Current Status of Radiotherapy in Soft Tissue Sarcomas
Martin Keisch, MD
Cancer Healthcare Associates
Miami Brachytherapy Center
University of Miami Hospital
Outline
• Review Sarcoma Treatment Data – Retrospective Data – Randomized Data
• Technique – Discuss various techniques – External Beam
• Preoperative • Postoperative
– Brachytherapy alone – Brachytherapy boost + external beam – Treatment volume
• Toxicity and Function:
– Acute Wound Issues – Fibrosis
Background • History and Natural History
– Amputation as the standard surgical technique until last 40 years
– Local Failure common after conservative surgery alone-Relative radioresistance necessitates pushing dose intensity
– Hematogenous metastasis common
– Systemic management still questionable benefit
– Pathologic Classifications Evolving continually
– Group of diseases with low incidence
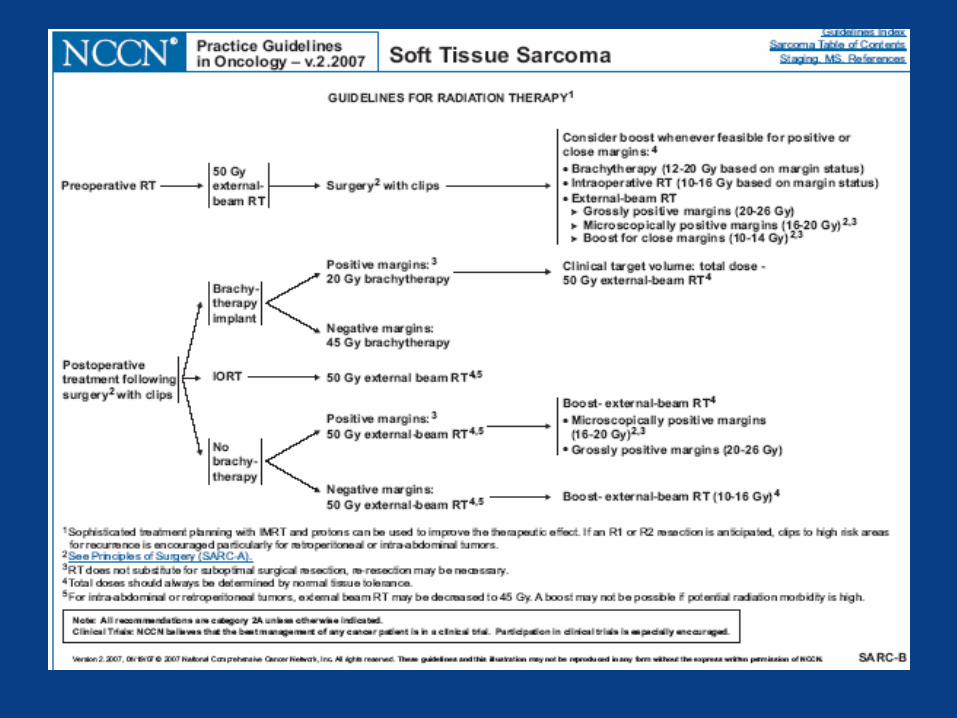
Pre-operative Therapy
•Used at some institutions to improve resectability
•Probably increases surgical complications
•Radiobiology is unclear due to potential for long break if post op boost needed
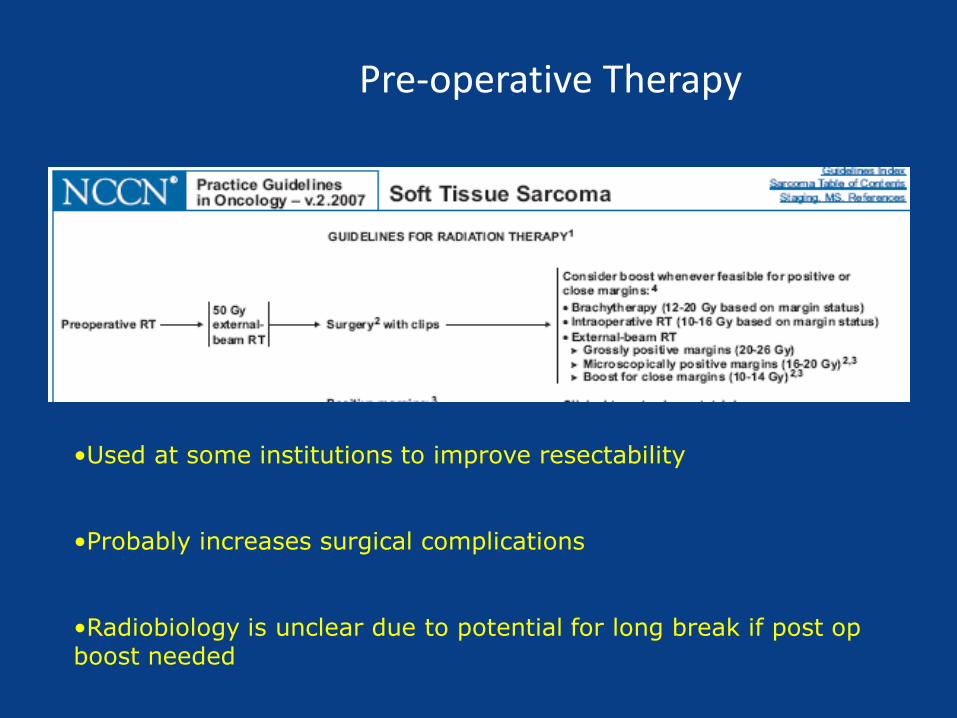
Post-Operative External Beam
•Bread and Butter of STS radiation
•“Easy”, Noninvasive, Least Targeted
•Probably increases late complication
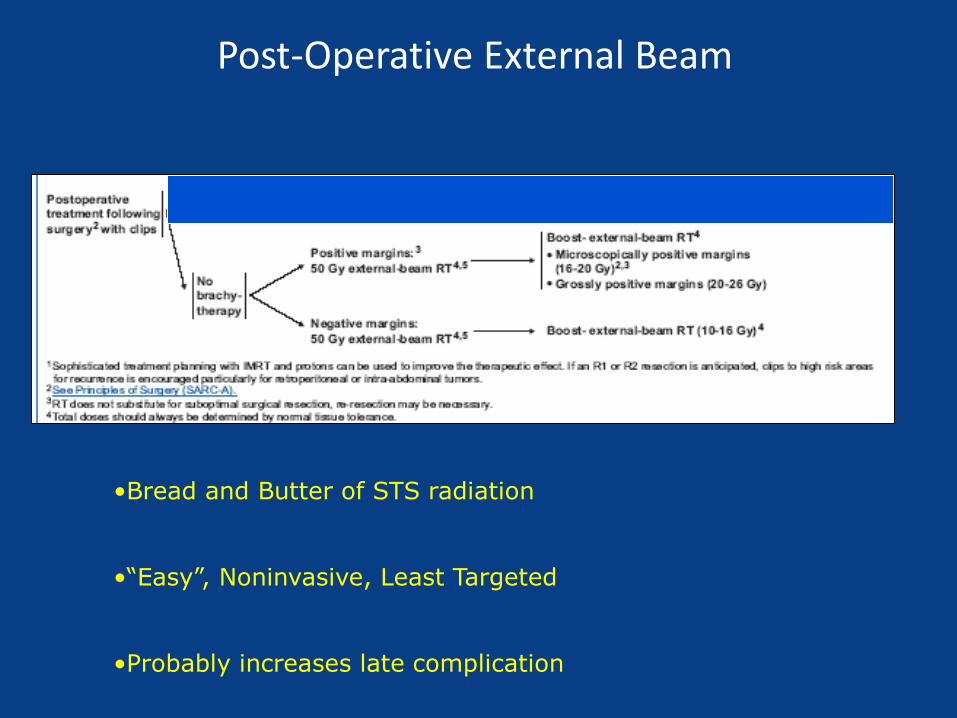
Post-Operative Radiation
Brachytherapy
Major advantages are probably targeting accuracy and dose intensity/timing
Operator dependent
Probably increases acute wound complications
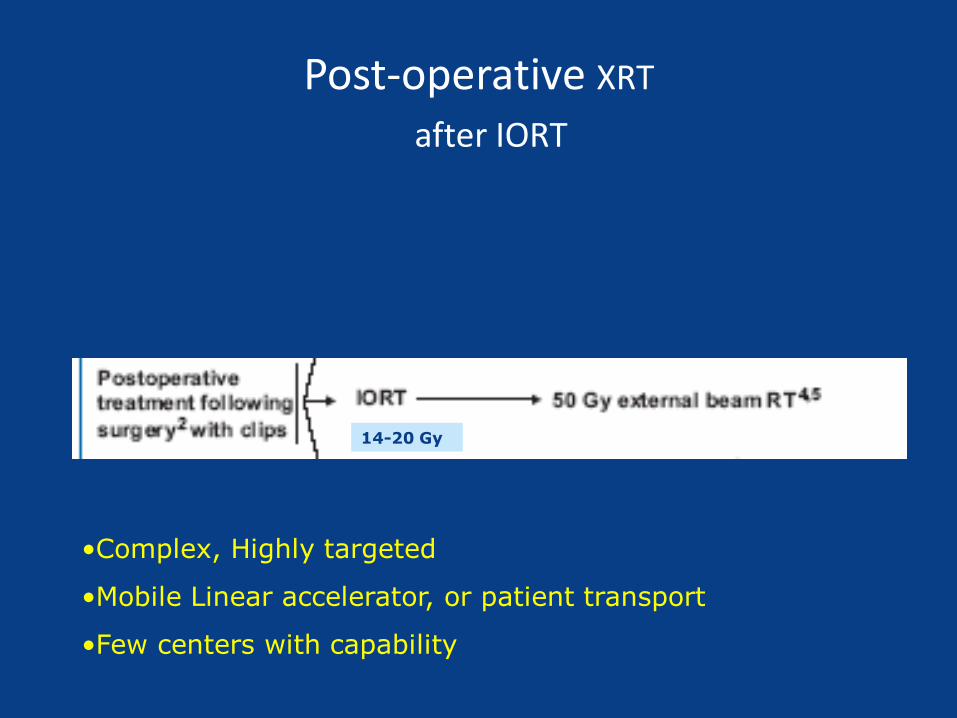
Post-operative XRT
after IORT
14-20 Gy
•Complex, Highly targeted
•Mobile Linear accelerator, or patient transport
•Few centers with capability
Basic Tenets of Radiotherapy
• More dose is better, Less volume is better
• No radiation is best
• The last 2 weeks of XRT are the hardest and most important
• Patient selection is key
• Techniques are local technology driven and sometimes user dependent

The Role of Radiation in Conservative Surgery
• 2 Randomized trials 1980’s-90’s
• NCI High Grade extremities
– 43 patients
– 4/27 LF CS vs. 0 in amputated group
– No diferrence in DFS or OS at five years
– + margins bad
• MSKCC mixed Grade
– 126 patients Brachytherapy vs. Conservative surgery only
– Decreased LF in BRT group for High Grade lesions
– No difference in DFS or Overall survival
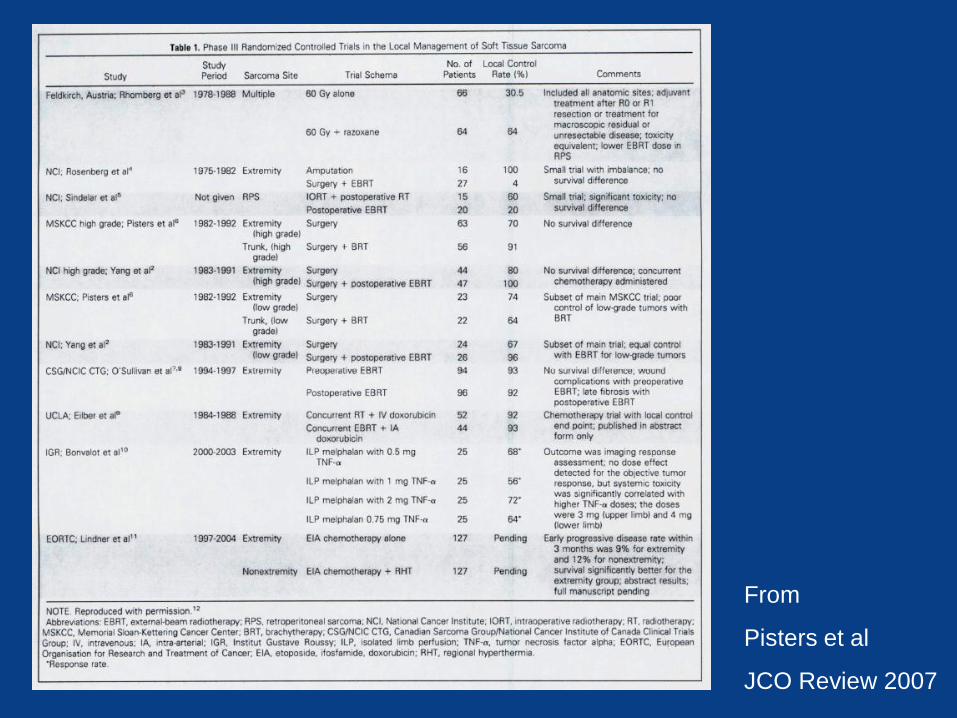
From
Pisters et al
JCO Review 2007
Randomized trials for Modern Chemotherapy
• Adria/Ifos based- mid 1990’s
• 4 studies, small numbers (59-134 pts) -Frutasci et al, Petrioli et al, Brodawicz et al, Gortzak et al
• 2 positive, 2 negative
• Modest benefits at best
• Confounded by heterogeneous pathologic subtypes
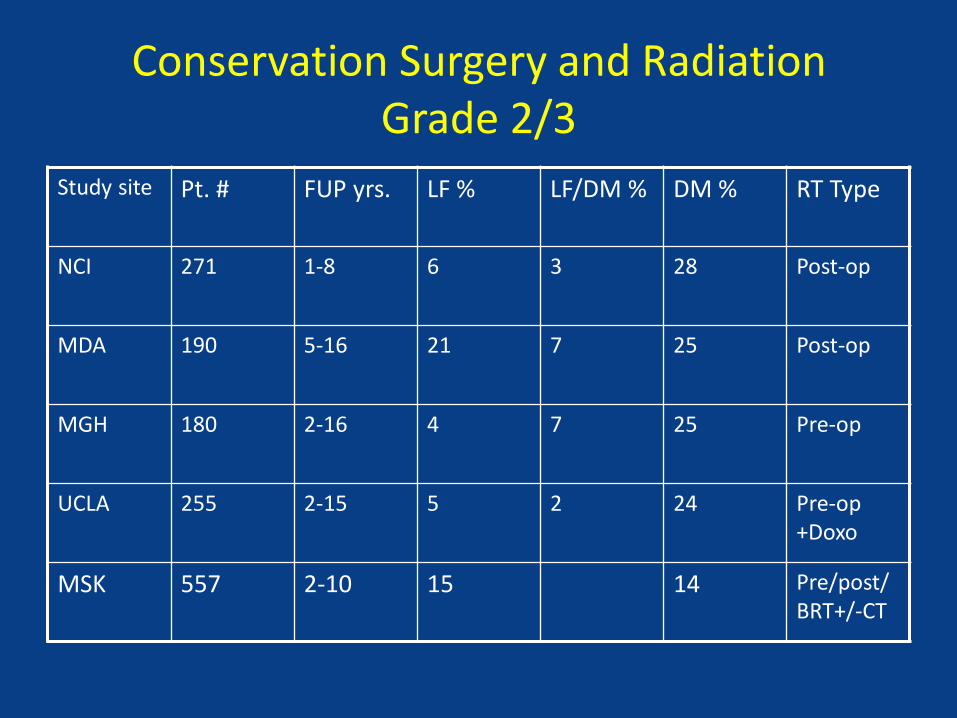
Conservation Surgery and Radiation Grade 2/3
Study site Pt. # FUP yrs. LF % LF/DM % DM % RT Type
NCI 271 1-8 6 3 28 Post-op
MDA 190 5-16 21 7 25 Post-op
MGH 180 2-16 4 7 25 Pre-op
UCLA 255 2-15 5 2 24 Pre-op +Doxo
MSK 557 2-10 15 14 Pre/post/BRT+/-CT
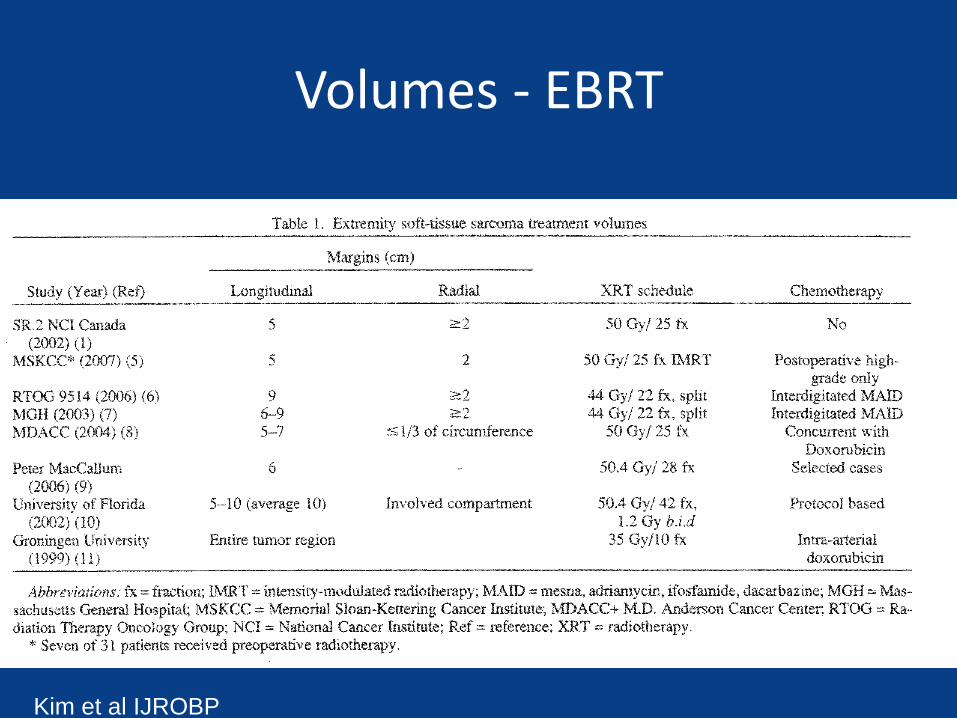
Volumes - EBRT
Kim et al IJROBP
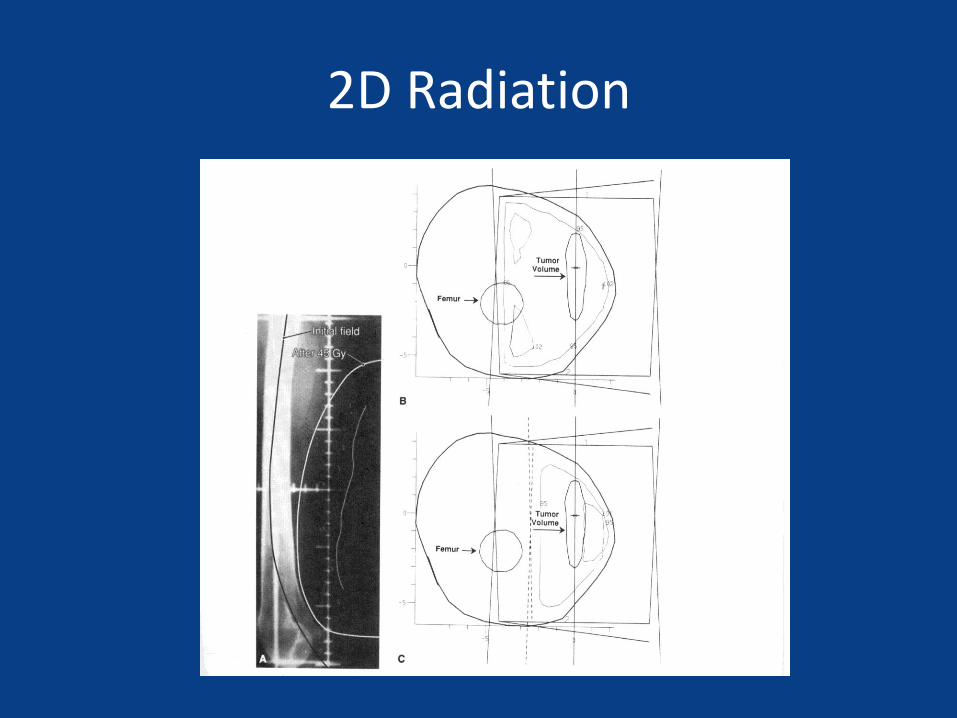
2D Radiation
Volumes - EBRT
• Reductions indicated? In the modern era of IMRT/IGRT
• Preoperatively on the the tumor NOT the operative bed (more like Brachytherapy)
• Postoperatively Much larger field sizes historically – need to target like Brachytherapy (need to go to the Operating Room)
Going to the OR
• But don’t want to do Brachytherapy?
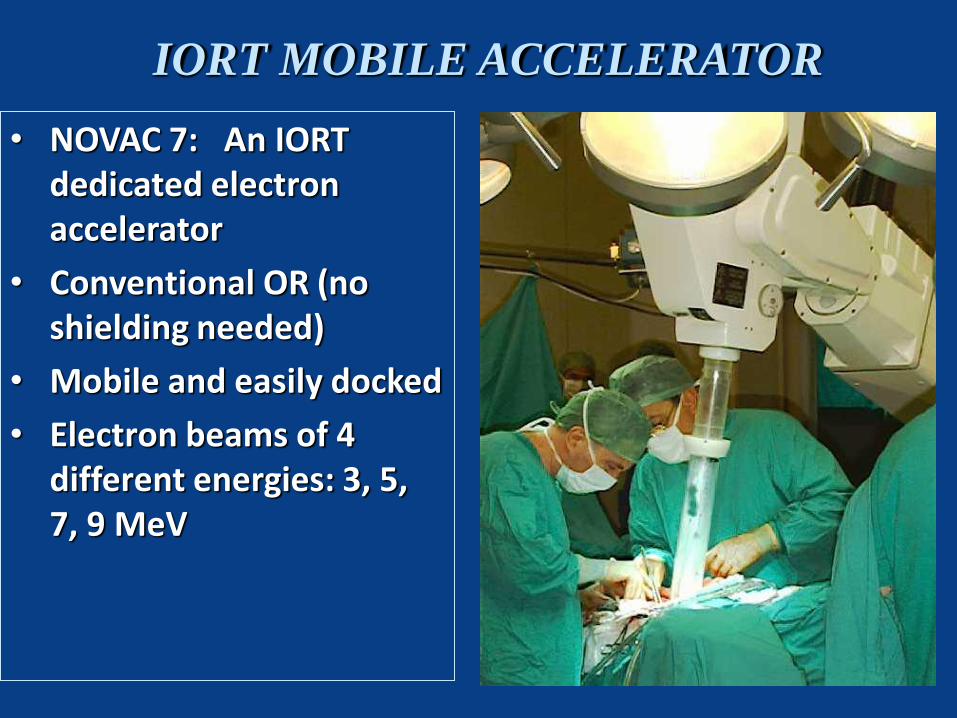
• NOVAC 7: An IORT dedicated electron accelerator
• Conventional OR (no shielding needed)
• Mobile and easily docked
• Electron beams of 4 different energies: 3, 5, 7, 9 MeV
IORT MOBILE ACCELERATOR
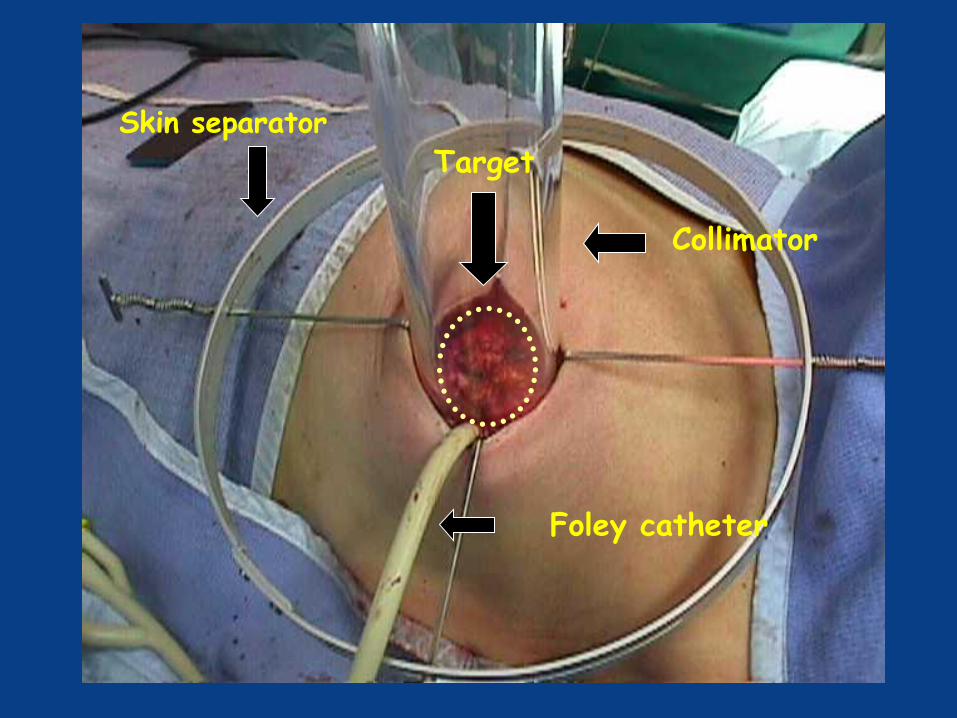
Collimator
Skin separator
Foley catheter
Target
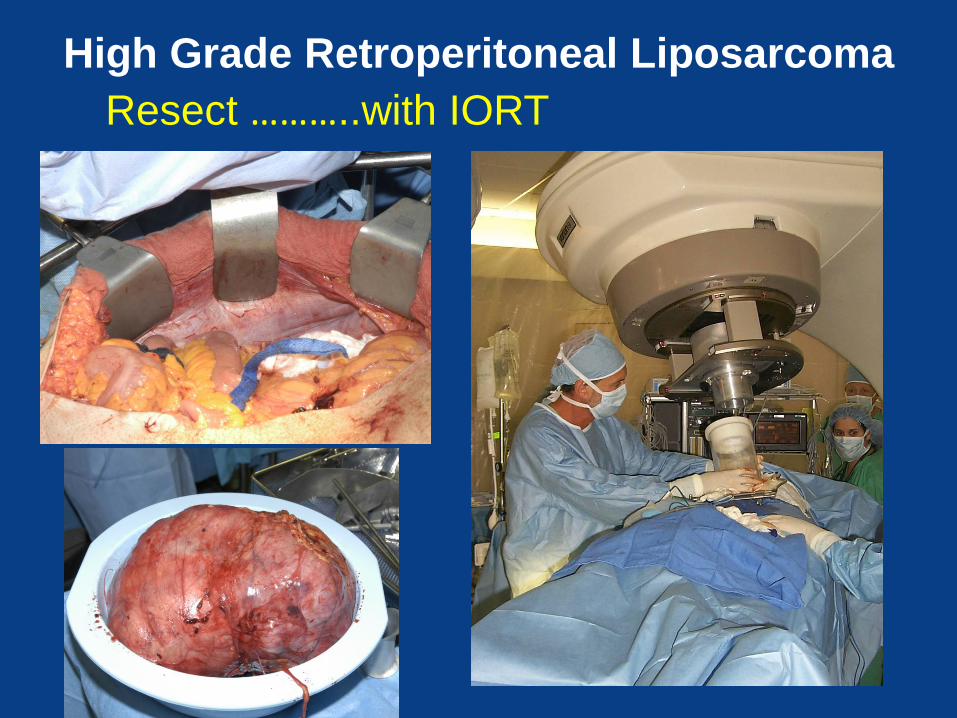
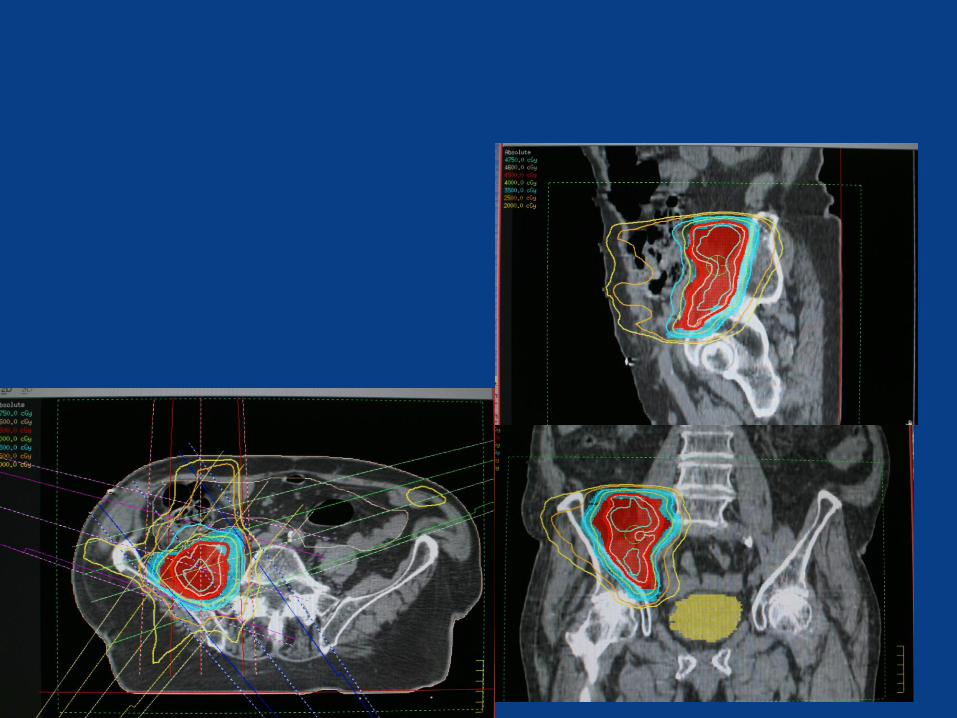
High Grade Retroperitoneal Liposarcoma
Resect ………..with IORT
Not going to the OR
• Didn’t think so…….



Wound healing after preoperative radiation for sarcoma of soft tissues.
Bujko K, Suit HD, Springfield DS, Convery K. Department of Radiation Oncology, Massachusetts General Hospital
– Morbidity from wound healing retrospectively analyzed – 202 consecutive patients with tumors of the soft tissue treated with
preoperative irradiation and conservative operation – boost dose was given to 143 patients (71 percent) postoperatively.
– The overall wound complication rate was 37 percent.
– One patient died because of necrotizing fasciitis.
– In 33 instances (16.5 percent), secondary operation was necessary,
including six patients (3 percent) who required amputation.
– The wounds in the remaining 40 patients (20 percent) were treated without operation.
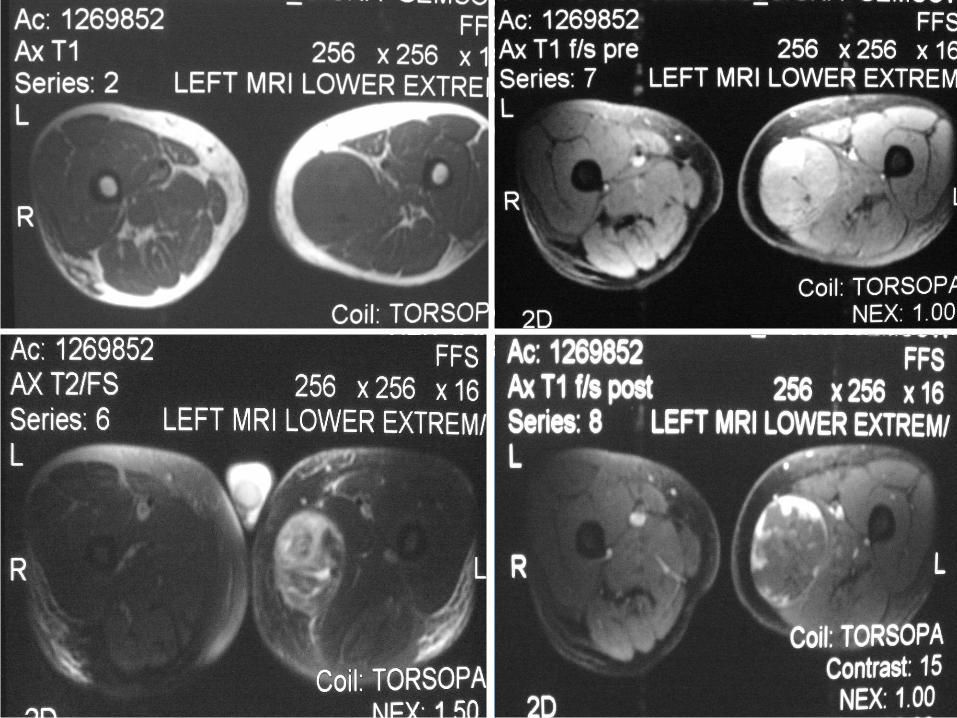
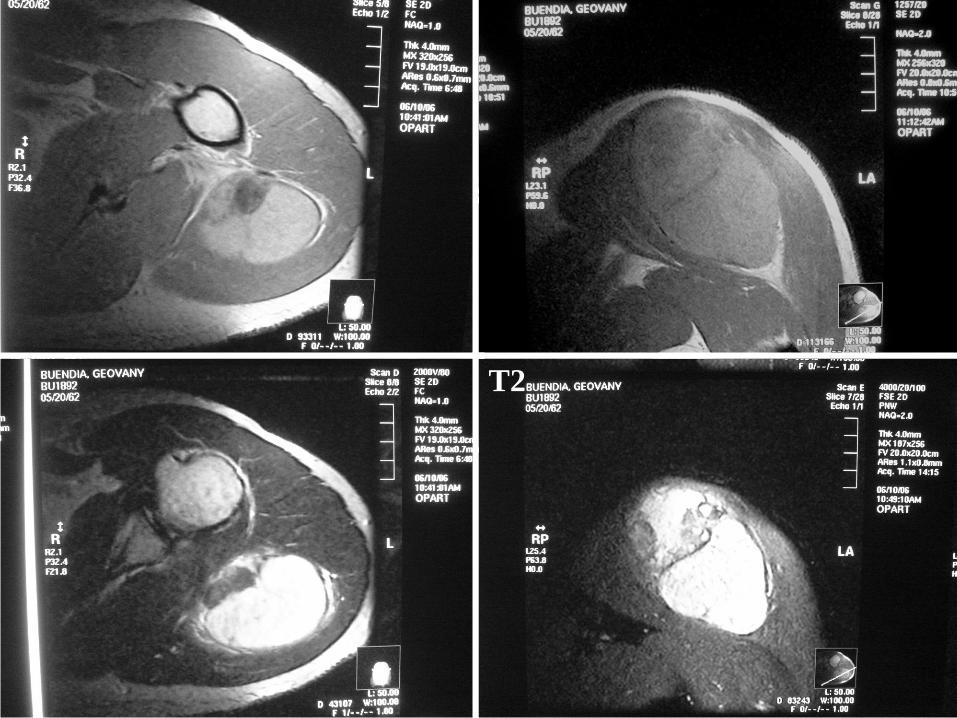
IMRT Case
• 42 y male with enlarging left thigh mass x 4 mo
• Pain with sitting/pressure; sometimes difficulty in extending the legs
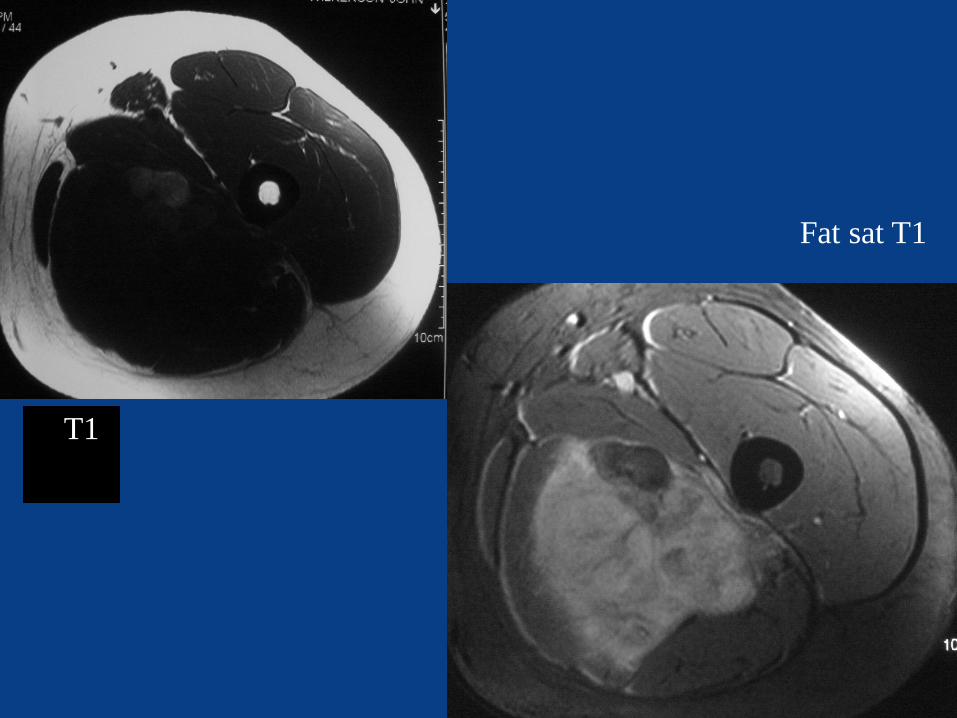
T1
Fat sat T1
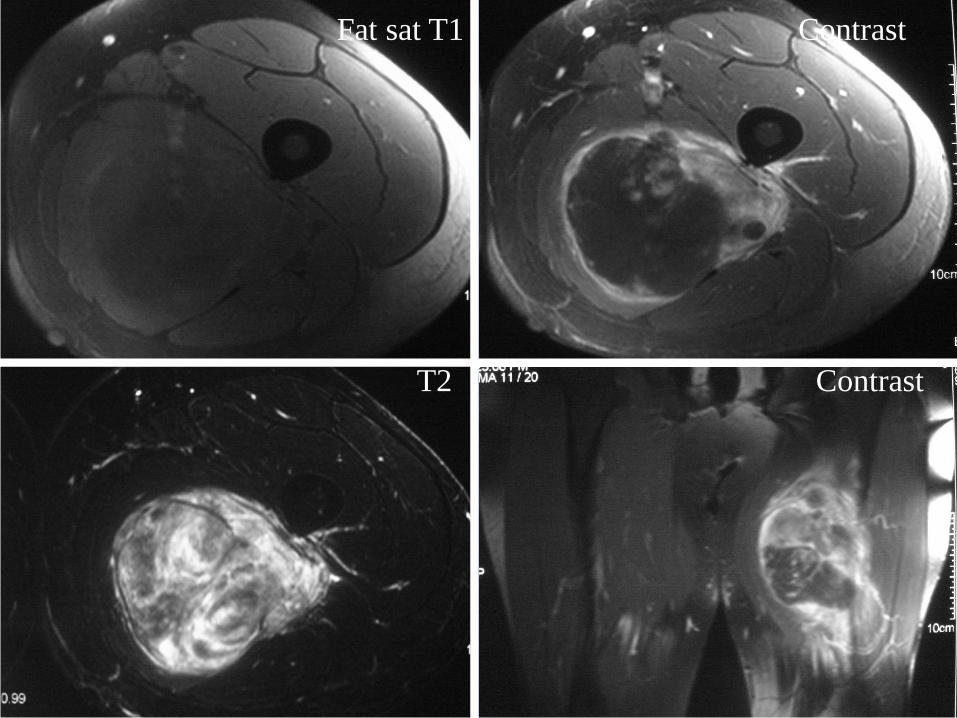
Fat sat T1 Contrast
T2 Contrast
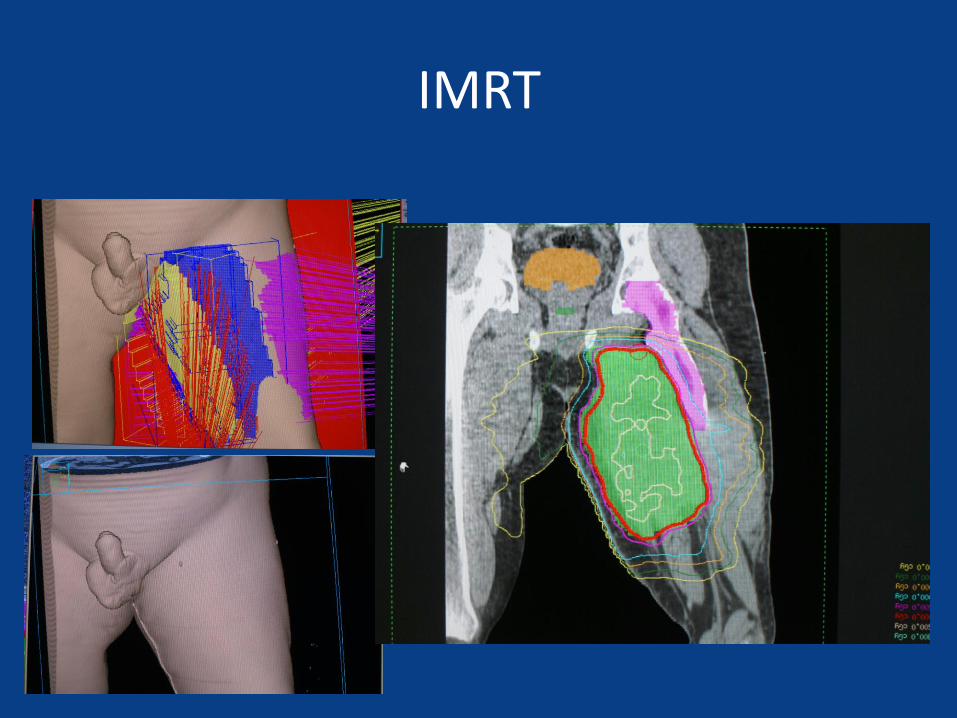
IMRT
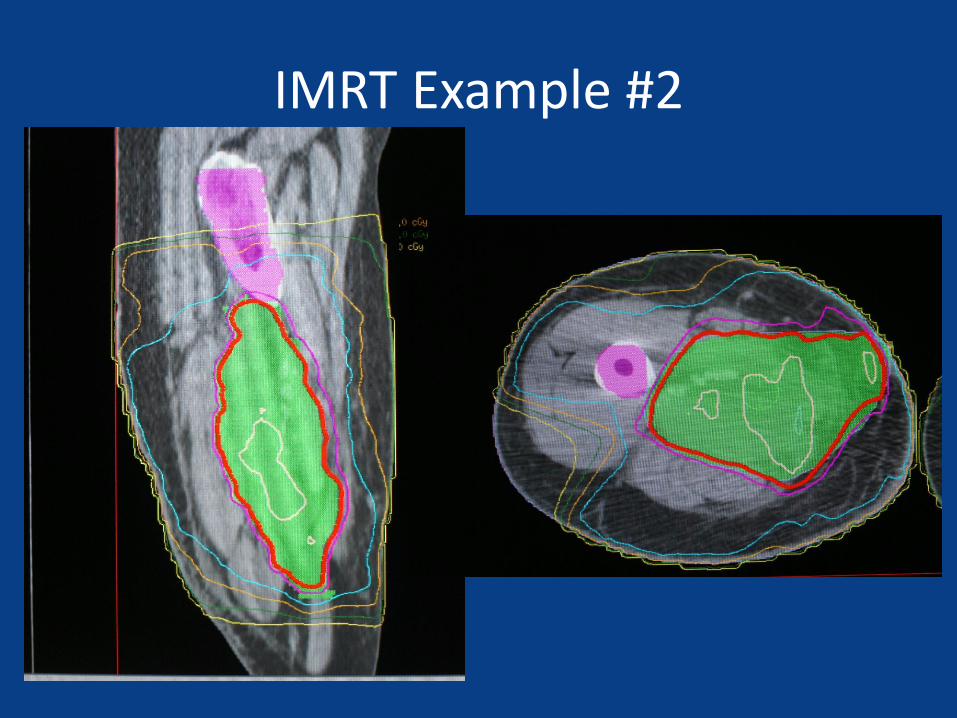
IMRT Example #2
Volumes - Brachytherapy
• Volume collapses
• Margin is on the tumor not the operative bed
• 2 cm distal/proximal, less radially
• Discordant to both pre and post op EBRT volumes
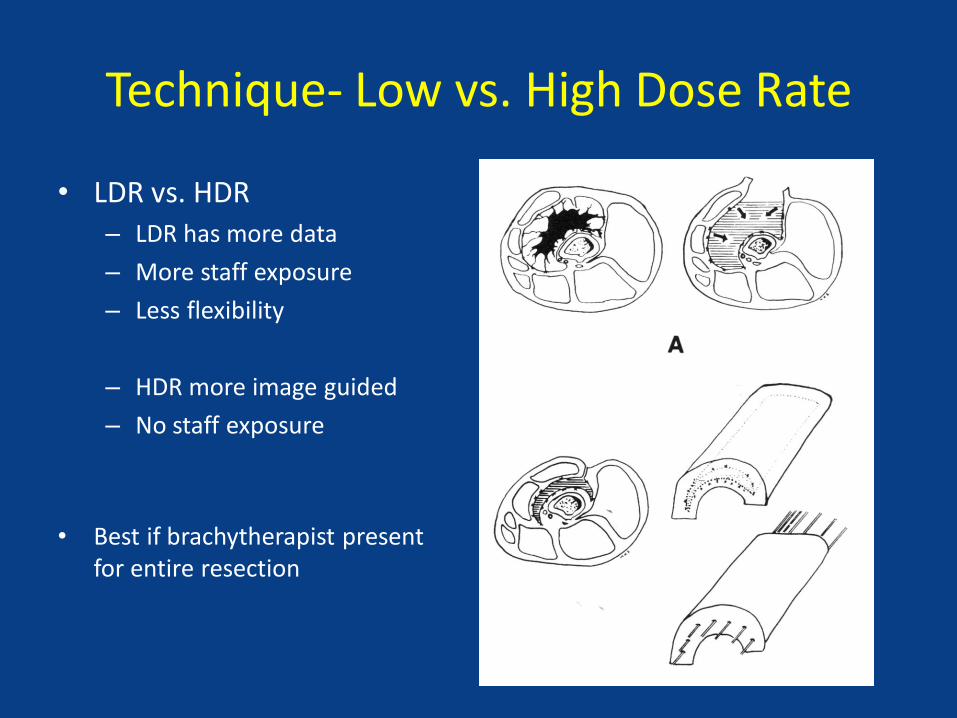
Technique- Low vs. High Dose Rate
• LDR vs. HDR – LDR has more data
– More staff exposure
– Less flexibility
– HDR more image guided
– No staff exposure
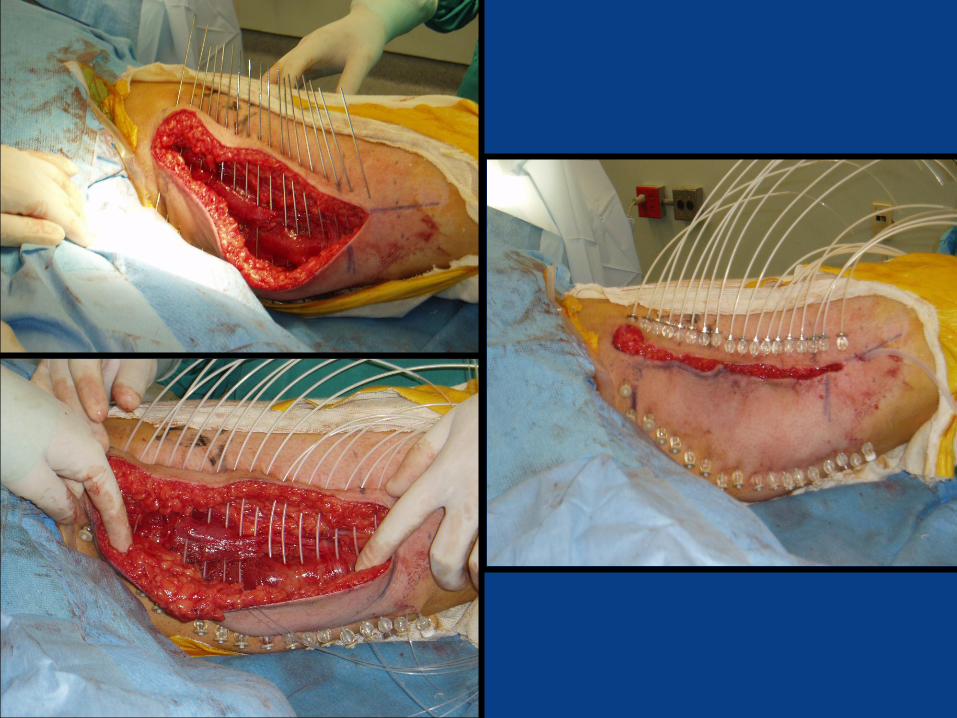
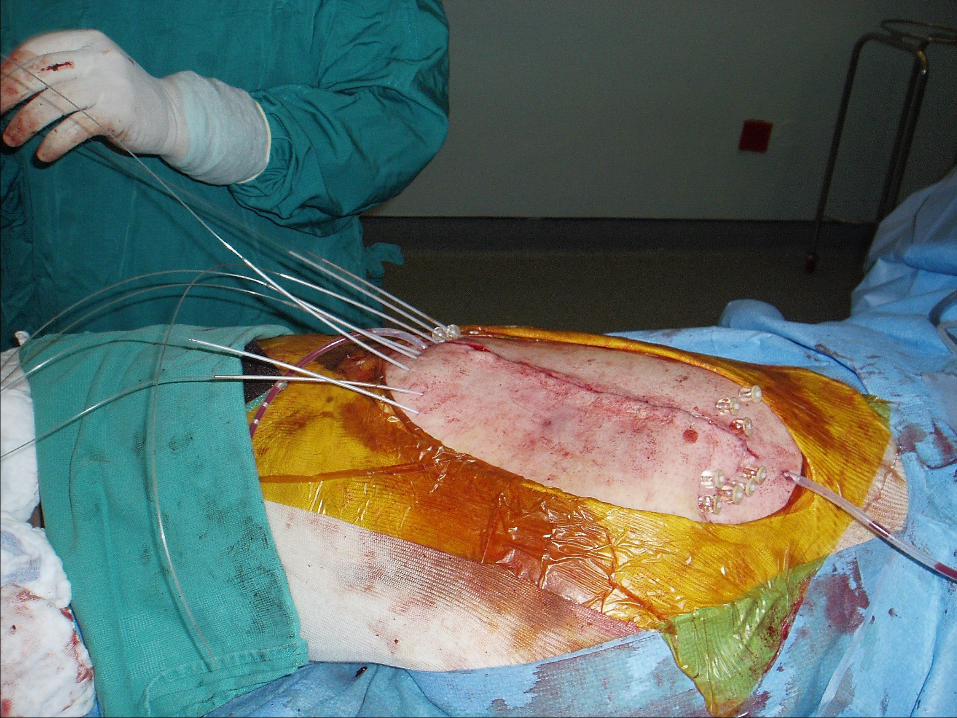
• Best if brachytherapist present for entire resection
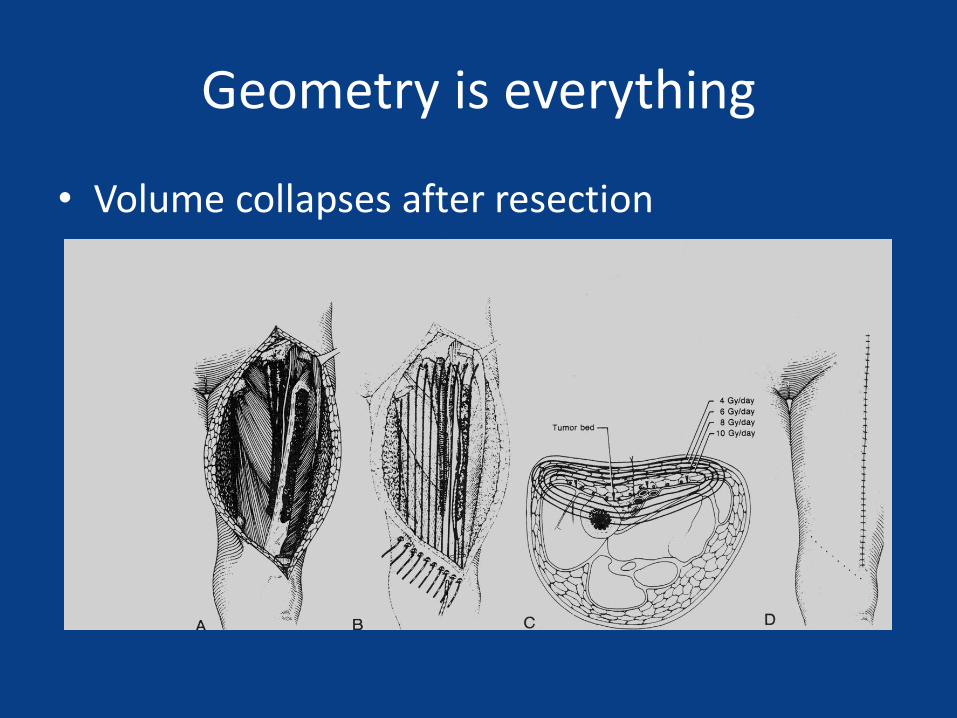
Geometry is everything
• Volume collapses after resection
Wound complications of adjuvant radiation therapy in patients with soft-tissue
sarcomas Ormsby MV, Hilaris BS, Nori D, Brennan MF
• loading of the catheters with radioactive sources on the first through the fifth postoperative days results in a 48% significant wound-complication rate
• catheters loaded five or more days after operation changed wound complications to 14% significant wound complications
• 10% of the 29 patients who did not receive radiation had wound complications of similar severity
• animal experiments would suggest that delay of application of radiation to one week after wounding is accompanied by significant improvement in wound-breaking strength, new H3 hydroxyproline accumulation, and improved force-tension curves
Ann Surg. 1989 Jul;210(1):93-9

MSKCC Low Dose Rate Implants
Mostly HDR Now
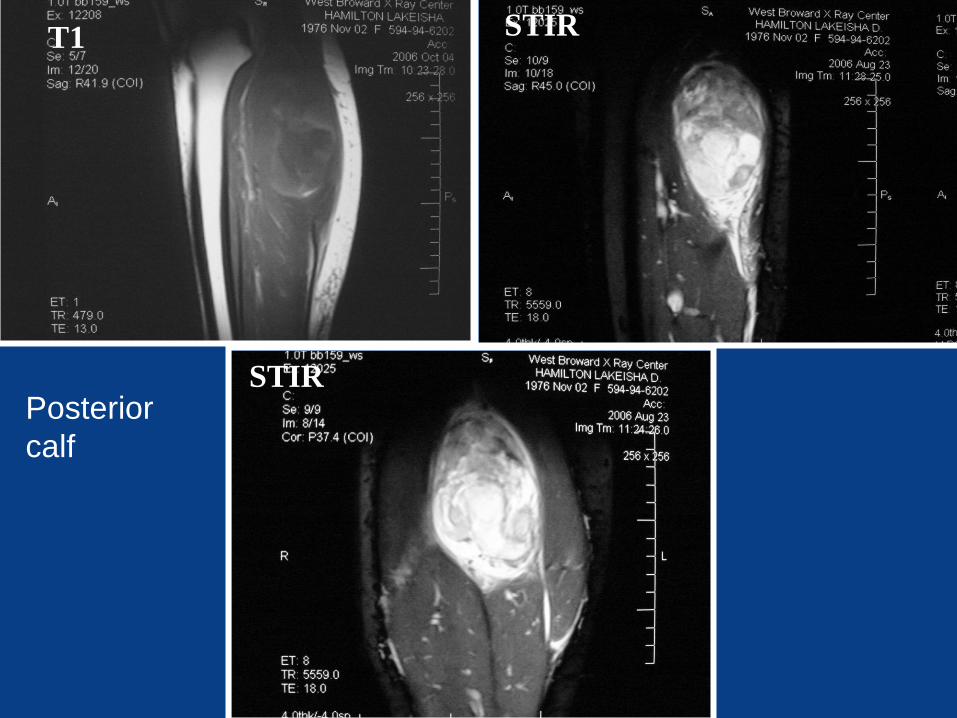
STIR T1
STIR
STIR
Posterior
calf

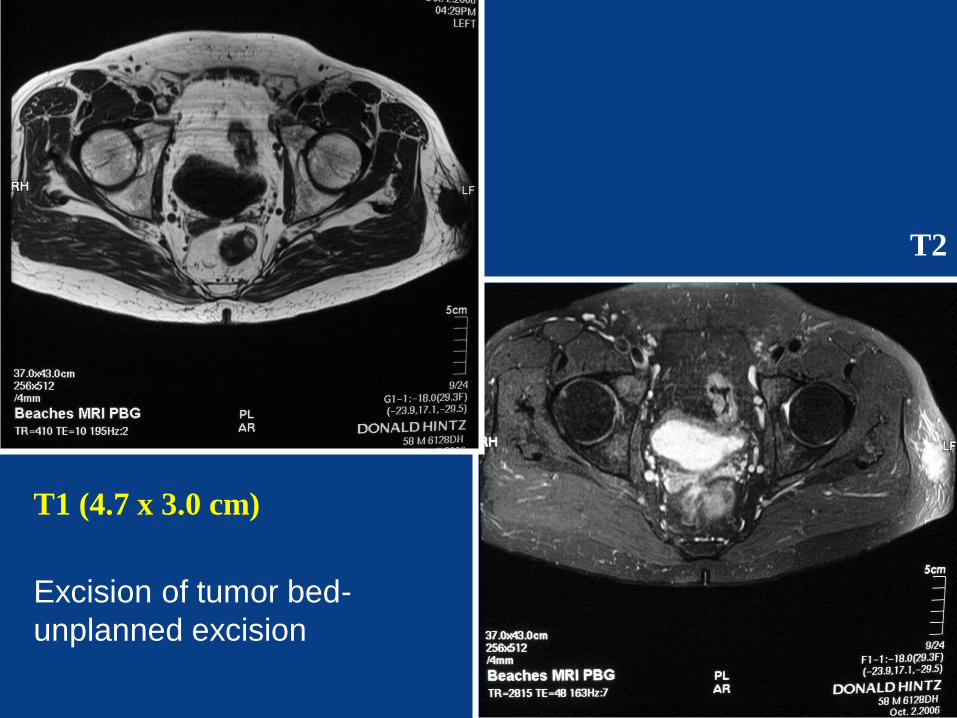
T1 (4.7 x 3.0 cm)
T2
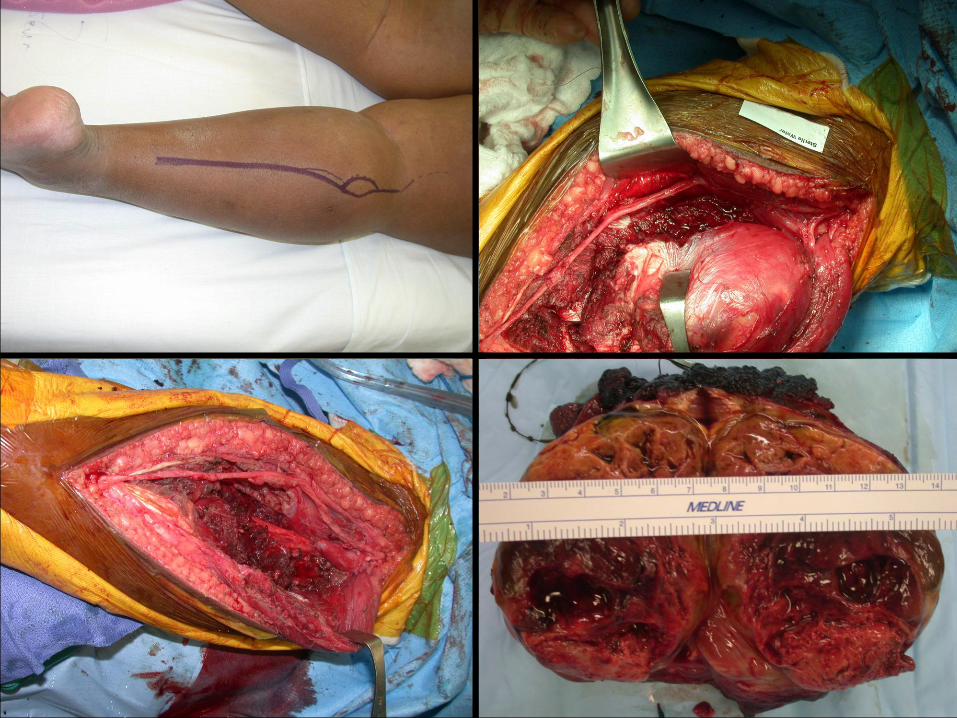
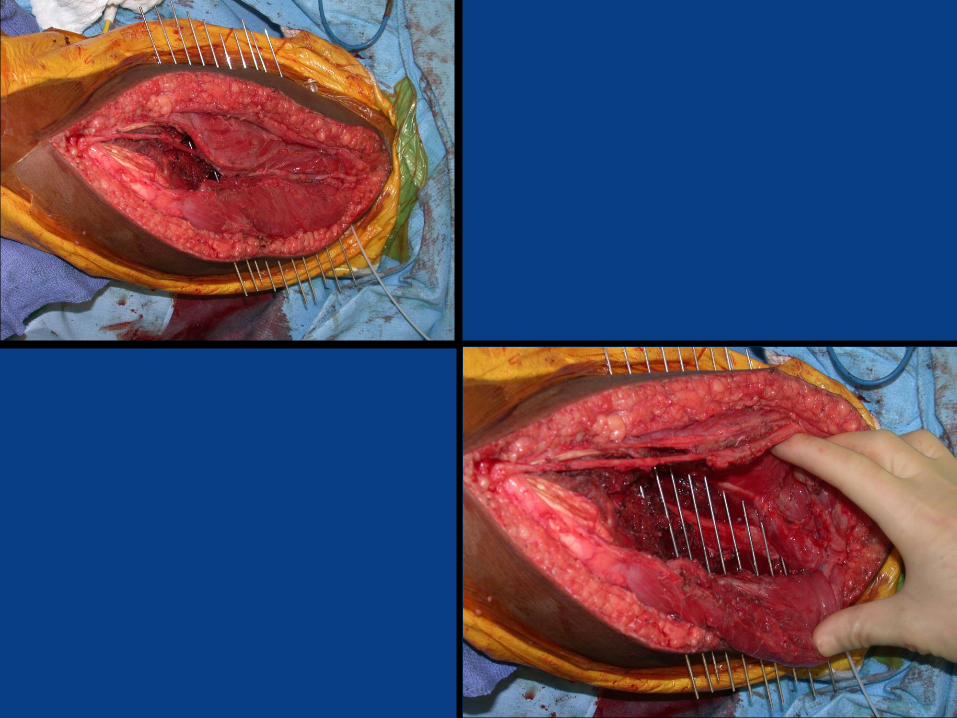
Excision of tumor bed-
unplanned excision

T2

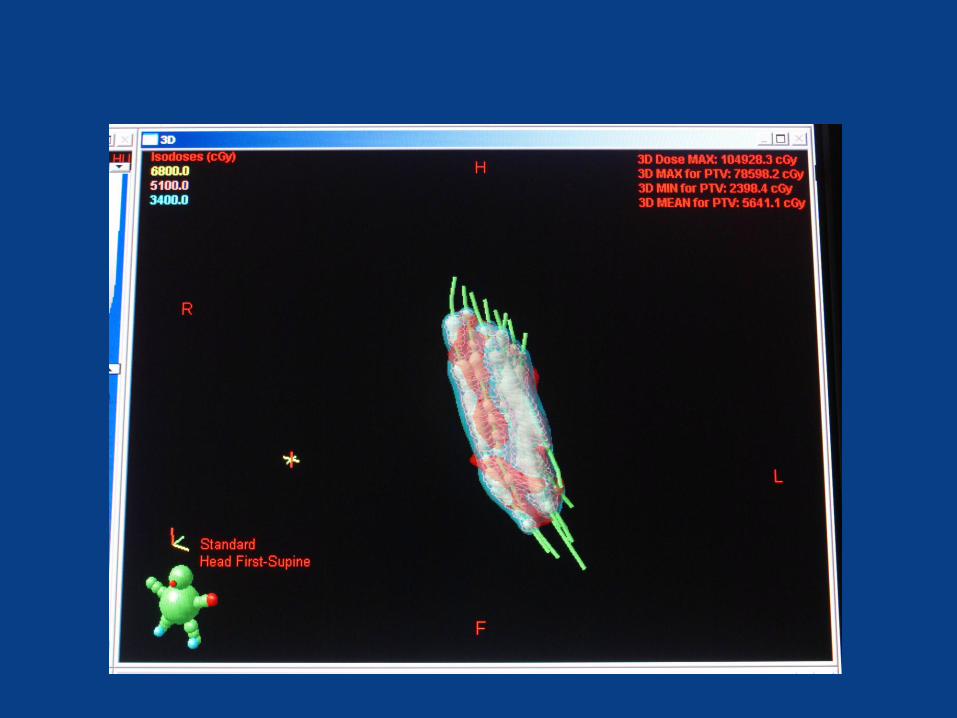
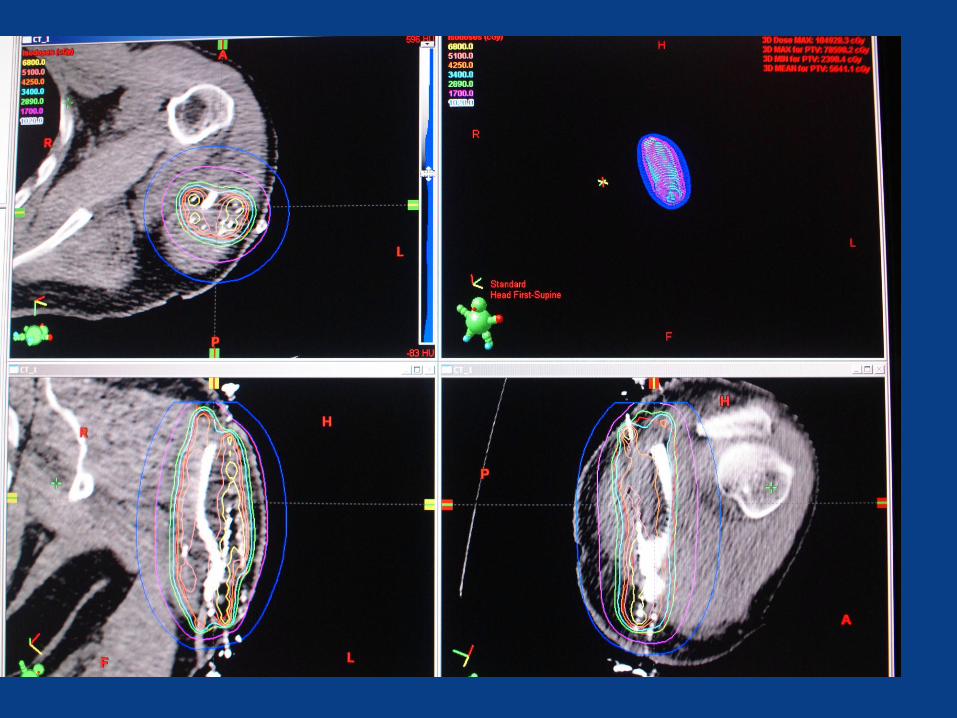
Re-Irradiation
• Highly conformal irradiation can limit
Toxicity from re-irradiation
• Data for benefit is limited Most series show high DM rate, significant complication
– MDAH series
• Tolerance generally good in my experience
Retreatment Case
• 80 yo female
• Presented with a new onset painless mass in her left thigh
• Past Hx of pleomorphic liposarcoma and post op Ext beam RTX (6300 cGY) in same location in 05-06

PE
• Diffuse swelling in LLE
• Well healed 20 cm scar on the medial aspect of thigh
• Radiation changes evident
• 2.0 x 2.0 cm firm mass palpable in the lower half of surgical incision.
• Bx done in office
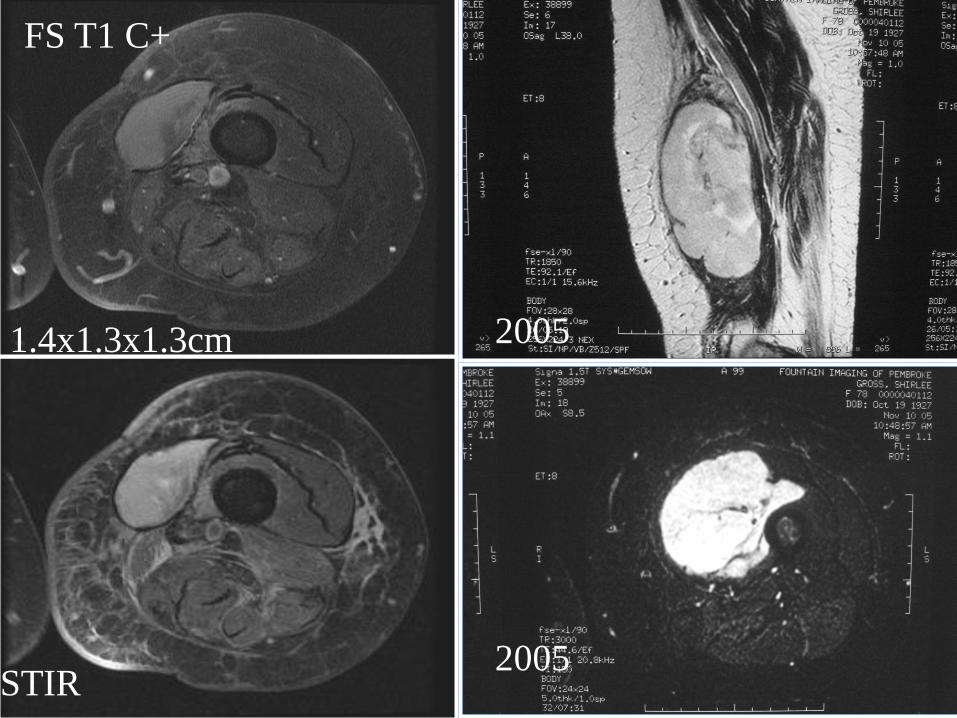
FS T1 C+
1.4x1.3x1.3cm
STIR
2005
2005


Boost Case
• 77 yo female with left thigh mass
• Notes increasing mass over 6 months
• Melanoma in situ removed from left thigh 12 yrs ago – No further treatment, follow up
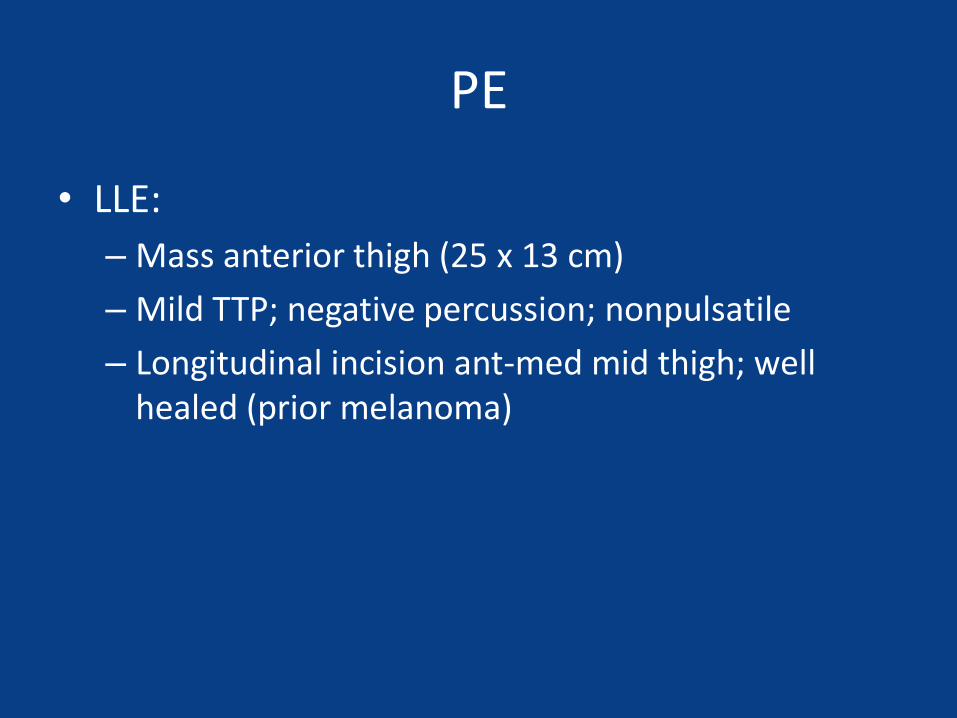
PE
• LLE:
– Mass anterior thigh (25 x 13 cm)
– Mild TTP; negative percussion; nonpulsatile
– Longitudinal incision ant-med mid thigh; well healed (prior melanoma)

GE T2
T1 T2
26 x 10 03/06
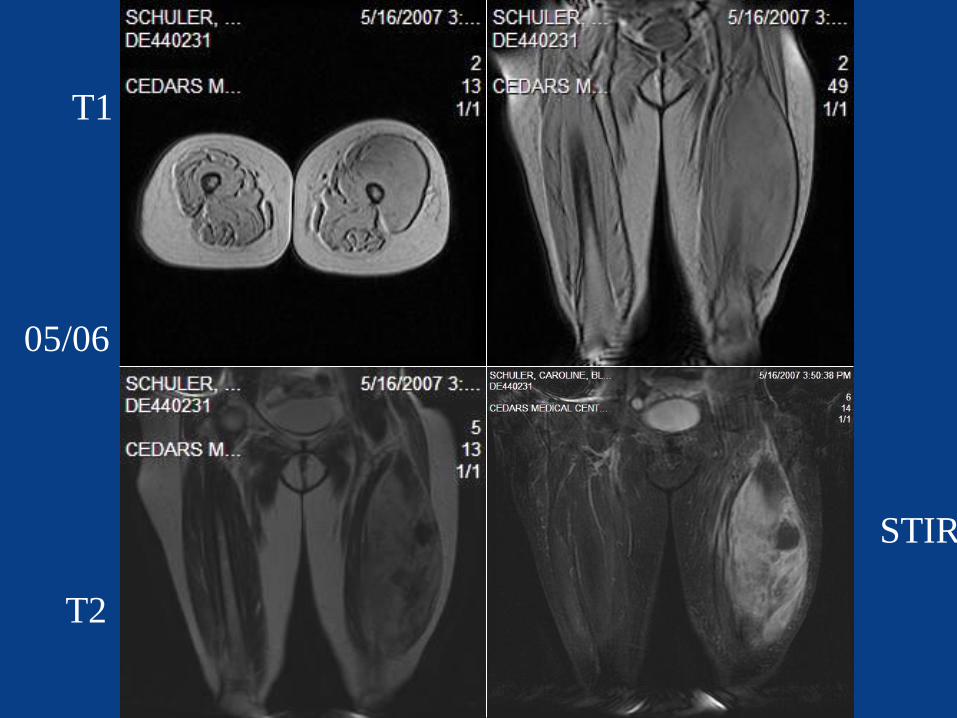
T1
T2
STIR
05/06

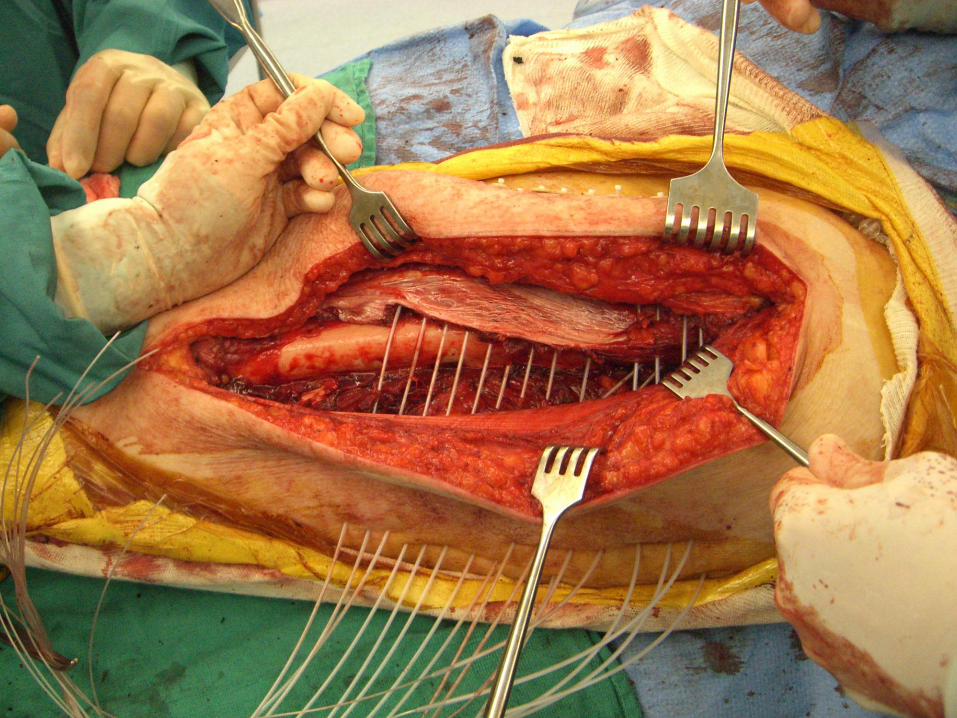
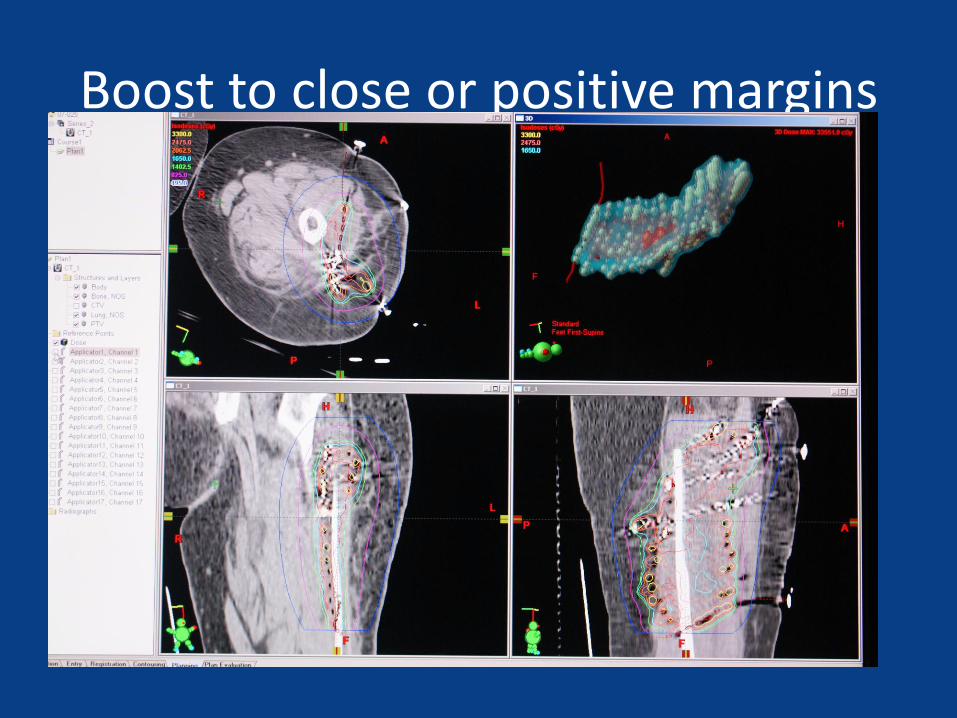
Boost to close or positive margins
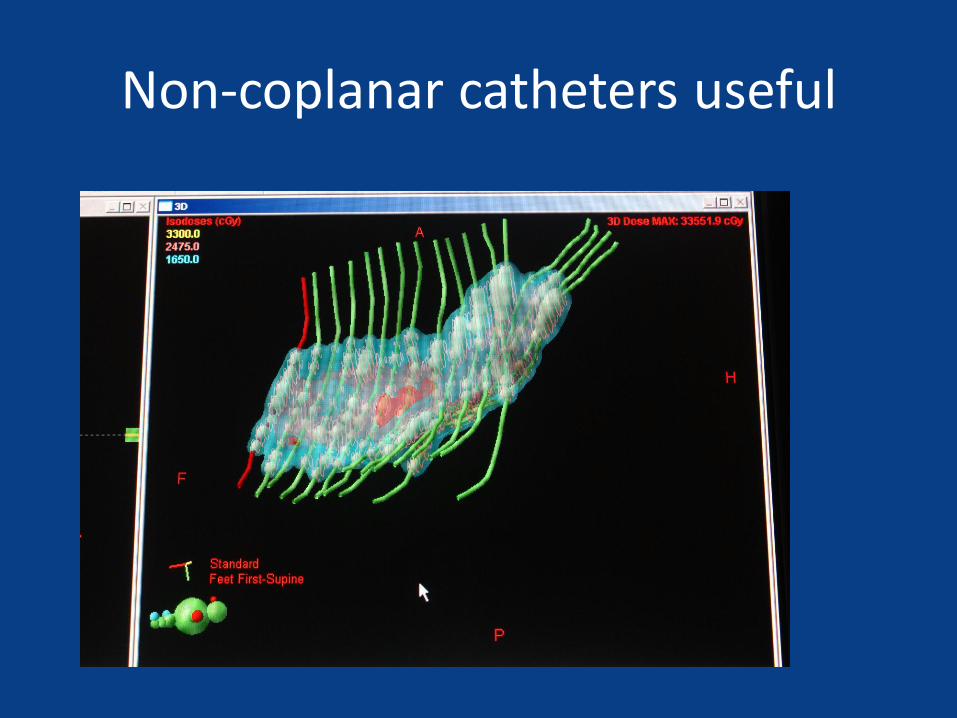
Non-coplanar catheters useful
University of Miami Experience
• Brachy centric
• Analysis presented in abstract CORR
• Higher wound complication rate with Brachy especially in medial thigh
• Better Late tolerance even in patients with wound complications
Conclusions
• Very poorly studied due to low incidence and broad spectrum of pathologies and anatomic locations
• Volume and dose are critical to control and complications
• No single technique is clearly superior for all settings
• It is always worth observing the surgical resection

Issues not Covered
• Effect of close vs positive surgical margin
• Impact of unplanned excision on LC and OS
• Importance of percent necrosis after neoadjuvant chemotherapy
Recommended