
Cardiac Amyloidosis Shifting from Hopeless to Hopeful? Kia Afshar Director, Amyloid Heart Program, IMC Heart Failure: Continuum of Care October 17th, 2015

• None
• I will be discussing some possible future treatments that are currently being investigated but are not FDA approved at this time
Disclosures

• A group of disorders caused by abnormal folding, aggregation, and accumulation of a protein resulting in insoluble fiber deposition into tissues
• Deposits of these amyloid fibrils progressively interfere with the structure/ function of affected organs throughout the body
What is Amyloidosis ?
Biochim Biophys Acta 2005;1753:11 Neth J Med 2004;62:104

Immunoglobulin Kappa light chain
Lysozyme
Apolipoprotein A-1
Transthyretin
X-ray diffraction pattern
Amyloid fibrils

Precursor Protein Amyloid Fibrils
Blood 2009;114:3147

The 23 Amyloidogenic Proteins

The Cardiac Amyloidogenic Proteins

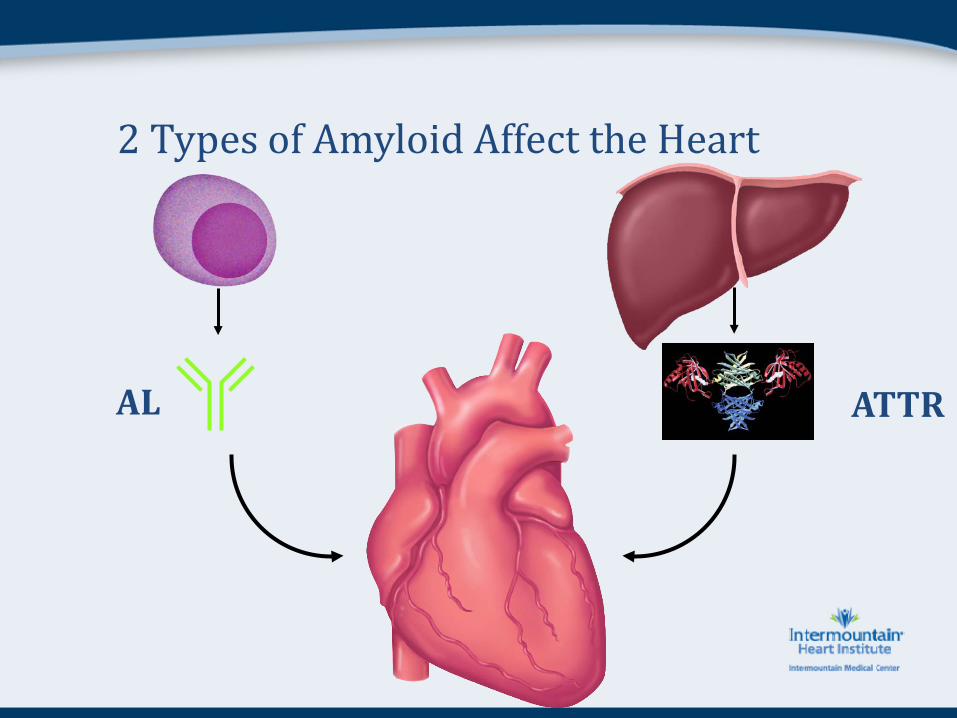
2 Types of Amyloid Affect the Heart
AL ATTR

AL Amyloid
AL
Synonyms: • Primary Amyloid

• Plasma cell dyscrasia related to diseases such as multiple myeloma and monoclonal gammopathy of undetermined significance (MGUS) that produce excess immunoglobulin (paraproteinemia) that happen to be amyloidogenic
• Precursor amyloidogenic protein = Ig light chain (AL)
• AL deposits can develop in any organ system (except brain). Most common: heart and kidney
Next most common: GI (Liver and Lumen)
Then: Peripheral and Autonomic nerves
Finally: Anywhere else except the brain
AL Amyloidosis: Etiology & Pathogenesis


• Most common presenting symptoms are nonspecific
• Symptoms and physical findings vary widely, depending on organ involvement
Fatigue and Weight loss
Carpal tunnel syndrome
Renal – nephrotic range proteinuria (in nondiabetic)
Cardiovascular – restrictive CM
Peripheral neuropathy (symmetric)
GI involvement – hepatomegaly, GI, elevated isolated elevated alkaline phosphatase
Autonomic neuropathy – orthostatic hypotension, bowel dysregulation
AL Amyloidosis: Clinical Features

General Cardiac Neuropathy Orthostatic hypotension Hepatosplenomegaly Macroglossia Ecchymosis (periorbital) Musculoskeletal system
AL Amyloidosis: Physical Findings


• SPEP and UPEP
• Serum and urine immunofixation
• Serum free light chains
AL Amyloidosis: Laboratory Testing

AL Amyloidosis: Serum Free Light Chains
An Abnormal Ratio Proves a Clonal Plasma Cell Disorder - Useful for Diagnosis, Prognosis, Response Assessment Dispenzieri et al. Leukemia 23, 215–224, 2009

AL Amyloidosis: Serum Free Light Chains
• Survival:
• Untreated AL amyloid: 12 months
• Untreated AL w/ cardiac symptoms: 4-6 months
AL Amyloidosis: Disease Specific Treatment

• Prior to the year 2000, there were treatments for plasma cell dyscrasias, however those plasma cell dyscrasias associated with AL amyloid had no treatment options.
• In the last 10-15 years, there have been improved treatment options for those with plasma cell dyscrasias with associated AL amyloid
AL Amyloidosis: Disease Specific Treatment

AL
Cardiac involvement 30-50%
Kidneys Common
Autonomic NS Common
Peripheral NS Common
Carpal Tunnel Sometimes
GI Tract Sometimes
Liver Sometimes
Macroglossia Rare but specific for AL
Periorbital ecchymosis Rare but specific for AL
Age 30-80 yrs
Demographics Anyone
Prognosis 4 to 15 months
Treatment ChemoRx
2 Types of Amyloid Affect the Heart
AL ATTR

Transthyretin Amyloid
ATTR

• Normal blood protein
• Also known as “prealbumin” • Synthesized mainly in liver (but also choroid & retina)
• Transports 25% circulating thyroxine and Vitamin A (retinol) • Circulates as tetramer of 4 identical subunits of 127 AA each
Transthyretin (TTR)

Pathogenesis of Transthyretin Amyloidosis
Chakrabartty, A., PNAS 98, 14757-14759, 2001

Transthyretin Cardiac Amyloid
“Wild-type” protein
Normal function, no amyloid
“Mutant” protein
“Senile” cardiac amyloid
“Familial” cardiac amyloid
ATTR
F.A.P.
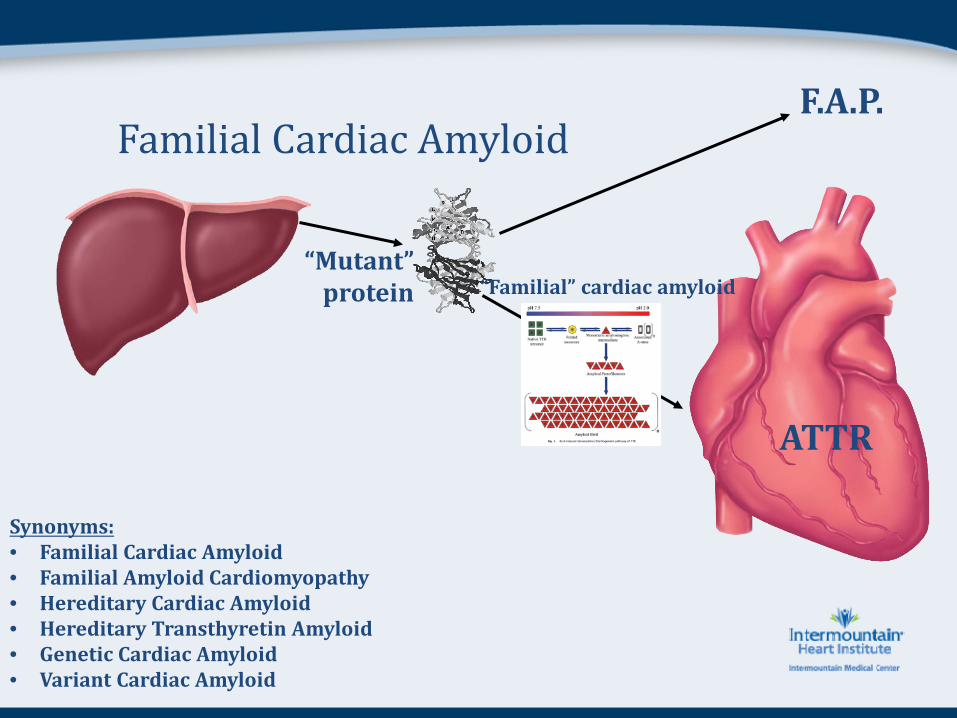
Familial Cardiac Amyloid
“Mutant” protein “Familial” cardiac amyloid
ATTR
F.A.P.
Synonyms: • Familial Cardiac Amyloid • Familial Amyloid Cardiomyopathy • Hereditary Cardiac Amyloid • Hereditary Transthyretin Amyloid • Genetic Cardiac Amyloid • Variant Cardiac Amyloid

Neuropathy

• Approximately 100 mutations associated with amyloidosis worldwide.
• Neuropathy and cardiomyopathy most common.
• Some associated with renal, vitreous, or leptomeningeal amyloid.
• Inheritance is autosomal dominant, penetrance is very high
• Organ Involvement:
• Depends mostly on mutation/geography etc.
Familial Cardiac Amyloid Epidemiology

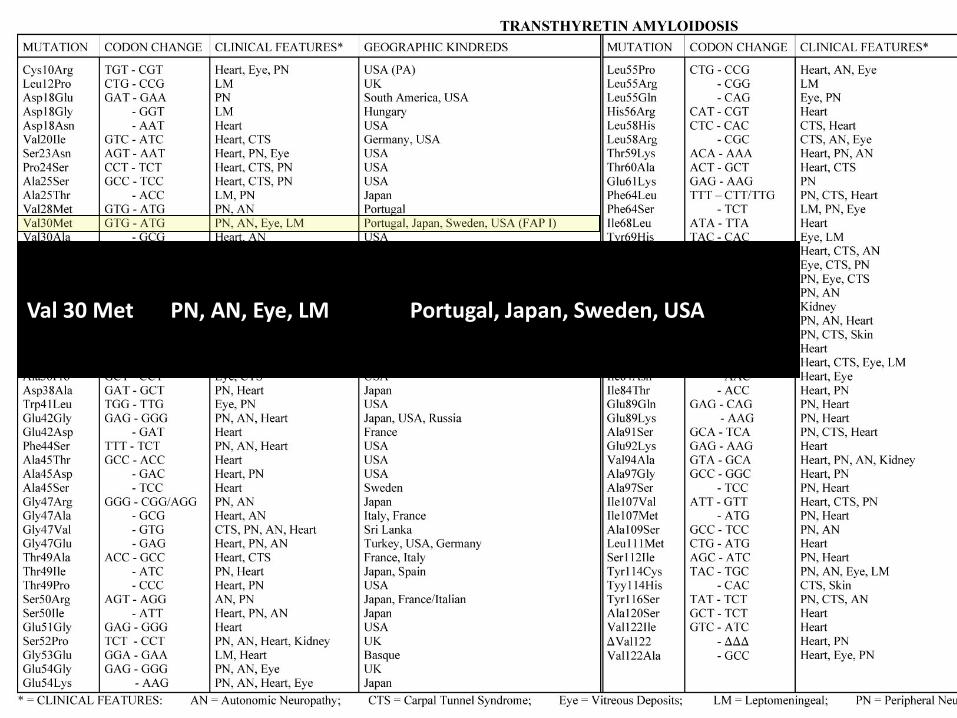
Val 30 Met PN, AN, Eye, LM Portugal, Japan, Sweden, USA

Thr 60 Ala Heart, Carpal Tunnel Northern Ireland (Donegal), USA

Val 122 Ile Heart USA

Phenotype “Neurologic” “Cardiac”
V122I I68L
L111M T60A S77Y
E89L
I107V F64L E89Q
T49A
V30M early onset
V30M late onset
G47A
Familial Cardiac Amyloid Genotypic-Phenotypic Correlation
Organ Transplantation • The mutant TTR is mainly produced in liver
• Orthotopic liver transplant gets rid of main source of variant/mutant protein resulting in a patient now with the wild-type TTR
• However, there is evidence that some patients had progression of their cardiac dysfunction after OLTx.
• Thus, combined OLTx/OHTx began
Familial Cardiac Amyloid Disease Specific Treatment (prior to 2015)

• Liver transplant alone (FAP)
• Combined liver and heart transplant (FAP/FAC)
• Heart transplant alone (FAC - ? V122I mutation)
Familial Cardiac Amyloid Disease Specific Treatment (prior to 2015)

AL Mutant ATTR
Cardiac involvement 30-50% Depends on mutation
Kidneys Common Normal
Autonomic NS Common Depends on mutation
Peripheral NS Common Depends on mutation
Carpal Tunnel Sometimes Occasionally
GI Tract Sometimes Rarely
Liver Sometimes Source of mutant protein
Macroglossia Rare but specific for AL Never
Periorbital ecchymosis Rare but specific for AL Never
Age 30-80 yrs 35-75 yrs
Demographics Anyone Depends on mutation
Prognosis 4 to 15 months 70 months
Treatment ChemoRx Transplants

Transthyretin Cardiac Amyloid
“Wild-type” protein
Normal function, no amyloid
“Mutant” protein
“Senile” cardiac amyloid
“Familial” cardiac amyloid
ATTR
F.A.P.

Senile (wild-type) Cardiac Amyloid
“Wild-type” protein
Normal function, no amyloid
“Senile” cardiac amyloid ATTR

Senile (wild-type) Cardiac Amyloid
“Wild-type” protein
“Senile” cardiac amyloid ATTR

• Due to deposition of “wild-type” transthyretin
• Clinically only affects the heart and carpal tunnel
• A disease of white elderly men
• Age usually occurs in 70’s or 80’s (or older)
• 25% of men > 80yo have senile ATTR at autopsy
• Average life expectancy 7 years
Senile (wild-type) Cardiac Amyloid

Age of Onset of Symptomatic Patients: mutant TTR & wild-type TTR

• None
Senile (wild-type) Cardiac Amyloid: Disease Specific Treatment (prior to 2015)

AL Mutant ATTR Senile ATTR
Cardiac involvement 30-50% Depends on mutation 100%
Kidneys Common Normal Normal
Autonomic NS Common Depends on mutation Normal
Peripheral NS Common Depends on mutation Normal
Carpal Tunnel Sometimes Occasionally 50%
GI Tract Sometimes Rarely Normal
Liver Sometimes Source of mutant protein Normal
Macroglossia Rare but specific for AL Never Never
Periorbital ecchymosis Rare but specific for AL Never Never
Age 30-80 yrs 35-75 yrs 70-100 yrs
Demographics Anyone Depends on mutation Old white men
Prognosis 4 to 15 months 70 months 75 months
Treatment ChemoRx Transplants Supportive

78 year old man with refractory atrial fibrillation despite anti-arrhythmic medications and two afib ablations. Failed two DCCV while on anti-arrhythmics. Atrial fibrillation is very symptomatic despite rate control at 75 bpm.
Case presentation

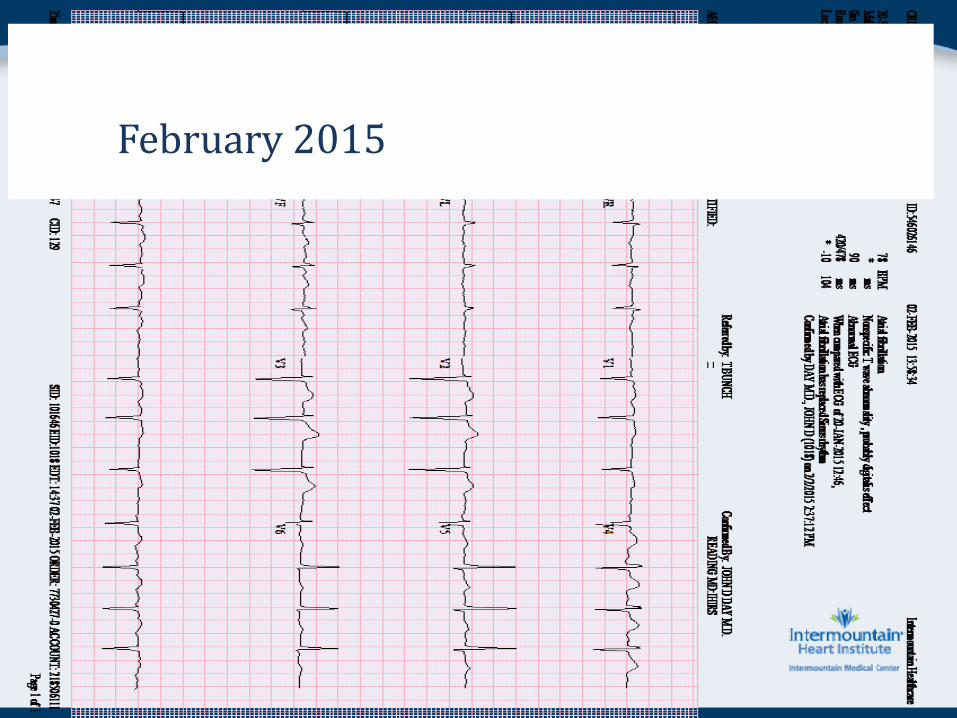
February 2015


February 2015

November 2004

September 2009

December 2011

February 2015

Classic EKG

• Low voltage (defined as < 5mm in all limb leads) is found in only 50% of patients with AL amyloid and only 25-30% in senile cardiac amyloid
• Do not look at precordial leads. Precordial leads are usually normal and can even meet LVH criteria.
• Pseudoinfarct seen in 60% of both senile and AL: Q waves and inverted T waves – usually inferior leads
• Atrial fibrillation is more common in senile (30%), then AL (20%), then mutant (10%)
• Can be associated w/ right-axis or extreme axis deviation
• EKG volts decreasing over time is a red-flag • Most important is to look at “Voltage-to-Mass” ratio by
looking at the EKG volts with echocardiogram thickness
EKG in Cardiac Amyloid

• Concentric LV and RV wall thickening
• Biatrial dilatation
• Restrictive filling pattern with low e’
• Interatrial septal thickening
• Preserved EF early on
• Systolic dysfunction as disease progresses
• Strain imaging with apical sparing of longitudinal strain
Cardiac Amyloid: Summary of Echo findings

• Definitive diagnosis of amyloidosis requires tissue for histological assessment – endomyocardial biopsy
• Typically after tissue diagnosis is confirmed, then need to know which type of amyloidosis (AL vs mutant TTR vs senile TTR) because this affects management, treatment, and prognosis.
Cardiac Amyloid Diagnosis

Diagnostic Approach Clinical + Echo + ECG
Endomyocardial biopsy
SPEP, UPEP, free light chain assay, etc
κ or λ light chains
Heme/Onc Consult
Transthyretin
Genetic testing
Mutant TTR Wild Type TTR

Cardiac Amyloid Management
CA

#1) Alleviated HF symptoms:
Optimization of fluid status is #1 cardinal tenet of cardiac amyloid
• Loop diuretics and spironolactone.
• Steep diastolic filling curve – narrow window of “euvolemia”
• Tachycardia is compensatory for fixed stroke volume. Thus, avoid beta blockers
• CCBs and digoxin are contraindicated due to binding of the amyloid fibers
• ACE/ARBs and other vasodilators can lead profound hypotension from inability of autonomic system to compensate (especially in AL and mutant ATTR)
Cardiac Amyloid Management of Heart Failure

• Atrial fibrillation occurs in about 30% of ATTR patients • Restoration of sinus is challenging given atrial enlargement,
persistently elevated LA pressures, as well as amyloid infiltration of atrium
• Should attempt sinus rhythm with TEE/DCCV and/or AAD • Very high risk of thromboembolic phenomena, so all should be
anticoagulated • Amiodarone is presumed to be safe and can help with both
rhythm and rate control • PPM for amyloid patients with significant conduction disease
(e.g. - 1st deg AVB, RBBB, LAFB) given amyloid progression will eventually result in complete heart block.
• ICD is controversial since most deaths occur from PEA arrest and not VT/VF.
Cardiac Amyloid Management of Arrhythmias

Two-pronged approach
1st – alleviation of HF symptoms
2nd – slow or stop progression
Cardiac Amyloid Management

Two-pronged approach
1st – alleviation of HF symptoms
2nd – slow or stop progression
AL – Chemotherapy +/- SCT +/- OHTx
Mutant TTR – Liver Tx or Heart Tx or both
Senile TTR - none
Cardiac Amyloid Management (prior to 2015)
Two-pronged approach
1st – alleviation of HF symptoms
2nd – slow or stop progression
AL – Chemotherapy +/- SCT +/- OHTx
Mutant TTR – Liver Tx or Heart Tx or both or novel meds
Senile TTR – novel medications
Cardiac Amyloid Management (2015 and beyond)

Small molecule inhibitors
• Noticed that patients with dual mutation - V30M/T119M mutation - did not get the disease. Discovered that T119M caused increase barrier to dissociation from tetramer to monomer.
• Then noticed that when thyroxine was bound to V30M TTR it prevented dissociation into monomers
• Two molecules similar to thyroxine (except bound tighter to TTR tetramer) were then found: Diflunisal and Tafamidis
Transthyretin (ATTR) Cardiac Amyloid Treatments (2015 and beyond)

Block TTR production
Stabilize Tetramer Disrupt Amyloid
Fibrils

Small molecule inhibitors 1) Block production of transthyretin
2) Stabilize the tetramer to prevent monomers 3) Disrupt amyloid fibrils within tissue
Transthyretin (ATTR) Cardiac Amyloid Treatments (currently in trials)

Small molecule inhibitors 1) Block production of transthyretin
2) Stabilize the tetramer to prevent monomers 3) Disrupt amyloid fibrils within tissue
Transthyretin (ATTR) Cardiac Amyloid Treatments (currently in trials)

1) Antisense Oligonucleotide:
• Developed at Indiana University
• Suppresses 80% of TTR production
• Currently in Phase III trial (IV and SQ formulation)
2) Antisense RNA (ALN-TTR):
• Alnynam Technologies – Boston, MA
• Inhibits 50-90% of TTR mRNA production
• Currently in Phase III trial for F.A.P. (IV and SQ formulation)
3) Liver Transplantation:
Transthyretin (ATTR) Cardiac Amyloid 1) Block production of transthyretin

Small molecule inhibitors 1) Block production of transthyretin
2) Stabilize the tetramer to prevent monomers 3) Disrupt amyloid fibrils within tissue
Transthyretin (ATTR) Cardiac Amyloid Treatments (currently in trials)

1) Diflunisal
• NSAID (rarely used nowadays). PO formulation.
• Binds non-selectively to thyroxine binding site and stabilizes tetramer
• Promising results from The Diflunisal Trial in mutant TTR with neurological symptoms
2) Tafamidis
• Pfizer pharmaceuticals
• Binds tightly to thyroxine region to stabilize tetramer
• Currently in Phase III trial with mutant and senile TTR (PO formulation)
Transthyretin (ATTR) Cardiac Amyloid 2) Stabilize the tetramer

Small molecule inhibitors 1) Block production of transthyretin
2) Stabilize the tetramer to prevent monomers 3) Disrupt amyloid fibrils within tissue
Transthyretin (ATTR) Cardiac Amyloid Treatments (currently in trials)

1) Epigallocatechin-3-gallate (EGCG)
• Predominant polyphenol in green tea (PO extract)
• Been shown to decrease LV thickness, increase EF, and improve NYHA class in AL cardiac amyloid patients
• Current Phase II trial underway for TTR
2) Doxycycline
• Disrupts amyloid fibrils in transgenic mice
• Also, decrease prefibrillar aggregates in transgenic mice
• Currently in open label trial at 100mg BID
Transthyretin (ATTR) Cardiac Amyloid 3) Disrupt the amyloid fibrils
• Cardiac amyloid is more common than once perceived
• Two proteins (Ig light chains and TTR) are the cause of the three different types of cardiac amyloid (AL, mutant ATTR, senile ATTR)
• Suspicion should be very high if a patient has “LVH” on echocardiogram with low or normal EKG volts (“Voltage-to-Mass” ratio)
• Must know which precursor protein is being deposited as this alters management and prognosis – endomyocardial biopsy is gold standard
• Diuretics/volume status and avoiding contraindicated medications are the pillars in the supportive management in these patients
• New novel therapies are currently being studied and animal as well as Phase II-III studies have produced optimistic results
Summary
Recommended







![Uncharted waters: rare and unclassified cardiomyopathies ... · without a loading condition such as hypertension or valvular disease [7]. Cardiac amyloidosis Cardiac amyloidosis describes](https://img.dokumen.tips/doc/110x75/5f7f117d3a4eb942540eb802/uncharted-waters-rare-and-unclassified-cardiomyopathies-without-a-loading-condition.jpg)









