Cardioversion of Atrial Tachycardia and Flutter by Atrial Stimulation
STEPHEN J. GULOTTA, MD, FACC ALFRED L. ARONSON, MD
Manhasset, New York
Electrical stimulation of the right atrium using a bipolar electrode cath- eter terminated 9 episodes of atrial flutter in 8 patients and 32 episodes of atrial tachycardia in 1 patient. Six episodes of flutter were converted directly to sinus rhythm, and 3 were converted initially to atrial fibrillation with a slower ventricular rate and then to sinus rhythm. Conversion of atrial flutter to sinus rhythm by pacing rates slower than the atrial rates implies that interruption of a reentry circuit was responsible for termination of the arrhythmia.
Two separate mechanisms were found to terminate atrial tachycardia: (1) overdrive suppression, and (2) interruption of a reentry circuit by delivery of a single appropriately timed stimulus. Attempts to convert atrial fibrillation to sinus rhythm by right atrial stimulation were unsuc- cessful.
This technique is a safe and effective method for terminating atrial tachycardia and flutter, especially in patients receiving large doses of digitalis. It may be performed repetitively at the bedside without anes- thesia and without discomfort to the patient.
Atria1 tachycardia and atria1 flutter frequently complicate or produce acute cardiac failure and unless converted or controlled can produce severe hemodynamic alterations in the presence of valvular or myo- cardial disease. Although cardioversion using transthoracic direct current countershock has been highly successful in terminating su- praventricular tachycardias, its use in patients receiving digitalis is not without danger.1-3 The development of newer, safer techniques for the treatment of rapid atria1 arrhythmias in the acutely ill, digitalized patient has significant clinical value.
In 1967, Massumi et al.” and Durrer et al.” reported the termination of supraventricular tachycardias in patients with Wolff-Parkinson- White syndrome by delivering a single electrical stimulus to the right atrium. Subsequently, Lister et al.” terminated supraventricular tachycardias in 10 patients by applying rapid repetitive electrical stimuli to the right atrium, and Zeft et al.’ reported the conversion of atria1 flutter to sinus rhythm in 8 of 10 patients by this same technique.
From the Division of Medicine (Cardiology), North Shore Hospital, Manhasset, N.Y., and the Department of Medicine, Cornell University Medical College, New York, N.Y. Manuscript received October 29, 1969, accepted January 9, 1970.
Address for reprints: Stephen J. Gulotta, MD, FACC, North Shore Hospital, Manhasset, N.Y. 11030.
Utilizing electrical stimulation of the right atrium, 9 episodes of atria1 flutter were converted to normal sinus rhythm in 8 pa- tients, and 32 episodes of atria1 tachycardia were converted to sinus rhythm in 1 patient. All patients had received large doses of digi- talis. In addition, the effects of electrical stimulation of the right atrium on long standing atria1 fibrillation were evaluated in 2 patients.
This renort demonstrates the safetv and efhcacv of atria1 stim- I ulation in digitalized patients and discusses anisms by which this technique terminates and flutter.
the possible mech- atria1 tachycardia
262 The American Journal of CARDIOLOGY

CARDIOVERSION OF ATRIAL TACHYCARDIA AND FLUTTER
Methods Under fluoroscopic control, bipolar electrode catheters
were inserted percutaneously through the femoral vein and were positioned in the right atrium so that 1 or both electrodes would lie against the endocardium, with the tip of the catheter directed away from the tricuspid valve. Electrical stimulation was carried out by a battery-driven (Medtronics, model 60’7) or isolated alternating current powered (American Optical, model 109’70R) pulse genera- tor. Impulses of 2 msec duration were delivered singly or repetitively at frequencies varying from 115 to 3751min. Current levels were varied from 5 to 20 ma. Stimulation rates and current amplitudes were altered independently in order to study numerous rate-current ratios.
In the 2 patients with atria1 fibrillation, stimulation rates were varied from 150 to 1200/min (Medtronics, model 1187), and the duration of impulses ranged from 0.2 to 10 msec. The bipolar electrodes were alternately spaced 1 em and 10 cm apart, and both electrodes were placed in contact with the endocardium.
Continuous monitoring of the electrocardiogram was performed during insertion of the catheter electrodes and during right atria1 stimulation. The electrocardiogram was recorded using either a standard instrument, an Elec-
TABLE I Results of Atrial Stimulation in 11 Patients
tronics for Medicine recorder or a $-channel ink jet recorder (Mingograf 34, Elema Schonander Co.). Patients and equipment were grounded so that the introduction of any undesirable current flow was prevented.
Results
The pertinent clinical data and the results of &trial stimulation in the 11 patients studied are presented in Table I.
In 5 of 8 patients with stable atria1 flutter, conver- sion directly to normal sinus rhythm occurred within 3 minutes after the initiation of atria1 stimuIation. In the remaining 3 patients conversion occurred ini- tially to atria1 fibrillation and then (within 2 hours) to normal sinus rhythm. In these 3 cases the ven- tricular rate slowed considerably with the onset of atria1 fibrillation, thus permitting a prompt im- provement in hemodynamic status.
Patient 1 responded the most rapidly, with conver- sion to normal sinus rhythm after 6 seconds of elec- trical pacing (Fig. 1). The fourth impulse terminated the flutter, and the fifth, seventh, eighth, tenth and
no. -
1
2
3
4
5
6
7
8
9
10
11
Age & sex Diigncds
Rhythm, Duration Drug Therapy
Results of Stimulrtfon
44M Congenital heart disease;
massive tricuspid re-
gurgitation 54M Rheumatic heart disease;
mitral stenosis; pul- monary edema
70M lschemic heart disease;
complete heart block (permanent pacemaker);
pacer failure
58M lschemic heart disease;
angina1 syndrome 52M lschemic heart disease;
acute cardiac failure
62F lschemic heart disease;
acute myocardial in-
farction 54M lschemic heart disease;
angina1 syndrome
73M lschemic heart disease;
acute myocardial in-
farction 42F No known organic
heart disease
50F Rheumatic heart disease; Atrial fibrilla- mitral stenosis tion, 4 years
44M Rheumatic heart disease; Atrial fibrilla- mitral insufficiency tion, 3 years
Atrial flutter, Digoxin (2 mg i.v.), Normal sinus 12 hours quinidine rhythm
Atrial flutter, Digoxin (2.75 mg i.v.), Normal sinus 36 hours quinidine rhythm
Atrial flutter,
2% years
Atrial flutter,
2 hours
Atrial flutter,
12 hours
Atrial flutter,
18 hours
Atrial flutter,
24 hours
Atrial flutter,
14 hours
Paroxysmal atrial tachy- cardia, 4 days
Digoxin (0.5 mg/day) Normal sinus
rhythm
Digoxin (0.5 mg/day)
Digoxin (1.5 mg Lv.),
quinidine,
lidocaine
Digoxin (2 mg i.v.),
lidocaine
Digoxin (1.5 mg i.v.)
Digoxin (2 mg i.v.)
Digoxin (3 mg i.v., and p.o.), quinidine, lidocaine, propranolol
Digoxin (0.5 mg/day)
Digoxin (0.5 mg/day)
Normal sinus
rhythm
Normal sinus
rhythm
Atrial fibrilla-
tion to normal
sinus rhythm Atrial fibrilla-
tion to normal sinus rhythm
Atrial fibrilla-
tion to normal
sinus rhythm
Temporary normal sinus rhythm
Ventricular rate slowed for 10 min
No change
i.v. = intravenously: p.0. = orally.
VOLUME 26, SEPTEMBER 1970 263

GULOTTA AND ARONSON
ATRIA1 FLUTTER ATRIA1 STIMULATION IlS/min
AK. MM. ATRIAL FLUTTER
ATRIAL STIYULATIOW 37Wmin
Figure 1. Patient 1. Continuous electrocar- diographic recording demonstrating atrial flutter with various degrees of block. The fourth electrical impulse (black arrows) ter- minates the flutter. Impulses 5, 7, 8, 10 and 11 capture the atrium. When pacing is stopped, sinus rhythm follows.
Figure 2. Patient 2. Continuous recording of intraatrial unipolar electrogram at paper speed of 50 mm/set demonstrating atrial flutter. Short (2.3 seconds) burst of atrial stimulation (middle panel) results in prompt conversion to stable sinus rhythm. Initiation and termination of atrial stimulation are indicated by black arrows. A = atrial com- plex; AUP = atrial unipolar electrogram; NSR = normal sinus rhythm; V = ven- tricular complex.
Figure 3. Patient 3. Continuous electrocar- diographic recording showing atrial flutter, complete heart block and pacer rhythm. Atrial stimulation was begun (top panel) and the rate of stimulation was varied in a ran- dom fashion resulting in conversion to nor- mal sinus rhythm (NSR). The heart block remained unchanged.
264 The American Journal of CARDIOLOGY
CARDIOVERSION OF ATRIAL TACHYCARDIA AND FLUTTER
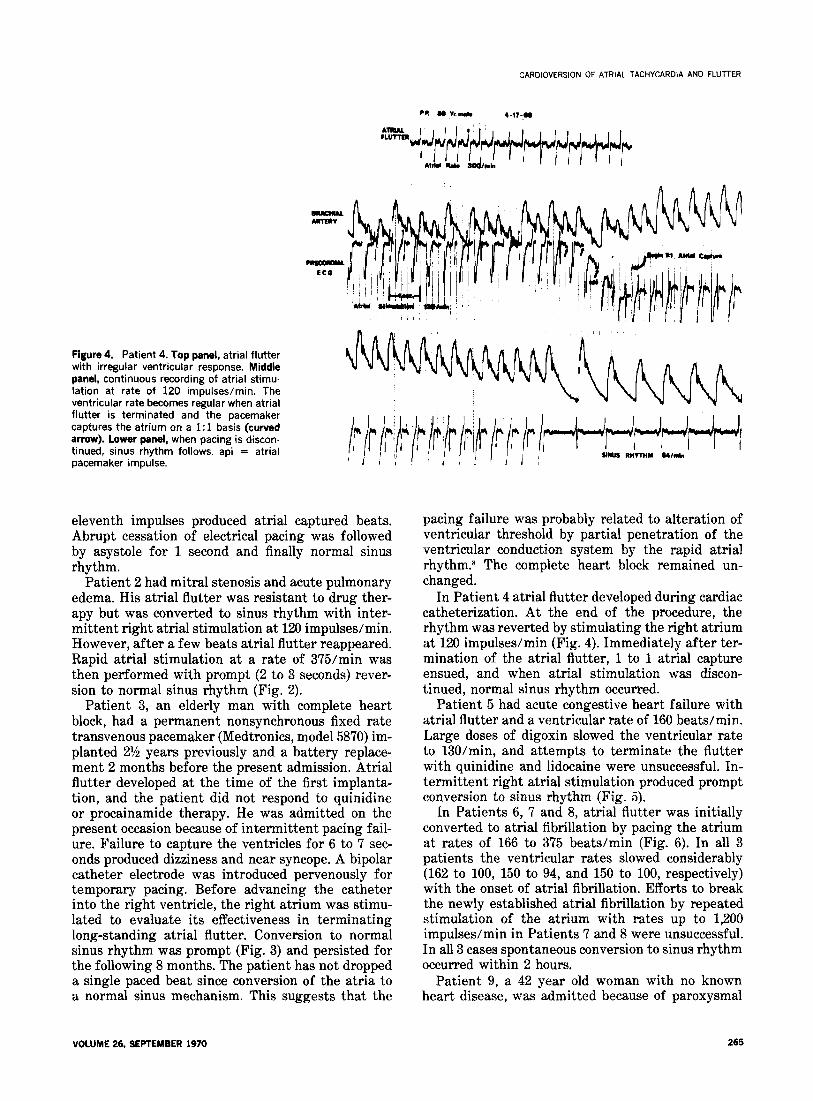
Figure 4. Patient 4. Top panel, atrial flutter with irregular ventricular response. Middle panel, continuous recording of atrial stimu- lation at rate of 120 impulses/min. The ventricular rate becomes regular when atrial flutter is terminated and the pacemaker captures the atrium on a 1: 1 basis (curved arrow). Lower panel, when pacing is discon tinued, sinus rhythm follows. api = atrial pacemaker impulse.
eleventh impulses produced atria1 captured beats. Abrupt cessation of electrical pacing was followed by asystole for 1 second and finally normal sinus rhythm.
Patient 2 had mitral stenosis and acute pulmonary edema. His atria1 flutter was resistant to drug ther- apy but was converted to sinus rhythm with inter- mittent right atria1 stimulation at 120 impulses/min. However, after a few beats atria1 flutter reappeared. Rapid atria1 stimulation at a rate of 375/min was then performed with prompt (2 to 3 seconds) rever- sion to normal sinus rhythm (Fig. 2).
Patient 3, an elderly man with complete heart block, had a permanent nonsynchronous fixed rate transvenous pacemaker (Medtronics, model 5870) im- planted 2% years previously and a battery replace- ment 2 months before the present admission. Atria1 flutter developed at the time of the first implanta- tion, and the patient did not respond to quinidine or procainamide therapy. He was admitted on the present occasion because of intermittent pacing fail- ure. Failure to capture the ventricles for 6 to 7 sec- onds produced dizziness and near syncope. A bipolar catheter electrode was introduced per-venously for temporary pacing. Before advancing the catheter into the right ventricle, the right atrium was stimu- lated to evaluate its effectiveness in terminating long-standing atria1 flutter. Conversion to normal sinus rhythm was prompt (Fig. 3) and persisted for the following 8 months. The patient has not dropped a single paced beat since conversion of the atria to a normal sinus mechanism. This suggests that the
VOLUME 26. SEPTEMBER 1970 265
pacing failure was probably related to alteration of ventricular threshold by partial penetration of the ventricular conduction system by the rapid atria1 rhythm.* The complete heart block remained un- changed.
In Patient 4 atria1 flutter developed during cardiac catheterization. At the end of the procedure, the rhythm was reverted by stimulating the right atrium at 120 impulses/min (Fig. 4). Immediately after ter- mination of the atria1 flutter, 1 to 1 atria1 capture ensued, and when atria1 stimulation was discon- tinued, normal sinus rhythm occurred.
Patient 5 had acute congestive heart failure with atria1 flutter and a ventricular rate of 160 beats/min. Large doses of digoxin slowed the ventricular rate to 130/min, and attempts to terminate the flutter with quinidine and lidocaine were unsuccessful. In- termittent right atria1 stimulation produced prompt conversion to sinus rhythm (Fig. 5).
In Patients 6, ‘7 and 8, atria1 flutter was initially converted to atria1 fibrillation by pacing the atrium at rates of 166 to 375 beats/min (Fig. 6). In all 3 patients the ventricular rates slowed considerably (162 to 100, 150 to 94, and 150 to 100, respectively) with the onset of atria1 fibrillation. Efforts to break the newly established atria1 fibrillation by repeated stimulation of the atrium with rates up to 1,200 impulses/min in Patients 7 and 8 were unsuccessful. In all 3 cases spontaneous conversion to sinus rhythm occurred within 2 hours.
Patient 9, a 42 year old woman with no known heart disease, was admitted because of paroxysmal

GULOTTA AND ARONSON
atria1 tachycardia (140 to 180 beats/min). The P wave configuration (Fig. 7) suggested a coronary sinus or left atria1 mechanism. Since the tachycardia did not respond to digitalis, quinidine, lidocaine or proprano- 101 therapy, attempts were made to terminate the rhythm by atria1 pacing. Unipolar atria1 electrograms (Fig. 8) were obtained before stimulation. The QS pattern of the P wave recorded near the entrance of the inferior vena cava indicated that this area was the locus of the abnormal pacemaker. On 32 occasions the tachycardia was easily broken with right atria1 stimulation but recurred after short in- tervals. Two independent mechanisms appeared to terminate this patient’s tachycardia: (1) overdrive suppression (Fig. 9), and (2) interruption of a reentry circuit (Fig. 10). Since hospitalization the patient has been maintained successfully on digitalis and pro- pranolol therapy.
In 2 patients (Cases 10 and 11) with long standing atria1 fibrillation attempts to restore sinus rhythm were unsuccessful. The stimulating electrodes were placed 10 cm apart and positioned so that both elec- trodes contacted the atria1 endocardium. Stimulation of at least 3 different pairs of sites in the atrium, using current amplitudes of 5 to 20 ma and stimula- tion rates up to 1,200 impulses/min, was performed. The impulse duration was varied from 0.2 to 10 msec. Atria1 fibrillation persisted in both cases; however, in Patient 10 the fibrillatory waves became smaller and finer, and the ventricular rate slowed transiently from 80 to 68 beats/min.
Figure 5. Patient 5. Panel A, atrial flutter with irregular ventricular response. Panels B, C and D, continuous electrocardiographic recording at paper speed of 25 mm/set dur- ing right atrial stimulation. Both rate and amplitude were varied randomly. Panel E, the third complex is a sinus beat, and the fourth is a premature atrial beat. The fifth is sinus and is followed by a nonconducted premature atrial beat that is followed by 3 junctional beats and, finally, stable sinus rhythm.
Mechanisms responsible for terminating atria1 flutter: The electrophysiologic mechanism respon- sible for producing atria1 flutter has not been defined precisely. Most clinical and experimental data sup- port the circus movement theory.g Similarly, some supraventricular tachycardias represent reentry rhythms that are produced by circus movements in the atrioventricular conduction system.l”
Our results lend support to the circus movement theory of atria1 flutter. In 5 patients with flutter conversion directly to sinus rhythm occurred after brief periods of right atria1 stimulation at rates that were slower than the intrinsic atria1 rate. In Patient 1, the fourth electrical impulse terminated the flut- ter. The suppression of a rapidly firing pacemaker is not likely to be accomplished by a single impulse or by a stimulation rate slower than the atria1 pace- maker. Therefore, our observations support the hy- pothesis that the mechanism responsible for the suc- cess of this technique is the interruption of a reentry circuit.
A second mechanism responsible for terminating atria1 flutter was seen in the 3 patients in whom temporary atria1 fibrillation developed after atria1 stimulation. Initiation of atria1 fibrillation after stimulation at a rate of 166/min (Patient 6) supports the proposal of Haft and associates I1 that when pac- ing impulses fall during the atria1 vulnerable period, unstable atria1 fibrillation is produced which sub-
266 The American Journal of CARDIOLOGY

CARDIOVERSION OF ATRIAL TACHYCARDIA AND FLUTTER
Figure 6. Patient 6. Panel A, atrial flutter with a ventricular rate of 162 beats/min. Atrial stimulation is begun at 166/min. Panel C, cessation of electrical stimulation is fol- lowed by atrial fibrillation with a slower ven- tricular response.
.--
NRIIL FIBRILLArloW I”,*”
Figure 7. Patient 9. Standard 12 lead elec- trocardiogram showing low atrial rhythm. Spontaneous increase in heart rate to 150-160 beats/min is seen in precordial leads.
Figure 8. Patient 9. Simultaneous electro- cardiographic leads II and Ill and atrial uni- ’ polar electrogram (AUP) taken at different levels in the right atrium (RA). Panel on the right was recorded with atrial electrode close to the entrance of inferior vena cava. The completely negative P wave recorded intra- atrially at this level suggests that this is the site of the abnormal pacemaker.
VOLUME 26. SEPTEMBER 1970 267

GULOTTA AND ARONSON
r I I
Figure 9. Patient 9, a 4.2 year old woman. Atrial tachycardia terminated by overdrive suppression. Upper and lower panels are recordings of leads I, II, Ill. Note negative P in leads II and Ill. Bottom line marks each electrical impulse. The first burst of atrial stimulation (top panel, arrows) captures the atrium but fails to break the tachycardia. The second (top panel) and third period of atrial stimulation also capture the atrium and, with cessation of atrial pacing, sinus rhythm follows.
I I I ----
Figure 10. Patient 9. Top panel is another example of overdrive suppression. Lower panel demonstrates termination of tachycardia with single impulses. The first and fourth impulses produce noncon- ducted premature atrial beats (curved arrows), each of which is followed by a 0.92 second pause and, finally, a sinus beat. This mechanism was effective only when the electrical impulse was deliv- ered wrthtn 0.20 and 0.22 second of the preceding P wave. API = atrial pacemaker impulses; J = junctional escape beat; P = sinus beats.
sequently reverts spontaneously to a normal sinus mechanism. The slowing of the ventricular rate in Patients 6,7 and 8 after the onset of atria1 fibrillation was related to the increased number of atria1 im- pulses arriving at the atrioventricular junctional tis- sue during fibrillation. Many of the impulses only partially penetrate the junctional tissue but render it, nevertheless, refractory to the atria1 impulses that immediately follow (repetitive concealed conduction). Slowing the ventricular rate by increasing the atria1 rate has been used therapeutically by Lister et al.” in both sinus and junctional tachycardias.
Atria1 tachycardia was terminated by 2 separate mechanisms in Patient 9. On numerous occasions it was possible to capture the atrium by stimulation at rates exceeding those of the tachycardia (Fig. 9). With “overdrive pacing”, the ectopic pacemaker was suppressed or inactivated, and upon cessation of atria1 stimulation, normal sinus rhythm was restored.
This same patient also responded on several oc- casions by a mechanism that very likely involved the interruption of a reentry circuit by a single, stra- tegically placed electrical impulse (Fig. 10). It is unlikely that 1 premature atria1 beat could inactivate a single repetitively firing focus. Our observations demonstrated that the tachycardia was terminated only when a pacing impulse fell 0.20 to 0.22 second after the preceding P wave and produced a noncon- ducted atria1 beat. The finding of a critical period
The American Journal of CARDIOLOGY

during which the impulse must fall is very suggestive that a reentry mechanism was operative in main- taining the tachycardia. It is possible that earlier pacemaker stimuli were discharged into a refractory atrium and that later stimuli failed to enter the circus pathway at a time when propagating impulses could be interrupted.
Safety and hazards of the method: All patients studied were receiving digitalis. Most had received high doses of intravenous digoxin making trans- thoracic direct current cardioversion potentially dan- gerous.‘-” Two patients (Cases 6 and 8) were acutely ill after myocardial infarction and would have been judged poor risks for even light anesthesia, as would the 2 patients (Cases 2 and 5) who had acute cardiac failure.
No complications of the technique have been ob- served, and no postconversion arrhythmias related to digitalis were encountered. The safety and relia- bility of percutaneous femoral vein insertion of a temporary electrode catheter has been demonstrated previously.‘” Use of fluoroscopic monitoring avoided any risk of inadvertent entry of the catheter into the right ventricle, which represents the major po- tential hazard of this technique.
CARDIOVERSION OF ATRIAL TACHYCARDIA AND FLUTTER
Clinical value: As described, the electrode cath- eter was routinely used to evaluate atria1 rhythm disturbances. This is of significant diagnostic value in patients with rapid or complex supraventricular rhythms, especially when aberrant ventricular con- duction is also present. Although unipolar atria1 elec- trograms were presented in this study, the additional value of bipolar atria1 electrograms for the accurate assessment of complex arrhythmias should be stressed.
The ease with which a pacing catheter can be passed into the right atrium, the diagnostic value of obtaining atria1 electrograms from the catheter, the high success rate of converting atria1 flutter and atria1 tachycardia to sinus rhythm (or to atria1 fibril- lation with slowing of the ventricular rate), the pos- sibility of leaving the catheter in place to diagnose and treat repeated paroxysms of supraventricular tachycardia, and the ability to perform atria1 stimu- lation repetitively at the bedside without need for anesthesia, might well make this procedure the treatment of choice for the cardioversion of all su- praventricular tachycardias except atria1 fibrillation. Its safety and applicability in patients receiving high doses of digitalis glycosides has been demonstrated.
1.
2.
3.
4.
5.
6.
References
Lown B, Kleigler R, Williams J: Cardioversion and digitalis drugs: changed threshold to electric shock in digitalized animals. Circ Res 17:519-531, 1965 Rabbino W, Likoff W, Dreifus LS: Complications and limitations of direct current countershock. JAMA 190:417-420, 1964 Kleigler R. Lown B: Cardioversion and digitalis. I. Clinical stud- ies. Circulation 33:878-887, 1966 Massumi RA, Kisten AD, Tawakkol AA: Termination of recipro- eating tachycardia by atrial stimulation,
7. Zeft HJ, Cobb FR, Waxman MV, et al: Right atrial stimulation in the treatment of atrial flutter. Ann Intern Med 70447-456, 1969
Circulation 36:637-643, 1967
beats in the initiation and termination of supraventricular tachycardia in the Wolff-Parkinson-White syndrome. Circulation 36:644-662, 1967
Durrer D, Schoo L, Schuilenberg RM, et al:
Lister JW, Cohen LS, Bernstein WH, et al:
Role of premature
Treatment of supra- ventricular tachycardias by rapid atrial stimulation, Circulation 38:1044-1059, 1968
10.
8. Rytand DA: The circus movement (entrapped circuit wave) hypothesis and atrial flutter. Ann Intern Med 65:125-159, 1966
9. MoeGK, Cotten W, Vick RL: Experimentally induced paroxysmal AV nodal tachycardia in the dog. Amer Heart J 65:87-92, 1963 Preston TA: Atrial ohasic inhibition of imolanted cardiac pace-
11.
12.
makers (abstr). Circulation 38:Suppl 6:1581 1968 Haft JI, Kosowsky BD, Lau SH, et al: Termination of atrial flutter by rapid electrical pacing of the right atrium. Amer J Cardiol 20:239-244, 1967 Aronson AL, Gulotta SJ: Efficacy of percutaneous femoral vein insertion for temporary pacemaker therapy (abstr). Circulation 4O:Suppl 3:38, 1969
VOLUME 26, SEPTEMBER 1970 269
Recommended