BIOAVAILABILITY
Dr. JEEVAN JACOBJunior ResidentDept. of Pharmacology


Definition
“The rate and extent to which the active ingredient or active moiety is absorbed from a drug product and becomes available at the site of action”
US FDA Code of Federal Regulations Title 21, 320.1(a)

Bioavailable fraction (F), refers to the fraction of administered dose that enters the systemic circulation in unchanged form
F = Bioavailable dose Administered dose

Factors affecting Bioavailability of a Drug
1.Pharmaceutical Factors
2. Pharmacological factors

Pharmaceutical Factors
Drug administered
DISINTEGRATE
DISSOLVE
Gets Absorbed
Tab/ cap
Powders & Suspensions

These depends on Particle size - smaller the size, faster the dissolution
and thus the absorptionE.g. Microfined Aspirin
Form - Amorphous form gets absorbed faster
than crystalline formE.g. Amorphous Chloramphenicol

•Degree of Ionization - Unionized form penetrates the GI mucosal lining quickly
Weakly acidic drugs: Aspirin, Barbiturates→ Stomach, duodenum Weakly basic drugs: Pethidine, Ephedrine→ Small intestine
Strongly acidic / basic drugs: Highly ionized & poorly absorbed

Salt Form- Gets absorbed fasterE.g. Phenytoin Sodium
Water of hydration- anhydrous forms gets absorbed
faster

Nature of Excipients and Adjuvant
-They are used as filling materials-Binding agents or to get target
size
Eg. Lactose, Polysorbate 80 etc are wetting agents which enhance solvent penetration in drug particles and minimize aggregation of particles

Outbreak of Phenytoin toxicity in epileptic patients in Brisbane, Australia during 196850 Pts developed Phenytoin toxicity
In them the blood phenytoin levels were above the therapeutic range.
The excipient in the responsible phenytoin capsules had been changed several months before the outbreak
This change was probably causing the altered blood phenytoin concentrations.

Pharmacological FactorsGastric Emptying and GI motility- Faster the Gastric Emptying,
faster it reaches the small Intestine with large surface area
- by Fasting, anxiety Hyperthyroidism
- by Fatty diet, Depression, Anticholinergic drugs

Gastro Intestinal disease
Eg. Celiac Sprue - Malabsorption of fat
Amoxicillin absorptionCephalexin absorptionAmpicillin absorption

Gastro Intestinal disease
Eg. Crohn’s Disease
TMP absorptionSMX absorption

Food-Usually empty stomach favors
absorption-Some drugs like Griseofulvin,
absorption is enhanced by Fatty meal
-Vitamin C ↑ Iron absorption, Phytates retard it
- Calcium ↓ absorption of Tetracyclines

Drug Interaction
-Liquid Paraffin Emulsifies fat and thus decrease absorption of Vitamins ADEK
-Antacids with Ca, Mg, Al etc can reduce the BA of Tetracyclines

First pass metabolism
• Gut wall (e.g. Isoprenaline)• Liver (e.g. Opoids, ß-blockers,
Nitrates)

Pharmacogenetic FactorsGenetically mediated variations in
drug response
Eg. G6PDH deficiency causes hemolysis with Oxidant drugs like Primaquine,INH, Nalidixic acid, Menadione etc

Pseudo cholinesterase deficiency causes prolonged apnoea with Succinyl choline
Acetylator polymorphism
FAST ACETYLATORS
SLOW ACETYLATORS
SHIP – Sulfa, Hydralazine, INH, Procainamide

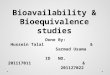
Representation of Bioavailability Data
Cmax
Tmax
AUC
time
concentration

22
Representation of Bioavailability Data
Construction of plasma concentration vs time curve.
Initial rise in curve indicates that drug is absorbed at a faster rate than it is metabolized or excreted. (absorption phase)
It continues to rise until a peak conc. is obtained (Cmax) - rate of absorption = rate of excretion.

23
Representation of Bioavailability Data(cont’d)
At the beginning of the descending portion of the curve, both absorption and elimination is taking place - elimination is faster.
After a time absorption ceases and the conc. of drug in plasma is determined only by the rate of elimination. (the elimination phase of the curve)

24
Absolute bioavailability
It is measured by comparing the area under the drug concentration–time curve after extravascular administration to that after IV administration

25
IV bolus
0 5 10 15 20 25 300
20
40
60
80
100
Time
Concentration Area under
concentration curve (AUC)

26
0 5 10 15 20 25 300
20
40
60
80
100
Time
Concentration
Oral dosage form
Area under concentration curve
(AUC)

27
Absolute bioavailability
0 5 10 15 20 25 300
20
40
60
80
100
Time
Concentration
For the same dose (IV vs. Oral), the bioavailability is given by:
IV
oral
AUC
AUCF

28
Relative bioavailabilityThe relative bioavailability is the
systemic availability of a drug product (A) compared to another drug product (B).

29
0 5 10 15 20 25 300
20
40
60
80
100
Time
Concentration
Oral dosage form (product A)
Area under concentration curve
(AUC)

30
0 5 10 15 20 25 300
20
40
60
80
100
Time
Concentration
Oral dosage form (product B)
Area under concentration curve
(AUC)

31
0 5 10 15 20 25 300
20
40
60
80
100
Time
Concentration
Relative bioavailability
For the same dose (IV vs. Oral), the bioavailability is given by:
)(
)(
BAUC
AAUCF
oral
oral

32
Measurement of bioavailability
Pharmacokinetic methods ( indirect ) 1. Blood analysis 2. Urinary excretion data
Pharmacodynamic methods ( direct ) 1. Acute pharmacological response 2. Therapeutic response

33
1.Blood analysis The plasma concentration – time curve
A direct relationship exists between the concentration of drug at the site of action & concentration of drug in the plasma.
Serial blood samples are taken after drug administration & analyzed for drug concentration.

34

35
Parameters determined
Peak Plasma Concentration (Cmax)
Time of Peak concentration (tmax). Area Under Curve (AUC)
Minimum Effective Concentration (MEC) Maximum Safe Concentration (MSC) Onset of action. Duration of action
Pharmacokinetic parameters
Pharmacodynamics parameters

36
AUC or Extent of absorption can be measured by many methods…
1.Planimeter Instrument for mechanically measuring the area
2. Cut & weigh method AUC is cut & weighed on analytical balance. The weight
obtained is converted to proper unit by dividing it by the weight of a unit area of same paper.

3. Trapezoidal method
4. Plotting Graph on Rectilinear graph paper
5. Using a Transparency with a preprinted grid

AUC2-3 = Cp2 + Cp3 x (t3 - t2)
2
AUC: Trapezoidal Rule

39
2. Urinary excretion data
The is another method of determination of bioavailability provided that the active ingredient is excreted unchanged in the significant quantity of urine.
The cumulative amount of active drug excreted in urine is directly proportional to extent of systemic drug absorption.
The rate of drug excretion is directly proportional to rate of systemic drug absorption.

40
Advantages of Urinary excretion data
Useful when there is lack of sufficiently sensitive analytical techniques to measure concentration of drug in plasma.
Noninvasive method therefore better subject compliance.
Convenience of collecting urine samples in comparison to drawing of blood periodically.
If any case the urine drug concentration is low, assaying of larger sample volume is done.
Direct measurement of bioavailability, both absolute & relative is possible

41

42
Bioavailability is determined by….
F = (U ) oral . D IV (U ) IV . D oral
U = Cumulative amt of unchanged drug excreted in urine D IV = IV dose
D oral = oral dose
F = absolute bioavailability

Pharmacodynamic methods ( direct )
1. Acute pharmacological response 2. Therapeutic response
43

1. Acute pharmacological response
Bioavailability can be determined from the acute pharmacologic effect – time curve as well as from dose response graph.
E.g.: pupil diameter, heart rate or BP can be useful as an index of drug bioavailability
DISADVANTAGE is that pharmacological response tends to be more variable and thus accurate correlation between the measured response and drug available from the formulation is difficult

45
2.Therapeutic response
This method is based on the observing the clinical response to a drug formulation given to a patients suffering from disease for which it is intended to be used.
Eg. For anti inflammatory drugs, the reduction in the inflammation is determined.
The major DRAWBACK is quantification of observed response is too improper to allow for reasonable assessment of relative bioavailability between two dosage forms of a same drug.

BIOEQUIVALENCE“Two preparation of drug are
considered bioequivalent when the rate and extend of bioavailability of active drug from other is not significantly different under suitable condition”

So if the plasma level profiles of two dosage forms of same drug are comparable and super imposable
And their BA difference is not more than 20-25%

Chemical EquivalenceIf two or more dosage forms of
same drug contain same labeled quantities of drug as prescribed in pharmacopeia, they are chemically equivalent
E.g. Dilantin and Eptoin

Clinical EquivalenceTwo drugs are said to be clinically
equivalent if they provide identical in vivo pharmacological response
E.g. Dilantin and Eptoin

Therapeutic EquivalenceIf structurally different drugs can
provide same therapeutic response as another drug, then they are called therapeutically equivalent
Eg: Trifluperazine { Phenothiazine } may be TE to Haloperidol { Butyrophenol } in treating schizophrenia

ReferenceEssentials of Medical Pharmacology,
7th Ed. KDT
Principles of Pharmacology, 2nd Ed. Sharma & Sharma
Text book of Medical Pharmacology,1st Ed.Srivastava
www. fda. gov

THANK YOU
Recommended