
This article was downloaded by: [University of Delaware]On: 05 October 2014, At: 10:30Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
International Journal of Health Promotion andEducationPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/rhpe20
Components of Health Promoting Schools inUgandan primary schools: a pilot studyEriab M Nkamba a , Sylvia Tilford b & Sonia A Williams ca Faculty of Medicine , Makerere University , Kampala , Ugandab Leeds Metropolitan University , UKc Department of Dental Public Health , University of Leeds , UKPublished online: 17 May 2013.
To cite this article: Eriab M Nkamba , Sylvia Tilford & Sonia A Williams (2008) Components of Health PromotingSchools in Ugandan primary schools: a pilot study, International Journal of Health Promotion and Education, 46:3,84-93, DOI: 10.1080/14635240.2008.10708134
To link to this article: http://dx.doi.org/10.1080/14635240.2008.10708134
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”)contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensorsmake no representations or warranties whatsoever as to the accuracy, completeness, or suitabilityfor any purpose of the Content. Any opinions and views expressed in this publication are the opinionsand views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy ofthe Content should not be relied upon and should be independently verified with primary sources ofinformation. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands,costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly orindirectly in connection with, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial orsystematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution inany form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

84 Components of Health Promoting Schools in Ugandan primary schools: a pilot study
Components of Health Promoting Schools in Ugandan primary schools: a pilot study By Eriab M Nkamba, Faculty of Medicine, Makerere University Kampala, Uganda; Sylvia Tilford, Faculty of Health, Leeds Metropolitan University, UK; and Sonia A Williams, Department of Dental Public Health, University of Leeds, UK
Key words: Health promoting schools, children's health, Uganda.
Abstract
Health Promoting Schools (HPSs) represent key settings through which health can be improved. The World Health Organisation (WHO) has provided component indicators but data on the degree of coverage of these key components of HPSs in many countries are limited. The aim of this pilot study was to determine whether and to what extent information on the components of HPSs in Ugandan primary schools could be generated using focus group discussions (FGD) as well as through observational data.
Four schools (two rural and two urban) were randomly selected from the sampling frame of 18 rural and 76 urban government-aided primary schools in Mbale District, Uganda. Focus group discussions (FGDs) involving teachers, parents and pupils were held at each school. Indicators of HPSs were also observed and recorded at each of the selected schools. A scoring system was devised based on the number of positive attributes derived from the WHO list of component indicators. Descriptive analysis from FGDs and observational data was also undertaken.
Overall, the urban schools had a higher number of positive observations than rural schools for HPS indicators with some marked variation between urban and rural schools for specific indicators. This pilot study provided data to show that coverage of HPS components by different schools could be successfully evaluated using FGD and observational findings. Those strengths and shortcomings identified within and between the four schools necessitate further exploration with a larger scale study.
Introduction
The concept of Health Promoting Schools (HPS) is a key component of the settings approach to health promotion (WHO 1996a). The HPS model extends beyond the formal health education curriculum to include a consideration of physical and social environments of schools and partnerships with
families and others in pursuit of better health (WHO 1996b). Students can be influenced at developmental stages when lifelong behaviours are being established (MMWR 1996, WHO 1996a). Secondary socialisation derived from the school setting, plus parenting, offer the potential to build healthy norms, values and habits for a lifetime (Brody et al. 2002). Schools also provide the opportunity to reach other sections of the population, including school personnel, parents and members of the wider community (WHO 1996a).
The components of a HPS have been categorised in various ways (Allensworth & Kolbe 1987, WHO 1996a), but co-ordination between these different sectors is also important (St Leger 1999). These components include:
School Health Education (SHE): This involves curriculum-based educational activities, designed to help students acquire knowledge, attitudes, beliefs and skills needed to make informed healthy decisions and practise healthy behaviours. Health topics should be based on young people's needs, be realistically achievable and integrated across broad sections of the curriculum (WHO 1996b, Makuch & Reschke 2001, WHO 2003).
School Nutrition and Food Services: Poor nutritional status is associated with impaired growth, ill health and lower educational attainment (Horwitz 1983). School feeding programmes increase food availability while increasing and promoting healthy eating (WHO 1998). Such programmes need to be complemented by appropriate nutrition education within the formal curriculum. In addition, micronutrient supplements, including vitamin A capsules (to prevent blindness), iron tablets (to prevent anaemia) and iodized oil or salt (to prevent goitre) can be easily distributed by teachers at low cost (FAO/WHO 1992, Del Rosso & Marek 1996, Hall et al. 2002).
School and Community Collaboration: Families and communities can help students to understand, practise and share what they learn about health in the classroom and to cooperate in efforts to enhance the health promoting aspects of the environment (WHO/UNESCO/UNICEF 1992). In addition, acquisition of health-related behaviour patterns is easier when students receive relevant information through different channels (parents, teachers, peers
Dow
nloa
ded
by [
Uni
vers
ity o
f D
elaw
are]
at 1
0:30
05
Oct
ober
201
4
Components of Health Promoting Schools in Ugandan primary schools: a pilot study 85
and mass media) (Kelder et al. 1995, MMWR 1996). Physical Education and Recreation: Physical
education and recreation help individuals acquire physical fitness and provide opportunities for building self-confidence (WHO 1996b ). However, participation in sport risks the possibility of injury, and requires coordinated and effective school-based injury-prevention policies and procedures, alongside staff development and an appropriate physical environment (Sleet 1994).
Mental health and wellbeing: School counselling programmes provide social support in coping with difficulties, adjustments, growth and development, thus providing a buffer for stressful life events experienced by students and others (WHO 1996b ). Informal social support can also help students to resist pressures towards unhealthy behaviours (e.g. unhealthy eating) which are influenced by social forces (MMWR 1996).
Health promotion for school personnel: A HPS is concerned with the health of all its members, including the teachers. Teachers can also act as important role models for students and others. Preservice and in-service training can aid teachers to acquire health promotion knowledge which they can then use to improve their own health and also disseminate to students (MMWR 1996).
School Health Environment: The physical environment includes school buildings, interior structures, play grounds, eating facilities, water and foods provided at school and the surroundings in which the school is situated. The psychosocial school environment involves relationships between teachers and students, among teachers, and between parents and teachers (WHO, 1996b).
School Health Services (SHS): Collaborative working between the school and health services can result in aspects of health promotion, disease prevention and care being made available in school, in a cost-effective way with minimum disruption to learning and school activities (Petersen & Torres 1999). Designated personnel could include trained school nurses, designated teachers or a school health team who have had appropriate training (WHO 1996b, WHO 2003).
There are a significant number of examples of HPS interventions in Africa, for example, in Tanzania (Klep et al. 1997, Mwanri et al. 2001), Uganda (Kinsman et al. 2001), Nigeria (Oye-Adeniran 2004) and South Africa (Flisher et al. 2000). In addition, programmes addressing individual components have been cited. In Uganda, water, sanitation and hygiene, community mobilisation activities and school health education have all been reported as having positive impacts on school children (World Bank 1998).
School-based health programmes have formerly been characterised as heavily focussed on disease prevention, being uncoordinated, lacking integration, poorly evaluated and disseminated (Whiman et al.
2000). A move away from individual to multiple (intervention) strategies and adoption of the HPS concept is developing widely and dissemination of evidence of effectiveness has increased (Lister-Sharp et al. 1999, Whiman et al. 2000).
WHO (2000) has set guidelines on how to collect information on all components of HPSs. However, there are no generally agreed methods for evaluation of HPS interventions (Mukoma & Flisher 2004). Studies have addressed different components of HPS and subsequent comparison of such findings is difficult. There is need for a situational analysis that addresses ALL components as a prerequisite for a region-wide or country-wide assessment of the potential for interventions.
The aim of the present study was to conduct a situational analysis using WHO component indicators for HPS (WHO 1996a) at four Ugandan primary schools using mixed methodology. In addition to testing the methodology, this pilot study could help to indicate to what extent these schools were supportive of health promotion.
Materials and Methods
Study location: The study was conducted in the Eastern Region of Uganda, Mbale district, in Bungokho (rural) and Mbale municipality (urban) counties. Mbale Municipality covers a radius of Skm. The average number of pupils in urban schools was approximately 1200, compared with 400 in rural schools. Agriculture represents the main economic activity and major crops are coffee, beans, plantains (Matooke), maize, onions, Irish potatoes, carrots, sweet potatoes and cotton. Many serve as both cash and food crops.
Most health problems in Mbale can be related to poverty, illiteracy, malnutrition, malaria, poor living conditions and HIV/AIDS (District Director Health Services (DDHS) August 2004: personal communication). The district has one district hospital and a secondary referral hospital. Literacy rates for the district remain low at 64% for males and 49% for females. However, following the introduction of Universal Primary Education (UPE) in 1997, student enrolment has increased significantly although academic standards are still considered to be low (DDHS August 2004: personal communication).
Study design and sampling: The study was conducted during the period- August to November, 2004. Lists of schools provided by the District Education Officer were used to identify all primary schools satisfying the inclusion criteria and four schools (two urban and two rural) were recruited. Urban schools had to be at least 1km apart and rural schools at least 1 Okm apart in order to achieve potential variation between the environments of different schools. The sampling frame consisted of mixed, day government aided schools (Pine et al. 1997). Schools
CD 0 0
"' "' ~ E :::1 z ~ ~ :::1 g
I :::1
"C w o!S
~ E e a. ~ m J:
'5 (ij E :::1 0 ...., (ij c: 0
J
Dow
nloa
ded
by [
Uni
vers
ity o
f D
elaw
are]
at 1
0:30
05
Oct
ober
201
4
86 Components of Health Promoting Schools in Ugandan primary schools: a pilot study
('")
~ co 0 0 N ('")
Q; J:J E :::l z ~ Q)
E :::l g c: 0
~ :::l "0 UJ ell c: 0 :g E e a.
.<=
'iii Q)
I
0 c;; E :::l 0 ...., c;; c: 0
~ E .2l .!:
were selected using simple random sampling, while purposive sampling (Babbie 1990) was employed for selection of a mixed group of participants for focus group discussions (FGDs ). Any member of the school (student, teacher, support staff, parent) was eligible to participate in the study although the head teacher at each school guided the investigator during selection of participants. Teachers were selected on the basis of their responsibilities within the schools (e.g science teachers, teachers in charge of the curriculum, senior female teachers, and administrator and other teachers available at the time).
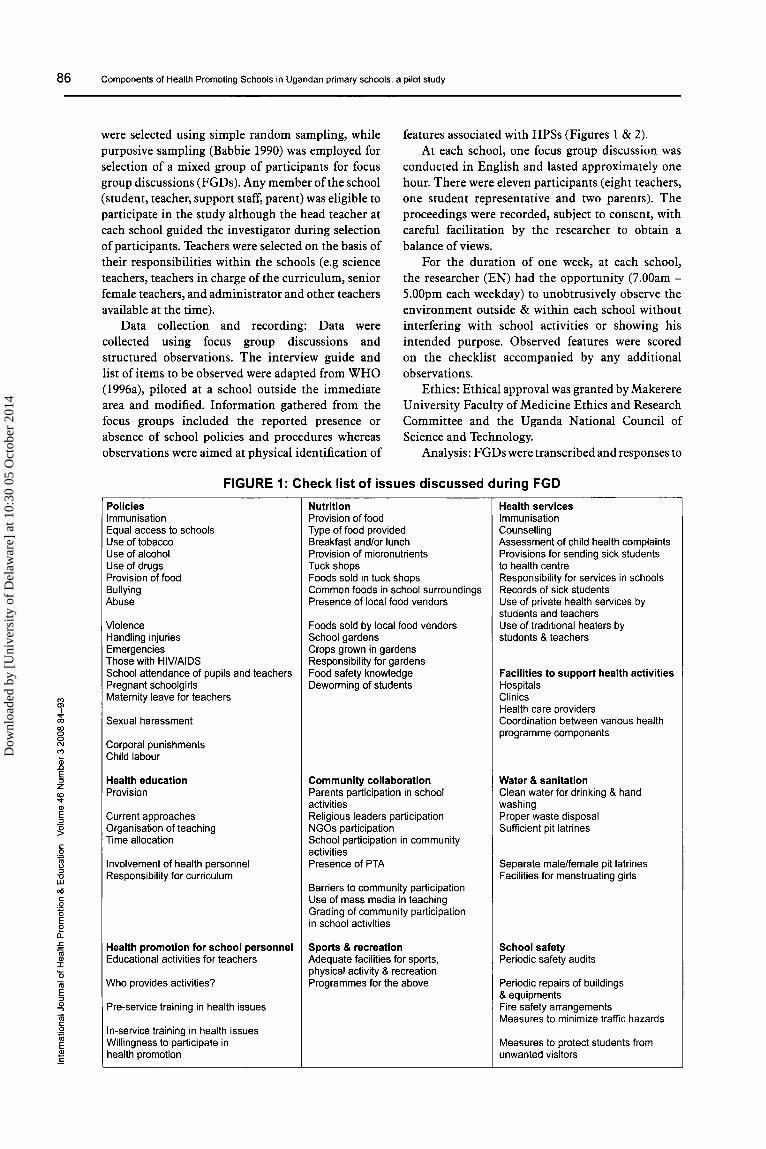
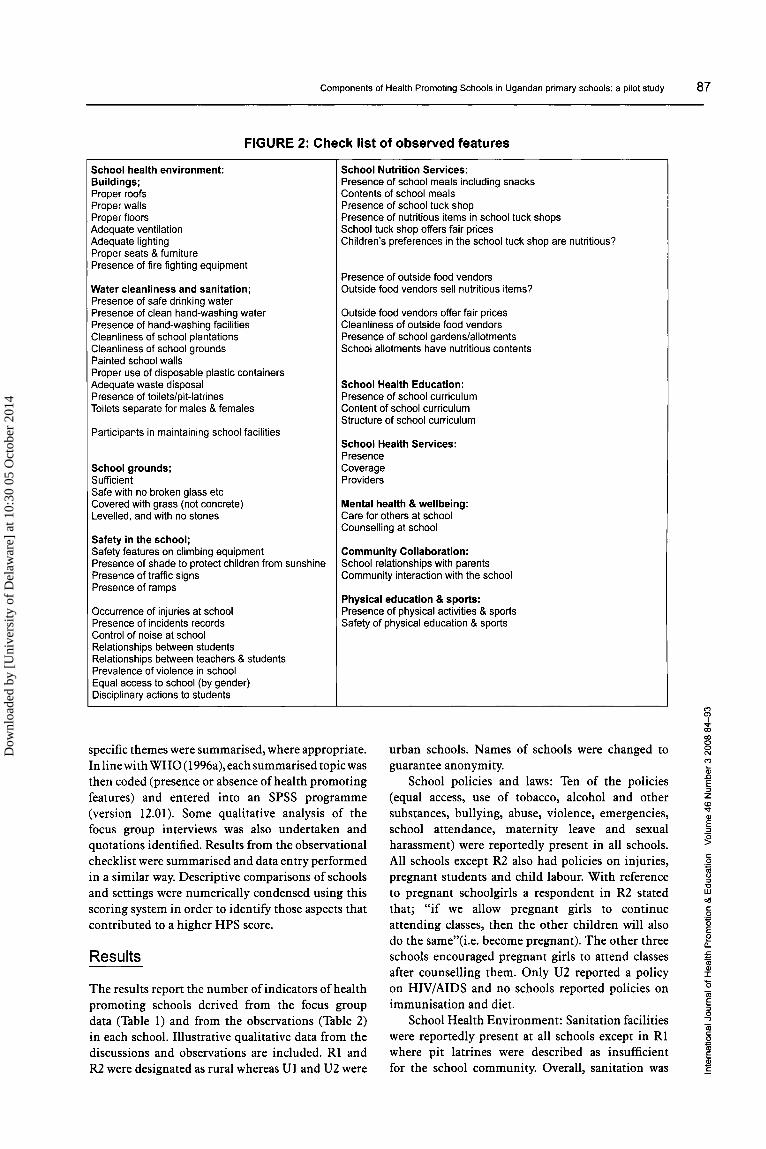
Data collection and recording: Data were collected using focus group discussions and structured observations. The interview guide and list of items to be observed were adapted from WHO (1996a), piloted at a school outside the immediate area and modified. Information gathered from the focus groups included the reported presence or absence of school policies and procedures whereas observations were aimed at physical identification of
features associated with HPSs (Figures 1 & 2). At each school, one focus group discussion was
conducted in English and lasted approximately one hour. There were eleven participants (eight teachers, one student representative and two parents). The proceedings were recorded, subject to consent, with careful facilitation by the researcher to obtain a balance of views.
For the duration of one week, at each school, the researcher (EN) had the opportunity (7.00am-5.00pm each weekday) to unobtrusively observe the environment outside & within each school without interfering with school activities or showing his intended purpose. Observed features were scored on the checklist accompanied by any additional observations.
Ethics: Ethical approval was granted by Makerere University Faculty of Medicine Ethics and Research Committee and the Uganda National Council of Science and Technology.
Analysis: FGDs were transcribed and responses to
FIGURE 1: Check list of issues discussed during FGD
Policies Nutrition Health services Immunisation Provision of food Immunisation Equal access to schools Type of food provided Counselling Use of tobacco Breakfast and/or lunch Assessment of child health complaints Use of alcohol Provision of micronutrients Provisions for sending sick students Use of drugs Tuck shops to health centre Provision of food Foods sold in tuck shops Responsibility for services in schools Bullying Common foods in school surroundings Records of sick students Abuse Presence of local food vendors Use of private health services by
students and teachers Violence Foods sold by local food vendors Use of traditional healers by Handling injuries School gardens students & teachers Emergencies Crops grown in gardens Those with HIV/AIDS Responsibility for gardens School attendance of pupils and teachers Food safety knowledge Facilities to support health activities Pregnant schoolgirls Deworming of students Hospitals Maternity leave for teachers Clinics
Health care providers Sexual harassment Coordination between various health
programme components Corporal punishments Child labour
Health education Community collaboration Water & sanitation Provision Parents participation in school Clean water for drinking & hand
activities washing Current approaches Religious leaders participation Proper waste disposal Organisation of teaching NGOs participation Sufficient pit latrines Time allocation School participation in community
activities Involvement of health personnel Presence of PTA Separate male/female pit latrines Responsibility for curriculum Facilities for menstruating girls
Barriers to community participation Use of mass media in teaching Grading of community participation in school activities
Health promotion for school personnel Sports & recreation School safety Educational activities for teachers Adequate facilities for sports, Periodic safety audits
physical activity & recreation Who provides activities? Programmes for the above Periodic repairs of buildings
& equipments Pre-service training in health issues Fire safety arrangements
Measures to minimize traffic hazards In-service training in health issues Willingness to participate in Measures to protect students from health promotion unwanted visitors
Dow
nloa
ded
by [
Uni
vers
ity o
f D
elaw
are]
at 1
0:30
05
Oct
ober
201
4
Components of Health Promoting Schools in Ugandan primary schools: a pilot study 87
FIGURE 2: Check list of observed features
School health environment: Buildings; Proper roofs Proper walls Proper floors Adequate ventilation Adequate lighting Proper seats & furniture Presence of fire fighting equipment
Water cleanliness and sanitation; Presence of safe drinking water Presence of clean hand-washing water Presence of hand-washing facilities Cleanliness of school plantations Cleanliness of school grounds Painted school walls Proper use of disposable plastic containers Adequate waste disposal Presence of toilets/pit-latrines Toilets separate for males & females
Participants in maintaining school facilities
School grounds; Sufficient Safe with no broken glass etc Covered with grass (not concrete) Levelled, and with no stones
Safety in the school; Safety features on climbing equipment Presence of shade to protect children from sunshine Presence of traffic signs Presence of ramps
Occurrence of injuries at school Presence of incidents records Control of noise at school Relationships between students Relationships between teachers & students Prevalence of violence in school Equal access to school (by gender) Disciplinary actions to students
School Nutrition Services: Presence of school meals including snacks Contents of school meals Presence of school tuck shop Presence of nutritious items in school tuck shops School tuck shop offers fair prices Children's preferences in the school tuck shop are nutritious?
Presence of outside food vendors Outside food vendors sell nutritious items?
Outside food vendors offer fair prices Cleanliness of outside food vendors Presence of school gardens/allotments School allotments have nutritious contents
School Health Education: Presence of school curriculum Content of school curriculum Structure of school curriculum
School Health Services: Presence Coverage Providers
Mental health & wellbeing: Care for others at school Counselling at school
Community Collaboration: School relationships with parents Community interaction with the school
Physical education & sports: Presence of physical activities & sports Safety of physical education & sports
specific themes were summarised, where appropriate. In line with WHO (1996a), each summarised topic was then coded (presence or absence of health promoting features) and entered into an SPSS programme (version 12.01). Some qualitative analysis of the focus group interviews was also undertaken and quotations identified. Results from the observational checklist were summarised and data entry performed in a similar way. Descriptive comparisons of schools and settings were numerically condensed using this scoring system in order to identify those aspects that contributed to a higher HPS score.
urban schools. Names of schools were changed to guarantee anonymity.
School policies and laws: Ten of the policies (equal access, use of tobacco, alcohol and other substances, bullying, abuse, violence, emergencies, school attendance, maternity leave and sexual harassment) were reportedly present in all schools. All schools except R2 also had policies on injuries, pregnant students and child labour. With reference to pregnant schoolgirls a respondent in R2 stated that; "if we allow pregnant girls to continue attending classes, then the other children will also do the same"( i.e. become pregnant). The other three schools encouraged pregnant girls to attend classes after counselling them. Only U2 reported a policy on HIV/AIDS and no schools reported policies on immunisation and diet.
Results
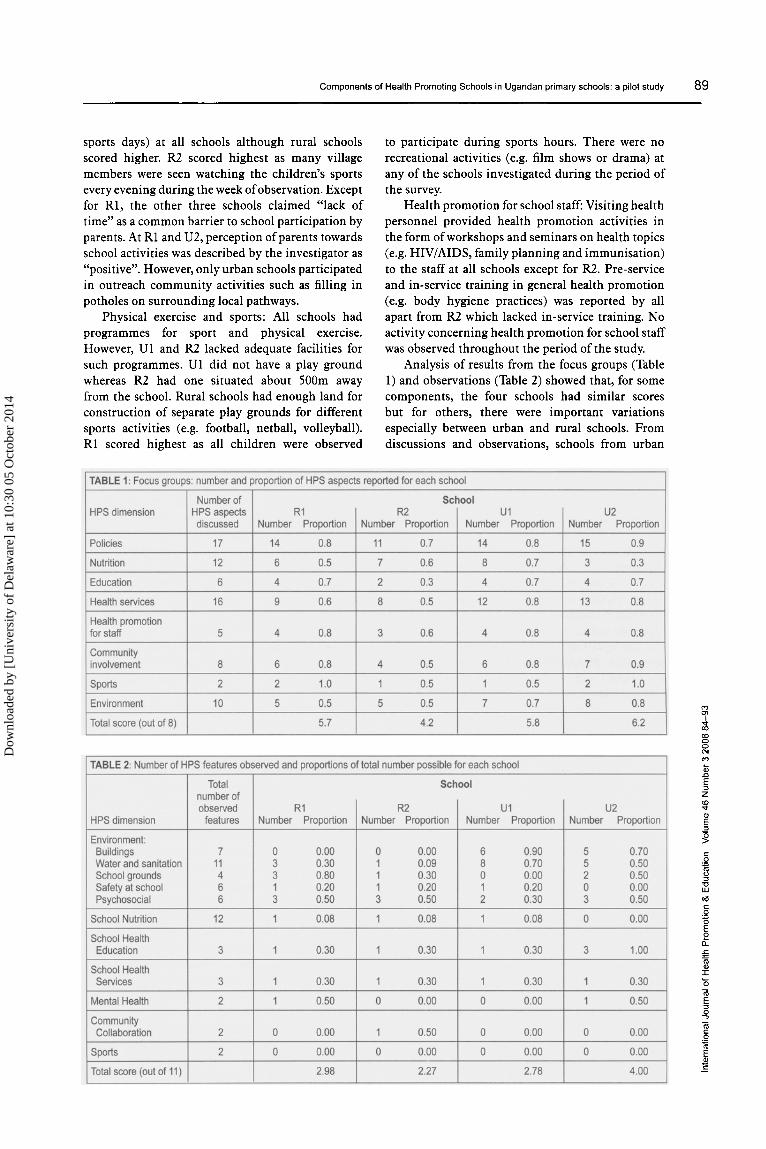
The results report the number of indicators of health promoting schools derived from the focus group data (Table 1) and from the observations (Table 2) in each school. Illustrative qualitative data from the discussions and observations are included. Rl and R2 were designated as rural whereas Uland U2 were
School Health Environment: Sanitation facilities were reportedly present at all schools except in Rl where pit latrines were described as insufficient for the school community. Overall, sanitation was
"' ~ <Xl 0 0 N
"' Q; .c E :J z (L)
""" Ql E :J
:g
" 0
~ :J "0 UJ <>15
" 0
'5 E 2 c.. E "' Ql I
0 "iii E :J 0 ...., "iii " 0
~ E ~ E
Dow
nloa
ded
by [
Uni
vers
ity o
f D
elaw
are]
at 1
0:30
05
Oct
ober
201
4

88 Components of Health Promoting Schools in Ugandan primary schools: a pilot study
"' Cl
~ (X) 0 0 N
"' Q; ~
E :J z <0 ..,. CD E :J
g c 0
~ u :J -o LJ.J all c 0
'E E e
o._
£ <1i CD I
0 <1i c :; 0 -,
<1i c 0 -~
E .'!l E
better in urban than rural schools (e.g. urban had separate male and female pit latrines). Hand washing facilities were reported as present in all schools. R2 did not have facilities for menstruating girls and Ul declined to give a response. In Rl, it was stated that "plans are underway to get a change of dress similar in design and colour to the school uniform for girls who soil their dresses during menstruation periods such that the other students (especially boys) do not recognise that something has gone wrong". From the observations, all schools had access to safe water for drinking and hand-washing. In addition, students participated in the cleaning of school compounds. All schools had specified sites within the school compounds for burning waste although R2 was not adequately dealing with plastic containers.
Students were allegedly protected from unwanted visitors at all schools as visitors reported to school offices. However, none had fire safety arrangements or measures to minimise traffic hazards. Observations were in conformity with the reported data.
Periodic safety audits for repairs of buildings and equipment were only reported in the urban schools. Observations also revealed that both rural schools had rusty iron roofing sheets on most buildings with unpainted walls, dusty floors and poor ventilation although conditions in Rl were relatively better than in R2. All buildings in Ul had electric lighting, but some buildings in U2 and all buildings in the rural schools depended on natural light. Adequate furniture was seen in both urban schools, but some children in the rural schools were observed to study while seated on the floor. Ul had inadequate space for school compounds, including play grounds. No foreign objects such as broken glass were observed in play areas, although stones which could present hazards were noted on existing play grounds.
Psychosocial environment: No cases of violence were seen although some minor disagreements were witnessed in all schools. Relationships between students and teachers appeared to be good at all schools except at Ul where some teachers were observed to be harsh to students (e.g. caning on students' heads) particularly if they were late for classes. All schools showed some degree of care for others as children were seen comforting their peers following accidents (e.g. falls while playing). U2 had less control over noise within the school whereas R2 did not offer any form of counselling.
School Food and Nutrition Services: None of the schools provided students with free school meals or with micronutrient supplements during school hours. Ul was the only school with a school tuck shop where sales included fizzy drinks, various items of confectionary and mineral water. U2 had access to a near-by shop where students bought similar items. Some teachers thought that provision of food for school children was not their responsibility. For example one teacher from U2 stated that; "we are
here to teach them but not to provide them with food".
Children at all four schools accessed local food vendors during lunch break to buy items such as ripe sweet bananas, fresh cooked maize, and other local fruits. Items were reportedly cheaper than in the local markets. School gardens were cultivated by students and teachers at all schools except U2 which lacked a garden. Food crops from school gardens and local vendors did not differ from the reported staple foods in the areas and mainly provided sources of carbohydrates (e.g. cassava, maize, potatoes and rice). Children at all four schools were reported to have some knowledge about food safety (e.g. safe storage of foods, washing hands before eating and consumption of fully cooked foods). Children in all schools participated once a year in deworming programmes against hookworms (to avoid anaemia). Observations regarding foods and drinks sold, and the content of school gardens concurred with results from the previous discussions. Children classified as orphans in Rl and Ul were seen to be receiving school lunches funded by Compassion (an NGO). Food supplied was mainly cooked cone maize flour and beans.
School Health Education was claimed to be integrated into other subjects in all four schools and materials plus methods used (e.g. posters and topics at general assemblies) were similar. All schools except R2 used mass media in the form of radio programmes to provide some special health messages (e.g. on HIV/AIDS) to both teachers and children during school hours. School staff participated in the selection of subjects for the curriculum and health service personnel participated in health education at all schools except R2. Time allocated to health education per week varied between the schools- Ul (200 minutes), R2 (90 minutes), U2 and Rl (not specified).
School Health Services: There were variations between the schools. R2 reported lack of first aid services, possibly linked to lack of teacher training. U2 was the only school where immunisation services were available. Except for R2, teachers from the other three schools stated that they provided health care support (counselling, health checking for body hygiene, and referrals) for school communities. Only urban schools claimed that they kept records of incidents (e.g. accidents, sickness) for students although physical existence of records was only witnessed at Ul. In addition to use of private health care services, urban schools reportedly availed themselves of traditional healers. All schools allegedly accessed clinics and health care providers, but hospital services were felt to be much more accessible for urban schools.
Community collaboration: The local community was reported as involved and participating in school activities (e.g. attendance at school festivals and
Dow
nloa
ded
by [
Uni
vers
ity o
f D
elaw
are]
at 1
0:30
05
Oct
ober
201
4
Components of Health Promoting Schools in Ugandan primary schools: a pilot study 89
sports days) at all schools although rural schools scored higher. R2 scored highest as many village members were seen watching the children's sports every evening during the week of observation. Except for Rl, the other three schools claimed "lack of time" as a common barrier to school participation by parents. At Rl and U2, perception of parents towards school activities was described by the investigator as "positive". However, only urban schools participated in outreach community activities such as filling in potholes on surrounding local pathways.
Physical exercise and sports: All schools had programmes for sport and physical exercise. However, Ul and R2 lacked adequate facilities for such programmes. Ul did not have a play ground whereas R2 had one situated about SOOm away from the school. Rural schools had enough land for construction of separate play grounds for different sports activities (e.g. football, netball, volleyball). Rl scored highest as all children were observed
to participate during sports hours. There were no recreational activities (e.g. film shows or drama) at any of the schools investigated during the period of the survey.
Health promotion for school staff: Visiting health personnel provided health promotion activities in the form of workshops and seminars on health topics (e.g. HIV/AIDS, family planning and immunisation) to the staff at all schools except for R2. Pre-service and in-service training in general health promotion (e.g. body hygiene practices) was reported by all apart from R2 which lacked in-service training. No activity concerning health promotion for school staff was observed throughout the period of the study.
Analysis of results from the focus groups (Table l) and observations (Table 2) showed that, for some components, the four schools had similar scores but for others, there were important variations especially between urban and rural schools. From discussions and observations, schools from urban
(")
i co 0 0 N (")
Q; Il E :::1 z <!> '<t
<1> E :::1
:g <:::
.Q
1§ :::1 '0 UJ 0(1
<::: 0 :g E e [l.
:5 'iii <1> J:
0 'iii E :::1 0 ...., 'iii <::: 0
~ E
~
Dow
nloa
ded
by [
Uni
vers
ity o
f D
elaw
are]
at 1
0:30
05
Oct
ober
201
4

90 Components of Health Promoting Schools in Ugandan primary schools: a pilot study
"" 9' .... co co 0 0 N
"" ~ E ::l z
CD .... Q)
E ::l
~
settings recorded higher proportions of HPS aspects for the major components described in the literature review.
Discussion
Mbale district from the Eastern Region of Uganda was selected as fairly representative of that country, providing both urban and rural school settings. However, caution should be taken when interpreting 'urban' and 'rural' settings for a given country. Levels of urbanisation are relative and Ugandan definitions of urban areas and schools are likely to be different from those of other countries.
Purposive sampling was adopted for the FGDs as is customary, in order to elicit a broad range of views (Babbie 1990). While a typical sample is desirable, it was assumed that the head teachers' guidance on participant selection was appropriate. Nevertheless, the choice of a single student will have underrepresented opinions on some issues (e.g. the impact of school health promotion initiatives), however well the FGD was moderated. Future studies will need to ensure an increased student representation, preferably using separate focus groups and with parental and other community involvement also organised. FGD validity can be affected by the accuracy of respondents' reports, for example, in self reporting beliefs and behaviours, subjects may report what they perceive as the correct answers rather than what they actually believe or do. Participants may also be unwilling to discuss socially undesirable behaviours (Rose 1997). Validity of reported data was verified by personal observations, although the period of one school week will tend to highlight regular rather than occasional events. These factors may also help to explain why the score for the FGDs was higher than for observational data.
In focusing on defined aspects of HPS the study gave limited attention to the concept of HPS held by participants. This can be addressed in a wider study which would also aim to extend the qualitative analysis of data. Within rural or urban settings, it was also difficult to conclude that the two schools from either setting were equally rural or equally urban. In addition, the crude system used in allocation of scores could not allow for confounders (e.g. school size, location and resource accessibility). However, the findings provide an insight into the present and offer a basis on which further research could be conducted.
The results provide data on components of HPS present in the study schools so that aspects for future development can be identified. These findings can also support the schools themselves to pinpoint their own starting points for further development. Building healthy national policies and the development of intersectoral collaboration are major strategies consistent with the Ottawa Charter (WHO 1986) and
the Primary Health Care Approach (WHO 1978) and such policies are integral to a settings approach to health promotion. National school policies aimed at promoting health among schoolchildren in Uganda include guidelines for school construction and maintenance, immunisation requirements upon entry to primary schools, equity (e.g. gender, tribal, social class), bullying, sexual harassment and use of substances, among others. The schools scored relatively high in reported policies and the results indicated that the four schools were following national policies to differing extents. However, the data indicated that there were gaps in translating policies into action in a number of areas.
Coordinating mechanisms at the national, district and local/school levels can help transform national policies into action. However, lack of many policies at R2 suggested that there was little collaboration between the school and education authorities, supported by the fact that school teachers were not involved during formulation of the school curriculum. Community involvement at all stages of an initiative is another pillar which ensures that implementation and sustainability are effected (WHO 1978, 1986). Lack of immunisation requirements at all schools in the presence of a national policy on immunisation also suggested weakness in collaboration between the Ministry of Education and the schools or that school communities had not been involved during the formulation of policies.
A clear omission was the lack in all schools of policies on diet and micronutrient supplementation. Evidence from studies in Jamaica (Simeon 1998) and U ganda(Dolan & PCD 1998)suggest that programmes that alleviate hunger in schools are likely to result in improvements in school achievement. The foods reportedly accessible to children in all schools (from tuck shops, food vendors and at home) were mainly sources of carbohydrates. In addition, children from urban schools were more exposed to refined sugars than those in the rural schools. Absence of school gardens at U2limited the students from gaining food growing skills. It is recommended that school food services such as the tuck shops, local food vendors and school gardens offer a variety of healthy food choices and limit the availability of foods with low nutritional value (Santos Roy 1996) to ensure that knowledge and skills developed in the classroom can have an immediate practical impact (MMWR 1996).
Integration of school health education (SHE) with other subjects was found in all schools but the quality of that provision would need to be examined by more detailed evaluation of process and outcome (WHO 1996b ). The effectiveness of SHE is affected by the amount of classroom time devoted to the programme (Education Development Centre, Inc. 1995). Where health education is integrated into other subjects it can be difficult to assess the total time involved as was the case for two schools in this study.
Dow
nloa
ded
by [
Uni
vers
ity o
f D
elaw
are]
at 1
0:30
05
Oct
ober
201
4

Components of Health Promoting Schools in Ugandan primary schools: a pilot study 91
Research shows that training of teachers improves the implementation ofhealth promotion programmes (Connell et al. 1985). Training can be provided as part of initial teacher training but effective health promoting schools initiatives also require in-service training for career development. One of the rural schools (R2) had particular shortcomings as far as training was concerned. In-service training for school staff can enable them to acquire personal skills and adopt healthy lifestyles which can then be disseminated more widely during their teaching.
Differences were noted in how health care was organised and provided in the schools. Although equitable distribution of health services has been recommended by WHO (1978), rural schools lacked access to hospital facilities. Use of private clinics by school communities was reported at all the schools. WHO (2003) recommends that in establishing a SHS, it is necessary to assess what health services are available in the community which need not be duplicated in the school setting. Schools can make significant contributions to services.
Successful implementation and sustainability of HPS projects requires collaboration with others (e.g. surrounding community and other agencies, both governmental and non-governmental) (WHO 1978, 1986). In the current study, communities at all schools investigated were reported to participate in school activities (e.g. sports, drama, school open days and general meetings). However, the extent of participation as conceived within the HPS concept was relatively limited and some negative perceptions of communities were identified in two of the schools. Participation in community activities appeared to be better in urban than in rural schools although the reasons for this difference did not emerge. However much the community would like to get involved in school health programmes, some factors such as lack of time and transport, cultural and language barriers, previous negative experiences or attitudes towards school can hinder their participation (Fullan 1991, White et al. 1992, Hahn et al. 1996).
Supportive school environments depend on both the physical (buildings, grounds, interior structures) and psychosocial environment. Poor sanitation is the key element in contaminating the environment, spreading pathogens, and transmitting disease (Williams et al. 1990, WHO 1996b). Responses from all schools indicated that relatively good sanitation existed although observational data (particularly on buildings, water and sanitation) indicated that rural schools exhibited a poorer school environment in this respect. Regardless of the presence of handwashing facilities, diarrhoeal diseases were reported by all the schools. Possibly the 'good sanitation' described was a biased social desirability response since respondents might be embarrassed to admit that they endured poor sanitary conditions. Data on domestic sanitation would clarify whether the
causes of diarrhoea arose from their home or school environments.
The two urban schools, taken together, scored higher than their rural counterparts in the proportion of health promoting schools components noted on the basis of both FGD and observations. There were a number of fairly clear differences between schools in the two areas. Urban school-buildings were structurally sounder (e.g. cemented floors, nonleaking roofs). Yet in contrast, rural schools offered more space for school gardens and provided access to outside vendors who normally sold fresh foods and fruits to school communities. In contrast, urban schools did not permit entry to outside vendors. Here, young people had access, through a tuck shop in one urban school and a nearby shop at the other, to more refined carbohydrate snacks and confectionery, thus providing less healthy options when compared to their rural peers.
Within the context of the key components of health promoting schools, individual schools may choose their own priorities for action. It would not be appropriate to conclude that a given school was not health promoting if it lacked what it did not consider to be a priority (WHO 1999). Schools in urban and rural areas may have different priorities and it would be logical to consider rural and urban settings as two different entities such that schools from each location are compared with similar schools. On the basis of the quantitative summations the schools here can be placed in descending order on indicators of the health promoting school: U2, U1, R1 and R2.
This pilot study should precede a larger scale study involving more schools to elicit whether the findings identified here are more generalisable and in particular, whether certain differences between rural and urban schools perpetuate inequalities. Some suggestions can be fed back to participating schools which they may wish to consider in moving forward in developing their schools as health promoting settings: to review policies in place in schools and identify omissions; to consider the extent to which policies are actually implemented and the activities in relation to specific aspects of health are properly integrated; to give particular attention to policies on nutrition and health and ensure that all aspects of the school are consistent with these policies. In particular all schools might consider the possibilities for extending the range of foods available to children and reducing access to refined carbohydrates.
Conclusions
A pilot feasibility study of a situational analysis using WHO component indicators for HPS was successfully conducted in four Ugandan primary schools using focus group discussions and participant observation. Taken together the urban schools had a higher
"' CJ)
~ CXl 0 0 N
"' Q; .c E :::J z
"' q-(J)
E :::J
~ c 0
~ :::J "0 w all c 0 :g E e a. £
'" "' I
0
'" E :::J 0 .,
'" c .Q 1ii E ~ E
Dow
nloa
ded
by [
Uni
vers
ity o
f D
elaw
are]
at 1
0:30
05
Oct
ober
201
4
92 Components of Health Promoting Schools in Ugandan primary schools: a pilot study
("")
~ "' 0 0 N ("")
(i; .0 E ::J z
CD
"'" QJ
E ::J
g c:
.Q
~ ::J "0 UJ oil c: 0
~ E e a. .s:::
~ I
0 n; E ::J 0 ...., n; c: 0
~ E $ .=
number of positive observations than rural schools for HPS indicators with some marked variation between urban and rural schools for specific indicators. Those strengths and shortcomings identified within and between the four schools necessitate further exploration with a larger scale study.
Acknowledgements
The authors would like to extend their sincere thanks to the Department of Dental Public Health, University of Leeds; Makerere University, Uganda and the participating schools for their support with this study.
References
Allensworth D & Kolbe LJ ( 1987). The comprehensive school health programme: exploring an expanded concept. Journal of School Health, 57(10), 409-411.
Babbie E (1990). Non-probability sampling. In: Survey research methods; 2nd edn. Belmont, California: Wadsworth publishing company.
Brody G H, Dorsey S, Forehand R & Armistead L (2002). Unique and protective contributions of parenting and classroom processes to the adjustment of American children living in singleparent families. Child Development, 73 (1), 274-286.
Connell DB, Turner RR & Mason EF (1985). Summary of findings of the school health education evaluation: health promotion effectiveness, implementation, and costs. Journal of School Health, 8, 316-321.
Del Rosso JM, & Marek T (1996): Class Action: improving school performance in the developing world through better health and nutrition. Directions in development series. Washington D.C: World Bank.
Dolan C. & PCD (1998). School Based Health & Nutrition Programmes: findings from a survey of donor and agency support [Online]. [Accessed 2nd February 2005]. Available from World Wide Web: <http://www.schoolsandhealth.org/ countries/uganda.htm>
Education Development Centre, Inc. (1995). Education for Health: A Guide to Implementing a Comprehensive Approach to School Health Education. Atlanta G.A: Centres for Disease Control and Prevention.
FAO/WHO (1992). Nutrition: The Global Challenge. Final Report of the Conference. Rome: International Conference on Nutrition (ICN).
Flisher, AJ, Cloete, K Johnson, B. Et al (2000) Health Promoting Schools: lessons from Avondale Primary School., in Donal, D, Dawes, A.and Louw, J. Addressing Child Adversity. Cape Town David Philip:
Fullan M (1991). The new meaning of educational
change. 2nd edn. New York: Teachers College Press.
Hahn EJ, Simpson MR & Kidd P (1996). Cues to
parent involvement in drug prevention and school activities. Journal of School Health, 66(5), 165-170.
Hall A, Roschink N, Ouattara F et al. (2002): A randomised trial in Mali of the efficacy of weekly iron suoolementation given by teachers on the haemoglobin concentration of schoolchildren. Public Health Nutrition, 5(3), 413-418.
Horwitz A (1983). Why Teach Nutrition and to Whom? In: Nutrition Intervention Strategies in National Development, Chapter 31. New York: Academic Press.
Kelder SH, Perry CL, Lytle LA & Klepp KI (1995). Community-wide youth nutrition education: long term outcomes of the Minnesota Heart Health Programme. Health Education Research, 10(2), 119-131.
Kinsman J, Harrison S, Kengeya-Kayondo J et al. (1999). Implementation of a comprehensive AIDS education programme for schools in Masaka District, Uganda. AIDS CARE, 11(5), 591-601.
Klepp KI, Ndeki SS, Leshabari MT, Hannan PJ, Lyimo BA (1997). AIDS education in Tanzania: promoting risk reduction among primary school children. American Journal of Public Health, 87(12), 1931-1936.
Lister-Sharp D, Chapman S, Stewart-Brown S & Sowden A (1999). Health promoting schools and health promotion in schools: two systematic reviews. Health Technology Assessment, 3(22), 1-209.
Makuch A & Reschke K (2001). Playing games in promoting childhood dental health. Patient Education and Counselling, 43, 105-110.
MMWR (1996). Guidelines for School Health Programmes to Promote Lifelong Healthy Eating. Morbidity and Mortality Weekly Report, 45(RR-9), 1-41.
Mukoma W & Flisher AJ (2004). Evaluations of health promoting schools: a review of nine studies. Health Promotion International, 19(3), 357-368.
Mwanri L, Worsley A, Masika J, (2001). School and anaemia prevention: current reality and opportunities - a Tanzanian case study. Health Promotion International, 16(4), 321-331.
Oye-Adeniran BA, Adewole IF, lwere N, Mahmoud P. (2004). Promoting sexual and reproductive health and rights in Nigeria through change in medical school curriculum. African Journal of Reproductive Health, 8(1), 85-91.
Petersen PE & Torres AM (1999). Preventive oral health care and health promotion provided for children and adolescents by the Municipal Dental Health Service in Denmark. International Journal of Paediatric Dentistry 9, 81-91.
Dow
nloa
ded
by [
Uni
vers
ity o
f D
elaw
are]
at 1
0:30
05
Oct
ober
201
4
Components of Health Promoting Schools in Ugandan primary schools: a pilot study 93
Pine C, Pitts NB & Nugent ZJ (1997). British Association for the Study of Community Dentistry (BASCO) guidance on sampling for surveys of child dental health - A BASCD coordinated Dental Epidemiology Programme quality standard. Community Dental Health, 14, (Suppll), 10-17.
Rose L (1997). Qualitative research methods - data collection and analysis. In: Research Methods in Primary Care. Eds: Y Carter & C Thomas, p 44. Marcham Road, Abingdon: Radcliffe Medical Press Ltd.
Santos Roy DD (1996). No junk food in the school canteen. World Health Magazine, 49(4), 23.
Simeon DT (1998). School feeding in Jamaica: a review of its evaluation. American Journal of Clinical Nutrition, 67(suppl), 790-794.
Sleet DA (1994). Injury prevention. In: P Cortese & K Middleton (eds). The comprehensive school health challenge: promoting health through education. Santa Cruz, CA: ETR Associates. pp 443-489.
St Leger LH (1999). The opportunities and effectiveness of the health promoting primary school in improving child health- a review of the claims and evidence. Health Education Research, 14, 51-69.
Whiman CV, Aldinger C, Levinger B, Birdthistle I & Jones J (2000). Education For All (EFA) 2000 assessment: Thematic Study on School Health and Nutrition (final draft). Education Development Centre: WHO.
White KR, Taylor JJ & Moss VD ( 1992). Does research support claims about the benefits of involving parents in early intervention programmes? Review of Educational Research, 62,92-125.
WHO (1978). Alma-Ata 1978. Primary Health Care: report on the conference of Primary Health Care. Geneva: WHO.
WHO (1986). Ottawa Charter for Health Promotion. International Conference on Health Promotion 17-21, November 1986. Ottawa: WHO.
WHO (1996a). Promoting Health through Schools: The World Health Organization's Global School Health Initiative. Geneva: WHO (WHO/HPR/ HEP/96.4).
WHO (1996b). The Status of School Health. Geneva: WHO (WHO/HPR/HEP/96.1).
WHO (1998). Healthy Nutrition: An Essential Element of a Health Promoting School. Geneva: WHO.
WHO (1999). Preventing HIV/AIDS/STI and related discrimination: An important responsibility of Health-Promoting Schools. Geneva: WHO (WHO/HPR/HEP /98.6 ).
WHO (2000). Local Action. Creating Health Promoting Schools: Information series on school health. Geneva: WHO (WHO/NMH/HPS/00.4).
WHO (2003). Oral Health Promotion: An Essential
Element of a Health-Promoting School. Geneva: WHO.
WHO/UNESCO/UNICEF ( 1992). Comprehensive School Health Education: Suggested Guidelines for Action. Geneva: WHO.
Williams T, Moon A & Williams M (1990). Food, Environment and Health: a guide for primary school teachers. Geneva: WHO.
World Bank (1998). School Health Programmes by Country [Online]. [Accessed 2nd February 2005]. Available from World Wide Web: <http://www. schoolsandhealth.org/countries/uganda.htm>
Address for Correspondence
Dr. Eriab Moses Nkamba C/o Makindye Medical Centre PO Box 452 Kampala, Uganda E-mail: [email protected] +
"' ~ <X)
<X) 0 0 N
"' ~ E ::J z
«:> ...,. Q)
E ::J
;g c .Q
~ ::J '0 w o1S c 0
~ E E'
[l_
:5 ~ I 0
'" c :; 0 ....,
'" c .Q 1ii E .$ c
Dow
nloa
ded
by [
Uni
vers
ity o
f D
elaw
are]
at 1
0:30
05
Oct
ober
201
4
Recommended





![A health and nutrition promoting schools [Autosaved] (1)](https://img.dokumen.tips/doc/110x75/58f16c8e1a28ab8b188b466d/a-health-and-nutrition-promoting-schools-autosaved-1.jpg)











