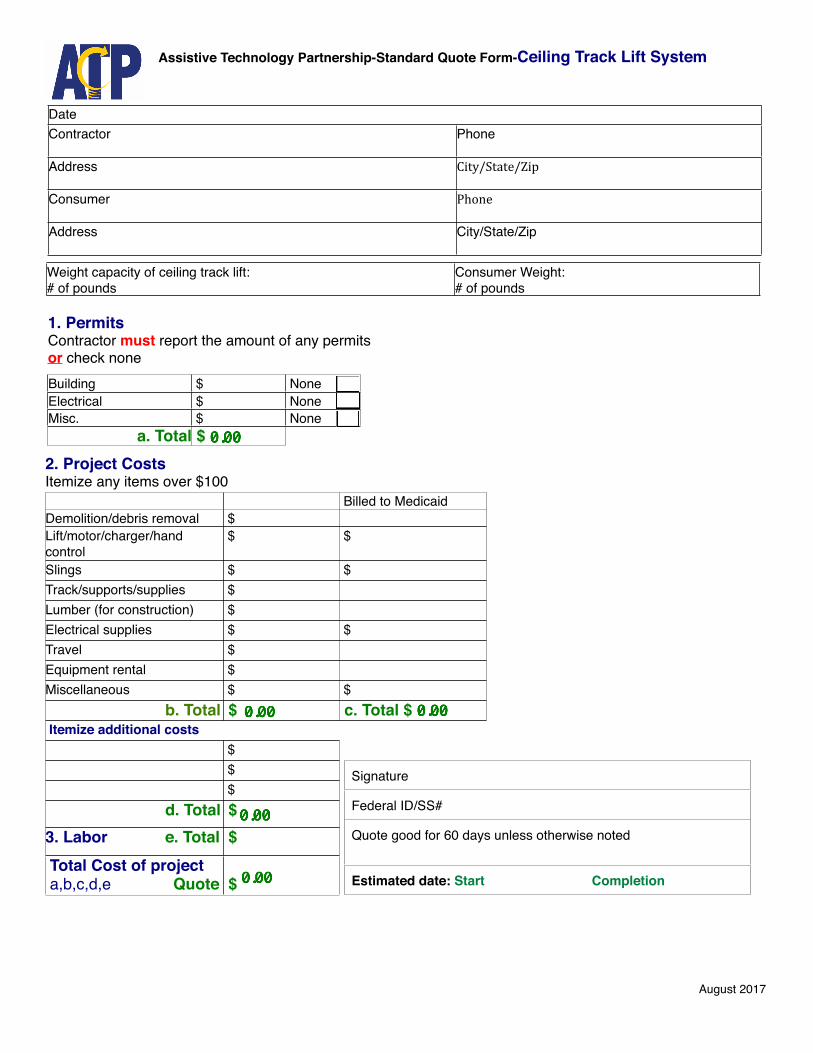
DateDateContractor Phone
Address City/State/Zip
Consumer Phone
Address City/State/Zip
1. Permits Contractor must report the amount of any permitsor check none
Assistive Technology Partnership-Standard Quote Form-Ceiling Track Lift System
August 2017
2. Project CostsItemize any items over $1002. Project CostsItemize any items over $1002. Project CostsItemize any items over $100
Billed to MedicaidDemolition/debris removal $Lift/motor/charger/hand control
$ $
Slings $ $Track/supports/supplies $Lumber (for construction) $Electrical supplies $ $Travel $Equipment rental $Miscellaneous $ $ b. Total $ c. Total $ Itemize additional costs Itemize additional costs
$ $
$ d. Total $3. Labor e. Total $ Total Cost of project a,b,c,d,e Quote $
Signature
Federal ID/SS#
Quote good for 60 days unless otherwise noted
Estimated date: Start Completion
Weight capacity of ceiling track lift: # of pounds
Consumer Weight: # of pounds
Building $ NoneElectrical $ NoneMisc. $ None
a. Total $
Recommended

















