
BOARD OF DIRECTORS MEETING
Wednesday June 30, 2021 1845h – 2015h
OPEN SESSION AGENDA
Board Members: David Pyper (Chair), Nicola Melchers, Denise Smith, Tom Dean, Elaine Habicher, Tim Edworthy, Katie Hamilton, Jody Stecho, Sara Alvarado, Lynn Woeller, Ian Miles, Diane Wilkinson
Ex officio Members: Patrick Gaskin, Stephanie Pearsall, Dr. Asim Masood, Dr. Heather MacLeod, Dr. Vlad Miropolsky
Page 1 of 2
Vision To provide exceptional healthcare by
exceptional people
Mission A progressive acute care hospital and
teaching facility committed to quality and integrated patient centered care
Values
Caring, Respect, Innovation, Collaboration, Accountability
*Agenda Item (* Indicates attachment) (TBC- to be circulated) Page #
Time Responsibility Purpose
1. CALL TO ORDER 1845 D. Pyper 1.1 Land Acknowledgement
Confirmation of Quorum (7) Welcome Guests (Margaret McKinnon and Julia Goyal and Stephanie Pearsall, VP CNE)
Confirmation
1.2 Declarations of Conflict Declaration 1.3 Consent Agenda
(Any Board member may request that any item be removed from this consent agenda and moved to the regular agenda.) 1.3.1 Minutes of May 26, 2021* 1.3.2 CEO Report* 1.3.3 Board Work Plan* 1.3.4 Balanced Scorecard 2021/22*
2 5 11 18
Approval
1.4 Confirmation of Agenda D. Pyper Approval 2. PRESENTATIONS
2.1 Patient Story* 2.2 CMH Wellness and Well-being Program 2021/22* 2.3 Diversity, Equity and Inclusion*
19 22 50
1847 1855 1915
L. Barefoot
T. Clark P. Gaskin
Information Information Information
3. DISCUSSION ITEMS 3.1 Chair’s Report
3.1.1 General Update 3.1.2 Events Calendar*
69
1930
D. Pyper D. Pyper
Information Information
3.2 Resources Committee 3.2.1 Declaration of Compliance Broader Public Sector Accountability Act Attestation (BPSAA) Schedule A*
71
1935
T. Edworthy
Approval
3.3 Quality Committee (June 16, 2021) 3.3.1 Tri-Hospital Research Ethics Board (THREB)
Annual Report 2020/21 and THREB Terms of Reference *
3.3.2 Patient Experience Update* 3.3.3 Patient and Family Council Annual Update* 3.3.4 Trillium Gift of Life Network/Organ Donation Update*
76
93 115 120
1940
I. Miles
Approval
Information Information Information
3.4 Medical Advisory Committee 3.4.1 May 12, 2021 Meeting Summary* 3.4.2 Privileging and Credentialing*
123 127
1955
Dr. A. Masood Dr. A. Masood
Information Approval
3.5 CEO Update 3.5.1 COVID* 3.5.2 Other Matters
• Comparative Statistics on Usage of Employee Family Assistance Program (EFAP)*
132
133
2010 P. Gaskin P. Gaskin
Information Information
4. ADJOURNMENT 2015 D. Pyper Approval
5. DATE OF NEXT MEETING: September 29, 2021

Cambridge Memorial Hospital BOARD OF DIRECTORS MEETING
Wednesday, May 26, 2021 OPEN SESSION
Minutes of the open session of the Board of Directors meeting, held virtually on May 26, 2021 Present:
Mr. D. Pyper Mr. T. Edworthy Mr. I. Miles Mr. T. Dean Ms. E. Habicher Dr. V. Miropolsky Ms. D. Smith Mr. P. Gaskin Ms. D. Wilkinson Ms. S. Hett Ms. N. Melchers Ms. L. Woeller Ms. K. Hamilton
Regrets: Ms. J. Stecho , Ms. S. Alavardo, Dr. H. MacLeod, Dr. A. Masood
Staff Present:
S. Beckhoff, T. Clark Guests: Recorder: Ms. C. Vandervalk P- Present, R – Regrets, T – Present via Teleconference 1. CALL TO ORDER
Mr. Pyper called the meeting to order at 1700 hours.
1.1. Territorial Acknowledgement Mr. Pyper presented the Territorial Acknowledgement.
1.2. Confirmation of Quorum Quorum requirements having been met, the meeting proceeded, as per the agenda.
1.3. Conflict of Interest
Board members were asked to declare any known conflicts of interest regarding this meeting. There being none the meeting continued as per usual.
1.4. Consent Agenda o Minutes of April 28, 2021*
Governance Policies 2-A-08 Board Charter 2-A-12 Executive Committee Charter 2-B-20 Executive Compensation Policy 2-D-02 Board Policy Development, Review and Approval 2-D-10 Guidance for Decision Making Process 2-A-10 Audit Committee Charter 2-A-18 Quality Committee Charter 2-A-30 Responsibilities of Director 2-A-32 Responsibilities of Non Director on Board Committees
o CEO Report*
2

Board of Directors Meeting (Open Session) May 26, 2021 Page 2
o Corporate Scorecard* o Board Work Plan* o Annual CEO Certificate of Compliance*
The consent agenda was approved as circulated.
1.4 Confirmation of Agenda MOTION: (Dean/Edworthy) that, the agenda be approved as circulated CARRIED
2. Presentations
2.1 Diversity, Equity and Inclusion (DEI) Update Ms. Iromoto provided an update on the progress of the DEI Council. The first meeting of the DEI will take place on Thursday May 27 where the survey results including the qualitative comments, from this solicit input from the DEI Council on key DEI Initiatives. The deliverables of the DEI:
1. DEI Governance Model 2. Supports and Enablers 3. Understand organizational data to understand DEI gaps challenges 4. DEI Objectives and Success Metrics 5. Identify and plan a phased roll of out of select DEI initiatives aligned to CMH goals
objectives
2.2 Patient Story CMH Experience with GTA Patient Transfers to CMH during COVID Wave3. During recent critical ICU shortage in Wave 3, thousands of COVID + patients were transferred out of the GTA and Cambridge quickly responded to welcome these patients and made best attempts to manage the anxieties of their families and loved ones. Ms. Barefoot shared a story of a family who had 4 different members in for different hospitals and how this transpired for a family.
3. Discussion Items
3.1 Chair’s Report 3.1.1 General Update The Chair provided an update of his activities of late.
3.1.2 Events calendar The events calendar was reviewed.
3.2 Medical Advisory Committee
This agenda item was moved to the Closed session of the meeting due to Dr. Masood joining later in meeting.
3.3 CEO Update 3.3.1 COVID Update
Mr. Gaskin and Ms.Hett provided an brief overview, and highlighted the following: • Covid assessment clinic has reopened its drive thru • committed to accelerate the 2nd doses of vaccine to our frontline facing staff
3.3.2 CMH Strategic Priorities 2021-22
Circulated for information
4. ADJOUNMENT The meeting adjourned at 1756h. (Edworthy)
3

Board of Directors Meeting (Open Session) May 26, 2021 Page 3
5. DATE OF NEXT MEETING The next scheduled meeting is June 30, 2021 David Pyper Board Director CMH Board of Directors
Patrick Gaskin Board Secretary CMH Board of Directors
4

Page 1 of 6
CMH President & CEO Report July 2021
for CMH (June), CMHF (June), CMHVA (June), MAC (July)
This report provides a brief update on some key activities within CMH. Stories are organized by three strategic pillars and the COVID-19 pandemic. As always, I’m happy to answer questions and discuss issues within this report or other matters.
Prove Patient Matter Most Key priority “accelerate access to care for patients…” description:
• Recap of the goal: o By March 31, 2021 the hospital will seek to accelerate access to care for our
patients by achieving planned PCOP (post-construction operating plan) growth
o Sandra Hett is the executive sponsor for this priority with Nicole Craven and April McCulloch as operational leads
• Key activities and accomplishments this past month include: o The perioperative program continues to ramp up surgical activity and is
planning to be at full capacity by July 12 (subject to the need to continue to support COVID-19 care for our community and Region). There will be a summer closure the week of July 26 to recognize the staff and their efforts supporting other hospital programs throughout the pandemic.
o Elective hip and knee patients having same day surgery will continue to see growth this year creating bed capacity as well as meeting the expectations of patients looking to recover at home rather than having a hospital admission.
o Wait time metrics for cancer surgeries continue to be within target. o Regarding the Medicine Program, there was a pause on any new work
while the team prioritized wave 3 operations. Work underway to start process to reduce beds on MED C towards closure at end of August. This unit was put into place at the request of the Ministry at the beginning of the pandemic.
o The ICU reduced its operation from 22 beds to 17 to maintain capacity relief as per the Provincial Critical Care plan and directives across the
5

Page 2 of 6
system. The ICU is currently experiencing a surge of positive COVID patients due in part to the Delta variant presence in Waterloo Region.
o Redeployed staff have started to return to the OR with a plan to slowly move back as surgical services continue to resume. Planning at the time of this report is to have all staff back to the Perioperative program by mid-July.
o Since April 4, we accepted 20 GTA patients for care in our ICU and Medicine through system leveling process. We continue to operate MED B4 as a second location to complement MED A2 in the care of patients with COVID. No further patients from the GTA to this region have occurred recently. Patient repatriation back to the GTA has been occurring in order to create capacity regionally for new COVID positive patients
Cheryl Livingston joins the Board’s Quality Committee
• Cheryl Livingston, Director of Diagnostic Imaging, joined the Quality Committee of the Board for the staff member position.
• Cheryl replaces Kyle Leslie; who ended his two-year term in June 2021. The staff member is a requirement for hospital quality committees and is described as “a person who works in the hospital who is not a member of the College of Physicians and Surgeons or the College of Nurses”.
• Cheryl joined CMH in 2019. Cheryl has an MBA from the Sandermoen School of Business, University of Fredericton with a specialty in Business Analytics Leadership and is professionally associated with the College of Medical Radiation and Imaging Technologists of Ontario, in Nuclear Medicine. Cheryl is also a Six Sigma Greenbelt.
• While at CMH, Cheryl was involved in several quality achievements such as the implementation of imbedded Ultrasound service in the Emergency Department to reduce ED wait time and improve patient experience, led the first implementation of a Foreign Exam Management solution with SWODIN DI-r to enhance access to comparative imaging exams across LHINs 1-4 for CMH patients and most recently, the execution of Savience, a software solution which provides on-line booking at the COVID Assessment
Increase Joy in work Key priority “keep staff and physicians safe and engaged” description
• Recap of the goal: o CMH will continue to work through its employee engagement strategy and
focus on keeping staff and physicians safe and engaged
6

Page 3 of 6
o The executive sponsors of this priority are Sandra Hett and Trevor Clark with Susan Toth and Kim Siegel as operational leads
• Key activities and accomplishments this past month include: o Three on-site COVID vaccination clinics supported by Grand River
Hospital team for staff and physicians, first dose and expedited second doses have been held. CMH successfully applied to Public Health to hold ongoing COVID vaccination clinics at CMH – the first one was held on June 24
o Development of Wellness/Well-being program o Staff survey closed and results are being reviewed o Employee Engagement Council Meeting on June 22, 2022 o Pride Month awareness o Green day promoted to support Muslim Association of Kitchener Drive by
rally in recognition of the family of 4 killed in the anti-Muslim attack in London Ontario on June 11, 2021
o Indigenous residential school tragedy awareness o Planning to decentralize staff screening and mask exchange on June 23,
2021 o Crucial Conversations facilitated for Mental Health Clerical Staff o Fish! Philosophy facilitated for Food Services staff
“What’s on your mind? Virtual town hall launched
• Regularly scheduled “What’s on your Mind?” (WOYM) virtual town halls were launched in June with the executive leadership team.
• These town halls are intended to provide staff and physicians with updates and give the opportunity to ask leadership questions, share their ideas or to highlight concerns
• The format is simple. Anyone in attendance can type their question into the chat line and someone from the team answers. Or they can send their question to the on-line “WOYM?” forum and it will be posted on their behalf.
• Should one not get answered in a session (FYI - this was not the case on June 15), the question could be deferred to the next town hall or answered through the “WOYM?” forum
• The executive team will trial these town halls on different days and times until a spot that accommodates most staff and physicians is found.
‘Walk a mile’ in your shoes (figuratively)
• It is said that job shadowing gives one an opportunity to learn firsthand what a person’s job looks like and it is an excellent way to learn more about the accountabilities inherent with the role.
• For this purpose, Patrick Gaskin has offered to ‘walk a mile’ with staff over the summer months to observe and learn more about their many responsibilities.
• So far the initiative is going well and he has walked or is scheduled to walk with staff on seven separate occasions
COVID-19: How are we doing? Staff Survey
7

Page 4 of 6
• The fourth installation of the “How Are Ae Doing?” survey was offered at the end of May and closed in June. New to this survey were some wellness questions that will be used to develop a program to support staff wellbeing.
• The results from the surveys were validated by the Employee Engagement Council and CMH management, prior to being shared organization wide.
Wellness & Wellbeing Engagement Specialist to be hired
• The hospital received a generous donation to support our wellness and well-being efforts. With these funds, the hospital is posting a specialist position to help develop and execute tactics in support of the wellness and wellbeing program.
• Work continues on the three-year employee engagement plan using the IHI Joy in Work framework.
• COVID has brought wellness and well-being to the forefront – which is one of the dimensions in the framework.
CMH Staff Trust Fund develops diversity bursary
• The CMH Staff Trust Fund is an independent, self-governing private foundation that is supported solely by CMH staff via payroll deduction. For almost 50 years, it has directed these funds to help local charities in our community.
• For 2021, the CMH Staff Trust Fund is offering an education bursary for the purpose of increasing diversity in health care.
• The bursary is to assist African Canadians, Indigenous people, persons of colour, persons with disabilities and/or people identifying as LGBTQ2S+ in their pursuit of post-secondary education in a health-related discipline. Three bursary awards of $1000 each are available and the application deadline is July 29.
• Besides the bursaries, the Staff Trust Fund supports the United Way of Cambridge (40% of yearly total) and targets a different local charity (30%) on a yearly basis. For 2021, it will be the Cambridge Self Help Food Bank.
“Celebrating you, Celebrating summer” a hit
• Despite the limitations imposed by the pandemic, a creative initiative was made to usher in the summer season.
• In lieu of the popular CMH BBQ, an ice cream truck was brought on site to provide all staff, physicians and volunteers a sweet treat. Prizes were drawn every 15 minutes and announced on the hour between 1300 and 1900 hours.
• Over 700 ice creams were served on June 22 – the first full day of summer.
Lead Boldly
8

Page 5 of 6
Key Priority “meet evolving needs of our community through adaptive execution of CRP Phase 3” description • Recap of the goal:
o The CRP project is starting up again with the complete refurbishment of the Wing B patient care facility. The hospital will deliver the Phase 3 part of this project on-time and on-budget.
o Mike Prociw is the executive sponsor of this priority with Bill Prokopowich as the operational lead
• Key activities and accomplishments this past month: o Construction is progressing well during the first phase of the Diagnostic
Imaging renovation and is unfolding according to schedule o CMH received a revised schedule reflecting most of the impacts from the
efficiencies identified by CRP staff. The schedule now reflects a five-month reduction, updating the planned delay to 192 days instead of 293.
o More gains to the schedule may be had with proposed changes made to the delay linked with temporary exiting and to parts of the DI renovations.
o The closure of Wing B has been pushed out to the end of January 2022. o The Kitchen renovation project is complete. Training is underway with a
planned open house and celebration on Tuesday June 29. The kitchen will go into service on Tuesday July 6.
Key Priority “prepare for clinical transformation though re-initiating our
evaluation of a new HIS system” description • Recap of the goal:
o CMH current Health Information System (HIS) is out of date. By the end of March 2021, the hospital will prepare for digital transformation by reinitiating the evaluation of a new HIS system.
o The reason for this key priority is that the outdated system is creating inefficiencies and the need to seize opportunities to enhance patient care through digital transformation. The hospital is also obligated, through its Ontario Health Team (OHT) partnership to adopt digital tools. Finally, there is a need to improve information management at the hospital.
o Mari Iromoto is the executive sponsor. Prithu Prakash is the operational lead.
• Key activities and accomplishments for this past month include: o Preliminary meetings conducted with Cerner as we expand our evaluation
process. o Plans are in place to reset and relaunch the HIS Evaluation Committee
meetings in July o The recruitment of HIS Project Lead will begin
Food Services introduces B-Lean Food Assembly technology
• As Food Services prepares to receive their brand new kitchen in July, it got a jump on new technology implemented their new B-Lean food assembly system.
9

Page 6 of 6
• The new system takes less space to assemble patient meal trays and is much more efficient and better ergonomically for staff, which improves tray accuracy.
• The bonus is that the assembly no longer needs to be done within a refrigerated area as the unit has its own refrigeration.
• The system has only been implemented for breakfast trays in June. This was purposely done to provide staff with the opportunity to learn and become familiar with this technology before it is used full-time in the new kitchen.
COVID-19 Pandemic Staff and physician screening changes
• The Staff and physician screening program – an early strategy the hospital the hospital used to keep its people safe –changed to a decentralized model on Wednesday June 23. Part of the reason for the change was to make way for the growing CRP project. More importantly, a high number of staff and physicians are double-vaccinated and they have shown a commitment to hand hygiene and wearing PPE.
• The new process provides staff and physicians with the means to do their hand hygiene and swap masks when they get to their unit/department. Furthermore, staff and physicians may screen prior to coming to work or when they log into their computer.
• Based on feedback from staff and physicians, two more staff-only entrances were added to Wing A and C respectively to accommodate Lot #1 and #3 parking. Both can be accessed by card, 24/7. Staff-only entrances are a requirement of the Ministry
Pop-up COVID vaccination clinics a success
• CMH offered first doses to new staff and expedited second doses at its first pop-up clinic on June 2. Another followed the week following and was done in partnership with Grand River Hospital.
• In a CMH first, the hospital offered its first CMH-led clinic on June 24 that was staffed and led by CMH staff.
10

Agenda Item 1.3.3 BOARD WORK PLAN – 2020-21
Page 1 of 7 = Due C = Complete I = In progress D = Delayed 25 June 2021
Charter Section #4
Action (Italics-comments) Committee Responsible
Sept Oct Nov Jan Feb Apr May Jun
Tone at the Top
a-i, ii a-iii
Approve CEO goals and objectives Approve COS goals and objectives
Mid-year CEO assessment input from Board Mid-year COS assessment input from Board
Mid-year/Year-end CEO report and assessment Mid-year/Year-end COS report and assessment CEO evaluation/feedback – mid-year COS evaluation/feedback – mid-year
CEO evaluation/feedback –year end and performance based compensation COS evaluation/feedback –year end and performance based compensation
Executive
Board
Executive
Executive
Executive
C n/a
C C I I I I
I I
√ √ √ √ √ √
Reviewing the performance assessments of the VPs – summary report provided to the Board (as per policy 2-B-10)
Executive √
b Strategic Plan: approve process, participate in development, approve plan
(done in 2017; will be done again in 2018-19) Board
b Progress report on Strategic Plan (2x year Jan for 17-19 plan) Board D
√
b-iii-c Approve annual Quality Improvement Plan (QIP) Quality D
11

Agenda Item 1.3.3 BOARD WORK PLAN – 2020-21
Page 2 of 7 = Due C = Complete I = In progress D = Delayed 25 June 2021
Charter Section #4
Action (Italics-comments) Committee Responsible
Sept Oct Nov Jan Feb Apr May Jun
b-iii-c Review and approve the Hospital Services Accountability Agreement (H-SAA)
Review and approve Multi-Sector Accountability Agreement (MSAA) Review and Approve Community Annual Planning Submission (CAPS) Review and Approve Hospital Accountability Planning Submission (HAPS)
Resources, Quality
D D D
C C C
b-iii-C Monitor performance indicators and progress toward achieving the quality improvement plan
Quality C
C
C
c-i-B c-i-B
Critical incidents report – (as per the Excellent Care for All Act). (Brought forward to Board at each meeting – approved Nov 27, 2019)
Monitor, mitigate, decrease and respond to principal risks
Quality
Audit
C
C
C
C
C
C
C
C
√
c-i-E c-i-F c-i-F c-i-F
Review the functioning of the Corporation, in relation to the objects of the Corporation the Bylaw, Legislation, and the HSAA
Governance
C
C
C
√
Receive and review the Corporate Scorecard
Board
I
C
C
C
C
Declaration of Compliance with M-SAA Schedule G (due Oct 31 and Apr 30 to the WWLHIN)
Resources
C
C
Declaration of Compliance with BPSAA Schedule A (due May 31 to the WWLHIN)
Resources I
√
Receive and review quarterly the CEO certificate of compliance regarding the obligations for payments of salaries, wages, benefits, statutory deductions and financial statements
Resources C
C
C
C
Procedures to monitor and ensure compliance with applicable legislation and regulations
Audit C
CAPS & HAPS not required for 2021/22
12

Agenda Item 1.3.3 BOARD WORK PLAN – 2020-21
Page 3 of 7 = Due C = Complete I = In progress D = Delayed 25 June 2021
Charter Section #4
Action (Italics-comments) Committee Responsible
Sept Oct Nov Jan Feb Apr May Jun
e-i-A
Receive a summary report on: • CEO succession plan and process • COS succession plan and process • Succession plan for executive management and professional staff
leadership
Executive Executive Executive
C C
√
Professional Staff
f-i-A f-i-B/C
Ensure the effectiveness and fairness of the credentialing process Monitor indicators of clinical outcomes, quality of service, patient safety
and achievement of desired outcomes
MAC/Quality
MAC
I
I
I
C
C
C
C
√
f-i-C Make the final appointment, reappointment and privilege decisions for Medical/Professional Staff
Oversee the Medical/Professional Staff through and with the MAC and COS
Board
COS
C
C
C
C
C
C
C
C
C
C
C
C
√ √
Build Relationships
g Build and maintain good relationships with the Corporation’s key stakeholders The Board shall build and maintain good relationships with the
Corporation’s key stakeholders including, without limitation, MOH, Ontario Health, community leaders, patients, employees, families, other health service providers and other key stakeholders, donors and the Cambridge Memorial Hospital Foundation (” Foundation”) and the Cambridge Memorial Hospital Volunteers Association.
Present Annual Volunteer Association Presentation
Board
C
Financial Viability
13

Agenda Item 1.3.3 BOARD WORK PLAN – 2020-21
Page 4 of 7 = Due C = Complete I = In progress D = Delayed 25 June 2021
Charter Section #4
Action (Italics-comments) Committee Responsible
Sept Oct Nov Jan Feb Apr May Jun
h-i-A,C h-i-A,C h-i-A, B h-i-A i-i-C
Review and approve multi-year capital strategy Review and approve multi-year information technology strategy
Resources Resources
C
C
Review and approve annual operating plan – service changes, operating plan, capital plan, salary increases, material amendments to benefit plans, programs and policies
Resources/ Quality
C
C
Approve the year-end financial statements Board C
Approve key financial objectives that support the corporation’s financial needs (including capital allocations and expenditures) (assumptions for following year budget)
Review of management programs to oversee compliance with financial principles and policies
Resources
Resources
I
C
C
Board Effectiveness
i Establish Board Work Plan Board C
i-i-A Ensure Board Members adhere to corporate governance principles and guidelines Declaration of conflict agreement signed by Directors
Governance
√
i-i-B Ensure the Board’s own effectiveness and efficiency, including monitoring the effectiveness of individual Directors and Board officers and employing a process for Board renewal that embraces evaluation and continuous improvement
Governance/ Board
√
i-i-C Ensure compliance with audit and accounting principles Audit C i-i-D
Periodically review and revise governance policies, processes and structures as appropriate
Governance
C
C
C C C C
Fundraising
14
Agenda Item 1.3.3 BOARD WORK PLAN – 2020-21
Page 5 of 7 = Due C = Complete I = In progress D = Delayed 25 June 2021
Charter Section #4
Action (Italics-comments) Committee Responsible
Sept Oct Nov Jan Feb Apr May Jun
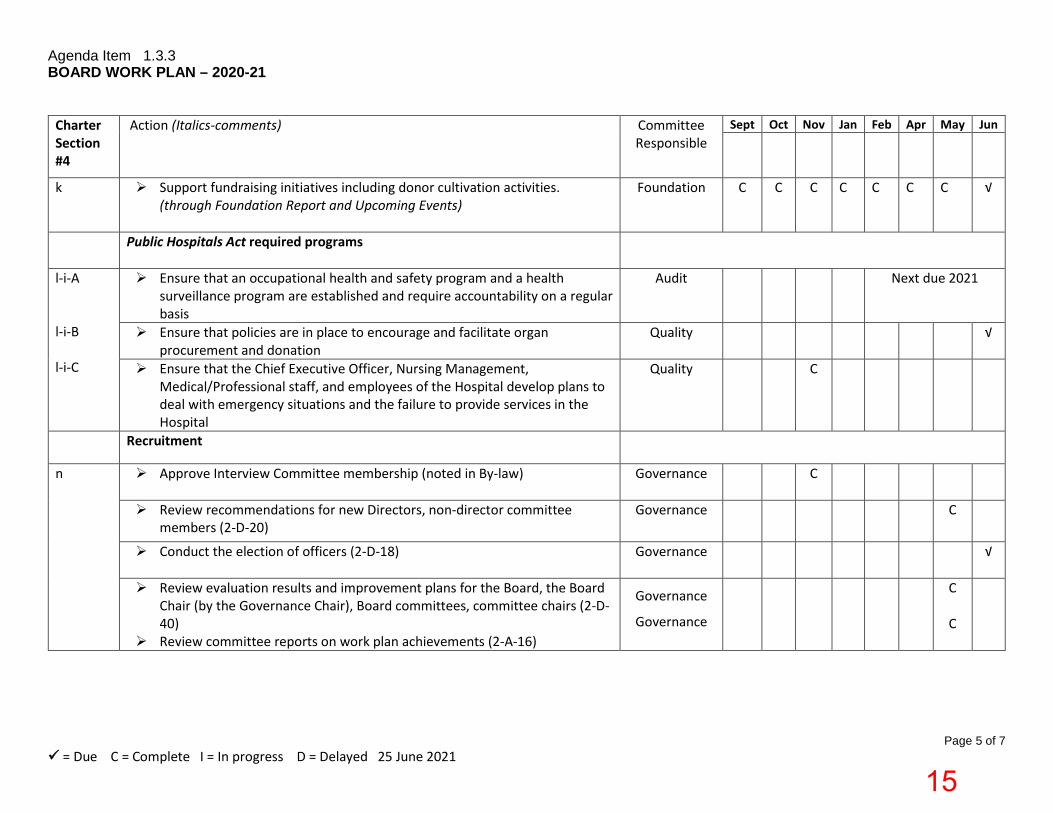
k Support fundraising initiatives including donor cultivation activities. (through Foundation Report and Upcoming Events)
Foundation C
C
C
C C C C √
Public Hospitals Act required programs
l-i-A l-i-B l-i-C
Ensure that an occupational health and safety program and a health surveillance program are established and require accountability on a regular basis
Audit
Next due 2021
Ensure that policies are in place to encourage and facilitate organ procurement and donation
Quality
√
Ensure that the Chief Executive Officer, Nursing Management, Medical/Professional staff, and employees of the Hospital develop plans to deal with emergency situations and the failure to provide services in the Hospital
Quality
C
Recruitment
n
Approve Interview Committee membership (noted in By-law) Governance C
Review recommendations for new Directors, non-director committee members (2-D-20)
Governance
C
Conduct the election of officers (2-D-18) Governance √
Review evaluation results and improvement plans for the Board, the Board Chair (by the Governance Chair), Board committees, committee chairs (2-D-40)
Review committee reports on work plan achievements (2-A-16)
Governance
Governance
C
C
15
Agenda Item 1.3.3 BOARD WORK PLAN – 2020-21
Page 6 of 7 = Due C = Complete I = In progress D = Delayed 25 June 2021
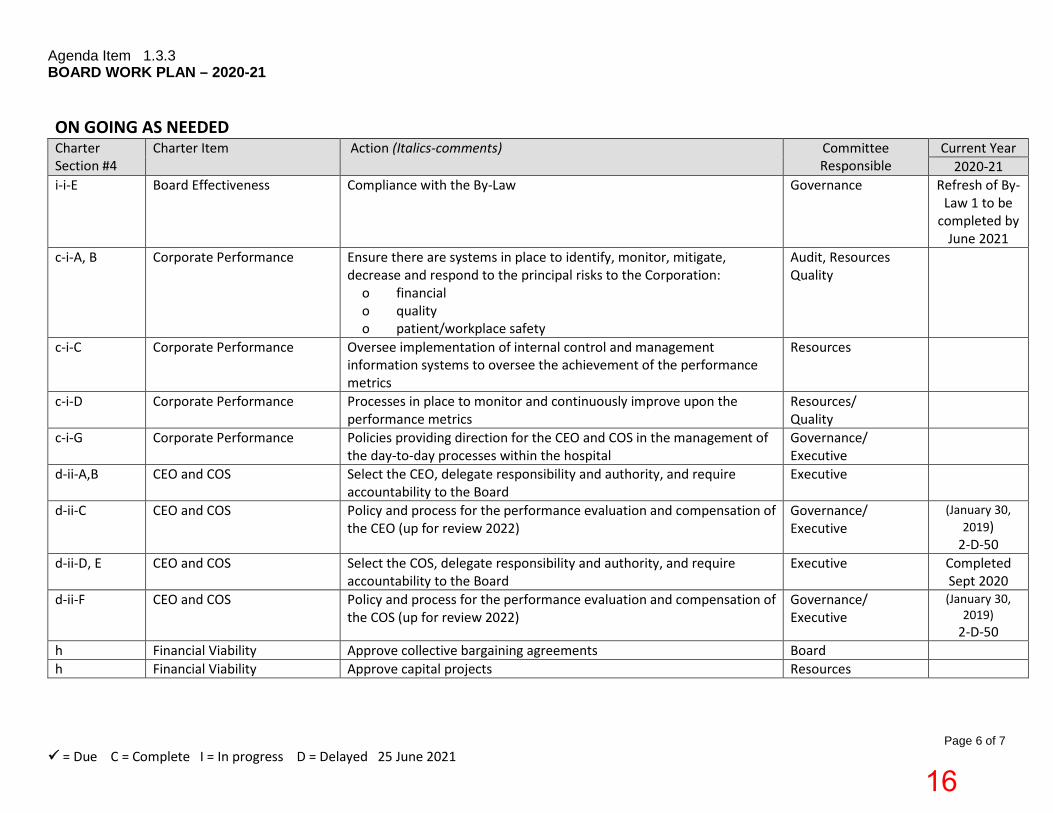
ON GOING AS NEEDED Charter Section #4
Charter Item Action (Italics-comments) Committee Responsible
Current Year 2020-21
i-i-E Board Effectiveness Compliance with the By-Law Governance Refresh of By-Law 1 to be
completed by June 2021
c-i-A, B Corporate Performance Ensure there are systems in place to identify, monitor, mitigate, decrease and respond to the principal risks to the Corporation:
o financial o quality o patient/workplace safety
Audit, Resources Quality
c-i-C
Corporate Performance Oversee implementation of internal control and management information systems to oversee the achievement of the performance metrics
Resources
c-i-D Corporate Performance Processes in place to monitor and continuously improve upon the performance metrics
Resources/ Quality
c-i-G Corporate Performance Policies providing direction for the CEO and COS in the management of the day-to-day processes within the hospital
Governance/ Executive
d-ii-A,B CEO and COS Select the CEO, delegate responsibility and authority, and require accountability to the Board
Executive
d-ii-C CEO and COS Policy and process for the performance evaluation and compensation of the CEO (up for review 2022)
Governance/ Executive
(January 30, 2019)
2-D-50 d-ii-D, E CEO and COS
Select the COS, delegate responsibility and authority, and require accountability to the Board
Executive Completed Sept 2020
d-ii-F CEO and COS Policy and process for the performance evaluation and compensation of the COS (up for review 2022)
Governance/ Executive
(January 30, 2019)
2-D-50 h Financial Viability Approve collective bargaining agreements Board h Financial Viability Approve capital projects Resources
16

Agenda Item 1.3.3 BOARD WORK PLAN – 2020-21
Page 7 of 7 = Due C = Complete I = In progress D = Delayed 25 June 2021
ON GOING AS NEEDED – Led by CEO/COS – reported in CEO report/Quality Presentations Charter Section #4
Charter Item Action (Italics-comments) Committee Responsible
j-i-A Communication and Community Relationships
Establish processes for community engagement to receive public input on material issues
Board oversight Led by CEO
j-i-B Communication and Community Relationships
Promote effective collaboration and engagement between the Corporation and its community, particularly as it relates to organizational planning, mission and vision
Board oversight Led by CEO/COS and Chair
j-i-C Communication and Community Relationships
Work collaboratively with other community agencies and institutions in meeting the healthcare needs of the community
Board oversight Led by CEO/COS Quality
j-i-D Communication and Community Relationships
Maintain information on the website Board oversight Led by CEO
j-i-E Communication and Community Relationships
Establish a communication policy for the Corporation; review periodically (2-D-11 – reviewed April 2019, next review 2022)
Board oversight Led by CEO
m Communications Policy Oversee the maintenance of effective stakeholder relations through the Corporation’s communications policy and programs (updated communication plan (2020-2023) to be approved by Board in 2021)
Board oversight Led by CEO
17

Oversight Committee
Indicators Prior Year Period
Patient Flow - Time To IP bed 90th% tile 15.3 Apr-21Medication Reconciliation at Admit 92.0 May-21Medication Reconciliation at Discharge 92.0 May-21Patient Experience- Enough Information at Discharge 51.3 Apr-21Patient Experience- Would you recommend CMH? 69.6 Apr-21Percent ALC Days (closed cases) 24.4 Apr-21
Hospital Standardized Mortality Ratio (HSMR all cases) 117.2 Feb-21
30 Day Readmission Rate for CHF patients 14.0 Mar-21
30 Day Readmission Rate for COPD patients 12.7 Mar-21
Workplace Violence Reported Incidents 5.5 May-21Overtime Hours (average per pay period) 2,094.3 Jun-21Sick Hours (average per pay period) 2,171.8 Jun-21
Conservable Bed Days (MEDA,MEDB,MEDC) 42.3 Apr-21Quality Based Procedures - Bundled Care Volumes --- ---Quality Based Procedures – Cancer Care Ontario Volumes --- ---Quality Based Procedures – Ministry of Health Volumes --- ---Weighted Cases (All IP Acute + Day Surgery) (average) 1,100.0 Apr-21
Days since last critical patient safety event (Severity level 5/6) 38Days since last incident of workplace violence 6 At Risk
*Includes Closed,In-Progress and New Cases*
Quadruple Aim
Better Care Experience
Joy in Work
Better Health Outcomes
Improved Efficiency
Alignment Unit of Measure
Watch
Watch
Watch Ratio
Watch Hours
Strategic Priority
%
Quality
Resource
Draft CMH Balanced Scorecard, FY2021/2022
YTD
44.4
QIP Hours 11.4 19.0
54.0%Watch
Watch
Watch
Target Status
96.091.0
%
Strategic Priority %
14.0
15.5
16.3
14.5
Strategic Priority Hours 2,344.0 837.0
25.9Watch60.066.7
1,940.0
Forecasted to Achieve
2,353.0
48.2
116.6 100.0
--- ---38.0
Strategic Priority
--- ---
100.0100.0
%
%
%
Strategic Priority --- ---
QIP % 2.5 12.0
% 15.0
Quality
Resource
Forecasted Not to Achieve
Watch
Strategic Priority HIG weight 1,346.0 1,252.0
Updated: June, 2021
18

Visiting at CMH … A Critical Look in the Mirror
Liane Barefoot, Director Patient Experience, Quality & RiskJune 30, 2021
19

“ ““ “
It feels cruel and unnecessary and is inconsistent with science and patient-centred care. I urge you to update your (end of life visiting) policies immediately for my father and other patients like him.
Because she did not meet the definition of ‘imminent end of life’ she did spend the majority of her final days alone, confused and frightened. Unfathomable!!!
Critical look in the Mirror –multidisciplinary with a focus on risk assessment
Some areas where we were doing better than GTA –consensus to hold status quo
End of Life – large variation in our practice – we knew we HAD to do better
Our call to action!
20

While dealing with “wild cards”
• Delta Variant• Waterloo Region numbers• Outbreaks at St. Mary’s and Grand River Hospital
Paradigm ShiftInitial Focus on End of Life
FROM‘imminent end of life’Restrictive policy language
TOLiberal access to …How might we? If we can’t do (xyz) what CAN we offer? Philosophical switch in thinking
21

Staff and PhysicianWellness and Well-being Program
June 2021
22

Wellness – focused on individual –and what they need to do – healthy eating, fitness, sleep, mindfulnessWell-being – focused more broadly to include the organizational responsibilityCMH approach is holistic – looking at wellness and well-being
23

Why is this program a priority?
76% of health care workers reported exhaustion and burnout
48% of care workers have considered retiring, quitting their jobs or changing their careers after the COVID-19 pandemic
39% of health care workers reported that they did not feel that they had adequate emotional support
45% of managers felt well prepared to do their job in 2020
Advisory Board Survey
24

CMH experience is no different
“I am tired and so are my coworkers. I generally love my job here at CMH but have "no reserves" left. The workload is large and fluctuating, with ongoing "pivoting". Ongoing change. All of us with shorter "fuses" and have become much more "reactive". It is difficult to take a day off to rejuvenate given available backfill. So much change and chaos which is stressful, tiring and difficult to integrate.”
Comment from staff/physician survey – June 2021
25

CMH experience is no different
“I have utilized exercise and good eating habits as a way to remain physically well and have made sleep a priority in my routine. I feel stressed, overwhelmed, underproductive, and limited in my abilities to perform my role as I would like to, due to many factors that are out of my control. I work very long hours, and don't have the ability to spend time with friends and family, which normally are important outlets for me. When I am away from work, it is hard to disconnect - due to staffing challenges, and unit acuity issues. I am just doing my best to keep going, and am hoping for relief soon with the COVID situation improving.”
Comment from staff/physician survey – June 202126

CMH experience is no different
“Like everyone, I feel tired and a little burnt out. I miss my family and social events. The last year has added stress and worry to all. For quite some time I felt that I had a handle on this and to focus on positive thoughts and be grateful for all the good. I did not realize that a little sorrow was creeping in and affecting me until a situation occurred, I cried for 3 days, lost sleep etc. By the end of each week, I feel exhausted. We try not to worry and put on a brave face for our teams, each other and most of all family. It takes its toll so we need to be good to ourselves too.”
Comment from staff/physician survey – June 2021
27

ALL STAFF - 'Strongly Agree or Strongly Satisfied' or 'Agree or Somewhat Satisfied' (Q3, 4, 6-12) /
'Positive Impact' or 'No Impact' (Q5) QUESTION JUNE
2021 NOV 2020
JUNE 2020*
APRIL 2020
Number of Respondents 240 359 238 358 Q3 Over the past several weeks, CMH has effectively
communicated at organizational level/Satisfied with our ability to keep you informed
83% 89% 94% 87%
Q4 Over the past several weeks, CMH has effectively communicated at unit/departmental level/Satisfied with our ability to keep you informed
78% 83% 82%
Q5 Over the past months, how has COVID-19 impacted your personal life?
13% 22% 25% 23%
Q6
Overall, I feel safe working at CMH 83% 80% 80% 53%
Q7 I believe CMH has developed a consistent approach to managing the risks associated with COVID-19/CMH is effectively managing the risks associated with COVID-19
84% 84% 80%
Q8 I have access to adequate resources (PPE) and supports to assist me in coping with COVID at work
87% 81% 72% 54%
Q9 I have access to resources I need to support my own health and wellness
79% 78% 79% 51%
Q10 The senior leaders at CMH have demonstrated a commitment to providing a safe and healthy workplace
77% 78% 78% 69%
Q11 The department leaders at CMH have demonstrated a commitment to providing a safe and healthy workplace
84% 81% 80%
Q12 The people I work with are supportive of each other 91% 89% 93% 93%
Staff and Physician Survey Results
Slight decline in effectiveness of communication at both organizational and departmental level
87% of staff negatively impacted by COVID-19
28

Staff and Physician Survey ResultsDrilldown on Well-beingJune 2021
% of staff who rated their well-being on a 5 point scale as either a 4 or 5 (excellent) for the following areas:Physical 55%Spiritual 45%Mental 37%Social/Interpersonal 33%
Overall Well-being 40%
Significant impact of COVID-19 on staff self-assessment of their well-being, particularly mental, social/ interpersonal and overall
How would you rate your well-being in the following areas:
29

CMH’s Aim is to Create a Joy Filled Workplace
“The most joyful, productive, engaged staff feel both physically and psychologically safe, appreciate the meaning and purpose of their work, have some choice and control over their time, experience camaraderie with others at work, and perceive their work life to be fair and equitable.”
30

Improving Joy in Work Framework
31

CMH’s Focus- “Core 4 + 1”
Employee Engagement Strategic Plan 2019-2022 identified four core areas of focus from the framework. 5th component, Wellness and Resilience, has been identified as a program priority Physical and Psychological Safety
Meaning and Purpose
Teamwork and Camaraderie
Choice and Autonomy
Wellness and Resilience32

Program Overview
Based on the Institute for Healthcare Improvement’s (IHI) Framework for Improving Joy in Work, which is one of the hospital’s three strategic pillars
Builds on initiatives identified in the 2019-2022 Employee Engagement Strategic Plan
Initiatives identified in the Employee Engagement Strategic Plan and new tactics are being incorporated into the program
33

Wellness and Well-being Program Goals
To support the organization to realize its vision of helping staff and physicians find joy in work which will improve staff engagement and satisfaction, patient experience, quality of care, patient safety and organizational performance
To facilitate the implementation of initiatives identified in the Employee Engagement Strategic Plan (2019-22)
To provide staff and physicians with opportunities to model organizational values and behaviours
34

Wellness & Well-being Program Goals(cont’d)
To assist the organization to deliver on its promise to address the issues of burnout and fatigue
To improve staff engagement scores that have historically measured low on Accreditation Canada’s WorkLife Pulse Survey results (see next page)
35

Accreditation Canada WorkLife Pulse Survey Results
2019 2017 2015JOBI am given enough time to do what is expected in my job. 51% 51% 45%I am consulted about changes affecting my job. 55% 51% 45%I receive recognition for good work. 62% 54% 49%My supervisor provides feedback on how well I am doing my job. 68% 65% 57%WORK ENVIRONMENTSenior managers effectively communicate the organization’s goals 61% 62% 64%ORGANIZATIONI have good opportunities to develop my career 47% 51% 48%Senior managers are committed to providing high-quality care 59% 56% 58%Senior managers act on staff feedback 38% 38% 38%Senior managers are committed to providing a safe and healthy workplace 56% 57% 53%INDIVIDUAL OUTCOMESI am able to balance my family and personal life work 67% 64% 66%In the last 12 months, would you say that most days at work were…(stress level) 58% 54% 54%Overall, how satisfied are you with your job? 68% 65% 63%ORGANIZATIONAL OUTCOMESHow frequently do you look forward to going to work? 64% 63% 60%Overall, how would you rate your organization as a place to work? 42% 36% 35%
Percentages show the % of staff who responded “Agree” or “Strongly Agree” to the statement 36

Physical and Psychological Safety - defined
Free from physical harm
Feeling secure and capable of changing
Feeling free to express relevant thought and feelings or to speak up about unsafe conditions without retribution
37

Physical and Psychological Safety-Tactics Include:
Provide emotional support in the workplace Conduct staff safety training Open enrollment to leadership development
curriculum
Offer Mental Health First Aid for new leaders (offered by the Mental Health Commission of Canada)
See separate attachment for full list of tactics 38

Meaning and Purpose – defined
Direct line of sight for each person from daily work to the mission, vision and goals of the organization
Constancy of purpose is evident in words and actions of leaders
39

Meaning and Purpose –Tactics Include:
Refresh organizational values statements (CCAIR)
Collaborate at unit level to create value statements
Update Value Based Conversation tool and process
Acknowledge staff/physicians/volunteers through ICCAIR awards – organization wide recognition program
See plan for all tactics 40

Choice and Autonomy – defined
Choice and flexibility in daily lives and work
Some choice in how to execute daily responsibilities
Having a voice in the way things are done in daily work
Part of decision-making on processes, changes, and improvements that affect individuals
41

Choice and Autonomy-Tactics Include:
Formulate rapid improvement initiatives Improve staff scheduling / recruitment Standardize team huddles Conduct staff and physician surveys
See plan for all tactics
42

Camaraderie and Teamwork – defined
Feeling of mutual support and companionship
Working together towards something meaningful
Trust in the organization’s senior leadership
For CMH: The focus for teamwork is across departments and units
43

Camaraderie and Teamwork-Tactics Include:
Update organizational Code of Conduct
Launch Diversity, Equity and Inclusion Council
Standardize supports for celebrating professions
Scheduled senior executive rounding
See plan for all tactics
44

Wellness and Resilience – defined
Taking care of oneself
Facing adversity and becoming stronger
Manage stress effectively
Having access to support systems including mental health support
Finding our work / life balance
45
Wellness and Resilience-Tactics Include:
Provide Employee and Family Assistance Program
Ensure access to vacation time
Introduce Peer to Peer support program
Source a multi-dimensional wellness series
See plan for all tactics
46

Plan Oversight
Employee Engagement Council will provide overall stewardship of program
Medical Professional Staff Association and Operations Committee will be asked to provide input and ongoing feedback
Director, Human Resources is accountable for program
Wellness / Well-being Specialist to be hired to support program implementation
47

Next Steps
Gather input from key stakeholder groups into program
Confirm lead person responsible and implementation timelines for each tactic
Development of communications strategy to disseminate and promote program
Recruitment of Wellness / Well-being Specialist
48

Cambridge Memorial HospitalStaff and Physician Wellness and Well-being Program Overview
Joy in Work: Wellness and Well-being TacticsPhysical and Psychological Safety
* Provide emotional support in the workplace Improve * Availability to CMH ethicist 24/7 Continue* Extend open enrollment to leadership curriculum Improve * Access to online wellness / well-being support resources* Responsive onsite critical incident debriefing Improve * Interactive Town Halls* Offer Mental Health First Aid for leaders Resume * Ready access to Personal Protective Equipment* Develop and disseminate Accessibility Plan Resume * Train and educate on IPAC and HSW standards
* Administration of vaccines (COVID-19, Influenza) * Perform ergonomic assessments, training and education* Conduct staff safety training
Meaning and Purpose
* Refresh organizational values statements (CCAIR) New * Acknowledge through ICCAIR awards- organization wide recognition Continue* Collaborate at unit level to create value statements New * Recognize leaders through ''ATE the Elephant' award* Update Value Based Conversation tool and process Improve * Celebrate career achievement awards* Broaden access to patient feedback boards Improve * Post Thought of the Day and Friday File
* Conduct staff and physician education sessions
Choice and Autonomy
* Improve staff scheduling / recruitment Improve * Conduct staff and physician surveys Continue
* Standardize team huddles Improve * Interactive What's On Your Mind site* Formulate rapid improvement initiatives Improve * Supportive Tuition Assistance program
Camaraderie & Teamwork
* Launch Diversity, Equity and Inclusion Council New * Offer mediation / alternative dispute resolution Continue* Develop Wellness / Well-being Communication Plan New * Plan organizational celebrations / events* Introduce Walk-a-Mile job shadowing New * Promote organizational awareness / acknowledgements* Update organizational Code of Conduct Improve * Leverage Employee Engagement Council* Standardize supports for celebrating professions Improve * Provide access to vacation donation program* Scheduled SMC rounding Resume
Wellness and Resilience
* Introduce Peer to Peer support program New * Promote staff discount program Continue* Source a multi-dimensional wellness series New* Establish private / quiet space for staff New* Adopt facility dog New* Install touchless water refill stations New* Provide Employee and Family Assistance Program Improve* Ensure access to vacation time Improve

49

CMH Diversity PlanYear One: 2021-2022
50

Elevate the understanding of diverseexperiences of staff with the goal to integrateour insights to strengthen the culture andpractices at CMH
DEI efforts are a subset of Wellness & Wellbeing program as part of our ongoing commitment to “Keep staff and physicianssafe and engaged”
Overview2021/22 strategic priority
alignment
Developing a Diversity Plan for CMH has been identified as a corporate priority in 2021
Joy in Work
51

Through consultation with the Diversity Council and rest of organization, we have identified 5 Emerging Priority Themes to focus CMH efforts
Be more deliberate with inclusive languageand images depicted in CMH communications
Provide education and tools to heighten awareness, better understand bias and equip people in their role in allyship
Develop safe spaces to set the right tone for our environments and where staff can turn to when needed
Strengthen/establish processes and policiesto reinforce behaviours and practice
Ensure desired culture is reflected and aligned to our refreshed corporate values
52

“What did we hear?
Why are we doing this?
What will success look like?
Proposed Tactics for Year One:
PRIO
RIT
Y
Inclusive Language“There are no visible symbols of inclusion outwardly visible to the public i.e. Pride/BIPOC inclusivity flag”
CMH wants to be more deliberate with inclusive
language and images depicted in hospital
communications
• IMPROVE responses to: Diversity is reflected across Cambridge Memorial Hospital through visuals, brochures, photographs, art, images, media, signs and symbols
1• Improve use of inclusive language and
images in corporate materials
• Identify and build partnerships with external organizations (vendors, community agencies) who have a commitment to DEI
• Celebrate holidays and events for identity groups by creating and following DEI calendar
53

“What did we hear?
Why are we doing this?
What will success look like?
Proposed Tactics for Year One:
PRIO
RIT
Y
Education and Tools“I think there are some large gaps in terms of people's awareness of the concepts of diversity, equity and inclusion that need to be addressed carefully”
CMH believes it is important to provide education and
tools to heighten awareness, better understand bias and equip people in their role in
allyship
• # of leaders trained in priority education
• IMPROVE responses to: Diversity is reflected across Cambridge Memorial Hospital through appropriate and respectful communications
2• "Cultural awareness training“ – Am I
even aware of how people identify?
• Unconscious bias training – Am I even aware of my own biases?
• Provide allyship training – how can I feel equipped to comfortably approach a situation or interaction to provide support?
54

“What did we hear?
Why are we doing this?
What will success look like?
Proposed Tactics for Year One:
PRIO
RIT
Y
Safe Spaces“Lack of support for staff when being
discriminated against”
“I hear racist and negative gender identity comments in my department
frequently”
“My name continues to be mispronounced – I have given up
correcting people”
CMH wants to develop safe spaces to set the right tone
for our environments and where staff and physicians can turn to when needed
• IMPROVE responses to: Cambridge Memorial Hospital is a safe place for me and others to express racial, cultural, ethnic, gender, first language, religious, sexual, ability, or other identity differences
3• Provide tools to guide safe discussion in
meetings and interactions• Create online site for DEI on hospital
intranet (or MS Teams) with repository of key tools and materials for easy access
• Invite people to share their lived experiences on history, cultural observances to raise awareness and seek understanding of history/experiences of the broader community
• Explore creating Ombudsperson role
55

“What did we hear?
Why are we doing this?
What will success look like?
Proposed Tactics for Year One:
PRIO
RIT
Y Key Processes and Policies“One or two people in a department
with these views cause divides and influence greatly”
CMH wants to strengthen/establish
processes and policies to reinforce behaviours and
practice
• IMPROVE responses to: Diversity is reflected across CMH through representation of staff across different levels of the organization and different departments
• LOWER responses to: Do you have any concerns related to fair hiring practices, or process for movement within or upwards at CMH?
4• Be more deliberate in creating diverse
recruitment panels
• Explore a buddy/mentorship program for newhires
• Use exit surveys/interviews to identify if influenced by discrimination or non-inclusive environment
56

“What did we hear?
Why are we doing this?
What will success look like?
Proposed Tactics for Year One:
PRIO
RIT
Y
Corporate Values• I was completely disregarded and
disrespected
CMH want to ensure desired culture is reflected and aligned to our refreshed
corporate values
• IMPROVE responses to: Diversity is reflected across Cambridge Memorial Hospital through policies and procedures, e-learning
5• Establish and promote an active
Diversity Council
• Integrate inclusion into the leader competency framework
• Ensure workplace policies are free from bias
57

Next Steps• Continue to validate the emerging themes with
hospital• Continue to identify and validate success metrics• Conduct deeper dive on priority tactics with SMC
Directors at June 29th Directors Council meeting• Share our draft DEI plan to hospital and Board by
June 30th
58

Agenda Item 3.2.1
Page 1 of 2 May 2021
Date: May 19, 2021 Issue: Broader Public Sector Accountability Act Attestation Prepared for: Resources Committee Purpose: ☒ Approval ☐ Discussion ☐ Information Prepared by: Ernie Sersen, Director, Finance Approved by: Trevor Clark, VP Finance and Corporate Services and CFO Attachments/Related Documents: Hospital Report on Consultant Use Appendix C – Broader Public Sector Accountability Act Attestation Schedule A to Appendix C Alignment with CMH Priorities
2021-22 Strategic Plan
No ☒
2021-22 Integrated Risk Management Priorities
No ☒
2021-22 Priorities
No ☒ ☐ Prove Patients Matter Most ☐ Staff and Physician Wellbeing ☐ Accelerating Access to Care ☐ Increase Joy in Work ☐ Length of Stay ☐ Keeping Staff and Physicians Safe and Engaged ☐ Lead Boldly ☐ CRP Phase 3 ☐ Executing CRP Phase 3 ☐ Multi-year Fiscal & Capital Strategy ☐ Completing our HIS Evaluation
Recommendation/Motion That the Resources Committee recommends to the Board approval of the Hospital Report on Consultant Use and attestation prepared by the President and CEO in accordance with section 15 of the Broader Public Sector Accountability Act 2010 (BPSAA) for the period April 1, 2020 to March 31, 2021. Executive Summary Upon the review of consulting expenditures incurred during the fiscal year, it was concluded that Cambridge Memorial Hospital appropriately followed the requirements of the Broader Public Sector Accountability Act. Background All transactions allocated to consultant fees and professional fees for the fiscal year ending March 31, 2021 were reviewed to determine if they complied with the BPSA guidelines. In order to determine if the expenditure was a consulting expenditure the following definition was used: “consultant means a person or entity that under an agreement, other than an employment agreement, provides expert or strategic advice and related services for consideration and decision–making.”
BRIEFING NOTE
71

Agenda Item 3.2.1
Page 2 of 2 May 2021
As part of the accountability requirements from the BPSAA, the hospital is required to prepare the attached report concerning the use of consultants, using a prescribed template. The Board is required to approve this report and attestation. Analysis The attached Hospital Report on Consultant Use lists consulting expenditures incurred during the 2020/21 fiscal year. No issues were identified as part of the review.
72

Hospital Report on Consultant Use
Name of Hospital: Cambridge Memorial Hospital
NAME OF LHIN: Waterloo Wellington LHIN
REPORTING PERIOD: April 1, 2020 to March 31, 2021
No. Consultant Firm Name
Name and Title of Consulting Contract
Contract Term
(If the contract term has been extended please
include the original contract term and the
amended contract term)
Procurement Value (A+B+C)
A=Original Value
B=Value of Amendments C=Total Procurement
Value
Total Paid ($)
Consultant Selection Process (Open
Competitive, Invitational Competitive, Non-
competitive – If non-competitive explanation
required
Modifications to Agreement (if yes, did
the procurement documents permit
modifications to the term or value of the agreement?)
1 Korn Ferry Hay Group Ltd
Compensation review The contract term was based on a fixed output
$ 2,740 The contract went through a RFP process.
No modifications
2 Promeus Recruitment of executive team
The contract term was based on a fixed output
$ 25,812 The contract went through a RFP process.
No modifications
3 Tegria Services Group-Can, Inc.
MEDITECH Expanse review
The contract term was based on a fixed output
$ 50,945 The contract went through a RFQ process.
No modifications
73

2
No. Consultant Firm Name
Name and Title of Consulting Contract
Contract Term
(If the contract term has been extended please
include the original contract term and the
amended contract term)
Procurement Value (A+B+C)
A=Original Value
B=Value of Amendments C=Total Procurement
Value
Total Paid ($)
Consultant Selection Process (Open
Competitive, Invitational Competitive, Non-
competitive – If non-competitive explanation
required
Modifications to Agreement (if yes, did
the procurement documents permit
modifications to the term or value of the agreement?)
4 Benard & Associates Six clinical investigations The contract term was based on a fixed output
$ 37,406 The contract was non-competitive / limited tendering based on the knowledge and subject matter of the deliverable.
No modifications
5 Stantec Architecture Ltd. Phase 2 accessibility review
The contract term was based on a fixed output.
$ 10,189 The contract went through a RFQ process
No modifications
6 Aera Corporation Assistance with cogeneration plant implementation issues
Contract based on defined deliverables within prescribed time lines.
$ 61,656 The contract was non-competitive / limited tendering based on the knowledge and subject matter of the deliverable.
No modification
7 Hays Specialist Recruitment
Clinical recruitment Contract based on defined deliverables within prescribed time lines.
$ 10,189 The contract was non-competitive / limited tendering based on the
No modification
74
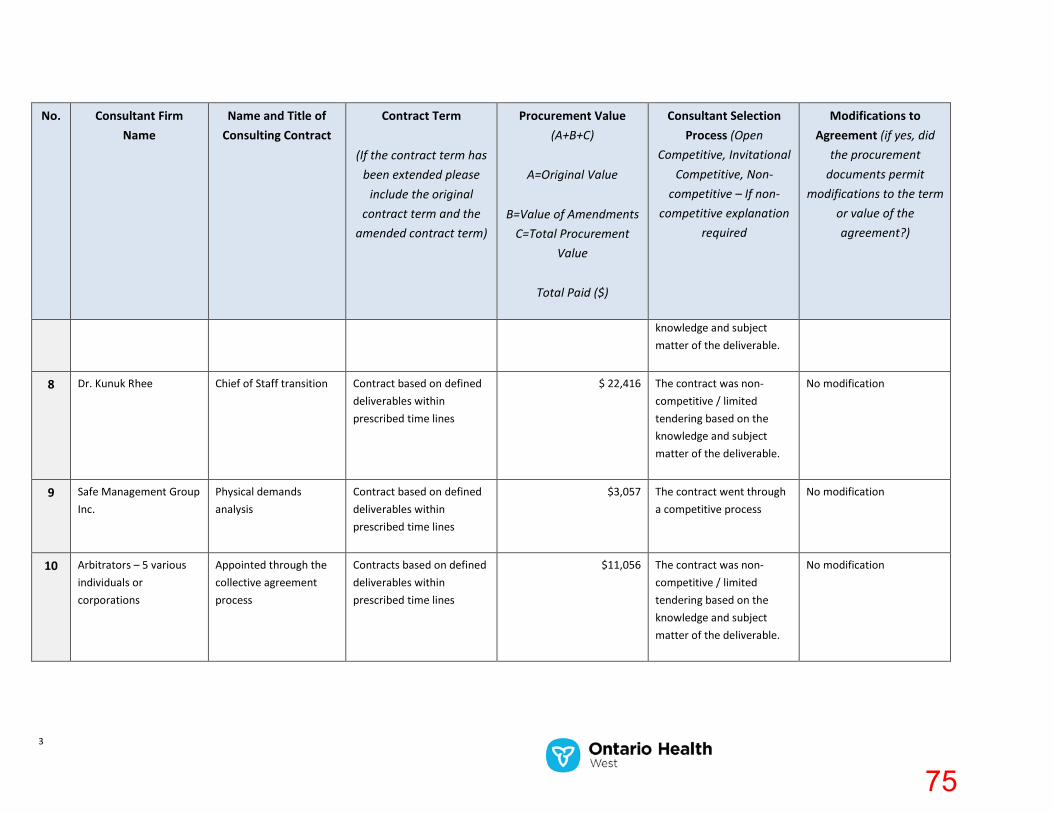
3
No. Consultant Firm Name
Name and Title of Consulting Contract
Contract Term
(If the contract term has been extended please
include the original contract term and the
amended contract term)
Procurement Value (A+B+C)
A=Original Value
B=Value of Amendments C=Total Procurement
Value
Total Paid ($)
Consultant Selection Process (Open
Competitive, Invitational Competitive, Non-
competitive – If non-competitive explanation
required
Modifications to Agreement (if yes, did
the procurement documents permit
modifications to the term or value of the agreement?)
knowledge and subject matter of the deliverable.
8 Dr. Kunuk Rhee Chief of Staff transition Contract based on defined deliverables within prescribed time lines
$ 22,416 The contract was non-competitive / limited tendering based on the knowledge and subject matter of the deliverable.
No modification
9 Safe Management Group Inc.
Physical demands analysis
Contract based on defined deliverables within prescribed time lines
$3,057 The contract went through a competitive process
No modification
10 Arbitrators – 5 various individuals or corporations
Appointed through the collective agreement process
Contracts based on defined deliverables within prescribed time lines
$11,056 The contract was non-competitive / limited tendering based on the knowledge and subject matter of the deliverable.
No modification
75

Agenda Item 3.3.1
Page 1 of 3 May 2021(2)
Date: June 16, 2021 Issue: Quality Committee, June 16, 2021 Prepared for: Board of Directors – OPEN Purpose: ☒ Approval ☐ Discussion ☒ Information ☐ Seeking Direction Prepared by: Iris Anderson, Administrative Assistant, Clinical Programs Approved by: Sandra Hett, Vice President of Clinical Programs & CNE
Attachments/Related Documents: • THREB Annual Report 2020/21 and THREB Terms of Reference Program• Patient Experience update• Patient Family Advisory Council update• Trillium Gift of Life Network/Organ Donation update
Presentation: Pharmacy (Found in Package 2)
Alignment with CMH Priorities
2021-22 Strategic Plan
No ☐
2021-22 Integrated Risk Management Priorities
No ☐
2021-22 Priorities
No ☐☒ Prove Patients Matter Most ☒ Staff and Physician Wellbeing ☐ Accelerating Access to Care☒ Increase Joy in Work ☐ Length of Stay ☒ Keeping Staff and Physicians Safe and Engaged ☒ Lead Boldly ☐ CRP Phase 3 ☐ Executing CRP Phase 3
☐ Multi-year Fiscal & Capital Strategy ☐ Completing our HIS Evaluation
Items for Board Approval
PROPOSED MOTION: That the Board of Directors approves the THREB Annual Report for 2020/21 and THREB Terms of Reference, as presented.
Tri-Hospital Research Ethics Board: THREB Annual Report for 2020/21 and THREB Terms of Reference Ms. Hett reported that Dr. M. Coughlin, who has supported THREB since 2005 has recently retired, and will be replaced by Dr. A. Williams.
Ms. Hett will be retiring on June 30, 2021, and Ms. J. Ropotyn, CMH Professional Practice Specialist, will assume the role of CMH THREB Administrative Lead.
MOTION: (Adair/Ostofe) that, the Quality Committee recommends to the Board of Directors the approval of the THREB Annual Report for 2020/21 and THREB Terms of Reference, as presented. CARRIED
The above will be brought forward to the Board of Directors to approve the THREB Annual Report for 2020/21 and THREB Terms of Reference, as presented.
BRIEFING NOTE
76

Page 2 of 3 May 2021(2)
Items for Board Information
Pharmacy Ms. Visocchi, Director of Pharmacy, and Mr. T. Clark, Vice President of Finance & Corporate Services, joined the meeting at 0705h. Ms. Hett introduced the guests to the Committee members.
As highlighted in the pre-circulated presentation, Ms. Visocchi noted the following: • Supporting the COVID-19 pandemic:
o Pharmacy staff – role in the regional vaccine clinicso Worked collaboratively with all the regional hospitals in the set-up of vaccine
clinics, management of vaccine supplies, and storage of drugso Regional COVID Vaccine Clinic administers over 2000 doses a dayo Supporting bed expansion and patient moves throughout the pandemico COVID medication therapieso CMH recently hosted in-house pop-up vaccine clinic to staff and physicians
• Ontario College of Pharmacists – next inspection date is November 2021o Focus will be on non-sterile compounding procedures, narcotic procedures and
safety, and staff assessments• Sustained Medication Reconciliation in absence of HIS• The Omnicell cabinets will be upgraded in the Fall 2021 (17 cabinets)
The floor was opened to questions and comments.
Ms. Visocchi reported there are no vacancies in the department. Pharmacy has a full complement of staff. All new employees go through a robust on-boarding process to help them understand CMH nuances. Each new pharmacist will work with the physicians and oriented in every clinical unit to learn/manage all types of patients.
In response to a question, Ms. Visocchi shared her concern of increased volumes of patients in Medical Day Care and chemotherapy. As displayed in the pre-circulated report, the trend line on Drug Administered graph illustrates an increase in the number of drugs (mixtures) due to more complicated chemo therapies.
A short discussion took place regarding the benefits of the closed loop medication system that is only possible with a new HIS.
The Committee members provided positive feedback of the pre-viewed program video, and Mr. Beckhoff was acknowledged as the videographer.
Patient Experience – update As per the previously circulated presentation, Ms. Ottman highlighted the following:
• Over the course of the pandemic, CMH has had periods of complete lockdown tovisitors, other than for End of Life patients
• CMH yielding 32 virtual visits a day, weekly• Management conducts a weekly review of visitor restrictions• iPads in circulation to meeting virtual visits needs• Will continue with virtual visits post pandemic• Complaints received are linked to visitor restrictions and communication challenges
related to COVID
77

Page 3 of 3 May 2021(2)
Patient Family Advisory Council – update In reference to the pre-circulated briefing note, Ms. Kimpson presented some highlights of PFAC activities and discussions for 2020/21.
Management has engaged PFAC to share in its organizational priorities. PFAC agendas are now structured and aligned with its Strategic Priorities: 1) Digital Health, 2), Diversity, Equity and Inclusion, and 3) Eyes and Ears of the Community.
Ms. Barefoot noted that a temporary role of Community Ambassador was created. Ms. Kimpson assumed the role and assisted CMH on a daily basis focusing exclusively on COVID (from March 2020 to Mach 2021).
Trillium Gift of Life Network/Organ Donation – update The Committee members were directed to the previously circulated briefing note and TGLN performance data. No discussion took place.
78

Page 1 of 2 May 2021(2)
Date: June 7, 2021 Issue: Annual Review of Tri-Hospital Research Ethics Board (THREB) Annual Report and Terms of Reference Prepared for: Quality Committee Purpose: ☒ Approval ☐ Discussion ☐ Information ☐ Seeking Direction Prepared by: Sandra Hett, Vice President Clinical Programs & CNE Approved by: Patrick Gaskin, President & CEO Attachments/Related Documents: Appendix 1: THREB Terms of Reference Appendix 2: 2020/21 THREB Annual Report Appendix 3: Resume of Dr. Alison Williams Alignment with CMH Priorities
2021-22 Strategic Plan
No ☐
2021-22 Integrated Risk Management Priorities
No ☐
2021-22 Priorities
No ☐ ☒ Prove Patients Matter Most ☐ Staff and Physician Wellbeing ☐ Accelerating Access to Care ☐ Increase Joy in Work ☐ Length of Stay ☐ Keeping Staff and Physicians Safe and Engaged ☐ Lead Boldly ☐ CRP Phase 3 ☐ Executing CRP Phase 3 ☐ Multi-year Fiscal & Capital Strategy ☐ Completing our HIS Evaluation
Proposed motion, that the Quality Committee recommends the THREB Annual Report as presented and terms of reference be forwarded to the Board for approval.
Background In order for hospitals to create an environment that supports research, a well-functioning research and ethics board is essential. Accreditation Canada standards, Health Canada Regulations, Tri- Council Policy Statement (TCPS2) dictate the requirement for a properly constituted research board of record.
Cambridge Memorial Hospital joined the existing Waterloo Region hospital research and ethics board in 2001 which then evolved to the Tri-Hospital Research Ethics Board (THREB). The terms of reference document 3 members per organization. Sandra Hett, Vice President Clinical Programs & CNE is the CMH THREB member until her retirement in June 2021 and Julia Ropotyn, Professional Practice Specialist will assume this role starting July 2021. Recruitment for a CMH physician replacement has been unsuccessful to date, however will continue to pursue this goal and at this time there is physician representation from GRH. The membership numbers per organization have varied over the years and the collective goal is to ensure clinical perspectives (physician, pharmacist etc.) vs absolute membership numbers.
BRIEFING NOTE
79

Page 2 of 2 May 2021(2)
The THREB terms of reference are reviewed and approved by the participating hospital boards on an annual basis. In accordance with the terms of reference, there is an annual summary report produced. Of note the Chairperson, Dr. Michael Coughlin who has supported THREB since 2005 retired in June 2021 and was replaced by Dr. Alison Williams (see resume attached, Appendix 3). You will see by this resume that she is extremely well qualified with significant relevant experience. She was able to join the June meeting (Dr. Coughlin’s final meeting) and her participation validated that THREB will be well served during her term. As a reminder S. Hett was on the THREB chair interview panel as well as member of the CMH PFAC representing this perspective on behalf of all three hospitals. At CMH, the QC has the accountability to review the annual report (see Appendix 1), the terms of reference (see Appendix 2) and provide a recommendation to the CMH board for approval. The Annual Report was reviewed and finalized by THREB (June 2021) as presented. The Terms of Reference have been reviewed by THREB (June 2021) with no changes
80

THREB Annual Report 2020/2021
TRI‐HOSPITAL RESEARCH ETHICS BOARD
ANNUAL REPORT for 2020/2021
To THREB Members and
Board of Directors of Cambridge Memorial Hospital
Board of Directors of Grand River Hospital
Board of Trustees of St. Mary’s General Hospital
(Submitted by Michael D. Coughlin, Ph.D., Chair of THREB)
Overview: This past year has been one of changes and challenges, the “Year of COVID‐19.” The lastin‐person meeting of the THREB was in April of 2020. Most of the work has changed to now being done
electronically: by email, by Zoom and by digital documents. Most of the research is and has been quite
understandably focused on projects dealing with COVID‐related issues. There has been a turnover in
membership, and the THREB will be welcoming a new Chair. As I retire as Chair, I want to express my
gratitude to the hospitals for their involvement and support over the years for the THREB.
1. Introduction
For the hospitals to create an environment conducive to well‐conducted research it is important to have
a well‐functioning and well‐respected Research Ethics Board (REB). To comply with Accreditation
Standards, Health Canada Regulations, the Tri‐Council Policy Statement (TCPS2), standards of practice
and laws around research in general, research done at hospitals in Canada must be approved by a
properly constituted REB authorized by the hospital corporation, that is, an "REB of Record" for the
institution. Prior to 1998, Grand River Hospital (GRH) had its own research review committee
(Committee on Ethical Research). In 1998 a Joint Research Ethics Committee (JREC) was approved by the
Board of Directors of GRH and the Board of Trustees of St. Mary’s General Hospital (SMGH). It was
initially chaired by Terry Dean from Pharmacy at GRH and then by Nancy Martin from Research and
Performance Metrics. In 2001, Cambridge Memorial Hospital (CMH) requested to become part of the
REB and JREC became the Tri‐Hospital Research Ethics Board (THREB). At the time, this was an
innovative model in Ontario for doing research ethics review at community hospitals and has been
emulated by other hospitals. Since 2005, the THREB has been chaired by Michael Coughlin. This year the
THREB will welcome a new Chair, Alison Williams. At GRH and CMH, other Research Ethics Boards such
as the Ontario Cancer Research Ethics Board have been added as "REB of Record", primarily for multi‐
centre cancer studies. In addition, all three hospitals also have agreements with Clinical Trials Ontario
(CTO), which can assign a CTO‐approved REB as “REB of Record” for certain multi‐centre studies.
In brief, THREB is a shared resource of the three hospitals, GRH, SMGH and CMH, and reports to the
Boards of all three hospitals through an administrative liaison person, i.e. a VP or Senior Administrator
from each of the hospitals who sits as a member on the THREB. These administrators are voting
members of THREB and attend the monthly meetings. In addition, these administrators take on the role
1
81

THREB Annual Report 2020/2021
of ensuring that all research that is to be done at their respective hospitals has administrative approval,
i.e. that the financial, resource, privacy and contract issues have been attended to.
All hospitals contribute to support THREB, with equal yearly contributions from each hospital. Some
supplementary support can come from fees charged for industry‐sponsored research. GRH supplies the
THREB with office space, some operating equipment, IT support, and web‐hosting. SMGH has taken on
the role of providing financial administration of the THREB budget. While THREB has its own budget, for
accountability purposes THREB reports to the SMGH liaison person for financial and administrative
matters.
Monthly meetings of the full THREB have usually rotated through the three hospitals, but more recently
have been held as Zoom meetings due to COVID‐19 restrictions.
The Tri‐Hospital Research Ethics Board operates in compliance with the Tri‐Council Policy Statement:
Ethical Conduct for Research Involving Humans [TCPS2 (2018)], the ICH Good Clinical Practice
Guidelines, Division 5 Health Canada Food and Drug Regulations and other applicable regulations.
2. THREB Office
The THREB office consists of an Administrative Coordinator, currently Shelley Croth, paid as a contract
position (2 days per week) and the Chair, Michael D. Coughlin Ph.D., who receives a consultant fee
currently based on a set time of 20 hours per month. As of July 2021 the new Chair will be Alison
Williams, Ph.D. The budget report for 2020/2021 is included in this document.
3. Membership
The membership of the THREB is, according to the Terms of Reference, set up to comply with the TCPS2
requirements and is intended to include at least three members from each hospital, two community
members and the Chair. A continuing challenge for all REBs, and even more so for a community hospital‐
based REB like THREB, is to recruit the necessary mix of members. Despite the turnover of a number of
members and the need still to fill 3 positions, the membership nevertheless nearly fulfills the
requirements of the terms of reference. After a nearly 2 year search for a representative from the area
of pharmacy, that position was taken on by Keith Miller. Robert Howe was replaced by Kevin Stinson.
Unfortunately, two of the three physician members have left the THREB and we will need to actively
recruit for those positions. Of special note, Dr. Ed Chouinard from CMH served on the THREB for 15
years until he retired from practice. The membership for the 2020‐2021 years (with changes noted) has
been:
COUGHLIN, Michael, PhD To June 2021 Outgoing Chair, Ethics
Williams, Alison, PhD From June 2021 Incoming Chair, Ethics
CHOUINARD, Edmond, MD To June 2020
2005‐2020
Medicine, CMH
2
82

THREB Annual Report 2020/2021
FERGUSON, Sherri, CHRL Administration, SMGH
GIROLAMETTO, Carla, MA, CCRP, MSc Administration, Clinical Trials, GRH
HETT, Sandra, BScN, MN To June 2021 Administration, CMH
ROPOTYN, Julia, BScN, MScHSEd From June 2021 Administration, CMH
HOWE, Robert, MBA To Feb, 2021 Performance Improvement, SMGH
LEE, Young , MBA, CMA, BSc(OT) To Jan 2021 Administration, GRH
MILLER, Keith, PharmD From June,
2020
Pharmacy,, GRH
NAYIAGER, Trishana, MSc(HRM), CCRA Community Member, Research methods
STAHLKE, Amy, LLB Community Member, Law, Privacy
STINSON, Kevin, PhD From Feb, 2021 Infectious Disease, SMGH
WASSEF, Anthony, MD Cardiology, SMGH
4. Professional Development of Members
Up until recently, the first part of most THREB meetings was devoted to an educational component,
often a discussion of articles in the journal Ethics and Human Research from the Hastings Center. THREB
had an institutional subscription to the journal with access for every THREB member. With the change in
the way the journal was distributed, it appears we may not have re‐subscribed. Alternatively, other
issues of research ethics review or REB development are discussed.
One of the ways through which REB members across the country share and develop their knowledge,
practices and new policies is through participation in the annual conference of the Canadian Association
of Research Ethics Boards (CAREB). The CAREB conference includes updates and new developments not
only for the Canadian context but also from the U.S. research ethics review organizations that often
have an impact on Canadian practice. THREB attempts to send some members to the conference each
year (depending on the budget) to allow members to get a sense of the national scope of research ethics
and to bring back any new developments. Due to COVID‐19 restrictions, the 2020 CAREB conference
was canceled. The 2021 CAREB conference was held virtually and 3 THREB members attended at least
parts of the meeting.
3
83

THREB Annual Report 2020/2021
5. Statistics on Projects Reviewed
NOTE: For historical reasons of study numbering, the statistics on research studies are based on the
calendar year. To coordinate with the hospital budget year, the THREB budget information is based on
the April‐March fiscal year.
During the 2020 calendar year, THREB received a total of 29 new studies and carried out a total of 139
reviews, including 28 new studies (one had been withdrawn after submission), and the monitoring of a
total of 92 ongoing studies. Beginning in March of 2020 the THREB received a significant number of
studies around various aspects of COVID‐19. Actually, most of the studies in 2020 understandably
revolved around COVID‐19. The THREB office also responds to inquiries regarding the determination of
whether studies were to be considered research or quality initiatives. Since some of the projects involve
two or more of the hospitals, the sums for the new and ongoing studies will be greater than the number
indicated above. This year, one study involved all three hospitals and 11 others were joint GRH/SMGH studies.
New and Ongoing Studies
by Hospital 2020
0
50
100
CMH GRH SMGH
New Industry New Other Total Ongoing
2020 New Studies Ongoing Studies
Industry Other
CMH 0 2 8
GRH 0 20 60
SMGH 1 18 40
Projects Reviewed 2020
0
10
20
30
40
50
60
New Projects Amendments Annual
Renewals
Studies
Completed
Total Full Board Delegated
Types of Studies Submitted in 2020
A. Chart review 6
New Projects Submitted in 2020 29
New Projects Reviewed in 2020 28
Full Board 8
Delegated 20
Amendments Reviewed 34
Full Board 10
Delegated 24
Annual Renewals 53
Full Board 49
Delegated 4
Studies Completed 24
___
Total Reviews 139
Total Open Files 97
4
84

THREB Annual Report 2020/2021
B. Clinical – drug 3
C. Clinical – non‐drug Note: many of these projects involved either the COVID blood bank or the COVID registry
17
D. Survey/Questionnaire/ Focus‐groups 3
Industry Non‐industry Total
2004 8 13 21
2005 14 13 27
2006 13 15 28
2007 9 22 31
2008 8 29 37
2009 11 19 30
2010 11 21 32
2011 6 20 26
2012 5 24 29
2013 10 21 31
2014 4 22 26
2015 6 14 20
2016 5 31 36
2017 3 25 28
2018 1 25 26
2019 2 18 20
2020 1 28 29
5
85

THREB Annual Report 2020/2021
6. Budget Issues
Over the past 10 or so years, the total number of new studies has varied but averaged around 27 per
year. However, the relative distribution between industry‐sponsored and other studies has continued
to change, with a general downward trend in industry‐sponsored studies.
Fees from industry‐sponsored studies initially provided for approximately half of the THREB budget, but
that is no longer happening. Therefore, for the 2017/18 fiscal year the three hospitals all agreed to
increase their commitment to $18,000 per hospital to cover essentially the full cost of the THREB with
the understanding that any increased income from industry‐sponsored studies would be used to lessen
the following year’s contributions from the hospitals. Thus, the 2018/19 year’s industry fees allowed
the contribution per hospital requested for the 2019/20 year to be $16,000, and the industry fees from
2019/20 lowered the request for the 2020/21 year to $14,000. For the 2021/22 year, the industry fees
collected in 2020/21 will allow a contribution request of $15,000 per hospital. Some surplus is still
retained for unexpected expenses and, when it is possible again, to send one or two other THREB
members to the annual meeting of the Canadian Association of Research Ethics Boards (CAREB) as do
most REBs.
Regarding unexpected expenses, for example, in the new fiscal year there has been already a significant
expense for 2 new computers for the THREB office since GRH Digital Services considered the old ones
quite outdated. In addition there will be the extra payments for the orientation overlap for the new
Chair.
THREB office work and meetings have become completely (hopefully someday only “mostly”) virtual,
and while that eliminated the nominal cost of catering, it has meant an increase in time needed to deal
electronically with submission and review of documents. Currently, the management and review of the
electronic documentation takes more administrative time than when it was paper‐based and office
communication could be done quickly and without the need for back and forth emails. As the Chair’s
work increased over the years with the increasing amount and complexity of REB demands, the hourly
fee was kept the same but the dedicated time agreed to by the hospitals increased from 10hr/month in
2005 to 15hr/month in 2009 to 20hr/month in 2011 where it has remained until now. One of the tasks
of the new Chair will be to work out the new requirements for dealing virtually with administration of
the THREB and what the resulting time requirements are.
7. Terms of Reference
The THREB members reviewed the THREB Terms of Reference at the September, 2020 meeting and saw
no need for any further changes at the time.
The THREB members recommend that the current Terms of Reference submitted and approved in 2019
be given continuing approval by the hospital Boards.
6
86

THREB Annual Report 2020/2021
7
8. Federal Wide Assurance
In order to receive research grants from United States government agencies such as NIH, the hospitals
and the REB (IRB) must be registered with the U.S. Health and Human Services. All three hospitals
remain registered and have a Federal Wide Assurance until at least 2022. The THREB registration is for 3
years and is currently active until January of 2022. The THREB registration is reviewed and renewed
when membership changes. With the new chair and change in other members the renewal will need to
be done soon.
9. Coordinated Review of Research Projects with the University of Waterloo
Several years ago, THREB and research administration at the University of Waterloo developed a process
to coordinate review of research projects that involve researchers at both institutions. The process was
then approved as part of the Terms of Reference and began to be implemented in 2015. Since then
usually there are a few projects a year that go through the coordinated review process. In 2020 only one
of the 29 research projects submitted were handled through the coordinated review process.
10. Potential Future Developments
Two major new developments for THREB are 1) the transition to a new Chair, and 2) the need to
develop processes to deal with the new reality of a mostly virtual office and mostly virtual meetings.
Both will necessarily lead to changes in how things are done.
As said in previous reports, there has been a two decade‐long push to get accreditation of REBs in
Canada. The introduction of a process for accreditation of REBs for participation in Clinical Trials Ontario
(CTO), and similar work in some other provinces suggests that an accreditation process will be required
at some point in the future and will involve the three councils as well as Health Canada in the
development. However, little progress was reported at either the 2018 or 2019 meeting or the 2021
virtual meeting of the Canadian Association or Research Ethics Boards (CAREB), though some REBs go
through an accreditation process with an organization from the United States.
Of possibly more immediate consequence will be the influence of developments in the United States
around the way consent forms will be required to be constructed to make them easier to understand.
Also the push in the U.S. to have clinical trials reviewed by a single REB (not unlike the CTO process in
Ontario) will at some point likely have an impact in Canada
In the meantime, the THREB is committed to ensuring that all members complete the TCPS2 tutorial;
and all current members except some new members have completed it. This tutorial is mandated for
researchers at all the universities and teaching hospitals in Ontario that I have checked with. At the 5 or
6 community hospitals which I surveyed last year, completion of the tutorial is required for REB
members, but none of those I communicated with had yet made the tutorial a requirement for
researchers, though most were contemplating doing so. The THREB is still working on deciding if and
when it should require completion of the tutorial by researchers, recognizing that such educational
requirements belong within the jurisdiction of the hospitals.
87

THREB Annual Report 2020/2021
8
8. BUDGET 2020/2021
THREB BUDGET REPORT April 2020‐March 2021
Expenses Projected Actual
Revenue
Projected* Actual
Balance
Beginning balance
$ 35,417.06
Sponsor payments 0 $ 9,000.00
Chair ‐20hr/month + HST $ 27,120.00 $ 25,342.40 From CTO projects 0 $ 0
St. Mary's $ 18,000.00 $ 14,000.00
Administrative Asst. (2d/week)
2d/week pay, benefits, $ 22,000.00
$ 20,160.85
plus some OT or student work Cambridge $ 18,000.00 $ 14,000.00
E&HR Subscription for members $ 500.00 $ 0
Monthly lunch $ 1,100.00 $ 0 Grand River
$ 18,000.00
$ 14,000.00
Postage, Courier. General supplies $ 100.00 $
Education ‐ conferences, etc $ 2,000.00 $ 0
Bell Teleconference/Zoom $ 1,000.00 $ 496.86
CAREB Membership $ 150.00 $ 127.36
Office supplies $ 600.00 $ 485.48
Minor Equipment $ ‐ $ ‐
Appreciation gift to members $ 650.00 $ 650.00 Misc $ 500.00 $ 0
To be confirmed: Bell charges $ 1,042.08
TOTAL $ 54,920.00 $ 48,305.04 $ 5 4 ,000.00 $ 51,000.00
‐
Fiscal year‐end balance
$ 2,694.96
Total year‐end Final Balance
$ 38,112.02
* Projected revenue indicates the 2017 agreed‐upon hospital contributions to fully fund the operations of the THREB, with the understanding that sponsor revenue from a current year would be deducted from the subsequent year’s actual contribution request.
88

TERMS OF REFERENCE FOR
TRI-HOSPITAL RESEARCH ETHICS BOARD (THREB) CAMBRIDGE MEMORIAL HOSPITAL
GRAND RIVER HOSPITAL ST. MARY’S GENERAL HOSPITAL
MANDATE The primary mandate of the Tri-Hospital Research Ethics Board (THREB) is to determine the ethical acceptability of research proposed by the hospital(s), by researchers having an association with the hospital(s), or research involving patients or staff at Cambridge Memorial Hospital, Grand River Hospital, or St. Mary’s General Hospital, with the exception of research reviewed by an alternate Research Ethics Board of Record* for the hospital(s). . In discharging this mandate, the Tri-Hospital Research Ethics Board (THREB) has the authority to approve, reject, propose modifications to, or terminate any proposed or ongoing research involving human subjects that is conducted within the hospital(s), again, with the exception of research reviewed by an alternate Research Ethics Board of Record for the hospital(s). THREB complies with the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (TCPS2), the International Conference on Harmonization Good Clinical Practice Consolidated Guideline (GCP), Part C Division 5 of the Food and Drug Regulations of Health Canada, the provisions of the Ontario Personal Health Information Protection act (PHIPA) and the United States Food and Drug Administration regulations at the Code of Federal Regulations (CFR) Title 21 Part 50 and CFR Title 45 Part 46 and other applicable laws and guidelines. RESPONSIBILITIES:
1. To protect the rights, safety and wellbeing of research participants in all healthrelated research studies conducted under the auspices of Cambridge Memorial Hospital, Grand River Hospital or St. Mary’s General Hospital, with the exception of that research reviewed by an alternate Board of Record for the hospital(s),
2. To provide all submitted health-related research protocols appropriate ethical and scientific review in accordance with the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (TCPS2) and other applicable laws and guidelines,
3. To continue review of the ethical and scientific acceptability of research conducted under the auspices of the THREB,
89

Terms of Reference Tri-Hospital Research Ethics Board Page 2 of 4
Revised: November 6, 2002; October 5, 2005; November 1, 2006; December 2014; January 2017; Reviewed 2018, 2019, 2020.
4. To provide education regarding research guidelines to the membership of the THREB in order to promote adherence by researchers to the TCPS2 and other accepted standards, as applicable,
5. To review submitted proposals for alignment with the mission, vision, and values of the participating hospitals(s),
6. To determine that any impact on the resources of Cambridge Memorial Hospital, Grand River Hospital or St. Mary’s General Hospital has been assessed, and
7. To prepare and provide an annual THREB summary report to the three hospital boards.
CORPORATE ACCOUNTABILITY The THREB receives its authority from and reports to the Board of Directors of Cambridge Memorial Hospital, the Board of Directors of Grand River Hospital and the Board of Trustees of St. Mary’s General Hospital. The THREB will review its Terms of Reference annually and present them to the hospital Boards for approval. AUTHORITY OF THREB The THREB has the authority and responsibility to approve, propose modifications to, or reject research involving human participants, monitor ongoing research and to suspend or terminate any research being carried out within or under the auspices of the member hospitals, with the exception of research reviewed by an alternate Research Ethics Board of Record for the hospital(s). The member hospitals retain the authority to reject any THREB approved research. In order for the THREB to retain the independence required of it by the TCPS2, a decision made by the THREB to reject research may not be overruled by member hospitals. The THREB may establish formal agreements with other institutions or organizations to facilitate review and approval processes of multi-site research projects which are under review by another Research Ethics Board. Such agreements will require a formal decision of the THREB membership and signature of the Chair. The decisions of the THREB are open to appeal through an appeal mechanism established by the member hospitals.
90

Terms of Reference Tri-Hospital Research Ethics Board Page 3 of 4
Revised: November 6, 2002; October 5, 2005; November 1, 2006; December 2014; January 2017; Reviewed 2018, 2019, 2020.
MEMBERSHIP The THREB must have membership that meets the requirements of the TCPS2, GCP and PHIPA. The THREB will be comprised, in addition to the Chair, of three representatives from each hospital, approved by the CEOs of their respective hospitals, and including:
• two members who have broad expertise in the methodologies and the areas of science reviewed by the board;
• physician representative(s); • member(s) from the discipline of ethics; • two lay members without affiliation to the hospitals, recruited from the
community; • clinical pharmacist(s); • one executive representative from each hospital; • member(s) knowledgeable in Canadian law relevant to the research; • member(s) knowledgeable in privacy issues; • ad-hoc reviewers as necessary (non-voting).
Membership will be for a renewable 3 year term. Members will complete relevant training and education as required by the Chairperson. CHAIRPERSON The Chairperson is approved by the Boards of the three hospitals for a renewable three year term, and must have experience on a Research Ethics Board with education and expertise in research methodology and research ethics. The Chairperson shall be the THREB’s official spokesperson. DECISIONS Although attempts will be made to reach consensus on decisions, a vote of the majority present will be taken as the Tri-Hospital Research Ethics Board’s decision provided there is a quorum. Written positions are encouraged to facilitate discussion when a member cannot attend. Committee members must be absent from the meeting for the portion where his/her application (Principal Investigator or Sub-investigator) is being considered or whenever there is a conflict of interest. QUORUM
91

Terms of Reference Tri-Hospital Research Ethics Board Page 4 of 4
Revised: November 6, 2002; October 5, 2005; November 1, 2006; December 2014; January 2017; Reviewed 2018, 2019, 2020.
A quorum shall be constituted so long as a majority of the total number of voting THREB members is present. For decisions affecting the THREB itself, the quorum must also include at least one representative from each of the THREB hospitals. MEETINGS Meetings will be held at least 9 times a year at a set time. At the discretion of the Chairperson, scheduled meetings may be cancelled or additional meetings called. ATTENDANCE
• Members must notify the Chairperson if they are unable to attend a meeting • Frequent unexplained absences will be addressed by the Chairperson
CONFIDENTIALITY The THREB is bound by Tri-Council Policy Statement, and the respective hospitals’ policies on the release of information. The THREB meeting agenda, minutes, and information contained in research proposals submitted for ethics review are all confidential. Official copies of reviewed proposals will be retained by the THREB Office for as long as legally required.
* A Research Ethics Board of Record is a Research Ethics Board that has been appointed by an institution under whose auspices a research study is being conducted to serve as the primary or sole authority for the research ethics oversight of the study. (See: Canadian General Standards Board: Research Ethics Oversight of Biomedical Clinical Trials.) OCREB is currently an alternate REB of Record for CMH and GRH for multi-centre cancer studies.
92

Patient ExperienceSemi-Annual Report
June 1, 2021
Jane OttmanPatient Experience Lead
Liane Barefoot Director – Patient Experience, Quality & Risk
Agenda Item 3.3.2
93

Who We Serve
• Current and former patients• Family members/care partners• Visitors• Staff and Volunteers• Professional and medical staff • Liaison to community groups
294

Patient Experience Lead
Jane Ottman, BScN RN, MHSc
• Utilizing past experience in stakeholder relations/engagement, clinical management and education to elevate the Human Experience at Cambridge Memorial Hospital
• Passionate about building relationships to improve the human experience
395
What our patients are saying
496

Patient Experience 2020-21* Volumes
518 Files 970 Issues
488 Complaints
232 Compliments
250 Requests/Suggestions
*Apr-Dec data is complete; Jan-Mar data is still open and subject to change
597

Total Feedback Files by Fiscal Year
• Files = new unique complaints/compliments/suggestions• Straight-line extrapolation would show total files at fiscal year-end of 612 files, which
is approximately a 16% increase in annual volume likely indicative of COVID-related issues from April – December 2020
698

Distribution of Issue Types
• Trend of reduction in proportion of complaints has continued into 2020/21; compliments have remained static over 2019/20 to 2020/21
799

Complaints by Department
• Looking at Q3 YTD for the Emergency Dept. complaints, there was a decrease of 21% in total ED visits, and a decrease of 14% in total ED complaints for the same period
8100

Reasons for Complaints – 2020/21
72%
9101

Compliments by Department
10102

Reasons for Compliments – 2020/21
97%
11103

• ECFAA 2010 Response Time Regulation = 5 calendar days• Includes all closed files; based on unique file IDs and time between date of notification
and date of first response
Time from Initiation to First Response
Days to Response All
Types
Fiscal 2017/18
Fiscal 2018/19
Fiscal2019/20
Fiscal2020/21
YTD
Same day 69.0% 68.6% 75.7% 84.0%
Less than 2 days 87.0% 83.8% 97.5% 94.8%
Less than 5 days 94.0% 91.0% 99.4% 99.1%
12104

External Satisfaction Survey% Top Box Answers to ‘Would You Recommend?’
• Red = below 50th percentile as compared to Community Hospitals • Green = above 50th percentile as compared to Community Hospitals
Unit 2016-17 YE
2017-18 YE
2018-19 YE
2019-20 YE
2020-21 YTD (as of May 20, 2021)
Community Hospital 50th
%tile
Community Hospital 75th
%tile
OBS 46.7%PR: 5
59.2%PR: 32
38.1%PR: 1
56.5%PR: 19
76.9%PR: 66
73.0% 78.0%Surgery 58.2%
PR: 2154.4%PR: 15
56.2%PR: 18
59.5%PR: 22
73.5%PR: 48
Medical 46.8%PR: 5
47.5%PR: 5
44.3%PR: 4
48.8%PR: 7
61.9%PR: 18
ED 47.1%PR: 15
42.9%PR: 10
42.4%PR: 7
46.6%PR: 15
62.3%PR: 24
65.0% 72.6%
13105

External Satisfaction SurveyPhysical Environment
24%31%
62%
39%55%
76%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MED SURG OBS
% T
op
Bo
x
Unit
Quiet around room at night
FY1920 FY2021 ‡
45%54%
64%73% 68%
75%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MED SURG OBS
% T
op
Bo
x
Unit
Room kept clean during stay
FY1920 FY2021 ‡
‡ Data is not final and subject to change
- Full fiscal year in A-wing:- For Medicine A and OBS; much of 2020/21 surgery patients on Paediatrics in A wing- Quiet – work done to increase staff awareness re: importance of quiet at night, and on OBS – private rooms
and more spread on compared to old unit
14106

External Satisfaction SurveyRespect and Dignity: Involvement in Care
51%66%
77%
40%
73%80%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MED SURG OBS
% T
op
Bo
x
Unit
Involved in decisions about care
FY1920 FY2021 ‡
‡ Data is not final and subject to change
- Visitor restrictions with limited presence of care partners – challenges to obtain information; not at bedside when clinical staff present
- Communication challenges related to COVID-19 – difficult to involve in a timely manner- Support for anxieties/fears has shown no significant change from 2019/20 to 2020/21
69% 73% 79%
34%
61%73%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MED SURG OBS
% T
op
Bo
x
Unit
Family and friends involved in decisions about care
FY1920 FY2021 ‡
15107

Visiting CMH• Over course of fiscal year, CMH has had periods of
complete lockdown to visitors other than for End-of-Life – challenging for patients and care partners, and for clinical staff
• Since spring 2020, where virtual visits (VV) were only offered 5 days/week from 9-5, CMH now has up to 32 VV spots/day and 7 days/week
• Currently, have 30 in-person visits/day with each patient allowed 1 designated visitor/care partner
• Weekly review of visitor restrictions
16108

COVID-19 – Virtual Visiting
• There are now 4 iPads in circulation to meet VV schedule needs
• All on stands so patient/family can have privacy while having face time or zoom call
• In addition to 4 in circulation for VV, there are iPads in ED, ICU, Medicine A, Rehab and Inpatient Surgery
17109

Moments Elevating the Human Experience• Care partners with patients in the ED for <18
years and >70 years• iPads for virtual family consultations and therapy
updates on units• Plans for accommodation of mom/baby dyad, and
regular accommodation for patients with hearing or sight impairments (iPad, Hearing Society remote interpreters, service animal inclusion)
18110

Moments….
• Accommodation of less traditional care partner visiting – outdoor dog visits
• Welcoming GTA patients displaced by 3rd wave
19111
Moments….
• Excellent compliments highlighting examples of staff living CMH values:
• “Without exception, every person I came in contact with treated me with respect and compassion and always went out of their way to see that my needs, both physical and emotional, were being taken care of”
• “I mattered to both these wonderful doctors…With COVID and all that’s going on, again I mattered and I just wanted to share this experience. My thanks to all in the emergency dept. to the wonderful woman who did my bloodwork and all the people who did my tests and most of all to the wonderful Drs. Shoop and Salama.”
20112

What Worries us Most
• Limited scheduled visitor appointments vs. return to open visiting hours – when??
• CRP – interim space on C-wing – C3 has challenges related to space and privacy
• Additional units moving to C-wing• Intent vs. Impact – continued communication
challenges between physicians/staff and patients
21113

Questions??
22114

Agenda Item 3.3.2
Page 1 of 5 May 2021(2)
Date: May 25, 2021 Issue: PFAC Annual Update Prepared for: Quality Committee Purpose: ☐ Approval ☐ Discussion ☒ Information ☐ Seeking Direction Prepared by: Liane Barefoot, Director Patient Experience, Quality & Risk Corey Kimpson, Chair PFAC Approved by: Mari Iromoto, Senior Director, Strategy & Performance Attachments/Related Documents: None Alignment with CMH Priorities
2021-22 Strategic Plan
No ☐
2021-22 Integrated Risk Management Priorities
No ☐
2021-22 Priorities
No ☐ ☒ Prove Patients Matter Most ☒ Staff and Physician Wellbeing ☐ Accelerating Access to Care ☐ Increase Joy in Work ☐ Length of Stay ☐ Keeping Staff and Physicians Safe and Engaged ☐ Lead Boldly ☐ CRP Phase 3 ☐ Executing CRP Phase 3 ☐ Multi-year Fiscal & Capital Strategy ☐ Completing our HIS Evaluation
Background The last update on the PFAC was presented to Quality Committee in June 2020 and included a summary of activities from September 2019 June 2020. This briefing note will provide an update of PFAC activities/discussions from September 2020 June 2021. Council Membership PFAC was initially established in December 2014 and is currently at nine (9) active members plus one (1) staff representative who joined the council in September 2016. This year two (2) of our founding members reached their six-year mark and as per terms of reference, completed their tenure with the PFAC. We offer sincere thanks to Becca Kadar and Andrea Stebbings for being part of the early conversations and staying the course with us for six years! In addition, our staff representative Sarah Kreller has resigned from CMH and as such, May 2021 was her last meeting. Throughout the past year we have been successful at recruiting four (4) new members to PFAC. Welcome to Colleen Bulla, Paula Pavia, Julie Koehler and Jan Owens. Finally, this year we have invited a member of the Mental Health Family Advisory Council (MH-FAC) to join our meetings to facilitate some cross-over work. Two (2) MH-FAC members
BRIEFING NOTE
115

Agenda Item 3.3.2
Page 2 of 5 May 2021(2)
alternate attendance and act as back up for one another. A warm welcome to Deb Bartucci and Alison Fitzpatrick from the MH-FAC. 2020-21 Year in Review As many committees across the hospital slowed, or in some cases paused, PFAC has continued to meet monthly throughout the entire duration of COVID. April 2020 was a teleconference, October 2020 was a socially distanced in-person meeting, and all others have been video conferences via TEAMS. Kudos to our PFAC members for adapting, ‘showing’ up every month with their cameras on and continuing to be a VERY engaged group. Below is a summary of some highlights from the 2020-21 council year: Strategic Priority Alignment As priorities across the organization have needed to be evaluated and re-evaluated over the past year, management has engaged PFAC to share these organizational priorities. PFAC meeting agendas are now structured with a section dedicated to the Strategic Priority Updates and highlight PFAC engagement in these initiatives.
1. Digital Health: PFAC as a group have participated in the Meditech Expanse evaluation sessions that were patient facing (i.e. patient discharge summaries, patient portal, link to community providers). As we move to expand our Hospital Information System (HIS) evaluation to include Cerner, PFAC members will continue to be involved in this process. Corey Kimpson was involved in the selection of Savience, the online booking system that was initially piloted with the COVID Assessment Centre. Corey was involved in selection, build, and testing. Many PFAC members shared real-life updates on how they (or their family members) found the system once it went live. It is intended that Savience will be expanded to other areas such as diagnostic imaging. Paula Pavia has volunteered to join the Clinical Informatics Committee once it resumes. Four (4) PFAC members (Jan Owens, Colleen Bulla, Paula Pavia, & Suzanne Sarrazin) have volunteered to provide input into the Patient Entertainment System selection which is currently out for request for proposal and slated to be evaluated in the coming months.
2. Diversity, Equity & Inclusion: Based on personal availability, PFAC members were invited to attend 1, 2, or all 3 of the Advisory Board learning sessions offered to leadership of CMH and Grand River Hospital concurrently. The list below will illustrate the outstanding participation by PFAC members in this important introduction to concepts of Diversity, Equity & Inclusion. Combined, they attended a whopping 16 sessions!
• Corey Kimpson – attended 3 sessions • Paul Pavia – attended 3 sessions • Sharon Wohlgemut – attended 3 sessions • Colleen Bulla – attended 2 sessions • Jan Owens – attended 2 sessions • Suzanne Sarrazin – attended 2 sessions • Alison Fitzpatrick – attended 1 session
Corey Kimpson has completed an online Indigenous Cultural Safety Training course.
116

Agenda Item 3.3.2
Page 3 of 5 May 2021(2)
3. Eyes and Ears of the Community: Throughout COVID we have left this as a standing item on the agenda to ask our PFAC members what they are hearing and seeing in our community. We have asked them to be intentional in their interactions with family, friends, neighbors and to overtly ask how CMH is doing throughout the pandemic. A few examples of items which they have brought forward include:
• Inability to access in-person family physician appointments and how this might be impacting volumes in the ED
• Care partner experiences in the ED as it related to inequitable application of the exception criteria
• Linking with care partners at the time of discharge to explain discharge plans when care partners have not attended
• Community hesitation/fear about coming to the hospital – especially early in the pandemic
Care Partners/Visiting at CMH Not surprisingly, PFAC members have been very interested in weighing in on the many iterations of our visitor restrictions over the past year. They provided input early on about the restrictions in ED which resulted in staff education and liberalizing the criteria. They have also provided personal experiences (positive & negative) about how the criteria has been applied in ED, inpatients, Women’s & Children, and end of life situations. Our ultimate goal, post COVID, is to get back to the Open Visiting for Care Partners. Corey Kimpson continues to attend the weekly meetings regarding the visitor policy to provide patient and community perspectives. External Presentations Corey Kimpson, Chair of PFAC and Liane Barefoot, Director Patient Experience, Quality & Risk presented two (2) breakout sessions at the Beryl Institute annual conference in April 2021. The first was a 40-minute session titled ‘Using a Risk Lens to Resume Visiting During COVID’ that examined how CMH has engaged a wide group of stakeholders to weigh risks/benefits as we have alternated between resuming and shuttering visiting throughout the pandemic. The second was ~ a 12-minute segment of a larger session. We partnered with PFAC members from London, England and Green Bay, Wisconsin to showcase how PFAC members were engaged (or not) throughout COVID in three different countries. Community Ambassador Role As with the majority of the world, functions inside CMH have focused almost exclusively on COVID since mid-March 2020. Early on in the pandemic we identified a need for a role that intersected Communications Patient Experience Community Relations. As such, a temporary part time role of Community Ambassador was created and Corey Kimpson assisted us on a daily basis from inside the hospital from March 2020 to March 2021.
117

Agenda Item 3.3.2
Page 4 of 5 May 2021(2)
From the perspective of a patient/community member, she challenged our processes, policy changes, worked tirelessly to shed a spotlight on less known individuals and departments to the community, responded to social media posts, and acted as a liaison with many community organizations, but most notably the Cambridge Mask Makers. Recruitment Over the past year PFAC members have been involved in the interviews for the following roles.
• Chief of Staff – Corey Kimpson • Vice President Corporate Services, CFO – Sharon Wohlgemut • Vice President Clinical Services, CNE – Alison Fitzpatrick • Clinical Director of Medical Programs – Sharon Wohlgemut • Diversity, Equity & Inclusion Project Manager – Alison Fitzpatrick • Tri-Hospitals Research Ethics Board (THREB) Board Chair – Colleen Bulla
This too is a standing item on our agendas to ensure PFAC members were provided the opportunity to ask questions related to patient experience and/or philosophy of patient engagement during the interview, and felt that their voice was equal to those of staff members’ voices. Upcoming Year As we look ahead to the coming years there is a commitment from PFAC members to develop and implement an inventory of our current members that aims to capture which programs/services at CMH they have interacted with, plus which segment(s) of the Cambridge and North Dumfries community (gender identification, age group, ethnic group, etc.) they feel competent representing and advocating on behalf of. This will ultimately inform more purposeful recruitment with the ultimate goal of acknowledging and closing some of the identified gaps. As an offshoot of this work recruitment of the vacant staff role(s) to PFAC will intentionally aligned to areas of work/interest.
118

Agenda Item 3.3.2
Page 5 of 5 May 2021(2)
By June 2022 Corey Kimpson will have completed her six-year tenure with PFAC so the next year will be spent creating and implementing a succession plan for our PFAC chair role which will need to be implemented by September 2022. Finally, PFAC members are interested in exploring and defining some overlap work with the Employee Engagement Council as the Beryl Institute has introduced their newest concept titled the ‘Human Experience’ which collectively acknowledges the role that the clinician, caregiver AND patient all have to play.
119

Agenda Item 3.3.4
Page 1 of 2 May 2021(2)
Date: June 2, 2021 Issue: Update on Trillium Gift of Life Performance Metrics Q3 2020/21 Prepared for: Quality Committee Purpose: ☐ Approval ☐ Discussion ☒ Information ☐ Seeking Direction Prepared by: Sandra Hett, VP Clinical Programs & CNE Attachment/Related Document:
Appendix 1: Organ & Tissue Performance Dashboard 2020/21 Alignment with CMH Priorities
2021-22 Strategic Plan
No ☐
2021-22 Integrated Risk Management Priorities
No ☐
2021-22 Priorities
No ☐ ☒ Prove Patients Matter Most ☐ Staff and Physician Wellbeing ☒ Accelerating Access to Care ☐ Increase Joy in Work ☐ Length of Stay ☐ Keeping Staff and Physicians Safe and Engaged ☐ Lead Boldly ☐ CRP Phase 3 ☐ Executing CRP Phase 3 ☐ Multi-year Fiscal & Capital Strategy ☐ Completing our HIS Evaluation
Background The Gift of Life Act (1990) identifies obligations for designated facilities (hospital) with expected partnership with Trillium Gift of Life Network in implementation of mandatory practices for organ procurement. Trillium Gift of Life Network (TGLN) is Ontario's organ and tissue donation agency. Trillium Gift of Life Network was created to help save and enhance lives by maximizing organ and tissue donations for transplantation. Living donation is becoming an increasingly important source of organs for transplant. Trillium Gift of Life Network has now transferred to Ontario Health with the legislative changes (Bill 74 The Peoples Health Care Act 2019). This created a new health agency and provided the ability to transfer TGLN to this agency effective April 1, 2021. Cambridge Memorial Hospital hosts regular meetings to review data provided by TGLN and work on any improvement strategies required. See Appendix 1 - Q3 20 21 dashboard attached and definitions of performance metrics monitored. (Q4 data not available until the end of June). This data was reviewed by the CMH Organ and Tissue Donation Committee in April 2021. Analysis Routine Notification Rate is 96 % for Q3 with a year to date average of 98%. The 19/20 rate for CMH was 95%. This process requires ongoing education with new nursing staff and while remains above the provincial target, there is the expectation of 100 % which was achieved in Q1 with focused education.
BRIEFING NOTE
120

Agenda Item 3.3.4
Page 2 of 2 May 2021(2)
The Eligible Approach Rate for Q3 remains at 100%. This metric was introduced and publicly reported in 2017/18 at which time CMH performance was 75%. The Conversion Rate for Q3 is low at 0% however this needs to be taken in context with the eligible approach rate which is 100%. (19/20 YTD for CMH is 33 % which represents 6 potential donors and 2 actual donors). If there had been missed notifications, families would not have had the opportunity to make a decision about donation. The goal for conversion rate is set at 63% because not all Ontarians have organ donation as a part of their end-of-life plans. The tissue notification rate at CMH remains variable with ICU at 100%, ED and the clinical floors around 70%. The timeline for notification is either prior to the imminent death or up to 1-hour post time of death. The issue here is creating this as a priority for these clinical teams as a priority function when it is merely notification.
121

Trillium Gift of Life Network2 122

Agenda Item 3.4.1
Page 1 of 4 May 2021(2)
Date: June 10, 2021 Issue: Medical Advisory Committee – OPEN SESSION Prepared for: Board of Directors Purpose: ☐ Approval ☐ Discussion ☒ Information ☐ Seeking Direction Prepared by: Dr. Asim Masood, Chief of Staff & VP, Medical Affairs Approved by: Mr. Patrick Gaskin, CEO Attachments/Related Documents: Alignment with CMH Priorities
2021-22 Strategic Plan
No ☐
2021-22 Integrated Risk Management Priorities
No ☐
2021-22 Priorities
No ☐ ☒ Prove Patients Matter Most ☒ Staff and Physician Wellbeing ☒ Accelerating Access to Care ☐ Increase Joy in Work ☒ Length of Stay ☒ Keeping Staff and Physicians Safe and Engaged ☒ Lead Boldly ☒ CRP Phase 3 ☒ Executing CRP Phase 3 ☐ Multi-year Fiscal & Capital Strategy ☒ Completing our HIS Evaluation
Items for Board Information Visiting at CMH At the time this briefing note was prepared, a cross section of individuals was invited to broadly look at a visiting (inpatient, attending appointments, & accessing hospital services) as we prepare to enter Phase 1 (anticipated to be on June 14, 2021), Phase 2 (as early as July 6, 2021) and Phase 3 (as early as July 27, 2021) in the province of Ontario. The consensus of the group is to remain status quo for the time being and catch up at Phase 3 where there are any variances. A more fulsome update of the progressive plan with regard to visiting and support persons at CMH will be provided at the June 16, 2021 CLST meeting. The information will be presented to CSLT next week. The following new Medical Directive was approved: Medical Directive: Manual Busopan & Glucagon This Medical Directive supports trained Medical Radiation and Imaging Technologists (MRTs) working in Diagnostic Imaging with the knowledge, skill and judgement to administer either hyoscine butylbromide (Buscopan) or glucagon to adult (18 years of age and older) patients referred to CMH for a Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) examination of the abdomen and/or pelvis to reduce motion artifact from peristalsis. COVID-19 Update Dr. K. Nuri provided the following update on June 9, 2021 numbers:
BRIEFING NOTE
123

Agenda Item 3.4.1
Page 2 of 4 May 2021(2)
Global Update National Update Total Confirmed Cases: 173,674,509 Total Confirmed Cases in Canada: 1,395,410 Total Deaths: 3,744,408 Total Deaths in Canada: 25,790 CF: 2.1% CF: 1.8% Vaccination: 2,092,683,229 DA Provincial Update Regional Update Total Confirmed Cases in Ontario:
537,487 New Cases:
New Cases: 411 Total Confirmed Cases in Local Region:
16,338
Total Deaths in Ontario: 8,920 New Cases: 54 CF: 1.7% Active: 342 LTC Outbreaks: 20 LTC/RH Outbreaks: 1 Hospitalizations: 571 Hospitalizations / ICU: 34/20
ICU ICU on a ventilator: 466-
383/314-273 on a
vent
Screened Positive: 307
VOC: B.1.1.7: B.1.351: P.1
134,608 1,125 4,073
VOC: B.1.1.7: B.1.351: B.1.617: P.1.60
3,003
7 13 60
Vaccine: TDA: Fully vaccinated:
10,445,119 1,282,676 (8.8%) of
population
CMH Update ICU: 2 (1 intubated) Med A:2
A significant shelter outbreak taking place in the region that started at the KW shelter. The situation is not controlled and has spread quickly as individuals in shelters are not following public health measures and many are rejecting testing and vaccinations. There have been 4 individuals from shelters admitted to another hospital. A request has been put out for extra staffing support. Critical Care Update & Service Resumption Across the province critical care is slowly improving every day. Now under 500 patients in ICU as a province. CMH has not had a new patient for some time, however, we still have chronic patients in ICU. We are now seeing volume in ICU increase from other diseases. The CCSO has asked for a submission on how we will reduce the beds we currently have. We have been asked to close 5 ICU beds to go down to 17. Staff are slowly redeploying back to their original
124

Agenda Item 3.4.1
Page 3 of 4 May 2021(2)
services. The next schedule for ICU nursing staff does not include any redeployed staff. We are still in our expanded state; however, we are operating at our usual baseline bed level. For the last week or so, our regional partners have had a little surge in COVID patients and a patient from GRH was requested to transfer to CMH, however, it did not happen for other reasons. Our medical manpower staffing during the daytime for ICU has gone back to normal. Currently still have assistance from anesthesia department in the evenings which is slated to end on June 13th and we will revert to our usual schedules and complement of GIM, ICU and Hospitalists. Our Hospitalists have stepped up and increased their hours in the evenings and will continue this for the foreseeable future. Standing Monthly Reports Expect to end the year, has been included in the pre-circulated material. Have included a brief status update was included in the material on how we are progressing against each item.
Clinical Coding & Documentation Review Committee Total Weighted Cases Recovered 272 Total QBPs Recovered 100 Total QBP Funding Recovered $683,785 Total Weighted Cases Recovered $1,230,664 Total Funding Recovered $1,914,449
• One of the opportunities identified through the reviews was coding / documentation for
palliative care (1) Coders need to have clear and precise documentation to fully optimize weighted cases, funding for QVPs and HSRM results and (2) Opportunities around coding and documentation for palliative coding of DNR.
• Next steps: o Coding clinics and education sessions through the summer on specific topics. o Summary of key findings and areas for improvement will be reviewed with the
Clinical Coding and Documentation Review Committee. DEI Update The DEI plan has been identified as a corporate priority as we move towards a more inclusive culture. It is a priority to elevate the understanding of diverse experiences of staff with the goal to integrate our insights to strengthen the culture and practices at CMH. Looking to keep staff and physicians safe and engaged by developing a CMH strategy and planned rollout of initiatives for workplace DEI by June 30, 2021. Preliminary survey results can be reviewed on the CMH Intranet Diversity, Equity & Inclusion page (Diversity, Equity & Inclusion). All staff with a CMH email have access to the Canadian Centre for Diversity and Inclusion’s (CCDI) website and webinars and newsletter (subscribe to CCDI directly). PFAC Update Ms. Corey Kimpson provided the following update for PFAC:
• PFAC continues to meet virtually. Continue to be active with CMH projects, including the review of the patient entertainment system update.
• Work continues with visitor / care partner policy as we look to reduce restrictions on all units and have more flexibility. PFAC recognizes that this is an area where balance is required in order to keep everyone safe.
• 7 PFAC members attended 16 of the Advisory Board Diversity and Inclusivity sessions.
125

Agenda Item 3.4.1
Page 4 of 4 May 2021(2)
• PFAC working to survey members and develop an inventory of member experiences and backgrounds to broaden the lens and viewpoint to ensure membership is representative of the Cambridge community.
• Ms. C. Kimpson has joined the newly formed standing committee on equity and inclusivity.
• Community is excited about COVID vaccinations but there is still confusion around how and when to receive a vaccination. The community are trying to help each other with scheduling vaccinations.
• Some PFAC members whose terms on the committee are ending in June 2022 and work will be taking place over the summer on the Succession Plan to fill the gaps.
126

Agenda Item 3.4.2
Page 1 of 5 May 2021(2)
Date: June 10, 2021 Issue: Medical Advisory Committee – Privileges & Credentialing
(May Credentialing Committee) Prepared for: Board of Directors Purpose: ☒ Approval ☐ Discussion ☐ Information ☐ Seeking Direction Prepared by: Dr. Asim Masood, Chief of Staff & VP, Medical Affairs Approved by: Mr. Patrick Gaskin, CEO Attachments/Related Documents: Alignment with CMH Priorities
2021-22 Strategic Plan
No ☐
2021-22 Integrated Risk Management Priorities
No ☐
2021-22 Priorities
No ☐ ☒ Prove Patients Matter Most ☒ Staff and Physician Wellbeing ☒ Accelerating Access to Care ☐ Increase Joy in Work ☒ Length of Stay ☒ Keeping Staff and Physicians Safe and Engaged ☒ Lead Boldly ☒ CRP Phase 3 ☒ Executing CRP Phase 3 ☐ Multi-year Fiscal & Capital Strategy ☒ Completing our HIS Evaluation
Recommendation/Motion Proposed Board Motion: That the recommended privileges for ratification and granting be approved as presented to the Board. Committee motion: Applications for privileges as displayed be approved. CARRIED
BRIEFING NOTE
127

Agenda Item 3.4.2
Page 2 of 5 May 2021(2)
Credentialing Files for Review (May 2021 Credentials Committee):
Name Department Specialty Appointment Reason Supervisor Recommended/ Not
Recommended
Comments
Dr. Greg Hall
Emergency Courtesy with Admitting
Relinquishing privileges at end of current cycle, has not worked here for years
Dr. Arthur Eugenio
☐ Recommended ☒ Recommended with comments ☐ Not Recommended
Privileges will be relinquished at the end of this cycle (June 30, 2021)
Dr. Jatinder Juss
Medicine Internal Medicine
Locum Requesting an extension of locum privileges from July 1 – Dec 31, 2021
Dr. Augustin Nguyen
☒ Recommended ☐ Recommended with comments ☐ Not Recommended
Dr. Steven Wong
Emergency Locum Requesting Locum Privileges from July 1, 2021 – July 1, 2022
Dr. Arthur Eugenio
☒ Recommended ☐ Recommended with comments ☐ Not Recommended
Dr. Kaiser Qureshy
Surgery ENT Locum Requesting extension of locum privileges for regional on-call from June 2, 2021 – June 30, 2022
Dr. Ingrid Whitehead
☐ Recommended ☒ Recommended with comments ☐ Not Recommended
Query transition to Courtesy – will work with Dr. Whitehead to transition
128

Agenda Item 3.4.2
Page 3 of 5 May 2021(2)
Name Department Specialty Appointment Reason Supervisor Recommended/ Not
Recommended
Comments
Dr. Ali Almhri
Medicine Internal Medicine
Locum Requesting an extension of locum privileges from July 1 – Dec 31, 2021
Dr. Augustin Nguyen
☒ Recommended ☐ Recommended with comments ☐ Not Recommended
Dr. Mohammed Farooqi
Medicine Internal Medicine
Locum Requesting an extension of locum privileges from July 1 – Dec 31, 2021
Dr. Augustin Nguyen
☒ Recommended ☐ Recommended with comments ☐ Not Recommended
Dr. Patrick Lindsay
Medicine Internal Medicine
Locum Requesting an extension of locum privileges from July 1 – Dec 31, 2021
Dr. Augustin Nguyen
☒ Recommended ☐ Recommended with comments ☐ Not Recommended
Dr. Tianyang Dai
Medicine Oncology Division
GPO Locum Requesting locum privileges from July 1, 2021 – Jan 1, 2022
Dr. Lyndsay Evans
☒ Recommended ☐ Recommended with comments ☐ Not Recommended
Dr. Haseeb Naveed
Emergency Locum Requesting locum privileges from Aug 1, 2021 – Aug 1, 2022
Dr. Arthur Eugenio
☒ Recommended ☐ Recommended with comments ☐ Not Recommended
Has EM
129

Agenda Item 3.4.2
Page 4 of 5 May 2021(2)
Name Department Specialty Appointment Reason Supervisor Recommended/ Not
Recommended
Comments
Dr. Jasmine (Ching Ho) Tsang
Psychiatry Psychiatrist Associate Resigning from Associate staff effective July 16, 2021
Dr. Anjali Sharma
☒ Recommended ☐ Recommended with comments ☐ Not Recommended
Dr. Mary Mathews
Hospital Medicine
Hospitalist Locum Requesting an extension of locum privileges from June 2 – Sept 2, 2021
Dr. Jenny Legassie
☒ Recommended ☐ Recommended with comments ☐ Not Recommended
Dr. Tanu Sharma
Hospital Medicine
Hospitalist Active – moving to locum
Resigning Active privileges effective July 19, 2021 and switching to locum
Dr. Jenny Legassie
☒ Recommended ☐ Recommended with comments ☐ Not Recommended
Ms. Paige Leslie
Women & Children’s Midwifery
Midwife Associate Resigning privileges effective June 20, 2021
Ms. Corine Witteveen
☒ Recommended ☐ Recommended with comments ☐ Not Recommended
2021 E-Reappointment Applications for Approval DEPARTMENT OF EMERGENCY Dr. Derek Poon DEPARTMENT OF FAMILY MEDICINE Dr.Gerald Achtymicuk - Active Dr. Mekalai Kumanan – Active
130

Agenda Item 3.4.2
Page 5 of 5 May 2021(2)
DEPARTMENT OF HOSPITAL MEDICINE Dr. Tudor Ponoran – Active DEPARTMENT OF INTERNAL MEDICINE Dr. Alaa Alhendi – Courtesy with Admitting Dr. Hem Jain – Affiliate DEPARTMENT OF PEDIATRICS Dr. Ashish Porwal - Active DEPARTMENT OF RADIOLOGY Dr. Olfat Kamel Hasan – Courtesy without Admitting DEPARTMENT OF SURGERY Dr. Paul Mathew - Active
131

CMH COVID-19 Dashboard – June 25th
Waterloo Region ICU
Capacity
ICU CRCI ICU CRCI Vented Total % Occupancy
CMH 7 7 76%GRH 12 8 72%GGH 3 2 62%SMGH 6 5 62%
Ontario New Cases
Rolling 7 Day
CRCI in ICU
Rolling 7 day avg CRCI in ICU
% Vaccine 1 Dose
% Vaccine 2 Dose
256 292 299 322 75.83% 29.08%
Total Active Covid-19 Cases @ CMH : 77 Day Average Active Covid-19 Cases @ CMH : 10
WaterlooRegion
New Cases
Rolling 7 Day
CRCI in ICU
Rolling 7 day avgCRCI in ICU
% Vaccine 1 Dose
% Vaccine 2 Dose
63 58 28 27 75.58% 23.44%
132
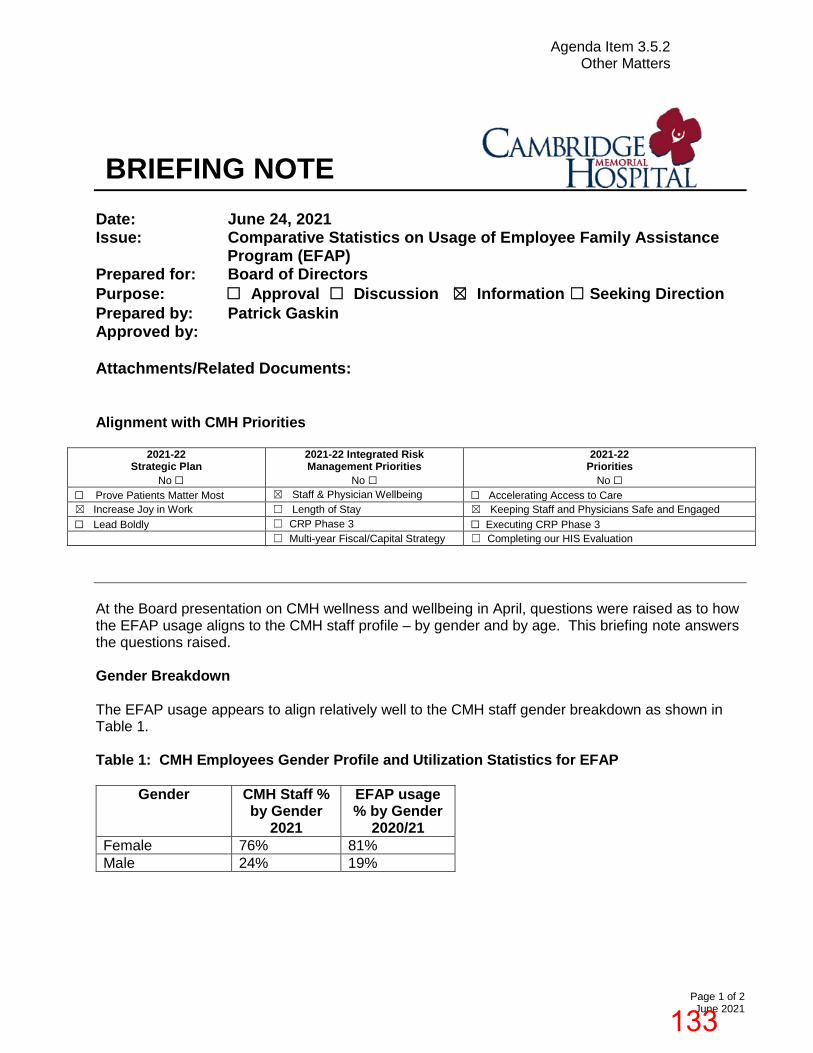
Agenda Item 3.5.2 Other Matters
Page 1 of 2 June 2021
Date: June 24, 2021 Issue: Comparative Statistics on Usage of Employee Family Assistance
Program (EFAP) Prepared for: Board of Directors Purpose: ☐ Approval ☐ Discussion ☒ Information ☐ Seeking Direction Prepared by: Patrick Gaskin Approved by: Attachments/Related Documents: Alignment with CMH Priorities
2021-22 Strategic Plan
No ☐
2021-22 Integrated Risk Management Priorities
No ☐
2021-22 Priorities
No ☐ ☐ Prove Patients Matter Most ☒ Staff & Physician Wellbeing ☐ Accelerating Access to Care ☒ Increase Joy in Work ☐ Length of Stay ☒ Keeping Staff and Physicians Safe and Engaged ☐ Lead Boldly ☐ CRP Phase 3 ☐ Executing CRP Phase 3 ☐ Multi-year Fiscal/Capital Strategy ☐ Completing our HIS Evaluation
At the Board presentation on CMH wellness and wellbeing in April, questions were raised as to how the EFAP usage aligns to the CMH staff profile – by gender and by age. This briefing note answers the questions raised. Gender Breakdown The EFAP usage appears to align relatively well to the CMH staff gender breakdown as shown in Table 1.
Table 1: CMH Employees Gender Profile and Utilization Statistics for EFAP
Gender CMH Staff % by Gender
2021
EFAP usage % by Gender
2020/21 Female 76% 81% Male 24% 19%
BRIEFING NOTE
133

Agenda Item 3.5.2 Other Matters
Page 2 of 2 June 2021
Age Breakdown The EFAP usage as a percentage by age is relatively comparable to the staff age breakdown for the 31 to 40 and 41 to 50 age groups. This collective age cohort (31-50) accounts for 47% of the CMH staff. Other age cohorts are not as well aligned to their EFAP usage. At this time, the reasons for this are not known. This may be explored more through the work of the Employee Engagement Council and through the work associated with the wellness and well-being program. Table 2: CMH Employees Age Profile and Utilization Statistics EFAP
Age CMH Staff % by Age 2021
EFAP usage % by Age 2020/21
< = 20 2% 14% 21 – 30 23% 18% 31 – 40 24% 24% 41 – 50 23% 26% 51 – 60 21% 14% 61+ 8% 4%
134
Recommended

















