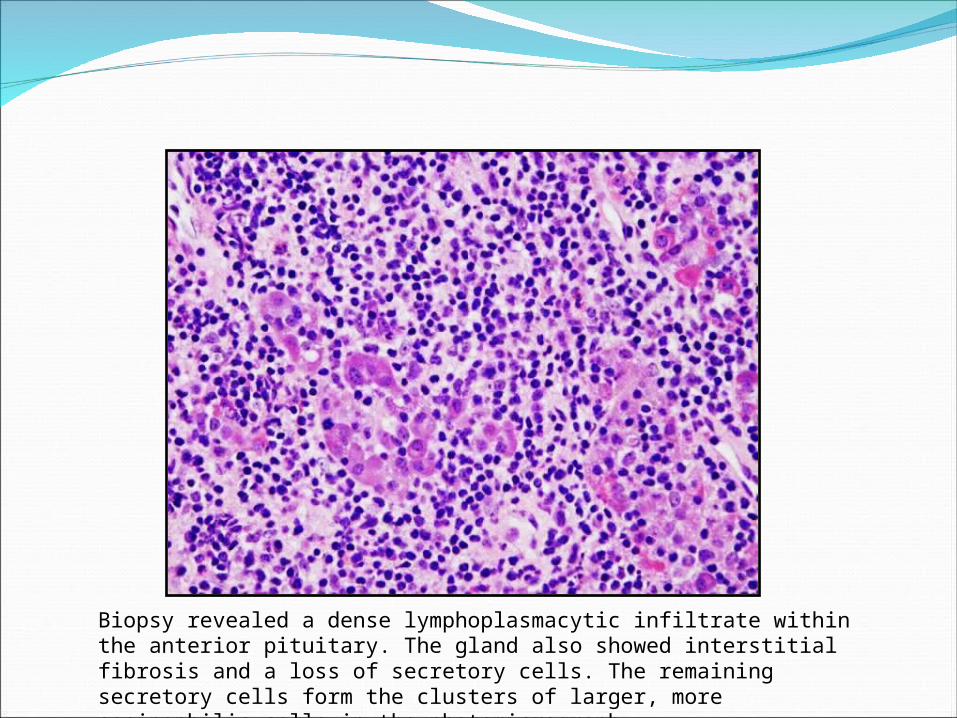
Biopsy revealed a dense lymphoplasmacytic infiltrate within the anterior pituitary. The gland also showed interstitial fibrosis and a loss of secretory cells. The remaining secretory cells form the clusters of larger, more eosinophilic cells in the photomicrograph.
Lymphocytic hypophysitis Females > males, with a ratio of approximately 5:1
Often during last months of pregnancy or first few months postpartum
Often have family history of autoimmune disease
Sometimes associated with Hashimoto’s thyroiditis or Graves’ disease
No adverse effect on fetus
Presents as hypopituitarism and/or mass effect—headache or visual field cuts
If unrecognized, may cause death from panhypopituitarism
Treatment includes hormonal replacement and surgery to reduce mass effect.

Diagnostic signs:
Thick non-tapered stalk, with or without pituitary mass
Supra, intrasellar mass
Areas of low T2 signal peripherally or/and in cavernous sinuses
Usually < 10 mm but may be up to 2-3 cm
Rounded pituitary gland with infundibulum that appears thickened, nontapering, or bulbous
Lymphocytic hypophysitis

CLINICAL HISTORY: 73-year-old female with acute headache and right-sided weakness.
CASE #3


Differential Diagnosis Hypertensive hemorrhage
Deep structures (basal ganglia, thalami, cerebellum) but may also occur in cortex and subcortical white matter
Hemorrhagic infarct
Hemorrhagic metastases
Cerebral amyloid angiopathy
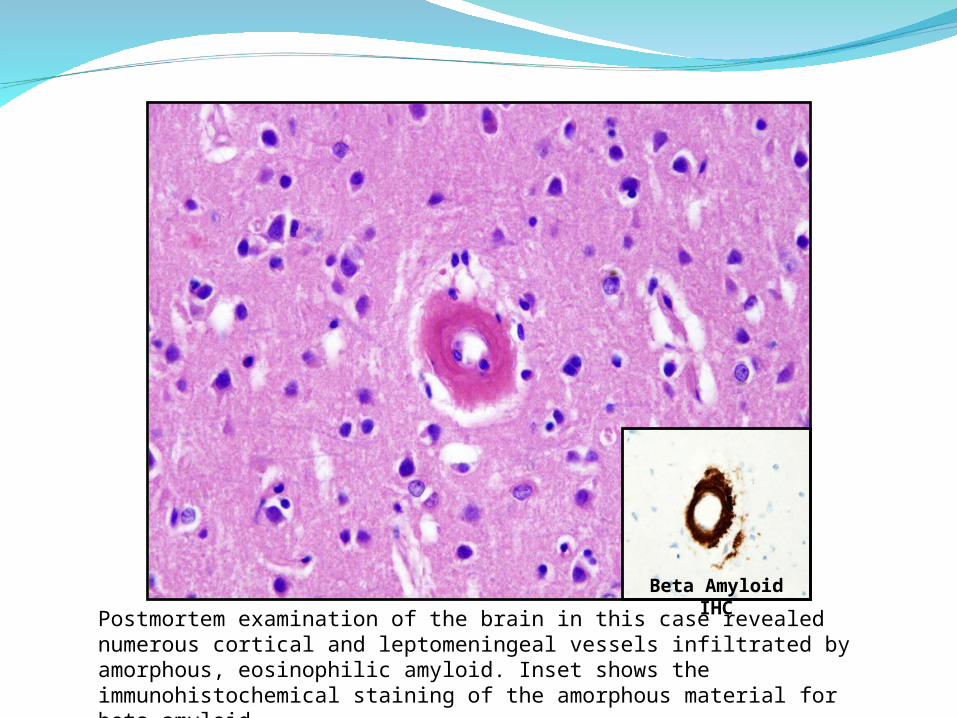
Beta Amyloid IHC
Postmortem examination of the brain in this case revealed numerous cortical and leptomeningeal vessels infiltrated by amorphous, eosinophilic amyloid. Inset shows the immunohistochemical staining of the amorphous material for beta amyloid.

Cerebral amyloid angiopathy (CAA) Deposition of beta amyloid in cortical and leptomeningeal vessels
Common in older patients
Often associated with Alzheimer’s disease
Complications of CAA include intracerebral lobar hemorrhage, microbleeds, subarachnoid hemorrhage, cerebral infarcts, inflammatory CAA, and white-matter abnormalities.

CAA Imaging Look for:
Lobar hemorrhage(s) of different ages
Multifocal areas of susceptibility artifacts corresponding to chronic microbleeds, particularly in cortex
Hemorrhage may extend to subarachnoid space or into ventricles
Acute lobar hemorrhage tends to be large
Protocol advice:
Recommend T2*-weighted sequence in all patients > 60 years of age

CLINICAL HISTORY: 65-year-old man with history of renal cell carcinoma first diagnosed in 1994. He has since had numerous surgeries for metastases to the brain. He also had stereotactic radiosurgery for an olfactory groove-based lesion, which was presumed to be a meningioma.
Case #4


CLINICAL HISTORY (continued): A few months later the presumed meningioma developed surrounding edema, became larger, and demonstrated areas of different enhancement intensity and T2 signal.
Case #4

Biopsy of the olfactory-groove lesion revealed a meningioma (right half of photomicrograph). Also present within the meningioma was a focus of metastatic renal cell carcinoma (left half of photomicrograph).

Tumor-to-tumor metastasis Metastasis of a systemic cancer to an intracranial tumor is rare.
Most often, the CNS tumor is a meningioma. Other reported types of intracranial tumors harboring a metastasis include 8th-nerve schwannoma, glioma, hemangioblastoma, and pituitary adenoma.
Breast and lung are the most common primary sites, with breast being the most common site.
Renal cell carcinoma metastatic to a meningioma has been reported only rarely. Renal cell carcinoma may also metastasize to a hemangioblastoma in the context of the von Hippel-Lindau syndrome.
Lanotte M, et al. Systemic cancer metastasis in a meningioma: Report of two cases and review of the literature. Clinical Neurology and Neurosurgery 111 (2009) 87–93.

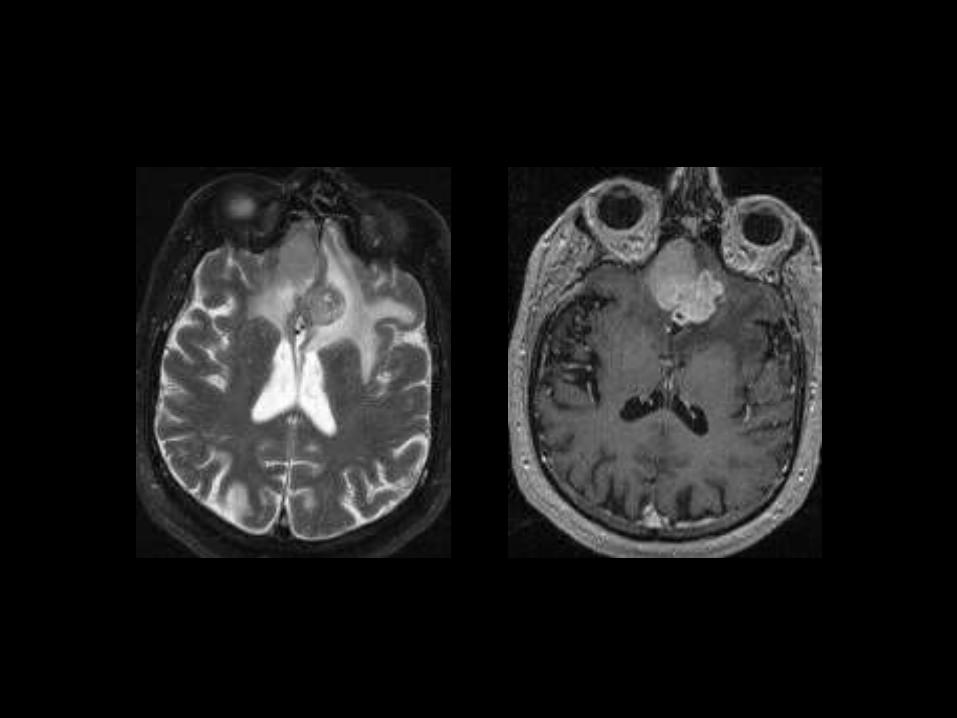
CLINICAL HISTORY: 2-year-old African-American girl with left eye strabismus for 9 months.
Case #5


Differential Diagnosis Retinoblastoma
Calcifications, enhancement, mass of low T2 signal intensity
Persistent hyperplastic primary vitreous
Coat’s disease
Retinal astrocytoma
Rare; isolated or in association with tuberous sclerosis (TSC)
Ocular toxocariasis

PHPV Congenital
Due to incomplete regression of embryonic ocular blood supply
Imaging
Best diagnostic clue: Hyperdense or hyperintense small globe, retrolental soft tissue, no Ca++
Retinal detachment common
Central linear structure: Cloquet’s canal
Layering blood or debris may be present
PHPV is the most common intraocular abnormality to be confused with retinoblastoma
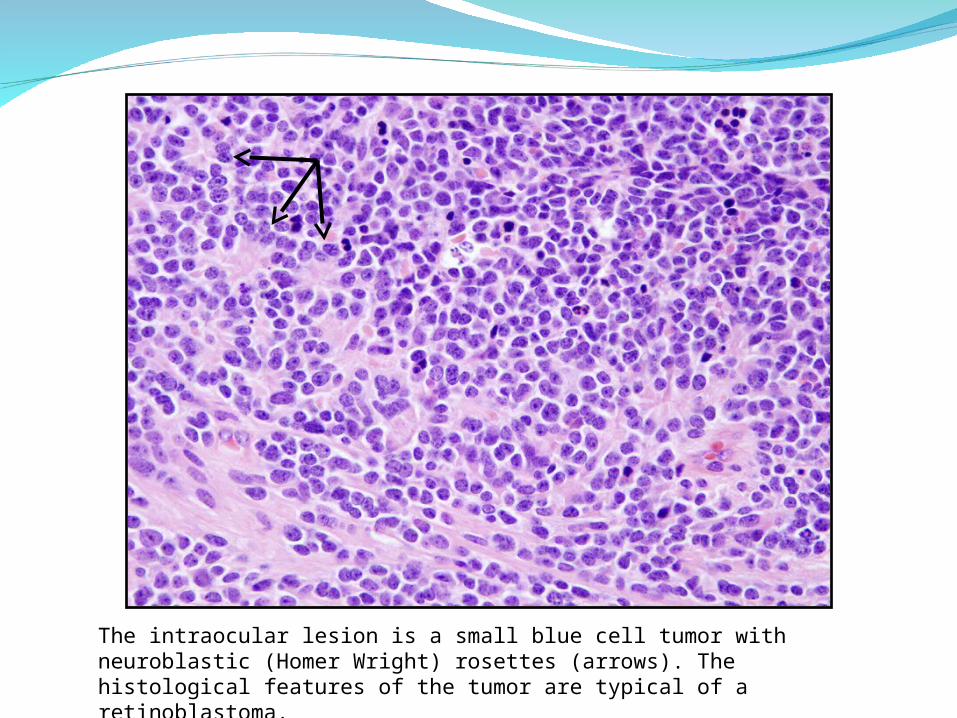
The intraocular lesion is a small blue cell tumor with neuroblastic (Homer Wright) rosettes (arrows). The histological features of the tumor are typical of a retinoblastoma.

RetinoblastomaCT:
Calcified intraocular mass
Unilateral in 70-75%
MR: T2 Hypointense relative to vitreous
Moderate to marked heterogeneous enhancement
Best for assessing extraocular and intracranial disease
Recommended