
COLLABORATION IN CARDIOVASCULAR INTERVENTIONS: A NON-ZERO SOLUTION
Department of Surgery Grand RoundsApril 4, 2012

DISCLOSURES
• No financial conflicts
• Off-label uses of devices
ASSERTIONS
1. Traditional barriers between medical specialties result in a provider-centric rather than a patient-centric healthcare system
2. These barriers are no longer compatible with the effective application of today’s interventional technologies
3. Elimination of these barriers improves patient outcomes (win) and offers a non-zero opportunity for providers (win-win)

Traditional barriers between medical specialties result in a provider-centric rather than a patient-centric healthcare system
ORGANIZED BY PROVIER SKILL SET NOT PATIENTS CONDITION
Conditions-Disease Process• Coronary Artery Disease• Valvular Disease• Heart Failure• Aortic Disease• Peripheral Vascular Disease
Specialties-Skills/Knowledge• Cardiology• Interventional Cardiology• Cardiac Surgery• Vascular Surgery• Radiology

CARE IS DECENTRALIZED• Patients are forced to seek
care sequentially from various subspecialites (eg multiple appts)
• Lack of centralization results in poor information transfer between providers and duplicative care
• Ultimately, patients forced to make decisions based on complex information provided by multiple disparate sources with competing interests
Interventional Cardiology General
Cardiology
Surgery
Treatment

QUICK POLL
• What is the difference between a “root aneurysm” and a “AAA”?
• Who is most appropriate to manage these conditions?

ANSWER
• When most physicians don’t know the differences and appropriate treatment . . . Why do we expect patients to know where to seek care. . .
– Cardiology?– Interventional Cardiology?– Cardiac Surgery?– Vascular Surgery?– Radiology?

PATIENT CENTRIC MODEL
Disease-Specific “Clinic” (eg, CAD, Valve, HF, Ao) w Cards/Imaging/IC/CVS
Diagnostics
Referring Treatment
REASONS FOR DIVISIONS• Cultural
– Education/skill sets/knowledge base– How physicians are identified– Mentors/Colleagues/Interests
• Resources– Tools– Physically location
• Office space• Point of service (Clinic vs OR vs Cath Lab)
• Competition• Resentment
– “You only refer me your disasters . . . and your complications . . . and at night/weekends”

These barriers are no longer compatible with the effective application of today’s interventional technologies

Drugs Open Surgery
TREATMENT OPTIONS

Drugs Open Surgery
TREATMENT OPTIONS
Medical Physician Surgeon
• Its clear who provides which services• More likely to be complementary, less likely competing

ERA OF INTERVENTIONS
• Implantation pacemaker -1958• Balloon embolectomy - 1960• Angioplasty – 1974• Coronary angioplasty – 1977• Implantable ICD - 1980• Cardiac ablation – 1980s• Self expanding vascular stent – 1985• Endovascular aneurysm repair – 1987• Thoracic endovascular aneurysm repair – 1994• Transcatheter valves - 2002

Drugs Open Surgery
CONTINUUM OF INVASIVENESS OF THERAPY
Interventions MISHybrid
TAVR

TAVR
Procedural Steps• Planning CT and echo: Imaging for aorta,
aortic valve, lower extremities• Vascular access
– Percutaneous– Femoral, iliac, apical, axillary, aortic
• Pass large bore sheath– Currently approved device is only slightly smaller
in caliber than a garden hose
• Cross the aortic valve• Balloon valvuloplasty/valve replacement
– Under echo and fluoro guidance
• Vascular repair
Specialty• Rads/Cards/CVS
• IC/VS• CVS• CVS/IC
• IC• IC
• CVS

ACCESS FOR TAVR

DEFINITION
• Team - Comprises a group of people linked in a common purpose


TEAM
• Have members with complementary skills and generate synergy.
• Especially appropriate for conducting tasks that are high in complexity and have many interdependent subtasks.
• Allow each member to maximize their strengths and minimize their weaknesses
• Improve on what is possible for an individual actor

IN HEALTHCARE, “TEAM” MEMBERS OFTEN HAVE NEARLY IDENTICAL SKILLS


Eliminations of these barriers improves patient outcomes and offers a non-zero opportunity for providers

REASONS FOR DIVISIONS• Cultural
– Education/skill sets/knowledge base– How physicians are identified– Mentors/Colleagues/Interests
• Resources– Tools– Physically location
• Office space• Point of service (Clinic vs OR vs Cath Lab)
• Competition• Resentment
– “You only refer me your disasters . . . and your complications . . . and at night/weekends”

ZERO SUM GAME
• Participant's gain (or loss) of utility is exactly balanced by the losses (or gains) of the utility of the other participant(s).
• For one to gain, another must loss
• Example: if one person eats a piece of a cake there is less cake for the other partiers

STENT WARS
• Coronary Revascularization – different competing therapies offered by different specialties– PCI/IC vs CABG/CTS
• Peripheral Revascularization – a different therapy from one field, multiple specialties offering an alternative competing therapy– Vascular vs IR vs IC
• Dominate interaction between 4 fields: CTS, IC, IR, and Vasc– Not collegial but adversarial/competative


NON-ZERO SUM
“The more complex societies get . . . the more complex the networks of interdependence. . . the more people are forced in their own interests to find. . . [non-zero] win-win solutions instead of win-lose solutions. . .
We find as our interdependence increases . . . we do better when other people do better as well”
—an ex-US President, December 2000

GAME THEORY
• Zero-sum– participant's gain (or loss) of
utility is exactly balanced by the losses (or gains) of the utility of the other participant(s).
– If one gains, another losses; only Win-Lose
– Example: cuts and eats a piece of cake there is less cake for the other partiers
• Non-zero-sum– a participant's gain (or
loss) of utility is not balanced by the losses (or gains) of the utility of the other participant(s).
– Win-Win (and Lose-Lose) scenarios exist
– Example: Prisoners’ dilemma

PRISONERS DILEMMA
• The gains of one player are not equally offset by the losses of the other.
• If non-cooperation, they get total 40 years
• If both cooperate, total 2 years in prison

REVELATION
• 75 cardiac surgery programs and 79 cath labs in a 25 mile radius
• What if we work together and . . . try to take cases from guys across the street . . . rather than cases from the guys across the hall?

OUR EXPERIMENT
• Create a team composed of members with different skills sets/from different disciplines• Cardiology• Vascular surgery• Radiology
• Looked for opportunities to collaborate to expand our services
• Leverage unique skills and existing systems• Focus on patient centric care
• Interventional Cardiology• Cardiac Surgery

KEYS TO SUCCESS

TRANSPARENCY/SHARE THE WORK
• Coronary revascularization cases discussed with both IC and CTS
• Valve cases discussed valve conf and valve clinic
• Aortic cases discussed aortic conf and valve clinic

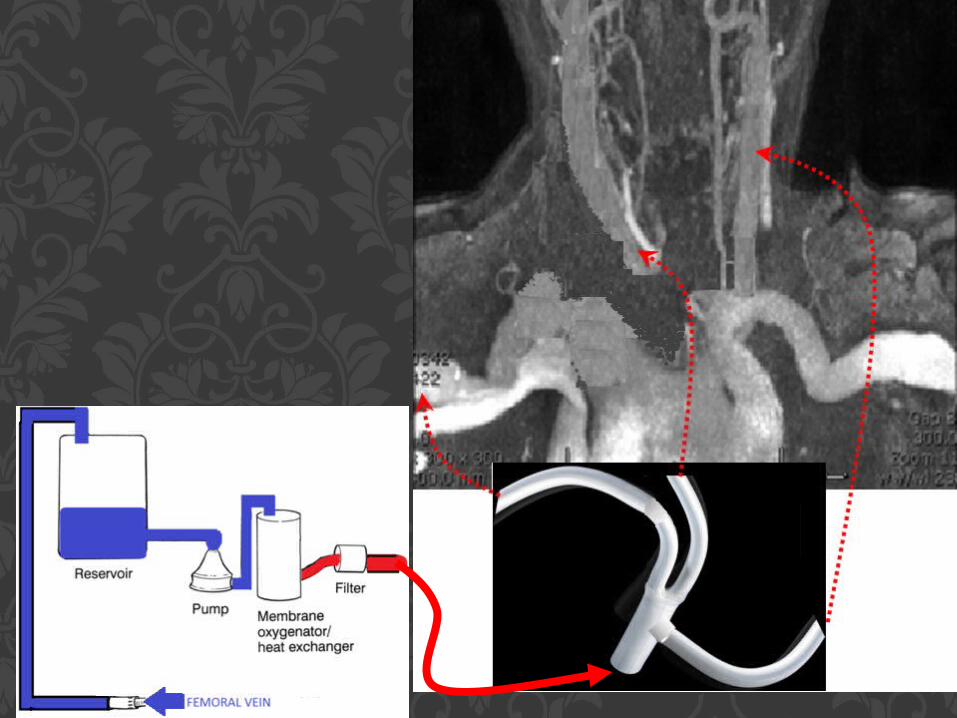
LEVERAGE ESTABLISHED SYSTEMS
• Example: ECMO– Emergency surgery only exists in Level 1 Trauma
Centers and on TV– It takes 1-3 hours to open an OR– Cath lab can be activated in 30 mins or less– >80% of ECMO is initiated in the cath lab– Faster (and cheaper)– Also allows an opportunity to collaborate

COMMITMENT TO PURPOSE
• 73yo Jehovah's Witness is transferred from OSH after being loaded with plavix with a diagnosis of Type A dissection– Accepted by cardiology (AS)– Repeat CT (KD) performed read by contained rupture Asc
Ao– Reviewed by Vasc (RM) and CTS (MR)– Underwent replacement of AscAo/Hemiarch (MR) POD #4– Discharged to rehab on POD #10– Pt will return as outpatient for PCI

AO DEBRACHING/REOP ARCH
Darwin Eton, MDProfessor of Surgery

A B

D


STENT LAD
POSITIVE STRESS TEST



LCCARCCA
Cervical Debranching


LCCA
RCCA
RAx
LScA

25 C

RCCA
RAx
LCCA
LScA


Vascutek Gelweave 4 Plexus

RCCA
RAx
LCCA
LScA
Aorta

Edwards Magna Bioprosthetic Aortic Valve

PROXIMAL DACRON ARCH GRAFT
ANASTOMOSIS

Stepwise Disconnection of Extracranial Circuit on CPB from
1. LCCA, and repair artery
2. RCCA, and attach RCCA to Dacron Limb
3. RAx, and attach RAx to Dacron Limb
FINAL STEPS

RCCARAxLCCA

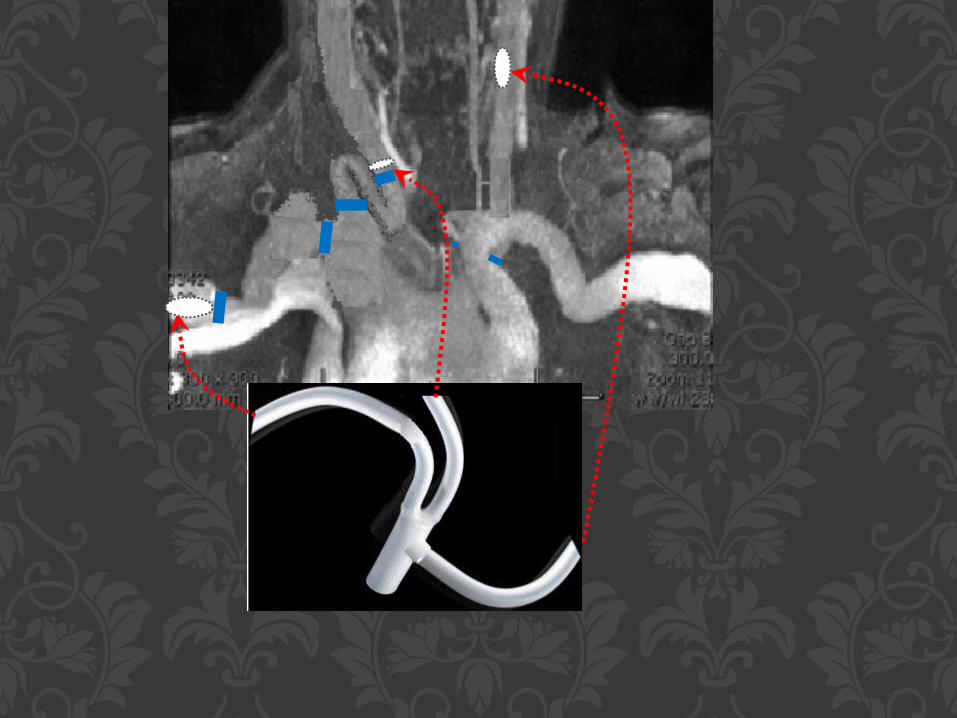
Ascending Aortic Pseudoaneurysm
Ross Milner, MD
Associate Professor of Surgery
Co-Director, Center for Aortic Diseases

History
• 57-year old man
• Type A Dissection Repair in 2007
• Presented recently with chest pain
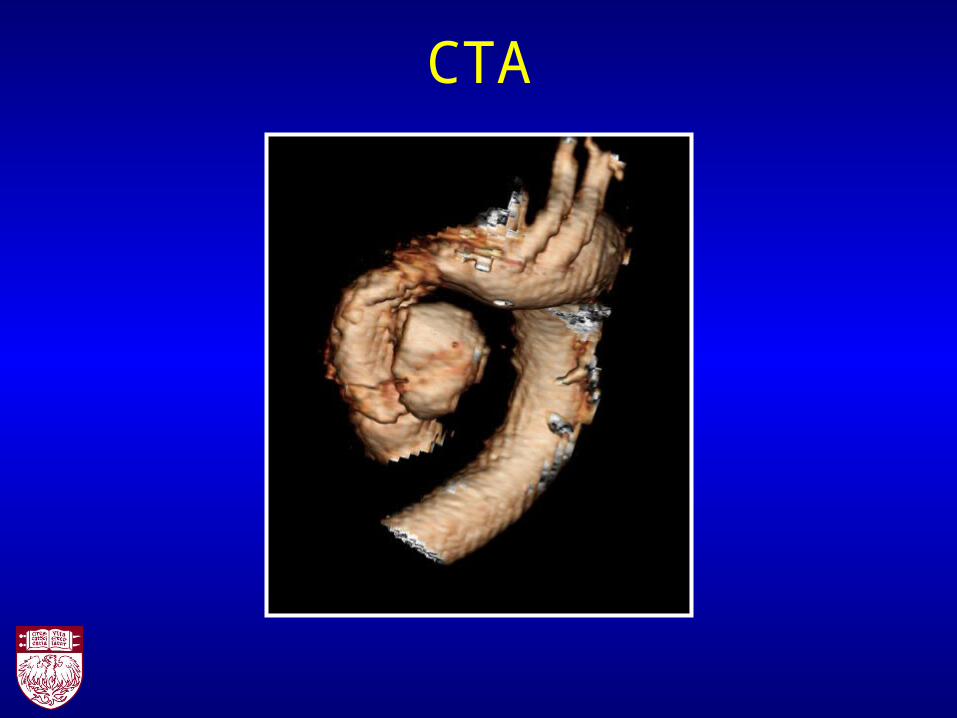
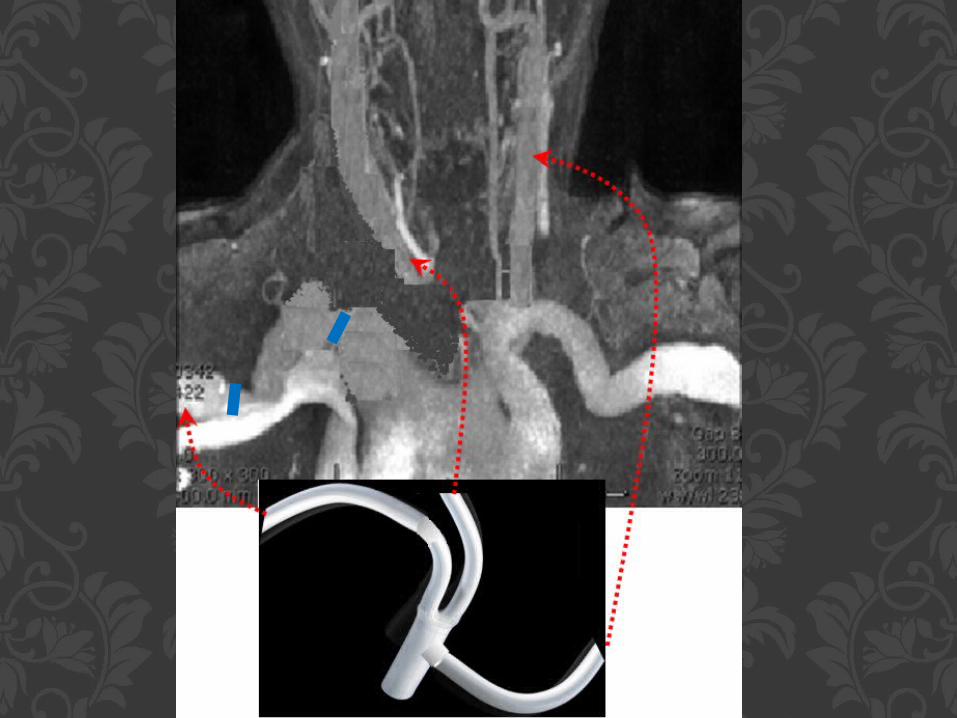
CTA

Plan
• Aortogram• Cardiac cath

Plan
• Aortogram• Cardiac cath
• Multivessel CAD discovered: Potentially treatable with PCI

Cardiac catheterization
Aortic root injection Selective cannulation of pseudoaneurysm using
coronary catheter

Cardiac catheterization95% diagonal lesion
Nonobstructive LAD disease 70% circumflex/ obtuse
marginal lesion
Moderate – severe diffuse RCA disease
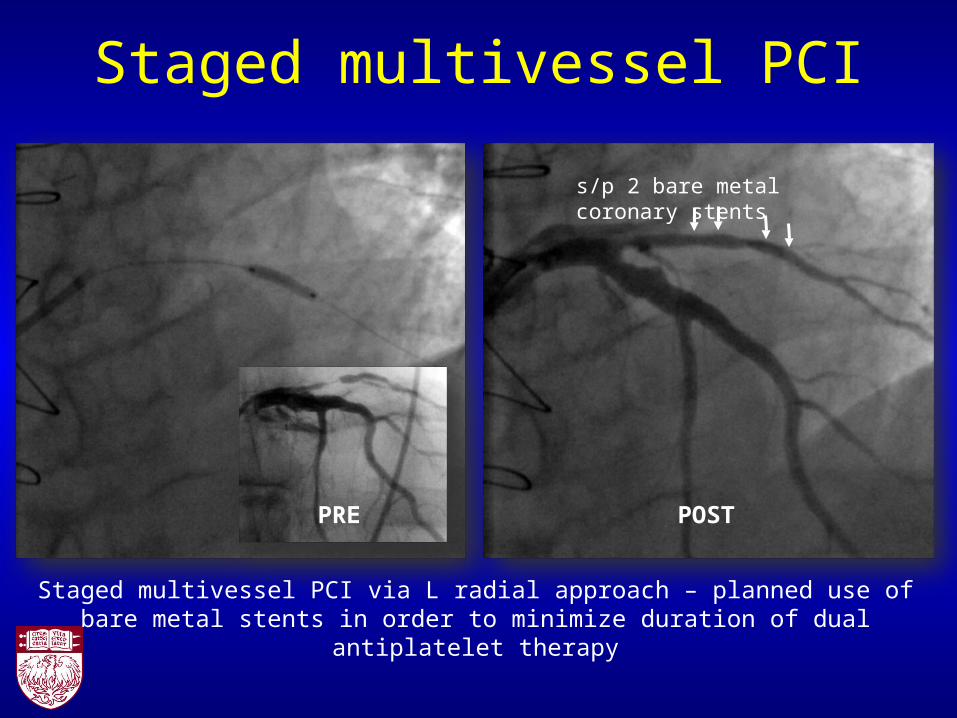
Staged multivessel PCI
Staged multivessel PCI via L radial approach – planned use of bare metal stents in order to minimize duration of dual antiplatelet therapy
PRE POST
s/p 2 bare metal coronary stents

Staged multivessel PCI
PRE POST
s/p 1 bare metal biliary stent

Treatment
• PCI completed on bivalirudin anticoagulation and clopidogrel (Plavix) (Dr. Sandeep Nathan)
• Wait 2 weeks and hold clopidogrel
• OR for repair

OR
• Bilateral axillary cutdown
• Percutaneous left femoral vein
• CPB
• TEE
• 3 specialties operating together

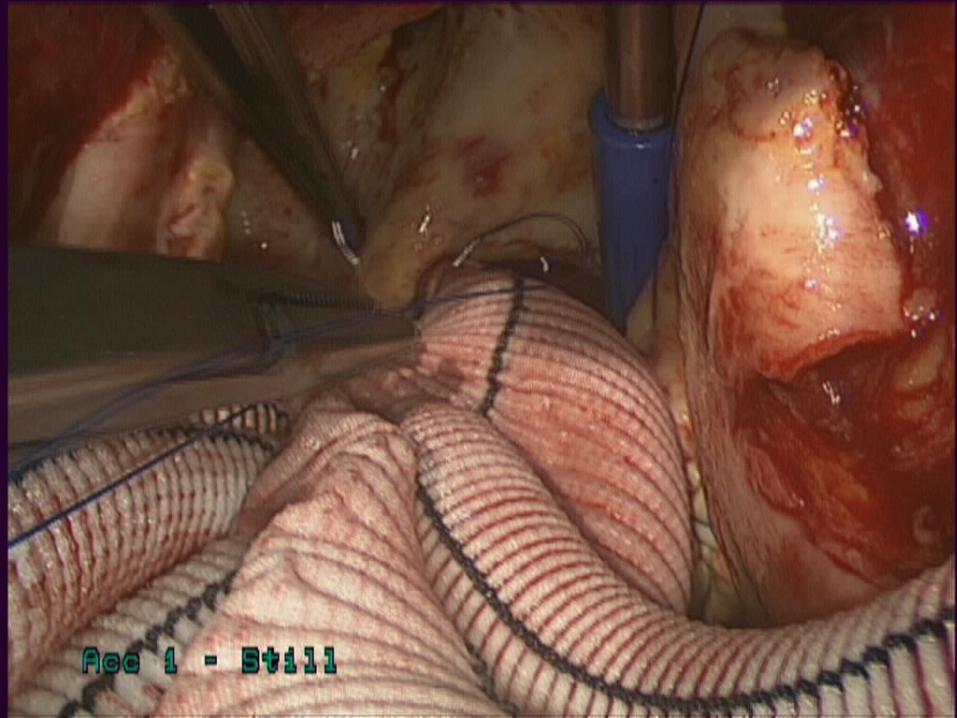
Axillary Cutdown

Stent Placement

Stent Placement (cont)
Selective cannulation of left main coronary to protect during aortic stent grafting

Stent Placement (cont)

Stent Placement (cont)

Team

Post-op TEE

Post-op TEE

Transcatheter Aortic valve Closure
Atman ShahCo-Director, Transcatheter Valve
Therapies

Introduction• Left ventricular assist
devices (LVADs) are increasingly being used in the treatment of end-stage heart failure
• Bridge-to-Destination or Bridge-to-Transplant
• Forecasts suggest 100,000 implants annually in the US
Cowger J, et al. Circ Heart Fail 2010;3:668–74

Aortic Insufficiency• AI can occur in 51% of LVAD patients
at 18 months• Associated with increased mortality• The newly implanted LVAD may result
in functional closure of the AV• Exact mechanism of AI in uncertain,
but aortic root dilation and myxoid degeneration may be factors
Cowger J, et al. Circ Heart Fail 2010;3:668–74Toda K, et al. Ann Thorac Surg 2011;92:929–3.
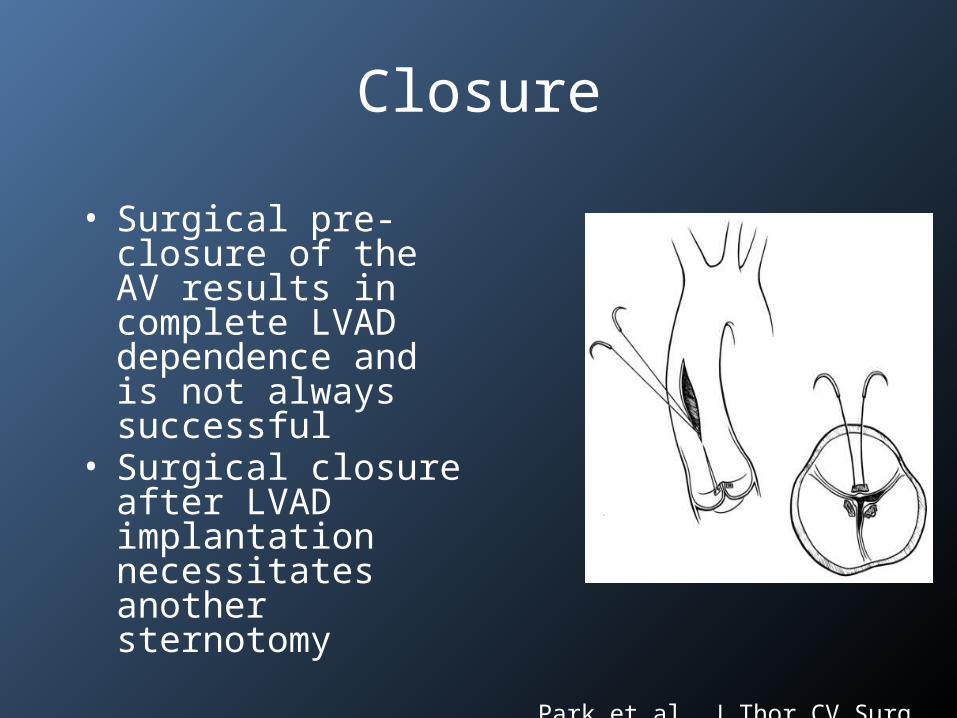
Closure
• Surgical pre-closure of the AV results in complete LVAD dependence and is not always successful
• Surgical closure after LVAD implantation necessitates another sternotomy
Park et al. J Thor CV Surg 2004;127:264-8.

Severe AI
Transcatheter Closure
• Grohmann et al reported a case of AV closure via a surgical cutdown and use of an Amplatzer VSD device
• Riede et al reported transcatheter treatment of AI in a neonate with hypoplastic left heart syndrome
Riede FT, et al. Cath Cardiol Int 2009;74:913–5.Grohmann J, et al. Eur J Cardiothorac Surg 2011;39:e181–3.

Approach
• After the AV was crossed, a 9Fr TorqVue catheter (AGA Medical/SJM) was advanced into the LV
• A 30mm Amplatzer Cribiform Septal Occluder was loaded and deployed across the AV
• Coronary angiography demonstarted patent coronaries

Cath Imaging

2D and 3D Imaging
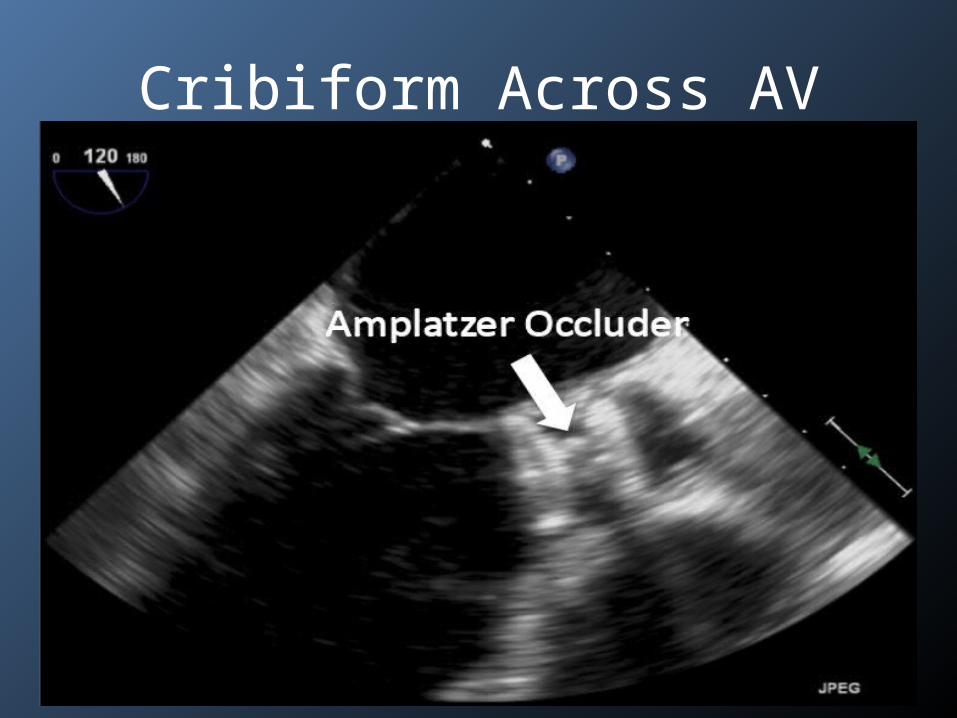
Cribiform Across AV

Resolution of AI

Clinical Improvement

SUCCESS?
• Better working environment• Learn new skill sets• Broader understanding of disease process and
available therapies• Easier acquisition of others input even when
unplanned– Complications
• Shift to patient centric delivery of care• Expand practice

EXPAND PRACTICE
• ECMO• Hybrid Coronary Revascularization• Hybrid Peripheral Revascularization• Hybrid Aortic Surgery/Arch Debranching• EVAR/TEVAR• TAVR

OBSTACLES
• Resources – local issue• Reimbursement – payor issue• Playing field – being addressed
• For Providers: Win-Win• For Patients: Win• Win-Win-Win
Recommended









![Homocysteine-lowering interventions for preventing … · 2018. 12. 15. · [Intervention Review] Homocysteine-lowering interventions for preventing cardiovascular events Arturo J](https://img.dokumen.tips/doc/110x75/5ff89452656730039f05d58a/homocysteine-lowering-interventions-for-preventing-2018-12-15-intervention.jpg)







