
Journal of Advanced Nursing, 1997, 25, 801-808
Can action research be applied in developingclinical teaching?
Kristiina Hyrkas MNSc RNActing Senior Lecturer, Doctoral Student, University of Tampere, Department of NursingScience, Tampere. Finland
Accepted for publication 19 April 1996
HYRKAS K. (1997) Journal of Advanced Nursing 25, 801-808Can action research be applied in developing clinical teaching?Nursing education has undergone significant changes during the last twodecades in Finland. However, clinical teaching has remained unchanged eventhough it forms the most extensive part of nursing education. National andinternational research results have also exposed several problems for clinicalteaching. In the Finnish nursing education system these problems haveremained unsolved probably because many ofthe suggestions for development,based on research results, presuppose changes in both the college and healthcare systems. The whole system of clinical teaching was changed during theyears 1992-1993 in one nursing college and in one hospital in Tampere,Finland. Action research as a research strategy was applied in this study. Thepurpose of this paper is to describe the solutions sought and to assess if actionresearch can be applied to the development of clinical teaching.
INTRODUCTION
In Finland in recent years the length and content of nursingeducation have changed. However, the clinical teachingcomponent has remained unchanged even though it formsthe most extensive part of nursing education and providesprofound experience for the professional growth of nursingstudents. Depending on the chosen specialization theamount of clinical experience varies from 50 to 60% ofthe total hours of the main subject. In reality this meansthat approximately three-quarters of tbe teaching duringthe clinical experience is accomplished outside the officialcolleges in different kinds of social and health careservice organizations (Ammattikasvatushallitus 1989,Opetushallitus 1991).
Clinical experience is expected to be an integral part ofnursing education. It has been seen that sldlls and knowl-edge learned in the classroom setting only make sensewhen they are applied in clinical practice (Jacobson 1966,Ammattikasvatushallitus 1989, Dunn et al. 1995).
One special feature of the Finnish nursing education
Correspondence: Kristiina Hyrkas, University of Tampere, Department ofNursing Science, PO Box 607, FIN-33101 Tampere, Finland.
system is that the clinical teaching is co-ordinated by nurs-ing teachers from the colleges of nin-sing but, even thoughthe nursing teacher is present in the clinical settings, theactual bedside teaching is carried out by staff nurses. Thereason for this is that the teachers' role in clinical settingsis very unclear and legally uncertain; the teachers are notlegal members of the social and health care serviceorganizations.
From 1992 to 1993 a project was undertaken in Tampere,Finland. The aim of the project was to develop clinicalteaching as a goal-oriented, planned and collaborativesystem by systematic planning and reorganization betweena nursing college and a 282-bed hospital. Action researchwas chosen as the most appropriate methodology for theproject. The focus of this paper is to try to answer thequestion 'Can action research be applied in developingclinical teaching?' by a closer consideration of an exampleof how action research was applied and also by discussingthe problems raised.
Review ofthe problems in clinical teaching
In Finnish nursing education clinical experience has beenconsidered to be very difficult to accomplish both in
© 1997 Blackwell Science Ltd 801
K, Hyrkas
quantity and quality. One of the main problems of thesystem seems to be tbe flexibility in the curriculum. Thisis a result of the hierarchic structure of the curriculum ontwo different levels: the objectives are loosely determinedat both national and college levels leaving teachers a lotof freedom in their interpretation. Most of tbe personnelin social and health care service organizations, however,have not completed higher education. This means thatthe frames of reference to plan and accomplishclinical teaching and supervision may vary greatly(Ammattikasvatushallitus 1989).
The problems of clinical practice have been noted ininternational research. The results reveal that clinical stud-ies have not been adequately founded and tberefore theffndings tend to be vague and ambiguous (Forthergill-Bourbonnais & Smith-Higuchi 1995). The reason for thisdifficulty has been found to be poor goal orientation andinadequate and baphazard planning. Students accomplisbjust the routine duties and work together (Costello 1989).Individual and all-inclusive nursing does not form theessential content of the studies, as students learn toaccomplish single tasks and task-centred nursing. Clinicalstudies do not support the educational goals to be attained.In Finland it has been found that minimal time has beenspent on clinical teaching and supervision even thoughclinical experiences are stated to be the most importantlearning opportunities for students' professional growth(Leino-Kilpi et al. 1987).
These findings are notable because, in the Finnish nurs-ing education system, clinical teaching is organized by tbenursing teachers from the nursing colleges. The nursingteachers are responsible for the educational arrangementof clinical practice, and the personnel in social and healthcare service organizations are responsible for the super-vision ofthe students. The problems mentioned above arehardly likely to diminish the classical problem of thetheory and practice gap. Time as a resource is also expens-ive and needs to be taken into consideration because ofeconomic constraints; financial resources for Finnish nurs-ing education are decreasing (Hokkanen et al. 1994,Bamad & Dunn 1994).
ACTION RESEARCH AS A RESEARCHIMETHOD
Attempts have been made to define action research inseveral different ways, with Cohen & Manion (1980)stating that there is no generally accepted definitionfor action research. Tbis problem can be seen to originatefrom the fact that action research is seen more as astrategy for change than as a research method. In spite oftbe differences between tbese definitions, four similarand common cbaracteristics have been found identifyingthat action research seeks (Holter & Schwarz-Barcott1993):
1 to achieve collaboration between researcher andpractitioners;
2 to solve problems in practice;3 to aim at change;4 to strive for theory development.
The role of the researcher in action research differs fromthat of the traditional researcher's as the researcher is anactive member in the community. In action research theresearcher's intention is to solve problems in practice and,on the other hand, to collect data, which are essential forthe action and its development and are also of scientificinterest. However, the focus is also on collaborationbetween the researcher and tbe respondents. The partici-pating members in action research are in an equal positionthroughout the entire researcb process so that, during itsprogress, the researcher and respondents are able to con-trol all the different phases (Carr & Kemmis 1986, Argyrisef al. 1987, Holter & Schwarz-Barcott 1993).
Phases
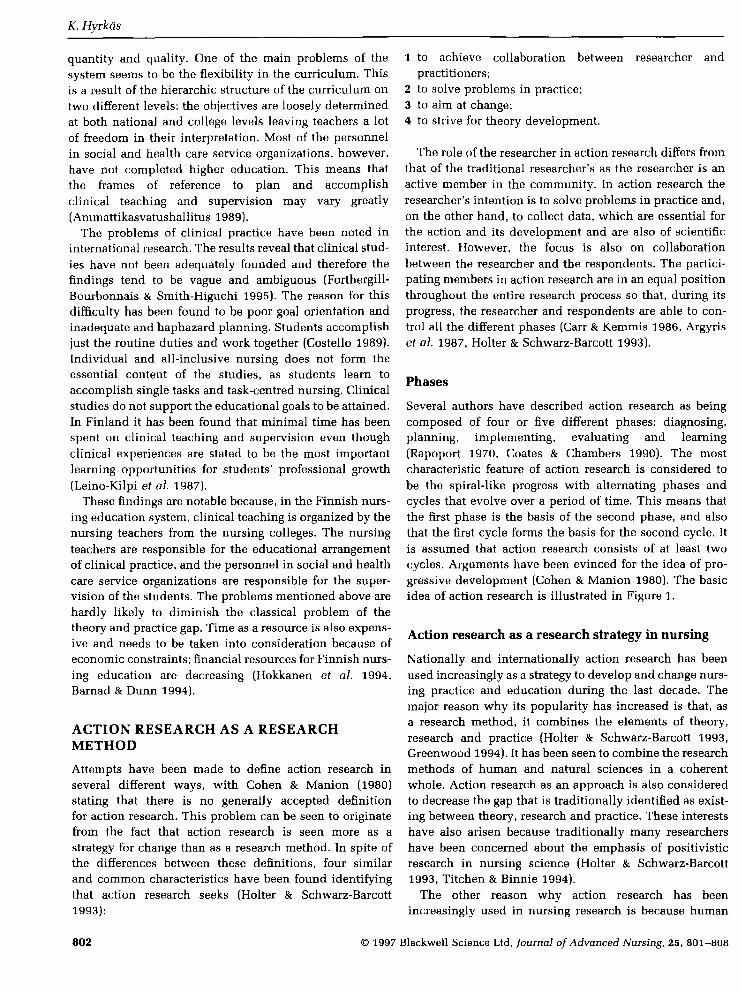
Several authors have described action researcb as beingcomposed of four or five different phases: diagnosing,planning, implementing, evaluating and learning(Rapoport 1970, Coates & Chambers 1990). Tbe mostcharacteristic feature of action research is considered tobe the spiral-like progress with alternating phases andcycles that evolve over a period of time. This means thatthe first phase is tbe basis of the second phase, and alsothat the first cycle forms the basis for the second cycle. Itis assumed that action research consists of at least twocycles. Arguments have been evinced for the idea of pro-gressive development (Cohen & Manion 1980). The basicidea of action research is illustrated in Figure 1.
Action research as a research strategy in nursing
Nationally and internationally action research has beenused increasingly as a strategy to develop and change nurs-ing practice and education during the last decade. Themajor reason why its popularity has increased is that, asa researcb method, it combines the elements of theory,researcb and practice (Holter & Schwarz-Barcott 1993,Greenwood 1994). It has been seen to combine the researchmethods of human and natural sciences in a coherentwhole. Action research as an approach is also consideredto decrease the gap that is fraditionally identified as exist-ing between theory, research and practice. These interestshave also arisen because traditionally many researchershave been concerned about the emphasis of positivisticresearch in nursing science (Holter & Schwarz-Barcott1993, Titchen & Binnie 1994).
The other reason why action research has beenincreasingly used in nursing researcb is because human
802 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 801-808
Action research in clinical teaching
First cycle Second cycle Third cycle ^ Figure 1 Action research, thephases, cycles and progress intime (Hyrkas 1996).
beings are considered as holistic. Humans are compre-hended as self directing, having initiative and beingresponsible for their own learning. Humans are seen notjust as passive participants in their working community,but also as being capable and willing to confribute to theircommunity's functions. The basic assumption in actionresearch is that only the members of a community canexplore and develop their own community's functions inthe best possible way. Action research increases the aware-ness of people by activating or initiating both change anddevelopment (Holter & Schwarz-Barcott 1993, Greenwood1994, Suojanen 1994).
In research concerning education, for example, teachershave traditionally been seen as passive objects of theinquiry or recipients of the results but not actual research-ers (Suojanen 1994). For the development of educationpractice this has not been appropriate. In recent years edu-cational organizations in Finland have been autonomizedand decision-making has been devolved to college level.As a result, researcb has revealed tbat more interest isbeing taken in the evaluation of one's own work and devel-opment. Action research has been emphasized as a poten-tial, participative and democratic way to inquire into anddevelop the performance of organizations and people(Kurtakko 1990, Suojanen 1994).
THE DIFFERENT APPROACHES IN ACTIONRESEARCH
Three different approaches have been traditionally ident-ified in action research based on natural and historical-hermeneutic as well as critical sciences. Holter & Schwarz-Barcott (1993) call these approaches technical collabor-ative, mutual collaboration and enhancement approaches,while Greenwood (1994) names them commissioned inter-vention, participatory action research and action science.Even though the approaches are named differently acommon basis can be found in their different interests inknowledge. This background can be stated to be in theHabermasian position in which knowledge is never'disinteresting' but always constructed by human agents
to serve particular human interests. These interests aretechnical, practical and emancipatory (Habermas 1974).
Action research based on technical interests includesthe assumption that instrumental knowledge allowshuman agents to control the natural world. The approachis based on a theoretical frame of reference or theory whichis determined beforehand. A certain intervention is testedand the main purpose is to find out if the interventionis applicable to practice. Collaboration between theresearcher and the members of the target community isbased on the problems, and the interventions are identifiedand specified beforehand. This approach is based on natu-ral sciences (Holter & Schwarz-Barcott 1993, Greenwood1994).
Based on practical interests practical knowledge isassumed to allow human beings to understand meaning inthe social world. In tbis type of action research theresearcher and the members of the community identify theproblems together. The causes of the problems and tbeanticipated interventions are planned togetber. Tbe back-ground of this approach is in the historical-hermeneuticsciences (Holter & Scbwarz-Barcott 1993, Greenwood 1994).
Emancipatory knowledge
Emancipatory interests focus on seeking the rationalautonomy of human beings. Emancipatory knowledge isfocused to reveal the extent to which practical understand-ing is systematically distorted by prevailing (sociopolit-ical) conditions. The knowledge is assumed to emancipatehuman agents from distorted values, norms or ideologyand oppression. In action research focused on these eman-cipatory interests the researcher has two goals: to scrutin-ize the problems and theory that explain and assistproblem solving and to help the members of the targetcommunity to identify and clarify the problems by increas-ing the collective consciousness. Tbis means that thedifferences between the theory and the current state ofpractice are exposed, and that the unvwitten rules in thecommunity are also expressed. The purpose is to exposethe values, norms and discrepancies in the community
' 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 801-808 803
K. Hyrkas
which might be the core ofthe problems. The starting pointof this approach is in the critical sciences (Holter &Schwarz-Barcott 1993, Greenwood 1994).
In this action research tbe main idea was to produceknowledge for the members of the target community andthe six project teachers in order to reflect their actions andalso to form the basis for change. This originated in theposition of Kemmis (1985) of the type of reflected knowl-edge and its meaning for change and learning. The datacollection was planned so that the assumptions of loiowl-edge from critical sciences presented by Argyris (1993)were taken into consideration in order to promote cbange.
During the data collection of this action research
1 the ability of human beings to receive and use knowl-edge was taken into consideration;
2 the data collected and the loiowledge gained were con-sidered to be useful botb in assessing tbe objectives ofaction and attaining the objectives. The objectives oftheaction were fixed with the members of the targetcommunity; and
3 the values of the members of tbe target community wererespected while producing the data. The loiowledge wasproduced so that the objectives according to tbemembers of the target community could be attained.
DEVELOPING THE PLANNING OF THECONTENT FOR CLINICAL TEACHING USINGACTION RESEARCH
Background
Developing clinical teaching in the Finnish nursing edu-cation system has been taken for granted by researcbers andalso by tbe National Board of Vocational Education. Themain objectives for development bave been specified as:clarification of the goals of the curriculum (Leino-Kilpi et aL1987, Hokkanen etal. 1994); students' increasing awarenessofthe goals (Leino-Kilpi et al. 1987, Hokkanen ef al. 1987);development ofthe planning ofthe content of clinical teach-ing (Ammattikasvatushallitus 1989, Hokkanen ef al. 1994);development of the methods for clinical teaching (Leino-Kilpi ef al. 1987, Hokkanen ef al. 1994); and developmentof self evaluation and evaluation methods (Leino-Kilpi1991, Holskanen ef al. 1994). All tbese objectives wereassumed in tbis research to be included in the systematicplanning process for clinical teaching, which has beendescribed by White & Ewan (1991).
The first cycle
At the beginning of tbe action researcb in 1992, six nursingteachers from the college of nursing were chosen to runthis project. These six teachers, excluding the projectleader, were responsible during the project for clinical
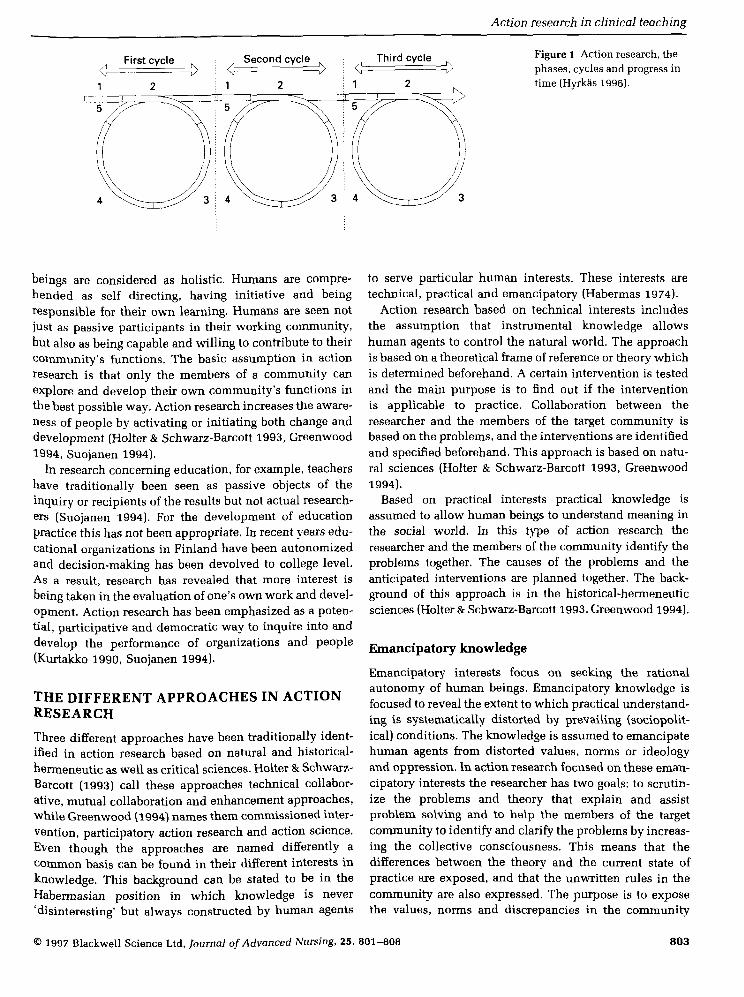
teaching in the eight wards (total of 282 beds) of one hospi-tal. Tbe fundamental change at the beginning was that thetraditional student group-centred way of clinical teachingwas reorganized on a unit-centred basis. Tbis meant inreality that the six nursing teachers from the nursing col-lege were no longer taking care of the clinical teaching oftheir 'own group', but ofall student groups in each clinicalarea. The six nursing teachers had one or two 'wards oftheir own' on which they worked. The student group-centred and unit-centred ways of organizing clinicalteaching are illustrated in Figure 2.
During the first cycle, in the first phase, the aims wereto describe the content of clinical teaching after reorganiz-ing the nursing teachers' work in clinical settings, and toincrease the personal knowledge of these six teachersabout tbeir function, work and related problems. Tbis pro-cess was canied out by asking them to keep diaries duringthe whole spring term in 1992. They were asked to writeabout tbe clinical teaching, problems, solutions andsuggestions for improvement. The mutual collaborationapproach emphasizes that the difference between theoryand reality will be exposed. For this reason the six teacherswere asked to WTite descriptions of planning,implementing and evaluating their clinical teaching. Thistheory or frame of reference was supposed to be the basisfor problem solution and clinical teaching development(White & Ewan 1991).
They also recorded tbe time that they spent clinicalteaching in a time log, the content of clinical teaching wasalso briefiy described. Tbe idea was to use tbis time log inconjunction with the dieiries because it was noted thatpeople kept diaries in tbeir own personal style. Afrerwardsboth the time and content described in the time log andthe description in the diaries could be compared. For tberesearcher this meant that more precise and reliable datawere available.
During the first cycle the pre-test was also accomplished.At tbe end of the spring term. May 1992, questionnaireswere delivered to 149 nursing students (response rate 136of 149 (91%)) and also to 136 qualified nurses in the hospi-tal (response rate 96 of 136 (71%)). The questionnaireswere intended to investigate the initial situation of goalorientation, clinical supervision or studying and evalu-ation. The pre-test revealed the situation for developingthe planning of the content of clinical teaching.
The diaries of the teachers were analysed duringsummer 1992. The content analysis revealed that the plan-ning of the content of clinical teaching was minimal. Thisresult was supported by the results of the analysis of theparallel time log. The six teachers had also reached thesame conclusion by tbemselves. The subject was discussedin the regular monthly meetings which were held through-out the whole project. In addition a meeting was held attbe end of eacb academic term in which the overallprogress was evaluated. One of the six teachers had
804 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 801-808

Action research in clinical teaching
Ward 1
Medical-surgical students
Midwifery students
Health visitor students
Ward 2 Ward 3
Teacher 1 Teacher 2 Teacher 3
Wardi Ward 2 Ward 3
Teacher 1 Teacher 2 Teacher 3
Figure 2 (a) Student group-centred clinical teaching, (b) Unit-centred clinical teaching.
included in her diary suggestions for written plans forclinical teaching. Tbis included an idea about aco-ordinating teacher, who would make the plan for clini-cal teaching with the teacher responsible for tbe theorylessons of the course in the college.
The second cycle
After the evaluation of the results of the first cycle the aimfor the second cycle was set. This was that the design ofthe frame of the written plan for the content of clinicalteaching should commence during the autumn term 1992.The basis for this design work was the diaries of the sixteachers. The problems and suggestions for developmentWere analysed using content analysis. The result of thisanalysis was that the main categories became the titles ofthe frame of the written plan for clinical teaching.
The format of the written plan for clinical teaching wasdiscussed several times during the monthly meetings. Thediscussions also dealt with how the plans should be madeand the planning process with students, nurses and theory
teachers. The aim of the second cycle was set to developthe written plans for clinical teaching for every studentgroup in the hospital, and to start the planning process fordeveloping the planning ofthe content of clinical teaching.
The second cycle started at the beginning of the springterm 1993. First the six project teachers identified theco-ordinators for the student groups. This meant in realitythat every student group had their 'ovwi' co-ordinatingteacher during the period they -weie in the hospital. Forthe project teachers this meant that they had to co-ordinatefrom one to three student groups. The total number of stud-ent groups was 10 and in each group there were from 18to 38 students. Each teacher began to make written plansfor her 'own' groups together with the theory teacher. Thewritten plan for clinical teaching was delivered to theother project teachers and qualified nurses on the wards.Copies of tbis written plan were also distributed to thestudents in the group.
At tbe end of the spring term all the written plans werecollected by the project leader for further analysis. Tbesix project teachers were asked to WTite about their
I 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 801-808 805

K. Hyrkas
experiences, perceived problems and suggestions for furtherdevelopment. An evaluative project meeting was held,which discussed the planning of the content of clinicalteaching, tbe problems involved and suggestions fordevelopment. The planning process was also evaluated.
During summer 1993 tbe written plans for clinical teach-ing were analysed as well as the problems and suggestionsfor development. On tbe basis of this analysis the need todevelop a written plan for clinical teaching was obvious.This was also identified by the six project teachers duringthe spring term evaluation meeting.
The third cycle
The third cycle was the last one in this action research.Tbe aims of this third cycle were: (1) to include the stud-ents and qualified nurses in tbe planning process; (2) todescribe the experiences of the project and the content ofclinical teaching at the end of the project evaluated by thesix project teachers; and (3) to describe the changes in goalorientation, clinical teaching and studying and evaluationaffected by planning ofthe content of clinical teaching andthe written plans for clinical teaching.
During the autumn term 1993 the content planning forclinical teaching continued and the written plans wererepeated. However, the format of the written plan wasrevised according to the suggestions for development atthe end of the second cycle.
During the third cycle the students and nurses on thewards also participated in the planning process. Theco-ordinating project teacher started the planning processfirst with the theory teacher. After this the planning pro-cess was continued with each respective student groupand finally with the nurses on the co-ordinating teacher's'ovm' ward. The written plans were delivered to other pro-ject teachers and to the other wards in the same manneras during the second cycle.
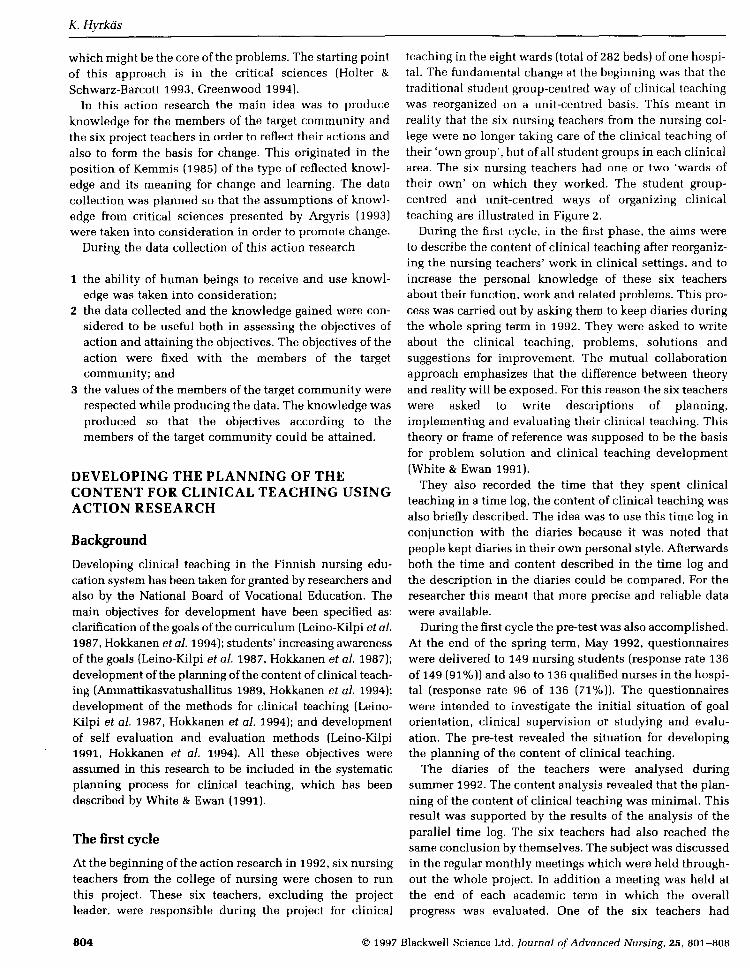
During the autumn term the project teachers again wrotediaries. As this was the last cycle of the action researchthe teachers were asked to describe their work and also toevaluate the changes in their work. The questionnaireswere redistributed at the end of the term to a further 132students and 107 nurses in the hospital. The response rateof students was 106 of 132 (80%) and of nurses 71 of 107(66%). As a summary all the cycles and phases arerepresented in detail in Figure 3.
PROBLEMS WITH RELIABILITY ANDVALIDITY
Action researcb is considered to be a very fiexible strategyfor change. For example, Cohen & Manion (1980) state thataction research is suitable for improving an organizationor renewing systems. It is characteristic of action researchthat its objectives, progress and content can be cbanged
during the research if necessary. It has been stated that inaction research things are examined in tbeir own circum-stances. This means that action research is tied in timeand in the organization in which it has been conducted.
In spite of its flexibility action research has been critic-ized heavily. Tbe criticism has mainly focused on tbe rep-etition ofthe research design, generalization ofthe results,evaluation of the effects of independent variables and alsothe role of the researcher. For example, it has been notedthat the researcher's active role in action research leads tothe evaluation of the researcher's own actions. This alsomeans that tbe objectivity may suffer (Kuitunen 1991).
The reliability and validity have also been criticizedheavily. Kuitunen (1991) examines validity and reliabilityin action research noting that often the only way to getfeedback from the intervention is to take measurements.The main question arises: how well has the researchersolved the problems concerning the measurements?However, in action research the main problem is usuallythe fact that the measurement results are also affected byvariables other than the one measured. This leads todifficulty in evaluating the effects of the intervention.
DISCUSSION
Several problems can be found in this action research. Forexample, one very major problem concerning reliabilityand validity was the inevitable changes in participatinggroups, and also that two of the original six teachers werereplaced during the research (one of the six project teach-ers retired and one leff to continue her own studies). Only51% (n = 71) of the qualified nurses participated in bothpre- and post-tests because of the changes in staff. Studentgroups changed regularly: the student groups in the pre-test were different from those in the post-test.
How could these problems be taken into consideration?Of the teachers' six diaries only four were used by theresearcher in the last cycle of this action research. Theother two diaries from the teachers who joined the projectnear its end had to be rejected because, affer close con-sideration, it was found that these two teachers did nothave the kind of knowledge, experience and understand-ing of the project to enable them to describe the changesin the last cycle of this action research. The drop-outs wereunfortunate as they limited the quality of data available.On the other hand, the other four diaries were writtenaccurately and were very detailed. The number of respon-dents (students and nurses) who did not complete thestudy may also have affected the quality of data.
Reliability
The reliability of the statements in the students' andnurses' questionnaires was checked both in the pre- andpost-tests using the Cronbacb alpha-coefficient. The
806 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 801-808

Action research in clinical teaching
Phase Cycle 1 Cycle 2 Cycle 3
1. Diagnosis of the problem
2. Planning the action
3. Carrying out the plan
4. Evaluation of the results
The content of clinical teachingClinical teaching and supervisionat the beginning of the project(pre-test)
Description of the teachers' workand the use of timeDescription of goal orientation,clinical teaching and supervisionand evaluation
Teachers' diaries and time logQuestionnaires to students and
The profiles of the content ofclinical teaching and the use oftime
5. Identification of the central Shortness of planning of thefindings content of clinical teaching,
the main problem, shortageof time
Problems and suggestions fordevelopment from teachers'diaries
Designing the written plan forclinical teaching
Experimentation of the writtenplans for clinical teaching
Teachers' evaluation of thewritten plans and the planningprocess of the content ofclinical teaching
The need for the developmentof the written plans forclinical teaching
The change in goal orientation,clinical supervision, studyingand evaluation (post-test)
Description of the teachers' workand the use of the timeDescription of goal orientation,clinical teaching and supervisionand evaluation
Teachers' diaries and time logQuestionnaires to students andnurses
Change
Clinical teaching evaluated bythe project teachersThe use of time in clinicalteachingStudents' and nurses' opinionsof goal orientation, clinicalteaching, studying and evaluationChi-square tests of the change
Figure 3 The different phases and cycles in this action research.
reliability was considered good because the coefficientsVaried from 0-675 to 0-832. Because the students were fromdifferent groups in the pre- and post-tests and also only51% of tbe qualified nurses answered both times, this lim-ited the variety available for different statistical methods.However, the methods used were percentage distributions,means, standard deviations and cross tabulations as wellas content analysis and chi-square tests. Log-linear model-ling was also used, which can be considered as an answerto the critique of the problems of generalization andrepetitiveness of the research design.
As mentioned earlier, action research should include atleast two cycles. In this research three cycles were com-pleted. However, the time for developing the planning ofthe content of clinical teaching was too short. It was easyto see, for example, in tbe project teachers' diaries that theactivities were not established in such a short time. Thesame perception was supported by the results of the post-test. Both the students' and nurses' were more uncertainin their opinions of goal orientation, studying, supervisionand evaluation. The increase in uncertainty was minor butvery obvious.
Because the problems in action research are very varied,linked to several levels of action and composed of different'target' communities the results are sometimes very diffi-cult to examine. Action research as a method is also verydemanding. However, there is one very important con-
dition for successful application of action research whichhas to be considered from tbe first to the last cycle.Reliability and validity have to be constantly monitoredthroughout the process in every cycle. The mistakesbecome more significeint the longer the research continuesbecause of tbeir repetition and the way that they can mis-lead the researcher.
CONCLUSION
It is suggested that action reseeirch could be used indeveloping clinical teaching. This study could be con-sidered to be highly relevant to Finland at the momentbecause nursing education has gone through so manychanges in a very short time. The cuiiiculvim content hascheaiged as well as the length of training. However, untilthis study was completed very little attention had beenpaid to the development of clinical teaching even thoughthe importance of this learning experience has been knownfrom beginning of nursing education.
Attention to the quality of clinical teaching in nursingeducation is increasing in Finland. Paradoxically thereason for this is that, in 1994, the nursing colleges startedto pay social and health care organizations for students'clinical placements in hospitals. This payment increasesthe total cost of education per student by approximately10-40%. However, the questions still remain. What is tbe
' 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 801-808 807

K. Hyrkas
quality of the clinical teaching they receive? What will thequality be if only tbe financial aspects are considered andclinical experiences from an educational viewpoint areignored?
References
Ammattikasvatushallitus [National Board of Vocational Edu-cation] (1989) Kaytannollinen opetus terveydenhuoltoalan kou-lutuksessa. Muistio kaytannon opetuksen kehittamiseksi.[Clinical teaching in health care education. Memo ofthe devel-opment for clinical teaching.] Tutkimuksia ja selosteita, no. 19.Ammattikasvatushallitus, Helsinki.
Argyris C. (1993) Knowledge for Action: A Guide to OvercomingBarriers to Organizational Change. Josey-Brass, San Francisco.
Argyris C, Putman R. & McLain Smith D. (1987) Action Science.Concepts. Methods and Skills for Research and Intervention.)osey-Brass, San Francisco.
Bamad A.G. & Dunn S.V. (1994) Issues in the organization andstructure of clinical education for undergraduate nursing pro-grammes. Journal of Nursing Education 33, 420-422.
Carr W. & Kemmis S. (1986) Becoming Critical: Knowing throughAction Research. Deakin University Press, Victoria.
Coates V. & Chambers M. (1990) Developing a system of studentprofiling through action research. Nurse Education Today 10,83-91.
Cohen S. & Manion E. (1980) Research Methods in Education.Croom Helm, London.
Costello J. (1989) Learning from each other: peer teaching andlearning in student nurse training. Nurse Education Today 9.203-206.
Dunn S., Stockhausen L., Thornton R. & Barnard A. (1995) Therelationship between clinical education format and selectedstudent learning outcomes. Journal of Nursing Education34(1), 16-24.
Forthergill-Bourbonnais F. & Smith-Higuchi K. (1995) Selectingclinical learning experiences: an analysis of the factorsinvolved. Journal of Nursing Education 34 (1), 37-41.
Creenwood J. (1994) Action research and action researchers: someintroductory considerations. Contemporary Nurse 3, 84-92.
Habermas J. (1974) Theory and Practice. Heinemann, London.Hokkanen P., Lappalainen M. & Lappalainen S. (1994) Terveyden-
huollon kaytannon opetuksen kehittOmiskokeilu vuosina1990-1993. [Experiment in Developing Clinical Teachingduring the Years 1990-1993.J Opetushallitus [National Boardof Education), Helsinki.
Holter I. & Schwarz-Barcott D. (1993) Action research: what is it?How has it heen used and how can it be used in nursing? Journalof Advanced Nursing 18, 298-304.
Hyrkas K. (1996) KaytanniJn opetuken sisallon suunnittelun kehit-taminen terveydenhuoltoalan koulutuksessa. [Developing theplanning of clinical teaching in healthcare education.)Lisensiaattitutkimus, Tampereen yliopisto, hoitotieteen laitos.
[Unpublished Licentiate thesis. University of Tampere,Department of Nursing Science.[
Jacohson M. (1966) Effective and ineffective behaviour of teachersof nursing as determined hy their students. Nursing Research15, 218-244.
Kemmis S. (1985) Action research and the policies of reflection.In Reflection: Turning Experience into Learning (Boud D.,Keogh R. & Walker D. eds), Kogan, London, pp. 139-163.
Kuitunen K. (1991) Toimintatutkimuksen tulosten arviointi jamittaamisongelmat. [Evaluating the Results of Action Researchand the Problems with Measurement.] Tampereen yliopisto,Yhteiskuntatieteiden tutkimuslaitos, Tyoelaman tutkimus-keskus [University of Tampere, Research Institute for SocialSciences], Tampere.
Kurtakko K. (1990) Toimintatutkimus koulun ja opetuksen kehit-tamisesta. [Action Research in Developing Schools andEducation.] Tutkimusraportteja ja selvityksia 11 [Research andReports 11] Lapin korkeakoulun kasvatustieteellisia julkaisujaB [Publications of the University of Lapland, Department ofEducational Sciences]. Rovaniemi.
Leino-Kilpi H. (1991) Kehittavan opiskelija-arvioinnin kokeiluterveydenhuoltoalalla. [Experiment in developmental studentevaluation in health care.] Loppuraportti 1, yleinen osa.Opetushallituksen julkaisusarja. [Conclusions 1, general part.Publications of the National Board of Education.] Raporttisarja1/1991. Valtion painatuskeskus, Helsinki.
Leino-Kilpi H., Raisanen A., Vaatainen I., Iivonen M-L., Kainua O.,Mehtala L. & Tolonen L. (1987) Terveydenhuollon kaytan-nollisen opetuksen Ja sen arvioinnin kehittaminen palvelujar-jestelmassd. [Developing Clinical Teaching and Evaluation inHealth Care Organization.] Tutkimuksia ja selosteita [Researchand reports] no. 7/87. Ammattikasvatushallitus, Suunnittelu-jakehittOmisosasto [National Board of Vocational Education,Department of Planning and Development], Valtion painatus-keskus, Helsinki.
Opetushallitus [National Board of Education] (1991) Sairaanho-itaja. katiloja terveydenhoitaja. Opetussuunnitelman perusteet.[The Nurse, Midwife and Health Visitor. The National CoreCurriculum.] Opetushallituksen julkaisusarjat, opetussuunnit-elmasarjat 1/1991. VARP-kustannus, Helsinki.
Rapoport (1970) Three dilemmas in action research. HumanRelation 23, 499-513.
Suojanen U. (1994) Toimintatutkimus opettajan tyon kehittajana.[Action research for developing the teacher's work.] In Opetta-jaksi kasvaminen. Turun luokanopettaja koulutuksen linjojenhahmottelua [Professional Growth ofa Teacher] (Tahtinen J. ed)Turun yliopiston kasvatustieteiden tiedekunnan julkaisusarjaB:46, Turku [University of Turku, Department of EducationalSciences[, pp. 129-154.
Titchen A. & Binnie A. (1994) Action research: a strategy fortheory generation and testing. International Journal of NursingStudies 31, 1-12.
White R. & Ewan C. (1991) Clinical Teaching in Nursing. Chapman& Hall, London.
808 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 801-808

Recommended

















