
Continuous Quality Improvement
Enter YOUR Service Area along with Lead and
Facilitator Name!

Making Ideas Work
Catalyst for Change
CQI Purpose
CQI is a process that empowers staff by
involving everyone in the evaluation and improvement of the effectiveness and
efficiency of services provided by Children and Family Services

CQI Philosophy Basic concept: small, continuous steps
toward achieving better results Focus: self-directed, self-determined
change; leadership is by all Process through which teams:
Identify needs, goals, resources and strengths toward achieving results;
Develop action plans to improve services; and Forward unresolved issues to the next CQI level.

Key Processes in CQI
CQI Service Area and State Teams: Identify and solve barriers to service delivery and achievement of outcomes
Management Reports and Data: Keep the work on track and watch the results
Reviews of Case Work Quality: Promote
high quality case work and best practices

CQI Process
Identify and solve barriers to service delivery and achieve outcomes
Increase knowledge through data and reports
Create action plans for improvement & continued improvement
Case reviews and use of the review results to improve practice

CQI Process (cont)
All Staff members are involved in evaluating the effectiveness and efficiency of services provided to Children and Families
Examines internal systems, procedures and outcomes
Examines relationships and interactions between CFS and other stakeholders
Identifies strengths

CQI Process (cont)
Creative Inclusive Recurring Empowering Structured Solution-focused Efficient Action-oriented Common Sense Driven

Evolution of CQI in Nebraska
Development of CQI Unit and Quality Assurance Team
Performance Based Contracting Compliance vs. Improvement Accreditation (future)

Accreditation Overview
Purpose of Accreditation: Accreditation provides a number of benefits to
agencies: set of nationally recognized standards of
excellence to gauge DCF against means of system reform and practice
improvement national recognition as an accredited agency peer review from people who truly understand
public human service practice an opportunity to conduct a self study that will
lead to improved and streamlined policies and practices

Types of Accreditation Joint Commission for The Accreditation of
Healthcare Organizations (JCAHO) – medical model, used with hospitals and behavioral healthcare organizations
Commission on Accreditation for Rehabilitative Facilities (CARF) – geared as the name suggests for rehabilitative facilities
National Association for the Education for Young Children (NAEYC) – child care associations
The Council on Accreditation of Services for Children and Families (COA) – designed for services based on a social-work, community model

Overview of CQI
Provide Children and Families with the highest quality programs with demonstrated positive outcomes
Ongoing process of identifying, describing and analyzing system strengths and weaknesses
Continuously assess and modify programs and processes based on objective information
Strategically plan to promote continued improvement
Overview (cont)
Dependent upon active inclusion and participation of staff, children, youth , families and stakeholders throughout CQI process
Supports system-wide initiatives such as the development and implementation of Program Improvement Plans (PIP), case reviews, Accreditation processes and other critical initiatives

CQI Key Principles
Data and information Data and measurement Active engagement of Staff Improvement Continuous learning

CQI Cycle of Improvement
CQI Teams: Service Areas and State Level
Identify and solve barriers to service
delivery and achievement of
outcomes

CQI Team Mission Statement
This team, through a partnership with internal and external stakeholders, will focus active attention on the unique strengths and needs of the children and families we serve, in order to achieve measurable, positive outcomes in safety, permanency, and well-being at the local Service Area Level.

Service Area CQI Teams Members of a Service Area CQI team:
Membership means that every staff member has a voice in decisions about the agency
Everyone helps to lead the agency Your Team may:
Have 8-12 members within the Service Area Meet at least quarterly
Service Area Team represented on State Network
Teams to be facilitated by Central Office Quality Assurance Program Specialist

CQI Team Members Local Service Area HHS Staff & Contractors Field Staff Training Staff Legal parties (County Attorneys and/or Judges &
DHHS Legal) Foster Care Review Board CASA Education Probation Foster Parents Youth and Families Family Organizations

CQI Team Roles Team Leader (DHHS Children and Family
Services Administrators or other designee) – reinforces work of the teams and represents team’s work to internal and external entities
Team Facilitator (DHHS Central Office QA) – manages team meeting process
Team Scribe (Local DHHS Staff) – logistics, records comments and activities of the team
Team Members – participate and represent their area

Team Leader – DHHS Administration
Develop the agenda jointly with QA Facilitator
Discuss with QA Staff available data for meeting
Delegate team tasks as needed Ensure that the developed corrective action
plans and strength plans are monitored and updated
Report progress State CQI Team
Facilitator - Quality Assurance Program Specialists Role
Develop, prepare and disseminate data and additional information to Service Area CQI Teams
Facilitate action and improvement by: Coordinating and facilitating Service Area CQI
meetings Liaison between management and staff Mentoring and guiding staff toward use of best
practices Coordinating with other Service Area QA Staff

Facilitator - Quality Assurance Program Specialists Role (cont.)
Coordinate implementation of special initiatives and projects
Advocate for statewide system changes that will improve results
Present participants’ ideas that are unable to attend
Read trends Anticipate barriers Identify strengths
CQI Teams
Decision-Making
Identification of needs, goals, available resources and strengths of services, staff and community partners Current performance (baseline) to future
performance (agency goals)
Focus on topics of interest such as Safety, Mini CFSR, Family Team Meeting, Contract Monitoring, etc.

CQI Teams Design and promote development of
strategies which can be implemented to alleviate the identified issues Identify 3 areas for change Identify 3 areas of strength If data indicates an issue related to
Safety, at least one of the areas for change will be in Safety: otherwise, areas for change will be selected for which the information and data indicates the greatest need for improvement

CQI Teams
Implement and monitor local corrective action plans to resolve identified issues Corrective Action Plans and Strength
Analysis Plans will be posted on a shared website
Forward unresolved issues to State CQI Team for possible resolution Policy changes, statewide training needs,
etc.

CQI Statewide Team
Team will review all Corrective Action Plans from the Service Areas as well as strengths in practice
Team will identify statewide trends of best practice and areas needing improvement
Analyze statewide information and data Develop statewide strategies for change
in areas of Practice, Policy and Training

Management Reports and Data
Keeping the work on track
Monitoring the results

Management Data Reports Team Participants will analyze existing data,
contribute additional data/relevant information, and hypothesize contributions at the following levels: Client Level (Are there ways to solve the
problem by changing how we interact with the client?)
Program Level (Are there ways to solve the problem by modifying the program that serves the client?)
Community Level (Are there ways to solve the problem through local community resources?)

Management Data Reports Management information systems (NFOCUS,
Case Review, QA Reports) Outcome measurements (Mini CFSR reports,
Safety Model reports, FTM reports, Compass) Case Review quality (Case Review System) Customer surveys Required Contractor program evaluation
reports (EBP, Disaster Plan, Quarterly reports, etc.)

CFSR Outcomes
Safety Permanency Well-Being

CFSR Performance
Baseline Data Describes current and historical views of
outcomes Describes Agency achievement of the
outcomes

Federal CFSR Findings
Outcome Associations
Includes the 35 States reviewed in 2002-2004
Case worker contacts with children and families demonstrate a high performance on Safety, Permanency and Well Being Outcomes

Findings Regarding Safety

Associations Between Safety Outcome 2 and other Indicators
Significant associations exist between Safety Outcome 2 and these indicators:
Needs & Services of Child, Parents, Foster Parents
Parents’ Involvement in Case Planning
Caseworker Visits with Child
Caseworker Visits with Parents
Timeliness of Initiating Investigations

Findings Regarding Permanency

Relationship of Well-Being to Permanency
Positive ratings on
• Services to children, parents, foster parents
• Involvement of parents in case planning
• Caseworker visits with children
• Caseworker visits with parents
Substantial
achievement on
• Timely achievement of permanency (Outcome P1)
• Preserving children’s connections while in foster care (Outcome P2)
supports . . .
Factors Associated with Timely Reunification, Guardianship, and Permanent Relative Placement
The strongest associations with timely reunification guardianship, and permanent relative placement include:
Caseworker Visits with Parents
Child’s Visits with Parents and Siblings in Foster Care
Services to Children, Parents, & Foster Parents
Family/Child Involvement in Case Planning
ASFA Requirements Regarding Termination of Parental Rights
Placement Stability

Factors Associated with Timely Adoption
The strongest associations with timely adoption include:
Needs & Services for Children, Parents and Foster Parents
Holding timely permanency hearings
Holding timely six-month case reviews
ASFA requirements regarding termination of parental rights

Factors Associated with Placement Stability
The strongest associations with placement stability include:
Placement with relatives
Services to children, parents, and foster parents
Involvement of children and parents in case planning
Caseworker contacts with parents (not children)
Age of child – most stable are ages 0 - 6 and 16 - 18 –
least stable are ages 13 - 15
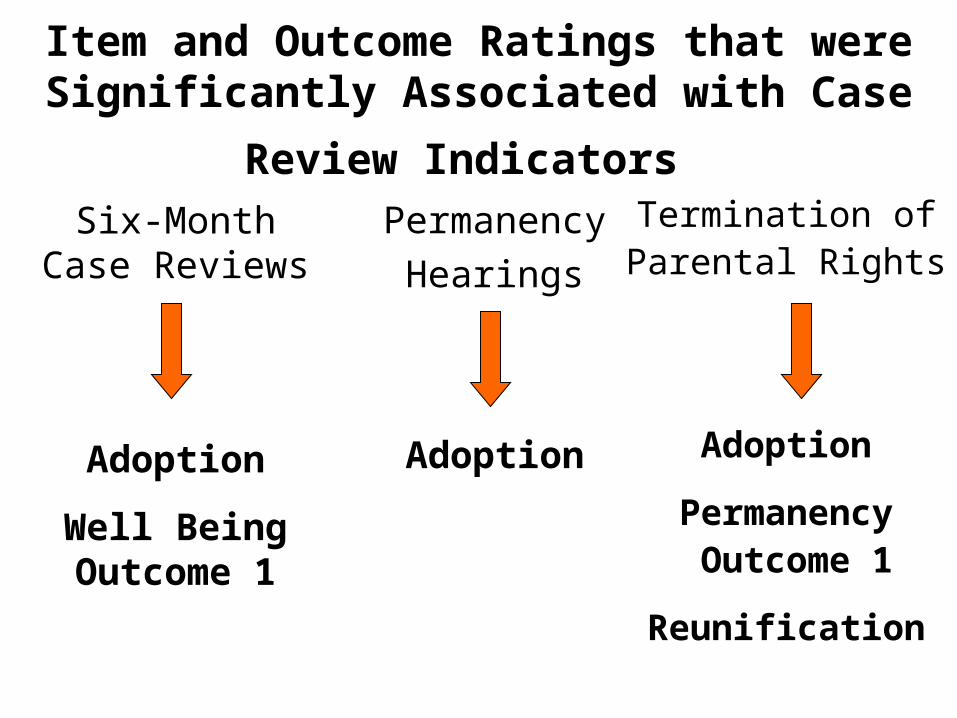
Item and Outcome Ratings that were Significantly
Associated with Case Review Indicators
Permanency
Hearings
Adoption
Termination ofParental Rights
Adoption
Permanency Outcome 1
Reunification
Six-Month Case Reviews
Adoption
Well Being Outcome 1

Findings Regarding Child & Family Well-Being

Association with Systemic Factors
States in substantial conformity with these 2 systemic factors had significantly higher percentages of cases rated substantially achieved for Well Being Outcome 1 than States that were not in substantial conformity with these systemic factors.
Service Array
Quality Assurance

Well Being: The Importance of
Caseworker Visits with Parents and Children

91% of the cases rated as a strength for Caseworker Visits with Parents were also
rated as a strength for Caseworker Visits with Children.
Caseworker Visits
with
Children
Caseworker Visits
with
Parents
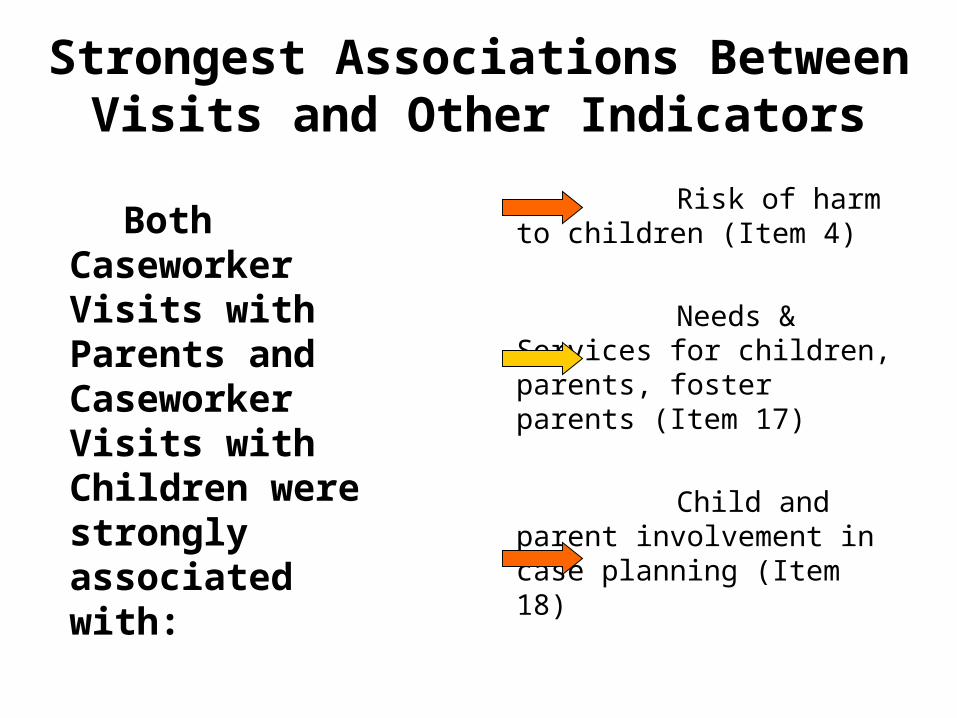
Strongest Associations Between Visits and Other Indicators
Both Caseworker Visits with Parents and Caseworker Visits with Children were strongly associated with:
Risk of harm to children (Item 4)
Needs & Services for children, parents, foster parents (Item 17)
Child and parent involvement in case planning (Item 18)

Other Significant Associations Between Visits and Indicators
Caseworker Visits with Parents and Caseworker Visits with Children were also strongly associated with:
Services to protect children at home Safety Outcome 1 Safety Outcome 2 Timely permanency goals Timely reunification Child’s visits with parents and siblings Relative placements Meeting educational needs Meeting physical health needs Meeting mental health needs
Recommended
![Tabletop Exercise Facilitator Handbook Template · Web viewFOR OFFICIAL USE ONLYAbout this Facilitator Guide FACILITATOR HANDBOOK [Exercise Name]Facilitator Handbook FACILITATOR HANDBOOK](https://img.dokumen.tips/doc/110x75/5ae2303b7f8b9a0d7d8bfd35/tabletop-exercise-facilitator-handbook-viewfor-official-use-onlyabout-this-facilitator.jpg)
















