
PREVENTIVE MEDICINE 11, 454-463 (1982)
Cancer Preventive Screening Behavior among Elderly Women ‘I*
DAVID D. CELENTANO, SAM SHAPIRO, AND CAROL S.WEISMAN
Health Services Research and Development Center, The Johns Hopkins Medical Institutions, 624 North Broadway, Baltimore, Maryland 21205
Screening procedures and recommendations for early detection of cervical and breast cancer are reviewed with special reference to suggested guidelines for screening among the elderly. Data on preventive practices related to cancer detection were obtained from 675 women in Maryland by telephone interviews. The elderly (65 years of age and older) re- ported fewer detection tests of any type; specifically, 23% report never having had a Pap test and an additional 28% have not had one within 5 years, compared with women under the age of 65, where 98% report having had a Pap test and 79% have had one within the past two years. Elderly women were also less likely than younger women to report receiving routine breast examinations by their physicians, to perform BSE, or to have been taught BSE by a health professional. Type of provider utilized, having a personal physician, and going to a gynecologist account for a significant proportion of the variance in screening practices.
INTRODUCTION
Malignant neoplasms are the second leading cause of death in adult women, accounting for some 23% of all mortality, and breast cancer is the leading site among all cancer deaths in women (1). Both the age-specific incidence and mor- tality rates for breast cancer increase with age (14). Approximately 36% of breast cancer incidence occurs in women aged 65 years and older; an even larger propor- tion of the mortality from breast cancer, 48%, is found in the aged population (3, 21). Similarly, approximately one-quarter (24%) of cervical cancer incidence (excluding carcinoma in situ) and almost 41% of all cervical cancer deaths occur in the population 65 years and older (21).
Secondary prevention approaches that promote the early detection of these diseases are available and seemingly accessible to all women (2). For breast cancer, breast palpation performed by a health professional is recommended (4, 23). Breast self-examination (BSE), while not conclusively proven to decrease the extent of breast disease when measured by stage, tumor size, or lymph node involvement (6,9, 15, 17, 19, 20), has been widely recommended by the American Cancer Society as a monthly procedure for every woman (4). Screening for cervi- cal cancer by the Pap test is widely accepted, although questions are raised peri- odically about the effkacy of this detection method (5, 10, 13). While the recom- mended periodicity of Pap testing has recently been revised by the ACS, it is currently suggested that asymptomatic women receive Pap tests every 3 years
’ Supported in part by Grant CA20322 from the National Cancer Institute. ’ A preliminary version of this paper was presented at the Annual Meeting of the American Public
Health Association, Detroit, Mich., October 23, 1980.
454
0091.7435/82/040454-10$02.00/O Copyright @ 1982 by Academic Press, Inc. AU rights of reproduction in any form reserved.

CANCER PREVENTIVE SCREENING BEHAVIOR 455
after two negative annual Pap tests are found (unless women are at high risk) (4). These recommendations hold for women through the age of 65 years, at which point routine screening is discontinued.
The cancer prevention and gerontology literatures (7,8, 18) make little mention of the special needs and problems of the elderly in participating in cancer detec- tion efforts. Indeed, there is almost no mention of any preventive actions to be taken to prevent or detect disease or to promote health (7, 16). Given the high incidence of cancer among the elderly for many cancers, the present study ad- dresses the extent to which the elderly are following recommended preventive ac- tions for the early detection of cancer. In this paper, factors which differentiate elderly women (here referred to most frequently as those women aged 65 years and older) from younger women in cancer screening participation will be explored.
METHODS
The data on preventive health behaviors related to cancer detection were col- lected in two waves of a telephone survey of a random sample of households listed in telephone directories in four nonmetropolitan counties in Maryland during 1979 and 1980. Households were predesignated to be either “female interview” or “male interview” households prior to interview in order to maximize the number of males to be interviewed (since it has generally been found in the telephone survey literature that women are more frequently found at home and that they are more likely to answer the telephone than are men among married couples). A total of 1600 household listings were sampled from the telephone directories; in 87.1% of the cases an interview was possible (in the remaining 206 cases the telephone number was no longer connected). Of the 1,394 eligible numbers, interviews were attempted with 795 women (i.e., in 57% of the eligible households. either a female was predesignated for interview or a “male interview” household did not have a male present), with 675 completed interviews obtained, yielding an overall re- sponse rate of 84.9%. Of the 120 women who were not interviewed, 101 refusals were obtained (12.7%) and there were 19 incomplete interviews (“breakoffs”). In households where more than one eligible woman was found, the “female head of household” was selected, resulting in a sample which is slightly older than that of the general population.
The structured interviews lasted approximately one-half hour and were con- ducted by trained, professional interviewers contracted by the study team. These interviewers were all experienced in conducting medically related interviews; no major discrepancies between the 11 interviewers were determined on any of the major variables of interest.
The surveys were conducted as part of the outreach program of a regional oncology center for the development of cancer control activities and organization in local communities (22). These nonmetropolitan areas were known to have few formal cancer control programs at the time of the surveys. Each was served by one community hospital, and local providers and agencies were interested in developing cancer control programs. The surveys encompassed rura,l and subur- ban (commuting distance to Baltimore) communities with a wide range of socio- economic levels and large numbers of the elderly. While there is some “truck

456 CELENTANO, SHAPIRO, AND WEISMAN
farming” and fishing industry, these communities can best be characterized as “rural non-farm,” for there is some light industry in each area. As the communities are predominantly white, data on nonwhites are excluded from the analyses, resulting in a base number of 634 women for the analysis. As no significant differences were found across the four communities, the data from each is com- bined herein. Further, the results from this study are generalizable only to non- metropolitan communities, for no urban populations were sampled. Also, while the sample was limited to those households with listed telephone numbers, thereby again reducing the generalizability of the Iindings, the prevalence of un- listed numbers in these communities is extremely low and telephone subscription is nearly universal.
RESULTS
Table 1 shows the proportion by age of women who report “ever” having had any test to detect cancer, in response to an open-ended question that did not define what such tests were but rather was designed to elicit respondents’ percep- tions of what cancer detection tests are. The proportion is constant for women aged 18 to 64 years, where approximately four in five report having had some test. At age 65, the proportion drops off to approximately two-thirds of women report- ing ever having had any detection test, while only one-half of respondents 75 years and older report ever having had any detection test.
With respect to cervical cancer screening specifically, women over the age of 65 years reveal deficient screening histories. Thirty-eight percent of women 75 years and older and 14% of women aged 65-74 years report never having had a Pap test. Further, 28% of the women 65 years and older who have ever had a Pap test reported that their last Pap test was performed at least 5 years previously. Thus, nearly one-half (5 1.2%) of elderly women in this sample have either never had a Pap test or have not had one in a long time. These findings are in distinct contrast to the findings for younger women, where some 98% of women under 65 years report having received a Pap test at some point in their lives, and 7% report receiving a Pap test within the past 24 months.
Figure 1 shows the distributions by age for the recency of the last Pap test reported by respondents. “Recency” has been defined as follows: (a) those who received their last Pap test within the past 2 years; (b) those reporting the most recent Pap test was at least 2 years previously (where the average time was 5l/2 years before); and (c) those who report never having had a Pap test. It can be seen that there is a strong, negative linear relationship between age and the proportion of women reporting a recent Pap test.
In attempting to account for these strong relationships with age, many factors were considered, including the usual source of medical care, types of medical care providers utilized in the past year, perceived health status, and attitudes and knowledge about cancer. Table 2 shows the usual source of medical care reported by women in this study. Women aged 55 years and older were more likely than women under 55 years to identify a family physician or general practitioner as the “regular” medical care provider. Approximately 28% of women under age 55 reported that an obstetrician-gynecologist was their usual source of medical care;

? TA
BLE
1 PE
RC
ENTA
GE
DIS
TRIB
UTI
ON
S O
F W
OM
EN
REP
OR
TIN
G E
VER
HAV
ING
R
ECEI
VED
VA
RIO
US
CAN
CER
DET
ECTI
ON
TE
STS,
BY
AGE=
z E
As
;
Type
of
canc
er
m
2 de
tect
ion
test
To
tal
<35
35-4
4 45
-54
55-6
4 65
-74
a75
X Zh
P 2
Any
self-
repo
rted
test
75
.4
74.4
81
.4
81.6
81
.0
64.5
51
.2
25.1
3 0.
001
(634
) is
(1
72)
(129
) (9
8)
(116
) 6’
6)
(43)
x
Rou
tine
phys
icia
n br
east
81
.5
95.3
86
.0
81.6
75
.8
73.8
40
.5
79.7
9 0.
001
E ex
amin
atio
n (6
33)
(172
) (1
2%
(98)
(1
16)
(76)
(4
2)
F Br
east
sel
f-exa
min
atio
n 90
.4
94.2
93
.0
96.1
87
.9
91.8
54
.1
65.5
1 0.
001
2 (6
25)
(172
) (1
2%
(98)
(1
16)
(73)
(3
7)
0 E a
Base
N g
iven
in
pare
nthe
ses
belo
w p
erce
ntag
es.
* x2
test
s ea
ch h
ave
five
degr
ees
of f
reed
om.
7 s B

458 CELENTANO, SHAPIRO, AND WEISMAN
100 I
go., ’ \\ =.. -.
80. -*. * --._ --__ -- l
70. '. '.
'\ *. '. 60. '. '.
SO-
40.
30-
20-
lo-
OT-
* --_ -______ t ‘,
Pap Test Within Two Years
18-34 35-44 45-54 55-64 65-74 7s
AGE
FIG. 1. Percentage distributions of recency of last Pap test by age.
TABLE 2 PERCENTAGE DISTRIBUTION OF USUAL SOURCE OF CARE REPORTED BY RESPONDENTS, BY AGE
&e General
practitioner Obstetrician- gynecologist Other” TotaP
<35 58.2 28.1 13.8 100.0 (189)
35-44 54.4 28.1 16.9 100.0 (136)
45-54 53.8 28.9 17.3 100.0 (104
55-64 65.3 5.8 28.1 100.0 (121)
65-74 72.1 1.3 26.0 100.0 (77)
75-k 81.8 0 18.2 100.0 (44
Total 61.3 19.4 19.3 100.0 (671)
a “Other” includes primarily Internal Medicine and its subspecialties (most notably Cardiology) and Surgical specialties.
* N given in parentheses.
CANCER PREVENTIVE SCREENING BEHAVIOR 459
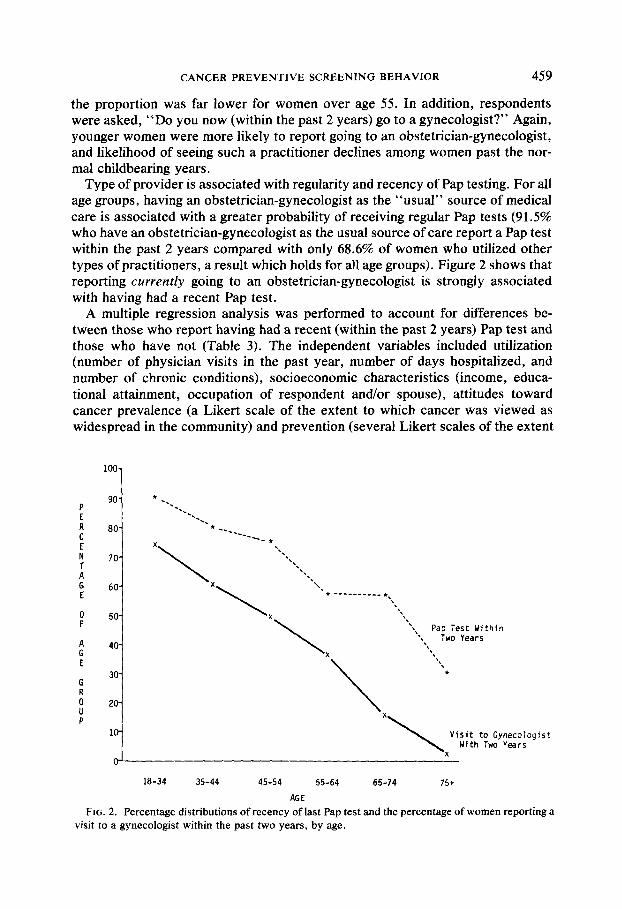
the proportion was far lower for women over age 55. In addition, respondents were asked, “Do you now (within the past 2 years) go to a gynecologist?” Again, younger women were more likely to report going to an obstetrician-gynecologist, and likelihood of seeing such a practitioner declines among women past the nor- mal childbearing years.
Type of provider is associated with regularity and recency of Pap testing. For all age groups, having an obstetrician-gynecologist as the “usual” source of medical care is associated with a greater probability of receiving regular Pap tests (91.5% who have an obstetrician-gynecologist as the usual source of care report a Pap test within the past 2 years compared with only 68.6% of women who utilized other types of practitioners, a result which holds for all age groups). Figure 2 shows that reporting currently going to an obstetrician-gynecologist is strongly associated with having had a recent Pap test.
A multiple regression analysis was performed to account for differences be- tween those who report having had a recent (within the past 2 years) Pap test and those who have not (Table 3). The independent variables included utilization (number of physician visits in the past year, number of days hospitalized, and number of chronic conditions), socioeconomic characteristics (income, educa- tional attainment, occupation of respondent and/or spouse), attitudes toward cancer prevalence (a Likert scale of the extent to which cancer was viewed as widespread in the community) and prevention (several Likert scales of the extent
loo-
go-
80-
70-
60-
50-
40-
30-
ZO-
lo-
* %.
%, %
l --- ---_
x --- *
\
‘\ ‘\
‘\ ‘.
‘.
x ‘.
\
‘. l --- ----___ l ,
‘\
x ‘\
\
‘\ ‘\
'. Pap Test Within
'\ Two Years
x '\
\
'\ '\
*
x
\
Visit to Gynecologist With Two Years
x 0’
18-34 35-44 45-54 55-64 65-74 75+
AGE
FIG. 2. Percentage distributions of recency of last Pap test and the percentage of women reporting a visit to a gynecologist within the past two years, by age.
460 CELENTANO, SHAPIRO, AND WEISMAN
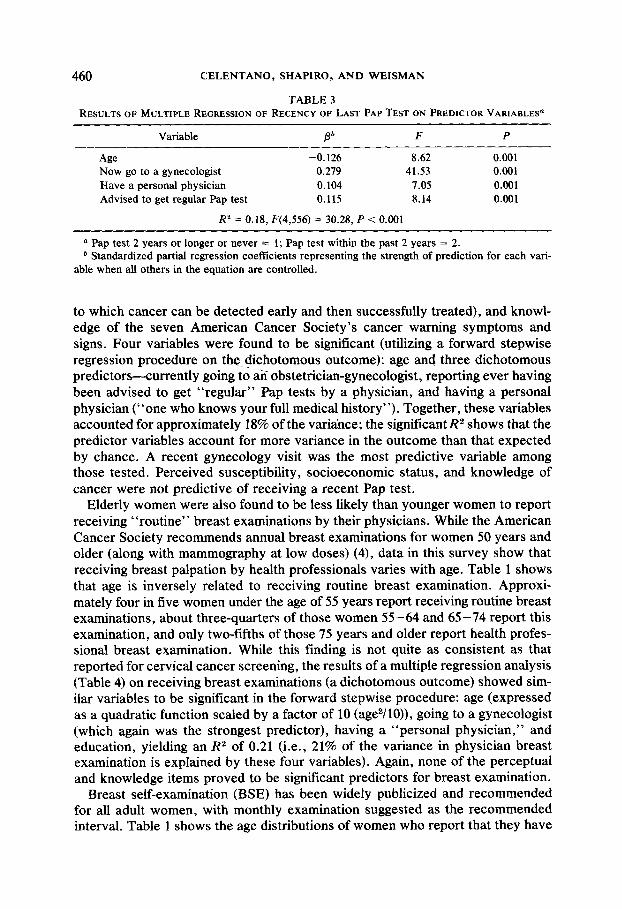
TABLE 3 RESULTS OF MULTIPLE REGRESSION OF RECENCY OF LAST PAP TEST ON PREDICTOR VARIABLES
Variable Pb F P
Age -0.126 8.62 0.001 Now go to a gynecologist 0.219 41.53 0.001 Have a personal physician 0.104 7.05 0.001 Advised to get regular Pap test 0.115 8.14 0.001
R2 = 0.18, F(4,556) = 30.28, P < 0.001
(1 Pap test 2 years or longer or never = 1; Pap test within the past 2 years = 2. * Standardized partial regression coefficients representing the strength of prediction for each vari-
able when all others in the equation are controlled.
to which cancer can be detected early and then successfully treated), and knowl- edge of the seven American Cancer Society’s cancer warning symptoms and signs. Four variables were found to be significant (utilizing a forward stepwise regression procedure on the. dichotomous outcome): age and three dichotomous predictors-currently going to an obstetrician-gynecologist, reporting ever having been advised to get “regular” Pap tests by a physician, and having a personal physician (“one who knows your full medical history”). Together, these variables accounted for approximately 18% of the variance; the significant R2 shows that the predictor variables account for more variance in the outcome than that expected by chance. A recent gynecology visit was the most predictive variable among those tested. Perceived susceptibility, socioeconomic status, and knowledge of cancer were not predictive of receiving a recent Pap test.
Elderly women were also found to be less likely than younger women to report receiving “routine” breast examinations by their physicians. While the American Cancer Society recommends annual breast examinations for women 50 years and older (along with mammography at low doses) (4), data in this survey show that receiving breast palpation by health professionals varies with age. Table 1 shows that age is inversely related to receiving routine breast examination. Approxi- mately four in five women under the age of 55 years report receiving routine breast examinations, about three-quarters of those women 55-64 and 65-74 report this examination, and only two-fifths of those 75 years and older report health profes- sional breast examination. While this finding is not quite as consistent as that reported for cervical cancer screening, the results of a multiple regression analysis (Table 4) on receiving breast examinations (a dichotomous outcome) showed sim- ilar variables to be significant in the forward stepwise procedure: age (expressed as a quadratic function scaled by a factor of 10 (age2/10)), going to a gynecologist (which again was the strongest predictor), having a “personal physician,” and education, yielding an R2 of 0.21 (i.e., 21% of the variance in physician breast examination is explained by these four variables). Again, none of the perceptual and knowledge items proved to be significant predictors for breast examination.
Breast self-examination (BSE) has been widely publicized and recommended for all adult women, with monthly examination suggested as the recommended interval. Table 1 shows the age distributions of women who report that they have

CANCER PREVENTIVE SCREENING BEHAVIOR
TABLE 4 RESULTS OF MULTIPLE REGRESSION OF PHYSICIAN BREAST EXAMINATION
ON PREDICTOR VARIABLE@
461
Variable Ob F P
Now to a gynecologist go 0.326 57.61 0.001 Age2 -0.136 9.80 0.001 Years of education 0.101 6.24 0.001 Have a personal physician 0.074 3.98 0.050
R* = 0.21,F(4,556) = 37.10,P < 0.001
L1 No physician breast examination = 0; physician breast examination reported = 1. b Standardized partial regression coefficients.
“ever” performed BSE. These self-reported rates of BSE are higher than compa- rable national figures (11). Among those who report that they currently perform BSE (defined as having done BSE at least one time during the previous year), there is a significant trend between age and the proportion of women reporting having been taught BSE by a health professional. Of women under age 65, 66% report being taught BSE, compared with 58% of those aged 45-64 and only 32% of women aged 65 years and older. Approximately 70% of women under the age of 65 years who report currentlypracticing BSE also report having received personal instruction, while only one-half of women over 65 years who report performing BSE state that they were taught the procedure by a health professional. Pamphlets and articles in women’s magazines were most often mentioned by elderly women as their primary source of information on BSE. While most of the women who report having been taught BSE by a health professional (most often a physician) state that they were not asked to demonstrate their competency to the instructor, elderly women report that they were much less likely to have been given the opportunity to show their proficiency as compared with younger women (20% and 41%, respectively). These findings are important because of the evidence that only one-to-one teaching leads to proper BSE practice (12). No differences were found in reported frequency of BSE by age, with almost 4 in 10 women reporting BSE at least monthly.
DISCUSSION
Several implications for cancer control activities can be drawn from these data concerning screening behavior among elderly women, a population at high risk for cancer. Compared with younger women, the older women surveyed in this study have less experience in cancer detection, both for cervical cancer screening and for breast cancer detection. The major factor accounting for these lower rates appear to be the type of provider utilized, with use of general practitioners being related to lesser experience with detection tests and use of gynecologists with increased regularity and recency of detection tests. Although other investigators have found that BSE performance is associated with having a “personal” physi- cian (12), obstetrician-gynecologist visits were found to be the most important variable in this study.

462 CELENTANO, SHAPIRO, AND WEISMAN
One inference that might be drawn from these data is that the observed differ- ences in screening behavior are indicative of cohort effects rather than a direct function of aging. That is, rather than suggesting that women change their utiliza- tion behavior as they age-particularly as they move out of the childbearing years-the data may be interpreted as suggesting that overall patterns of utilization among women are changing over time, with younger cohorts of women likely to be more representative of future patterns. In this study, elderly women are more likely to report never having had a Pap test, a finding which can be attributed in part to their utilization patterns and to the fact that the Pap test became a routine screening test only in the late 1950s and early 196Os, a time when the women now aged 65 years and older would have been moving out of the childbearing years. Among women currently of childbearing age, Pap testing is substantially more frequent and nearly universal among those who report seeing an obstetrician- gynecologist. Furthermore, the strong inverse relationship between age and see- ing an obstetrician-gynecologist shown in Fig. 2 suggests an increasing trend towards obstetrician-gynecologist utilization among younger women.
Associated with this inference is evidence of shifts in the pattern of medical care utilization in the general female population. With decreasing numbers of general practitioners, there is evidence of increasing utilization of internists and other specialists, including obstetrician-gynecologists. The increasing role of obstetri- cians and gynecologists in providing primary care services to women has been well documented (24,25). Thus, the availability and utilization of cancer detection procedures in the future may change due to changes in provider behavior and utilization patterns.
Nevertheless, most efforts at increasing participation in cancer detection are now focused upon young women and current recommendations and guidelines assume that all women have at one point been screened. However, this study shows that a larger proportion of elderly women have never been screened, and this group represents a population at high risk. Virtually all cervical cancer screening programs are targeted to women in the reproductive years, but a signifi- cant proportion of new cases of cervical cancer occur in the elderly. Likewise, breast cancer detection and BSE instruction are often heavily focused upon young women, even though the majority of the incidence and mortality occurs in the elderly population. Given the lack of attention paid to targeting cancer detection programs to the elderly, the low rates of screening experience and BSE perfor- mance among the elderly reported here are perhaps not surprising.
At present, one can speculate that the relatively low utilization of cancer screening procedures among the elderly relates to the primary care providers’ concerns when providing care to this population. Since it has been shown here that using family physicians as the usual source of care leads to lower rates of detection experience compared with using other types of providers, it may be that general practitioners and family physicians are not giving attention to preventive services for the elderly, but rather, are more concerned with their patients’ chronic problems. To increase utilization of Pap tests and to assure routine breast examinations among elderly women, increased efforts need to be directed at gen- eral practitioners and family physicians in recognizing the extent of the problem and their role in assuring adequate preventive health care.

CANCER PREVENTIVE SCREENING BEHAVIOR 463
REFERENCES
1. American Cancer Society. “Cancer Facts & Figures 1981.” American Cancer Society, New York, 1980.
2. Bailar, J. C. The case for cancer prevention. J. Nut. Cancer Inst. 62, 727-731 (1979). 3. Cutler, S. J., and Young, J. L. “Third National Cancer Survey: Incidence Data,” DHEW Publi-
cation 75-787, National Cancer Institute, Bethesda, Md. 1975. 4. Eddy, D. Guidelines for the cancer-related checkup; Recommendations and rationale. Cancer J.
C/in. 30, 194-240 (1980). 5. Foltz, A. M., and Kelsey, J. L. The annual Pap test: A dubious policy success. Milbank Mem.
Fund Quart. 56, 426-462 (1978). 6. Foster, R. S., Lang, S. P., Costanza, M. C., Worden, J. K., Haines, C. R., and Yates, J. W.
Breast self-examination practices and breast-cancer stage. New Engl. J. Med. 299, 265-270 (1978).
7. German, P. G., Shapiro, S., Chase, G. A., and Vollmer, M. H. Health care of the elderly in medically disadvantaged populations. Gerontologist 18, 547-555 (1978).
8. German, P. G. The elderly: A target group highly accessible to health education. Int. J. Health Educ. 21, 267-272 (1978).
9. Greenwald, P., Nasca, P. C., Lawrence, C. E., Horton, J., McGarrah, R. P., et al. Estimated effect of breast self-examination and routine physician examinations on breast-cancer mortality. New Engl. J. Med. 299, 271-273 (1978).
10. Lave, J. R., and Lave, L. B. Measuring the effectiveness of prevention. Milbank Mem. Fund Quart. 55, 273-289 (1977).
11. Leiberman Research, Inc. A basic study of public attitudes toward cancer and cancer tests- Highlights. A study conducted for the American Cancer Society. Lieberman Research Inc., New York, 1980.
12. McCusker, J., and Morrow, G. R. Factors related to the use of cancer early detection techniques. Prev. Med. 9, 388-397 (1980).
13. Miller, A. B. Screening for cancer of the cervix in Canada, post Walton, in “Screening in Cancer” (A. B. Miller, Ed.) International Union Against Cancer, Geneva, 1978.
14. Moolgavkar, S. H., Stevens, R. G., and Lee, J. A. H. Effects of age on incidence of breast cancer in females. J. Nut. Cancer Insf. 62, 493-501 (1979).
15’. Moore, F. D. Breast self-examination (Editorial). New Engl. J. Med. 299, 304-305 (1978). 16. National Institute on Aging. “Our Future Selves: A Research Plan Toward Understanding
Aging,” DHEW Publication 77- 1096, National Institutes of Health, Bethesda, Md., 1977. 17. Senie, R. T., Rosen, P. P., Lesser, M. L., and Kinne, D. W. Breast self-examination and medical
examination related to breast cancer stage. Amer. J. Public Health 71, 583-590 (1981). 18. Shanas, E., and Maddox, G. L. Aging, health and health resources, in “Handbook of Aging and
the Social Sciences” (H. Binstock and E. Shanas, Eds.), Van Nostrand, Reinhold, New York, 1976.
19. Smith, E. M., Francis, A. M., and Plissar, L. The effect of breast self-exam practices and physi- cian examinations on extent of disease at diagnosis. Prev. Med. 9, 409-417 (1980).
20. Thiessen, E. U. Breast self-examination in proper perspective. Cancer 28, 1537-1545 (1971). 21. U.S. Department of Health and Human Services. “Vital Statistics of the United States, 1976,”
Vol. II, “Mortality,” Part A. National Center for Health Statistics, Hyattsville, Md., 1980. 22. Vaughan, W. P., Waalkes, T. P., Lundhal, S., Shapiro, S., White, P., et al. The Frederick Cancer
Control Project-A model for regional oncology center/community collaboration in cancer control. Md. Sfate Med. J. 31, 37-42 (1982).
23. Venet, L., Strax, P., Venet, W., and Shapiro, S. Adequacies and inadequacies of breast examina- tions by physicians in mass screening. Cancer 28, 1546-1551 (1971).
24. Wechsler, H., et al. A follow-up study of residents in internal medicine, pediatrics and obstetrics- gynecology training programs in Massachusetts. New Engl. J. Med. 298, 15-21 (1978).
25. Willson, J. R., and Burkons, D. M. Obstetrician-gynecologists are primary physicians to women. Amer. J. Obstet. Gynecol. 126, 627-632 (1976).
Recommended

















