Case Report SessionRadiculopathy

1) Classification of pain• Pain has been classified into two major types: fast pain
and slow pain
• Fast pain = felt within about 0.1 second • Slow pain = after 1 second or more and then increases
slowly over many seconds and sometimes even minutes.
• Fast pain is also described by many alternative names, such as sharp pain, pricking pain, acute pain, and electric pain. Usually on the surface of skin.
• Slow pain also goes by many names, such as slow burning pain, aching pain, throbbing pain, nauseous pain, and chronic pain. It can occur both in the skin and in almost any deep tissue or organ.

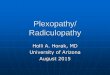
• Referred pain is pain in a part of the body that is fairly remote from the tissue causing the pain.
• For instance, pain in one of the visceral organs often is referred to an area on the body surface.
In the figure, branches of visceral pain fibers are shown to synapse in the spinal cord on the same second-order neurons (1 and 2) that receive pain signals from the skin. When the visceral pain fibers are stimulated, pain signals from the viscera are conducted through at least some of the same neurons that conduct pain signals from the skin, and the person has the feeling that the sensations originate in the skin itself.


• Visceral Pain = Essentially all visceral pain that originates in the thoracic and abdominal cavities is transmitted through small type C pain fibers and, therefore, can transmit only the chronic-aching-suffering type of pain.
• Causes of True Visceral Pain • Ischemia • Chemical Stimuli • Spasm of a Hollow Viscus • Overdistention of a Hollow Viscus • Insensitive Viscera


• Pain from the viscera is frequently localized to two surface areas of the body at the same time because of the dual transmission of pain through the referred visceral pathway and the direct parietal pathway.
Pain impulses pass first from the appendix through visceral pain fibers located within sympathetic nerve bundles, and then into the spinal cord at about T-10 or T-11; this pain is referred to an area around the umbilicus and is of the aching, cramping type.

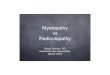
Anatomy





Disc space L3-4 L4-5 L5-S1 C4-5 C6-7 C7-T1
Root affected
L4 L5 S1 C5 C7 C8
Muscles affected
Quadriceps Peroneals, anterior tibial, extensor hallucis longus
Gluteus maximus, gastrocnemius, plantar flexor of toes
Deltoid, biceps
Triceps, wrist exrensors
Intrinsic hand muscles
Area of pain and sensory loss
Anterior thigh, medial shin
Great toe, dorsum of foot
Lateral foot, small toe
Shoulder, anterior arm, radial forearm
Thumb, middle fingers
Index, fourth fifth finger
Reflex affected
Knee jerk Posterior tibial Ankle jerk Biceps Triceps Triceps
Straight leg raising
Many not increase pain
Aggravates root pain
Aggravates root pain
- - -

Struktur peka nyeri vertebra• Kulit, jaringan subkutan
adiposa• Otot, kapsul dan sendi
ligamentum vertebrae• Lapisan luar anulus
fibrosus• Durameter dan jaringan
epidural fibroadiposa• Dinding vaskuler dan saraf

Nyeri Punggung Bawah• Definisi• Nyeri yang dirasakan di daerah punggung bawah. Dapat
berupa nyeri local,nyeri radikuler atau keduanya. Nyeri terasa di antara tepi iga terbawah dan lipat bokong bawah yaitu di daerah lumbal atau lumbosacral dan sering disertai dengan penjalaran nyeri kearah tungkai dan kaki

• Klasifikasi berdasarkan waktu onset1. NPB akut <6 minggu2. NPB subakut 6-12 minggu (bisa 4 minggu)3. NPB kronis >12 minggu
Klasifikasi berdasarkan triage klinis: *untuk menghindarkan pemeriksaan penunjang yang tidak perlu dan penanganan lebih terarah4. NPB dengan kelainan kelainan patologik serius (red-flags)5. NPB non spesifik6. NPB dengan sindroma radikuler

• Red Flags:
• Awitan NPB usia>55th
• Riwayat trauma (ringan, atau potensi osteoporosis)
• Nyeri konstan progresif memburuk dengan berbaring
• Deformitas structural• Riwayat keganasan• Kecanduan obat (suntikan)• Pemakaian steroid lama• Pemakaian imunosupresan• Luasnya gejala tanda neurologic
(gang. BAK, saddle anesthesia, loss sesibilitas progresif atau tanpa loss motoric sesuai radiks saraf)
• Kelainan neurologic menetap 1 bulan
• Restriksi fleksi lumbal berat <5cm• Demam
• YellowFlags
• Negative attitude that backpain is harmful
• Reduced activity level• Tendency depression• Social financial
problems

• Faktor resiko1. Umur 35-55 thn2. Jenis kelamin3. BMI4. Pekerjaan5. Aktivitas6. Posisi tubuh
• Etiologi1. Degeneratif (spondilosis,
HNP, stenosis spinalis, OA)2. Inflamasi (RA)3. Osteoporosis 4. Kongenital5. Gangguan sirkulasi
(aneurysma aorta abdominalis)
6. Tumor (Osteoma, paget’s disease,hemangioma)
7. Infesi (spondilitis TB)8. Psikoneurotik

• Patogenesis
Agen inflamasi menstimulasi reseptor
nyeri pada jaringan
Bradikinin, prostaglandin,leukot
rien
Ujung saraf nociceptor,
teraktivasi,impuls menjalas melalui spinal cord dan
melepaskan neuropeptida
Extravasasi pemb.darah dan aktivasi sel mast
Histaminpembengkakan jaringan

• Gejala klinis• Nyeri punggung bawah (sementara,lokal,atau
menjalar, dangkal atau dalam)• Nyeri lokal: bisa karena terkilir atau keseleo, sakit bila
dipalpasi, bisa ada spasme otot, bertambah atau berkurang bila berubah posisi• Nyeri menjalar: karena penekanan pangkal saraf• Referred pain

• Diagnosis• X-ray• Ct scan•Myelography•MRI
• Diagnosis banding• Cedera tendon achilles• Kompresi lumbal e.c fraktur

Penatalaksanaan Radikulopati
• Informasi dan edukasi• Farmakoterapi• Akut : asetaminofen, NSAID, muscle relaxant, opioid (nyeri berat), injeksi epidural.• Kronik : analgesic adjuvan• antidepresan trisiklik (amitriptilin), opioid (kalau sangat diperlukan), SSRE, anti dopamin

• Terapi nonfarmakologik• Akut : imobilisasi (lamanya tergantung kasus),
pengaturan berat badan, posisi tubuh dan aktivitas, modalitas termal (terapi panas dan dingin), masase, traksi (tergantung kasus), alat bantu (antara lain korset, tongkat).• Kronik : terapi psikologik, modulasi nyeri
(akupunktur, modalitas termal), latihan kondisi otot, rehabilitasi vokasional, pengaturan berat badan, posisi tubuh dan aktivitas.

• Invasif nonbedah• Blok saraf dengan anestetik lokal.• Injeksi steroid (metilprednisolon) pada epidural
untuk mengurangi pembengkakan edematous sehingga menurunkan kompresi pada radiks saraf.
• Bedah• Indikasi operasi pada HNP :• Skiatika dengan terapi konservatif selama lebih dari 4
minggu : nyeri berat / intractable / menetap / progresif.• Defisit neurologik memburuk.• Sindroma kauda.
• Stenosis kanal : setelah terapi konservatif tidak berhasil.• Terbukti adanya kompresi radiks berdasarkan
pemeriksaan neurofisiologik dan radiologik.
Recommended