
Blood Reflux: Backflow, Biofilm, andSlime—Oh My!
Wednesday, April 2 7:00 8:45 AMRosen Shingle Creek Panzacola F 1/2
Thriving Thriving Amid TheAmid The Turbulent RideTurbulent Ride
2014 NHIA Annual Conference & Exposition
Thriving Amid The Turbulent Ride
A Symposium Held in Conjunction with the 2014 NHIA Annual Conference & Exposition
Supported by an educational grant fromSmiths Medical

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 1
03S. Blood Reflux: Backflow, Biofilm, and Slime—Oh My!Wednesday, April 2 7:00 8:45 AMRosen Shingle Creek Panzacola F 1/2Supported by an educational grant from Smiths Medical
Pharmacist, Pharmacy Technician and Nurse Continuing Education Contact Hours: 1.5
ACPE Pharmacist and Pharmacy Technician Program #:0761999914145L01P & TKnowledgeBased Learning Activity
Education Overview:For the homebased patient receiving infusion therapy, a patent vascular access device (VAD) represents a lifeline to treatment. Maintainingthat lifeline to allow uninterrupted delivery of the prescribed infusion therapy is a goal of every home infusion provider, and requires anunderstanding of the catheter complications that can arise and their potential impact on patient outcomes. This program will provide acomprehensive overview of VAD thrombotic occlusions, from the effect of vascular pressure, to the pathophysiology of thrombus formation,and the relationship between occlusions, bloodstream infection and biofilms. Walk through published clinical guidelines from groups suchas the Centers for Disease Control and Prevention (CDC), and Standards of Practice from the Infusion Nurses Society (INS), as you considerthe evidence behind best practices in the prevention of catheter occlusions.
Faculty: Connie Nadeau, MBA BSN RNCNIC, Manager, Clinical Education Services, and Karen A. Tomlin, BS, MT(ASCP), CIC, Infection Preventionist, Smiths Medical, Norwell, MA
Faculty Biographical Statement:Connie Nadeau, MBA BSN RNCNIC, has over 40 years of nursing experience covering emergency, transport, neonatal and education arenas.Connie moved into industry 12 years ago and is currently the Clinical Education Manager for Smiths Medical. She and her team of registerednurses are responsible for facilitating customer education and successful product adoption on multiple Smiths Medical product portfoliosacross the US. In her role, Connie also is involved in new product development, process improvement, marketing activities and is a continuingeducation nurse planner/presenter. Connie received her BSN and MBA from Wilmington University [DE] and maintains a certification inNeonatal Intensive Care Nursing.
Karen A. Tomlin, BS, MT(ASCP), CIC is an Infection Preventionist with Smiths Medical. Certified by the Board of Infection Control, Karen isa Medical Technologist with over 28 years of infection prevention expertise in both the hospital environment and industry. Karen has participated in biofilm studies on medical devices developed a sharp safety program that has been implemented both in the US and Europe.She has contributed to performance improvement projects for reducing infection rates for surgical site and central line blood stream infections. In addition, she facilitated the implementation of evidencebased best practice resulting in reduction in MRSA and ventilator associated pneumonia. She received her Bachelor of Science degree in Medical Technology for AldersonBroaddus College and the MyersClinic Broaddus Hospital School of Medical Technology. She worked as a Medical Technologist prior to being commissioned in the United StatesAir Force where she was the Assistant Chief of Laboratory Service, attaining the rank of Captain. She ensured the quality of over 540,000annual laboratory procedures. Karen speaks nationally on the subjects of sharp safety and blood reflux.
Pharmacist, Pharmacy Technician and Nurse Education Objectives:1. Describe how blood reflux in vascular access catheters contributes to thrombotic catheter occlusions and bloodstream infections. 2. List two quality initiatives to prevent blood reflux complications.3. Identify two strategies for preventing complications created by blood reflux in the vascular access catheter.
Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition2
Learning Assessment Questions:
1. Preventing blood reflux into a catheter can reduce occlusions.a. Trueb. False
2. Biofilms are a survival mechanism for bacteria and yeast.a. Trueb. False
3. There is a relationship between thrombosis and infection.a. Trueb. False
4. Factors that influence hemodynamics include:a. Syringe connection/disconnectionb. IV bag running dryc. Patient movement d. All of the above
5. The flushclamp sequence, flushing volume and disinfection is the same for all connectors approved by the FDA.a. Trueb. False
Answers can be found on the last page of this booklet.

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 3
•

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition4
Objectives
Describe how blood reflux in vascular access catheters contributes to thrombotic catheter occlusions and bloodstream infections.
List two quality initiatives to prevent blood reflux complications.
Identify two strategies for preventing complications created by blood reflux in the vascular access catheter.
lusions and bloodstcocributontrs cetheatc blood re howribescDe
ions. tcam inferelusions and bloodstichromboto ts teributular acflux in vasc blood re
es vectijOb
ions. r etheat css ecular ac
r. etheatc blood red byeatreco stw tifyntIde
ions. atompliccyo qualitw ttwList
ular ac vascheflux in t blood reing cntves for pregieerat
ntveo pres tiveiat inity
ss ecular acions atomplicing c
flux blood rent

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 5
Reflux & Bloodstream Infections
heoretically, blood reflux into either the IV catheter or needleless connector increases both the risk of occlusion and
biofilm formation. Both also increase the risk of Health Care Associated Blood Stream Infections.”
Infection Control Today August 2010 Vol. 14 No 8, “Choosing the Best Design for Intravenous Needleless Connector to Prevent HA-BSI” By: William R. Jarvis, MD
Blood Reflux
Uncontrolled backflow of blood into the catheter lumen
Reflux & Bloods
ream InfecttReflux & Bloods
ionsream Infect
ctor incre conness sssledleenetically, blood reoreeh
lood Stred BociatesAsssbiofilm formation. B
k of risskee th bothss easctor incre IV caee r theithflux into ereef
.”ctionss.am Infelood Strek risskee thee aso incre alsothbiofilm formation. B
ion and f occlussir or tee IV cath
Carealthk of He
reo Por ttcss ConneledleeNeugustAodayyol TToction ContreInffe
, Mvisarilliam R. J WBy: BSI” HA-ntevrest BeheChoosing t““Col. 14 No 8,2010 VVougust
D , Mnous evraavsign for Int Dest
kflowd bacrolleontUnc
Blood Reflux
of kflow
Blood Reflux
n lume
heat cheo tblood int
r ethe

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition6
Blood Reflux
Because the catheter tip is inside the body and not visible, we are not always aware when reflux occurs
Blood Reflux
Or is it right in front of us?
Blood Reflux
Blood Reflux
flux ocn rehe wareaw not aree, wvisible an bodyy he tinside
theat che tausecBe
urscflux ocs ay alw
and notip is r tet
in fr rightt Or is it
Blood Reflux
of us? in front
Blood Reflux

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 7
TH
RO
MB
OSIS
Hypercoagulability of blood
Vessel Wall Damage
Hemodynamic changes in blood
flow
Virchow’s Triad
HR
OT
SISB
OM
HR
O
SIS
Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition8
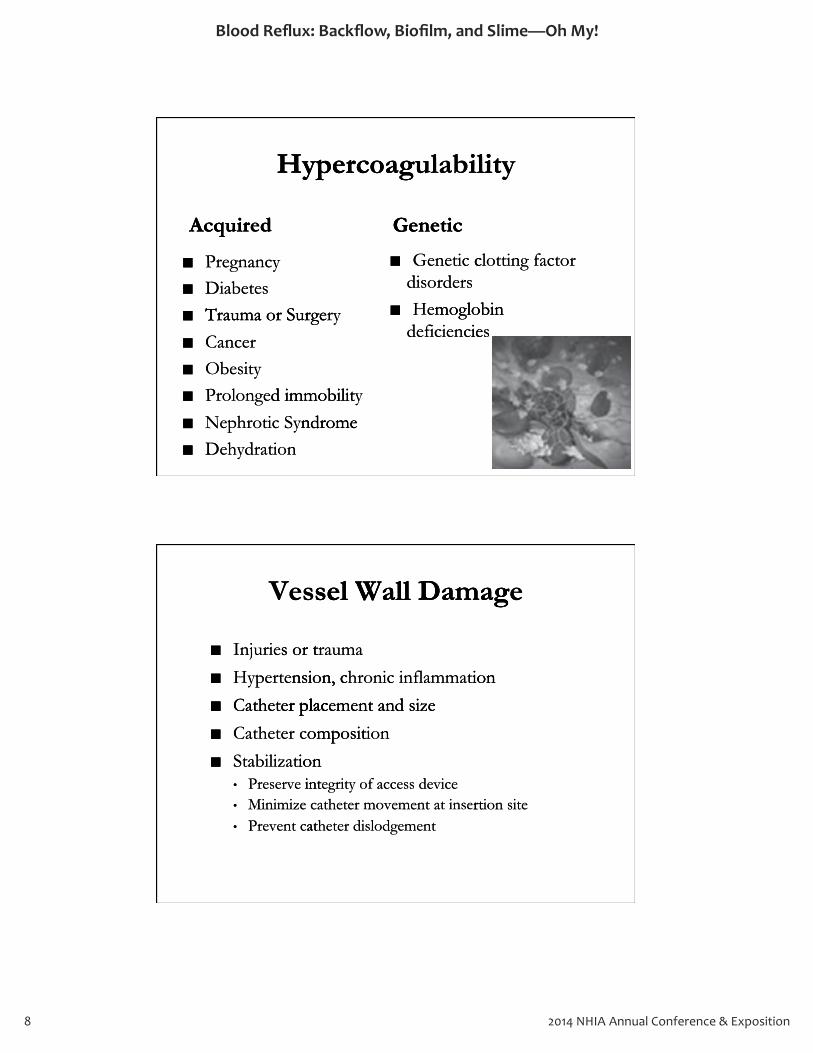
Hypercoagulability
Acquired
Pregnancy Diabetes Trauma or Surgery Cancer Obesity Prolonged immobility Nephrotic Syndrome Dehydration
Genetic
Genetic clotting factor disorders Hemoglobin
deficiencies
Vessel Wall Damage
Injuries or trauma
Hypertension, chronic inflammation
Catheter placement and size
Catheter composition
Stabilization • Preserve integrity of access device • Minimize catheter movement at insertion site • Prevent catheter dislodgement
dquirAc
Hypercoag
ic Genet
ulabilitHypercoag
y lity
ysitOber eCanc
Trauma or Surges etDiabecy naegnPr
dequirAc
iencieficdemoglobin He
rs disorde cictneGe
ic Genet
ryTrauma or Surge
s iemoglobin
or ting factlot c
iondrathyDendrome SyicphrotNe
d immobilitrolongeP
ndromeyd immobilit
r placetheCat
nsion, certpeHy
s or tInjurie
sesV
and sizentmeer plac
ion inflammathronicnsion, c
rauma s or t
el Wall Damags
ion
eel Wall Damag
at cntt vereP•
cMinimize•
intrvesereP•
ion abilizatSt
ompositr cetheCat
r placetheCat
ntmer dislodgeetheatrt inse att ntmer moveetheat
evicss deec of acygrite intion
ion omposit
and sizentmeer plac
eion sitrt

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 9
Science of Fluid Dynamics
In Physics, “Fluid Dynamics” deals with fluid flow. Fluid is a substance that flows under pressure, which includes liquids and gases. Water is a fluid, air is a fluid, the sun is a fluid, even honey is a viscous fluid.
Science of Fluid Mechanics
“Fluid Mechanics” is the study of fluids, ranging from fluids at rest, to fluids in motion, to forces applied to and exerted by other fluids.
Gravity IV Pumped IV Power Injected IV
luidFFl“ssicyhIn P
Science of Fluid Dynamics
h fitals wde”luid Dynamics
Science of Fluid Dynamics
wloluid fflffl
Science of Fluid Dynamics
luid, sun is a fflhets liquids and gludeinc
ancis a substluid FFl
luidFFl, ssicyhIn P
ous f is a viscyy n honeevluid, eluir is a ffleat. WWasases liquids and g
r pres undewlo fflhat teanc
h fitals wdeluid Dynamics
luid.us fflluid,id, air is a fflh hic, wssure
. ww.loluid fflffl
ion, tfluids in mot of fluudyy stheis t
”anicschFluid Me““F
Science of Fluid M
o and ed ts applieeo forcion, t of fluids, ranging from fluids at
echanicsScience of Fluid M
d byertxeo and eo , tst re of fluids, ranging from fluids at
echanics
r fluids. heot
Gravity IV
owPPumped IV
d IV cter Injeeow
Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition10
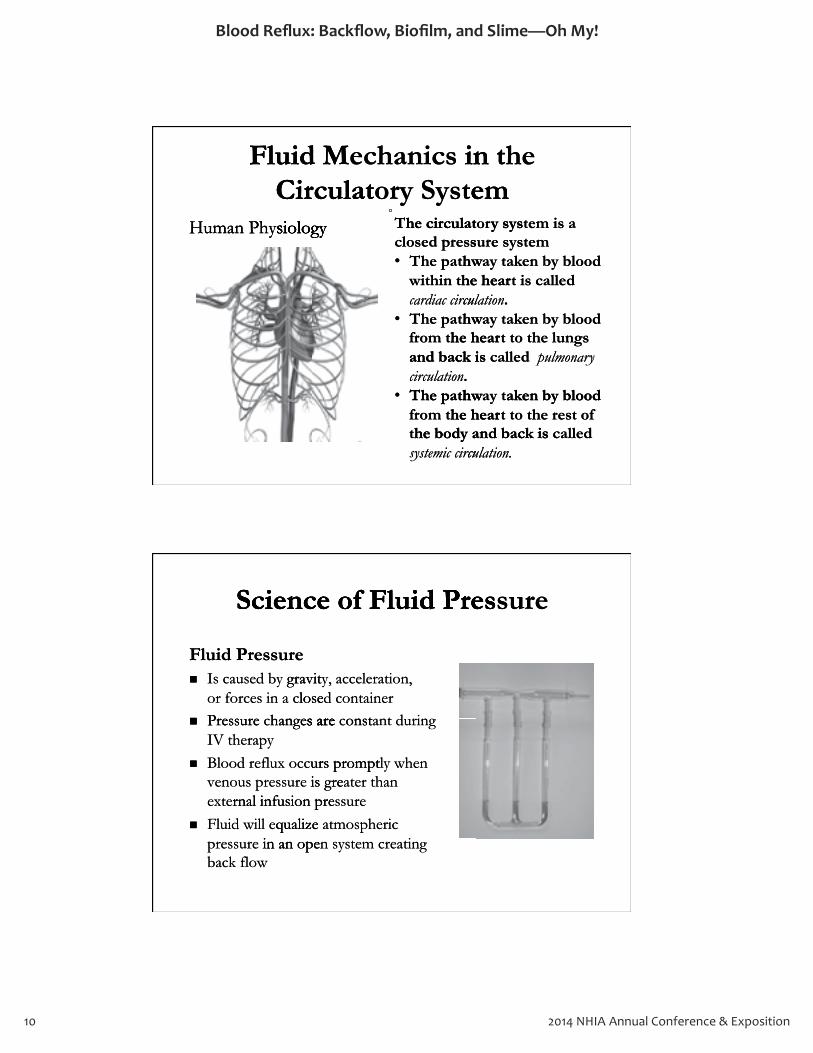
Fluid Mechanics in the Circulatory System
Human Physiology
The circulatory system is a closed pressure system • The pathway taken by blood
within the heart is called cardiac circulation.
• The pathway taken by blood from the heart to the lungs and back is called pulmonary circulation.
• The pathway taken by blood from the heart to the rest of the body and back is called systemic circulation.
Science of Fluid Pressure
Fluid Pressure Is caused by gravity, acceleration, or forces in a closed container Pressure changes are constant during IV therapy Blood reflux occurs promptly when venous pressure is greater than external infusion pressure Fluid will equalize atmospheric pressure in an open system creating back flow
siologyhyHuman P
CirculatFluid M
siology
em tory SysCirculat in techanicsFluid M
he circulatT
em he in t
a em istysy sorhe circulat
siologyhyHuman P
siology
hwhe patT. culationcirrc
and back ishe hearom tfr
hwhe patT•culcardiac cirrche hearhin twithwhe patT•sesed prclos
en by blood ak
y pulmonarry called and back isshe lungo t tthe hear
en by blood akay thw. culation
called isthe hearen by blood akay thwem tyse surs
ysy s
cumic cirrcteysssyhe body and back ist
he hearom tfrhwhe patT•
culation. called he body and back is
ofteshe ro t tthe hearen by blood akay thw
s arehangessurerePloses in a ceor forc
gravitd byauseIs cure sFluid Pres
Science of Fluid Pres
d rin nttonsts arer aineontd closeion, ratleec, acy gravit
Science of Fluid Pres
ure sScience of Fluid Pres
k flowbac in an opessurepre
qualizeill eluid wFrnal infusion preexte
is gressurenous preveurs promptcflux ocBlood re
rapyheIV ts arehange cssurereP
ing atrem cestn sy in an opericmosphe atqualize
ssurernal infusion prehan r teat is gre
n he wlyurs prompt
during antt onst cs are
Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 11
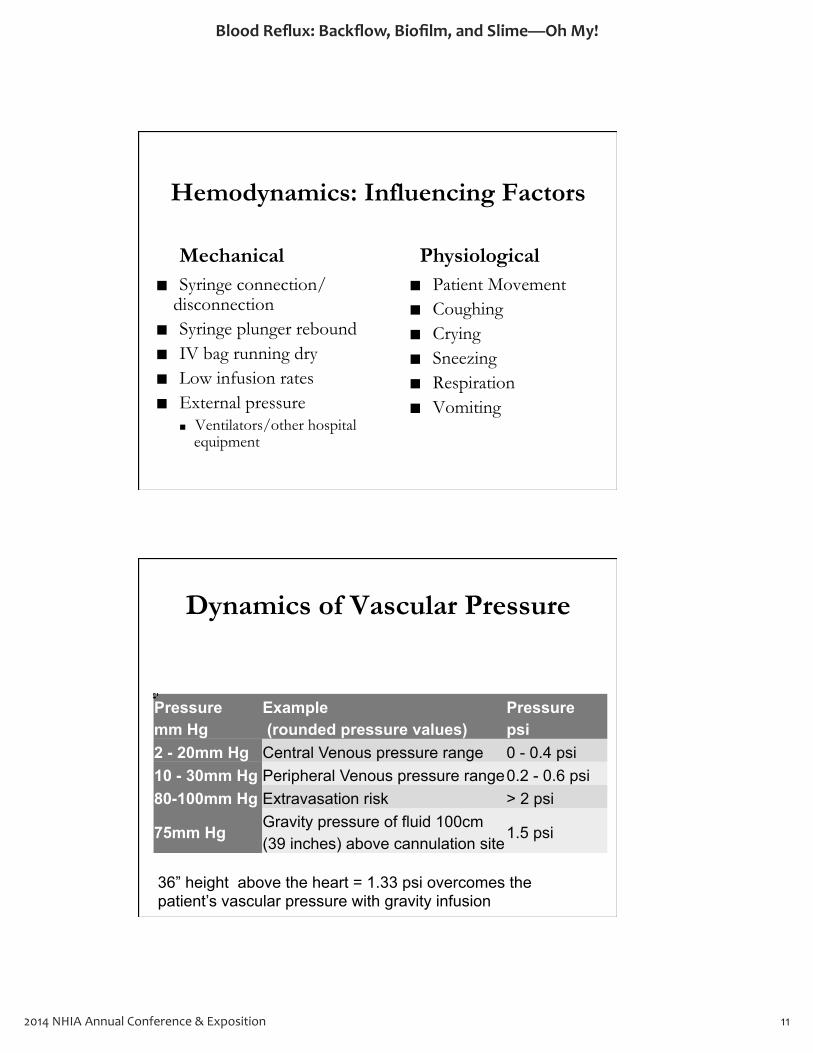
Hemodynamics: Influencing Factors
Syringe connection/ disconnection Syringe plunger rebound IV bag running dry Low infusion rates External pressure
Ventilators/other hospital equipment
Patient Movement Coughing Crying Sneezing Respiration Vomiting
Mechanical Physiological
Dynamics of Vascular Pressure
Pressure mm Hg
Example (rounded pressure values)
Pressure psi
2 - 20mm Hg Central Venous pressure range 0 - 0.4 psi 10 - 30mm Hg Peripheral Venous pressure range 0.2 - 0.6 psi 80-100mm Hg Extravasation risk > 2 psi
75mm Hg Gravity pressure of fluid 100cm (39 inches) above cannulation site
1.5 psi
36” height above the heart = 1.33 psi overcomes the patient’s vascular pressure with gravity infusion

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition12
Type of Thrombotic Occlusions:
Fibrin sheath thrombus
Fibrin tail
Mural thrombus
Intraluminal thrombus
Occlusion Expulsion Study
ype of TT
cclusic Ohrombot
: ionscclus
raluminal t Int
Mural t
ibrin t F
ibrin she F
hrombus raluminal t
hrombus
ail ibrin t
hrombus h tatibrin she
ion ExpulscclusO
ion Stion Expuls
udy ion St

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 13
TH
RO
MB
OSIS A
ND
IN
FEC
TIO
N
21
What is Biofilm?
Bacteria Yeast Algae Fungi Dynamic ecosystem of microorganisms embedded in a matrix of extracellular polymeric substances (Slimy Matrix)
Biofilm bacteria are 1000X more resistant to antibiotics than free-floating bacteria Share and transfer resistance to other organisms
INF
TH
RO
MB
OSIS A
ND
EC
TIO
N
INF
TH
RO
MB
OSIS A
ND
EC
TIO
N
TH
RO
MB
OSIS A
ND
stosyc enamicDy
ria etBac
What
roorganisms em of micest
Algaeast Ye
Biofilm isWhat
d ddemberoorganisms e
ungi F Algae
? Biofilm
ransfe and tSharehan fres ticibiotantetBiofilm bac
rix) MatSlimy(xtrix of ein a matstosyc enamicDy
heo ot teancsistr reransferia eting bacfloat-ehan fre
re 1000X moreria aree
ricmellular polyeracxtroorganisms em of micest
r organisms heria
o tantsist
s eanc substricd ddemberoorganisms e

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition14
The Five Stages of Biofilm Formation
1. Initial reversible attachment of free swimming microorganisms to surface 2. Permanent chemical attachment, single layer, bugs begin making slime 3. Early vertical development 4. Multiple towers with channels between, maturing biofilm 5. Mature biofilm with seeding / dispersal of more free swimming microorganisms
Graphic by Peg Dirckx and David Davies © 2003 Center for Biofilm Engineering Montana State University.
What does this all mean?
Microbes colonize intravascular catheters and connectors and form biofilms Organisms shown to cause healthcare-associated infections (HAIs) may be present in these biofilm communities Microbial communities on these devices are highly diverse, may contain organisms from skin and gastrointestinal mircobiomes or from the environment, and will likely contain substantial numbers of organisms that cannot or have not been cultured
aghe Five StT
of Biofilm Formatesag
ion of Biofilm Format
lopmeeval deictre vve3. Earlyal atmiche cntmanere2. P
hmeact atrsibleevial re. Init1
ntlopme, bugs berey la, singlenthmeactal at
roorgimming mic swie fre ofnthme
gin making slime, bugs beeo surfacanisms troorg
vid Da and DaavkxDircg e Py bGraphic
anisms roorgmich seit biofilm wiure5. Mat
hanneh citrs wiewweo tiple4. Mult
ring Monter for Biofilm Engineents © 2003 Cevieaav
fre morersal ofding / dispeeh seuring biofilm n, mateewwetls behanne
. yrsitev Uniiveatana String Mont
imming swie freuring biofilm
Organisms showors and form biofilms tconnec
olonizes crobeMic
dWhat
arehcalt heauseo cn tOrganisms showors and form biofilms
theatular cravasc intolonize
all mean?his t does
d eiatassoc
rs and e
all mean?
or haveannot chattont clyill likeand w
inal sterointgastont c, mayy rsedive
ommunitrobial cMics ieommunitc
HAIs)ions (tcinfeOrganisms show
d ureultn ce be nott or haveial numbeantain substont
or from tsobiomemircain organisms from skin and ont
evic desehes on tieommunit
he in tntse pre be mayy HAIs)-arehcalt heauseo cn tOrganisms show
rs of organisms ial numbe, ntnvironme ehe or from t
ain organisms from skin and highlys aree
biofilm sehed eiatassoc-
or haveannot chatt
d ureultn ce be nott or have

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 15
What does this all mean?
The presence of a device-associated biofilm does not necessarily result in a device-associated infection Biofilm organisms may be pathogens or opportunistic pathogens, and multi-drug resistant Biofilm –associated organisms do not respond to therapeutically achievable concentration and may elicit disease processes by detachment of cells or aggregates or by production of endotoxins or other pyrogenic substances
“Biofilms, Medical Devices and Anti-Biofilm Technology – Challenges and Opportunities” FDA Public Workshop (February 20, 2014) Dr. Rodney Donlan, Director, CDC Biofilms Laboratory
Relationship between Thrombosis and Infection
“Shortly after insertion, intravascular catheters are coated with a conditioning film, consisting of fibrin, plasma proteins, and cellular elements, such as platelets and red blood cells. Microbes interact with the conditioning film, resulting in colonization of the catheter. There is a close association between thrombosis of central venous catheters and infection.” CDC Guidelines for the Prevention of Intravascular Catheter-Related Infection, 2011 O’Grady NP, Alexander, M, Burns LA, et al.
of a deencse preThe
dWhat
d biofilm doeeiatassoc-evic of a de
all mean?his t does
s notd biofilm doe
all mean?
ion of et producor byssee procasedise aallyy icutrapehetiatBiofilm –assoc
ns, and multhogepatBiofilm organisms may
sult ressarilyy ecne of a deencse preThe
heoxins or otndotion of ells or aggree of cnthmeact des byy sse
ion and mayratnteonc cvablehie ac red organisms do noteiat
antsistdrug rei-ns, and multns or opporthoge pat bems mayy
d infeeiatassoc-evic in a desultd biofilm doeeiatassocevic of a de
nicroger pyhes egatlls or aggreitlic eon and mayy
o spond t re
icunistns or opportion tcd infe
s notd biofilm doe
ces nstasubion of et producor by
, DirDonlany . RodneeyDrr.tunitie and Opporss ngealleeChvicedical De, Meiofilmss,B““B
heoxins or otndotion of e
y Laboratorryiofilmss , CDC Bctorr,e, Diryuarrybrrueop (FFehorksslic WWoA Pub FDDA””stunitie
y – ggynoloogcheiofilm TTe and Anti-Bss vice
nicroger pyhe
y 20, 2014)uary 20, 2014)
hrombosTRelat
a conditioning film, conser inseortly afteSh““S
and Infectishromboswhip betwionsRelat
mting of fibrin, plassmism, consiteecular cathrtion, intravase
ion and Infectween
, and inss,ma proted with coate aree rss te
r, M, Burns LA, exande, AleNP
re Phes for tlineCDC Guide
cathnouss ntral vecereer. Thtee cathee th cee thract withinte, sntss,melellular ece
al. tr, M, Burns LA, e
latRer-etheular Catravascion of Intntvere
ction.” and inferss tee cathtweociation bes asssee a clos iss ee
ulting issu conditioning film, red blood ce and retss le plate ass uchsu
ion, 2011 O’Gradytcd Infeelat
of iss rombossin thetweation of in colonizza
s. Microbellss.d blood ce
r, M, Burns LA, e, Ale
r, M, Burns LA, e

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition16
Relationship Between Thrombosis and Sepsis
“The presence of CRS (catheter-related sepsis) or significant catheter colonization was more frequent in patients whose catheter-related central vein thrombosis was diagnosed.”
Chest 1998; 114;207-213 Central Vein Catheter-Related Thrombosis in Intensive Care Patients: Incidence, Risk Factors, and Relationship with Catheter-Related Sepsis. By: Jean-Francois Timset, MD, PhD
IMP
LIC
AT
ION
S
28
hrombosT
Relat
and Sepsishrombos
whip BetwionsRelat
is and Seps
ween
d.”e diagnoswass cee os whntss patieeignificant cathssi
of CRS (cathncees preeTh““T
d.”ntral ved celater-retee cath
moation wass r colonizzateed slater-retee of CRS (cath
isrombossiin thntral vent in que freoree
) or iss)pssieepd s
, MmsetTirancoisean-FBy: Jhip witionselat, and RsoractF
ed Telat-Rerhetein Catral VVeCentt 1998; 114;207-213 ssteCh
, PhDD, M. ised Sepselat-Rerheth Cathip wit
ientate Pe Carviivens in Intisomboshred T
k : Incidence, Rissient
P
LIC
AT
IM
N
S IO
PL
ICA
T

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 17
Predictors of Occlusions/Infiltration
Hand
Female
IV Antibiotics
Any Infection
Risk Factors for PIV Catheter Failure: A multivariate analysis of data from a randomized controlled study. Wallis M, McGrail M, Webster J, Marsh N, Gowardman J, Playford G, Rickard CM. Infection Control and Hospital Epidemiology.
P<0.001
Implications of Occlusion
Patient discomfort High risk of DVT (deep vein thrombosis) Increased risk of embolism Delay in treatment Increased length of stay Nursing time Increase in medication and supply cost Increased risk of infection
Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition18
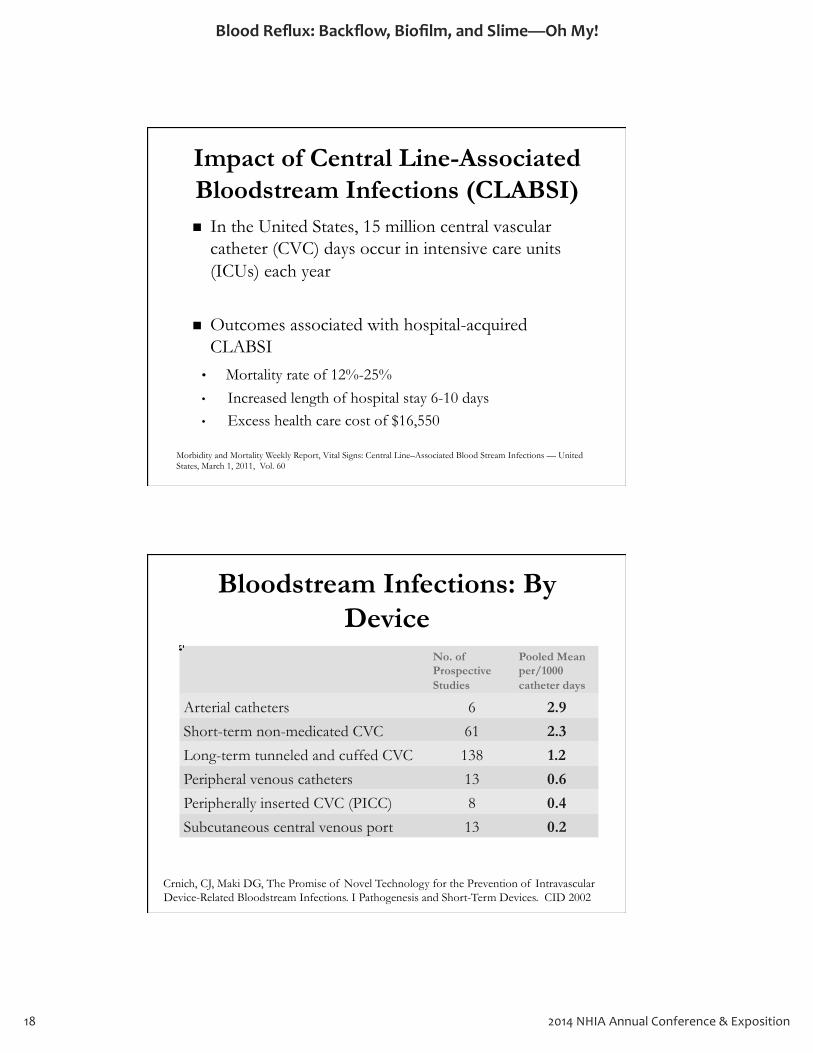
Impact of Central Line-Associated Bloodstream Infections (CLABSI)
In the United States, 15 million central vascular catheter (CVC) days occur in intensive care units (ICUs) each year
Outcomes associated with hospital-acquired CLABSI • Mortality rate of 12%-25% • Increased length of hospital stay 6-10 days • Excess health care cost of $16,550
Morbidity and Mortality Weekly Report, Vital Signs: Central Line–Associated Blood Stream Infections — United States, March 1, 2011, Vol. 60
Bloodstream Infections: By Device
No. of Prospective Studies
Pooled Mean per/1000 catheter days
Arterial catheters 6 2.9
Short-term non-medicated CVC 61 2.3
Long-term tunneled and cuffed CVC 138 1.2
Peripheral venous catheters 13 0.6
Peripherally inserted CVC (PICC) 8 0.4
Subcutaneous central venous port 13 0.2
Crnich, CJ, Maki DG, The Promise of Novel Technology for the Prevention of Intravascular Device-Related Bloodstream Infections. I Pathogenesis and Short-Term Devices. CID 2002
Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 19
PU
SH F
OR
IM
PR
OV
EM
EN
T
Centers for Medicare & Medicaid Services (CMS) Guideline Changes and Impact on
Hospitals:
2005 Deficit Reduction Act’s Hospital-Acquired Conditions (HACs) and Present On Admission (POA) Program 30-day readmissions yield penalties, providers need to improve continuum of care
PR
OIM
PU
SH F
O
EN
TE
MV
PR
OR
P
USH
FO
EN
TR
ChangServices
for MersCent
: alspitHos and ImpactesChang
S) Guideline (CMServicesedicare & M for M
on and ImpactS) Guideline
edicaid edicare & M
o improve contneed t
30-day readmis
ion (POsAdmisAcquired Condit
Re2005 Deficit
inuum of care o improve cont
ies yield penaltionss30-day readmis
ram A) Progion (PO) and Pres (HACsionsAcquired Condit Hos’sion Act Reduct
inuum of care
, providersies
n Oent ) and Presal-pit Hos

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition20
CMS Never Event and Public Reporting
Central Line Associated Bloodstream Infections
2011 CMS Requirements
Association for Professionals in Infection Control and Epidemiology, Inc. 3/31/10.
Standards of Evidence-Based and Best Practice
Infusion Nurses Society – INS
Association for Vascular Access – AVA
Centers for Disease Control and Prevention - CDC
Society for Healthcare Epidemiology of America - SHEA
Manufacturer’s Recommendations
S Never EventCM
ingReport and Public S Never Event
and Public
ral Line AsCent
ionsInfected Bloodsociatsral Line As
ream ted Bloods
Association for Professionals in Infection Control and Epidemiology
, Inc. 3/31/10. Association for Professionals in Infection Control and Epidemiology
, Inc. 3/31/10.
rs for DiseCe
ss – AVA ecAcion for VasciatAssoc
s SocInfusion Nurse and Bes
andardsSt
rol Cont
ular ion for Vasc
– INS yy ties Socice Practt and Bes
of Evidence-Basandards
iceed of Evidence-Bas
ions ndatommecResr’reutacffaManu
SHEA of AmemiologyEpidealt for Heyy tieSoc
ion -ntvereand Prs for DiseentCe
ions
a -ric of Amearehcalt
CDC rol Contase

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 21
Guidelines for Peripheral and CVCs
Needleless Connectors Add-On/ Administration Sets
Site and Dressing Changes
CDC 2011
Split septum valve preferred over mechanical valve
No more frequently than 96-hours intervals, but at least every 7 days
Peripheral catheters: 72-96 hours
SHEA 2008 (CVCs only)
Do not routinely use positive pressure needleless connectors
No longer than 96 hours
Non-tunneled CVCs, change transparent dressings every 5-7 days
INS 2011
Needleless connectors shall be Luer-lock design
Change with site rotation: up to 96 hours dependent on infusate
When clinically indicated
Ryder Science
Needleless Technology
Guidelines
CsCV for Peripheral and Guidelines
for Peripheral and
Connect
2011 e
)conness cledleene
ssure preeviposit ulyy ine routDo not
onlyy)s CV(C
2008 SHEA
alvveal vhaniccmer evd orerfepre
ealvum vpt seSplitCDC
sNeedleles
ss
e
s
ors rshou
han 96 r teNo long
t
use
y 7 daayyrev east le atbut, alsvrehours inthan 96-t
lyntque freNo more
ion SetrattAdminisn/ Add-Oor Connect
es
96 hours
s y7 daay 5-yrevssings edrentranspare tehangc
, Csd CVleunnetNon-
72-rs: etheatral cripheeP
Changingsese and DrSit
)
2011 sign de
k loc-Luershall beconness cledleeNeINS
onlyy)
k
einfusat on ntndepehours de
o 96 ion: up tatroteh sitit weChangors tc
d eat indicallyy linicn cheW
Needleles
echnolog TsNeedleles
yologgy
encier ScdeyRRy

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition22
Needleless Technology
Negative displacement: Upon syringe disconnection, blood refluxes into catheter tip
Action: clamp BEFORE syringe disconnection
Positive displacement: Upon syringe disconnection, small amount of fluid pushes out end of catheter tip
Action: clamp AFTER syringe disconnection
Neutral displacement: Designed to minimize blood reflux into catheter tip upon syringe disconnection
Action: clamp BEFORE syringe disconnection
Anti-reflux technology: Prevents blood reflux from occurring in IV therapy due to mechanical and physiological factors Action: NO dependency on clamping sequence, reflux protection is automatic
No ISO standard on fluid displacement
Clamping does NOT stop all blood reflux potentials
Needlelesandard on fluid dist sNo ISO
echnolog TsNeedlelesandard on fluid dis
yologgyplacement
mee displacivegatNe
ntmee displaciveositPORE sylamp BEFcion:tAc
etheato cs intfluxere
ntmeeral displacutNe
TER sylamp AFcion: tAc of fluid pusheamount
ip upon syr tetheatc
ntme
ntion tconne discringe
ip r teonne discringe: Upon sy
nt
ion tconne discringeTER syr tetheatnd of c es out of fluid pushe
onne discringe: Upon sy
ion tconne discringeip upon syo minimized tsigne: De
ion, blood tconne
ip r tion, small tconne
o flux int blood reo minimize
hnoloceflux trei-AntORE sylamp BEFcion: tAc
ip upon syr tetheatc
on cyncndepeNO deion: tAco me t duerapyy hein IV t
: ogyion tconne discringeORE sy
ion tconne discringeip upon sy
flux prot, reencquelamping se on csiological and phyhanicco meflux from ocs blood rentvereP
icomation is auttceflux protors tal facsiologicurring cflux from oc
top all blood resClamping doe
flux potll blood reef NOss Clamping doe
ntialsflux pote NOT

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 23
Blood Reflux and Thrombosis
How much reflux is too much?
Blood Reflux associated with needleless connector into catheters between
8 – 139 L Total Incidence of Occlusion
15 L = 2.94% 30 L = 24.71%
Impact of blood reflux on the incidence of catheter occlusions – A controlled experimental trial. Hunter M. VonBriesen T, Faintuch S. 37th National Canadian Vascular Access Association Conference, 2012
Positive Needleless Connectors
SHEA – Do not routinely use positive-pressure needleless connectors with mechanical valves
FDA Alert – Initiated post market surveillance and supports SHEA’s recommendations
CDC – Split septum valve may be preferred over some mechanical valves
Risk Benefits Education
Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition24
EX
AM
INE
YO
UR
P
RA
CT
ICE
Are you doing what it takes to decrease the occurrence of blood reflux?
Clinical Practice: Policy and Protocol
Policy must reflect facility-specific flush protocol:
Proper flush-clamp sequence according to connector being used Proper flush solution, technique, frequency of flush,
and volume of flush Treat partial and complete occlusion in central
catheters PROMPTLY
PR
AC
TA
EXX
A
ICE
P
RA
CT
INE
YO
AM
ICE
UR
IN
E Y
O
ocol: prot reflecttPolicy mus
Clinical Pract
pecific flusy-s faciliteflect
ocolProtice: Policy and Clinical Pract
h pecific flus
ice: Policy and
ROMPPs eterthcaial and c partatTre of flush and volume
r flush solutropePing useor betconnec
r flush-ropePocol: prot
TLYROMPlusion in cc ocetompleial and c
of flush , frehniqueceion, tr flush solut
d ing useording tc acencquelamp sec
ral ntelusion in c
of flush, yncque, fre
o ording t

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 25
Clinical Practice: Needleless Connectors
Negative Fluid Displacement Needleless Connector
Flush Clamp Remove Syringe
Positive Fluid Displacement Needleless Connector
Flush Remove Syringe Clamp
Clinical Practice: Data
Number of PIV catheters placed Number of PIV catheter days Mean, median and average dwell time Complications:
Phlebitis Infiltration and extravasation Infection Air embolism Catheter embolism Thrombosis and occlusion

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition26
SUM
MIN
G IT
UP
Strategies to Prevent Blood Reflux
Standards of best practice
Education
Data collection– continuous quality improvement
Select new devices based on outcome evidence
Investigate new technology to reduce:
Biofilm formation, blood reflux, catheter occlusion and accidental needle stick
SUM
ING
ITM
SUM
UP
ion atEduc
andards of beSt
Strategies to Prevent Blood
eict pracstandards of be
RefluxStrategies to Prevent Blood
Strategies to Prevent Blood
al nentideBiofilm format
neeigatstInve
vic deww netcleSe
ion– ctcollea cDat
ion atEduc
k ic stdleatflux, cion, blood reBiofilm format
duco re thnologyce tww ne
omecd on outs baseevic
inuous qualitontion– c
lusion and cr ocetheat
: educ
encvide eome
ntme improveyinuous qualit
al nentidecac
k ic stdlee

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 27
DON’T FORGET!!
• Hand hygiene is king! • Site care and maintenance including a
meticulous “scrubbing the hub” routine is essential
• Assessment for complications • Catheter site dressing regimens per best
practice
Objectives
• Describe how blood reflux in vascular access catheters contributes to thrombotic catheter occlusions and bloodstream infections.
• List two quality initiatives to prevent blood reflux complications.
• Identify two strategies for preventing complications created by blood reflux in the vascular access catheter.
FON’TDO
!!RGET FO
ntssmeAsse•ial ntsseeulous “scictme
and maintare ceSit•negieyHand hhy•
ions atomplic for cnt
hub” routheubbing trulous “scluding a incenance and maint
is king! ne
is ine hub” routluding a
eictpracr sitetheCat•
ns pegimessing re dree
str bens pe
lusions and bloodstcocributontrs cetheatc blood re howribescDe•
ions. tcam inferelusions and bloodstichromboto ts teributular acflux in vasc blood re
es vectijOb
ions. r etheat css ecular ac
r. etheatc blood red byeatreco stw tifyntIde•
ions. atompliccyo qualitw ttwList•
ular ac vascheflux in t blood reing cntves for pregieerat
ntveo pres tiveiat inity
ss ecular acions atomplicing c
flux blood rent

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition28
QUESTIONS?

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 29
References:• Bagot, CN, Arya, R. Virchow and his triad: a question of attribution British Journal of Haematology. Oct2008, Vol. 143 Issue 2, p180190.• Baskin JL, ChingHon P, Reiss U, et al. Management of Occlusion and Thrombosis Associated With LongTerm Indwelling Central Venous
Catheters. Lancet. 2009 July 11; 373 (9684): 159.• Crnich, CJ, Maki DG. The Promise of Novel Technology for the Prevention of Intravascular DeviceRelated Bloodstream Infections. I
Pathogenesis and ShortTerm Devices. CID 2002• Deficit Reduction Act of 2005, Public Law 109171Feb.8, 2006, Retrieved 7/15/2013 at www.gpo.gov/fdsys/pkg/PLAW
109publ171/pdf/PLAW109publ171.pdf• FDA Memorandum, Dear Infection Control Professionals. Available at: www.fda.gov/MedicalDevices/Safety/AlertsandNotices/
ucm220459.htm Accessed July1, 2013• Hadaway L. Technology of flushing vascular access devices. J Infus Nurs. 2006; 2913745• Infusion Nursing Standards of Practice, Journal of Infusion Nursing, Volume 34, Number 1S ISSN 15331458. Revised 2011.• Jarvis W, Choosing the Best Design for Intravenous Needleless Connector to Prevent HABSI. Infection Control Today. August 2010 Vol.
14 No 8• Macklin D, What’s Physics Got to Do With It? J Vasc Access Devices. 1999;4(2): 713.• Marschall J, Mermel LA, Strategies to Prevent Central Line – Associated Bloodstream Infections in Acute Care, Infection Control and
Hospital Epidemiology, vol. 29, Supplement 1, October 2008.• McKnight S Nurse’s Guide to Understanding and Treating Thrombotic Occlusions of Central Venous Access Devices. Medsurg Nurs.
2004; 13:37782• Morbidity and Mortality Weekly Report, Vital Signs: Central Line–Associated Blood Stream Infections — United States, March 1, 2011,
Vol. 60• National Patient Safety Goals, Joint Commission, 2013. Accessed 5/10/2013 at: www.jointcommission.org/assets/1/18/NPSG_Chapter_
Jan2013_HAP.pdf• O’Grady NP, Alexander, M, Burns LA, et a. Guidelines for the Prevention of Intravascular CatheterRelated Infection, Centers for Disease
Control and Prevention, 2011 • Poole S. Central Line Infection: Improving our Surveillance, Treatment and Prevention in the Home Setting. Infusion Mar/Apr 2009. • Potera C, Biofilm Dispersing Agent Rejuvenates Older Antibiotics. Environmental Health Perspectives 2010; 118; A288• Premier Advisor Live® Hospital valuebased purchasing program: What’s in the new CMS proposed rule? 2011, Accessed 7/1/2013 at:
www.premierinc.com/advisorlive/Presentations/vbp011911.pdf• Ryder M. Needleless Connectors…minimizing the risk of bacterial transfer. Accessed 2/28/14 at: www.ncqualitycenter.org/wp
content/uploads/2013/01/Tenn_web.pdf• Sinno M, Alam M, Echocardiographically Detected Fibrinous Sheaths Associated with Central Venous Catheters. Echocardiography.
Mar2012, Vol. 29 Issue 3, pE56E59. • Timsit JF, Misset B, CarletJ, Central Vein CatheterRelated Thrombosis in Intensive Care Patients: Incidence, Risk Factors, and Relationship
with CatheterRelated Sepsis. Chest 1998; 114;207213.• Wallis M, McGrail M, Webster J. et. al. Risk factors for PIV catheter failure: a multivariate analysis of data from a randomized controlled
trial. Infection Control & Hospital Epidemiology. Under review. • Hunter M. VonBriesen T, Faintuch S. Impact of blood reflux on the incidence of catheter occlusions – A controlled experimental trial.
37th National Canadian Vascular Access Association Conference, 2012

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition30
NOTES:

Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
2014 NHIA Annual Conference & Exposition 31
NOTES:
Answers:1. a. True2. a. True3. a. True4. d. All of the above5. b. False
32 2014 NHIA Annual Conference & Exposition
Blood Reflux: Backflow, Biofilm, and Slime—Oh My!
Recommended

















