Clinical CorrelationsClinical Correlations The NYU Internal Medicine Blog The NYU Internal Medicine Blog
A Daily Dose of MedicineA Daily Dose of Medicine
http://clinicalcorrelations.org

Medical Grand RoundsMedical Grand RoundsClinical VignetteClinical Vignette
December 17December 17thth, 2008, 2008
Anjali Grover, M.D.Anjali Grover, M.D.

Chief ComplaintChief Complaint
A 45 year old Hispanic male presents with A 45 year old Hispanic male presents with chest pain for 45 minutes.chest pain for 45 minutes.

History of Present IllnessHistory of Present Illness
• The patient was well until the evening of The patient was well until the evening of admission when he had the sudden onset admission when he had the sudden onset of non-radiating, sub-sternal chest of non-radiating, sub-sternal chest pressure while walking. pressure while walking.
• The chest pain was associated with The chest pain was associated with shortness of breath, light-headedness, shortness of breath, light-headedness, palpitations, diaphoresis and nausea palpitations, diaphoresis and nausea without vomiting. without vomiting.

Additional HistoryAdditional History
Past Medical History: Past Medical History: – HyperlipidemiaHyperlipidemia– DepressionDepressionPast Surgical History:Past Surgical History: none noneSocial history:Social history:
– Current smoker with a 25 pack year historyCurrent smoker with a 25 pack year history– Denies ethanol or illicit drug useDenies ethanol or illicit drug use
Family History:Family History: – Mother died of a myocardial infarction at age 76Mother died of a myocardial infarction at age 76
Allergies: Allergies: – No known drug allergiesNo known drug allergies
Medications:Medications:-- Simvastatin 40 mg daily-- Simvastatin 40 mg daily-- Aspirin 81 mg daily-- Aspirin 81 mg daily-- Fluoxetine 20 mg daily-- Fluoxetine 20 mg daily

Physical ExamPhysical ExamGeneral:General: In mild distress appearing anxious In mild distress appearing anxious
secondary to chest pain, appeared his stated age.secondary to chest pain, appeared his stated age.
T:97.1T:97.1ooF BP:159/82 HR:84 RR:16 F BP:159/82 HR:84 RR:16 OO2:97%RA:97%RA
The remainder of the physical exam was normalThe remainder of the physical exam was normal

LaboratoryLaboratory
Basic Metabolic Panel normalBasic Metabolic Panel normalComplete Blood Count normalComplete Blood Count normalHepatic Function Panel normalHepatic Function Panel normal
Time 0 hours Time 8 hours
Troponin 0.09 (normal <0.07) 0.01

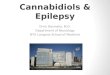
ImagingImagingECG: ECG: Sinus rhythm with rate of 63, 2 mm ST elevation Sinus rhythm with rate of 63, 2 mm ST elevation in V2, 1 mm up-slanting ST depression in II, III, aVf.in V2, 1 mm up-slanting ST depression in II, III, aVf.
Chest X-RayChest X-Ray: : No evidence of pulmonary congestion, No evidence of pulmonary congestion, infiltrate or effusions.infiltrate or effusions.

Working DiagnosesWorking Diagnoses
Acute Coronary Syndome: ST Elevation Acute Coronary Syndome: ST Elevation Myocardial Infarction (STEMI)Myocardial Infarction (STEMI)
Brugada SyndromeBrugada Syndrome

Hospital CourseHospital CourseEmergency Room course: Emergency Room course:
– Treated with: Treated with: Aspirin 325mgAspirin 325mg
Clopidogrel 300mgClopidogrel 300mg
Lopressor 5 mg IVP x 3Lopressor 5 mg IVP x 3
Morphine 4mg IVPMorphine 4mg IVP
Sub-lingual Nitroglycerine 0.4mg x 3Sub-lingual Nitroglycerine 0.4mg x 3
Heparin drip Heparin drip
Lipitor 80 mgLipitor 80 mg
The patient remained hemodynamically The patient remained hemodynamically stable, EKG changes were stable and his stable, EKG changes were stable and his chest pain resolved. chest pain resolved.

Hospital CourseHospital CourseHospital Day #1: Cardiac Catheterization revealed clean coronary
arteries Transthoracic Echocardiogram showed no
abnormalities
Hospital Day #2: Procainamide challenge performed to evaluate for
possible manifestations of Brugada Syndrome on EKG.
With procainamide, the patient’s 2mm “saddle-back” ST segment elevation in V2 converted to a “coved” ST segment elevation pattern.
These findings represented a positive procainamide challenge.

Hospital CourseHospital CourseHospital Day #3:Hospital Day #3: Electrophysiology Study performed for further risk stratification Electrophysiology Study performed for further risk stratification
revealed no inducible ventricular arrhythmias. revealed no inducible ventricular arrhythmias.
Intracardiac defibrillator placement was recommended to Intracardiac defibrillator placement was recommended to the patient, but he refused.the patient, but he refused.
He was discharged on Aspirin and Zocor.He was discharged on Aspirin and Zocor.
6 months later on follow-up in Cardiology Clinic, the 6 months later on follow-up in Cardiology Clinic, the patient agreed to ICD placement. It was placed shortly patient agreed to ICD placement. It was placed shortly thereafter.thereafter.

Final DiagnosisFinal Diagnosis
Type 2 Brugada SyndromeType 2 Brugada Syndrome
Recommended